
Abstract
Significance:
Hair follicles are complex miniorgans that reside in the dermal layer of the skin. When the skin is wounded, epidermal stem cells in the hair follicle activate and start migrating into the wound site, differentiating into epidermal cells. and contributing to the reepithelialization of the wound. The hair follicles represent the deepest epidermal elements in the skin, which are extremely beneficial in partial-thickness burns and abrasions where the skin can regenerate from the hair follicles.
Recent Advances:
Advanced animal models have demonstrated that the contribution of epidermal stem cells in the hair follicle bulge and isthmus regions is important for wound healing. In addition, several clinical studies have shown successful harvesting and transplantation of hair follicles as a treatment modality to accelerate wound healing.
Critical Issues:
Deep and large wounds require hospitalization and, without exception, surgical treatment. Harvesting and direct transplantation of hair follicles could provide a great source of autologous epidermal stem cells for wound healing. The procedure can be done in an outpatient setting, quickly and without creating a large donor site wound.
Future Directions:
Transplantation of hair follicles in a combination with novel biomaterials could provide advantageous treatment possibilities for both chronic wounds and burns. There is a substantial amount of molecular signaling data available on the role of hair follicles during wound repair, but almost all the data are derived from rodent models, and thus, more information from large animals and most importantly from humans would be beneficial and help to advance this promising treatment further.

Scope and Significance
Hair restoration techniques have demonstrated the feasibility of hair follicle harvesting and transplantation. In the procedure, single or groups of hair follicles are usually harvested from the occipital area and transplanted to a bald area, and within a couple of months, they start generating new hair fibers. 1 Several preclinical and clinical studies have demonstrated that hair follicles can also be transplanted and used as an autologous cell source for wound healing. 2 The purpose of this review is to introduce both preclinical and clinical evidence of hair follicle transplantation as an alternative treatment modality for wound healing.
Translational Relevance
