
Abstract
Significance:
Wound healing involves the phasic production of growth factors (GFs) and cytokines to progress an acute wound to a resolved scar. Dysregulation of these proteins contributes to both wound chronicity and excessive scarring. Direct supplementation of GFs and cytokines for treatment of healing and scarring complications has, however, been disappointing. Failings likely relate to an inability to deliver recombinant proteins at physiologically relevant levels to an environment conducive to healing.
Recent Advances:
Inspired by the extracellular matrix, natural biomaterials have been developed that resemble human skin, and are capable of delivering bioactives. Hybrid biomaterials made using multiple polymers, fabrication methods, and proteins are proving efficacious in animal models of acute and impaired wound healing.
Critical Issues:
For clinical translation, these delivery systems must be tailored for specific wound indications and the correct phase of healing. GFs and cytokines must be delivered in a controlled manner that will target specific healing or scarring impairments. Preclinical assessment in clinically relevant animal models of impaired or excessive healing is critical.
Future Directions:
Clinical success will likely depend on the GF or cytokine selected, their compatibility with the chosen biomaterial(s), degradation rate of the fabricated system, and the degree of control over release kinetics. Further testing is essential to assess which wound indications are most suited to specific delivery systems and to prove whether they provide superior efficacy over direct protein therapies.

Scope and Significance
This review introduces growth factors (GFs) and cytokines involved in the skin wound healing response and summarizes attempts to harness them as wound therapeutics from studies that meet 50% or more of the CONSORT randomized control trial reporting standards. Natural biomaterials developed as GF and cytokine delivery systems are then critiqued as to whether they offer therapeutic advantages over direct protein administration. Finally, a preclinical development pathway is proposed to aid translation of these wound and scar therapies.
Translational Relevance
Much is known about the roles of GFs and cytokines in successful, impaired, and excessive healing responses. Yet, attempts to harness them as wound therapeutics have yielded disappointing results. To address limitation associated with their administration, biomaterial-based delivery systems that offer tailored protein release, proteolytic and immune protection, and an extracellular matrix (ECM) replacement have been developed. While these systems are proving efficacious in preclinical models, it is unclear whether this will translate to human wound indications. To ensure success, it is critical that testing occurs in a standardized manner in clinically relevant wound models, in comparison to direct protein administration.
Clinical Relevance
Wound skin complications are highly prevalent and include surgical site infections, traumatic or combat injuries, burns, pressure ulcers in the immobile, foot and limb ulcers in the elderly, obese, and diabetic, as well as fibrotic and scarring disorders. While numerous GFs and cytokines have been tested for these pathologies, only selected treatments are approved for clinical use. Presently, Regranex® is the only GF product that is FDA-approved for treatment of neuropathic diabetic ulcers, with two others available in selected countries. As yet, no such treatments are available for pressure ulcers, or for surgical, traumatic, burn, infected, or scar-prone wounds.
The reasons why GF and cytokine therapies may have failed are numerous. Contributing factors likely include trial design limitations, poor patient compliance, risk of systemic action and immunogenicity, proteolytic degradation, and variability in the responsiveness and support for healing provided by the surrounding tissue. The net result being a failure to deliver therapeutically relevant levels of these proteins to a wound receptive to that intervention. Given the clinical need, it is critical that issues identified with GF and cytokine use be addressed. Natural biomaterials that provide sustained protein retention and delivery, along with a physical environment supportive of healing, thus offer hope in overcoming these limitations and addressing the growing health burden associated with cutaneous wounds.
Background
Cutaneous wounding stimulates a complex series of events that regulate the progression from an acute wound to a resolved scar (Fig. 1). This process involves a diverse number of cell types, ECM components, the regulatory GFs, and cytokines that direct their interactions. 1
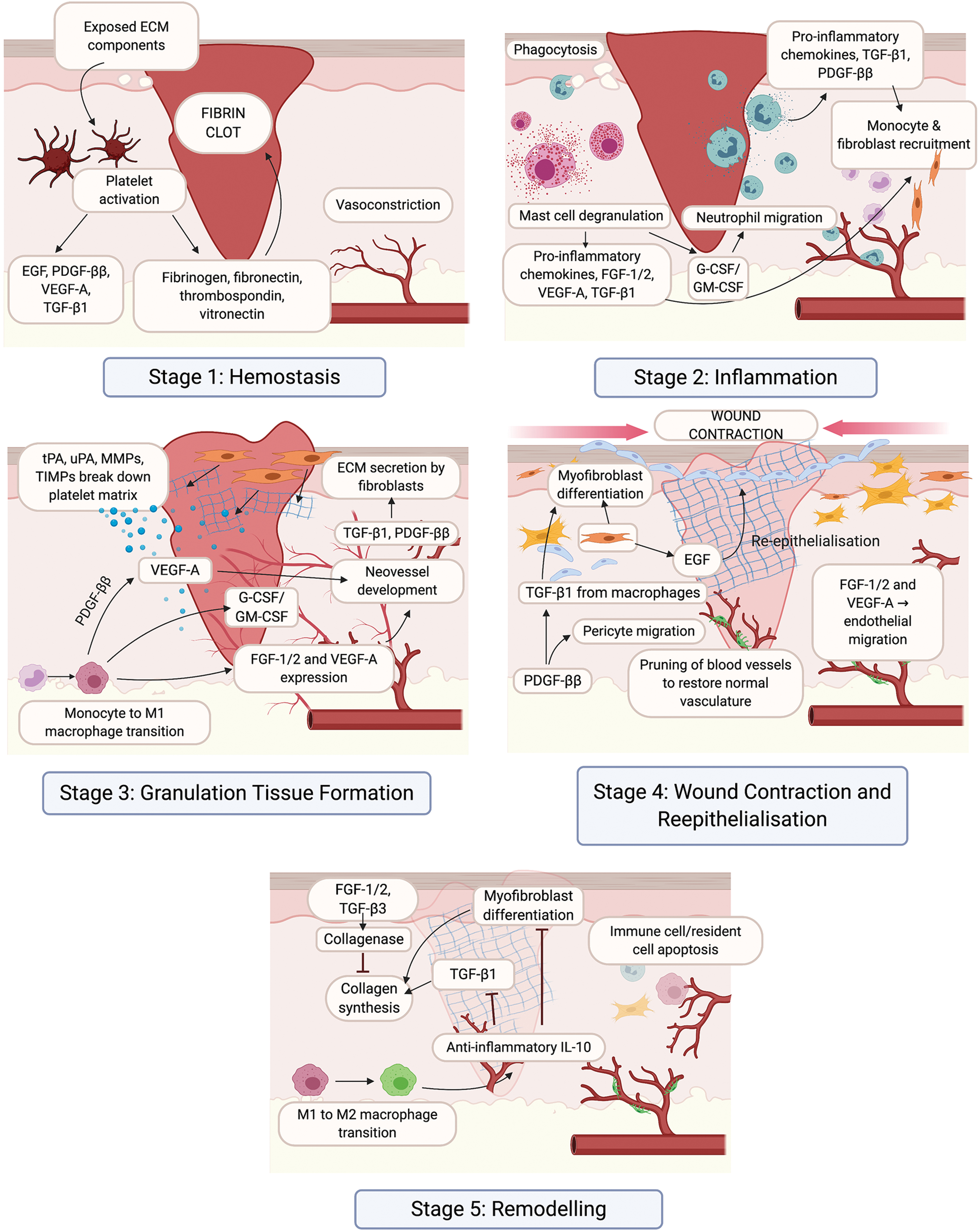
The wound healing response of the skin. There are five key stages in the wound healing response: hemostasis (1), inflammation (2), granulation tissue formation (3), wound contraction and reepithelialization (4), and remodeling (5). Critical cell types, GFs, and cytokines that regulate each stage of the wound healing response are indicated. ECM, extracellular matrix; EGF, epidermal growth factor; FGF, fibroblast growth factor; G-CSF, granulocyte colony-stimulating factor; GM-CSF, granulocyte-macrophage colony-stimulating factor; HA, hyaluronic acid; IL, interleukin; MMP, matrix metalloproteinases; PDGF, platelet-derived growth factor; TGF, transforming growth factor; tPA, tissue plasminogen activator; uPA, urokinase-type plasminogen activator; VEGF, vascular endothelial growth factor. Color images are available online.
Successful cutaneous wound healing
Following injury, the skin must reach hemostasis before it can begin to heal (Fig. 1). 2 Disruption of the endothelium exposes ECM components that activate platelets, initiating the coagulation cascade, with cleavage of fibrinogen by thrombin and release of fibronectin, thrombospondin, and vitronectin. This leads to platelet aggregation and formation of a fibrin clot to prevent blood loss, protects from microbial infiltration, and provides a scaffold for invasion of inflammatory cells in response to inflammatory cytokines and GFs released by platelets.
