
Abstract
Significance:
Scar management is an important concern in plastic surgery. Scar models that best mimic in vivo human scarring are essential for understanding scar development and progression, assessing the efficacy of therapeutics, and providing reliable and valid research outcomes.
Recent Advances:
In 2016, Lanier et al. proposed a new in vivo patient model, the Northwestern Abdominoplasty Scar Model, that overcomes the prior limitations of both animal and human models, with greater representativeness of the human scarring process, expedited recruitment, smaller sample requirements, and greater flexibility in the types and number of interventions that can be studied simultaneously.
Critical Issues:
Existing animal models suffer from limitations that impede generalization to human scars. Human scar studies are difficult to conduct and rarely used due to recruitment difficulties, ethical concerns regarding purposeful wounding, and inherent variability based on location, type of scar, and the heterogeneity of the host response between humans. Although overcoming many of these hurdles, the Northwestern Abdominoplasty Scar Model still has a few limitations. In addition, there remains a need for further study of and comparison between the Northwestern Abdominoplasty Scar Model and existing human and animal models, to inspire more widespread acceptance of a standardized human scar model.
Future Directions:
The Northwestern Abdominoplasty Scar Model is a critical stepping stone toward better human scar models. This model hopefully will inspire other in vivo patient models utilizing elective surgery to overcome recruitment and ethical concerns.

Scope and Significance
Scarring has been a cosmetic and pathological concern for patients and surgeons. 1 –4 Effective prevention and treatment necessitate closer insight into the human scarring process, and scar models are invaluable tools in studying each step of scar formation. This review will briefly discuss the limitations of current animal and human scar models and introduce the Northwestern Abdominoplasty Scar Model, an in vivo tool for investigating scar pathobiology, as well as evaluating therapeutics. We will then discuss the characteristics of the Northwestern Abdominoplasty Scar Model, as well as its specific advantages and disadvantages.
Translational Relevance
Scars provide significant psychological distress; preventing and treating scars are critical. 1,2,4 Although there are preventative and therapeutic scar treatments, corrective surgery remains a significant part of scar management, and there is no treatment that is efficacious yet unobtrusive and painless. 5,6 Pathological scars such as keloids remain difficult to treat, with some interventions only in early stages of implementation, and others reporting unsatisfactory recurrence rates. 7 The search continues for an ideal standard of care. 6 This review will discuss a new in vivo patient scarring model that will better assist researchers in studying scar pathogenesis and therapeutics.
Clinical Relevance
Scar models are crucial for evaluating scar treatments. Despite the advantage that in vivo models have been compared to animal, in vitro, and in silico models, there remains a lack of standardization in design, evaluation, and follow-up. 8 Most human studies have been limited to observational studies due to ethical concerns about purposeful wounding, and it has been difficult if not impossible to control variables such as location, demographics, and genetics. Before the Northwestern Abdominoplasty Scar Model, clinical trials utilizing in vivo patient scarring models also either required a large sample or suffered from intersubject variability. 9
Background
As a protective shield for the body, the skin is constantly exposed to potential external injury, and thus, wound healing is a vital process for the survival of all organisms. 10,11 After skin injury, the repair process includes regeneration and scarring. Although lower vertebrates and human embryonic tissues possess the ability to regenerate perfectly, adult individuals cannot regenerate the dermis or skin derivatives, forming collagenous scar tissue when the skin of adult humans is damaged past a particular depth within the dermis, determined to be a total wound depth of 0.56 mm. 10,12 –14 Scar tissue, although providing restoration of the epithelial barrier, is structurally and functionally distinct from normal skin. 15
As 100 million patients annually gain new scars due to 55 million elective surgeries and 25 million post-traumatic surgeries, scar formation poses a significant clinical problem in plastic surgery, especially considering the negative psychological impact of living with a scar. 1 –4 Scar models are crucial toward investigating scar development and testing therapeutics, and there are currently two major types of scar models: animal and human models, with human models being further separated into in vitro, in silico, ex vivo, and in vivo patient models. 8,16 Due to ethical and logistical limitations however, most scarring studies are conducted on animal models.