Multiple sophisticated animal studies have investigated the role of hair follicles during wound healing. It has been shown that when the skin is wounded, epidermal stem cells in the hair follicle activate and start migrating into the wound site, differentiating into epidermal cells, and contributing to the reepithelialization of the wound. 3,4 The important contribution of the hair follicles for wound healing has, for example, been demonstrated in a study that exhibited delayed reepithelialization in mutant mice that lacked all hair follicle development. 5,6
Clinical Relevance
Wounds that destroy the basal layer of the epidermis and the skin appendages (hair follicles and glands) require surgery to ensure healing. Skin grafting is the principal technology for treatment of full-thickness wounds. However, the technique is associated with problems such as poor graft take, infection, donor site morbidity. and lack of donor sites, especially in the treatment of large burns. 7 –9 Harvest and transplantation of hair follicles could provide a useful source of autologous keratinocytes for wound healing. Harvesting of hair follicles can be done quickly, utilizing established hair transplantation techniques and without creating a large donor site wound.
Background
Hair follicles are small organs that are present on most surfaces of the human body. They reside in the dermis and together with attached sebaceous gland and arrector pili muscle, they form an epidermal structure called pilosebaceous unit (Fig. 1A). Hair follicles are the smallest human organs that can regenerate and their most well-known function is to produce hair. 10 They consist of multiple epithelial and mesenchymal cell types and are structurally divided into distinct regions of the uppermost infundibulum, the isthmus, and the lower follicle that includes the bulge region as well as the dermal papilla (Fig. 1B). 11 The hair follicle cells in the bulge regions of the follicle are responsible for the uninterrupted renewal of hair follicles. First, they differentiate into highly proliferative matrix cells that further differentiate either into hair shaft cells or inner root sheath cells. Hair follicles regulate hair growth following a distinct growth cycle that involves an active growth phase (anagen), short transition phase (catagen), and resting phase of the hair follicle (telogen). 12
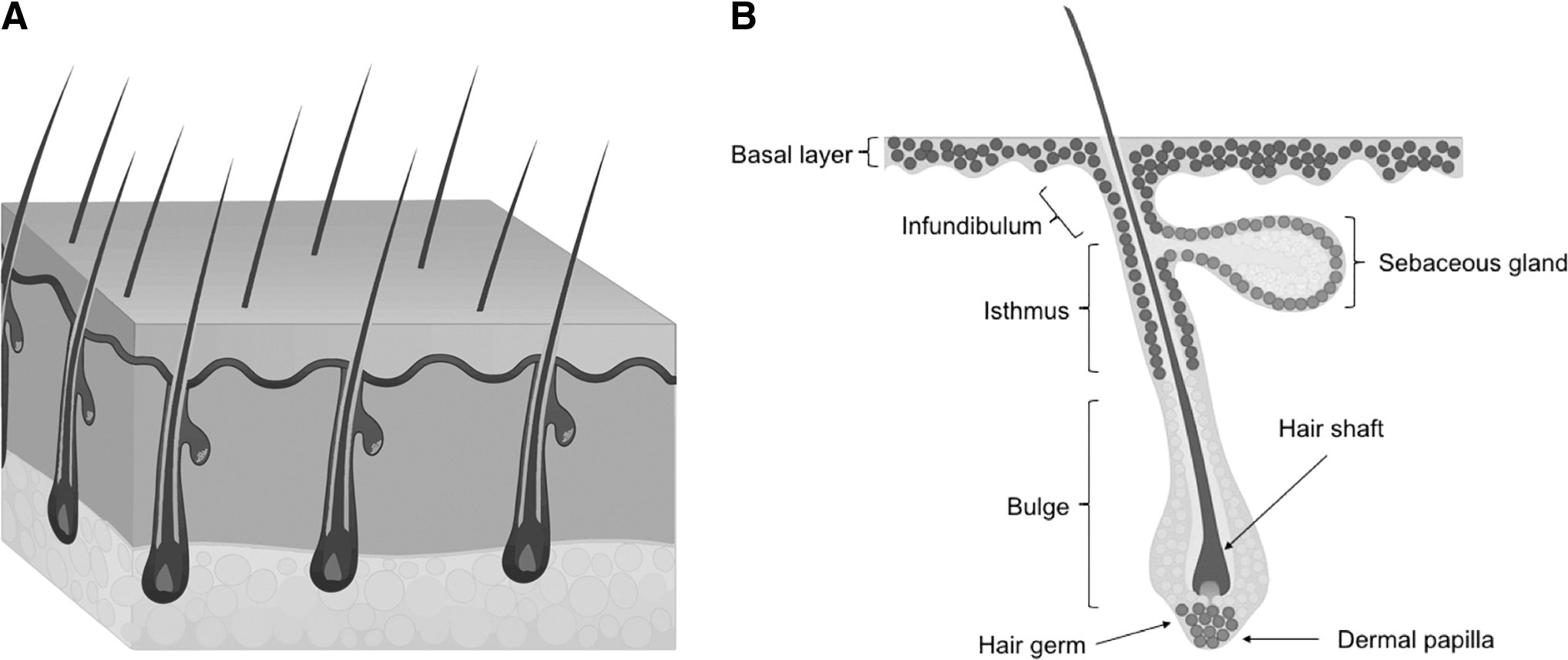
Hair follicle structure.
