
Abstract
Objective:
The aim of the study was to illustrate the differences in the cost-to-heal wounds using two methods: (1) reimbursement-based costing and (2) activity-based costing (ABC).
Approach:
A small cohort (100 patients with multiple wounds of which 1 was a diabetic foot ulcer [DFU]) was randomly selected from the U.S. Wound Registry to be representative of all patients with DFUs in the registry. Unit costs, resource utilization, and total costs were estimated through both methods. For the ABC method, costs were calculated in ranges: low, mid, and high.
Results:
The mean cost to heal through the reimbursement-based costing method was US$20,618 compared with a range of US$18,627–US$35,185 for the ABC method. About 20% of DFUs that cost US$10,000–US$20,000 to heal with the reimbursement-based costing method shifted to much higher values based on the ABC method. The percentage of costs represented by inpatient procedures was much lower for the reimbursement method compared with the ABC method.
Innovation and Conclusions:
The results show that (1) the “true” cost-to-heal DFUs strongly depend on the method used to calculate the costs, and (2) the reimbursement-based costing method may not accurately reflect real costs. The concept of aggregating episodes of care to obtain a single value equating to cost to heal is likely to remain a challenging exercise for the foreseeable future. A better approach may be to provide a range of cost values that are dependent on specific methods, such as the ABC method.
Marissa J. Carter, MA, PhD

Introduction
S
If we wish to ascertain the complete cost-to-heal wounds in aggregate (such as those wounds treated at a hospital outpatient wound care provider-based department [PBD]), all wounds must be included; certain wounds cannot be arbitrarily excluded, as is common in retrospective outcome studies. Examples of wounds that are often excluded include one-time consultations, wounds treated for many years, patients who fail to return, treatment failures such as amputations, or wounds still being treated when a patient dies. 12,13
Episode-of-care costs are different from charges to payers and reimbursement from governmental and/or private payers. 14 In general, episode-of-care costs represent the financial expense of providing a service for a specific condition or medical problem by providers throughout the continuum of care. Charges are the actual amounts billed to the patient or to the patient's medical insurance entity. Reimbursement is the amount of money paid for the service/procedure/product to the provider by the patient's medical insurance entity and/or the patient. The difference between the charges and reimbursement is known as the payment-to-charge ratio (PCR). 15
When research has been conducted to compare true resource cost versus the Centers for Medicare and Medicaid Services (CMS) approach to determining PCRs in acute care hospital stays and in PBDs, the results of some studies suggest that the care setting is not the real issue. 16,17 Although most health economists agree that activity-based costing (ABC) is the “gold standard” for calculating health care costs, how health care providers and payers (such as CMS) calculate episode-of-care costs depends on many factors, such as business models, geography, labor practices, catchment populations, and training/teaching practices, but to name a few. 16
The biggest concerns today are lack of ABC adoption, how to allocate indirect costs, and price transparency. 18 These concerns revolve around the difficulty in allocating direct costs (in this case, personnel and treatment costs related to wound care) versus indirect costs, which represent the cost of running the health care provider organization in terms of resources used to provide wound care.
Problem Addressed
This study was designed to illustrate the cost to heal a wound as calculated by the ABC method versus the reimbursement-based costing method.
Materials and Methods
Because the object of this study was to present a reasonably realistic comparison of the true cost to heal a wound versus reimbursement by payers, it was decided to create a small cohort of patients with diabetic foot ulcers (DFUs) whose episode of care originated from a PBD and to capture the most important episode-of-care costs. This study received an exemption from The Woodlands IRB.
Cohort creation
A cohort of 100 patients with DFUs was created by randomly selecting patients from the 57,706 DFUs within the U.S. Wound Registry with service dates from March 7, 2005 to November 30, 2016 in proportion to Wagner grade (1: 9.0%; 2: 46.4%; 3: 30.2%; 4: 14.2%; 5: 0.2%). As stated above, the primary care setting for this study was PBD.