During the inflammatory phase of wound healing (Fig. 1), 3 damaged endothelial cells facilitate entry of neutrophils to phagocytose debris and invading bacteria, and express proinflammatory cytokines that recruit monocytes and fibroblasts to initiate granulation tissue formation. Monocytes then differentiate into proinflammatory (M1) macrophages that produce matrix metalloproteinases (MMPs) to enhance migration through the fibrin clot. 4 M1 macrophages also produce GFs and cytokines that recruit endothelial cells into the provisional ECM, with the new blood vessels giving the tissue its highly vascularized and granular appearance. 5
Once granulation tissue formation has commenced, wound closure occurs through reepithelialization and contraction (Fig. 1). Keratinocytes migrate across the provisional matrix in response to GFs to restore the epithelial barrier. 6 This process is assisted by differentiation of fibroblasts into alpha-smooth muscle actin-expressing myofibroblasts that support wound contraction. 7 Transition of M1 macrophages into a M2 phenotype allows for expression of cytokines that dampen inflammation and cell proliferation. 4
GFs activate fibroblasts to secrete a new collagen-rich ECM that undergoes substantial remodeling (Fig. 1), a process that can last for years. 8 During this time, cellular recruitment ceases, with much of the infiltrate undergoing apoptosis. Recruitment of pericytes to the endothelium allows for maturation of its function. 9 Differentiation of the epithelium reestablishes barrier functionality, although regeneration of epithelial appendages, such as hair follicles and sweat glands, is minimal. 6 Fibroblasts continue to synthesize ECM, which transitions from type III to type I collagen, increasing tensile strength and structural integrity. GFs and MMPs produced by M2 macrophages regulate the realignment of collagen into highly organized bundles that strengthen the scar. 8
Cutaneous wound complications: impaired and excessive healing
Healing complications emerge in patients with vascular insufficiency and diabetic neuropathy, but chronicity can also occur in acute wounds following surgical, traumatic, or burn injury. 10 –12
Impaired healing results from disruptions in the transition between stages, leaving the wound in perpetual inflammation and hypoxia (Fig. 2). 3,12 Inflammatory and oxidative complications are driven by excess platelet activation, neutrophil and monocyte recruitment, production of proinflammatory cytokines, lipid mediators, reactive oxygen species (ROS), as well as MMP-mediated degradation of GFs, cytokines, and ECM. Damage to the vasculature results in a failure to deliver sufficient oxygen and nutrients to support repair. Persisting neutrophils and ROS production also damages the ECM causing cellular senescence. M1 macrophage persistence is observed, as these cells fail to differentiate into the proresolving M2 phenotype. Transition to a chronic state is also associated with formation of antibiotic-recalcitrant bacterial biofilm communities, which produce proteases that degrade GFs and cytokines. 13,14
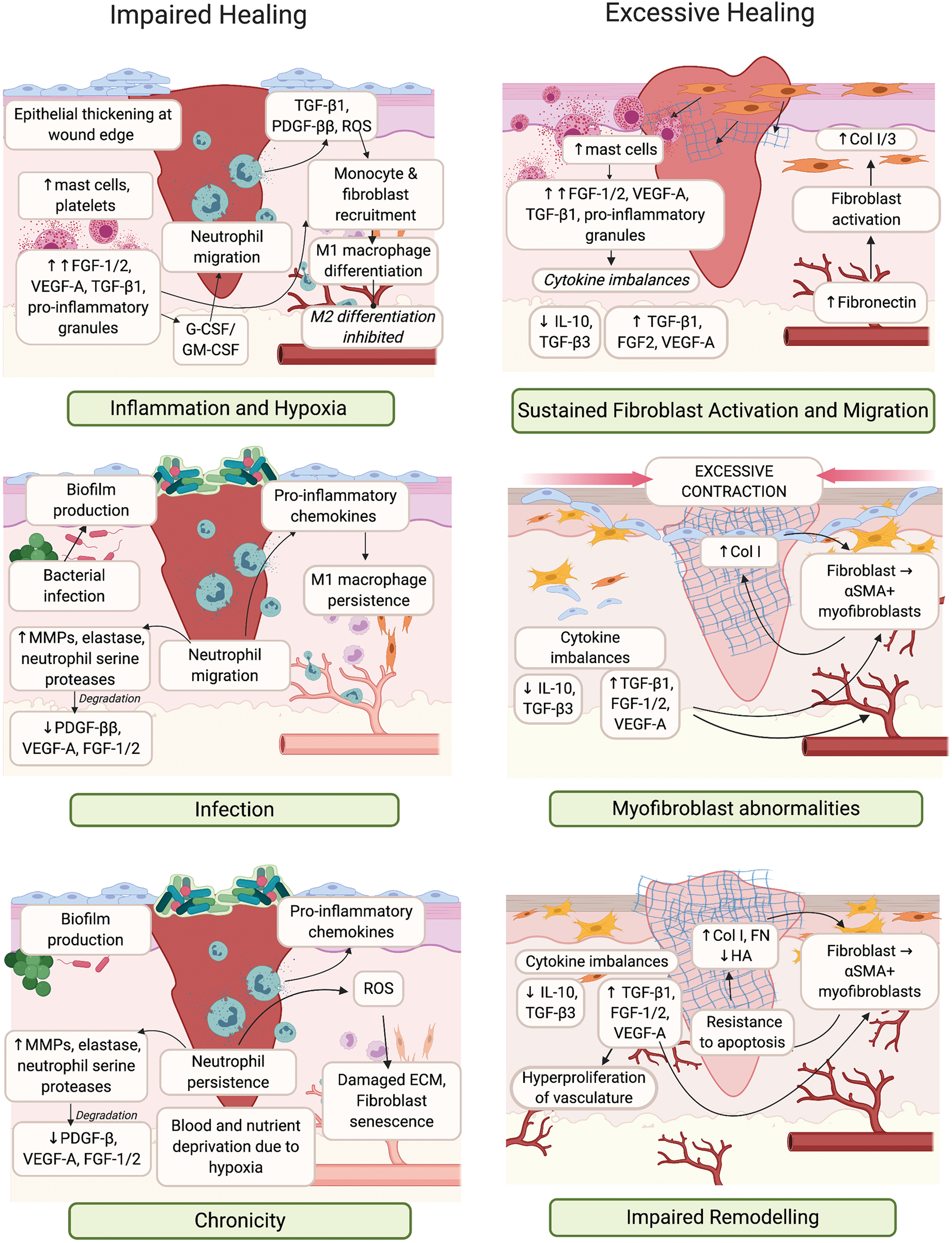
Impaired or excessive healing of skin wounds. Impaired healing occurs due to inflammation and infection, resulting in wound chronicity (left panel). Excessive healing occurs due to sustained inflammation and myofibroblast abnormalities, resulting in impaired remodeling (right panel). Critical cell types, GFs and cytokines that are dysregulated each stage of the wound healing response are indicate. αSMA, alpha-smooth muscle actin; Col, collagen; FN, fibronectin; ROS, reactive oxygen species. Color images are available online.
Cumulatively, the failure to produce ECM confounds GF and cytokine dysfunction, leading to defective granulation tissue formation and a hyperproliferative epidermis that prevents reepithelialization.
Where chronicity is defined as a lack of healing, excessive scarring is a case of exaggerated healing. 15 Hypertrophic scars are characterized by hyperproliferation of the ECM and surrounding vasculature, and form 1–3 months after tissue insult. However, unlike keloid scars, they do not extend outside of the original wound boundary. 16 These scars emerge as a result of excessive inflammation and ECM deposition (Fig. 2). Mast cell infiltration and degranulation contributes to increased histamine, proteoglycans, proteinases, proinflammatory cytokine, and GF levels. 17 Excess in these mediators sustains the activation of M2 macrophages, endothelial cells, and fibroblasts. 18 –20
Normal, hypertrophic, and keloid scars, in turn, are associated with greater extent, persistence, and dysfunction of the vascular and fibrotic responses, which leads to pronounced type I collagen deposition and bundle thickening, resulting in a characteristic lack of flexibility.
GFs and cytokines in the treatment of human wound indications
A multitude of GFs and cytokines are critical to skin repair, with their dysregulation contributing to impaired or excessive healing (Figs. 1 and 2). 21 –23 Their direct administration has also been trialled as treatments for chronic ulcers, burns, or scar-prone wounds, and those trials that meet 50% or more of the CONSORT reporting standards to clinical trials are listed in Table 1 (with the full CONSORT checklist provided in Supplementary Table S1). 24 Of particular importance are the epidermal growth factor (EGF), colony-stimulating factor (CSF), fibroblast growth factor (FGF), interleukin (IL), platelet-derived growth factor (PDGF), transforming growth factor (TGF), and vascular endothelial growth factor (VEGF) families.
Randomized control trials of cutaneous wound and scar treatments utilizing growth factors or cytokines
Until primary endpoint was reached.
Treatment timing or length not evident.
Adherence to CONSORT reporting standards.
CMC, carboxymethylcellulose; EGF, epidermal growth factor; FGF, fibroblast growth factor; G-CSF, granulocyte colony-stimulating factor; GM-CSF, granulocyte-macrophage colony-stimulating factor; HA, hyaluronic acid; IL, interleukin; PDGF, platelet-derived growth factor, TGF, transforming growth factor; VEGF, vascular endothelial growth factor.
