
Abstract
Objective:
Chronic wounds are long-term nonhealing wounds that are refractory to treatment. These wounds can present elevated protease levels, leading to rapid degradation of native and exogenously added growth factors. This work focused on developing a protease-resistant growth factor formulation for treatment of chronic wounds presented with high protease activity.
Approach:
This study developed protease-resistant growth factor formulations comprising elastin-like peptides (ELPs) fused with a known protease inhibitor peptide or growth factor. The ELP component of the fusion proteins allows assembly of heterogeneous nanoparticles (NPs) putting the inhibitor in close proximity to the growth factor to be protected.
Results:
We show successful preservation of growth factor activity in high human neutrophil elastase (HNE) environment and in human chronic wound fluid derived from patients. We further show that these NPs result in enhanced collagen remodeling and resolution of inflammation in a full thickness wound supplemented with HNE in genetically diabetic mice.
Innovation:
Development of heterogeneous NPs that put the protease inhibitor in close proximity of the growth factor. Moreover, the modular nature of the NPs allows for protection of multiple growth factors by the same inhibitor without changing the amino acid sequence of the growth factor.
Conclusion:
Our results indicate that the developed NPs hold tremendous promise in chronic wound healing therapy and may further help the translation of growth factor therapies to clinic. The customizable template for the NP design allows for multifaceted use across several fields in research and medicine.
Introduction
The public health impact of chronic wounds is staggering. There are ∼2.5 million pressure ulcers per year in the United States with greatest impact on the elderly and spinal cord injured persons. 1 Up to one-third of the 12 million individuals with diabetes mellitus in the United States develop a foot ulcer. 2 These wounds are refractory to treatment and frequently are complicated by infections, which may lead to amputation.
Among the many approaches available, one approach to chronic wound treatment is the use of bioactive proteins and factors that aim to correct irregular and dysfunctional cellular pathways present in chronic wounds. 3 –8 Platelet-derived growth factor (PDGF) that induces proliferation and migration in fibroblasts 9 is clinically approved for the treatment of chronic wounds (becaplermin; Regranex gel). 10 However, the clinical achievements of exogenous PDGF therapy are rather modest 11 and require the protein to be applied repeatedly in pharmacologic concentrations during a considerable length of time. 12 Although delivery systems have been developed that show promising results in animal models, their translation in clinics remains limited.
The highly inflammatory environment present in chronic wounds is one of the critical barriers to successful therapy of chronic wounds. Chronic wounds exhibit a prolonged inflammation coupled with high levels of proteases. 13 This includes matrix metalloproteinases (MMPs) and serine proteases derived from neutrophils such as human neutrophil elastase (HNE), proteinase-3, cathepsin-G, and urokinase plasminogen activator. 14 This is further documented by several clinical studies that have reported high levels of proteases in chronic wounds. 15
Elevated levels of elastases and MMPs have been detected in wound fluid from chronic wounds compared with acute wounds. 13 High levels of MMP-9 were detected in patients suffering from diabetic foot ulcers (14-fold), 16 pressure ulcers (10–25-fold), 17 and venous leg ulcers (7-fold). 18 Although proteases play an important role in matrix remodeling and angiogenesis in normal wound healing, elevated levels of proteases lead to impaired wound healing. 19 Recent data have clearly indicated a direct relationship between high protease activity and nonhealing chronic wounds. 20,21
Among all the proteases reported in chronic wounds, the presence and activities of MMPs have received the most attention. However, recent data have shown that other neutrophil-derived serine proteases such as HNE also affect healing of chronic wounds. 20 The presence of neutrophil-derived proteases particularly HNE and proteinase-3 enhance inflammation by recruiting and activating neutrophils. 22 Sustained high levels of proteases lead to degradation of extracellular components (fibronectin, collagen, etc.), growth factors, and their receptors thereby delaying or blocking wound healing. 19
Indeed, the ability of chronic wound fluids to degrade peptide growth factors is associated with increased elastase activity and diminished levels of protease inhibitors. 23,24 Therefore, in the highly proteolytic environments of chronic wounds, advanced wound healing modalities such as growth factor supplementation, stem cells, or other advanced protein-based products may not work because of rapid degradation induced by these potent proteases. Consequently, it is reasonable to believe that a successful growth factor therapy must include protection of the growth factor from proteolytic degradation in chronic wounds.
Our laboratory has developed a novel nanoparticulate delivery system based on elastin-like peptides (ELPs) for delivery of bioactive proteins to the wounds. 25 These comprise chimeric fusion proteins of the bioactive protein to be delivered and ELPs.