Imputation of outcomes
Outcomes of 51% of wounds were right censored due to unknown deaths, amputations, or transfers to other care settings. Because this study had only one group and was analyzed for illustrative rather than population-specific comparative purposes, outcomes were imputed simply. The study population most resembled the cohort studied by Prompers et al. 19 Consequently, for the right-censored wound outcomes, six deaths associated with patients were imputed. Although 4 wound outcomes were recorded as amputation, they were recategorized as major amputation (1) and minor amputation (3), with 14 minor amputations imputed and 4 major amputations imputed. The remainder of the right-censored wounds were assumed to heal over 5 years, and the time to heal was imputed based on a calculated Kaplan–Meier wound-healing trajectory for healed wounds. Individual imputation outcomes were also guided by patient comorbidities and the wound-healing trajectory available before right censoring. Visit count and debridement counts were adjusted (i.e., counts were added in proportion to the imputed extended treatment time based on the existing treatment time metrics).
Prompers et al. 20 observed that 46% of their patients required hospital inpatient care with 18% having lower extremity revascularization. In our cohort, with 22% of patients having an amputation, 18% required vascular surgery to improve blood flow to the limb bearing the DFU. Thirteen percent of patients were also imputed to have a hospital stay for a wound infection based on the data of Prompers et al. 20
Biologicals, dressings, durable medical equipment, home health care, and hyperbaric oxygen therapy
Use of cellular and/or tissue-based products for skin wounds (CTPs) and/or dressings with/without antimicrobials at each visit was captured from EHRs; this information was cross-walked to categories of products, and the number used throughout the episode of care. (Thirty-five percent of patients received home health care [HHC]: in this instance, dressing changes outside of the PBD were provided and paid for by the home health agency [HHA].) When hyperbaric oxygen therapy (HBOT) was provided, the number of sessions was counted. When negative pressure wound therapy durable medical equipment (NPWT DME) and/or other DME was/were provided, the total treatment time was calculated. It was assumed that new offloading boots were purchased every 6 months until the wound healed.
Medicare/Medicaid and private insurance reimbursement-based costing method
Medicare national average allowable payment rates are shown in Table 1 (2018; U.S. dollars). Since types of dressings vary enormously in the real world, and despite having good EHR data on the subject, and to make the cost calculations manageable, it was decided to simplify cost calculations by choosing one type of foam, antimicrobial, and collagen-based dressing. Likewise, it was assumed that each wound received daily foam dressings until the wound was healed although the patient could receive another dressing (e.g., collagen based, antimicrobial, applied for 1 week) during the course of treatment. In these instances, the foam dressing count was adjusted. Total counts for antimicrobial and collagen-based dressings for each were available and used in the calculations.
Medicare national average allowable reimbursement rates (2018; U.S. dollars)
CPT is a registered trademark of the American Medical Association.
Where appropriate, values include physician components as well as facility components.
A “PBD” is a hospital-based outpatient wound care provider-based department.
The PBD visit includes everything. Level 3 complexity was assumed for evaluation and management at all visits. If any debridement was performed at an initial or established clinic visit, separate billing for evaluation and management charges was not permitted.
If a patient receives any collagen-based or antimicrobial dressing, the cost of a foam dressing over 7 days is excluded.
No separate E/M codes permitted.
Coverage is only permitted if the Wagner grade is 3 or higher.
2015 Medicare data adjusted for inflation.
CMS, Centers for Medicare and Medicaid Services; CPT (code), Current Procedural Terminology; CTP, cellular and/or tissue-based product for skin wound; E/M, evaluation and management; HBOT, hyperbaric oxygen therapy; HCPCS, Healthcare Common Procedure Coding System; HHC, home health care; HHRG, home health resource group; MS-DRG, Medicare severity–diagnosis-related group; NPWT DME, negative pressure wound therapy durable medical equipment.
The dressing size was matched to the wound area at each PBD visit. When patients changed their own dressings at home in between PBD visits, it was assumed that Medicare administrative contractors and private payer local coverage determinations/medical policies would be utilized to reimburse DME suppliers depending on the type of dressing, the size of dressing, and the number provided. 26 The reimbursement to the DME suppliers was included in the study cost calculations.
