
Abstract
Objective:
No active treatment is required in the majority of cases of infantile hemangioma (IH), while they proliferate and involute without sequelae. However, ulceration, bleeding, or destruction/obstruction of important structures may occur in 10% of cases during the proliferating phase. These lesions lead to a disfigured appearance with redundant skin, fibrofatty residuum, protruding surface, drooping, and scarring. This study focused on prevention and management of disfiguring scars in involuted IH.
Approach:
A retrospective photography and chart review were performed for patients with IH who visited our hospital (Shinshu University Hospital).
Results:
The study population consisted of 107 patients with IH. The lesions were located on the head and neck (59.8%), trunk (27.1%), upper limb (7.5%), or lower limb (5.6%). Twenty-four patients (22.4%) underwent surgical excision of the disfigured lesion after involution. The percentage of surgical interventions was highest for lesions in the head and neck area (28.9%) compared with other regions. The fibrofatty tissue and redundant skin after involution of each lesion were partly resected and sutured. All suture lines were finally set on the wrinkle line or the anatomical borderline.
Innovation:
Although total excision of the lesion was impossible in some cases, a natural surface contour was obtained. The operative scar was not visible in the residual damaged skin after involution.
Conclusion:
Effective preventive therapies during the proliferating phase are required to avoid tissue damage due to hyperexpansion of the surrounding tissue and surface breakdown to present excellent cosmetic results in patients with IH.

INTRODUCTION
Infantile hemangioma (IH) is a benign tumor of the proliferating vascular endothelium, 1 and is the most common tumor of infancy seen in approximately 4–5% of Caucasians 2 but with a prevalence of 0.8–1.7% in Japanese infants. 3 IH grows rapidly during the first 9 months of life (proliferating phase) and 80% of its size is achieved by 3.2 ± 1.7 months. 4 The tumor begins to shrink after 12 months of age (involuting phase), and involution stops in most children by 5 years of age (involuted phase). 5 After involution, children may have a residual disfigured appearance, such as anetoderma from loss of elasticity, fibrofatty residuum involving scattered tiny vessels in a field of fat and fibrous tissue observed on histological examination, redundant skin, protruding surface, drooping, scarring, telangiectasia, and/or destruction of anatomical structures, as sequelae of excess tissue expansion, ulceration, and local bacterial infection.
No active treatment is required in almost 90% of IHs, while they proliferate and involute without sequelae. 6 However, ulceration, bleeding, or destruction/obstruction of important structures may occur in 10% of cases during the proliferating phase. Many treatments have been developed for problematic proliferating hemangioma, including oral beta blockers, 7 –9 oral corticosteroids (CSs), 10 –13 intralesional CSs, 14 –16 topical medication, 17 –20 pulsed-dye laser treatment, 21 –23 and resection. Although some surgeons perform surgical interventions during the proliferating phase, 24 operative treatment in infancy is generally not recommended. 25 Operating on a highly vascular hemangioma in an infant is associated with greater complications (e.g., bleeding, iatrogenic injury, wound dehiscence) compared with removal of an involuted tumor. Although surgical intervention of hemangioma during the proliferating phase is uncommon, patients may require operative treatment in childhood because approximately 50% of hemangiomas leave residual disfiguration. 5 Reconstructive procedures should be considered after 3.5 years of age because the tumor does not improve significantly after this time and long-term memory and self-esteem begin to form at this age. 26 Staged excisions can be readily accomplished for involuted hemangiomas of the lip, cheeks, glabella, and scalp.
CLINICAL PROBLEM ADDRESSED
Disfiguring scars in involuted IH, especially on unconcealed areas, have an adverse effect on patients' quality of life. Therefore, they are important clinical issues that should be prevented and repaired.
This study focused on prevention and management of disfiguring scars in involuted IH. Esthetically important points and problems regarding excision of involuted hemangiomas were ascertained and preventive therapeutic options are discussed to present a summary of surgical procedures with a review of the relevant literature.
