
Abstract
Significance:
Fractional resurfacing involves producing arrays of microinjuries on the skin, by thermal or mechanical means, to trigger tissue regeneration. Originally developed for cosmetic enhancement, fractional resurfacing induces a broad array of improvements in the structural and functional qualities of the treated skin and is especially effective at returning defective skin to a more normal state. In addition to fascinating questions about the nature of this remarkable regenerative capacity, there may be potential utility in ulcer prevention by halting or even reversing the progressive decline in overall skin quality that usually precedes chronic wound development.
Recent Advances:
Photoaging and scarring are the two skin defects most commonly treated by fractional resurfacing, and the treatment produces profound and long-lasting improvements in skin quality, both clinically and at the cellular/histologic level. Chronic wounds usually occur in skin that is compromised by various pathologic factors, and many of the defects found in this ulcer-prone skin are similar to those that have seen improvements after fractional resurfacing.
Critical Issues:
The mechanisms responsible for the regenerative capacity of fractional resurfacing are mostly unknown, as is how ulcer-prone skin, which is usually afflicted by stressors external to the skin tissue itself, would respond to fractional resurfacing.
Future Directions:
Better understanding of the cellular and molecular mechanisms underlying the unique healing response to fractional resurfacing could reveal fundamental information about adult tissue regeneration, lead to improvements in current applications, as well as new therapies in other pathologic conditions.
Joshua Tam, PhD

Scope and Significance
Fractional resurfacing induces improvements in a broad array of structural and functional qualities in the treated skin. Here, we will review the clinical effects of fractional resurfacing, putative mechanisms involved, key unanswered questions, and potential application in chronic wound prevention.
Translational Relevance
Microinjuries induced by fractional resurfacing appear to have a unique regenerative capacity, perhaps best exemplified by their ability to produce dramatic improvements in scar tissue. The cellular processes and molecular mechanisms involved in this rare example of adult tissue regeneration, and its applicability in other defective skin conditions are promising avenues for translational investigations.
Clinical Relevance
Since many options for fractional resurfacing are already clinically available, expanding their utility to other skin defects should be relatively straightforward. Better understanding of the underlying mechanisms could enable more rational selection of treatment modality and parameters, which are currently widely variable and based mostly on the individual practitioner's clinical experience.
Overview
Fractional resurfacing to induce skin remodeling
Outside of early gestation, human skin wounds mostly heal by scarring, which is characterized by disorganized microanatomy, absence of dermal appendages, and myriad other structural and functional defects. 1 There is, however, one notable exception to this generalization: small (nominally 500 μm or less in diameter) wounds can regenerate completely, without scarring, even when total tissue loss is substantial—up to 50% of skin tissue within a treatment area can be removed in the form of microinjuries, and the subsequent remodeling process can actually lead to better-quality skin (Fig. 1). 