
Abstract
Objective:
To explore the clinical efficacy and advantages of five-in-one comprehensive limb salvage technologies for the treatment of severe diabetic foot ulcer (DFU).
Approach:
Clinical data for 120 patients with severe DFU treated between January 2012 and December 2017 were analyzed retrospectively. The control group (48 cases) was treated with traditional therapies, including controlling blood sugar, improving microcirculation, preserving nerve function, and dressing changes, whereas the experimental group (72 cases) was treated with traditional therapy combined with additional techniques, such as early and thorough debridement, negative pressure wound therapy, revascularization, and skin graft or flap. Ankle–brachial index (ABI), transcutaneous oxygen pressure (TcPO2), wound healing rate, healing time, ulcer recurrence rate, and amputation rate were recorded.
Results:
Compared with the control group, the experimental group significantly improved wound healing rate (93.1% vs. 72.9%; p < 0.01), decreased wound healing time (16.2 ± 5.4 days vs. 32.2 ± 7.8 days; p < 0.05), reduced major limb amputation rate (1.4% vs. 10.4%, p < 0.05), and ulcer recurrence rate (5.6% vs. 14.6%; p < 0.05). There were no significant differences in amputation rate between experimental and control group (29.2% vs. 33.3%, p = 0.628). After revascularization, the revascularization group showed significantly improved ABI (0.75 ± 0.21 vs. 0.35 ± 0.16, p < 0.05) and TcPO2 (36 ± 6 mmHg vs. 15 ± 4 mmHg, p < 0.05).
Innovation:
We propose a five-in-one comprehensive treatment method, which provides a multidisciplinary cooperative model for comprehensive medical and surgical treatments for DFU.
Conclusion:
The five-in-one comprehensive limb salvage treatment technologies played a vital role in enhancing the healing rate of severe DFU, shortening the healing time, and reducing the rate of recurrence and major amputation, thus improving the overall quality of life.

Introduction
Currently, Diabetes is one of the major health problems in the world due to its high morbidity and mortality. 1 Diabetics have a 25% lifetime risk of developing foot ulcers that have a poor prognosis. 2 About 14–24% of diabetic foot (DF) patients must undergo amputation. 3 In many countries, DF is already the leading cause of amputation. 4 The recommended management for diabetic foot ulcer (DFU) included: symptomatic treatment, pressure unloading, anti-infection, wound bed preparation, surgical treatment, adjuvant treatment, and prevention of DFU recurrence. 5 Despite its frequency, the pathophysiology of DF is complex and few standardized treatment plans and specialized clinical departments for treatment of DF are available in China. Given the limited treatments for complicated and refractory DFU, many diabetes patients do not receive timely, professional, systematic, and effective treatment. As such, improved treatments for chronic wounds in DFU that can heal ulcer wounds and decrease the amputation rate are needed to improve the quality of life for diabetics and reduce the economic burden of diabetes. Based on extensive clinical research, in this study, we propose a five-in-one comprehensive treatment method that involves: (1) medical symptom treatment; (2) early and thorough debridement, (3) vascular reconstruction, (4) wound bed preparation by negative pressure wound therapy (NPWT), and (5) subsequent dressing change, surgical skin graft, or flap transplantation in accordance with wound conditions. This five-in-one comprehensive treatment approach produced good clinical results.
Clinical Problem Addressed
The current study compares the ankle–brachial index (ABI), transcutaneous oxygen pressure (TcPO2), wound healing rate, healing time, ulcer recurrence rate, and amputation rate in five-in-one comprehensive limb salvage technology groups and traditional therapy groups to explore the clinical efficacy and advantages of five-in-one comprehensive limb salvage technologies.
Materials and Methods
Clinical data and research methodology
Study subjects: DF patients admitted between January 2012 and December 2017
The inclusion criteria were: (1) Diagnosed with DFU; (2) Wagner Grade ≥26; (3) age >18 years; (4) absence of any other severe complications (see exclusion criteria).
The exclusion criteria were: (1) Patients that had complications of severe hematologic system diseases (e.g., severe anemia, aplastic anemia, acute and chronic leukemia, platelet dysfunction, thrombocytopenic purpura); (2) patients receiving glucocorticoids or immunosuppressive therapies; (3) patients who had experienced severe cerebrovascular accident, acute myocardial infarction, renal failure, severe arrhythmia, or heart failure with cardiac function Level III or Level IV during the previous 3–6 months; and (4) patients with malignant tumor or patients receiving radiotherapy and chemotherapy.