The only FDA-approved GF treatment for neuropathic ulcers is recombinant human (rh)PDGF-ββ delivered in a carboxymethylcellulose (CMC) hydrogel (Regranex). A biosimilar (Plermin™) was launched in India in 2013. PDGF-ββ is released during hemostasis by activated platelets to promote migration of neutrophils, macrophages, and fibroblasts, induce granulation tissue formation, and recruit pericytes to new blood vessels (Fig. 1). 25 Expression of PDGF-ββ is decreased in chronic wounds (Fig. 2). 26
Once or twice daily application of rhPDGF-ββ hydrogel led to more complete healing of nonhealing diabetic foot ulcers (Table 1), 27 –29 with a trend toward faster healing in pressure ulcers 30,31 but not hypertensive ulcers. 32 Faster reepithelialization of traumatic wounds was also observed following hydrogel treatment. 33 It has noted that in these trials, there was extensive variability in wound closure rates for placebo and standard care controls, and in response to rhPDGF-ββ hydrogel, meaning that large trials were needed to demonstrate a treatment effect. 34
An increased risk of death from cancer was also observed, 35 which was postulated to result from systemic leakage of PDGF-ββ from the wound stimulated the growth of preexisting cancers expressing its receptor. As a result, Regranex was issued a black-box warning by the FDA in 2008, but this was removed in 2018 in response to postmarketing analysis that showed no increased risk of cancer or cancer mortality. 36
Three products containing rhEGF are available for treatment of diabetic foot ulcers. Heberprot-P® is registered in 15 countries and is administered by intralesional injection to recalcitrant ulcers. Easyef® is a topical spray approved for diabetic foot ulcers in four Asian countries. Regen-D™ is a topical hydrogel commercialized in India. EGF is produced by activated platelets, M1 and M2 macrophages, and fibroblasts and drives reepithelialization (Fig. 1). 37 Expression of EGF is limited in chronic wounds (Fig. 2). 26
An early clinical study with rhEGF administered topically once or twice daily to diabetic foot ulcers showed more complete healing than the cream control (Table 1). 38 Complete healing of superficial ulcers in diabetic patients was also accelerated by rhEGF when administered by twice daily topical spray 39 or intralesional injection three times per week, 40 with variable findings from the topical hydrogel. 41,42 Short-term topical administration of rhEGF in thyroidectomy incisions led to improvements in scar parameters relating to pliability and thickness. 43
A topical spray containing rhFGF-2 (Fiblast®) is marketed for skin ulcers in Japan, while rhFGF-1 has been evaluated for skin ulcers and burns. FGF-1 and FGF-2, also known as acidic and basic FGF, respectively, are produced by most skin cells. These GFs increase keratinocyte, endothelial, and fibroblast motility to promote reepithelialization and granulation tissue formation (Fig. 1). 44 FGF-2 also regulates the production of collagenase/MMP1 to refine the newly synthesised ECM.
Decreased expression of FGF-2 has been observed in chronic wounds (Fig. 2). 26 Following daily application of rhFGF-2 using topical sprays (Table 1), severe pressure ulcers showed trends toward faster healing, 45,46 while diabetic patients with neuropathic ulcers of mixed severity showed no change in healing. 47 Treatment of partial-thickness burns with topical rhFGF-2 spray, also elicited improvements in healing rate and scar flexibility. 48 Daily topical administration of rhFGF-1 accelerated healing in partial-thickness burns and skin graft donor sites (Table 1) 49 and showed greater healing improvements than rhFGF-2 in chronic wounds of diabetic patients. 50
A topical hydrogel administering rhVEGF-A (Telbermin) was discontinued following a Phase II trial. VEGF-A is produced by most skin cells and mediates fibrin deposition, MMP production, monocyte recruitment, reepithelialization, and angiogenesis (Fig. 1). 8,51 Chronic wounds show abnormally low levels of VEGF-A protein, 26 while excess VEGF-A has been implicated in wound inflammation, edema, and scar formation (Fig. 2). 20 Diabetic foot ulcers only showed a trend toward faster healing following treatment every second day with this hydrogel (Table 1). 52 This indicates the lack of progression for Telbermin and may relate to the treatment's failure to achieve complete wound closure.
Granulocyte colony-stimulating factor (G-CSF) and granulocyte macrophage colony-stimulating factor (GM-CSF) are cytokines developed as therapeutics for other indications. 53,54 Leucomax® (rhGM-CSF) is a FDA-approved immune stimulator administered following chemotherapy and bone marrow transplantation, while Neupogen® and Granocyte® (rhG-CSF) are indicated to reduce neutropenia. Produced by a range of skin cells, these cytokines stimulate neutrophil proliferation, differentiation, and infiltration of the wound bed (Fig. 1). 53,54 GM-CSF also promotes reepithelialization and vascularization, and myofibroblast-mediated wound contraction.
Trials in patients with infected diabetic foot ulcers yielded inconsistent results following daily treatment with rhG-CSF (Table 1). 55 –57 Treatment of chronic and pressure ulcers with rhGM-CSF also yielded variable results, 45,58 but complete healing was observed with venous ulcers following weekly administration. 59 These inconsistent results may, in part, be due to the production of neutralizing antibodies against the rhGM-CSF, which have been observed following repeated subcutaneous administrations to immune-competent individuals. 60
Other cytokines have been explored as antiscarring therapies. Avotermin, a rhTGF-β3 preparation, showed promise in Phase II trials, but failed to improve scar appearance following scar-revision surgery in Phase III trials. 61 The TGF-β family are multifunctional cytokines produced by inflammatory and resident skin cells, that recruit inflammatory cells to the wound, and induce blood vessel formation (Fig. 1). 62 While TGF-β1 promotes collagen deposition, TGF-β3 inhibits this and promotes ECM remodeling (Fig. 2).
rhTGF-β3 was first trialled in pressure ulcers, with accelerated healing observed following daily administration with a topical hydrogel (Table 1). 63 Intradermal administration of rhTGF-β3, before and after skin incisions, varicose vein, or scar revision surgery improved scar aesthetics for 5–12 months (Table 1). 64 –67 Inconsistencies between the design of the Phase II and Phase III trials, such as in the timing of treatments and the timing and measurement of scarring outcomes, may have contributed to the lack of progression for Avotermin.
Another cytokine explored for antiscarring purposes is IL-10 (Ilodecakin), which following a Phase II trial did not progress further after Avotermin failed. IL-10 is an anti-inflammatory cytokine produced by leukocytes, which suppresses inflammatory and fibrotic gene expression, reducing myofibroblast contractility, and limits collagen deposition through induction of MMP1 (Fig. 1). 68 IL-10 is considered necessary for scarless fetal wound healing and has a protective role for skin conditions such as psoriasis. Intradermal administration of rhIL-10, before or after skin incisions, showed a reduced scar width and transient improvements in scar aesthetics at selected doses (Table 1). 69,70
In summary, with numerous trials conducted in patients with chronic ulcers, only three GF therapies increased complete healing (Table 1), and are now approved for clinical use, although for specific indications or in limited countries. Importantly, no GF or cytokine therapies enhanced healing of pressure ulcers, traumatic, infected, and burn wounds sufficiently to warrant approval. In addition, GFs and cytokines therapies showed only partial or temporary improvements in scarring following experimental or surgical incisions. Many reasons have been proposed as to why GF and cytokine therapies failed to achieve meaningful outcomes. These include difficulties designing clinical trials for wound therapies, defining appropriate measures of treatment success, the costs associated with development and testing, and issues with efficacy or safety. 71
Most trials have attempted to standardize protocols, but as evidence in the trials with rhPDGF-ββ, 34 differences in ulcer duration, size, and intrinsic healing capacity greatly influence healing. Interpatient variability, with regard to this wound microenvironment, also results in differences in responsiveness to GF and cytokine interventions. The ability to stratify wounds into those likely to be responsive to a specific GF or cytokine treatment is thus critical to clinical success. Identification of molecular biomarkers that may indicate whether wounds are likely to heal or not heal will greatly help selection of trial participants. 72
Another significant issue is that the FDA currently only accepts complete wound healing as an endpoint for chronic ulcer trials. 73 As shown with the trials assessing rhVEGF-A, 52,73 it can be difficult to demonstrate a significant difference between groups if patients do not heal within the study timeframe. GF and cytokine therapies may progress further if patient follow-up is extended and alternative outcomes such as time to heal, rate of wound size reduction, or health-related quality of life are deemed acceptable. Trials of scar therapies are also limited in that there is at present no standardized outcome measure to indicate treatment success. 74 Differences between the trials with rhTGF-β3 indicate how scar assessment protocols can alter trial outcomes. 61,64,67
Financial implications can also influence whether and how GF or cytokine wound healing therapies are trialled. 71 Randomized controlled trials are very costly and investors are looking for strong intellectual property, and the shortest, most cost-effective route to the largest potential market for a given product. Much of the knowledge regarding GFs and cytokines is already in the public domain presenting limited scope for patents, which is likely to reduce investment. Thus innovative production or delivery systems and novel treatment combinations tailored for specific indications are essential to maximizing patent claims and obtaining trial sponsorship. 75 Commercial considerations can also influence clinical trial design. 71 Instead of choosing the subset of patients most likely to benefit from the treatment, a study population maybe chosen to support future marketing claims, or adjusted during the course of the trial to meet enrolment targets.