ELPs are biodegradable, nonimmunogenic polymers composed of tandemly repeated blocks of (Val-Pro-Gly-X-Gly)N, a sequence motif derived from the hydrophobic domain of tropoelastin, 26 a soluble precursor form of elastin. An interesting property of ELPs is their ability to undergo phase transition at physiological temperatures. At temperatures below their inverse transition temperature, also known as the lower critical solution temperature, they are soluble in aqueous solutions. However, as the temperature is raised above the transition temperature, they undergo an entropically driven, temperature-induced contraction and self-assembly, rendering them insoluble.
This property enables recombinant ELPs to be expressed in bacteria and rapidly purified to high homogeneity using inverse temperature cycling (ITC). 27 Our laboratory has shown that chimeric fusion proteins comprising recombinant growth factor and ELPs retain the bioactivity of the growth factor and the characteristic phase transition property of ELPs. 28 –30 The chimeric peptides self-assemble into nanoparticles (NPs), which, when applied to full thickness chronic wounds in diabetic mice enhanced wound healing.
In this study, we describe a novel nanoparticulate protease-resistant growth factor formulation for the treatment of chronic wounds. The NPs consist of 2 chimeric fusion proteins comprising ELPs and either PDGF or a HNE inhibiting peptide. The 2 chimeric fusion proteins result in the formation of heterogeneous NPs owing to the unique phase transitioning properties of ELPs.
In addition to the PDGF chimeric fusion protein, we also developed several other potentially useful growth factor formulations for use in chronic wound treatment and which might also be subject to proteases degradation, including keratinocyte growth factor (KGF), epidermal growth factor (EGF), and vascular endothelial growth factor (VEGF), to test the efficiency of the HNE inhibitor on several growth factors intrinsic to the wound healing process.
These NPs extended the half-life of the growth factor significantly both in the presence of purified HNE and in human chronic wound fluid derived from patients. In addition, we further show that these NPs result in enhanced collagen remodeling and resolution of inflammation in a full thickness wound supplemented with HNE in genetically diabetic mice. Our results indicate that the developed NPs hold tremendous promise in chronic wound healing therapy and may further help in the translation of growth factor chronic wound healing therapies to clinic.
Clinical Problem Addressed
Certain chronic wounds present with high protease environments limiting the efficacy of growth factors or biologics because of protease-mediated degradation. In this study we describe novel NPs that protect growth factors from protease-mediated degradation thereby improving their efficacy in high protease environments.
Materials and Methods
Synthesis of expression plasmids containing genes encoding PMPD2-ELP and PDGF-ELP
Genes encoding human recombinant PDGF-BB (rPDGF-BB) (accession no. NP_002599, amino acids 82–190) and the HNE inhibitory PMPD2 peptide (EEKCTPGQVKQQDCNTCTCTPTGVWGCTLMGCQPA) 31 were individually cloned in frame with the gene encoding ELP ([(VPGVG)2-VPGLG-(VPGVG)2]10-DYKDDDDK) at the N-terminus within the PUC19 plasmid. This new fusion DNA fragment (now coding either PMPD2-ELP or PDGF-ELP) was then excised using PflmI and BglI from the PUC19 vector and cloned into a modified pET25B+ vector containing an Sfi1 site as described previously. 29 This same process was repeated for EGF, KGF, and VEGF. All gene sequences were confirmed by sequencing after inserting them in the expression plasmid.
Expression and purification of fusion proteins
The pET25B+ vector containing the fusion proteins was expressed in BLR-D cells. Bacteria were first inoculated in 75 mL terrific broth (TB; 4 mL glycerol, 12.6 g potassium dibasic, 2.4 g potassium monobasic, 24 g tryptone,12 g yeast, all sourced from Thermofisher, in 1 L deionized [DI] water) medium overnight. The next day the 75 mL culture was transferred to 1 L of TB medium and the cells were cultured overnight. Bacterial cells were harvested the next day using a centrifuge (3,000 g, 10 min).
The cells were suspended in phosphate-buffered saline (PBS) and lysed by sonication on ice (12 min total with cycles of 30 s on and 30 s off). After pelleting the cell debris the ELP fusion proteins were purified using ITC as described previously. 25 The transition of PDGF-ELP and PMPD2-ELP was induced with the addition of 3 M NaCl and 1 M NaCl and warming to 42°C. Three rounds of cycling ensured protein purity, which was further tested by western blots and total protein gels. After inverse cycling the protein was resuspended in the DI water and dialyzed overnight against DI water to get rid of contaminated salts. After dialysis the proteins were lyophilized and stored at room temperature till further use.
Chronic wound fluid collection and quantification
Wound fluid from chronic wound patients was collected at Kent Hospital under a protocol approved by the Care New England—Kent Hospital Institutional Review Board. The wound fluid was collected using filter papers wetted with PBS as described previously 18 and shipped to Tampa on dry ice for analysis. Filter papers containing the wound fluid were stored at −80°C till further use.