General data
A total of 120 patients who satisfied the above criteria were divided into 2 groups according to treatment methods. The traditional treatment group (control group) had 48 patients, whereas the five-in-one comprehensive limb salvage treatment group (experimental group) had 72 cases. The specific data are shown in Table 1. The two groups showed no significant differences (p > 0.05) in Wagner grading, gender, ulcer area, age, course of disease, location, and vascular occlusion (ABI and TcPO2). All patients underwent vascular ultrasonography or CT angiography and foot X-ray before surgery. There were 14 cases of complications with hypertension, 11 cases of coronary heart disease, 6 cases of prior myocardial infarction, and 4 cases of prior cerebral infarction. All patients involved in these cases had no history of cerebral hemorrhage within the previous 6 months. All cases met the diagnostic criteria for diabetes, arteriosclerosis obliterans of lower extremities, and DFU. The main causes of DFU were nail injury, burns, crush injuries due to ill-fitting shoes, mosquito bites, and ankle scratches. All patients experienced coldness, numbness, pain, and intermittent claudication of the feet and/or lower limbs. All patients experienced varying degrees of lower extremity vascular disease. In 76 patients in this study (63.3%), the degree of vascular occlusion exceeded 50%.
Demographic data
ABI, ankle–brachial index; TcPO2, transcutaneous oxygen pressure.
Treatment methodology
Control group
Patients in the control group underwent traditional treatment methods: (1) Medical symptom treatment: After hospital admission all patients were offered low-salt and low-fat diabetic diets, and their blood glucose was strictly controlled at normal levels (<10.0 and <7.8 mM, for random and fasting blood glucose, respectively). 7 Conventional alprostadil injection was adopted to improve peripheral circulation and mecobalamin tablets were given to support nerve health. Antibiotics were used according to wound bacteria culture results and systemic conditions. Supportive treatment was applied for anemia and hypoalbuminemia and other conditions. (2) Surgical debridement and dressing changes were made to remove necrotic tissue according to the wound size and depth. Limbs with severe infectious and ischemic necrosis were amputated. In the control group, the dressings were changed repeatedly until the wound had healed.
Experimental group
In addition to traditional medical treatments, patients in the experimental group underwent the following treatments according to the wound conditions: (1) Early and thorough debridement: For severe DFU, surgical debridement is recommended immediately after admission. Necrotic tissue, degenerated tendon, and necrotic bone were removed while retaining sufficient parabiotic tissue to cover the epiphysis and maximize limb function. Bone fragments were removed in patients with osteomyelitis. Amputation was performed in patients with severe infectious and ischemic necrosis and no significant improvement after revascularization. (2) NPWT: all wounds were treated with NPWT for wound bed preparation after debridement. The pressure was delivered using the intermittent mode and maintained between 75 and 125 mmHg. The NPWT was removed after 5–7 days to observe the formation of granulation tissue. If the wound bed was not satisfactory, additional debridement was applied and NPWT was resumed until the ideal wound granulation was achieved. (3) Vascular reconstruction: The blood vessels of the lower extremities were first evaluated. All patients should complete routine examinations such as vascular ultrasound or lower extremity artery computer tomographic angiogram (CTA) after admission. The indications for vascular reconstruction were persistent rest pain, vascular ultrasound, or CTA refers arteriosclerosis obliterans (ASO), 8 ABI <0.40, and patients without severe cardiopulmonary insufficiency or vital organ damage. For patients meeting the above indications, vascular reconstruction surgery was performed. Revascularization involved endovascular treatment (EVT) and bypass grafting (BPG). Through revascularization, we reopened stenotic vessels and improved limb circulation. (4) Wound repair: After wound bed preparation, the following wound repair procedure was conducted: (a) for superficial wounds, dressings were changed until epithelium regeneration was achieved; (b) for large and refractory wounds with little secretion and fresh granules without edema, skin grafting was used to repair the wound; (c) for some wounds with exposed bone and tendon, the skin flap was used for coverage. The crystal clear flowchart is shown in Fig. 1.