Hair follicles have been harvested and transplanted successfully for decades to treat baldness. In the procedure, small grafts containing one or more hair follicles are harvested usually from the occipital area of the head and transplanted into the bald area. Within a few months, the transplanted hair follicles start growing new hair that is resistant to the hormone (dihydrotestosterone) that causes hair loss and is thus considered permanent. The harvested hair grafts contain epidermis and almost all of the dermis, surrounding the hair follicle. 1,13 Currently, different techniques, including common follicular unit transplantation (FUT) and follicular unit extraction (FUE), are used to restore hair. FUT is a technique where first a strip of donor scalp is removed from the occipital area. Subsequently, naturally occurring groups of 1–4 hairs, called follicular units (FUs), are surgically separated from each other and further transplanted into the balding areas. The donor area is sutured leaving a linear scar. In FUE, individual FUs are excised directly from the scalp using a 0.8 to 1 mm needle-like punch. This procedure will result in a series of tiny dot scars in the donor area. 14,15
Over the years, wound care professionals have come to notice that interestingly, areas with high hair follicle density heal faster than the areas with less or without hair. In 1942, Brown and McDowell were the first to propose that beside hair formation, hair follicles also play a role in wound healing. In their article, Epithelial Healing and Transplantation of Skin, they suggested that during wound repair, the cells of the hair follicles dedifferentiate to cells that contribute to wound healing. They also noted that this must be the reason why wounds in the body regions without hair follicles, such as in soles and palms, heal slower than in the hair bearing areas. 16 Next, in 1945, Bishop published a study where he had investigated the role of hair follicles in wound healing by creating different depth wounds on his own forearm. His clinical and histological observations indicated that shallow wounds where hair follicles had remained intact healed faster. He also showed that in such wounds, reepithelialization started around the hair follicles, whereas in deeper wounds, the reepithelialization occurred only from the wound edges, thus taking much longer (Fig. 2). 17
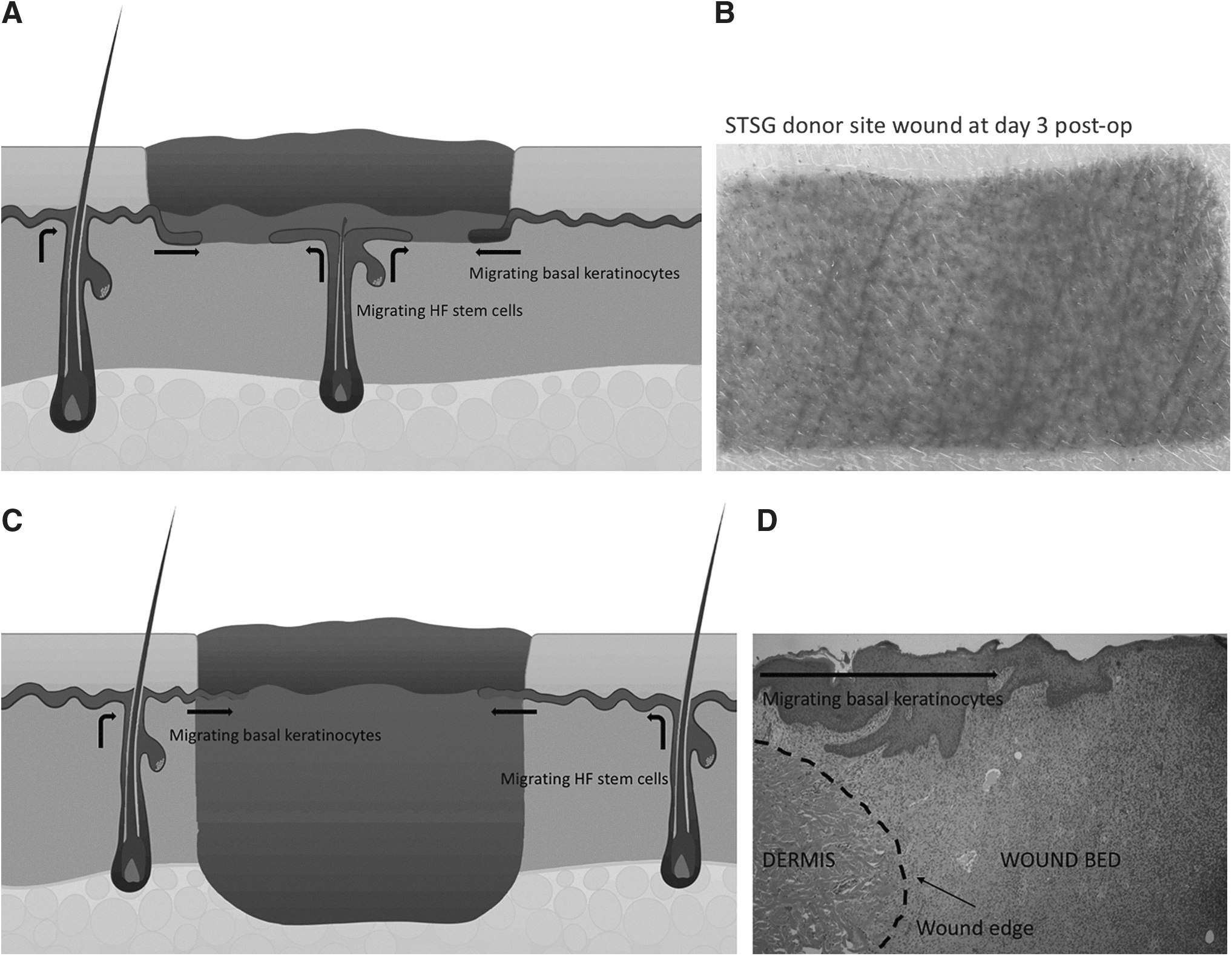
The role of hair follicles in superficial and full-thickness wound healing.