MATERIALS AND METHODS
The study was reviewed and approved by the Committee for Medical Ethics of Shinshu University School of Medicine Institutional Review Board (IRB no. 4168). A retrospective photography and chart review was performed for patients with IH who visited our hospital (Shinshu University Hospital) between January 1, 2001, and December 31, 2012, and were managed by the author (S.Y.). The clinical records, including operative reports and photographs of each patient, were studied. The site of each lesion, the age at the time of first visit, therapies during the proliferating phase, surgical interventions other than laser therapy, timing of surgery, and follow-up details after the operation, were examined.
RESULTS
A total of 107 patients with IH, consisting of 77 (72%) female infants (female-to-male ratio 2.6:1), were included in this study. The lesions were located on the head and neck (59.8%), trunk (27.1%), upper limb (7.5%), or lower limb (5.6%). The patients ranged in age at the time of the first visit from 7 days to 7 years old, with a mean of 12.4 ± 16.1 months (mean ± standard deviation). The purposes of the visits were variable and included red birthmarks, enlargement of protruding red or bluish mass, surface breakdown of the lesion, and disfigurement after shrinkage. Seven patients were treated with any therapeutic medication during the proliferating phase. One orbital lesion and one glabella lesion were treated with systemic CS, and one glabella lesion and one lip lesion were treated with local injection of CS. Two orbital lesions and one chest lesion were treated with oral propranolol. A total of 24 patients (22.4%) underwent surgical excision of the disfigured lesion after involution. Surgical interventions were more frequent in the head and neck area (28.9%) compared to other areas. Data of all patients included in this study are summarized in Table 1.
Data of all patients
CS, corticosteroid.
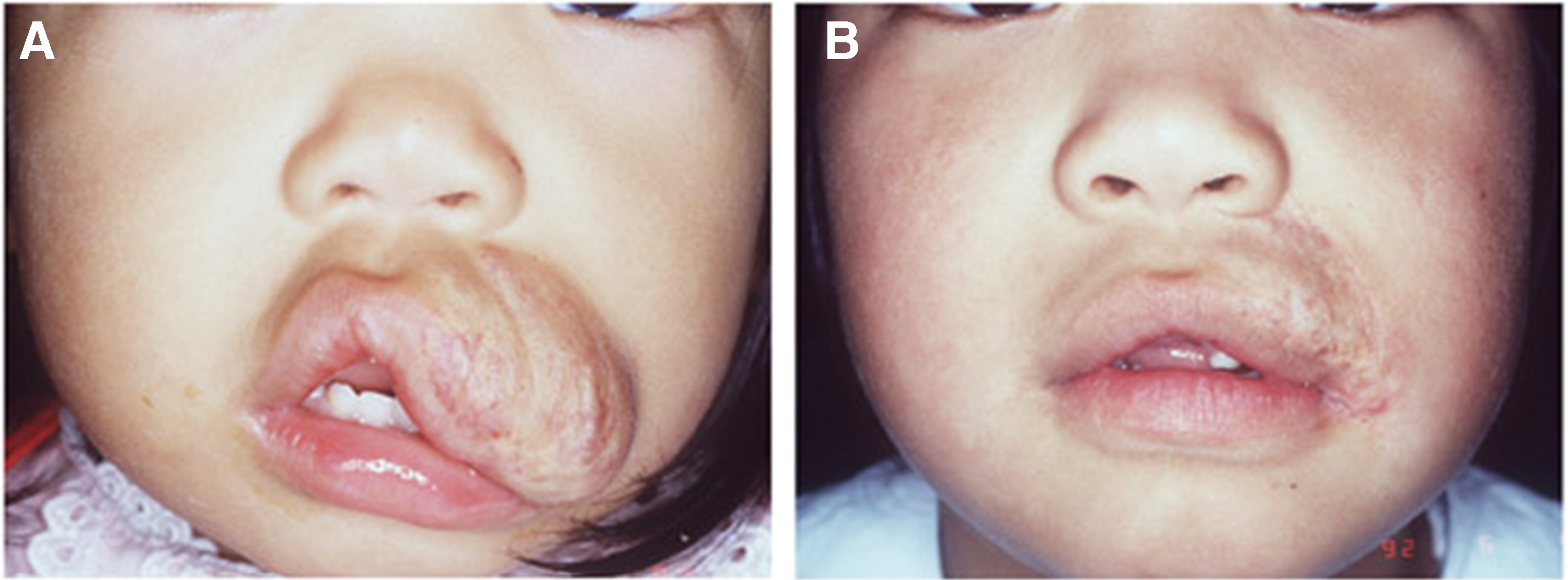
Lesions occurred most frequently in the head and neck area (64/107 cases, 59.8% of total cases), especially on the scalp and forehead (29/64 cases, 45.3% of head and neck cases). One occipital scalp lesion and one forehead lesion were excised early during the proliferating phase to avoid surface breakdown and bleeding. Surface breakdown, such as erosion and ulceration, occurred in two cases with occipital scalp lesions and two with lesions on the lips. Details of patients with lesions on the head and neck are shown in Table 2.