The therapeutic efficacy of recombinant proteins can also be compromised by the proteolytic nature of chronic wounds, 14 and by systemic or immunogenic clearance. 60,76 The net result being that GF and cytokines may not have been delivered to receptive wounds at therapeutically relevant levels. This issue can be overcome by increasing the frequency or dosage of the protein administered. 21 But these changes in the treatment regimen likely reduce patient compliance, 10,11,77 and may exasperate local hypersensitivity reactions and the risk of systemic action on healthy or cancerous tissue. 35,76
Given the extreme clinical need, and the promise offered by GF and cytokine therapies across a broad range of wound complication, it is critical that the issues identified with their clinical application be addressed. Natural biomaterials can retain GFs and cytokines within the wound, while providing sustained local delivery and a physical environment supportive of healing processes (Fig. 3). Innovative combination therapies may therefore offer greater efficacy, safety, and patentability, thus addressing many of the limitations associated with direct GF or cytokine administration.
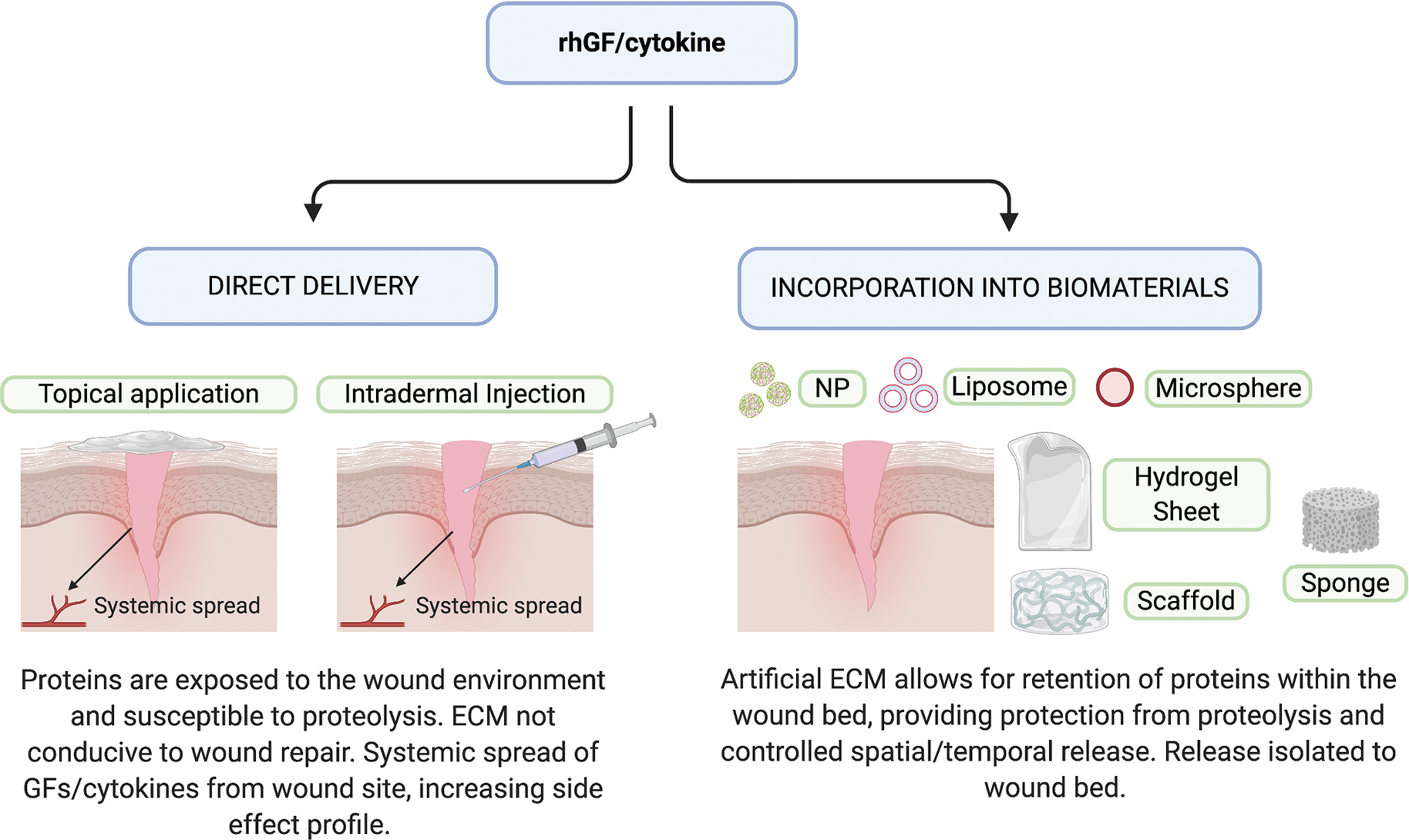
Methods for delivering GFs and cytokines to skin wounds. Direct delivery of rhGFs or cytokines is achieved via topical application or intradermal injection (left), with only short-term bioactivity, due to proteolysis and an ECM not able to support their action. Biomaterial-based delivery is achieved through the incorporation of rhGFs or cytokines into an ECM-like hydrogel, scaffold, sponge, or particle (right) that offers proteolytic protection and structural support for sustained bioactivity. ECM, extracellular matrix; NP, nanoparticles to list of abbreviations; rh, recombinant human. Color images are available online.
Such GF and cytokine delivery systems are in development with the first in human clinical trials (Table 1). For example, administration of FGF-2 applied in a collagen sponge to chronic ulcers 78 and to traumatic wounds 79 showed greater closure relative to the sponge alone. GM-CSF delivery with an alginate dressing was trialled in chronic ulcers, 80 and a GM-CSF-gelatin hydrogel accelerated closure of partial thickness burns when applied daily. 81 –83 The appearance of established scars was also improved following 12 weeks of twice daily treatment with rhTGF-β3 in a silicone-hyaluronate cream. 84 GF and cytokine delivery systems therefore offer potential as therapies for cutaneous wound indications. But to ensure their success, it is critical to evaluate which biomaterials are most compatible with specific GF and cytokine delivery systems, and to prove their superior efficacy and safety relative to direct protein therapies.
Discussion
Biomaterials as repositories for GF and cytokine delivery
Biomaterial-based scaffolds have become very popular due to their unique biocompatibility, ease of functionalization, and release capability. When fabricated, these biomaterials function as a three-dimensional (3D) biomimetic ECM, simulating the arrangement and role of their native counterpart. The ECM is composed of fibrous proteins, as well as an abundance of proteoglycan. 85 The proteins provide important adhesive domains that anchor cells to the ECM, and with proteoglycans, direct cellular function through their interactions with GFs and cytokines. When a wound occurs, both cells and surrounding ECM are lost. Reconstruction of the ECM while simultaneously supplying GFs or cytokines is thus an attractive strategy to promote wound healing.
Natural biomaterials
Two biomaterial groups are commonly used for GF and cytokine release, categorized as either natural or synthetic polymers. This review will concentrate on biomaterials made up partly with natural polymers, as they have been established to stimulate wound healing. 86 Natural biomaterials possess inherent advantages such as being nontoxic, susceptible to cell-triggered proteolytic degradation and natural remodeling, and able to present ligands to cells. 87 Natural wound biomaterials are composed of either polysaccharides, such as chitosan, alginate, glycosaminoglycans (GAGs) and cellulose; or proteins, such as collagen, gelatin, and fibrin (Table 2). 88 The most utilized subsets are collagen, hyaluronate/hyaluronic acid (HA), and chitosan due to their low immunogenicity, biocompatibility, and biodegradability. These macromolecules are typically used to form hydrogels, composed of 3D hydrophilic polymeric network that simulates ECM and absorb large amounts of fluids. 89
Details of natural polymers commonly used for growth factor and cytokine delivery
ECM, extracellular matrix; GA, glutaraldehyde; GAG, glycosaminoglycan; TG, transglutiminase.
Numerous hydrogel delivery systems have been explored for wound healing applications, the most common of which being chitosan. Chitosan, derived from the alkaline deacetylation of chitin, is a linear polysaccharide consisting of (1,4)-linked 2-amino-deoxy-β-
Natural biomaterial delivery systems evaluated for cutaneous wound and scarring indications
CBD, collagen-binding domain; TFA, trifluoroacetic acid.
Another commonly used natural polymer is alginate, an algae or bacteria-derived polysaccharide, composed of a linear copolymer of homopolymeric blocks of 1,4-linked β-
Another commonly used polysaccharide is HA. HA is a linear, nonsulfated GAG composed of repeated units of glucoronic acid and N-acetylglucosamine. HA has important biological functions, as it is the main nonprotein component of ECM and contributes to elastoviscosity, hydration, and cellular function. 99 HA has been used for selected wound delivery systems (Tables 3 and 4), with conjugation of FGF-2 to an amine-modified HA, coupled with oxidized heparin, used to produce a HA-heparin hydrogel, with increased GF stability and activity. 100
Composite biomaterial delivery systems evaluated for cutaneous wound and scarring indications
CMC, carboxymethylcellulose; EUP, galacturonic acid-containing polysaccharide; NP, nanoparticle; PCL, polycaprolactone; PEGDA, poly(ethylene glycol) diacrylate; PVA, poly(vinyl alcohol); SF, silk fibroid.