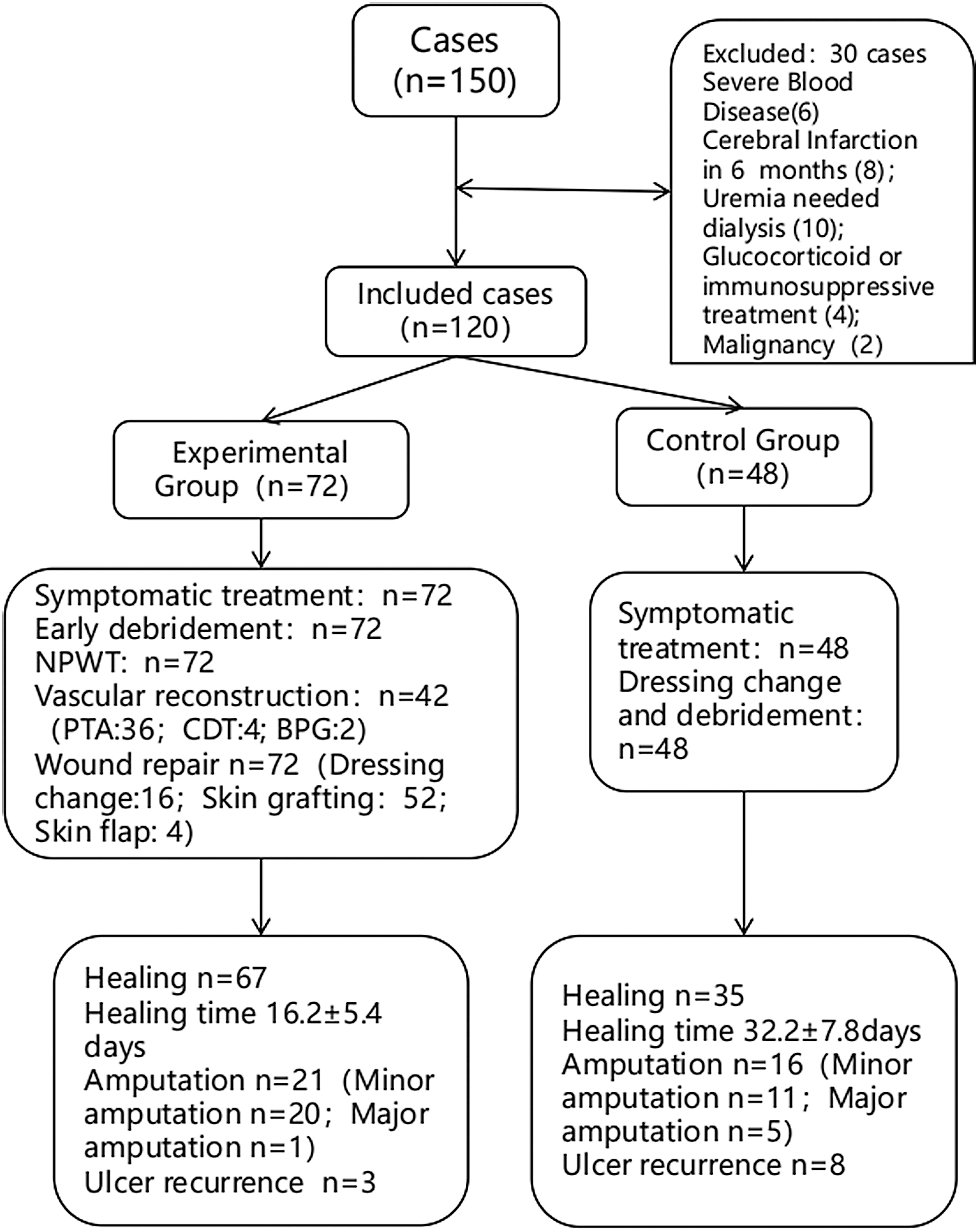
The flowchart of subjects assessed for participation in the study.
Evaluation of treatment efficacy
Observation indicators
Before and after treatment, we observed and recorded ABI and TcPO2, wound healing rate, healing time, ulcer recurrence rate, and amputation rate.
Criteria for evaluating treatment efficacy
After 1 month of admission, the outcomes of the treatment were categorized as: Cure: 100% wound closure; markedly effective: reduction in ulcer size by ≥2/3 with no exudation; effective: reduction in ulcer size by ≥1/3 with no significant exudation and little granulation; ineffective: no obvious change or further enlargement of the gangrenous wound. Healing cases include cured cases, and cases for which the treatment was effective or markedly effective. Healing time is the duration of the treatment until the wound is healed effectively (including cure, markedly effective and effective).
Follow-up
After discharge, patient follow-up continued for 6–12 months. Patients with nonhealing DFU were followed up once a week and patients with healed DFU were followed up once a month after discharge. All patients were under strict blood glucose control, consumed a low-salt and low-fat diet and received neurotrophic treatment. The criteria for DFU recurrence was wound deterioration or ulcer recurrence. Results of evaluations were recorded for all study cases.
Statistical methods
For parametric data, when variances in the groups were the same, a one-way ANOVA was used to compare differences among groups. For nonparametric data, or when variances in the groups differed, a χ 2 test was performed. All statistical analyses were performed using SPSS version-20.0 software (IBM), and a p-value <0.05 was considered significant. For survival analysis, the Kaplan–Meier curve was performed.