For analysis and quantification of HNE activity in the wound fluid, the frozen filter paper samples containing the wound fluid was immersed in 150 μL of assay buffer (100 mM (4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid [HEPES]), 500 mM NaCl, 0.05% Tween-20) to elute proteins from the wound fluid. The solution containing the eluted protein was then assayed for HNE activity using colorimetric drug discovery kits of HNE (catalog no. BML-AK497-0001; Enzo LifeSciences) as per the manufacturer's recommendations. This kit contains highly specific colorimetric substrate of HNE (MeOSuc-AAPV-pNA). The hydrolysis of the substrate increases the absorbance at 405 nm.
A plot of the increased absorbance with time was generated where the slope of the curve is directly related to the enzyme activity. Similar curves were generated with standard solutions containing known concentrations of purified HNE and slopes were calculated. Using these slopes, the activity of HNE in the wound fluid was then estimated. The wound fluid was then stored at −80°C for further use.
Growth factor degradation studies
PDGF-ELP (1 mg/mL in PBS, total volume 50 μL) was incubated with HNE (concentration of 250 μU/μL) at 37°C. At the indicated time points, 6 μL of the sample was collected and stored at −20°C till further use. These samples were then tested by western blots using an antibody for PDGF (Peprotech 500-P45, 0.2 μg/mL dilution used for blotting) to track for degradation of PDGF over time.
For assessing the activity of the NP formulations, a 1:2 by weight mixture of growth factor-ELP and PMPD2-ELP in PBS was created. HNE (250 μU/μL) was then added to these NPs (total volume = 50 μL) and the mixture was incubated at 37°C. At the indicated times, 6 μL of samples were collected. Growth factor degradation was then assessed by western blots using antibodies specific to the corresponding growth factor: PDGF (Peprotech 500-P45, 0.2 μg/mL dilution used for blotting), EGF (Peprotech, 500-P45, 1 μg/mL dilution used for blotting), KGF (Peprotech 500-P19, 1 μg/mL dilution was used for blotting), and VEGF (Novus NBP2-596, dilution 2 μg/mL used for western blotting).
For assessing the preservation of growth factor in wound fluid, the stored reconstituted wound fluid was used instead of PBS as described previously. The samples were then tested (along with a positive control) through western blots to observe the growth factor degradation over time and the relative percentage remaining of the protected growth factor versus the unprotected growth factor was compared.
The western blot membranes were exposed and the images collected for quantitative analysis by Fluorcheme. ImageJ was used to compare the pixel density for the protected and unprotected samples, with thicker darker pixelated lines indicating higher concentration of remaining PDGF. The resulting differences were calculated and reported as percentages remaining and the percentage of increased recovery.
Animals
Genetically diabetic female B6.BKS(D)-Leprdb /J mice were obtained from the Jackson Laboratory (Bar Harbor, ME). A total of 30 mice were used for all the treatment groups (HNE [n = 7], HNE+PMPD2-ELP [2 mg/mL, n = 7], HNE+ELP [2 mg/mL, n = 4], HNE+rPDGF [1 mg/mL, n = 4], HNE+PMPD2-ELP+PDGF-ELP [2 and 1 mg/mL respectively, n = 4], and PDGF-ELP [1 mg/mL, n = 4]). All mice were between 7 and 9 weeks old at the time of wounding. Each mouse was housed individually.
The animals were cared for in accordance with the guidelines set forth by the Committee on Laboratory Resources, National Institutes of Health, and the research integrity and compliance institutional animal care and use committee of the University of South Florida. All animals had free access to food and water, both before and after the operation.
Surgical procedures for wounding
The diabetic mice were anesthetized using 2–2.5% vaporized inhaled isoflurane (Iso Flo; Abbott Laboratories, North Chicago, IL). Under sterile conditions, the dorsal area was totally depilated and a single full-thickness excisional square wound (1 × 1 cm2) was created on the upper back of each mouse using a pair of sharp scissors. About 100 μL of fibrin gel supplemented with HNE (250 μU/μL) was then applied immediately after wounding for a week (2 treatments/week). After this week of HNE supplementation, the test groups were either treated with HNE, HNE+ELP (2 mg/mL), HNE+rPDGF (1 mg/mL), HNE+PMPD2-ELP+PDGF-ELP (2 and 1 mg/mL), PDGF-ELP (2 mg/mL), or HNE+PMPD2-ELP (2 mg/mL) suspended in a fibrin gel for 2 weeks (2 treatments/week).
