
Abstract
Objective:
To determine whether multilayer silicone foam dressings can prevent pressure ulcers arising in the sacrum and coccyx of patients with persistent severe diarrhea and/or fragile skin.
Approach:
This randomized, 14-day controlled trial included 600 hospitalized patients with persistent severe diarrhea and/or fragile skin who were at high risk of developing pressure ulcers. All participants were enrolled from three Japanese institutions. Participants meeting all inclusion and exclusion criteria were randomized using the Excel program to receive standard care (control; n = 300) recommended by Japanese guidelines or multilayer silicone foam dressings applied to the sacrum and coccyx (intervention; n = 300).
Results:
Significantly more participants in the control than the intervention group developed pressure ulcers (22 vs. 5, p = 0.001).
Innovation:
The incidence of pressure ulcers remains high in hospitalized patients at high risk of developing pressure ulcers. The present findings might contribute to novel preventive strategies for patients at high risk of developing pressure ulcers.
Conclusion:
Multilayer silicone foam dressings can prevent pressure ulcers of the sacrum and coccyx in patients with persistent severe diarrhea and/or fragile skin.

Introduction
A pressure ulcer is localized damage to the skin and/or underlying soft tissue usually over a bony prominence or related to a medical or other device. 1 The reported prevalence of pressure ulcers developing among inpatients at university hospitals in Japan is 1.58%, 2 compared with 12.3% reported by the International Pressure Ulcer Prevalence Survey. 3 However, severe pressure ulcers defined as full-thickness skin loss account for 43.0% of pressure ulcers that develop in Japanese patients, 2 and this is considerably worse than the previously identified 14%. 4
The high prevalence of pressure ulcers is an important issue that requires attention, particularly because patients who develop them often require long-term hospitalization or have comorbidities such as infection. 5,6 Extended hospitalization imposes a significantly higher cost burden on the national health and social welfare system. 7,8
The Japanese government has implemented various plans for medical fee reimbursement starting from a penalty system that was introduced in 2002 to the pressure ulcer high-risk incentive system in 2006. The latter reimburses 5,000 yen per admission of a high-risk patient to a hospital that requires the full-time participation of nurses specializing in wound, ostomy, and continence care in interdisciplinary teams that manage pressure ulcers. The following are factors that place patients at high risk of developing pressure ulcers: shock, extreme peripheral circulation insufficiency, a need for continuous sedation or analgesics such as narcotics, procedures requiring general anesthesia for ≥6 h, surgery in a specific/unusual position, persistent severe diarrhea, fragile skin, extant pressure ulcers, extreme bony prominences, moist skin, or edema. The high-risk incentive system can be applied to patients with at least one of the above factors.
Clinical Problem Addressed
Pressure ulcers remain prevalent despite the high-risk incentive system. The estimated rate of pressure ulcer occurrence at university hospitals is 0.94%. 2 One study concluded that prophylactic dressings might prevent pressure ulcers, 9 and some guidelines recommend applying polyurethane foam dressings to prevent pressure ulcers arising on bony prominences that are frequently subjected to friction and shear such as the heels and sacrum. 10 Multilayered soft silicone foam dressings can help to prevent sacral and heel pressure ulcers in critically ill patients and aged residents in care facilities. 11,12 However, to apply multilayered soft silicone foam dressings to all patients might be extremely expensive. Therefore, very high-risk patients should be identified.
We reviewed the charts of 3,018 patients who were admitted to the University of Tokyo Hospital between April 1, 2014 and March 31, 2015 and were at high risk of developing pressure ulcers. 13 We found that 48 (1.59%) of these patients developed pressure ulcers at the sacrum (n = 24; 0.80%), coccyx (n = 20; 0.66%), and heels (n = 4; 0.13%). Pressure ulcers at sacral and coccygeal sites were associated with persistent severe diarrhea and fragile skin, respectively. These findings suggested that protecting the skin of these sites in such patients could prevent pressure ulcers.
Therefore, we aimed to clarify whether multilayer silicone foam dressings can prevent sacral and coccygeal pressure ulcers in high-risk patients with persistent severe diarrhea and/or fragile skin. High-risk patients were defined as those with at least one of the following factors: shock, extreme peripheral circulation insufficiency, need for continuous sedation or analgesics such as narcotics, procedures requiring general anesthesia for ≥6 h, surgery in a specific/unusual position, persistent severe diarrhea, fragile skin, extant pressure ulcers, extreme bony prominences, moist skin, and edema.