2 –4 Various clinical modalities have been developed to take advantage of this phenomenon (Fig. 2), whereby arrays of microinjuries are produced by thermal (lasers and radiofrequency) or mechanical (microneedling) means, to induce tissue remodeling via a process known as fractional resurfacing. Our group has also utilized this principle to develop a new technology to harvest autologous skin tissue for wound repair 5,6 —this technology was the subject of our 2016 WHF 3M Fellowship research, and is now in early stages of clinical use. In this article, we will focus mainly on laser-based treatments, namely ablative fractional laser (AFL) and nonablative fractional laser (NAFL), as these have been studied more extensively than other modalities.
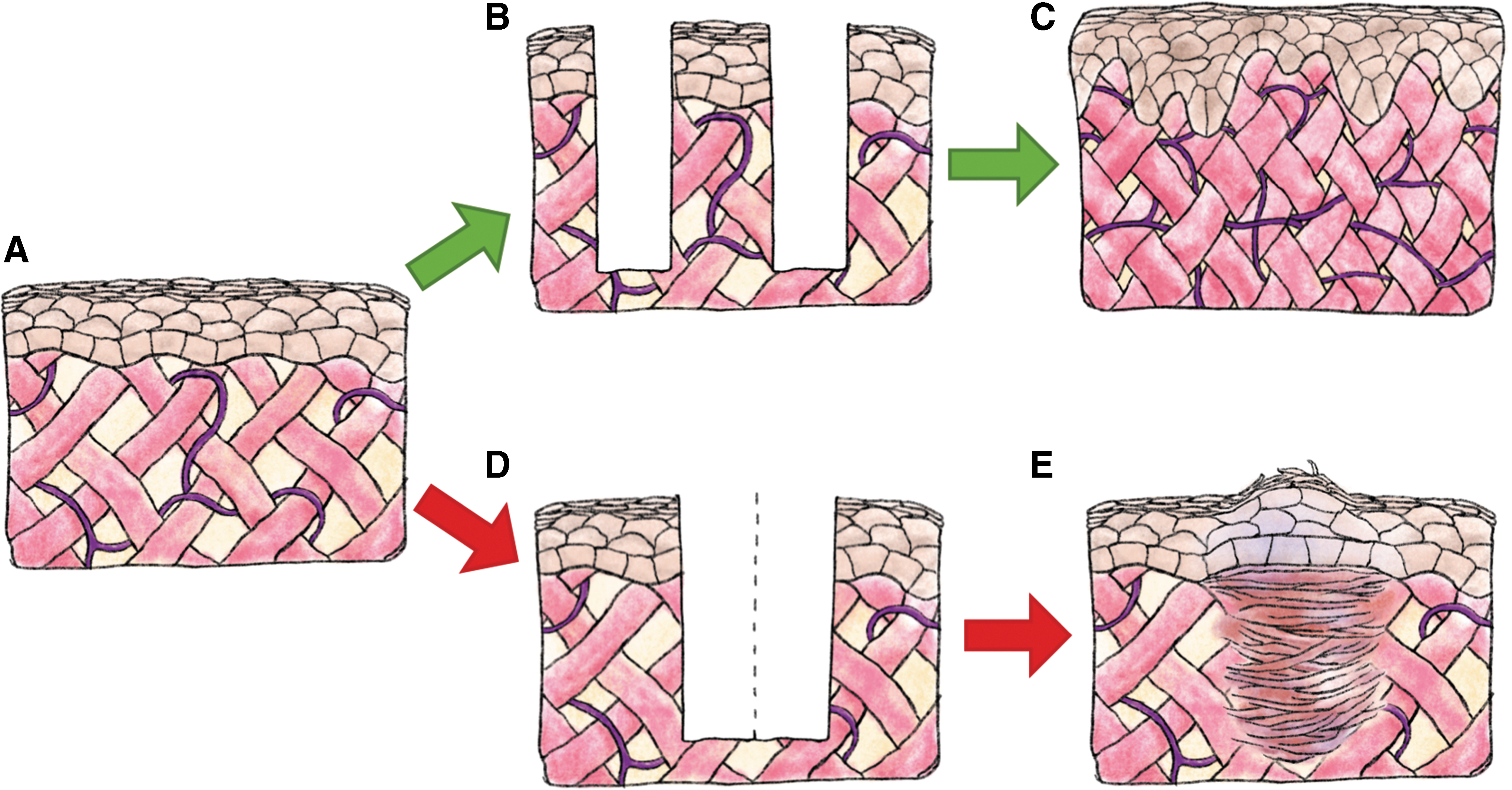
Size-dependent dichotomy in healing response. Untreated skin tissue is depicted in

Current clinical options for producing microinjuries.
Discussion
Fractional resurfacing is a popular procedure to “rejuvenate” skin by reducing the visible signs of photoaging, such as rhytids and dyschromia, 4 but beyond cosmetic enhancements, the treatment also leads to broad improvements in skin quality, including increased dermal thickness, synthesis and remodeling of extracellular matrix (ECM) components, reduced atypical keratinocytes, increased vascularity, improved rete ridge formation, reduced senescent fibroblast population, and restoration of proper response to ultraviolet light. 7 –9 Fractional resurfacing also has a unique ability to induce dramatic and lasting functional improvements in skin scars, including normalizing scar thickness, reducing pain and pruritus (suggesting resolution of underlying inflammation), increasing tissue pliability and range of motion, and improving overall quality of life. 10 –14 There have even been anecdotal reports of functional hair follicles and sweat glands regenerating in scars that had been devoid of these structures. 15,16
Curiously, fractional resurfacing seems to stimulate different remodeling responses in different defects. In hypertrophic scars consisting of dense, thick, disorganized collagen bundles, AFL induces looser but more organized collagen. 14,17,18 Conversely, atrophic scars—characterized by a paucity of collagen leading to depressions in the skin—respond to AFL by thickening of the epidermis and increasing dermal collagen deposition. 19 These findings suggest that, rather than inducing a constant set of effects, fractional resurfacing elicits a homeostatic response that returns the tissue to a more normal state. Consistent with this view, healthy skin showed no histological evidence of fractional resurfacing after 3 months 2,20 (whereas beneficial effects on scar remodeling persist for years 11 ), and pretreatment of normal skin in a large animal model provided no benefit toward the subsequent surgical scarring response. 21
Mechanisms
Despite strong clinical evidence of efficacy in a variety of dermatological conditions, the mechanism by which fractional resurfacing asserts its effects is still unclear. A few studies have detailed the histological and biochemical changes following fractional resurfacing, with particular focus on ECM arrangement, and known regulators of tissue remodeling, such as the transforming growth factor-β (TGFβ) pathway, matrix metalloproteinases (MMPs), and heat shock proteins (HSPs). These findings provide some insights into the potential mechanism of fractional resurfacing, but perturbation studies that could demonstrate which of these components are causal versus correlative are still lacking. It should also be noted that there is little clinical consensus on treatment settings (e.g., microinjury density and energy settings), and these vary widely in the literature. In this discussion, we will disregard specific treatment settings, and simply categorize treatments according to the modality used to produce microinjuries.