When patients received care by a HHA during the time the patient had the wound, the HHA provided the dressings. The HHC costs were calculated as 60-day episodes of care using the home health resource group (HHRG) code C2F2S1. Because HHRG national average allowable payment rates 24 depend on quality reporting adjustments, each of these payment rates was multiplied by the HHRG code weighting factor and averaged.
When patients were admitted to the acute care hospital, the 2015 Medicare severity–diagnosis-related group (MS-DRG) national average figures were used and inflated to 2018 values using the Consumer Price Index inflation calculator.
Because 50% of patients in the study cohort group had private insurance, rather than Medicare, the reimbursement-based costs per wound were calculated by multiplying the final Medicare costs by 1.36 to obtain private payer reimbursement values. 27
Activity-based costing
The ABC method divides costs into two groups: (1) direct costs that are related to personnel time, procedures, and products used to treat the patient; and (2) indirect costs that are generally related to the cost of operating the business and the equipment used.
Initial PBD visits assumed 30 min of a physician's time based on mapping level 3 complexity Current Procedural Terminology (CPT) codes to time 28 and 30 min of a nurse's time. For established PBD visits, these times were halved. Debridements carried out at the initial clinic visit assumed a further 30 min of the physician's time with subsequent debridements taking 15 min. CPT applications and 2-h HBOT sessions assumed 15 and 30 min, respectively, of a physician's time.
Costs of dressings were estimated from public sources using key brand names (information withheld here to prevent publicity) (Table 2). Hospital PBD charges for CTPs and HBOT used in the cohort were obtained from the chargemasters of California hospitals (2016 charges; minimum of five different values except for Primatrix in which only two values were located), 31 converted to costs using published cost-to-charge ratios, 32 and averaged. The obtained costs of all consumables were benchmarked as mean costs; higher and lower costs were set to +25% and −25% of the mean to represent a range.
Direct costs based on activity-based costing (2018; U.S. dollars)
Source costs were inflated to 2018 prices.
Ratios for costs of minor and major amputation and vascular intervention between CMS and Barshes et al. 35 averaged, and then multiplied by the cost of wound infection for CMS (US$5,028).
In the United States, indirect costs, such as physical infrastructure, equipment, utilities, maintenance, EHRs, and administration/management of a PBD, are not known and are likely to vary enormously depending on the business model, the size of the hospital, and/or the parent organization, geographic location, and many other factors. 36 Brox et al. 37 calculated that indirect acute care hospital stay costs for abdominal aortic aneurysm repair were 43% of total costs in six U.S. hospital systems. Because we expect indirect costs as a percentage of total costs should be lower in a PBD, the benchmark was set to an arbitrary 30% ± 15% (i.e., 15–45% of direct costs).
Aggregate cost calculations
For the reimbursement-based costing method, costs at each PBD visit were based on each category/item's unit reimbursement except for DME (e.g., NPWT DME) and HHC whose reimbursement was paid over a period of time; the reimbursement for these items was added to the summed costs of PBD visits based on actual time ordered in the EHR. Reimbursements for wound care-related inpatient hospital stays were added to calculate the final cost.
The aggregate cost calculations for the ABC method were the same as those for the reimbursement-based costing method, except that costs for physician and nurse time at each visit were added to the cost of consumables to obtain direct costs.
While costs obtained through the reimbursement-based costing method had single values for each wound, costs obtained by the ABC method had three values (lower range, upper range, and mid-range). For example, the lower range used 75% of benchmark direct costs plus 15% of benchmark costs to represent indirect costs, whereas the upper range used benchmark direct costs × 1.25 plus 45% of benchmark costs to represent indirect costs. These ranges were calculated to estimate the uncertainty in costing associated with the ABC method.