Discussion
There are numerous studies addressing the role of hair follicle and its stem cells on wound healing. The following review will first discuss and introduce central preclinical studies that have comprehensively demonstrated that hair follicles play a part in wound healing. In addition, preclinical studies have indicated that two distinct stem cell populations that are located in the bulge and in the isthmus regions of the hair follicle contribute to wound healing (Table 1). 18,19 Subsequently, clinical studies that exhibit how hair follicles contribute to wound repair are summarized (Table 2).
Summary of the preclinical studies
Summary of the clinical studies
CTRL, Control; FUT, follicular unit transplantation; HF, hair follicle; STSG, split-thickness skin graft.
Preclinical evidence
In the skin, epidermal stem cells reside in the innermost basal layer of epidermis and in the hair follicles. During normal skin homeostasis, the stem cells in the basal layer constantly form new epidermis by dividing, committing to terminal differentiation, and migrating toward the surface of the skin. The hair follicle stem cells differentiate into highly proliferative matrix cells that further differentiate either into hair shaft cells or inner root sheath cells. 20 The hair follicle stem cells can be found in the bulge region and in the isthmus of the hair follicle. In unwounded skin, the stem cells in the bulge regenerate new hair and the cells in the isthmus renew the nonhair parts of the follicle. However, once a wound occurs, both stem cell populations respond to the injury. They start differentiating to epidermal cells and migrating to the wound site to help replace the lost epidermis. Interestingly, the stem cells found in the bulge and in the isthmus have different characteristics. The stem cells that reside in the hair follicle bulge regions can be localized with multiple markers, the most commonly employed markers being cluster of differentiation (CD)34 and Keratin 15. In the isthmus, CD34 and keratin 15 are negative, but instead express markers such as leucine-rich repeat containing G protein-coupled receptor 6 (LGR6) and leucine-rich alpha-2-glycoprotein 1 (LRG1) (Fig. 1B). 21,22 The molecular mechanisms of how the hair follicle stem cells contribute to wound healing are still not completely understood. It has been suggested that the Wnt signaling pathway would regulate the process. The Wnt signaling pathway is a major regulator of organ development by directing cell proliferation, differentiation, and migration. It also plays a key role in both wound healing and hair follicle regeneration. The Wnt signaling is activated when wound occurs and it has been demonstrated to contribute in every phase of the healing process by controlling inflammation, programming cell death, and recruiting stem cell reservoirs within the wound. In hair follicles, during homeostasis, it governs their regeneration and promotes hair growth. 23 –25
Bulge region stem cells
The contribution of hair follicles to wound healing has been recognized in several sophisticated animal models (Table 1). These studies demonstrate that during wound healing, hair follicle cells can migrate to the injury site and contribute to reepithelialization. In a mouse model, Taylor et al. found that hair follicle bulge cells are bipotent as they can give rise to not only the hair follicle but also the epidermis. They showed that in normal neonatal mouse skin, the cells in the hair follicle bulge contribute to homeostasis by migrating to the epidermis. This phenomenon was not seen in adult mice until a wound occurred. 26 In another mouse study published in Nature, Ito et al. studied whether hair follicle bulge cells are necessary for epidermal renewal. In the first phase of the study, they ablated the hair follicle cells with a suicide gene and demonstrated that the ablation led to a complete loss of hair follicles, but survival of the epidermis. Subsequently, using a transgenic mouse strain, they showed that during normal skin homeostasis, the hair follicle stem cells did not generate new epidermis. Next, they created a superficial wound and found that the cells migrated from the bulge to the wound site. Finally, they showed that the new epidermis contained cells from both the basal layer and the hair follicle. However, it was shown that over time, the cells originating from the hair follicles were replaced by keratinocytes of epidermal origin. Therefore, the authors concluded that the hair follicle stem cells in the bulge region responded quickly to epidermal wounding by generating short-lived “transient amplifying” cells responsible for acute wound repair. 