Transforming growth factor-β
TGFβ is important for normal wound healing, and a key regulator of fibrosis and scarring as it promotes expression of type I collagen (COL1A1) and tissue inhibitors of metalloproteinases (TIMPs). 22 TGFβ is secreted by immune cells during wound healing to stimulate fibroblast differentiation and collagenesis. 23 Latent TGFβ is stored in the ECM and can later be activated by matrix turnover, thereby coupling collagenesis to the mechanical properties of the ECM. 23 There are three TGFβ isoforms with distinct functions. TGFβ1 and TGFβ2 promote both wound healing and scar formation, while TGFβ3 inhibits scar formation and is considered particularly important for scarless healing of the fetus. 24 TGFβ signaling is often suppressed in chronic wounds. 25 TGFβ is also an important chemokine for macrophages and neutrophils following acute injury. 22
In photodamaged skin, TGFβ is upregulated 3 days post-AFL and expression decreases over 30 days. 26 Studies in burn scars using more frequent timepoints found biphasic TGFβ expression after fractional resurfacing. TGFβ1 and TGFβ3 are transiently upregulated 1 h postop. 27 TGFβ1 returns to baseline at 24–48 h, while TGFβ3 and TGFβ2 are downregulated compared to baseline. 27,28 TGFβ1 and TGFβ3 expression increases again 96 and 168 h postop. 27 One study on long-term TGFβ expression, using immunohistochemistry at baseline and 6 months postop, found that staining intensity for TGFβ1 is reduced at 6 months postop compared to pretreatment, and that TGFβ1 is primarily found in fibroblasts and in the ECM. 18
Interestingly, neutralization of TGFβ1 and TGFβ2 reduces scarring, but inhibition of just one of these has no effect, 29 highlighting the need to understand changes in each TGFβ isoform. However, the three TGFβ isoforms are frequently not distinguished in the literature, and TGFβ2 is often neglected even when individual isoforms are investigated. A better understanding of how each isoform is affected by fractional resurfacing, especially in the long term, is needed.
Heat shock protein
HSPs can be activated by many forms of stress, including heat, trauma, toxins, and hypoxia. 30 Classically, HSPs act as chaperones and promote cell survival by correcting stress-induced protein misconformations. 30,31 More recently, HSPs have been recognized as regulators of the wound healing response. 32 Dysregulation of HSPs is involved in a number of fibrotic conditions and different HSPs can either promote or inhibit TGFβ signaling. 33 –37 HSPs have also been investigated as potential therapeutic targets for fibrosis, either through inhibition (e.g., HSP90 inhibition reduces hepatic 38 and renal fibrosis 39 ) or induction (e.g., HSP70 induction reduces hepatic 40 and pulmonary fibrosis 41 ). These findings indicate competing roles for HSPs, and the relative importance of HSPs in fibrosis and wound healing is an area of ongoing research.
HSP47 is a chaperone involved in collagen processing, and its expression correlates with collagen synthesis and fibrosis progression in many organs. 33,42 The HSP70 family, primarily consisting of the constitutively expressed HSP73 and inducible HSP72, has also been studied in some detail. In photodamaged skin, AFL causes HSP70 upregulation from 1 h postop through day 14. 43 NAFL showed similar results. 44 The pattern of HSP expression has been further studied in healthy skin. NAFL caused upregulation of HSP47 and HSP70 in tissue immediately surrounding the microinjury at 1 day postop. 2,45 At day 7, HSP47 and HSP70 are expressed inside the treatment zone as well as more diffusely throughout the dermis. 45 NAFL and fractional radiofrequency microneedling have both been reported to induce HSP70 expression, 46,47 which is severely attenuated in diabetic skin, 48 with an expression time course that correlates with delayed healing. 49 Long-term upregulation of HSPs has been reported after large-area ablative laser resurfacing. 20 If a similar response occurs after fractional resurfacing, it could account for the ongoing remodeling of scars for months after treatment, although experimental confirmation is needed.