Limitations of animal models
Commonly accepted animal models include the Red Duroc porcine model, 17 –20 athymic murine model, 21 and the rabbit ear model. 9,22 –24 Many consider animal models inadequate for the study of human scars, despite their advantages. 9,25 –27 Cameron et al., 28 described the difficulty of developing an appropriate animal model, owing to the phylogenetic variation in wound healing. Genetics, epithelization, inflammation, and high skin tension are responsible for human hypertrophic scarring. 22 Animals generally scar well compared to humans, as increased body hair expedites epithelization, wound inflammation declines faster, and decreased skin tension promotes healing by contracture and ultimately reduces scarring by fibroblasts. 22
This is most demonstrated by multiple prior studies illustrating that increased mechanical stress exacerbates scarring in the Red Duroc pig. 29 –31 Attempts to counteract contraction include using the rabbit ear model and silicone/steel rings in mice, but scars only form when the wound diameter is >7 mm in the splinted rabbit ear, and there are concerns regarding the patency of silicone rings in mice while being housed during the study period. 32
In the mouse, primary wound contraction owing to the presence of panniculus carnosus, an extensive subcutaneous striated muscle layer that is lacking in humans, permits independent skin movement over the deeper tissues and is responsible for the rapid contraction of skin following wounding. 33 Additional differences between mouse and human skin include a denser hair covering, shorter hair growth cycle, and the absence of dermal papillae and apocrine glands. 28
In the rabbit model, the calculation of scar thickness through a hypertrophy index or scar elevation index is subject to natural inconsistency in the skin thickness of an animal. 22 Although there are histologic similarities, rabbit ear skin heals over a cartilaginous base, and its thickness is different from that of the human abdomen. 32 Ultimately, no animal model exhibits scarring that acceptably mimics that of humans. 8
Past attempts involving xenografts of human skin or hypertrophic scar in immunodeficient mice and rats are limited by these animals' size and led to scars that histologically resembled hypertrophic scars, but required significant suppression of the animal's immune system, hence limiting full extrapolation to the human milieu. 28,34 In addition, cell-mediated immunity is not truly eliminated, as injected subcutaneous keloid deteriorates over time and human skin grafts were observed to be static in appearance after 4 months. 17 A newer study, however, successfully grafted human xenografts onto pigs with a condition similar to human severe combined immune deficiency, which severely attenuated the immune response, allowing the graft to take. 34
Although pigs offer a much greater surface area of skin for study, use of any animal model requires navigating ethical hurdles regarding the purposeful chronic wounding and scarring of animals, and large animal models, like the Red Duroc porcine model, suffer the most from logistical limitations in expense, housing, and handling difficulties. 8,28 The rabbit ear model also suffers from logistical limitations in that fewer biologics are available for testing, making it difficult to manipulate particular cell signaling pathways and limiting the types of experiments that can be conducted. 22 Table 1 summarizes key differences in the benefits and drawbacks of each animal model.