27 Langton et al. studied the role of hair follicle stem cells in mutant mice that were lacking all hair follicle development on their tail. Longitudinal full-thickness incisions were created on the dorsal surface of the tail of 8- to 10-week-old mice and wound healing rate and mechanisms were studied. The results showed that in the absence of hair follicles, cutaneous wounds healed with a delay of reepithelialization. Many wounds in wild-type mice were closed in 3 days, whereas all the wounds in mutant mice were still open on day 4. This delay in healing was resolved by day 6 postwounding when all the wounds in both wild-type and mutant mice were completely reepithelialized. The study also demonstrated that in the absence of hair follicles contribution to wound healing, epidermal cells from a wider area around the wound participated in the repair process, suggesting that recruitment of epidermal stem cells from the basal layer continues until enough epidermal cells required for a complete wound closure are present. 5 In a porcine model, Nuutila et al. studied the role of hair follicle bulge stem cells in wound healing by harvesting and transplanting hair follicle containing dermal micrografts into porcine full-thickness wounds. The presence of hair follicle stem cells in the grafts was studied with immunohistochemistry. It was shown that before transplantation, the grafts were negative for epidermal cell markers and contained CD34-positive cells. Six days after transplantation, immunohistochemistry revealed that no CD34-positive cells were present in the wound, but instead, the grafts that were still visible expressed Keratin 14. Therefore, it was concluded that, by day 6, the CD34 cells had differentiated into Keratin 14-positive epidermal cells, which migrated from the hair follicles of the grafts and contributed to the reepithelialization. Furthermore, treatment with the hair follicle containing dermal grafts demonstrated comparable quality of healing to that of split-thickness skin grafts (STSGs) in terms of reepithelialization rates, wound contraction, and scar elevation index. 28 Similarly, also in pigs, Rubis et al. showed that split-thickness dermal grafts can resurface and provide definitive coverage of full-thickness skin deficits. 29
Isthmus stem cells
The role of isthmus stem cells is less investigated than the cells in the bulge region (Table 1). Jensen et al. were the first to identify the isthmus cells as a distinct stem cell population. In a murine model, they reported that there is a population of follicular keratinocytes residing in the upper isthmus between the infundibulum and bulge regions that are distinguished by low α6-integrin levels and are negative for CD34. They isolated the cells using fluorescence-activated cell sorting (FACS) and showed in vitro that they have high clonogenic, multipotent, and self-renewal capacities. 30 Similarly, Nath et al. isolated the cell population from the isthmus and subsequently expanded them in culture to study their characteristics and multipotency. They showed that the cells possessed a high self-renewal capacity and shared characteristics of putative hair follicle epithelial stem cells, such as the expression of LGR6 and keratins 18 and 19. In addition, it was demonstrated that under defined culturing conditions, the cells were able to differentiate into mesenchymal cell lineages. 31 Snippert et al. also found that the hair follicle stem cells in the isthmus are not CD34 or keratin 15 positive, but are expressing LGR6 instead. They further suggested that the LGR6+ cells are the most primitive epidermal stem cells being able to generate all cell lineages of the skin. The contribution of these cells to wound healing was studied in a mouse wound model by inducing cell lineage tracing. LGR6+ progeny was traced after wounding and it was shown that clones derived from LGR6+ cells were found in the basal layer of newly formed epithelium. 32 Also in a murine model, Lough et al. studied the role of LGR6+ cells in wound healing. LGR6+ cells were isolated using FACS, labeled with green fluorescence protein, and transplanted into the wound beds of nude mice. They studied the effect on wound healing and hair follicle development and concluded that transplantation of LGR6+ epithelial stem cells promoted epithelialization, hair growth, and angiogenesis. 33 In another study by the same group, it was shown in vitro that LGR6+ cells were able to undergo proliferation, differentiation, and migration following seeding onto a variety of collagen-based scaffolds. When the LGR6+ scaffold constructs were deployed onto wounds in a murine model, they induced epithelialization, hair growth, and angiogenesis, demonstrating that the construct was capable of the repair of full-thickness wounds and hair regeneration. 34
Clinical evidence
The role of hair follicles in human wound healing has been studied by harvesting and transplanting scalp skin grafts, transplanting single or groups of hair follicles to treat chronic wounds, and using hair follicle containing dermal grafts in the treatment of burns (Fig. 3). However, many of the existing clinical studies are not controlled and contain only a few patients. Therefore, it is difficult to draw definite conclusions on the efficacy of the treatment based on the information from these studies (Table 2).

Hair follicle transplantation.