Collagen synthesis and degradation
In healthy tissue, there is a balance between collagen synthesis and degradation. 50 Tipping that balance either way is pathologic—excessive collagen synthesis leads to hypertrophic scarring, while excessive degradation is characteristic of both skin aging and chronic wounds. 51 –53
Collagen degradation is commonly estimated through MMP expression, but many factors influence MMP activity—most notably TIMPs and synthesis in an inactive proenzyme form—and the more accurate method for determining collagen degrading activity is zymography 54 ; however, such studies have yet to be performed for laser resurfacing techniques. MMPs are a large group of enzymes with varying activities for the many components of the ECM (collagens, fibronectin, laminin, etc.). In photoaged skin, MMP-1, MMP-3, MMP-9, MMP-10, MMP-11, and MMP-13 are upregulated between day 7 and 14 post-AFL. MMP-1, MMP-3, and MMP-13 expression drops off after day 14, while MMP-9, MMP-10, and MMP-11 expression continues to increase through day 21. 55 Similar effects have been reported for other modalities. NAFL caused upregulation of MMP-1, MMP-3, and MMP-9 at day 1 postop, with significant decay at day 7. 44 It was also found that MMP-1 and MMP-3 were localized to the treatment zone, while MMP-9 was dispersed throughout the dermis. 44 It is likely that there are similar patterns of MMP expression across the modalities, although with varying magnitudes. Far fewer MMPs have been investigated for AFL in scar tissue. One study reported MMP-1 upregulation at 48 h postop and no significant change in MMP-13. 28
Collagen synthesis is typically approximated by collagen mRNA levels. In scars, collagen mRNA exhibits a biphasic response to AFL in line with TGFβ expression. Both (COL1A1) and type III collagen (COL3A1) are upregulated at 1 h postop, fall below or near baseline at 24–48 h, then are again upregulated at 168 h. 27,28 NAFL in photodamaged skin reduced COL1A1 and COL3A1 at 1 day postop, followed by upregulation from day 14 through 28, with procollagen I protein levels following the same trend. 56 Immunohistochemical investigation of NAFL in healthy skin showed gradual increase in COL3A1 staining inside the treatment zone until 1 week postop. 2 In a healthy mouse model, AFL caused increased protein levels of COL3A1 from day 3 through 56 postop and COL1A1 from day 28 through 56. 57
These findings are not altogether surprising—as with any acute injury, laser resurfacing promotes matrix turnover in the short-term. While the remodeling phase of wound healing can continue for over a year after injury, 51 this on its own does not fully explain why there is continued scar regression in the months following treatment. Long-term measurements are required to determine how fractional resurfacing changes the balance between collagen synthesis and degradation.
Apoptosis
Fractional resurfacing causes tissue damage through thermal and/or mechanical injury. Apoptosis is an essential component of the biological responses to tissue damage. Once viewed as a largely cell-autonomous process, there is now increasing understanding that apoptosis has significant impact on the local milieu, inducing proliferation and remodeling of adjacent cells and tissue, at least, in part, via ectopic expression of wingless/integrated (Wnt) and induction of p53. 58 Apoptosis plays a key role in wound healing by inducing mitogenic signals that drive regeneration, 59,60 but there is currently little data on how apoptosis may be involved in the regenerative effects of fractional resurfacing. 61 Apoptosis was observed within 24 h of AFL and steadily declined over 7 days. The authors concluded that apoptosis induces a paracrine cascade that leads to cell proliferation and stimulates stem or progenitor cells to participate in tissue regeneration. 61 Another study compared five different laser devices using TUNEL assay. Thermal tissue damage and penetration depth differed widely, as did the extent of apoptosis and necrosis, 62 and it is unclear whether clinical outcomes correlate with the extent, location, or distribution of apoptosis. It has been proposed that apoptosis can alter local tissue tension, induce remodeling in nearby tissue, and influence the behavior of neighboring cells through paracrine signaling. 58 Given that scars are characterized by increased stiffness that can be substantially improved by fractional resurfacing, apoptosis could play a role in treatment-induced tension relief in fibrotic tissues. Wnt proteins, which are often secreted by apoptotic cells, can regulate the cytoskeleton 63 and are also important signaling molecules in epidermal skin stem cells. 64 Whether those two mechanisms merely coexist or actually act in concert is unclear. 58
Other findings
Where overlap exists in the literature, cytokine expression between the different laser resurfacing modalities is generally similar. The proinflammatory cytokines interleukin (IL)-1β, IL-6, tumor necrosis factor alpha (TNFα), and monocyte chemoattractant protein 1 (MCP-1) are all upregulated shortly after treatment. IL-6 and MCP-1 return to baseline in 96 and 24 h, respectively. 27 TNFα expression significantly decays within 1 week. 44 IL-1β upregulation is longer-lived, with expression sustained up to 14 days postop. 44 One study reported basic fibroblast growth factor (FGF) expression decreased at 48 h, 28 while another found increased expression at 3 and 30 days postop. 26,57
Vascular endothelial growth factor (VEGF) is a key regulator of angiogenesis and vascular permeability in the early stages of the response to injury. AFL caused significant upregulation of VEGF at day 1 and 3 postop in a murine model, with no significant difference from controls after day 7, 57 while mild upregulation of VEGF up to 30 days postop was reported in photodamaged human skin. 26 These findings are consistent with reports of increased vascularity after fractional resurfacing. 9,65 It has also been reported that VEGF can influence MMP activity and collagen deposition 66 and there is some evidence that it may promote scar formation in later stages of wound healing. 67 Further investigation of VEGF is required to better understand its role in scar remodeling.