The wounds were dressed with a 2.5 × 2.5 cm piece of Tegaderm™ (3M Health Care, St Paul, MN). It should be noted that rPDGF group was treated 3 times a week to ensure adequate PDGF was applied, similar to previous PDGF studies.
Preparation of fibrin gels
Fibrin gel was prepared on the wound of the mice by mixing 2 fractions:1 fraction containing fibrinogen (6.25 mg/mL; Sigma, St Louis, MO), HNE, ELP proteins, and the other containing thrombin (12.5 U/mL; Sigma), CaCl2 (12.5 mM; Sigma) in 1 × Tris-buffered saline. After wounding the mice, 80 μL of the warm fibrinogen fraction containing the particles was mixed with 20 μL of the thrombin fraction in a tube and immediately applied to the wound topically. After the mixture was gelled (in <2 min), the wounds were covered with semipermeable polymer-based bandages (e.g., Tegaderm).
Histological evaluation of tissues
On the 21st day after wounding, the mice were killed by CO2, with cervical dislocation used after to ensure subject death. The wound sites were collected and bisected, followed by preservation in either formalin or 4% paraformaldehyde. Those samples preserved in 4% paraformaldehyde were then transferred to a 15% and 30% solution for 12–24 h each, before being preserved in optimal cutting temperature compound at −20°C. Tissue sections were then cut and mounted on slides.
Frozen sections were used to stain for CD45. Samples were first blocked in goat serum for 1 h. Then the sections were covered with primary CD45 antibody (1:50 in goat serum; Novus Biologicals) for 1 h. Sections were washed with PBS (5 min × 3) and Alexa Fluor 594-conjugated secondary antibody was used for detecting the primary antibody (1/200 dilution in goat serum, 1 h at room temperature; Invitrogen). The samples were then washed with PBS (5 min × 3) and a 4′,6-diamidino-2-phenylindole (DAPI) containing mounting medium (ProLong Diamond Antifade Mountant, P36966; Invitrogen) was used to mount the sections.
CD45-positive inflammatory cells were quantified by conducting inflammatory cell counts on 3 random microscopic fields of the wound site per each sample (n = 22). These inflammatory cell counts were then normalized to the control (those samples only treated with HNE, no NP treatment) for ease of comparison between groups, with the group's value normed to one in figures.
The formalin samples were stained with hematoxylin and eosin. For wound gap/ reepithelialization analysis, the Freehand tool in ImageJ was used to measure the distance of the sample (n = 30) wound gap on images taken containing the whole of the wound site.
The formalin samples were also stained with Mason's trichrome stain. ImageJ was used to quantify the matured collagen present at wound site by selecting and isolating for the blue of the stained collagen in the trichrome stain in a representative image of each of the samples. Each of these images encompassed the whole of the wound site, with ImageJ calculating how much of the image containing the correct blue wavelength of the collagen, with this being compared with the area of whole image to provide a percentage.
Statistical analysis
The statistical package used was the Excel Analysis toolpack, with which we conducted analysis of variance (ANOVA) and p-analysis to establish statistical significance.
Results
Rapid degradation of growth factor in human chronic wound fluid
When the collected human chronic wound fluid was incubated with PDGF, a clear trend of potent degradation was seen in the residual PDGF recovered at the various time points leading up to 24 h. Some samples showed complete degradation of the growth factor in <2 h, with most samples showing significant degradation overall (Fig. 1A, B).

Rapid degradation of the growth factor in chronic wound fluid.
Elevated protease activity in chronic wound fluids correlates to rapid growth factor degradation
Several studies have shown elevated HNE activity in chronic wounds, with these high levels being associated with increased probability of nonhealing chronic wounds. 20 To test whether HNE was responsible for the PDGF degradation seen in the chronic wound fluid, we performed a substrate-based assay to check HNE levels in human chronic wound fluid. Indeed, we found that 7 of 11 patients showed elevated HNE activity. Three patients had HNE levels associated with 90% probability of a wound being nonhealing (227 μU/μL) and 6 of the 11 patients had levels associated with 65% chance of a wound being nonhealing. 20
Specifically it was noted that those samples with elevated levels of HNE seemed to correlate with those samples that most potently degraded the growth factor (Fig. 1C).
Creation of HNE inhibiting fusion protein PMPD2-ELP
Our results indicate that for successful application of growth factor therapy in chronic wounds with high protease levels, the growth factor needs to be protected from protease-mediated degradation. To that end, we developed a fusion protein comprising an ELP and a previously described potent HNE inhibiting peptide, PMPD2. 31 We were successfully able to express the PMPD2-ELP protein in Escherichia coli and purify it (Fig. 2A, B).