Results
The cohort's mean age was 62.3 years, and it comprised of 63% males with 9% of patients having end-stage renal disease and 29% having peripheral vascular disease (Table 3). The mean wound area was 4.0 cm2, and the mean age was ∼7 months. Nearly one-third of the wounds were treated with HBOT, although only 24% were eligible for Medicare reimbursement. The mean PBD visit count was 11.8.
Patient and wound characteristics of the cohort
Multiple wounds present at some point during treatment of the selected wound.
ESRD, end-stage renal disease; IQR, interquartile range; SD, standard deviation.
The mean cost to heal through the reimbursement-based costing method was US$20,474 compared with the US$27,795 mid-range of the ABC method (Table 4). When the results for both costing methods were compared graphically, the reimbursement-based costing method data showed that while ∼18% of wounds were in the second least costly category, much of the ABC method cost for this category had shifted to higher values (Fig. 1). The mean cost-to-heal range for the ABC method was US$19,243–US$36,348 (Table 4) with costs almost double for the high-range ABC method compared with the low-range ABC method.
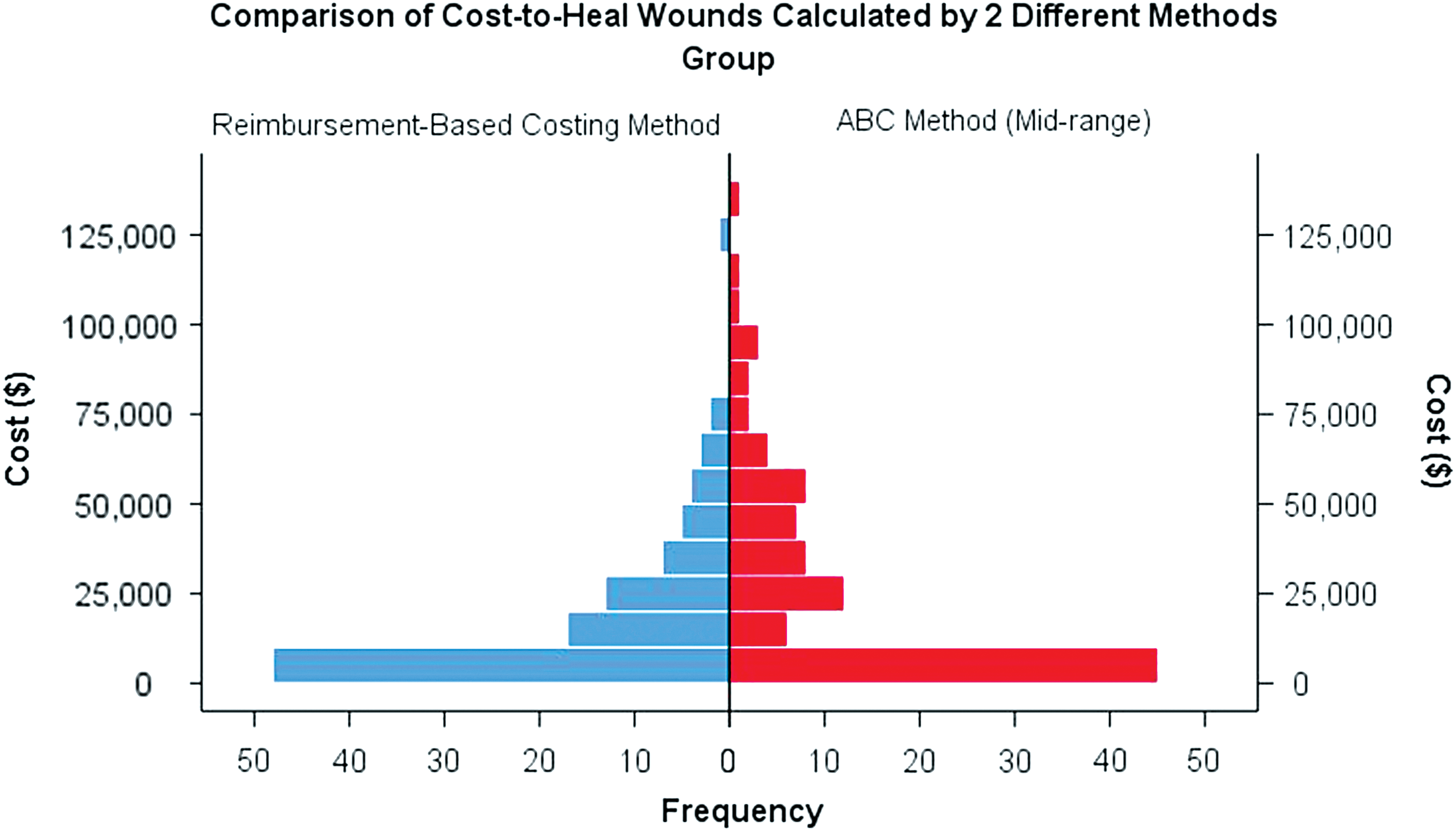
Histogram of cost to heal using the reimbursement-based costing method versus the ABC method (mid-range). ABC, activity-based costing. To see this illustration in color, the reader is referred to the web version of this article at
Comparison of costs by different methods
ABC, activity-based costing; CI, confidence interval.
