
Abstract
Objective:
Diabetes affects more than 29 million individuals in the United States, resulting in healthcare costs approaching $245 billion. Approximately 15% of these individuals will develop a chronic, non-healing foot ulcer (diabetic foot ulcer [DFU]) that, if untreated, may lead to amputation. The current treatments for DFU are expensive, have significant side-effects, and often result in non-compliance. A new topical treatment is described that accelerates cutaneous wound repair and is disease modifying by targeting underlying aberrant diabetic pathways.
Approach:
The efficacy of naltrexone (NTX), an opioid receptor antagonist, and Regranex® was compared in preclinical studies using type 1 diabetic rats. Dorsal cutaneous wounds were treated topically with 0.03% NTX, Regranex, or moisturizing cream alone. Wound closure, DNA synthesis, and cytokine production were monitored.
Results:
Wound closure rates with topical NTX in type 1 diabetic rats were comparable to Regranex. Topical NTX accelerated DNA synthesis, as measured by BrdU incorporation, increased mast cells, and enhanced expression of platelet-derived growth factor (PDGF) and vascular endothelial growth factor (VEGF), a marker for angiogenesis. Regranex had little effect on DNA synthesis, mast cells, and VEGF expression relative to vehicle-treated wounds, and it only temporarily increased PDGF expression. Fibroblast growth factor expression was not altered by either treatment.
Innovation:
Topical application of 0.03% NTX cream accelerates diabetic wound closure.
Conclusion:
Blockade of the opioid growth factor (OGF)-OGF receptor (OGFr) axis utilizing 0.03% NTX cream is comparable to standard care in preclinical studies, and it provides a safe, inexpensive, and effective alternative for treatment of diabetic wounds.

Introduction
M
The processes underlying wound healing are dynamic and culminate in the restoration of proper anatomical function of the tissue. 8,9 Wound closure occurs as a continuum of overlapping phases that involve re-epithelialization, inflammation, proliferation, and formation of granulation tissue during remodeling. Each phase is initiated by cytokines and growth factors, 7,10,11 and the secretion and expression of these cytokines appears to be compromised in hyperglycemic individuals and animals, leading to delayed cell replication. 9 –15 Many of the current therapies used for the treatment of DFU provide topical application of a cytokine or growth factor, 10 –12 but they are not disease-modifying treatments that address underlying defects related to diabetes. Regranex® is an FDA-approved standard of care for DFUs. 16 Preclinical and clinical studies have demonstrated that the active ingredient of platelet-derived growth factor (PDGF) is effective in wound restoration after topical application. 17 –19 However, this therapy is expensive and associated with side-effects and warnings that prevent extended usage. There remains a need for new alternative treatments for chronic, non-healing wounds.
The novel therapy discussed in this study is safe, inexpensive, effective, and targets one of the underlying dysregulated pathways in diabetes. The therapy utilizes topical application of the opioid antagonist naltrexone (NTX) to block the opioid growth factor (OGF)–OGF receptor (OGFr) regulatory pathway. Preclinical studies have shown that this small-molecular-weight compound (377 MW) can be dissolved in a carrier and topically applied to full-thickness wounds to accelerate repair of cutaneous wounds in type 1 diabetic rats, as well as in type 2 genetically diabetic mice (db/db). 13 –15 As an opioid receptor antagonist, NTX lacks intrinsic biological activity and works by blocking interactions between an inhibitory peptide and its receptor. 20,21 The mechanism of action involves extended blockade of the OGF-OGFr regulatory pathway 22 that has been reported to be dysregulated in diabetes, leading to overexpression of the inhibitory peptide, OGF, chemically termed [Met 5 enkephalin]. OGF levels are elevated in diabetic humans and animals, leading to downregulation of cell proliferation and renewal processes in wound healing. 23 –25 Total opioid receptor blockade by NTX restores the proliferating homeostasis required for tissue repair. 13 –15,22,26 –29
In this preclinical study, a comparison of effectiveness was made between the new NTX formulation (0.03%) and Regranex applied once daily for the treatment of cutaneous wounds in type 1 diabetic rats. In addition to cell replication, the appearance of mast cells as a marker of inflammation, and the expression of cytokines including vascular endothelial growth factor (VEGF), PDGF, and fibroblast growth factor (FGF) were evaluated for both therapies.