Comparison of animal scarring models
Limitations of human models
Existing human scar models are broadly organized into in vitro, in silico, ex vivo, and in vivo models. 8 Basic in vitro models utilize cultured cells derived from human scars, with more complex in vitro 3D skin models, including structural elements. 26,27,35 –41 In vitro skin scar models replicate the differentiation of fibroblasts to myofibroblasts, cells that synthesize enormous amounts of extracellular matrix (ECM) and fibrotic markers, leading to uncontrolled matrix contraction. 42 While in vitro models allow for detailed biochemical gene expression and histologic analysis, they are limited in that these in vitro models are only made up of cell types chosen to be added, limiting the study scope to only those cell types. 8,26 Most of the studies related to cell models that focused only on a single morphogen ultimately also neglected the complex scar tissue microenvironment. 27,43 Specifically, in vitro models fail to preserve the specific biological environment seen in vivo that includes the mature ECM, blood vessels, inflammatory cells, and intrinsic and extrinsic biochemical interactions. 44 As the cells are originally drawn from individual patients, genetic factors can impact scar outcomes and results may not be generalizable to other populations. 16,26 These models cannot test preventative interventions; samples are difficult to obtain from qualified patients. 37 Samples are also time limited, as the tissue is viable for only 6 weeks. 37
In silico models attempt to model human wound healing or scar development through mathematical modeling to simulate cell behavior. 8 In silico models, as they require no tissue, bypass the logistics and ethical considerations involved in human or animal tissue studies but, as a result, generalization to the human scarring process is difficult. 8
In silico models are effective for certain measures that can be computed, such as population dynamics and movement of cells, but cannot measure other parameters such as scar appearance. 45 Ex vivo models involve maintaining whole human skin in culture. 8 Although ex vivo models benefit from a more realistically complex picture of scarring, there are several significant drawbacks. 8 Ex vivo models are not suitable for long-term studies, and there is currently no accepted procedure for tissue collection (full or partial thickness biopsy) or culture conditions, leading to significant variation from study to study. 8
In vivo models can be divided into healthy volunteer models and patient models and are most representative of the natural human scarring process. 8 Volunteer human models recruit healthy subjects and subject them to purposeful wounding: incisions, excisions, burns, tape stripping, scratching, and blistering. 8 Study subjects can be recruited to control demographic factors and can serve as a control for themselves, but volunteer human models can only be used to study acute wounds, not chronic wounds. 8 In addition, there is no guarantee that subjects will scar poorly, making it difficult to study forms of poor scarring such as keloid or hypertrophic scars. 8
Patient models recruit patients with preexisting chronic scars, pathologic scars, or patients undergoing surgical or other procedures that will involve the wound healing process. 8 Patient models can assess both normal and pathologic scars, can involve more damaging purposeful wounding such as incisions, and are important for therapeutic testing and drug development. 8 However, keloids cannot be studied; as there is a risk of exacerbating existing scarring, it is difficult to control scar characteristics, and the patient populations recruited may be skewed by demographic characteristics. 8 In general, patient model studies are also a more time-consuming and difficult process. 8,26
Discussion
In 2016, Lanier et al. 9 from the Division of Plastic Surgery at Northwestern University Feinberg School of Medicine developed an in vivo patient scarring model: The Northwestern Abdominoplasty Scar Model, the purpose of which was to develop a clinically relevant model of healing and scarring. 9 Using the availability of patients who are to undergo an abdominoplasty, scars or wounds can be created in the pannus, to be excised as part of the abdominoplasty procedure.
Figures 1 –4 illustrate the model on an Asian American patient. As shown in Figure 1, using local anesthesia in the clinic, a maximum of twenty 2-cm full-thickness horizontal wounds were created on a stretch of skin organized into a neat grid, with both sides mirroring each other. 9 Both control and interventional groups were represented within a single patient. 9 The number of wounds, grid size, and wound types can be varied according to investigator preference and if there is any concern of neighboring scars affecting scar outcomes. 9 The model permits both visual examination and record keeping with pictures, as well as biopsy with histological and biochemical analysis. 9 The sample study discussed in Lanier et al. varied both experimental drug versus control and tested high versus low dose, drawing data from both biopsies and pictures taken over the study duration. 9

Excision day—creating scars. Scars on the abdomen were created in the office by a senior plastic surgeon. The abdominal skin and subcutaneous tissue were diffusely infiltrated with dilute local anesthetic and closed by simple interrupted 4-0 Prolene sutures. This figure illustrates the patient's abdomen immediately after the procedure.