When costs were broken down by category and determined as a percentage of total costs by the reimbursement-based costing method and the ABC (mid-range) method, the evaluation and management (E/M) and dressings cost percentages were much higher, the PBD procedures and HHC cost percentages were slightly higher, and the acute care inpatient stays were much lower for the reimbursement-based costing method compared with the mid-range ABC method (Fig. 2).
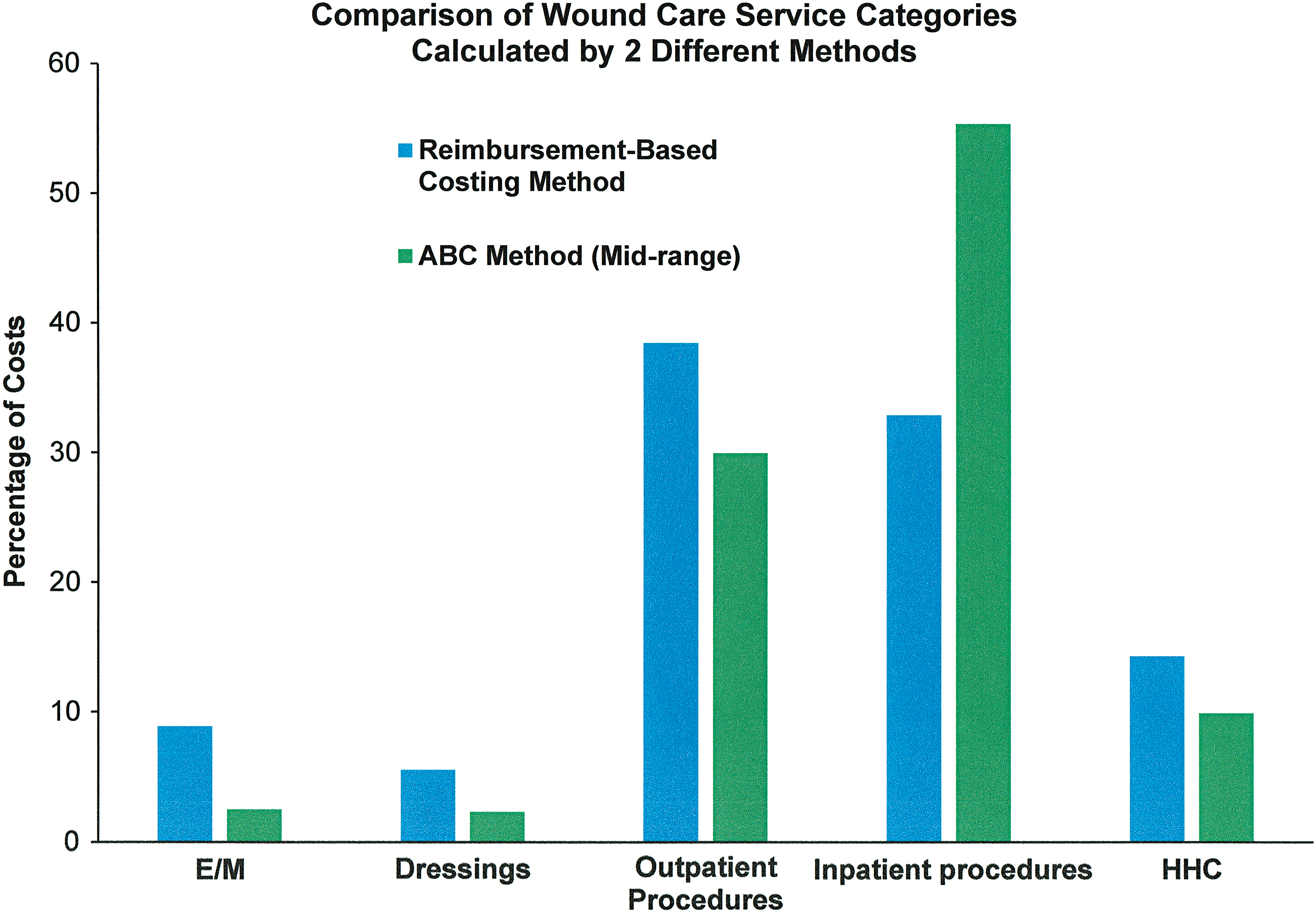
Comparison of costs of various wound care service categories using the reimbursement-based costing method and the ABC method (mid-range). E/M, evaluation and management; HHC, home health care. To see this illustration in color, the reader is referred to the web version of this article at
Discussion
The authors of a published 2017 systematic review 11 of cost-of-illness studies regarding chronic ulcers noted that of the 36 reviewed studies, 53% used bottom-up methodology, which is the general approach to the ABC method used in this study (i.e., unit costs multiplied by resources used). The mean cost of DFUs per episode of care, from a healthcare public payer perspective, was calculated as US$31,024—much higher than the reimbursement-based costing method estimates, but well within the ABC method mid-to-high range cost. Based on a comparison of the systematic review costs with the cohort costs calculated in this study, the cohort costs are likely to be both realistic and reasonable, although a small cohort of patients was used for illustrative purposes.
Most health economic studies on wound care report costs based on Medicare reimbursement. There is a good reason for this: data are publicly available for wound care-related services, procedures, and products in various care settings, although navigating the billing rules for their disparate payment systems can be challenging and often requires compromises to enable modeling. While health economists can equate the reimbursement-based costing method to the cost of wound healing (assuming a patient can be tracked through all care settings), sometimes there are suspicions that “true” costs are not captured. This arises, in part, because the majority of PBDs in the United