Results
Revascularization and wound treatment
A total of 46 patients in the experimental group had indications for revascularization, which was accepted by 42 patients. Among them, 36 were treated by percutaneous transluminal angioplasty (PTA); 4 by catheter-directed thrombolysis (CDT); and 2 by BPG. The postoperative ABI and TcPO2 were improved after revascularization compared with preoperative levels (ABI: 0.75 ± 0.21 vs. 0.35 ± 0.16; TcPO2: 36 ± 6 mmHg vs. 15 ± 4 mmHg) (p < 0.05) (Table 2). A typical case is shown in Fig. 2.
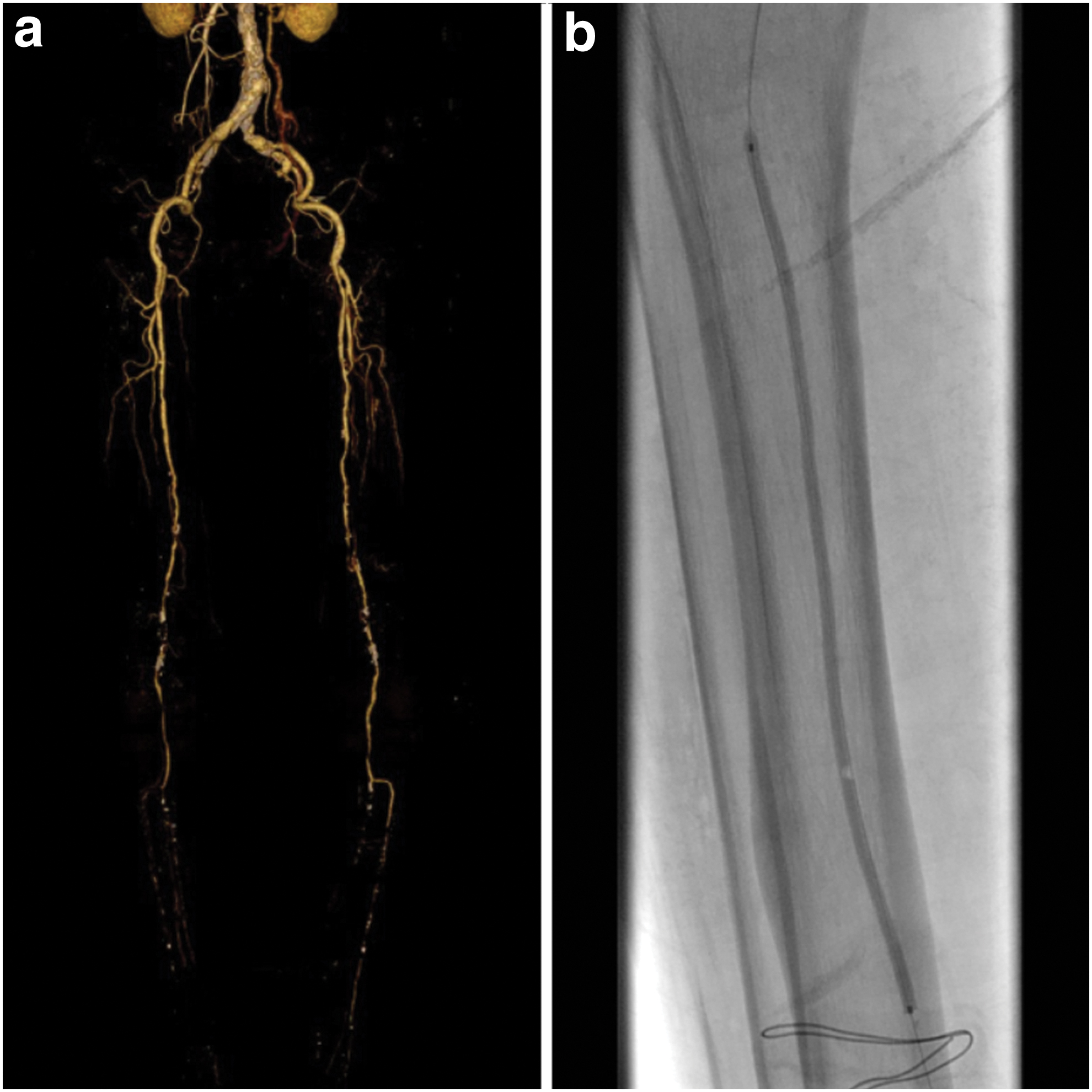
Revascularization of lower limb.
Comparison of vasculature conditions between the pre and past of revascularization
Healing condition
The five-in-one treatment produced significant improvements in wound healing. Among the 72 patients in the experimental group, wounds in 67 patients (93.0%) had healed with an average healing time of 16.2 ± 5.4 days. Among the 48 patients in the control group, 35 patients (72.9%) had healed with an average healing time of 32.2 ± 7.8 (p < 0.01) (Table 3).