Clinical Problem Addressed
A major complication of diabetes is delayed closure of full-thickness cutaneous wounds. The standard of care therapy, Regranex, works by increasing PDGF. Regranex is expensive and associated with severe side-effects, including cancer, and even death. An alternative therapy is NTX. It is FDA approved for systemic use, and it is safe and effective after topical application to full-thickness wounds in preclinical studies. NTX is a disease-modifying therapy that targets the underlying diabetic pathophysiology by blocking elevated enkephalin levels and their OGFr receptors to enhance cell replication at all stages of wound remodeling. In this comparison study with the standard care treatment, NTX effectively accelerates wound closure in type 1 diabetic rats by upregulating wound remodeling factors. These data support clinical investigations for topical NTX treatment.
Materials and Methods
Animals and induction of diabetes
Adult male Sprague-Dawley rats (Charles River Laboratories, Wilmington, MA) that were 6 weeks of age were housed in AAALAC-approved facilities, with water and food (2018 Global Rodent Diet, Teklad®, Indianapolis, IN) provided ad libitum. All animals were treated humanely; experimental protocols were approved by the Institutional Animal Care and Use Committee at Penn State University College of Medicine and conformed to guidelines of the National Institutes of Health.
At 6 weeks of age, rats were rendered hyperglycemic by two consecutive injections (i.p.) of 40 mg/kg streptozotocin (STZ; Sigma, St. Louis, MO) that were dissolved in citrate buffer (pH 4.5). Normal rats received only i.p. injections of citrate buffer. This regimen produced insulin-dependent type 1 diabetes within 4–5 days. Although this model of hyperglycemia and subsequent delayed wound healing does not mimic the long-term chronic, pressure wounds associated with human diabetes, the model lends itself to a study of mechanism and therapeutic response. 30
Body weights were recorded periodically. Blood glucose measurements were taken by using a True Track Smart System glucometer (Home Diagnostics, Ft. Lauderdale, FL). Three independent experiments were performed over a period of 9 months; each experiment had ∼15 rats rendered hyperglycemic. In each experiment, rats remained hyperglycemic (blood glucose >350 mg/dL) for 5 weeks before the study without insulin supplementation. At the start of each experiment if the rat had blood glucose measurements greater than 600 mg/dL or appeared lethargic and unwilling to eat, the animal was not included in the experiment.
Cutaneous wound surgery
Full-thickness cutaneous wounds were created as previously described. 13,14 In brief, on the day before surgery, the dorsum of each rat was shaved by using an electric razor followed by application of Nair® to remove all hair. Rats were humanely anesthetized by an i.p. injection of a mixture of ketamine (50 mg/kg; Ketaject®), xylazine (5 mg/kg; TranquiVed®, Vedco), and acepromazine (1 mg/kg; acepromazine maleate; Vedco). Four excisional circular (6 mm diameter) skin wounds were created 1 cm off the midline on each rat under sterile conditions. Wounds were created to the level of the panniculus muscle by using disposable biopsy punches (Accuderm), swabbed with an antiseptic surgical scrub, and left without dressing. All surgeries were conducted between 08:00 and 11:00 h to alleviate the potential effects of diurnal rhythm.
Wound treatment and closure
Topical treatment of wounds with NTX, Regranex, or vehicle was randomized for each rat to control for placement of wound and treatment response. NTX was dissolved in sterile saline (v/v) for a final dosage of 0.03% NTX in Neutrogena moisturizing cream, 0.1 mL sterile saline was dissolved in Neutrogena cream, and Regranex was used directly from the pharmaceutical-grade tube. Each formulation was applied once daily (1 × ) at 09:00 h. The fourth wound received one of the treatments in a random manner.
Residual wound sizes were visualized at 20 × magnification by using a Nikon Coolpix L820 camera mounted on an Olympus BH2-RFCA microscope and photographed by using Spot Advanced software; the digital camera was placed on a stable tripod located ∼15 cm above the animal. Measurements were calibrated with a ruler photographed adjacent to the wounds. Animals were sedated in a regulated vaporizer with a 2.5% isoflurane-oxygen mixture, and photographs were taken immediately after surgery (day 0) and every other day for 2 weeks. Areal analysis of each wound was performed by using Image J software, and the percent area of residual defect was calculated.
BrdU labeling and DNA synthesis
To assess cell replication, rats were injected with bromodeoxyuridine (100 mg/kg, 0.2 mL BrdU; Sigma-Aldrich) at 6 and 3 h before euthanasia on day 4. Tissue sections were stained with anti-BrdU antibody (1:50; Invitrogen) that was tagged with streptavidin (1:2,000; Invitrogen) and counterstained with hematoxylin. BrdU-labeling indexes were determined as the percentage of positive BrdU-labeled basal epithelial cells per total basal epithelial cells lateral to the wound site.