Data of patients with head and neck lesions
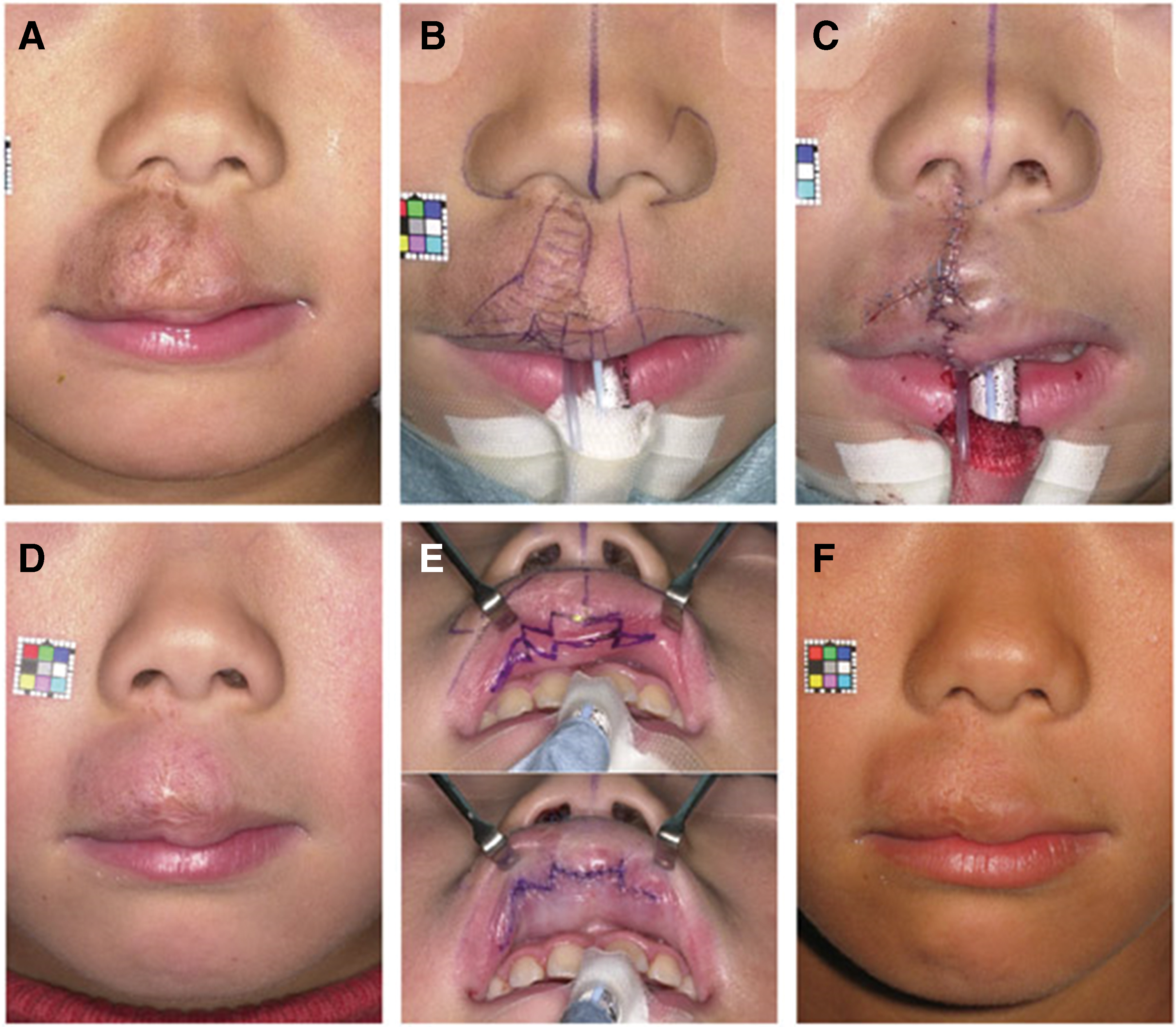
Twenty-two surgical procedures were performed during the involuted stage at 5–11 years of age. The mean age of these patients was 6.2 ± 1.4 years. The fibrofatty tissue and redundant skin after involution of each lesion were partly resected and sutured under general anesthesia. Two trunk lesions were removed by circular excision/purse-string closure at the first stage and lenticular excision/linear closure at the second stage, 27 while the others were removed by primary lenticular excision/linear closure. All suture lines were finally set on the wrinkle line or an anatomical borderline, including the hairline, upper eyelid fold, subciliary line of the lower eyelid, nasolabial crease, medial aspect of the philtral ridge, upper border of the white skin roll, vertical wrinkle of the vermilion, and the free margin of the oral mucosa. Liposuction was applied to reduce the volume of the cheek in one case. Follow-up revision surgery was needed in six patients with head and neck lesions. Although complete total excision of the lesion was impossible in some cases, natural three-dimensional contours of the surface were obtained not only statically but also dynamically. The operative scar was not visible in the residual slightly damaged skin after involution.
Representative cases are illustrated in Figs. 1–4.


DISCUSSION
Prevalence
IH is more common in female infants, and recent data suggest female-to-male ratios ranging from 1.4:1 to 3:1. 28 The ratio in this study, 2.6:1, was within this range. This gender difference has not been explained definitively. IH has been reported on the head and neck (60–79%), trunk (13.6–25%), or extremities (7.4–15%). 26 The proportions of lesion locations in this study (head and neck: 59.8%; trunk: 27.1%; extremities: 13.1%) were similar to the published data. IH was reported to have a reduced prevalence rate in the Japanese population (0.8–1.7%) 3 compared to Western populations (4–5%). 2 The reason for this ethnic difference in prevalence rate is not yet clear. However, this prevalence rate in Japan was derived from an older survey performed by Hidano et al. in 1986. 3 Multicenter or large-scale epidemiological surveys are required to obtain more recent data for ethnic comparisons.
Timing of excision