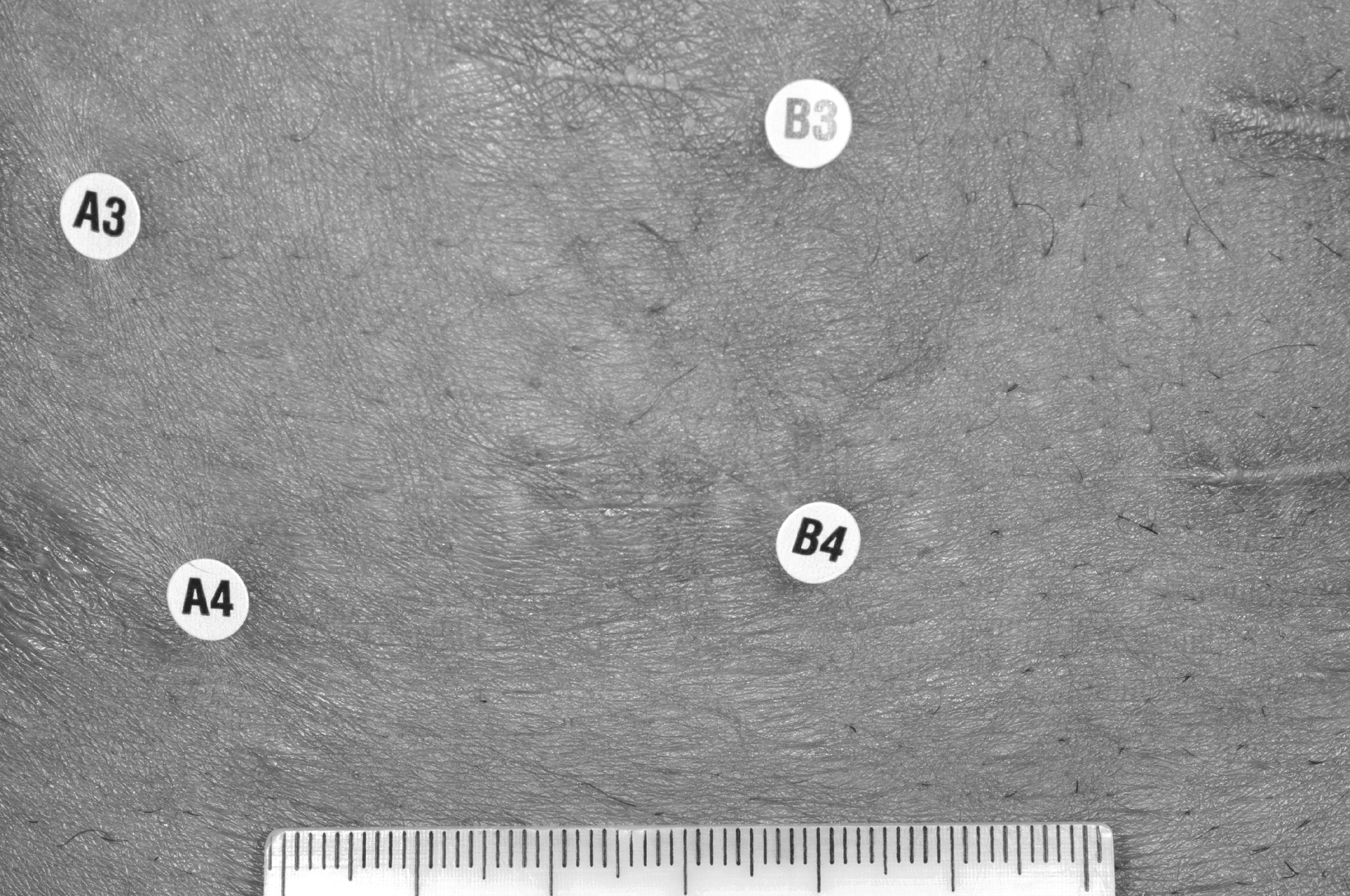
The complexity of the interventions demonstrates the flexibility of the abdominoplasty model in studying multiple different interventions simultaneously in the same patient and the rich qualitative and quantitative data that can be gathered. 9 Figures 2 and 3 illustrate an abdomen 8 weeks postwounding, with each hemiabdomen receiving randomly assigned drug or placebo. After the study duration, any time from several weeks to months later, the skin containing the wounds is removed as a part of an abdominoplasty. 9 Figure 4 illustrates an abdomen 12 weeks postwounding, 1 week before the planned abdominoplasty on week 13. Figures 5 –8 illustrate this model on, respectively, an African American and a Caucasian patient. Future human studies performed in a similar vein as Gurtner et al. 29 that utilize the elective abdominoplasty could benefit significantly from the Northwestern Abdominoplasty Model.