Quantitative immunohistochemistry
On days 1, 2, and 4 after initial surgery, rats were humanely euthanized and a 3-cm2 region of skin encompassing the original wound was removed. At least 6 wounds/treatment group were bisected, fixed in 10% neutral buffered formalin, and processed for paraffin embedding. Skin sections (10 μm thick) were stained with hematoxylin-eosin for a general assessment of toxicity and pathology. Early inflammation was examined by mast cell proliferation in paraffin sections that were stained with 0.04% toluidine blue and counter-stained with fast green. Angiogenesis was monitored by expression of VEGF immunohistochemical staining with polyclonal antibodies to VEGF (1:200, sc-152; Santa Cruz). 31,32 In addition, PDGF and FGF-2 cytokines were evaluated by immunohistochemical staining with polyclonal antibodies to PDGF (1:75, Ab21234; Abcam, Cambridge, MA) and FGF-2 (1:500, Ab106245; Abcam, Cambridge, MA); all primary reactions were followed by staining with goat anti-rabbit (1:1,000; ThermoFisher) secondary antibodies. Antibody retrieval was completed by placing slides in a pressure cooker for 3 min in sodium citrate buffer or EDTA buffer.
DNA-labeling indexes were determined by counting cells incorporating BrdU divided by the total number of cells. Mast cell number and cytokine expression were quantitatively assessed by counting the number of positively stained cells within a grid. Inasmuch as possible, an individual masked to the treatment group counted and recorded the data. In general, 3–4 sections from 3–5 wounds per treatment group were evaluated.
Statistical analysis
Body weights and glucose measurements were evaluated by using the Student's two-tailed t-test. Residual wound areas, epithelial thicknesses, and BrdU-labeling indexes were analyzed by using analysis of variance (ANOVA), with subsequent planned comparisons made with Newman-Keuls tests. A statistical power analysis for the number of wounds treated, as well as the number of sections per wound required for morphological reliability, was based on previous experiments.
Results
Body weight and blood glucose measurements
The mean weight of all male rats was 170 ± 2 g at the start of experimentation. Approximately 6 weeks after STZ injection, the diabetic animals weighed 324 ± 7 g in comparison to normal controls weighing 399 ± 18 g. Diabetic rats had significantly elevated blood glucose levels within 2–3 days of STZ injections (∼540 mg/dL), and by the initiation of wound surgery, glucose levels in the type 1 diabetic (DB) rats were 563 ± 12 mg/dL in comparison to normal, non-diabetic rats with glucose levels of 124 ± 6 mg/dL.
Full-thickness wound closure
Overall analyses of wound closure indicated that wounds in diabetic rats healed more slowly (at least p < 0.05) than those in normal animals. A comparison of Regranex and NTX treatments in type 1 diabetic rats revealed that both treatments accelerated wound closure (Fig. 1). An evaluation of residual wound size over a 14 day period demonstrated that within 48 h of treatment, wound sizes in the DB/R and DB/NTX groups were smaller than those in the DB/Vehicle group, with the mean DB/R group reaching statistical significance. At 4, 8, and 10 days, both treatment groups had wound areas that were significantly smaller than those in the DB/Vehicle group. By day 12, the DB/NTX group was statistically smaller, although the wound size was virtually negligible. At no time did the DB/NTX and DB/R groups demonstrate differences in residual wound size or rates of closure.

Wound closure is accelerated by treatment with topical NTX or Regranex®.
Histopathology and immunohistochemical studies
Hematoxylin- and eosin-stained sections of wounds did not show significant cell death or structural pathology in response to treatment with either 0.03% NTX or Regranex.
DNA-labeling indexes
Given that most of the processes involved with wound closure require cell replication, levels of DNA synthesis were evaluated to determine the mechanism of action for NTX and Regranex (Fig. 2). Evaluation of wounds from normal rats treated with vehicle revealed BrdU-labeling indexes of 47.6% ± 3.5% in comparison to those with 29.3% ± 1.9% DNA incorporation in diabetic rats receiving vehicle. However, BrdU incorporation in wounds of diabetic rats receiving NTX demonstrated 41.9% ± 2.3% labeling, a 43% increase over DB/Vehicle rats (p < 0.001), and comparable to that of normal animals. Regranex treatment had little effect on cell proliferation as the DNA synthesis rates were 21.0 ± 3.6, nearly 50% less than NTX treatment.