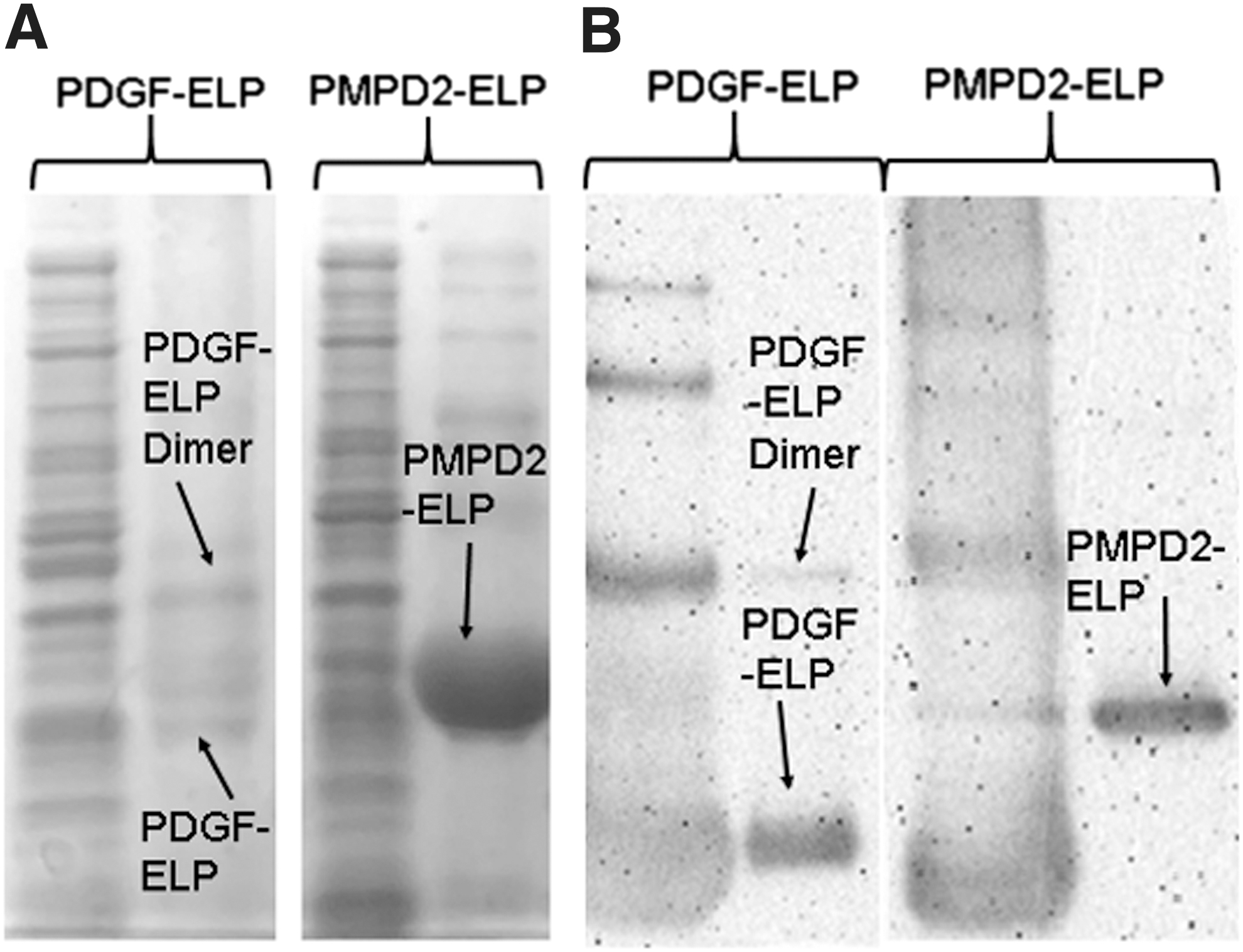
Expression and purification of chimeric fusion peptides. PDGF and PMPD2 were cloned in front of the elastin-like peptide L10-flag, in the cloning vector PUC19 using PflMI and BglI sites.
After successful purification, PMPD2-ELP was incubated with HNE to determine if the new molecule would degrade in the presence of the protease (compared with a similarly made molecule PDGF-ELP). Our results confirm that the PMPD2-ELP does not significantly degrade at HNE levels that degraded PDGF-ELP (Fig. 3A). We tested the inhibitory property of PMPD2-ELP toward HNE using a substrate-based kinetic assay (Fig. 3B). Indeed, PMPD2-ELP blocked HNE at concentrations of 0.5, 1, and 2 mg/mL. In addition, ELP alone did not inhibit HNE activity suggesting that the PMPD2 present in the fusion protein was responsible for the inhibition.

PMPD2-ELP inhibits recombinant HNE.