Eight weeks after excision day—full view with labels. All hemiabdomens received injection with either the investigational drug or a dilution-matched placebo randomly. Dosing schedules varied, with injections repeated as often as every 2 weeks for a total of 10 weeks before tissue analysis during the abdominoplasty at week 13.
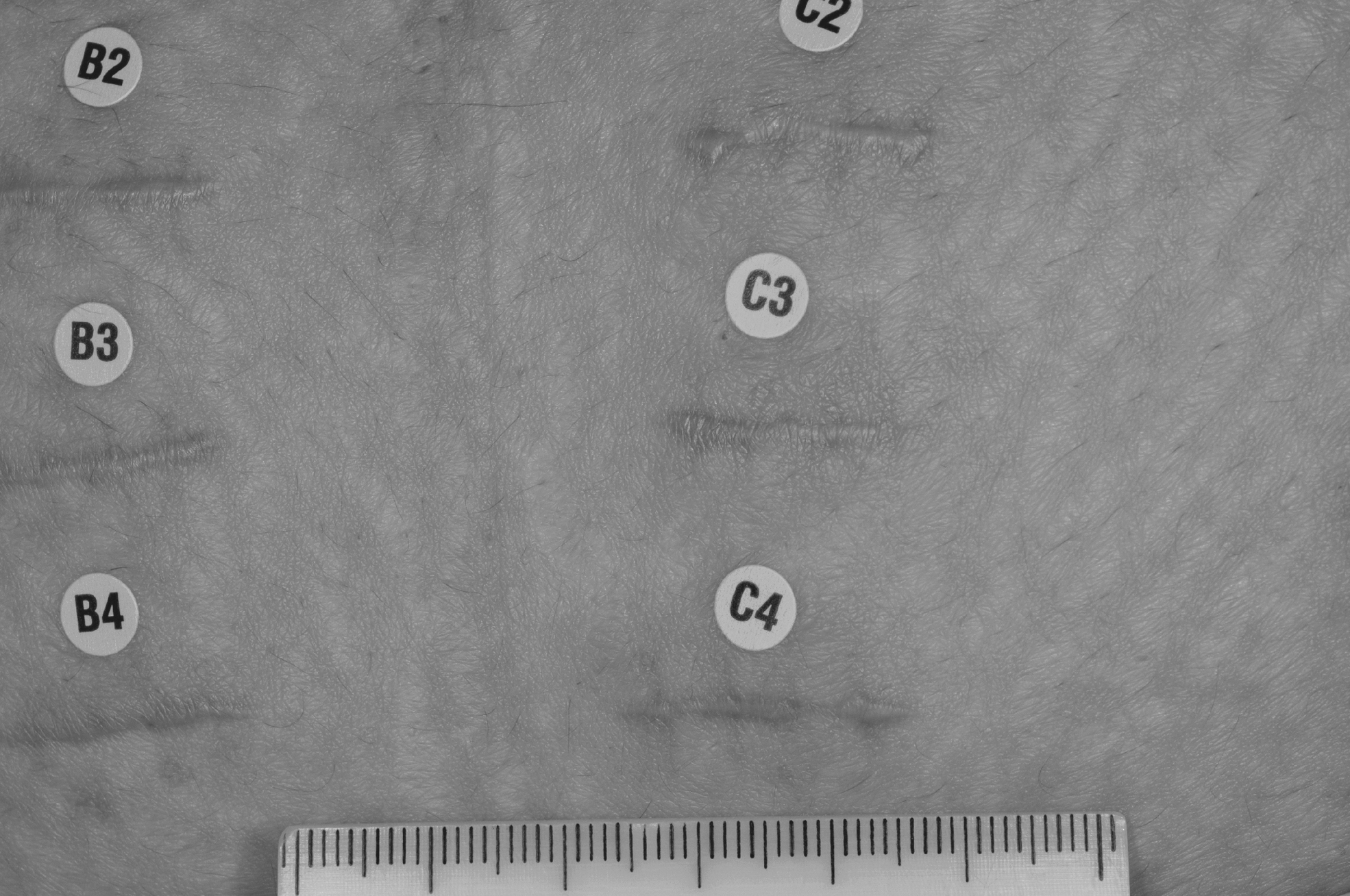
Eight weeks postexcision day—detailed close-up view of individual scars.