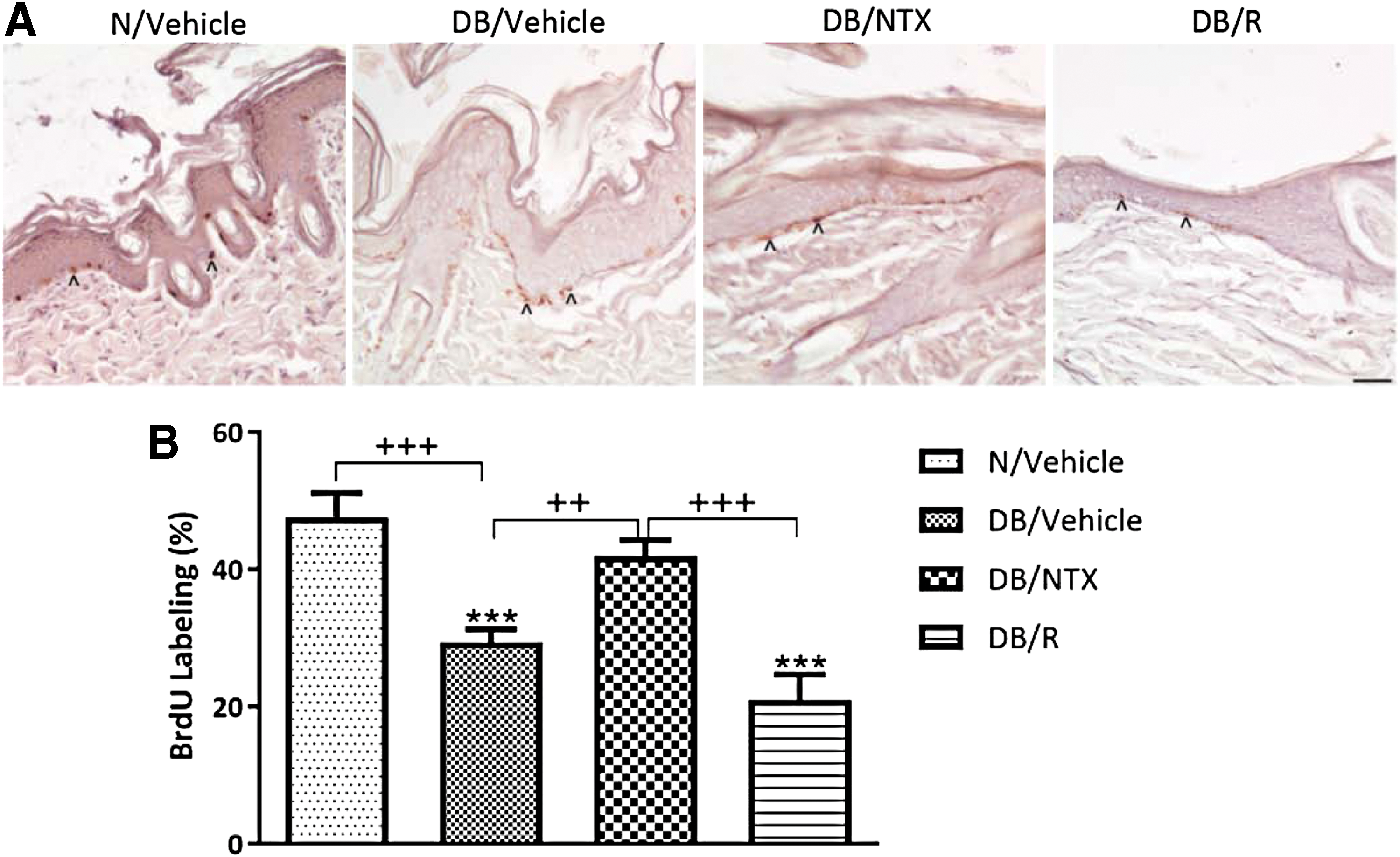
Cell proliferation in the basal epithelial layer of renewed skin.
Mast cell number
Total numbers of mast cells per mm2 of granulation tissue were determined from grid counts on day 1 (Fig. 3). Within 24 h of injury, the overall mast cell number was diminished in the skin of T1D rats, but tissue treated with NTX demonstrated more mast cells than either vehicle-treated or Regranex-treated skin (p < 0.05).