Combination therapies evaluated for cutaneous wound and scarring indications
EGT, exuberant granulation tissue formation; HBD, heparin-binding domain; PAAm, polyacrylamide; PDMS, polydimethylsiloxane; PEG, poly(ethylene glycol); PEO, poly(ethylene oxide); PEtU, polyetherurethane; PLGA, poly(lactic-co-glycolic acid); PlGF, placental growth factor; STZ, streptozotocin.
Heparin is another commonly used linear polysaccharide and is composed of a complex heterogeneous mixture of highly sulfated repeating disaccharide units, consisting of an uronic acid (
Collagen, the most abundant ECM protein, has garnered much interest for biomedical applications. Collagen fibers can sustain mechanical stress, support different cell types, and function as anchors for various GFs and cytokines. 103 Collagen is classified into type I to XXVIII types, among these type I is the most utilized. Much research has been reported on collagen constructs for GF and cytokine release for wound healing applications (Tables 3–5). EGF and FGF-2 have been incorporated into denatured collagen sponges. 104,105 Collagen membranes have been loaded with PDGF-ββ, 106 VEGF-A in sulfhydryl-modified scaffolds, 107 and EGF with a scaffold that comprised collagen and elastin. 108
Gelatin-based hydrogels derived from collagen hydrolysis have also been extensively used. GFs or cytokines can be loaded into gelatin-based delivery systems via electrostatic interactions and coupling reactions (Tables 3 and 4). 109 Specific examples include fabrication of gelatin microspheres to deliver FGF-2 and EGF, 110,111 genipin-crosslinked gelatin micropheres incorporating VEGF-A, 112 and gelatin sheets to deliver FGF-2. 113 A sponge composed of electrospun fibers of plant-derived polysaccharide crosslinked using gluteraldehyde (GA) to gelatin was also created to specifically bind PDGF-ββ. 114
Another commonly used biomaterial is fibrin, a structural protein involved in the clotting process that is formed by polymerization of the plasma protein, fibrinogen. Fibrin is the primary component in clots and provides a natural scaffold for infiltrating blood and skin cells and has been extensively investigated as a sealant (Tables 3–5). 115 A fibrin sealant was combined with fibroblasts and PDGF-ββ to support granulation tissue formation, 116 while a fibrin matrix delivering keratinocytes and EGF was used to enhance reepithelialization. 117
Biomaterial delivery system platforms
Naturally based hydrogels are mechanically weak; therefore control of their physicomechanical and biological characteristics is a major drawback. In an attempt to improve their biological performance, researchers have turned to fabrication techniques such as nanoparticle (NP) technology, which includes liposomes, microspheres, and bead formation. Interest in NP research for biomedical purposes relates to their nanoscale dimension, and ability to diffuse across membranes, and carry bioactive agents (Fig. 4). 118 NP composition can differ depending on the source material (Tables 3–5).
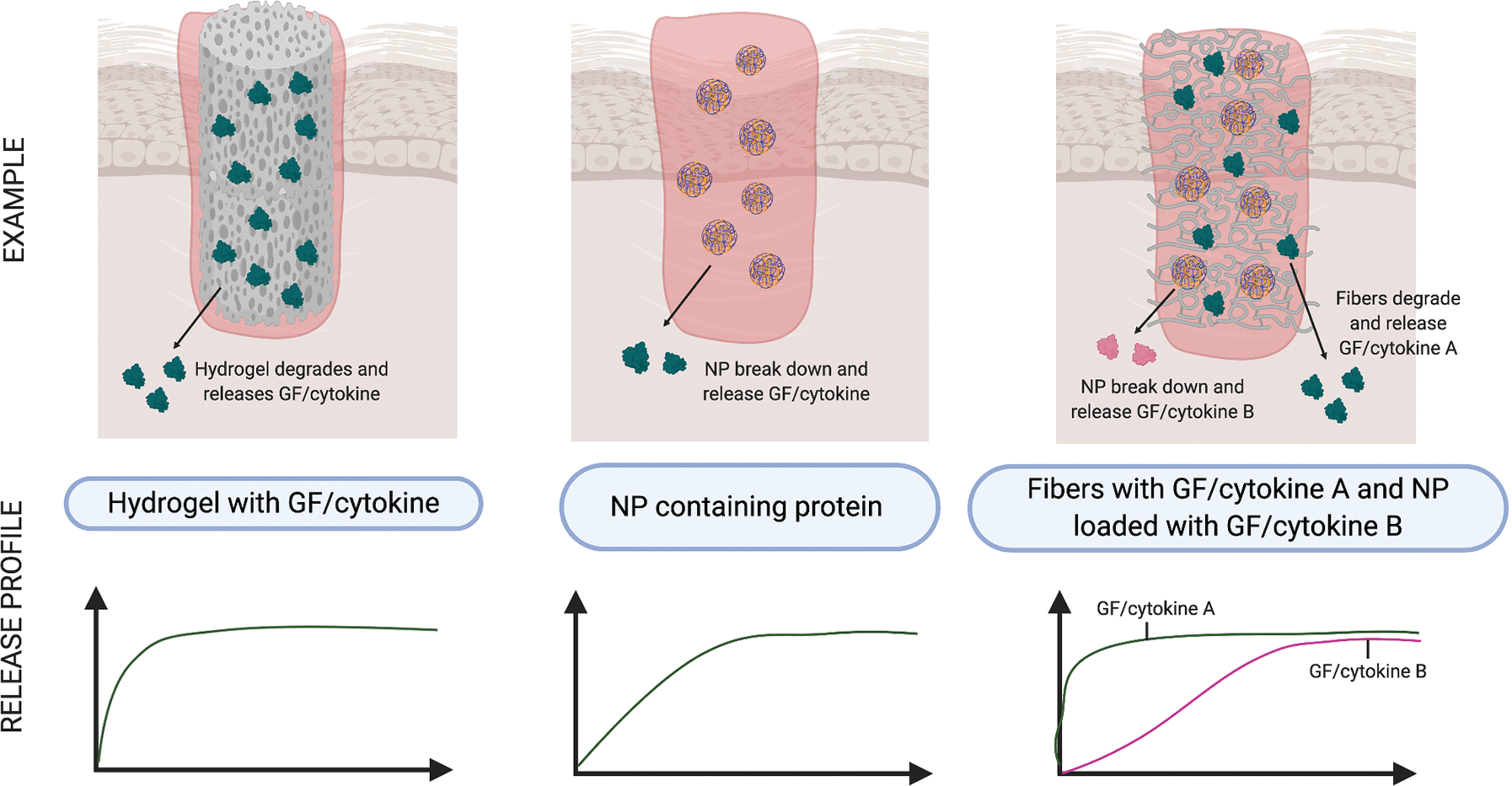
Tailored release of GFs and cytokines to skin wounds using composite biomaterials. Hydrogels containing GF or cytokines allow for rapid diffusion into the wound bed upon absorption of wound fluids (left panel). NPs encapsulating GFs or cytokines allow for sustained release coinciding with degradation of the NP (center panel). Hybrid biomaterials consisting of fibers containing GFs or cytokines and NPs encapsulating GFs or cytokines allows for biphasic release following degradation of the fiber then the NP (right panel). NP, nanoparticle. Color images are available online.
Liposomes, composed of a natural or synthetic phospholipid shell, can entrap hydrophilic GFs and cytokines in their aqueous core. Liposomes are made by introducing a aqueous buffer into a mixture of phospholipid and organic solvent; with the organic solvent then removed by evaporation under reduced pressure. 119 For wound healing applications, lipid NPs have been used to encapsulate EGF. 120,121 Other nanocarriers trialled for GFs and cytokines include those made from proteins or polysaccharides, 122 –126 synthetic polymers, 127 and carbon. 128
Biodegradable microspheres are colloidal systems made using either natural or synthetic materials, such as poly(lactic-co-glycolic acid) (PLGA), gelatin, or other polymer composites (Tables 4 and 5). 129 They are able to load, protect, and control the release of GFs and cytokines (Fig. 4). Passive delivery can occur with diffusion of the protein through the biomaterial as they degrade. As an example, gelatin microspheres can be prepared by creating a gelatin-olive oil emulsion, then adding acetone to induce gelation, followed by crosslinking using GA. The microspheres are then incubated with a protein solution to facilitate absorption. EGF-loaded gelatin microspheres were fabricated using this method. 110
To improve their structural performance, natural biomaterials are used to develop scaffolds, such as sponges, sheets/films, and composite hydrogels (Fig. 4). 129 The simplest method to encapsulate proteins within these is to mix proteins with the polymers before gelation or solidification (Fig. 4 and Tables 3–5). Once encapsulated, the biomaterial can be prepared using phase separation, particulate leaching and solvent casting, gas foaming, freeze drying, and/or melt molding. 130 Collagen sponge fabrication, structural, and protein release rate are influenced by the collagen type, amount, concentration, and the crosslinking agents used. 131 As an example, various crosslinking agents, namely GA, genipin, and 1-ethyl-3-(3-dimethylaminopropyl) carbodiimide, were mixed with a collagen solution, cooled and cast into Teflon molds, with EGF solution added dropwise to the crosslinked sponges. 104
Physically crosslinked hydrogels are formed by molecular self-assembly due to ionic or hydrogen bonds; while chemical gels are formed by covalent bonds. 132 Ionic bonds are made by crosslinking an anionic polymer, such as alginate, with various divalent cations, for example, calcium. These can occur via a number of routes and include photopolymerization, enzyme-induced crosslinking, “click” chemistry, including Michael type-addition, Diels-Alder “click” reaction, oxime formation, and Schiff base formation. 133 GFs and cytokines can be freely incorporated within the network allowing for natural interactions with the polymer, or can be also crosslinked to the polymer (Fig. 4 and Tables 3–5). In an example of Schiff base formation, low molecular weight water-soluble chitosan was functionalized with amino groups using lactose introduced through a condensation reaction. Sodium periodate-treated heparin and FGF-2 solutions were then mixed with the modified chitosan to create a crosslinked hydrogel. 93
Hybrid delivery systems
Current efforts in biomaterial development combine mechanically strong synthetic polymers with the biomemetic natural polymers, so to as to retain tissue biocompatibility, while enhancing the longevity of the scaffold. In parallel, phasic delivery of GFs and cytokines is enabled through their incorporation into nanocarriers, such as liposomes, NPs, or nanofibers embedded within each polymer (Fig. 4 and Tables 4 and 5). For example, FGF-2-loaded alginate microspheres encapsulated in a composite CMC-chitosan and poly(vinyl alcohol) (PVA) hydrogel. 134 In addition, hybrid delivery systems encompassing multiple bioactive components have been investigated (Figs. 4 and 5 and Table 5).