Comparison of healing conditions between the two groups of patients
In the experimental group, 38 patients (52.8%) were cured. The treatment was markedly effective for 17 patients (23.6%), effective for 12 patients (16.7%), and ineffective for 4 patients (5.6%). One patient (1.4%) was lost to follow-up. The healing rate was 93.1% (Table 3).
The Kaplan–Meier graph in Fig. 3 shows a significant reduction in the healing time of experimental group compared with the control group.
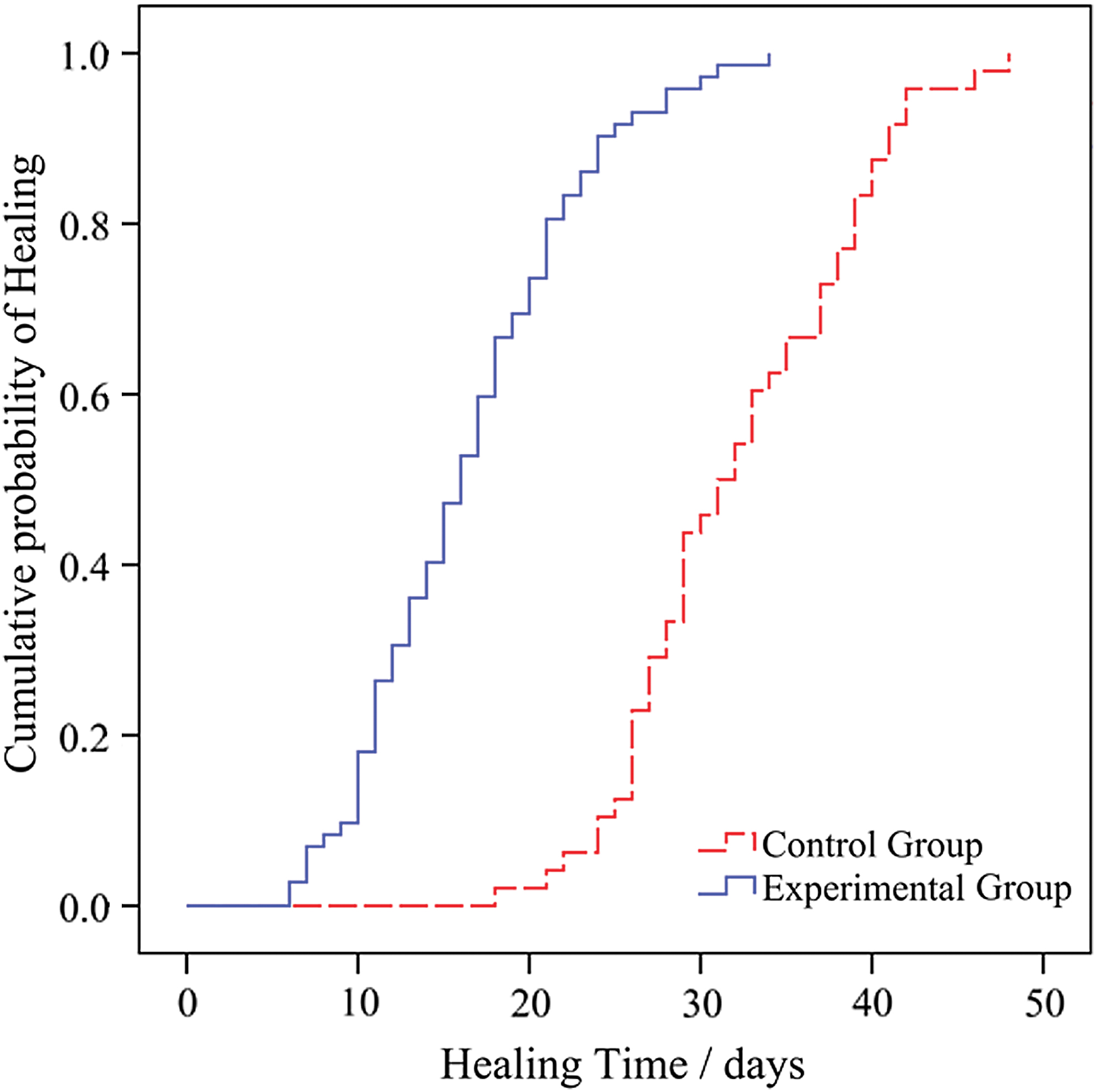
Kaplan–Meier plot for the cumulative proportion of patients healed. Color images are available online.