Qu et al. showed that miR-18a and miR-19a expression is increased after AFL in scars. 28 These miRNAs belong to the miR-17/92 cluster, which has been shown to suppress TGFβ signaling. 68 Most research to date has focused on the role of miR-17/92 in cancer, but a few studies have also indicated a potential protective role in fibrosis. 69,70
Kim et al. performed the only transcriptome level study to date for fractional laser resurfacing, although their analysis of the dataset was limited to a handful of genes. 71 This study looked at AFL in healthy skin and emphasized Wnt5a, an antiapoptotic gene and fibroblast mitogen, and cysteine-rich angiogenic inducer 61 (CYR61), which has been shown to inhibit COL1A1 synthesis and promote degradation. It was also shown that CYR61 expression was upregulated throughout the dermis, rather than isolated to the injury sites.
Other modalities for fractional resurfacing
Microneedling is another common method for producing microinjuries. It is generally not as effective as laser resurfacing but has lower risk of negative outcomes, so it has achieved some popularity as a treatment for individuals seeking minor improvements. Microneedling involves a drum covered in fine needles (usually 0.5–1.5 mm in length) repeatedly rolled over the skin to create hundreds of punctures per square centimeter. 72,73 It is most commonly used for treatment of atrophic scars from acne, as it has shown limited success for hypertrophic scars. 74
The mechanism of microneedling has received even less attention than that of laser resurfacing. At one point, a theory for microneedling was proposed based on the needles creating electrical field perturbations to stimulate proliferation and release of growth factors. 74 However, recent publications suggest that microneedling functions similarly to fractional laser resurfacing. Microinjuries induce a minor acute immune response, with associated release of inflammatory cytokines. TGFβ and FGF promote fibroblast proliferation and differentiation, increased matrix turnover, and angiogenesis. The result is normalization of the matrix architecture with increased deposition of collagen and elastin. 73,75
Fractional radiofrequency irradiation is another common microinjury method. Similar to NAFL, this technique creates small, isolated columns of thermal injury. The main benefits of radiofrequency over laser resurfacing are less disruption of the epidermis, lower risk of dyspigmentation, and avoidance of side effects caused by light absorption by melanin in darker skin types. 78 Broadly speaking, fractional radiofrequency causes similar effects to laser resurfacing, with upregulation of HSPs, MMPs, TGFβ, and proinflammatory cytokines leading to increased collagen type I, collagen type III, and elastin in the dermis. 79,80
Mechanically removing small cores of skin tissue by fractional skin harvesting is a relatively new technique. Our group has primarily focused on using it to obtain autologous tissue for wound repair, but others have shown that the procedure leads to improvements in skin qualities in the porcine model, including thickening of both epidermis and papillary dermis, increased rete ride undulation at the dermal–epidermal junction, and increased synthesis of collagen and elastin fibers. 65 This raises the potential for the treatment to have dual benefits—fractional skin harvesting from areas surrounding a wound could provide anatomically matched autologous skin tissue to be transplanted into the wound to accelerate healing, while the harvesting procedure could induce beneficial skin changes leading to increased resistance to further wounding.
Potential utility in chronic wound prevention
Chronic wounds typically occur in skin compromised by various underlying etiologies, such as complications associated with venous insufficiency (e.g. stasis dermatitis, 81 lipodermatosclerosis, 82 atrophie blanche 83 ), diabetes (e.g. microangiopathy, neuropathy, 84 necrobiosis lipoidica 85 ), prolonged pressure, and aging. Although the underlying etiology may differ, chronic wounds are almost always preceded by a progressive decline in the overall skin quality, which renders the skin more susceptible to injuries and less able to heal from them. Defects found in ulcer-prone skin include effacement of rete ridges (the undulating projections at the dermal–epidermal junction that anchor the epidermis to the underlying dermis), 86 abnormal epidermal structure and weakening of the epidermal barrier, 87,88 breakdown of ECM components 89,90 and disorganization of ECM structure, 86,91,92 fibrotic changes, 93,94 persistent inflammation, 92 accumulation of advanced glycation endproducts, 95 and senescent cells. 96,97 These deteriorations in skin quality often lead directly to negative functional consequences. Diabetes and venous insufficiency are both associated with a host of skin symptoms. 82,98 Flattening of the dermal–epidermal junction and disruption of the dermal ECM organization lead to significant declines in biomechanical properties of the skin. 99 The accumulation of senescent cells appears to be at least partially responsible for age-related disorders, as removal of senescent cells attenuates many of these disorders in animal models. 100 Prolonged and dysregulated inflammation is a major contributing factor to impaired ulcer healing. 101 The period of skin degradation before ulcer formation makes chronic wounds somewhat predictable, and also presents a potential window of opportunity for the application of prophylactic measures to prevent ulceration. This is not a new concept—various modalities such as barrier creams, compression therapy, and preventative offloading are routinely applied clinically for ulcer prevention by reducing the harmful impacts of external stressors on the skin. However, relatively few treatments are designed to directly improve the quality of the skin itself.