Early excision of IH during the proliferating phase is usually not necessary. However, factors that reduce the threshold for resection of a problematic proliferating lesion include (1) failure or contraindication to pharmacotherapy, (2) well localized in an anatomically safe area, (3) no requirement for complicated reconstruction, and (4) high likelihood that resection will be necessary in future (due to bulk or ulceration) with similar scarring. 5,25,29 Only two focal lesions (one occipital scalp lesion and one forehead lesion) in 107 cases were excised during the proliferating period to avoid surface breakdown and bleeding in our series.
Excision should be considered during the involuting phase if (1) the patient will obviously require resection after complete involution because of severe residual problems (i.e., postulceration scarring, expanded skin), (2) the operative scar can be estimated to be similar if excision is postponed, or (3) the scar is in a favorable location. The advantage of surgical intervention in early childhood (involuting phase) compared with late childhood (involuted phase) is that reconstruction can be performed before the child's development of memory or awareness of body differences. 25 For lesions on exposed areas, such as the face, which cause disfiguration that cannot be concealed, surgical intervention may be considered in early childhood. 24
If a child has a minor deformity, postponing intervention until involution has completed may curb the need for a procedure. 30 Waiting until the lesion has fully involuted and become less vascular before resection reduces the risk of problems, such as bleeding, iatrogenic injury, and healing problems, and ensures that the least amount of fibrofatty residuum and excess skin is resected, resulting in the smallest scar possible. 25
Couto et al. reported that most cases of IH do not improve significantly after 3.5 years of age, and suggested that reconstructive procedures should be considered at this age. 26 According to a natural history study of untreated IH, Bowers et al. reported that “complete spontaneous resolution of strawberry nevi is common, affecting approximately 50% by the age of 5 and 70% by the age of 7 years.” 31 We performed excisions at 6.2 ± 1.4 years of age with a mean ranging from 5 to 11 years. These can be accelerated before 4 years of age.