Heterogeneous NPs formed from PMPD2-ELP and GF-ELP protect growth factors from HNE-mediated degradation
The fused ELP sequences allowed us to create heterogeneous NPs comprising PMPD2-ELP and PDGF-ELP (Fig. 4A). These NPs protected PDGF from HNE-mediated degradation in buffered solutions containing HNE (250 μU/μL) compared with homogeneous NPs comprising the growth factors alone. Heterogeneous NPs containing PDGF-ELP, EGF-ELP, VEGF-ELP or KGF-ELP, and PMPD2-ELP all protected the respective growth factor from HNE-mediated degradation (Fig. 4B–E).

Heterogeneous NP protects growth factors from protease-mediated degradation.
We further tested the ability of PMPD2-ELP in protecting PDGF-ELP in patient chronic wound fluid. The heterogeneous NPs were incubated in the wound fluids for various times and samples were collected. The remaining PDGF was quantified using western blots. The results of the quantified western blots show that on average PMPD2-ELP preserved between 20 and 60% more growth factor, with the most prominent improvements being in at the HNE levels of 60–250 μU/μL (Fig. 4F, G).
PMPD2-ELP significantly reduces inflammation in vivo
Next, we tested the efficacy of the heterogeneous NP (PMPD2-ELP+PDGF-ELP) and its individual components (to act as controls, along with rPDGF), in vivo using a modified animal model of chronic wounds. The most commonly used animal model for testing the efficacy of wound healing products in vivo is the LEPR knockout diabetic mouse. However, this model does not exhibit high levels of HNE found in chronic wounds. So, we modified this model by applying HNE immediately after wounding and waiting for 7 days before treatment. HNE induced sustained inflammation for the entire length of the study.
The groups treated with HNE and HNE+PDGF-ELP showed large populations of neutrophils (Fig. 5A), above, even with, or directly below the epidermis level within and surrounding the wound, suggesting significant inflammation. PMPD2-ELP significantly reduced inflammation, whereas heterogeneous NP, ELP, and rPDGF showed limited reduction in inflammation (Fig. 5A).
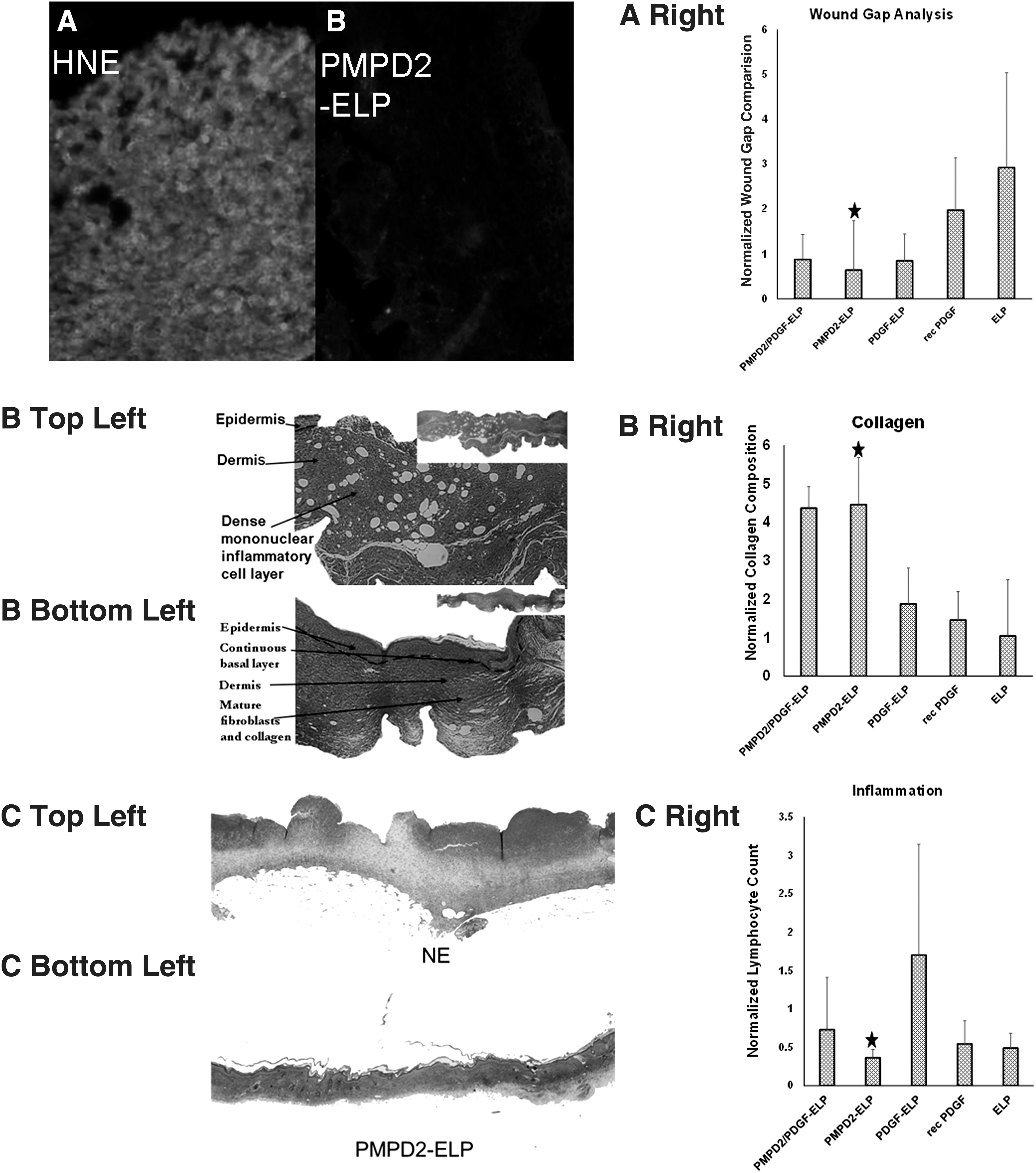
PMPD2-ELP reduced inflammation, improved collagen, and reduced wound gap. Full thickness wounds were created on the back of genetically diabetic mice. The mice were then treated with fibrin gel containing HNE, fibrin gel containing HNE+PMPD2-ELP, fibrin gel containing HNE+PMPD2-ELP+PDGF-ELP, fibrin gel containing HNE+PDGF-ELP, fibrin gel containing HNE+ELP, or fibrin gel containing HNE+recombinant PDGF.
PMPD2-ELP improves healing of full thickness wounds and collagen deposition