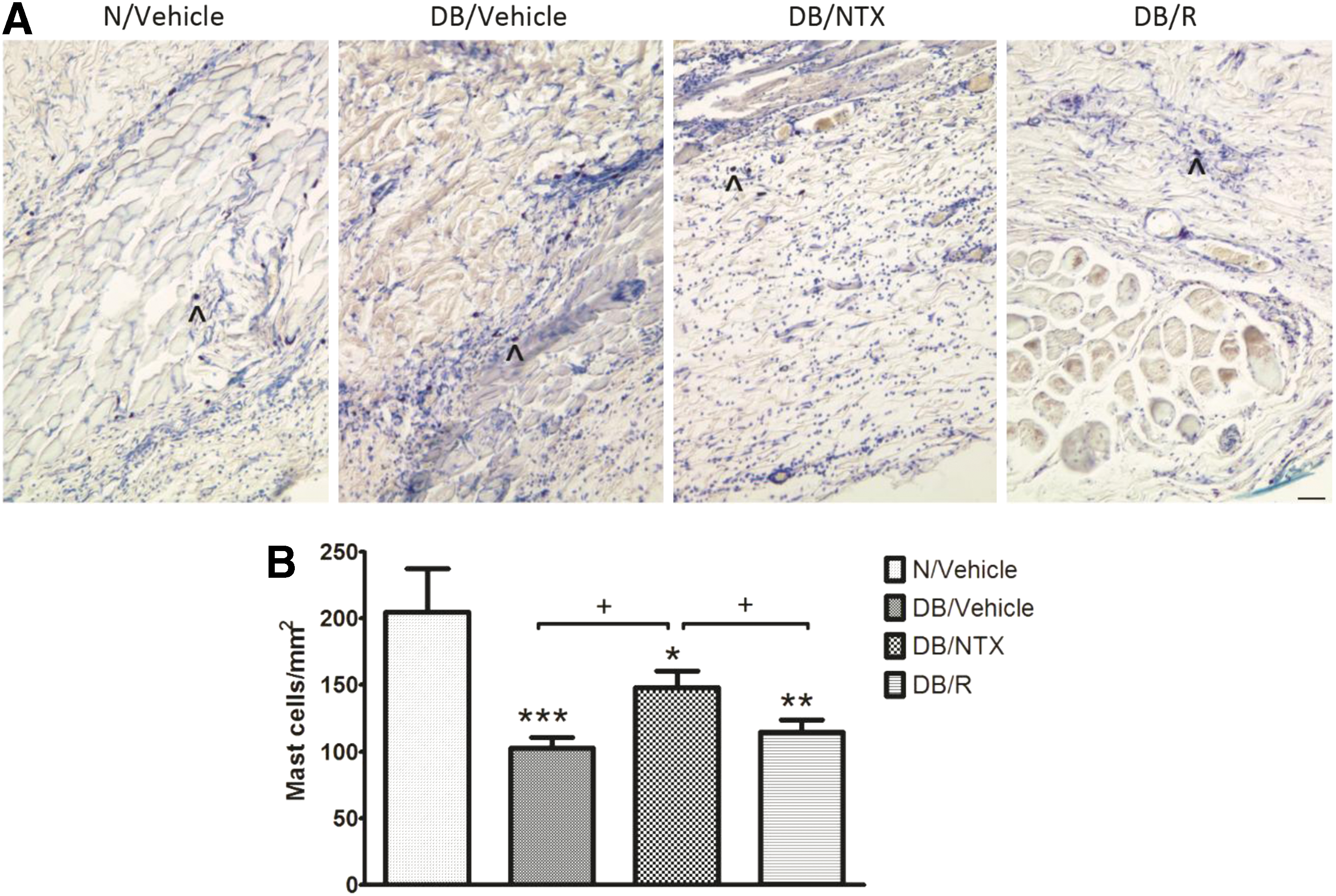
Mast cell proliferation and infiltration into the wound bed was assessed 1 day following wounding.
PDGF expression
Positively stained PDGF cells were located at the edge of the wound and deep in the wound matrix, embedded within the granulation tissue. Cells were counted within a grid and presented as the number of cells per mm2. Within 1 day of treatment, groups of DB animals receiving either Regranex or NTX had more than 1.5-fold (p < 0.01) PDGF+-stained cells than vehicle-treated wounds. The elevation in PDGF+ cells continued on day 2 and day 4, whereas Regranex treatment had no further effect, and levels returned to those observed in the DB/Vehicle rats (Fig. 4).