Images for a representative clinical patient that underwent five-in-one comprehensive limb salvage treatment are shown in Fig. 4.

The case of the five-in-one comprehensive limb salvage technologies of treating severe diabetic foot.
In the experimental group, 27 patients (64.3%) treated with revascularization were cured. Meanwhile, the treatment was markedly effective for eight patients (19.0%), effective for six patients (14.3%), and ineffective for one patient (2.4%). The healing rate was 97.6% (Table 4). Among experimental group patients that did not undergo revascularization, 11 patients (36.7%) were cured. The treatment was markedly effective, effective, and ineffective for nine, six, and three patients (30.0%, 20.0%, 10.0%), respectively. One patient (3.3%) was discharged for other reasons. The healing rate was 86.7% (Table 4).
Comparison of healing conditions after revascularization in the experimental group
In the control group, the wounds in 10 patients (20.8%) were cured. For the remaining patients, treatment for wound healing was markedly effective for 14 patients (29.2%), effective for 11 patients (22.9%), and ineffective for 9 patients (18.8%). Four patients (8.3%) were discharged for other reasons. The healing rate was 72.9%, which was substantially lower than that of the experimental group (p < 0.01; Table 3).
Amputation
In our research, 42 cases of diabetic foot gangrene (experimental group: 26; control group 16) were included. Among both groups, 37 patients underwent amputation during hospitalization. The total amputation rate in gangrene patients was 88.1% (Table 5).
Comparison of amputation (toes/minor/major limbs) condition in the diabetic foot gangrene patients
In the experimental group, 26 patients were diagnosed with diabetic foot gangrene. Twenty-one patients underwent amputation, including 15 cases of amputated toe (28 toes), 5 forefoot amputations, and 1 lower leg amputation. The amputation rate for major limbs was 1.4%. The total amputation rate for limbs (toes) was 29.2% in this group.
In the control group, 16 patients were diagnosed with diabetic foot gangrene, and all of them underwent amputation. Of these, 5 were toe amputations (12 toes), 6 were amputation of the forefoot, 3 were lower leg amputation, and 2 cases were amputation at the thigh. The amputation rate for major limbs was 10.4% and the total amputation rate was 33.3%. Thus, the major limb amputation rate for the experimental group was significantly lower than that of the control group (1.4% vs. 10.4%, p < 0.05), whereas there were no significant differences between the groups for the total amputation rate (29.2% experimental vs. 33.3% control; p < 0.63) (Tables 5 and 6).
Comparison of amputation (toes/minor/major limbs) condition in the two groups of patients
Follow-up
Among the study subjects, 117 (97.5%) were followed up for 6–12 months (2 and 1 patients were lost to follow-up in the experimental and control groups, respectively). In the experimental group, three patients (4.3%) had ulcer recurrence, whereas two cases had ulcer recurrence in situ and one case had ulcer recurrence at other locations. In the control group, eight patients had ulcer recurrence and there were four cases of ulcer recurrence in situ and four cases of ulcer recurrence at other locations. The recurrence rate for the control group was significantly higher than that for the experimental group (17.0% vs. 4.3%; p < 0.05; Table 7).
Comparison of ulcer recurrence rate in the two groups of patients
Discussion
Treatment decisions for DFU should be based on lesion severity, blood vessel condition, infection status, and neuropathy. 9 In our study, we concluded that the five-in-one comprehensive limb salvage treatment technologies enhanced the healing rate of severe DFU, shortened the healing time, and reduced the recurrence rate of ulcer and major amputation. Thus, we proposed this multidisciplinary model for treatment of DFU. The Burn Surgery department led the multidisciplinary team, endocrinologist provided treatment plans for blood glucose control, and vascular surgeon evaluated the need for the vascular reconstruction. Afterward, according to the chronic ulcer condition, surgeons performed surgical debridement or amputation, with NPWT. After evaluation of granulations of the wound, we treated with dressing change, skin graft, or local flap. For large tissue defect, we consulted our case with the Plastic Surgery and Microsurgery department. Follow-up study was conducted by Burn Surgery and Endocrinology departments. In the diagnosis and treatment of DFU, our multidisciplinary team closely cooperated and worked out the treatment plans, making the best of our medical resources. The results were discussed as follows.