Materials and Methods
Trial design
This randomized, stratified, open-label trial proceeded at three institutions in Japan. Participants (N = 600) were randomly assigned to intervention or control groups (n = 300 each; 1:1). No important changes were made to the methods after commencement of the trial.
The Ethics Committees at the Graduate School of Medicine and Faculty of Medicine, University of Tokyo, approved the study protocol (no. 11138) as did those at the other participating hospitals. The protocol was registered at the UMIN Clinical Trials Registry (UMIN000024609).
Participant
Hospital inpatients with persistent severe diarrhea and/or fragile skin were eligible for inclusion in the study; those with extant pressure ulcers or were aged <20 years were excluded. The fragile skin was defined as low-birth-weight baby, graft versus host disease, and jaundice in the pressure ulcer high-risk incentive system.
Nurses identified eligible patients soon after admission based on the pressure ulcer high-risk incentive system. Nurses specializing in wound, ostomy, and continence care, who were dedicated full-time to pressure ulcer management, informed all eligible patients about the study. Thereafter, all included patients or their guardians provided written informed consent to participate.
One hundred, 200, and 300 patients between April 2006 and April 2018 were, respectively, enrolled from an acute university hospital in Tokyo, a general hospital in Fukuoka City, and the emergency and critical care medical center of a university hospital in Tokyo.
Intervention
Multilayer silicone foam dressings (Mepilex®Border; Mölnlycke Healthcare, Göteborg, Sweden) were applied to the sacrum and coccyx of the intervention group and monitored daily by partially peeling the dressings to assess the skin and pressure ulcer development. Soiled or dislodged dressings were changed. Mepilex Border is a five-layer, soft silicone, bordered foam dressing that was originally developed to treat wounds.
All participants received standard care during the study period based on the Japanese guidelines. Such care comprised pressure risk screening, skin inspection and care, pressure area care such as repositioning every 2 h, and support surfaces such as alternating air mattresses. All care was provided by registered nurses who were regular employees of the participating hospitals. No dressing was used for the control group.
Outcome
The outcome measure was the incidence of pressure ulcers expressed as the total number of pressure ulcers that developed in the intervention and control groups during the study period.
All participants were followed for 2 weeks after enrollment until the end of the trial or when pressure ulcers developed, or the participant died or was discharged. Baseline data collected for both study groups included age, sex, height, weight, body mass index, causes of hospitalization, high-risk factors based on the pressure ulcer high-risk incentive system, the Braden scale, interface pressure, nutrition management, serum albumin level, urination, and defecation. Data collected from the two study groups comprised findings of daily assessments of sacral and coccygeal skin for pressure ulcer development. Pressure ulcers that developed during the study were staged according to the European Pressure Ulcer Advisory Panel (EPUAP), the National Pressure Ulcer Advisory Panel (NPUAP), and Pan Pacific Pressure Injury Alliance (PPPIA) guidelines. 1 All pressure ulcers were confirmed by nurses specializing in wound, ostomy, and continence care.
Sample size
A survey of the clinical charts of the 3,018 inpatients previously mentioned found that the numbers of the hospital inpatients with persistent severe diarrhea and/or fragile skin and of those who developed sacral and/or coccygeal pressure ulcer were 114 and 11 (9.6%), respectively. 13 The high risk in the survey of the clinical charts 13 was defined in the same way as that used in this research. Based on an expected incidence of pressure ulcers of 9.6% in the control group, we calculated that we would need a sample size of 600 participants (n = 300 per group) to achieve an 80% power to detect a significant difference between the intervention and control groups, corresponding to the predicted effect of a 4.8% reduction with a two-sided alpha of 5%. The method for comparing independent proportions was used for calculating sample size. 14
Randomization
Participants meeting all inclusion and exclusion criteria were randomized using the Excel program to the intervention or control group in a 1:1 ratio. An investigator who was blinded to the identity of the participants used computer software (the Excel program) to generate a series of random numbers. Participants were allocated to either the intervention or the control group at each participating institution based on these series of random numbers by nurses specializing in wound, ostomy, and continence care.