Hair-bearing donor site healing
Commonly, STSGs are harvested from the thigh or buttock because the skin in those areas is flat, regular, and easily accessible. However, often the donor sites heal slowly with visible scars. 35 Throughout the years, surgeons have used scalp as a donor site and demonstrated good results. In 1962, Crawford was the first to use the scalp as a donor site. They treated a young girl who was suffering from extensive deep burns with scalp grafts due to the lack of other donor sites. The results reported perfect graft take as well as rapid, both recipient and donor site, healing. Since then, the use of scalp as a donor site has been explored in multiple clinical studies and, in general, it has proven to be an excellent site, especially for thin skin graft harvesting. Moreover, the scalp can provide almost 10 percent of total body surface area and due to rapid donor site healing, it can be reharvested multiple times. 36 In a study by Barnett et al., the scalp was compared as a donor site to nonscalp donor sites. The study concluded that scalp is recommended as a donor site because of its availability, accessibility, excellent color match for facial grafting, and rapid healing. They also reported that covering the scalp donor site with a moist dressing further accelerated healing and allowed for a rapid reuse of the same site. 37 Similarly, Martinot et al. compared STSG donor site wound healing after harvesting grafts from the thigh and the scalp in pediatric burn patients. In total, 29 STSGs were harvested from the thigh and 39 from the scalp. The results showed that the scalp donor sites healed better than the donor sites created on the thighs. It was also shown that the transplanted STSGs from the scalp resulted in better quality of healing on the recipient site. Therefore, it was proposed that the difference in both donor and recipient site healing between the two STSGs was due to the hair follicle density in the graft. 38 Mimoun et al. harvested 945 scalp grafts from 757 adult patients and studied donor site healing. The study reported that a mean healing time was just over 6 days, demonstrating faster donor site healing in comparison to other donor skin areas. Also, no visible scars were observed. They further concluded that speedy scalp donor site healing minimized postoperative pain and enabled rapid reharvesting. In addition, they reported that after transplanting STSGs from scalp and from other body areas, no distinguishable differences at the recipient site were observed at the long-term evaluation. 39 Zakine et al. harvested two skin grafts from the same scalp donor site during the same procedure and reported that scalp was an excellent donor site because of rapid healing and the absence of visible scar. 40 Several other studies have also described the scalp as an advantageous donor site. 41 –46 Regardless, harvesting of uniformed, good quality, thin skin grafts from the scalp is technically very challenging due to its convex form. Therefore, despite its other benefits, burn surgeons continually choose to harvest the grafts from other regions if available.
In the treatment of chronic wounds
Hair transplantation has also been used to evaluate the utility of hair follicles in the treatment of chronic wounds. However, there are only a few properly controlled clinical studies that have compared hair follicle treatment to standard of care. In their controlled clinical trial, Yang et al. compared clinical outcomes of patients with chronic wounds following hair follicle therapy and STSG. In total, 40 patients were enrolled to the study, 20 receiving hair follicle transplantation and 20 conventional STSG. Furthermore, the patient ages and wound areas were similar between the study groups. Safety, healing duration, skin quality (recipient site), scar formation (donor site), and overall postoperative outcome were assessed at weeks 2, 8, and 12 postoperatively. The hair follicles were harvested from the scalp and transplanted into the wound bed at a density of 4 FUs per square centimeter, which was considered to be the minimum density required to ensure tissue regeneration. The study demonstrated that hair follicle therapy was safe and efficient in the treatment of chronic wounds. In comparison to STSG, the quality of both recipient and donor site healing was significantly better in the hair follicle-treated wounds. However, no difference in the duration of healing was observed. Overall, the study concluded that hair follicle therapy is safe and can achieve even better clinical outcomes than STSG in the treatment of chronic wounds. 47 Tausche et al. used hair follicle stem cells derived from the outer root sheath of plucked anagen hair follicles to produce an autologous epidermal equivalent, called EpiDex™. Subsequently, they performed a multicenter, randomized, prospective clinical trial to demonstrate that their tissue-engineered epidermal equivalent is safe and as effective as the current surgical standard, mesh graft, in the treatment of vascular leg ulcers. In total, 77 patients were enrolled to the study (EpiDex n = 43 and mesh graft n = 34). The results showed that there was no difference in the ulcer healing by week 12 between the EpiDex and the mesh graft. In addition, it was demonstrated that the EpiDex was well tolerated. 