There have been a few reports on using fractional resurfacing to treat chronic wounds, with enhanced healing after fractional laser treatments reported in an animal study of delayed diabetic healing 102 and several clinical cases of chronic wounds associated with scars, 103 –105 epidermolysis bullosa, 105 and traumatic lesions in the elderly. 106 More extensive studies are needed to determine if this treatment is broadly applicable to different chronic wound types. In particular, wounds associated with defects that are known to be ameliorated by fractional resurfacing (some examples listed in Table 1) may make for promising targets. Chronic wounds may respond differently to different fractional resurfacing modalities and treatment parameters, depending on specific underlying etiologies, disease stage, and wound care regimen (dressings, compression, topical and systemic therapies, debridement, and so on), and information on these differences should be helpful for deciding whether/when fractional resurfacing may be beneficial.
Skin defects found in ulcer-prone skin, and reports of similar defects ameliorated by fractional resurfacing
ECM, extracellular matrix; HSP, heat shock protein; TGFβ, transforming growth factor-β.
Given the ability of fractional resurfacing treatments to improve skin quality in different skin disorders, and particularly in ameliorating various defects (e.g., deficiencies in vascularization, ECM production and organization, accumulation of senescent cells) that are similar to those found in chronic wounds (Fig. 3; Table 1), it may be a potential approach to prevent skin ulceration by prophylactically reversing at least some of the defective qualities of ulcer-prone skin. In addition, using it to induce remodeling in scars from previously closed ulcers is another application that may positively impact the chronic wound trajectory, since scars are functionally defective and prone to reinjury 107 —properties that are likely to contribute to the high recurrence rate of chronic wounds. It should be noted that ulcer-prone skin is almost always afflicted by pathologies that extend beyond the local skin tissue (e.g., impaired circulation, nutritional deficiencies, biomechanical abnormalities), and these are unlikely to be affected by fractional resurfacing (or any other local treatment). However, to the extent that improved skin quality could benefit disease trajectory, fractional resurfacing may be a useful addition to the armamentarium of comprehensive chronic wound management. How ulcer-prone skin would respond to fractional resurfacing, and whether this treatment could reduce susceptibility to ulceration, should make for intriguing subjects for scientific and clinical investigations.
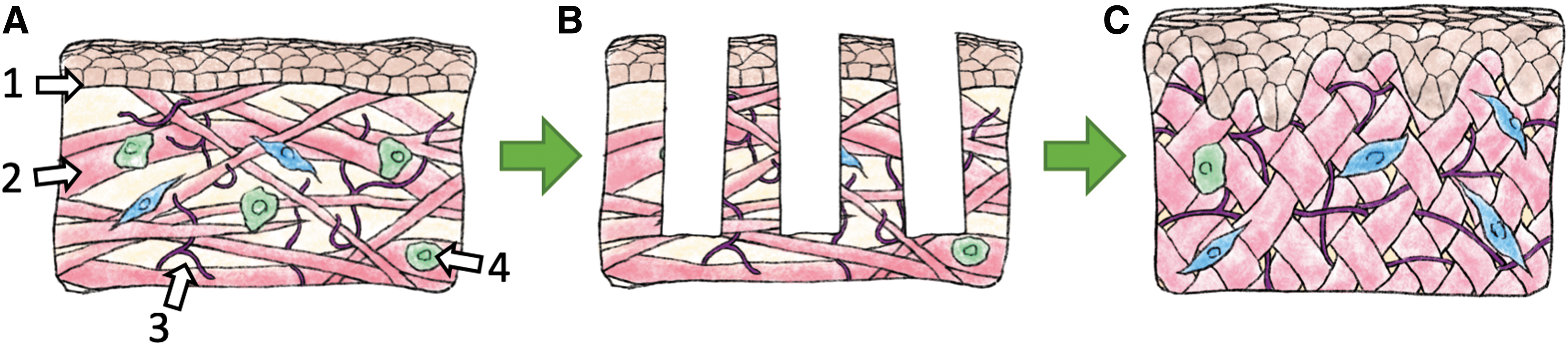
Corrective effects of fractional resurfacing on defects similar to those found in ulcer-prone skin.
Key remaining questions
While the clinical evidence is unequivocal that fractional resurfacing can induce dramatic regenerative effects, its mechanism(s) of action is still poorly understood. One fundamental unknown is why there is this size-dependent dichotomy in wound repair (Fig. 1), toward regeneration versus scarring. Considering that simple surgical incisions still heal by scarring, despite there being no tissue loss, it appears that factors such as wound volume, oxygen diffusion limit, and proximity of the wound area to uninjured tissue, are not primarily responsible. One potential contributor is the difference in local tissue mechanics–mechanical stresses have a profound effect on scarring, 108 and different wound shapes are likely to result in different mechanical cues, for example, small circular wounds may cause less disruption to Langer's lines than a longer wound of similar total volume. Other possibilities include different cell populations involved in repair (local cells from neighboring areas vs. those recruited from the systemic circulation), different activation status and behaviors in the same cell populations, and differences in the postinjury inflammatory response. Detailed, well-controlled comparisons of the healing responses following different wound sizes/shapes may yield important insights about deciding factors governing scarring versus regeneration in adult tissues.