Blinding
None of the participants, care providers, and outcome adjudicators was blinded to the interventions after assignment.
Statistical method
Participant characteristics are presented as frequencies and ratios (%) for categorical data and means (standard deviations) for continuous data. Statistical analyses were based on “intention to treat.” Statistical differences of the parameters between the two groups (the intervention group vs. the control group) were analyzed using the t-test, χ 2 test, or Fisher's exact test. The effects of intervention were determined by comparing the incidence of pressure ulcers between the two groups using Fisher exact and log-rank tests. Median survival is presented for each group with 95% confidence interval (CI), and treatment effects are shown as hazard ratios (HR) with 95% Wald CI estimated from a Cox proportional hazard model. Absolute risk reduction, relative risk reduction, and the number needed to treat were calculated. Data were statistically analyzed using IBM SPSS Statistics version 22 (IBM Corporation, Armonk, NY). The level of statistical significance was set at p = 0.05.
Results
Figure 1 shows the flow of patient enrollment, allocation, follow-up, and analysis throughout the trial according to the CONSORT protocol. All participants were followed up starting from 2 weeks after enrollment until the end of the trial or when pressure ulcers developed, or when the patient died or was discharged.
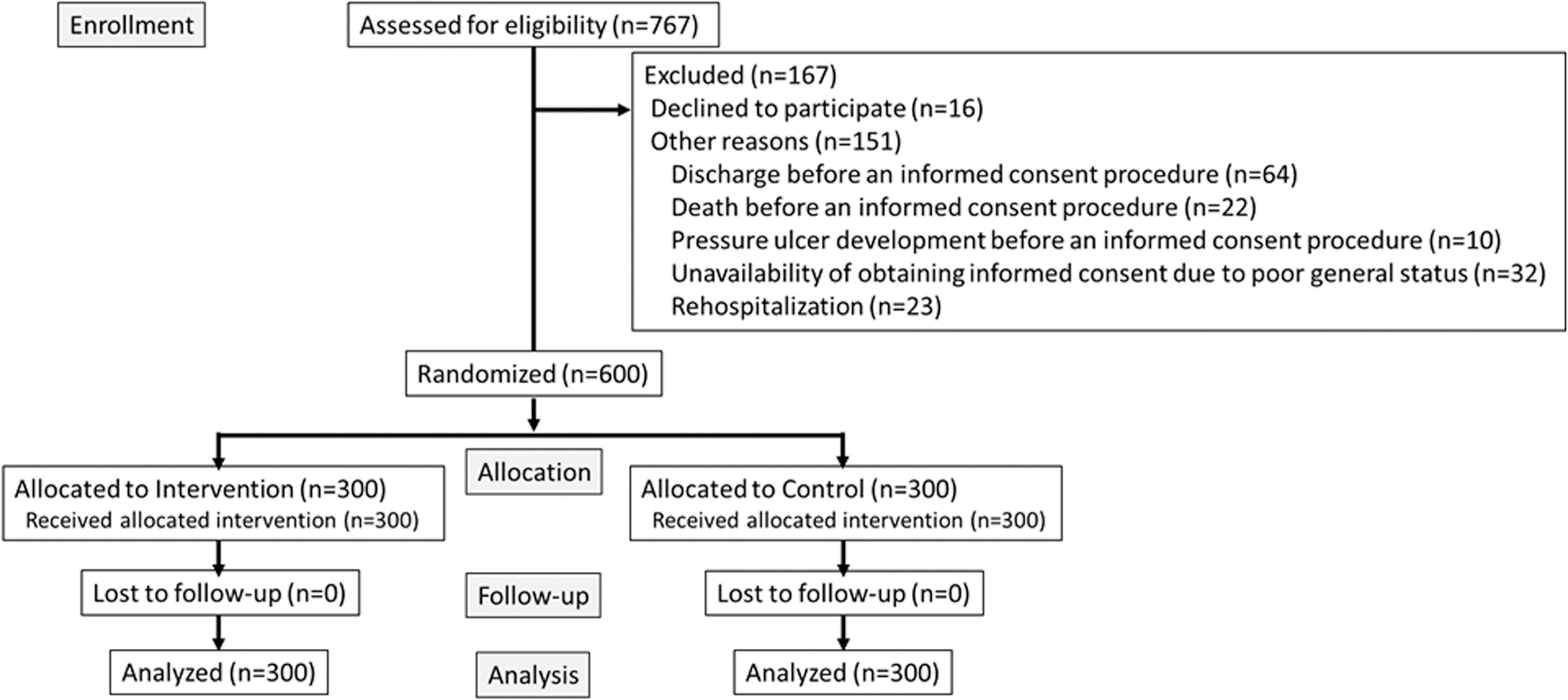
CONSORT diagram of participant flow through the study.