Next, we quantified wound closure resulting from the treatment of the various groups using ImageJ. The HNE group presented with the largest wound gap, followed by the HNE+ELP and HNE+rPDGF control group. Although HNE+PDGF-ELP and HNE+PMPD2-ELP+PDGF-ELP showed some improvement over the HNE control group, HNE+PMPD2-ELP group had the lowest wound gap length, with 75% of the sample having little or no gap between the basal layers (Fig. 5B).
We also quantified collagen deposition using a Mason's trichrome stain and quantified the “blueness” using ImageJ. The HNE+PMPD2-ELP and HNE+PMPD2-ELP+PDGF-ELP had the highest level of collagen deposition, followed by HNE-PDGF-ELP. Of interest, HNE+PDGF-ELP and HNE+rPDGF groups has similar collagen levels as that of HNE, possibly because of PDGF being degraded by HNE before the potential positive benefits of the growth factor could take effect (Fig. 5C).
Discussion
Chronic wounds are often associated with high protease activity that leads to degradation of biologics that are beneficial for healing thereby reducing their clinical efficacy. 32 In this study, we describe novel protease-resistant nanoparticulate growth factor formulations that protect the growth factor in the harsh chronic wound environment. The NPs consist of 2 ELP-based fusion proteins. These were recombinant growth factors fused with ELP and a protease inhibitor peptide (PMPD2) fused with ELP.
The fusion proteins retained the functional activity of the fused moiety and the phase transitioning property of ELP, thereby allowing formation of heterogeneous NPs containing the 2 fusion proteins. The heterogeneous NPs prevented the degradation of the growth factor in the formulation both in the presence of purified protease and biologically relevant chronic wound fluid derived from patients. Furthermore, the NPs showed enhanced reepithelialization, inflammation resolution, and collagen remodeling in full thickness wounds created in genetically diabetic mice in the presence of HNE.
Our data indicate that the majority of the patient chronic wound fluid samples significantly or completely degraded the growth factor within 24 h, with some samples degrading it completely in as little as 30 min. This is in contrast to a previously conducted specimen analysis that reported little or no degradation of PDGF in chronic wound fluid in 12 h. 33 However, the concentrations of growth factor used in that study was at least 100 times higher than what we used in our study. The study noted that the high concentration of the growth factor might have overwhelmed the proteases present in the wound bed.