There are a number of foundational questions whose answers should have broad implications for whether/how fractional techniques could be utilized to prevent/treat chronic wounds. One critical question is whether the various underlying etiologies associated with chronic wounds could change the threshold at which the skin could spontaneously heal and remodel after fractional resurfacing, since that ability is a prerequisite for applying fractional treatments. There is at least one clinical report of deficient healing after fractional resurfacing in skin damaged by exposure to radioactive phosphorus. 109 While arguably an extreme example, it does demonstrate the possibility for the skin quality to be so compromised that it has difficulty healing even very small wounds. This may also affect the choice of treatment modality, for example, nonablative treatments are generally considered to be less aggressive than ablative treatments, and the former may be more suitable for strengthening friable skin that may not tolerate ablative injuries. Conversely, ablative fractional treatments at more aggressive settings may provide a more potent “jolt” to push stalled wounds toward an acute healing response. The effectiveness of fractional resurfacing in treating photoaged skin is at least partly attributed to its ability to remove tissue with decades' worth of accumulated UV damage and replacing it with new tissue that had not (yet) been exposed to the sun. A similar mechanism may be beneficial for skin with accumulated damage due to aging, diabetes, and so on—this could be verified experimentally by measuring levels of known molecular byproducts associated with these etiologies. Other pertinent unknowns include potential differences in response based on body site (e.g., shin vs. plantar surface), the cellular sources of the various signaling molecules elicited by fractional resurfacing (described above in section “Mechanisms”), and whether there are specific differences in the healing response to microinjuries induced by thermal versus mechanical means. A better understanding of these practical questions could aid in more rational selection of treatment parameters and decisions regarding preventative versus therapeutic applications.
There remains a crucial missing link between the short-term response and long-term results of fractional resurfacing. The sequence of events immediately following treatment and the eventual histological changes are both well described, but the mechanism by which one leads to the other is poorly understood. Through speculation and bringing in elements from general fibrosis research, the pieces can be connected in a few different ways to formulate potential mechanisms. For scar remodeling, mechanical changes in the ECM may again play a substantial role. Microinjuries enable infiltration of the densely packed, highly cross-linked collagen fibrils that are resistant to degradation. 110,111 The acute inflammatory response recruits a population of cells (macrophages and neutrophils) that strongly promote matrix turnover as a part of the normal wound healing process. This short but potent response is sufficient to significantly reduce scar stiffness, as shown by immediate clinical improvements (e.g., patient showing improved range of motion in 3 days 13 ). But improvements continue long after resolution of inflammation. The long-term response could be initiated by the precipitous drop in tissue stiffness provided by the short-term activity. Collagen deposition and degradation is a dynamic process, even in long-healed scars. 52,53,112 Furthermore, tissue stiffness forms a crucial positive feedback loop with fibrosis; greater stiffness promotes collagen deposition and inhibits degradation, therefore promoting further increases in tissue stiffness. 