Baseline characteristics of the participants seemed balanced between the groups, although the score of friction and shear of the intervention group was significantly lower than one of the control group (Table 1). None of the participants was lost to follow-up in the intervention group; thus, data from all participants were included in the intention-to-treat analysis. Table 2 shows a statistically significant difference in the incidence of pressure ulcers that developed in the groups during the 2-week study period. The absolute risk reduction between the intervention and control group was 5.6%, and the relative risk reduction was 76.7%, which yielded a number needed to treat 18 (17.9) to prevent the development of one pressure ulcer in participants using the dressings.
Baseline demographics of participants
Data are shown as n (%) or as mean ± standard deviation.
n = 267.
n = 257.
Based on the pressure ulcer high-risk incentive system initiated by the Japanese government.
n = 299.
Missing data.
t-test.
χ 2 -test.
Fisher's exact test.
Incidence of pressure ulcers
Values are shown as n (%). Fisher's exact test.
The distribution and severity of pressure ulcers differed between the groups (Table 3). Five participants in the intervention group developed category/stage II sacral pressure ulcers.
Characteristics of pressure ulcers
Data are shown as n (%).
European Pressure Ulcer Advisory Panel (EPUAP), National Pressure Ulcer Advisory Panel (NPUAP), and Pan Pacific Pressure Injury Alliance (PPPIA), 2014.
Based on the pressure ulcer high-risk incentive system initiated by the Japanese government.
Figure 2 shows that the mean amounts of time required for pressure ulcers to develop in the intervention and control groups were 13.9 ± 0.0 (95% CI: 13.8–14.0) and 13.7 ± 0.1 (95% CI: 13.5–13.9) days, respectively (HR: 0.22; 95% CI: 0.08–0.58; p = 0.002). The incidence of pressure ulcers started to diverge in the control compared with the intervention group around day 3, and the rate at which these ulcers developed in the control group increased up to day 13 of the study.
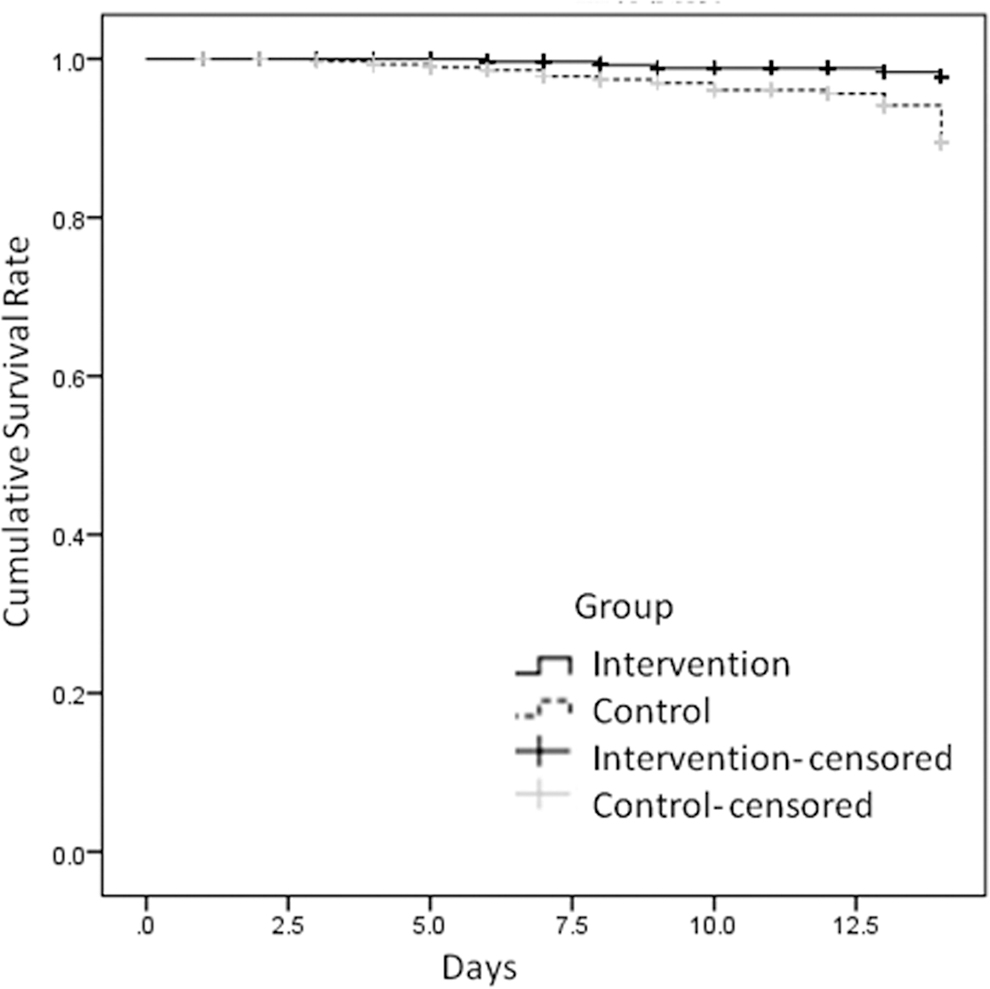
Kaplan–Meier survival analysis.
Harm
Adverse events comprising epidermal desquamation and itching paresthesia developed in one patient each. Pressure ulcers were not considered to be associated with wound dressings in these participants.
Discussion
The present study is the first to show that multilayer silicone foam dressings can prevent pressure ulcers from developing on the sacral and the coccygeal skin of high-risk patients who have persistent severe diarrhea and/or fragile skin. These dressings might serve to avoid skin damage caused by severe diarrhea and protect fragile skin from moisture and shear.