Therapies during the proliferating phase
Many treatments are available for problematic proliferating hemangioma, for example, oral beta blockers, 7 –9 oral CSs, 10 –13 intralesional CSs, 14 –16 topical medication, 17 –20 pulsed-dye laser treatment, 21 –23 and resection. These therapeutic managements during the proliferating phase have been indicated to treat life-threatening hemangioma and lesions with cosmetic problems, such as giant or remarkable lesions on the face, those with ulcerated and easy-to-bleed lesions, and those that may result in the development of functional impairment. However, there is no universal protocol for management of these lesions during the proliferating phase. The type of intervention is usually based on the training and experience of the attending physician. We administrated systemic CS, intralesional CS, or oral propranolol in only six problematic cases, mainly with lesions on or near the orbit or lip because of functional problems, such as visual or feeding impairment, and cosmetic problems. The frequencies of these therapies, especially beta blockers, are expected to increase further as their efficacy and safety become more established.
To avoid a residual severe disfigured appearance because of a large amount of severely redundant skin, fibrofatty residuum, protruding surface, drooping, and scarring, it is important to limit proliferation of the original hemangioma and avoid surface breakdown, including ulceration. Some therapies applied during the proliferating phase, including oral beta blockers, oral CSs, intralesional CS injection, and topical medication, can be effective and safe. Other potential options include early debulking with liposuction, early excision through the oral cavity, and flash lamp pulsed-dye laser irradiation to address the premonitory cutaneous mark. However, there is still controversy regarding the applicability of these methods. It will be necessary to verify whether these therapies can decrease the necessity for surgical intervention after complete involution of the lesion.
Wound care
Chamlin et al. performed a cross-sectional analysis in a multicenter prospective cohort study performed in 1,096 cases of IH, and reported complications with ulcers, with/without bleeding, in 173 (15.8%) cases. The median age of the patients was 4.0 months (SD = 8.5, mean = 6.6 months), and the age at the first examination was significantly lower in patients with ulcerated hemangioma (median = 3.5 months, mean = 3.98 months) than in those with nonulcerated hemangioma. 32 Ulcer formation was observed in 21 (30%) of 71 patients with lesions on the lower lip, 25 (25%) of 100 patients with lesions on the neck, and 46 (50%) of 93 patients with lesions in the perianal/perigenital area, and the frequency was lowest on the upper eyelid (p = 0.0140).
Ulceration, or breakdown of the IH skin surface, occurs with an estimated incidence of 5% to 21%. 21 In our study, surface breakdown, such as ulceration, was seen in two cases with lesions on the occipital scalp and two with lesions on the lip. These regions sustain maceration and friction, which may contribute to the development of ulceration. This leads to significant pain, bleeding, and secondary infection, and causes functional limitations, such as feeding difficulties, in cases of lip lesions and interference with urination or stooling in cases of perineal lesions. The management of ulcerated IHs includes attention to wound care, pain, and IH growth. 21 As ulceration usually results in severe distinct scarring, such as excavated surface, depigmentation, or alopecia on the scalp, with a risk of permanent disfigurement, prompt initiation of therapy is essential in the management of ulcerating IHs. There are many approaches for this purpose, including wound dressing, 21,33 topical antibacterial agents, 21,34 oral beta blockers, 35 and laser therapy. 21 –23 The management of ulcerated IHs includes paying attention to wound care, pain, and growth. 21
Most cases of ulceration improve with the abovementioned topical conservative approaches, such as application of wound dressing and antibacterial agents in wound care. Several case series have reported successful treatment of ulceration with propranolol, 35 and successful treatment has also been reported with topical timolol. 36 Systematic CSs may also be a reasonable alternative. 21 These therapies can suppress the proliferation of IH that causes ulceration. Although there have been reports regarding the effectiveness of laser therapy against ulceration, many are old and lack controls, and the evidence is not considered to be sufficient. 22,23 Laser treatment may be effective in a few cases, but as there is the risk of ulceration as a side effect of laser irradiation in nonulcerated IH, greater caution is needed in treating ulcerated lesions.