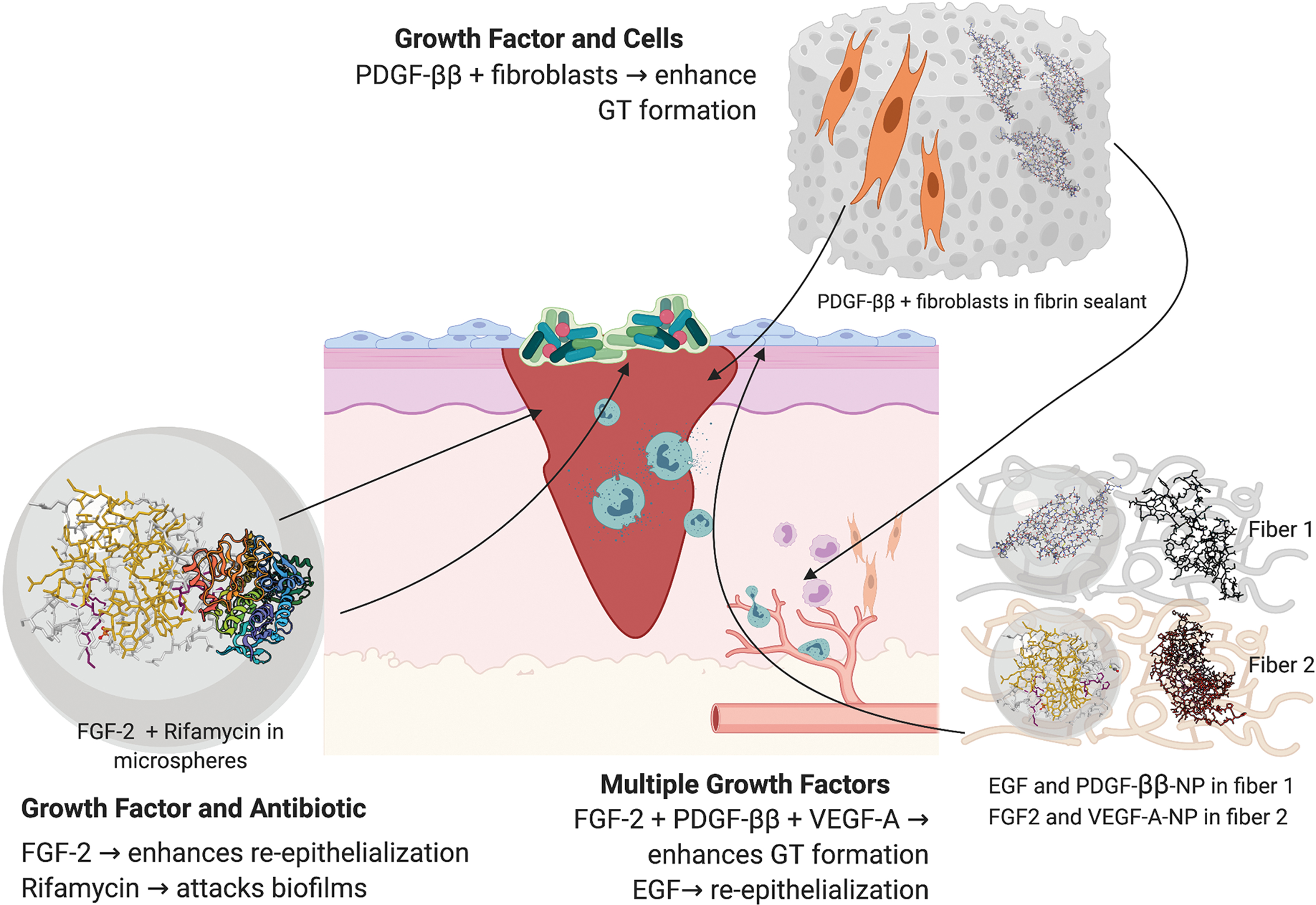
Hybrid biomaterials for delivery of GFs, cytokines, drugs, and/or cells to skin wounds. Examples include delivery of: PDGF-ββ with fibroblasts in a fibrin sealant to enhance GT formation, 116 FGF-2 and rifamycin in alginate microparticles for combined targeting of wound reepithelialization and biofilm infection, 98 and delivery of multiple GFs to enhance both epidermal and dermal repair using collagen nanofibers containing EGF and PDGF-ββ-NPs, and HA nanofibers containing FGF-2 and VEGF-A-NPs. 126 GT, granulation tissue. Color images are available online.
In a simple example, the antibiotic, rifamycin, was suspended in a CaCO3 solution, as was FGF-2, which was then used to solidify alginate droplets prepared using a microfluidics device. 98 But to create a stage-wise release pattern of multiple GFs, a NP-in-nanofiber structure was developed where VEGF-A and PDGF-ββ were individually encapsulated into gelatin NPs, which were mixed with a HA solution containing FGF-2, or a collagen EGF solution, before incorporation within nanofibers. 126 In a further example of this strategy, a composite chitosan-poly(ethylene oxide) (PEO) nanofibrous scaffold was embedded with VEGF, as well as PDGF-ββ-containing NPs. 135
Functionalization of wound biomaterials is becoming a major priority, so as to enhance the integratation of both protein and cellular therapies. Heparin and fibronectin fragments are commonly used to immobilize GFs within various scaffolds (Tables 3–5). 127,136 –138 GFs have also been added to fibrin scaffolds so as to support keratinocyte or fibroblast viability (Table 5). 116,117,139 Integrin-binding peptides, such as arginylglycylaspartic acid, have also been incorporated, along with GFs, to enhance the biocompatability of PEG hydrogels for endothelial progenitor cells. 140 Similarly, conjugation of anti-CD29 antibodies into collagen/PLGA-blended nanofibrous scaffolds was used to enrich the attachment of bone marrow-derived stem cells. 141
Alternative GF and cytokine sources, and methods of delivery, will continue to be explored. This includes the production of biomaterials containing platelet-rich plasma, which is rich in GFs and cytokines and can be derived directly from and administered to the same patient. 142 In another example, biomaterials made from the amniotic membrane from human placenta, including intact or decellularized matrices or hydrogels, naturally produce, or can be enriched with, GFs, cytokines, drugs, or stem cells. 143
In addition, natural and synthetic scaffolds are being used to increase the transfection efficiency of plasmid deoxyribonucleic acid (DNA) encoding angiogenic GFs for administration to ischemic or wounded tissue. 144,145 Stems cells are also being genetically engineered to produce angiogenic GFs and then applied directly, or within scaffolds, to skin wounds. 146,147 As illustrated by these innovations, future therapies will likely be tailored to specific wound environments and encompass multiple functionalized biomaterials, delivering selected biotherapeutic combinations through a range of mechanisms.
Several challenges, however, remain for the translation of these advanced biomaterial delivery systems. For example, more care is needed in the physicochemical characterization and synthesis of the scaffold with regard to polymer arrangement, orientation, and porosity. This must be performed in concert with the nanosystem developed for controlled or multistage release of the appropriate amount of protein, DNA and/or stem cells. Finally, comprehensive preclinical testing is vital to ensure the safety and efficacy of these complex systems before their entering into clinical trials.
Suitability of GF and cytokine delivery systems for cutaneous wound indications
As described, numerous studies have addressed the limitations associated with GF and cytokine therapies, by incorporating proteins into natural biomaterials fabricated into scaffolds, hydrogels, or various size particles. In the clinic, these combination therapies may provide superior efficacy relative to direct protein treatment. This section will evaluate the preclinical evidence as to the therapeutic advantages of GF and cytokine delivery systems for the treatment of ulcers, burns, and scar-prone wounds.
Tailored delivery of GFs and cytokines
Direct GF and cytokine treatments are not compatible with standard wound care, as they require specialized administration and frequent dressing changes. This can increase pain and discomfort for the patient and may prolong the healing process. 10,11,77 Sustained delivery systems could offer improved usability and patient compliance and as such enhance healing responses.