The demographic features of the groups were very similar (Table 1). Regarding the Braden scale, scores of friction and shear in the intervention group were significantly lower than in the control group. This result indicates that the intervention group had a significantly higher risk of pressure ulcers than the control group. Nevertheless, the incidence of pressure ulcers was significantly lower in the intervention group than in the control group. This could be because the intervention was effective enough to counteract the effects of friction and shear scores demonstrated by the Braden scale. Therefore, we determined that it was inappropriate to use friction and shear scores in the Braden scale as adjustment factors in multivariate analysis. Ultimately, multivariate analysis was not performed because there were no other factors for which a significant difference was noted between the two groups. Thus, the risk profiles of all patients in the two groups supported the validity of the results of the comparison of the clinical outcomes of the interventions. All of the included patients had been recently admitted to the participating hospitals, which is a grave aspect of the trial. Prophylactic dressings should be applied as soon as possible, because the close relationship between exposure to pressure and shear forces affects tissue tolerance in the development of pressure ulcers. 15 –17 All participants were followed from 2 weeks after enrollment until the end of the trial or when pressure ulcers developed, or the participant died or was discharged. That is, no participants were withdrawn during the study. The tendency was similar in a previous trial of high-risk, aged care residents in which only one withdrew. 12 Preventive care using multilayer silicone foam dressings should be easy for patients and health care providers to accept. Our study was originally powered to detect a 4.8% effect size between the groups and was calculated based on the results of a chart review in an acute university hospital in Tokyo. 13 The recruitment of our participants from an acute university hospital, a general hospital, and the emergency and critical care medical center of a university hospital had the effect of a large reduction (5.6%) in the incidence of pressure ulcers for the intervention, compared with the control group. Considering that the patients from the emergency and critical care medical center might have been at higher risk for pressure ulcers, our findings indicate that such ulcers were preventable at all three participating institutions. Nonetheless, our findings should be extrapolated with care. This trial proceeded at institutions that satisfied all the requirements of the pressure ulcer high-risk incentive system; that is, nurses specialized in wound, ostomy, and continence care managed preventive care for pressure ulcers, and interface pressure was appropriately controlled (Table 1). Such control significantly contributed to the present results.