Regional considerations
When considering surgical intervention, it is important to weigh the postoperative scar after removal of the lesion against the preoperative appearance of the lesion. Linear scars are ideally placed along relaxed skin tension lines in the anatomical area where the IH is located to facilitate the best possible cosmetic outcome. In the scalp region, the scar line should be perpendicular to the direction of the hair flow to hide the scar alopecia beneath the hair flow. Circular excision and purse-string closure are not suitable for scalp lesions because a circular area of scar is more visible than a linear scar due to alopecia that usually requires follow-up procedures. 25
IH of the auricular helix and nasal tip involve skin that is difficult to replace because it is thin and fixed to the underlying cartilage. Surgical procedures involving the eyelids, oral commissure, and genitalia also carry a risk of functional impairment.
Technical considerations
The purposes of involuted hemangioma excision are (1) to achieve normal and natural contours, (2) decrease redundant skin, fibrofatty residuum, and scar, and (3) to leave no noticeable operative scar. The primary goal is to achieve normal contours. The operative scar should be set on the borderline between anatomical units under the regional esthetic unit principle or the subunit or the miniunit principle. 37,38
Blepharoplasty and ptosis surgery techniques are suitable interventions for lesions on the eyelid. Facial rhytidectomy procedures are also useful for excision of temporal, cheek, parotid, or neck lesions and for tightening of redundant and drooping skin. Open rhinoplasty techniques are effective for excision of redundant fibrofatty residuum beneath the nasal skin or between cartilage and reconstruction of the cartilage frame that is necessary for a normal attractive shape of the nose. For lip deformities, some principles and procedures for repairing cleft lip or revising secondary deformities with scarring after primary nasolabial repair are often helpful. 39,40
As IH acts as a tissue expander, there is usually adequate skin to enable primary wound closure and skin grafts and flaps are rarely needed. Total excision of the lesion is not required because these tumors are benign. In cases with a large lesion, complete excision is impossible. The goal of the surgery is to improve the appearance around the lesion, and partial excision is often sufficient. To treat circular lesions located in exposed areas, the length of the scar and distortion of surrounding structures can be minimized by circular excision and purse-string closure. 27 Liposuction is useful to reduce the volume of deep lesions. Intraoral approaches can be applied to reduce the volume around the cheek and oral area. The amount of scar tissue as a sequela of the surgical intervention should be minimized as much as possible.
Limitations
Management of IH is difficult because lesions are heterogeneous, and there are many possible treatment methods. There have been very few comparative studies in this area except pharmaceutical studies (e.g., propranolol, CS). Although there have been reports regarding the effectiveness of many therapeutic procedures, including surgical interventions, many reports lacked controls, and the evidence is considered to be insufficient. This study is also a case series based on experience in one institute.
INNOVATION
This study showed that skillful plastic surgery procedures are indispensable for the correction of disfiguring scars due to involuted IH after excessive proliferation, especially in the head and neck area, even in cases treated with pharmacotherapy during the proliferating phase. The esthetic unit or subunit principle, cleft operation techniques, and some esthetic surgical procedures are useful and applicable in such cases. Complete total excision is often impossible and not necessary. Natural three-dimensional contours can usually be obtained without a conspicuous operative scar. More effective preventive therapies during the proliferating phase are also required to avoid disfiguring scars after tissue damage.
KEY FINDINGS
IH lesions were located on the head and neck (59.8%), trunk (27.1%), upper limb (7.5%), or lower limb (5.6%).
Almost 30% of patients required surgical intervention on the disfigured lesion after involution.
Although complete total excision was impossible in some cases, natural three-dimensional contours of the surface were obtained.
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
No funding was received for this study.
AUTHOR DISCLOSURE AND GHOSTWRITING
No competing financial interests exist. The content of this article was expressly written by the authors listed. No ghostwriters were used to write this article.
ABOUT THE AUTHORS