48 Ortega-Zilic et al. also performed an EpiDex study by treating 68 patients suffering from chronic wounds that were unresponsive to standard of care. The primary endpoint of the study was complete wound closure within 9 months after transplantation and the secondary endpoints were change of wound surface area and pain reduction. By the end of the study 74% of the chronic wounds treated with Epidex were completely healed and 12% of the patients did not respond to the treatment. Wound pain disappeared completely in 78% and partially in 13% of the patients. They concluded that the treatment with the stem cells derived from the hair follicle offered an opportunity to avoid conventional skin grafts in a significant number of patients suffering from chronic wounds. 49 In their randomized controlled clinical trial, Martínez et al. studied the role of hair follicles in wound healing by transplanting hair follicle containing punch grafts to venous leg ulcers and comparing the outcome to punch grafts without hair follicles. In total, 12 leg ulcers were treated with punch grafts harvested from the scalp and correspondingly, 12 leg ulcers were treated with punch grafts harvested from hairless areas of the body. The punch grafts were transplanted with a density of 5 grafts per square centimeter. Their results showed that the ulcers treated with scalp punch grafts healed statistically significantly better than the control punch grafts. They further concluded that hair punch grafting was a minimally invasive surgical procedure that appeared to be an effective treatment modality for chronic venous leg ulcers. 50,51
The following studies are pilot/feasibility studies that are lacking proper controls and/or contain only a few patients. In their clinical pilot study, Jiménez et al. transplanted autologous scalp follicular grafts into chronic leg ulcers to study feasibility and efficacy of the treatment. In total, 10 patients with ulcers who had not responded to topical medications and ambulatory medical care for 4 months or longer participated in the study. The ulcers were divided into treatment and control sites. The treatment sites received autologous scalp follicular grafts and the control sites remained nongrafted. The hair grafts were transplanted with a density of 5 follicular grafts per square centimeter.
At the 18-week endpoint, the authors observed almost 30% area reduction in the treated sites, whereas only 6.5% reduction was seen in the control sites. The authors concluded that hair follicle grafting was feasible in an outpatient setting and is a promising therapeutic alternative for nonhealing chronic leg ulcers. However, the authors did not compare the scalp grafts to conventional meshed STSGs. 52 In a noncontrolled single-patient case study, Fox et al. treated a man in his 60s with recurrent venous leg ulcers with punch grafts harvested from hair-bearing skin areas using the “stick and place” method. The “stick and place” is a hair transplantation method where the surgeon makes a slit with a needle or a blade and immediately places the graft into the incision. Approximately three grafts were transplanted per square centimeter. Their results showed that a month later, a 56% reduction in ulcer size was observed and they further concluded that punch grafts from body areas with high hair density are a viable source of follicular stem cells and a potential alternative for the treatment of chronic wounds. 53 In another noncontrolled case study, Alam et al. treated two patients (18- and 83-year-old males) suffering from nonhealing ulcers with FUT to promote wound healing. In their study the FUs were transplanted into the wound bed at an average density of 14 FUs per square centimeter. The results showed that regardless of the patients' age the FUT induced ulcer healing. The ulcer of the 18-year-old patient was considered fully reepithelialized and healed 3 weeks after FUT. Rapid healing was also seen in the ulcer of the 83-year-old patient. One month after FUT, a reduction in wound size as well as formation of new granulation tissue were observed. After 3 months, the ulcer had further reduced in size and completely healed by 6 months post-FUT. 54 Similarly, without a control treatment, Budamakuntla et al. used FUT to treat 15 patients with chronic nonhealing ulcers of more than 6 weeks. The FUs were harvested and transplanted into the ulcer bed at a density of 5 FUs per square centimeter. The study showed that 18 weeks posttransplantation, the wound area and volume were decreased by 49% and 72%, respectively. Thus, the authors further concluded that FUT is a feasible and promising therapeutic alternative for managing nonhealing chronic leg ulcers. 55
There is an increasing number of skin substitutes (from bioengineered skin to laboratory-cultured cells) that have been developed to offer either temporary or permanent wound closure depending on the composition of the product and to restore the functional and esthetic qualities of skin. In comparison to autografts, the biggest benefit of the skin substitutes is that not even a small donor site wound is required. This is very advantageous when the patient is fragile or in cases of large burns when rapid wound coverage is needed. However, no perfect skin substitute exists and therefore autotransplantation (if possible) or a combination of biomaterial and autograft is the most optimal treatment. 56 Hair follicle transplantation has also been combined with biomaterials in patient care. Narushima et al. used FUT together with an artificial dermis for scalp reconstruction in a noncontrolled two-patient case study. In the first phase, the scalp defect was covered with an artificial dermis. Subsequently, the dermal substitute was allowed to granulate until FUT was performed (3–4 FUs/cm2). After transplantation, in both cases, the artificial dermis reepithelialized from the implanted hair follicles. In addition, hair growth was evident on the treated scalp areas. The authors concluded that this technique to treat such defects was minimally invasive and cosmetically effective, and can be conveniently performed in an outpatient setting under local anesthesia. 57