States are hospital based: some hospitals may not know the real costs of running their PBDs (i.e., knowing if the PBD runs at a loss or a profit); other hospitals may assign indirect costs to the PBD based on a global analysis of services, procedures, and products provided and facility revenue generated from them (i.e., any outpatient or inpatient wound-related event that happens within the organization is moved into the wound care center cost “bucket”). Astute hospital administrators are also likely to be mindful that procedures, such as debridement, HBOT, and application of CTPs, account for the majority of a PBD's revenue. 38
In theory, the ABC method can fairly and accurately allocate all the costs involved in providing wound care treatment, but it is the apportionment of indirect costs that can be most difficult to estimate and mostly influence the total cost. This study shows that if the ABC method is used, indirect costs need to be ∼20% of total costs to equate to the reimbursement-based method—the point at which costs equal reimbursement payments. As the indirect cost percentage rises to 50% of the total cost, the “cost” of wound healing rises substantially. Health economists have not estimated the mean national indirect cost rate for PBDs and other hospital departments, but for certain inpatient surgeries it has been estimated as high as 60%. 39 The most difficult decision for administrators using the ABC method is to decide whether indirect costs should only reflect what happens in the PBDs, in which case the percentage of indirect costs will be relatively low, or use a functional DRG-like approach for aggregating indirect costs in which the resources used for wound care patients are apportioned irrespective of whether they happen in the PBD or any other organization's departments. Finally, even the ABC method does not include patient out-of-pocket costs, sometimes known as indirect costs from the societal perspective (the same term, which is confusing), and which is used less frequently in health economic analyses. These costs include insurance premiums, the cost of care not covered by insurance, loss of wages, transportation, and more intangible costs relating to loss of quality of life.