Twelve weeks postexcision day. At week 13, right before the abdominoplasty, scars were rated using a visual analog scale and an Investigator Scar Global Rating. During abdominoplasty, all experimental scars on a patient's abdomen were removed.

Excision day—African American patient.

Twelve weeks after excision day—full view with labels in an African American patient.
Twelve weeks after excision day—detailed close-up view of individual scars in an African American patient.

Seven months post-op image illustrating the removal of the skin utilized for the scarring model and the ultimate outcome of patients who opt to participate and undergo abdominoplasty after the study period.
It is important to note, however, that the Northwestern Abdominoplasty Scar Model relies upon ensuring strict informed consent during the recruitment process. 9 A patient must fully understand what the study entails in terms of the biopsies and images collected, the study length, the specific risks of and complications that may result from multiple abdominal wounds or the therapeutics tested, and that should they opt out of the abdominoplasty, scars that develop over the study duration will remain. 9
The abdominoplasty model is safe, as all 33 patients involved in the six clinical trials had no complications resulting from their participation in the study, but had complications occurred they would have been treated cost free to the patient. 9 In addition, the option of opting out of the study early is available to all study subjects in the form of receiving their abdominoplasty early. 9
The Northwestern Abdominoplasty Scar Model overcomes many prior limitations of human studies. Abdominoplasty is a common procedure in plastic surgery, and since patients who participate in the study can receive their abdominoplasty at reduced or no cost, recruitment is expedited. 9 The initial study had no difficulty recruiting 33 patients for the clinical trials. 9 As the skin is later removed during the abdominoplasty, there are no concerns of unsightly scarring in study subjects after study completion. 9
The creation of multiple wounds on a single patient, organized into mirrored pairs, facilitates the testing of multiple interventions in the form of specific therapeutics, dosing schedules, or dose amounts. 9 Organizing wounds into a grid with mirrored matched pairs on each patient effectively controls scar outcome variation based on location and skin tension, and randomization occurs at the patient level, in that each patient receives both control and experimental interventions, as opposed to the sample level, with different patients organized into either control or experimental groups. 9 Having a maximum of 20 scars, as opposed to a few, per patient also significantly reduces the necessary patient sample with which to approach statistical significance, 9 expediting recruitment and minimizing inherent patient-to-patient variabilities, typical of wound healing studies or patients.
Despite its advantages, the Northwestern Abdominoplasty Scar Model has several limitations. The abdominoplasty model demonstrated shallow horizontal incisions. 9 Deep, vertical, or even more complicated circular or curved scars are yet to be done. As a key facet of the methodology involves wounding the abdomen so that the abdominoplasty removes the skin involved in the study and prevents unnecessary chronic scarring, scar studies are limited only to that particular area. 9 The abdomen itself has low tension, making it difficult to study the effects of high tension on scar progression, outcomes, and the effect of therapeutics.
As patients seeking abdominoplasty are recruited for the study, it is uncertain as to how poorly they will scar, making it potentially difficult to study pathological scarring. Keloids in particular cannot be studied using this model, as patients who are predisposed to keloids are not enrolled due to fear of promoting further keloid formation.