The healing rate of the experimental group (93.1%) was significantly higher than that of the control group (72.9%) (p < 0.05). The healing time (16.2 ± 5.4 days) was significantly shorter than that of the control group (32.2 ± 7.8 days) (p < 0.05), which indicated that the wound healing condition may be improved by comprehensive treatment. The normal wound healing process went through three stages: inflammatory stage, proliferative stage, and mature stage. 10 However, peripheral neuropathy, peripheral vascular disease, infection, persistent hyperglycemia, and other factors could affect healing of DFU, leading to delayed healing or nonhealing. 10 In this study, various methods were used to intervene the wound healing inhibition factors, and then, to promote wound healing. Specific techniques of these five-in-one method have shown their effect on DFU in the previous literature, and our study aims to explore the effect of comprehensive treatment. Symptomatic medical treatment is important, including controlling blood sugar, improving microcirculation, preserving nerve function, and using antibiotics. 11 Debridement is the key to control infection and it cannot be replaced by antibiotics. 12,13 In this study, the control group used minor debridement or dressing change, resulting in smaller tissue defects. However, possible incomplete debridement may lead to more severe infection, and even worse, amputation, prolonged hospitalization, and higher medical costs. The experimental group emphasizes the thorough and extensive debridement at the early stage, so as to remove the necrotic tissue and control infection quickly even if it may cause large tissue defects. 13 NPWT is a reasonable choice for management of cutaneous wound. 14,15 It has been reported that NPWT has better effect in treating DFU than traditional dressing change by achieving better wound bed, shortening hospitalization, reducing nursing and dressing costs, and alleviating pain. 16 In this study, all the experimental groups received NPWT treatment, and the appropriate negative pressure, mode, and timing were selected according to the specific situation. Since most DFU in this study were associated with peripheral vascular diseases or infections, the application of NPWT should be more cautious. For severe infectious wound, NPWT should be applied to the wound without obvious infection or bleeding tendency after debridement and hemostasis. For sever ischemic wound, NPWT treatment may not be applicable because it might exacerbate ischemia, but low-pressure treatment would be effective in some cases. 16 After wound bed preparation, the granulation tissue is fresh and vigorous, which allows the wound to be repaired according to the situation. In general, smaller DFU areas (≤3 cm2) can be healed through dressing changes alone. For larger areas, further surgical repair is required. Surgical methods include autologous free skin grafting and skin flap transplantation. 17 In the experimental group, 16 cases were treated with routine dressing change, 52 cases underwent skin grafting, and 3 cases were treated by local flap.
In addition, an intragroup comparison of the revascularization in the experimental group indicated that, compared with the nonrevascularization group (86.7%), the revascularization group had a significantly higher wound healing rate (97.6%) (p < 0.05). Previous studies have also shown that vascular reconstruction can improve perfusion of lower limbs and promote wound healing. 18 But the indications, methods, and timing of revascularization were controversial. Generally speaking, severe limb ischemia requires vascular reconstruction, 19 but it has a debate over how to choose vascular reconstruction method. Currently, EVT is becoming the first choice for revascularization, but there was no obvious evidence to prove that EVT is superior to BPG. 20 In our research, 42 cases of revascularizations were performed, and among those, 36 patients underwent PTA, 4 patients underwent CDT, and 2 patients underwent BPG. For interventional treatment, diagnosis of TASC A and B lesions 21 that are generally considered to be the primary indication for EVT, and other indications for interventional treatments are listed as follows: single artery occlusion has better results compared with occlusion of multiple arteries; enhanced tibiofibular artery or the beginning of the anterior tibia or posterior tibial artery; and fewer collateral branches associated with shorter disease course. BPG was indicated in patients with younger age, less comorbidities, good vascular condition with available donor vessels, large tissue defect, and long lesion length. 22 After revascularization, the vascular reconstruction group showed significantly improved ABI (0.75 ± 0.21 vs. 0.35 ± 0.16, p < 0.05) and TcPO2 (36 ± 6 mmHg vs. 15 ± 4 mmHg, p < 0.05) compared with prevascularization. Besides, the timing of vascular reconstruction is also difficult to manage in clinical treatment. Debridement or revascularization, which one is the priority? The guidelines of the American Society for Vascular Surgery (SVS) and the International Working Group on the Diabetic Foot (IWGDF) emphasized the necessity for vascular reconstruction in ischemic lesions. 17 On the other hand, the Wound Healing Society (WHS) Guidelines suggest that the necrotic tissue should be thoroughly debrided. 5 In this study, for patients with indications of vascular reconstruction, debridement should be performed in advance if the wound is severely infected, and after infection controlled, vascular reconstruction should be performed during NPWT treatment time. 23 If the infection is not so severe, vascular reconstruction is recommended first. Most of the cases can effectively improve vascular conditions and promote granulation growth. However, the restenosis rate after EVT is relatively high, as well as recurrence rate of ulcer. Thus, the efficacy of EVT in DFU, especially the long-term efficacy, is still unclear. This study only analyzed the wound healing rate after vascular reconstruction and found that the wound healing rate was significantly improved after vascular reconstruction.