In the treatment of burns
Hair follicle ability to contribute to reepithelialization has also been utilized in the treatment of burn injuries by transplanting hair follicle containing dermal grafts. Zakine et al. harvested hair follicle containing dermal grafts from scalp to treat patients with third-degree burns. In total, 15 patients participated in the study and the dermal grafts were used to treat burn wounds on the limbs and hands. The grafts were meshed threefold for limbs and left unmeshed for hands. The study showed that the hair follicle stem cells included in the dermal graft allowed reepithelialization of the burn similar to STSGs. In addition, the clinical evaluation showed that the quality of the new epidermis was good and histology demonstrated that the thickness of the epidermis was normal. 40 Similarly, Lindford et al. treated acute burn wounds by grafting the burns with dermal grafts. At first, standard STSG was obtained, and subsequently, from the same site, another purely dermis split-thickness graft was harvested. The dermis graft was meshed to achieve an expansion ratio of 1:2. In total, 16 patients were treated with dermal grafts, graft take was complete in 15/16 cases. They showed that hair follicle stem cells in the dermal grafts mobilized, differentiated, and migrated onto the surface of the graft forming new epidermis, and thus, all grafts recorded over 90% epithelialization by week 4. The study also showed that no difference in donor site healing time was observed when compared to STSG. Therefore, it was concluded that hair follicle containing dermal grafts provide an additional autologous option for permanent coverage in the treatment of major burns without increasing donor site size or morbidity. 58 Navsaria et al. reported a case where they had reconstructed a head and neck full-thickness burn with a tissue-engineered dermal template that was 12 days later grafted with hair follicles. The hair follicles were obtained by excising an ellipse of occipital scalp. Single hair follicle containing micrografts were dissected out of the occipital graft and excised free from the subcutaneous fat. Consequently, the hair follicles were implanted through small incisions in the outer layer of the dermal template at a density of 2 follicles per square centimeter. This way, an expansion ratio of 1:5 was achieved. The treatment resulted in complete reepithelialization and a hair-bearing scalp. 59
Summary
In superficial wound healing where skin appendages have remained intact, reepithelialization starts simultaneously from the hair follicles and from the wound edges, making the wounds heal rapidly (Fig. 2A, B). Full-thickness wound healing where skin appendages have been destroyed, the wounds heal through granulation tissue formation and reepithelialization from the wound edges (Fig. 2C, D). However, several animal studies have demonstrated that during the repair process, the hair follicle stem cells in the hair follicles surrounding the wound contribute to wound healing by differentiating to epidermal cells and migrating to the wound site. In addition, clinical studies have confirmed the role of hair follicle stem cells in human wound healing. It has been shown that wounds in areas with high hair density such as the scalp heal faster than in nonhair bearing areas such as in palms and soles. Therefore, the scalp has been discovered to be an excellent donor site for skin graft harvesting, allowing rapid reharvesting. In addition, hair follicles have been transplanted successfully using common hair restoration techniques and as dermal grafts to treat chronic wounds and burns, and the outcomes have been comparable to STSG. However, most of the clinical trials do not compare hair follicle transplantation to current standard of care and contain only a few patients. In addition, there are no clinical studies where hair follicle transplantation would have been used in the treatment of large defects such as large burns. Therefore, more randomized, controlled clinical trials would be needed to properly investigate the utility of this technique as an alternative for STSG.
Take-Home Messages
Hair follicles contain epidermal stem cells that reside in the bulge and isthmus regions of the follicle.
When a wound occurs, the stem cells in the follicle differentiate and migrate to the wound site to form new epidermis.
Body areas with high hair density such as scalp heal faster than areas with lower hair density, such as palms and soles.
Hair follicles can be transplanted to treat wounds using common hair restoration techniques.
Footnotes
Acknowledgments and Funding Sources
No funding was received to support this work. Jessica Kiablick is gratefully acknowledged for making the graphs.
Author Disclosure And Ghostwriting
The author declares no conflict of interests. No ghostwriters were involved in the writing of this article.
About The Authors