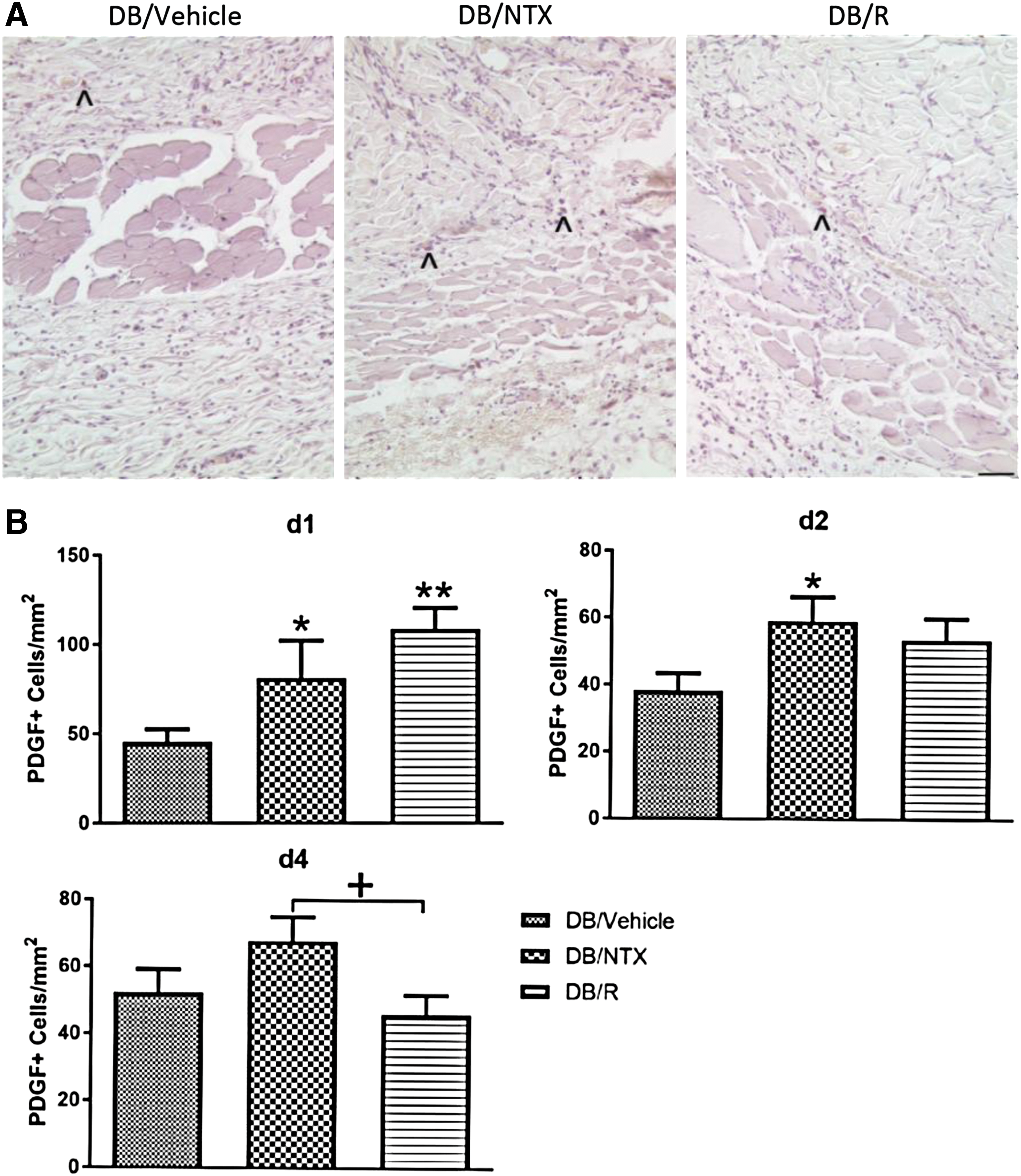
PDGF expression in full-thickness skin wounds from type 1 diabetic (DB) rats receiving daily treatment of a single drop of 0.03% NTX (DB/NTX) or saline (DB/Vehicle) dissolved in moisturizing cream, or Regranex (DB/R) for 1, 2, and 4 days.
VEGF expression
The percentage of VEGF-positive stained blood vessels on day 4 was 43% more for the NTX-treated group relative to diabetic controls (Fig. 5). Nearly 60% of all vessels in the NTX-treated group were positive for VEGF, relative to less than 40% of the vessels being VEGF positive in either the control or Regranex-treated rats.