113 A reduction in stiffness could tip the balance to be less in favor of collagen deposition, enabling long-term remodeling toward normal ECM. Changes in tissue stiffness could also explain the reduction in pruritis, as it has recently been shown that substrate stiffness can regulate mast cell recruitment and activation. 114 A summary of the putative mechanisms involved is depicted in Fig. 4. The importance of other factors discussed previously, such as HSPs, Wnt, and CYR61, and how they may fit into a potential mechanism needs to be addressed by future research.
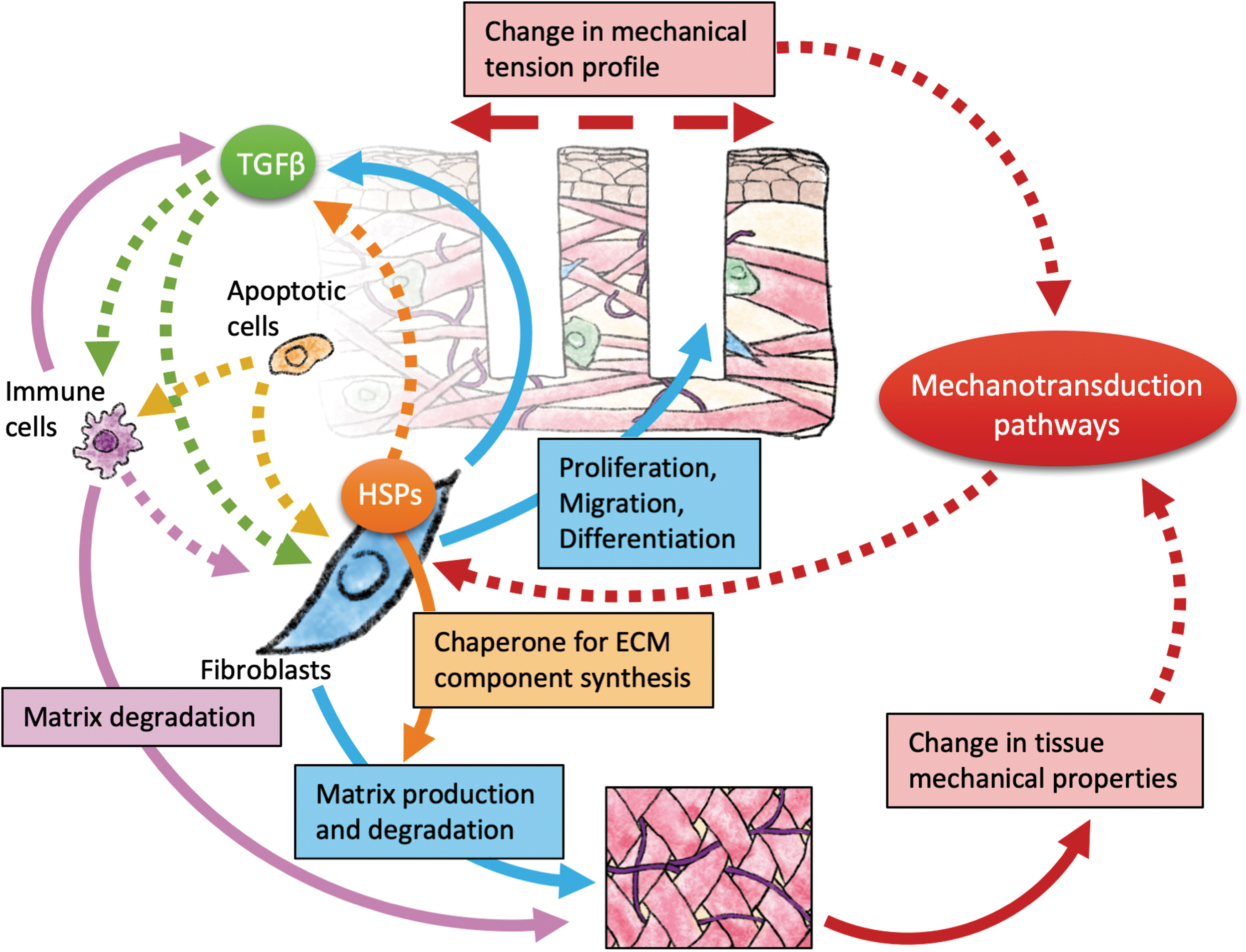
Putative mechanisms involved in fractional resurfacing-induced remodeling. Solid arrows denote direct involvement in specific processes, dotted arrows denote regulatory roles. The TGFβ pathway regulates fibroblast function both directly and indirectly through effects on immune cells. Both fibroblasts and immune cells also produce TGFβ. Paracrine signaling from apoptotic cells stimulates proliferation and differentiation of neighboring cells, and also modulate the inflammatory response. HSPs interact with TGFβ signaling and also serve as chaperones for the production of ECM components. Tissue biomechanics may be altered by both the microinjuries from fractional resurfacing and the ECM remodeling process, resulting in feedback regulation of fibroblast functions through mechanotransduction pathways. ECM, extracellular matrix; HSP, heat shock protein; TGFβ, transforming growth factor-β.
Summary
Fractional resurfacing is effective at correcting a wide range of defective skin qualities, most prominently in photoaging and scarring. Better understanding of the cellular and molecular mechanisms underlying the unique healing response to fractional resurfacing could reveal fundamental information about adult tissue regeneration, lead to improvements in current applications, as well as new therapies in other pathologic conditions.
Take Home Messages
Small wounds can regenerate completely, with no scarring
Clinical fractional resurfacing entails producing arrays of small wounds, by thermal or mechanical means, to induce tissue regeneration
Fractional resurfacing can produce homeostatic corrections in many structural and functional skin defects, particularly in photoaged skin and scars
Ulcer-prone skin is plagued by many similar defects, the potential utility of fractional resurfacing in the chronic wound setting remains to be explored.
Footnotes
Acknowledgments and Funding Sources
J.T. was supported by the 2016 Wound Healing Foundation 3M Fellowship Award. J.T. is partially supported by the Army, Navy, NIH, Air Force, VA and Health Affairs to support the AFIRM II effort, under Award No. W81XWH-13-2-0054. The U.S. Army Medical Research Acquisition Activity, Fort Detrick, Maryland, is the awarding and administering acquisition office. Opinions, interpretations, conclusions, and recommendations are those of the author and are not necessarily endorsed by the Department of Defense. J.T. and C.F. are partially supported by the Military Medicine Technology Transformation Collaborative, Award Number HU0001-17-2-0009. The Uniformed Services University of the Health Sciences (USU), Bethesda, Maryland is the awarding and administering office. The information or content and conclusions do not necessarily represent the official position or policy of, nor should any official endorsement be inferred on the part of, USU, the Department of Defense, or the U.S. Government.
Author Disclosure and Ghostwriting
The authors have no competing financial interests related to this article. The content of this article was expressly written by the authors listed. No ghostwriters were used to write this article.
About the Authors