However, there was no quantification or identification of proteases done in the wound fluid raising the possibility that the chronic wounds that were selected might have low levels of proteases. On the contrary, we observed a clear correlation between high levels of HNE in the wound fluid and PDGF degradation. Indeed, when PDGF was incubated with purified human HNE at levels similar to chronic wound fluid, we observed rapid degradation of the growth factor. Indeed, HNE has been reported to abolish the activity of PDGF. 24 Although high level of HNE is reported in a subset of chronic wounds, there is a close correlation between high levels of HNE and the probability of nonhealing chronic wounds. 20 The rapid degradation of PDGF in chronic wound fluid containing high HNE levels may explain the mixed success of PDGF therapies in clinics. 34 Although one can imagine using high concentration of the growth factor to counteract the protease activity, 33 it may not be beneficial as growth factors are biologically active at an optimum concentration, and leading to increased costs associated with PDGF therapy. 35
The developed heterogeneous NPs displayed significant improvement in growth factor preservation in chronic wound fluid derived from patients and in the presence of purified HNE. Our developed approach of creating protease-resistant growth factor formulations is different from previously described methods of creating protease-resistant growth factors. 36 –38 These methods focus on creating mutants of growth factors by deleting the protease cleavage site. Although useful, these methods are cumbersome and have limited applicability, as one needs to create a mutant for every growth factor to make it resistant to proteases.
In contrast, our developed method can employ the same fusion protein to protect multiple growth factors from degradation, thereby eliminating the need for engineering every growth factor for protection. Indeed, in this study we show the protection of 3 other growth factors using the same approach. Moreover, the assembly of heterogeneous NPs ensures that the protease inhibitors are in close proximity to the growth factors.
This strategy is different from simply mixing the protease inhibitors with the growth factors because the aggregating property of ELPs results in colocalization of growth factors with the protease inhibitors thereby neutralizing the protease that is a direct threat to the growth factor. Of interest, the NPs were not able to protect the growth factor from degradation in certain wound fluid samples that had low HNE activity. This may suggest that other proteases such as MMPs may be responsible for growth factor degradation.
However, the modular design of the NPs allows inclusion of multiple protease inhibitors to impart protection of the growth factor from various proteases. Thus, treatment strategies can be customized based on the particular protease profile detected in the wound under treatment.
The NPs resulted in improved reepithelialization, collagen remodeling, and inflammation resolution in full thickness wounds created in diabetic mice. These wounds were supplemented with recombinant HNE to mimic the same high protease environment found in chronic wounds because diabetic mice wounds do not exhibit high protease levels. The success of these formulations in this modified wound model suggests that the protease inhibitor in the NP did not have any negative impact in wound healing. Although certainly wounds artificially supplemented with proteases do not truly mimic the chronic wound physiology, these data show that our NPs were successful in a protease rich environment similar to human wounds.
We are currently testing the efficacy of these NPs in a swine model of chronic wounds to get them closer to translation.
Of interest, wounds treated with the HNE+PMPD2-ELP+PDGF-ELP, HNE+PMPD2-ELP, and HNE+ELP alone exhibited significant granulation and collagen production and maturation in this mouse model. These data suggest that ELP may affect dermal fibroblasts in a way that is potentially beneficial for wound healing. This result agrees with our previous work where ELP induced fibroblast proliferation. 25,39
Indeed, wounds treated with HNE+rPDGF or HNE+PDGF-ELP were similar to the controls (only treated with HNE) suggesting that PDGF has limited effect in the presence of HNE in these wounds. Finally, wounds treated with PMPD2-ELP showed the least number of inflammatory cells suggesting that PMPD2-ELP results in the resolution of inflammation in this mouse model with elevated HNE levels.
In summary, we have developed novel protease-resistant growth factor NPs for treatment of chronic wounds with high protease activity. These NPs protect the growth factor in human chronic wound fluid. Although we have shown that protection of the growth factor by including an HNE inhibitor in the NP design, the modular nature of the design allows the inclusion of inhibitors of other proteases found in chronic wounds such as MMPs.
Innovation
Development of heterogeneous NPs put the protease inhibitor in close proximity of the growth factor. Current methods focus on creating mutants by deleting the protease cleavage site for each growth factor. Our results indicate that using the same protease inhibitor multiple growth factors can be protected thereby eliminating the need to produce mutants for each growth factor. We show the rapid degradation of growth factors and the utility of the NPs in preserving them in chronic wound fluid obtained from patients. These NPs may result in the translation of growth factor-based wound healing therapies to clinics.
Key Findings
Elevated protease levels found in human chronic fluid have devastating degradative effect on growth factors PDGF, VEGF, KGF, and EGF.
Heterogeneous NP was successful at extending the half-life of various growth factors in high protease environment.
The NPs result in improved collagen deposition, reduced inflammation, and improved reepithelialization in a rodent model with protease levels similar to that found in human chronic wound.
Footnotes
Acknowledgment and Funding Sources
This work was funded by National Institutes of Health (NIH) grant R21AR068013 (P.K.).
Author Disclosure and Ghostwriting
The authors declare that no financial interests exist. This article was written by the authors listed. No ghostwriters were used to write this article.
About the Authors