Natural biomaterials have been formulated, which provide for a burst release of proteins that would be compatible with acute wound care (Fig. 4 and Tables 3 and 4). For example, chitosan hydrogels, films, and NPs were shown to release EGF in vitro within 3–48 h. 91,123,124,148,149 Mechanical stimulation of an alginate hydrogel offered pulsatile release of VEGF-A. 96 Controlled release from biomaterials can be provided by degradative enzymes within the wound environment. Release of VEGF-A from gelatin microspheres was shown to be substantially faster in the presence of collagenase, 112 as was FGF-2 from a collagen sponge, 104 and PDGF-ββ from galacturonic acid-containing polysaccharide (EUP) fibers within a gelatin sponge. 114 Hyaluronidase also facilitated the release of FGF-2 from a HA hydrogel. 150 Cleavage domains engineered between protein and biomaterial can also provide for enzyme-triggered release. For example, fusion of an α2-plasmin inhibitor sequence to VEGF-A or FGF-2, crosslinked to fibrin gels or a composite matrix, enabled release by coagulation factor XIIIa. 137,151
Importantly, delivery systems combining different biomaterials and fabrication techniques provide sustained release profiles that may have utility for slow-to-heal wounds (Fig. 4 and Tables 3 and 4). For example, EGF encapsulated in gelatin microspheres within a gelatin sponge provided release over 14 days, compared to the burst release offered by the sponge alone. 152 While cumulative release of VEGF-A from a fibrin hydrogel was observed over 7 days, 151 the incorporation of an anti-VEGF aptamer-fibrinogen macromer into the hydrogel extended release to 15 days. 153
A greater improvement was observed with an HA hydrogel, where the addition of heparin and synthetic polymers, extended the release of FGF-2 from 14 to over 35 days. 150 Chitosan NPs embedded in collagen nanofibers also offered extended release of G-CSF over 14 days. 125 Incorporation of synthetic polymers during fabrication presents another approach to extending delivery kinetics, as demonstrated by the encapsulation of FGF-2 in a polycaprolactone (PCL) microsphere within a composite chitosan/gelatin/PVA hydrogel, which provided protein release beyond 25 days. 154 These findings indicate that composite biomaterials offer the greatest delivery time-span, which may provide greatest compatibility with the care of chronic wounds.
Tailored delivery of GFs, cytokines, drugs, and/or cells
Impaired and excessive healing are exasperated by a range of factors, which suggests that future interventions will require a combinatorial approach, involving therapeutic proteins, drugs, and cells. Delivery systems can thus be designed to provide the benefit of an ECM with GFs and cytokines, while addressing other local factors that may limit their efficacy.
A number of studies have evaluated natural and composite biomaterials for the delivery of two or more GFs or cytokines to skin wounds (Fig. 5 and Table 5). A collagen membrane was developed to deliver EGF and FGF-2 over a 28-day period. 155 Proangiogenic factors, FGF-2 and VEGF-A, were combined in fibrin sealant, composite fibrin or chitosan scaffolds, and PLGA NPs in a composite fibrin sealant, offering cumulative release of both factors over 8 days. 127,138,156 A chitosan/PEO nanofiber system provided immediate release of VEGF-A, but extended release of PDGF-ββ beyond 7.5 days through its incorporation in PLGA NPs. 135 A multifactor delivery system encompassed collagen fibers releasing FGF-2 and VEGF-A NPs over 5 and 25 days, respectively, with HA fibers eluting EGF- and PDGF-ββ-NPs also over 25 days. 126 These tailored release systems allow for greater GF and cytokine control of wound progression through the phases of healing.
Other studies have evaluated natural and composite biomaterials for the delivery of GFs or cytokines with antibiotics (Fig. 5 and Table 5). A chitosan/polyacrylamide hydrogel was developed to deliver EGF along with piperacillin–tazobactam, showing release of the antibiotic within 10 h, and cumulative release of the EGF over 10 days. 157 VEGF-A-loaded PLGA microspheres within a chitosan HA hydrogel containing vancomycin showed cumulative release of the antibiotic and protein over 7 and 20 days, respectively. 158 As previously mentioned, biomaterials are also capable of delivering skin cells in parallel with GFs and cytokines (Fig. 5 and Table 5), so as to enhance both cell viability and healing responses. This includes fibroblasts embedded with PDGF-ββ in a fibrin sealant 116 and keratinocytes delivered with EGF in a fibrin matrix. 117 These findings give support to the concept of multifactorial delivery systems as wound therapeutics.
Retention and proteolytic protection of GFs and cytokines
The wound environment is harsh on directly applied proteins due to excess production of proteases, in particular, plasmin, MMPs, elastases, and bacterial proteases. 14 Biomaterials that offer proteolytic protection would therefore allow more physiologically relevant doses to be administered. In providing this protection, biomaterials will also aid the retention of the GFs and cytokines within the wound, thus preventing their systemic distribution and risk of inducing malignancy or immunogenicity.
While the GF and cytokine release profiles from biomaterials are often evaluated in vitro, they are rarely conducted in vivo or in a proteolytic environment (Tables 3–5). Most studies that evaluate release kinetics have done so in vitro using standard buffers. Physiologically relevant additions have included MMP-containing serum 97 or culture medium. 98,100,105,153 Protection of GFs in biomaterials has also been demonstrated in the presence of a serine protease, savinase, 124 and in wound fluid. 120
Limited studies have directly evaluated protein release from biomaterials within animal wounds. But FGF-2 released from gelatin sheets within diabetic mouse wounds was shown to be stable for 7 days, 113 EUP-fibers within a gelatin sponge sequestered PDGF-ββ in murine excisional wounds, 114 while liposome-delivered EGF persisted within rat incisional wounds for 5 days. 121
Although wound and plasma analyses in treated animals revealed release of GFs or cytokines from the biomaterial, 113,121 none of the studies reviewed examined the systemic distribution of these proteins. In addition, there were no attempts to detect antibody production in response to short- or long-term exposure to the biomaterial(s), or to the GFs and cytokines delivered. Further analyses are thus needed to determine whether biomaterials do indeed provide protection and retention of GF and cytokines within the wound bed.
Structural support for GF and cytokine action
A limitation of GF and cytokine therapies is that their action is dependent on ECM interactions, which in clinical scenarios, can exhibit altered structure and function. 8,159 Natural biomaterials that mimic the ECM could synergize with GFs and cytokines providing spatial cues to direct the migration and proliferation of skin cells into the wound bed.
Of the many GFs and cytokines delivery systems developed, only a few have been directly assessed for their biocompatibility, and ability to support skin cell attachment, migration, or proliferation in vitro (Tables 3–5). Toxicity of G-CSF-loaded chitosan NPs in a collagen/PCL hydrogel was evaluated for mesenchymal cells, 125 as was a chitosan/gelatin/PVA hydrogel containing FGF-2 for fibroblasts. 154 An alginate/chitosan hydrogel containing EGF was incubated with red blood cells, demonstrating clotting and hemostatic potential. 124 Cell attachment was demonstrated to a collagen hydrogel containing FGF-2 using adipocytes, 160 and to a chitosan/gelatin hydrogel containing diamond NPs encapsulating VEGF-A using endothelial cells. 128 Martino et al., went further still to show that a fibrin matrix containing VEGF-A+PDGF-ββ supported both endothelial cell and smooth muscle cell function in vitro. 161
More extensive analysis of the differential effects of biomaterials on skin cells has been performed for some delivery systems (Tables 3–5). The addition of EGF-loaded microspheres to a gelatin hydrogel-coated collagen matrix enhanced keratinocyte proliferation, while fibroblast proliferation was greatest on collagen matrix in the absence of gelatin. 152 The addition of anti-VEGF aptamer-fibrinogen macromers, so as to sequester VEGF-A, accelerated the growth of endothelial cells and keratinocytes, but not fibroblasts, within a fibrin hydrogel. 153
Collagen scaffolds incorporating EGF also enhanced the proliferation of keratinocytes and fibroblasts, with coculture of the cells maintained in vitro for 21 days. 108 This study went further to show that these cell types were also detected within the EGF scaffold in rat excisional wounds after 3 days. By contrast, a FGF-2-incorporated chitosan hydrogel was not retained in diabetic mouse wounds, as reepithelialization of the wound occurred beneath the biomaterial. 92 As these studies have been limited, it is not yet clear which biomaterials provide the best support for the growth of different skin layers. Furthermore, the impact of different biomaterials on inflammation, which can contribute to chronicity and scarring, has not been compared. In addition, it is not evident which biomaterials integrate into the wound, as opposed to providing topical GF and cytokine delivery.
GF and cytokine delivery systems as wound healing treatments
GF and cytokine therapies have been underwhelming with regard to their efficacy as therapeutics for chronic ulcers, traumatic burns, and scar-prone surgical incisions. One reason proposed for their clinical failings has been an inadequate translation from preclinical models. 162,163 These difficulties can be explained by preferential use of rodent models, when there is poor concordance between wound healing in rodents with that in humans, with rodent skin healing mostly by contraction, and human skin by reepithelialization. Larger animals offer greater similarity to human healing processes, but are less commonly used due to logistics.