In some cases, amputation is inevitable. The indications for minor amputations were acute osteomyelitis, neurotropic ulcer, arterial and venous blood flow to the other toes, and gangrene of toes with metatarsal affection. 24 Major amputations were considered when the wound could not be closed by a minor amputation or severely infected ischemic limbs, which could cause life-threatening conditions. 22 In our study, we observed no significant differences in the total amputation rate (amputation of toes/minor amputation/major amputation) between the experimental group and control group (29.2% vs. 33.3%, p = 0.628). The reasons may be as follows: First, the patients included in this study were severe DFU with Wagner grading ≥3, most DFU performed minor amputation to control infection in the early stage 25 ; second, high restenosis rate after vascular reconstruction and the presence of vascular reperfusion injury, resulting in ulcer recurrence and inevitable amputation 5 ; third, relatively small sample size can also affect the interpretation of the result. However, the major amputation rate of the experimental group was significantly lower than that of the control group (1.4% vs. 10.4%, p < 0.05). It may be related to reduce the amputation risk factors by comprehensive limb salvage technology to some extent.
Peripheral arterial disease and infection are the major factors leading to amputation in severe DFU. 26 The WIfI classification system of the SVS evaluates the risks of limb amputation and benefits of vascular reconstruction from Wound, Ischemia, and Foot Infection condition. 27 This classification is of great significance for clinical therapy and provides a new model for lower limb risk assessment. Comprehensive limb salvage therapy can improve the wound, ischemia, and infection condition to some extent, and some patients can achieve functional reconstruction without major or minor amputation. Major amputation could lead to loss of body function, reliance on the prosthesis, complicated prosthesis fitting, higher expenses of rehabilitation and medical care, residual limb abrasion, higher risks of ulcer recurrences, and higher mortality rate. 28 Thus, we knew that lower major amputation rate did make a difference.
Risk factors of ulcer recurrence include peripheral neuropathy, foot deformity, peripheral vascular disease, history of ulcer, amputation, and poor blood glucose control. 29 In this study, the recurrence rate of the experimental group (4.3%) was lower than that of the control group (17.0%) (p < 0.05), which may be because of reducing the recurrence-related factors by comprehensive treatment. Therefore, even after the ulcer heals, patients with these factors have higher possibility of ulcer recurrence. It was reported that the recurrence rate of DFU is about 40% within 1 year, almost 60% within 3 years, and 65% within 5 years. Long-term studies suggest that appropriate prevention can prevent ulcer recurrence to some extent. 5
In conclusion, comprehensive limb salvage treatment for DF reflects a multidisciplinary concept that integrates conventional, surgical, and maintenance treatments. In this study, the experimental group had significantly improved wound healing rates and shortened healing time, in addition to lower recurrence and amputation rates compared with the control group. According to the results of this study, a multidisciplinary cooperative model for comprehensive medical and surgical treatments should be established for DF. Through revascularization and microsurgery of local wounds, the amputation rate of gangrene patients was reduced while function was preserved to yield an overall improvement in patient quality of life.
Innovation
A five-in-one comprehensive treatment method provides a multidisciplinary cooperative model for comprehensive medical and surgical treatments for DF, and our study proves that it plays an important role in limb salvage for severe DF, which could be served as a clinical guidance in multidisciplinary and individualized treatment.
Key Findings
A five-in-one comprehensive treatment for DFU improves wound healing rate (72.9% vs. 93.1%; p < 0.01) and reduces wound healing time (16.2 ± 5.4 days vs. 32.2 ± 7.8 days; p < 0.05) than traditional treatment.
A five-in-one comprehensive treatment for DFU reduces amputation rate of major limbs (1.4% vs. 10.4%, p < 0.05), and reduces ulcer recurrence rate (5.6% vs. 14.6%; p < 0.05) than traditional treatment.
Revascularization can significantly improve ABI (0.75 ± 0.21 vs. 0.35 ± 0.16, p < 0.05) and TcPO2 (36 ± 6 mmHg vs. 15 ± 4 mmHg, p < 0.05) in patients with indications for revascularization therapy.
Footnotes
Acknowledgment and Funding Sources
None declared. This study was supported by the National Natural Science Foundation of China (Grant No. 81871566, 81671935), the Science and Technology Planning Project of Guangdong Province, China (Grant No. 2017A040405026), and the Science and Technology Planning Project of Guangzhou City (Grant No. 2018-0402-SF-0686), and the Natural Science Foundation of Guangdong Province, China (Grant No. 2017A030313619).
Author Disclosure and Ghostwriting
No competing financial interests exist. The content of this article was expressly written by the authors listed. No ghostwriters were used to write this article.
About the Authors