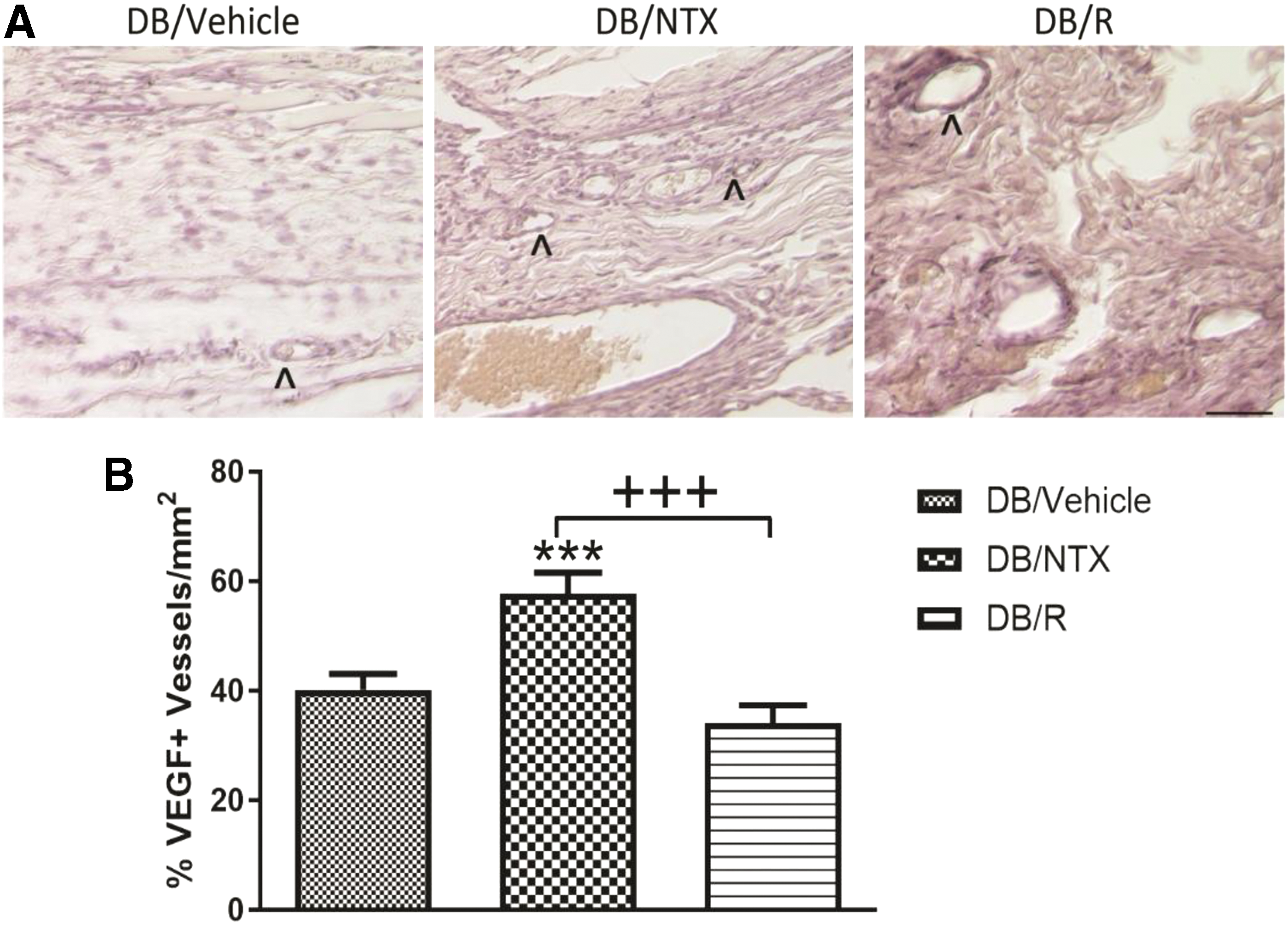
VEGF expression in
FGF-2 staining
After wounding and initial mast cell infiltration, cytokines, including FGF-2, PDGF, and VEGF, are detected circulating in the blood. FGF-2 cytokines are at the highest levels within 24 h of wounding. Examination of tissue surrounding the wound on days 1, 2, and 4 revealed that FGF staining was comparable among all treatment groups on all days examined.