Multilayer dressings combined with Safetac (Mölnlycke Healthcare) adhesive technology play a vital role in reducing shear and friction forces at the point of application and providing optimal microclimate management. Moreover, these dressings help to avoid moisture associated with diarrhea, although sacral area can easily become contaminated with urine and stool. Regarding pressure redistribution, dressings with adequate thickness will distribute forces over a larger area, thus reducing the magnitude of forces applied to the skin. 18 The texture and type of material used to construct the outer layer of a dressing will determine whether friction is increased or reduced, that is, a slippery surface will reduce friction. This is important because friction is the source of shear, and dressings translate shear force to the skin outside the area of concern. The interface of multiple layers within the dressing helps to absorb shear. Buckling at the edge of the adhesive border of dressings also absorbs shear. Computational modeling studies have shown that multilayered dressings are remarkably effective in reducing exposure to sustained soft tissue deformations and to stress. 17,19 Furthermore, this type of dressing has high vapor permeability, and maintaining a suitable microclimate could help protect fragile skin. Skin damage caused by fecal contamination is important to avoid pressure ulcers arising in patients with severe diarrhea. Backing film can protect the skin from fecal contamination, maceration, and infection. These functions might be causally related to the prevention of pressure ulcers.
The introduction of a cost-effective, national policy approach to the clinical setting carries weight. An annual savings of AUD 34.8 million has been achieved by implementing a national pressure ulcer prevention initiative to apply prophylactic multilayer foam dressings with Safetac to high-risk populations in acute hospitals in Australia. 20 Our strategy of focusing only on high-risk patients with persistent severe diarrhea and/or fragile skin might confer an even higher cost/benefit.
The present study has some limitations. First, the main cause of the category/stage II pressure ulcers in the sacral regions of five participants in the intervention group remains unclear. Furthermore, the number of participants was too small to consider potentially involved factors. Second, the difference of mean amounts of time required for pressure ulcers to develop in both groups might be of no clinical significance, and the long-term effect remains unknown. A follow-up of 2 weeks was decided considering the feasibility of the study. The participants remained in the participating institutions for only a few weeks; thus, follow-up for over 2 weeks would be challenging. However, we believe that the ability of multilayer foam dressings with Safetac to prevent ulcers persists beyond 2 weeks, because the difference in the incidences of pressure ulcers between the intervention and control groups widened over time. Third, we could not change the definition for “fragility” because, although it may be ambiguous, it is the definition used by health insurance systems. Fourth, we designed this study to involve the χ 2 test since it would be considered complete after 2 weeks had passed from the start of the survey, when any pressure ulcers developed, or at the time of death or discharge of the research participants. Although this method was appropriate from the clinical perspective of preventing the development of pressure ulcers during hospitalization, it might have been more appropriate, for the purpose of validating the preventative effects of a dressing on pressure ulcers, to design the study in a way to consider as dropouts those who had passed away, or been discharged from the hospital within 2 weeks from the start of the survey. Finally, it was not possible to blind data collectors to the nature of the treatment.
We concluded that multilayer silicone foam dressings can prevent pressure ulcers from developing in patients who have persistent severe diarrhea and/or fragile skin. This finding might contribute to a national strategy of pressure ulcer prevention among high-risk patients.
Innovation
A multilayer silicone foam dressing has recently been recommended to prevent pressure ulcers in adults, but which patients would derive the most benefit remained unclear. Here, we focused on patients with severe diarrhea and/or fragile skin, who were selected based on our previous experience in a practice setting. A policy of applying multilayer silicone form dressings should prevent pressure ulcers developing in high-risk patients and reduce the burden of medical costs in Japan.
Key Findings
More pressure ulcers developed in the control than the intervention group (22 (7.3%) vs. 5 (1.7%); p = 0.001).
Absolute and relative risk reductions between the intervention and control groups were 5.6% and 76.7%, which indicated that 18 patients need to be treated using the dressings to prevent the development of one pressure ulcer.
The incidence of pressure ulcers in the control and intervention groups began to diverge around day 3, and increased in the control group until day 13 of the study.
Footnotes
Acknowledgments and Funding Sources
This study was funded by research grants from the Japanese Society of Wound, Ostomy, and Continence Management.
Author Disclosure and Ghostwriting
The authors report no conflicts of interest in this work. The content of this article was expressly written by the authors listed. No ghostwriters were used to write this article.
About the Authors