While this study showed that the cost of PBD wound care alone (no inpatient-related costs) could easily be more expensive using the reimbursement-based costing method compared with the ABC method with indirect costs set at 30%, the reverse was true for inpatient wound care-related hospitalizations. Part of the reason for the latter may be the difficulty of calculating the true cost of hospitalizations; MS-DRG payments can be artificially low or high. 40 Another part of the reason is that, in general, PBD activities in hospitals may be subsidizing inpatient activities because inpatient profit margins may be low or negative, although peer-reviewed evidence for this supposition is lacking. What is known is that the care of patients with chronic ulcers shifted from inpatient to outpatient settings in the last 10 years to contain costs due to Medicare policy reimbursement changes. 41 This shift is probably due to rising inpatient costs associated with morbidity severity increases and lack of access to timely care. 42 Many publications are available for those interested in learning more about ABC methodology and how it can be applied in any given health care setting. 43 –45
Although the chosen cohort used in this study provided cost results well within literature values, it may still not be representative of Medicare or national populations. That said, because patient groups or treatments are not being directly compared, the calculated relative costs are likely to have merit even though there is some uncertainty in direct absolute costs themselves under the ABC methodology; for example, the manufacturer's average selling price of a CTP to an organization will depend on many factors, including the organization's clout and how much the manufacturer wants to sell to the organization. While extensive sensitivity analysis might have partially mitigated this uncertainty, the aim of the study was not to provide the most accurate cost estimates possible but rather to illustrate the different costing methods. Another limitation of the study is the cost issue of treating multiple wounds at the same PBD visits. In this study, this factor was ignored as there is no easy way to allocate certain costs. As just one example, consider HBOT provided for a Wagner 3 DFU in which a patient also has a contralateral Wagner 2 DFU that also benefits from the treatment. Should some of the cost of treatment be apportioned to the Wagner 2 DFU? It cannot be permitted under Medicare rules, but under ABC methodology it can be. The cost of antibiotics for infection and other wound-related drug prescriptions (e.g., pain medications for neuropathy) was also disregarded, although for most patients these costs are not likely to be high. Finally, imputation of outcomes was necessary in the cohort, and even though benchmarking was used, total costs may have been over- or underestimated as a result.
Innovation
Calculating the “true” cost-to-heal wounds is likely to remain a challenging exercise. The best approach may be to provide a range of values associated with specific treatment modalities and cost methods as illustrated in the results of this study. The results also suggest that compared with the ABC method, the reimbursement-based costing method may not capture the true costs of specific treatment categories and care settings. Therefore, clinicians, payers, and policy-makers are encouraged to become familiar with the ABC method, as it may help them better understand the true costs of providing wound-healing treatments in various care settings.
The reimbursement-based costing method is commonly used in wound care heath economic studies, but this method may not fully capture true costs. ABC methods may capture more true costs, but estimating indirect costs is challenging in this method.
Capturing an episode of care for a single DFU (or any other wound type) “from cradle to grave” presents problems because patients move between care settings, and may also have multiple ulcers at the same time or at overlapping time periods.
The results of the cohort study show that the “true” cost of wound healing may be an unrealistic concept; it may be better to think of the cost-to-heal wounds in ranges of costs.
Footnotes
Acknowledgments and Funding Sources
The author thanks Dr. Caroline E. Fife of the U.S. Wound Registry for permission to use data. There are no funding sources for this article.
Author Disclosure and Ghostwriting
No competing financial interests exist. The content of this article was expressly written by the author listed. No ghostwriters were used to write this article.
About the Author