Discussion
Delayed wound healing is a major complication associated with diabetes, particularly uncontrolled, and/or chronic diabetes such as that associated with T2D. Pressure-related wounds and DFUs affect nearly half of all people with diabetes at some point in their lifetime. In addition to the disabling side-effects of unhealed wounds, the diabetic patients become more vulnerable to infections that may, in fact, lead to more serious medical conditions requiring amputation. 1 –3 Previous studies in our laboratory have defined mechanisms that relate to reversing delayed wound repair, particularly in type 1 diabetic rats. 13 –15 These preclinical studies have demonstrated that topical application of NTX enhances epithelial cell replication, angiogenesis, and increases cytokine profiles related to healing skin. 13,14 In these studies, treatment with NTX decreased residual wound sizes by as much as fivefold relative to rats receiving three applications of vehicle only. DNA synthesis experiments revealed that epithelialization was accelerated, as was blood vessel formation. These preclinical studies were also confirmed in a mouse model of T2D. 33 The db/db mouse was surgically wounded and 10−5 M NTX dissolved in moisturizing cream was applied three times daily. Wound size was markedly reduced relative to diabetic mice receiving saline in cream. This work corroborates studies on corneal surface epithelialization where topical NTX dissolved in Vigamox® enhanced the healing of corneal abrasions in type 1 diabetic rats and rabbits, as well as in type 2 diabetic mice. 34,35
In the present study, a novel formulation and regimen was used. NTX was dissolved in moisturizing cream at 0.03%, and the application was once daily, rather than three times daily as previously published. 13,14 The results with one application of 0.03% NTX correlated well with those reported for three daily applications of 10−5 M NTX. 13 –15 In comparison to Regranex, wound healing was comparable in the type 1 diabetic rat and both treatments accelerated wound closure relative to rats receiving vehicle. Moreover, NTX targeted an underlying mechanism associated with diabetic complications by blocking the overexpression of OGF and its interfacing with OGFr to inhibit cell replication, resulting in delays in many phases of wound remodeling. BrdU labeling of the diabetic rats demonstrated that topical 0.03% NTX accelerated DNA synthesis and epithelial replication relative to both Regranex treatment and vehicle controls.
Early mast cell proliferation and/or migration into the wound bed were evident in NTX-treated tissues. These data corroborate earlier reports of enhanced mast cell number at 5 and 8 days 14 after NTX treatment and support the role of NTX to mediate both infection and inflammatory processes.
An evaluation of cytokine expression demonstrated that NTX also elevated VEGF expression, whereas Regranex had no effect on this angiogenesis marker. Both Regranex and NTX increased PDGF expression, and NTX extended the enhanced expression for 48 h relative to the effects recorded after Regranex treatment that lasted only 1 day. FGF-2 expression did not change, at least at the time points evaluated in these experiments.
These findings corroborate and extend our work on wound repair in type 1 and type 2 diabetic animals 36 that not only showed efficacy and safety of topical NTX but also supported our hypothesis that NTX is a disease-modifying therapy. In vitro studies with fibroblasts demonstrated that NTX was selectively blocking the OGFr to enhance cell replication. 37 Other selective opioid receptor antagonists, as well as other opioid agonists for mu, delta, and kappa receptors did not enhance cell replication, and specific receptor antagonists had no effect on enhancing wound closure in diabetic rats. 37
The present investigation utilizes a new preclinical formulation and dosage of NTX to demonstrate that continuous blockade of the OGF and OGFr regulatory pathway is an effective therapy for non-healing cutaneous ulcers in diabetes. The new formulation of 0.03% NTX applied topically once daily substantiates an alternative, effective therapy for DFUs and lends support for clinical trials. Given that the U.S. population with diabetes is approaching 29 million, and that there are 86 million individuals with pre-diabetes, 1 there is an urgent need to develop safe, inexpensive, and effective treatments for one of the many complications associated with the chronic disorder.
Innovation
The novel formulation and dosage of NTX, an opioid receptor antagonist, for topical treatment of diabetic cutaneous wounds is innovative. NTX is a disease-modifying therapy that blocks the interfacing of elevated inhibitory opioid peptides (OGF) associated with diabetes with its receptor (OGFr) to facilitate wound healing. NTX should be safe for topical administration as it is approved for chronic systemic administration. As a repurposed medication, NTX should be relatively inexpensive. This comparative preclinical study demonstrates that 0.03% NTX targeted underlying mechanisms of delayed diabetic wound healing and was as effective in healing cutaneous wounds as the standard of care.
• Topical application of NTX heals full-thickness cutaneous wounds at a rate comparable to standard care with Regranex.
• Topical NTX increases DNA synthesis in basal epithelial cells of the skin, whereas Regranex has little or no effect on cell replication.
• Topical NTX, but not Regranex, increases angiogenesis (number of VEGF+-stained vessels).
• Topical NTX is a disease-modifying therapy that blocks the inhibitory activity of heightened OGF levels with the specific receptor OGFr.
• Preclinical data support proof-of-concept clinical trials using topical NTX as a safe, effective, and inexpensive alternative for the treatment of diabetic foot ulcers.
Footnotes
Acknowledgments and Funding Sources
Work was supported, in part, by private funding to the laboratories of Drs. Zagon and McLaughlin.
Author Disclosure and Ghostwriting
No ghostwriting was involved. Drs. Zagon, Sassani, and McLaughlin hold a U.S. patent related to naltrexone composition for wound healing, but they receive no financial income. There are no other disclosures related to any author.
About the Authors