Over the course of the six trials using the abdominoplasty model, follow-up was, at maximum, 3 months before the abdominoplasty, and as a result the model is similarly limited by time course like other in vivo models. 9 Since in vivo models occur over days to months, these models and studies only capture the early phases of human scarring, a process that occurs over years. 8,9 The time course can be extended as needed, but it is uncertain as to what the maximum time course can be without significantly sacrificing recruitment rates and patient quality of life. 9 Table 2 summarizes the differences in benefits and drawbacks of each human model, including the Northwestern Abdominoplasty Scar Model.
Comparison of various human scarring models
As there is considerable variation in methodology from human study to study, there continues to be a need for a widely accepted standard in vivo human model. 8 The Northwestern Abdominoplasty Scar Model presents a novel in vivo human patient paradigm more representative of natural human scarring than existing animal models, without the significant difficulties of recruiting, ethical considerations, and controlling wound characteristics and location. 9
There are yet to be studies testing the limits of the Northwestern Abdominoplasty Scar Model with deeper scars and nonlinear scars, studies with longer durations, or studies comparing the abdominoplasty model with existing animal and human models. Although the Northwestern Abdominoplasty Scar Model still presents with several limitations, it will hopefully inspire more replicative and comparative studies using this model, as well as the development of other in vivo patient models that rely on elective surgery.
Summary
Scars contribute significant distress to patients, and both preventing and treating scars pose a significant challenge in plastic surgery. Study of human scar development and the effect of therapeutics require a model that best imitates the natural human scarring process. Scarring models can be subdivided primarily into animal and human models. Animal models include the porcine, athymic mouse, and rabbit ear models that each offer unique benefits and drawbacks. Ultimately, although animal scarring can be similar, it is not the best approximation of human scarring. The search for better human scarring models continues as an area of active research.
Human models can be further divided into in vitro, in silico, ex vivo, and in vivo models. In vitro models utilize either cell cultures or tissue engineering, while in silico models attempt to model scar development and cell behavior through mathematical models and computing. Ex vivo models attempt to cultivate scar tissue outside of the body, while in vivo models utilize scars on human subjects. In vivo human models can be further subdivided into patient and healthy volunteer models. Unfortunately, in vivo human models are limited by difficulty recruiting subjects, ethical considerations about purposeful wounding of study subjects, and variability in scars based on location.
The Northwestern Abdominoplasty Scar Model offers solutions to the limitations of prior in vivo human models. The model consists of patients seeking abdominoplasty, and as abdominoplasty is a common procedure and participants are offered the procedure without cost, subjects can be more readily recruited. Patients are wounded on skin that will later be removed during the abdominoplasty, reducing ethical concerns of purposeful wounding that may leave lasting scars. Multiple wounds can be made mirroring each other, reducing variability based on scar location, reducing the required study population, and increasing the number of interventions that can be tested on a single patient.
The Northwestern Abdominoplasty Scar Model is a promising new in vivo human patient model and can inspire other in vivo patient models utilizing elective surgeries to study scarring on various parts of the body.
Take-Home Messages
Animal scar models primarily consist of the Red Duroc Pig, Athymic Mouse, and Rabbit Ear Model, and although each model has its particular benefits, animal models still only approximate the natural scarring response in humans.
Human models consist of in vitro, in silico, ex vivo, and in vivo models. In vivo patient scarring models are primarily limited by the difficulty of recruitment, ethical concerns, and variability in preexisting scars based on scar location.
The Northwestern Abdominoplasty Scar Model is a new in vivo patient model that utilizes a highly desired surgical procedure to overcome recruitment limitations of prior models. Multiple wounds per patient both decrease inherent scar variability and allow greater flexibility in the testing of one or multiple interventions at once.
Footnotes
Acknowledgment and Funding Sources
Thanks to Rafael Mendoza MD for consultation and proofreading.
Author Disclosure and Ghostwriting
No competing financial interests exist. The content of this article was expressly written by the author(s) listed. No ghostwriters were used to write this article.
About the Authors