There is also a discordance between the healing parameters evaluated in animal models, relative to humans. Treatment success in humans is evaluated as the time till complete wound closure. While this measurement is possible in porcine wound models, it is less clear in rodents due to skin contraction. In addition, while wound inflammation, vascularization, reepithelialization, and scarring can be observed macroscopically to a certain extent in humans and pigs, the size of rodent wounds compromises these measures, meaning that wound biopsies must be taken from euthanized animals to facilitate each type and stage of wound analysis. Thus large numbers of animals are required to fully assess phasic wound responses to a given treatment.
The translatability of biomaterial-based GF and cytokine delivery systems to clinical use may therefore still be dependent on the preclinical models, in which they are tested, the healing parameters evaluated in them, and the number of animals that can be cost-effectively sourced for a given study.
The efficacy of GF and cytokine delivery systems has been evaluated in acute surgical wounds in the rat. A chitosan hydrogel encapsulating PDGF-ββ and VEGF-A improved the oxidative status of sutured incisions relative to hydrogel-treated controls. 164 Most GF and cytokine delivery systems have, however, been evaluated in acute full-thickness excisional wounds, either in the rat or mouse.
For example, FGF-2 and rifamycin-laden alginate microparticles accelerated healing relative to untreated excisional wounds in rats, with enhanced granulation tissue formation and angiogenesis relative to untreated controls. 98 Chitosan NPs delivering G-CSF or GM-CSF, embedded in a range of natural and synthetic fibers, induced faster healing in rats relative to empty biomaterial controls, with increased reepithelialization and granulation tissue formation observed. 123,125 Composite chitosan scaffolds delivering FGF-2 microspheres, FGF-2 with VEGF-A, and VEGF-A with PDGF-ββ-NPs induced healing of rat wounds to a greater extent than their scaffold controls, 135,138,154 with increases in wound contraction, granulation tissue formation, vascularization, and fibrosis reported.
Collagen-based systems incorporating EGF or FGF-2 also enhanced rat wound healing relative to their delivery controls. 108,160 EGF-loaded gelatin microspheres, delivered in either a gelatin sponge or collagen matrix, also accelerated healing of excisional wounds in rats when compared to the vehicles lacking EGF microspheres. 111,152
Fibrin hydrogels and matrices have instead been tested in mouse wounds, particularly for their capacity to delivery VEGF-A-encapsulated macromers or EGF with keratinocytes. 117,153 Faster healing was observed relative to individual components, with increased vascularization and collagen production, and epidermal regeneration observed for the macromer and EGF cell therapy, respectively. Incorporation of VEGF-A and FGF-2 into a fibrin sealant also sustained vascularization of a collagen matrix in a mouse wound model. 156 A rabbit excisional wound model has also been used to assess delivery of PDGF-ββ and fibroblasts using fibrin sealant, 116 with faster healing and granulation tissue formation observed after a single administration relative to sealant with or without keratinocytes.
It is important to note that across these studies, there is very little consistency in how wound healing was measured, and at which time-point each parameter was examined. As an example, Dehkordi et al., calculated the percentage wound closure, every second day for 13 days, 123 while Dogan et al., compared wound areas at day 7 and 14, postwounding. 111 Vijayan et al., evaluated histological parameters every 5 days from day 5 to 20, postwounding, 138 while Wilcke et al., examined wound vascularization after 2 and 4 weeks. 156 It is important that a consensus be reached regarding the most appropriate types and time frame for these analyses, so as to enable accurate comparisons between different therapeutics.
To make the rodent model more clinically relevant, a splinted full-thickness excisional wound model has been created, in which a silicon or steel ring is sutured to the skin around the wound, so as to limit contraction, thus enabling macroscopic measurements of reepithelialization. 165 This model was used in rats to examine the efficacy of a collagen membrane for dual delivery of EGF and FGF-7 over an extended course of 4 weeks. 155 This dual GF therapy led to faster wound healing, with improved vascularization and epidermal regeneration relative to the membrane with or without the individual GFs.
A splinted wound model was also used in mice to evaluate VEGF-A NPs in a composite fibrin-HA hydrogel and showed faster healing and a more mature vasculature than compared to wounds treated with the hydrogel alone. 122 This model was further adapted by inoculation of splinted rat wounds with Staphylococcus aureus derived from a patient with infected skin, so as to greater mimic an infected human ulcer. 158 The infected wound model was then used to test the efficacy of VEGF-A-loaded PLGA microspheres incorporated in a chitosan-HA hydrogel containing vancomycin, with a single treatment leading to faster healing and increased granulation tissue and vasculature formation relative to the hydrogel with and without each active component. 158
GF and cytokine delivery systems have also been evaluated in rodent burn models, with most common method of application being scald or thermal rod burns. 91,120,134,148 Scald burns offer the greatest translational relevance, while thermal rod burns provide greater control of burn depth. Partial-thickness scald burn in rats showed faster healing after daily treatment with alginate/chitosan hydrogel containing EGF relative to the hydrogel and EGF controls. 148 EGF delivered daily using a chitosan gel also increased reepithelialization of partial-thickness thermal burn in rats relative to hydrogel and EGF controls. 91 In an equivalent mouse model, liposomes encompassing FGF-2 within a silk fibroid core lead to faster healing and vascularization than FGF-2–treated control burns. 120 FGF-2-laden alginate/chitosan microspheres in a PVA hydrogel also accelerated healing in full-thickness thermal burns in rats when compared to hydrogel with or without FGF-2 controls. 134
A few studies have utilized chemical ablation of pancreatic beta cells through streptozotocin (STZ) injection to model type 1 diabetes in rats, so as to delay healing of full-thickness excisional wounds. 163 Delivery of EGF in chitosan NPs within a chitosan hydrogel to STZ-induced diabetic rat wounds showed faster healing relative to the hydrogel with or without EGF. 124 The combination therapy of collagen nanofibers containing EGF and PDGF-ββ-NPs, with HA nanofibers containing FGF-2 and VEGF-A-NPs, was also tested in STZ-induced diabetic rats, showing faster wound healing and vasculature improvements relative to the fibers with or without FGF-2 and EGF. 126
Leptin-deficient db/db mice, a monogenic model of diabetes exhibiting extreme obesity, are also commonly used, as full-thickness excisional wounds in these mice exhibit a substantial delay in repair processes. 163 Chitosan fabrications delivering FGF-2 led to faster healing and increased granulation tissue formation and vascularization of the diabetic wounds when compared to the chitosan alone. 92,166 Composite fibrin matrices delivering FGF-2 and placental growth factor (PlGF), VEGF-A and PDGF-ββ, or FGF-2/VEGF-A-laden NPs, also accelerated healing in the db/db mouse, with increased epidermal, granulation tissue, and vasculature formation than in wounds treated with the matrices alone. 127,137,161 Gelatin-based systems incorporating FGF-2 also enhanced healing of diabetic mice, increasing wound reepithelialization and vascularization relative to gelatin controls. 110,113
It should, however, be noted that these animals do not accurately represent type 2 diabetes, which is a polygenic metabolic disorder that can occur in the absence of obesity. It might be more relevant to therefore investigate GF and cytokine delivery systems in TALLYHO/JngJ or NONcNZO10/LtJ mice. 167 These mice better represent the polygenic nature of type 2 diabetes and exhibit impaired wound reepithelialization and granulation tissue formation, which in the case of NONcNZO10/LtJ mice is accelerated by topical administration of FGF-1. 168,169
Other studies utilized rodent models with local tissue hypoxia to assess the efficacy of delivery systems aimed at treating ulcers with vascular deficiency. In the skin flap model, an ischemic gradient was created in a flap of skin by severing the supplying blood vessels, and delivery of VEGF-A with a fibrin hydrogel reduced skin necrosis and increase vascularization in mice relative to the sealant control. 151 In the hind limb model, ischemia was created by ligation of the femoral artery, and here too, delivery of VEGF-A with an alginate or fibrin hydrogel, or FGF-2 in a chitosan gel, enhanced vascularization of mouse and rat limbs relative to biomaterial controls, respectively. 93,96,151 Delivery of PDGF-ββ engineered with a collagen-binding domain with a collagen membrane to an ischemic version of the rabbit excisional wound model showed treatment at the time of wounding led to faster reepithelialization and vascularization than with the membrane or native PDGF-ββ. 106
Only two studies have evaluated GF and cytokine delivery systems in nonrodent models. A pig excisional wound model was used to test a chitosan film containing EGF and showed that daily administration accelerated healing relative to wounds treated with the film only. 149 A viral GF and cytokine combination, VEGF-E and vIL-10, was administered in a collagen/HA hydrogel to limb wounds of horses, showing increased reepithelialization than with hydrogel alone. 170 The porcine and equine models better represent the rate of healing for human ulcers, with closure achieved on average after 27 and 50 days, respectively.
Most GF and cytokine delivery systems described above are tailored to specific aspects of the healing response, that is, angiogenesis, while very few aim to progress the wound through all phases of healing. Therapeutic success will likely depend on suppression of infection and inflammation, relief of hypoxia, and the promotion of granulation tissue and epidermal repair to facilitate wound closure. This will require the phasic delivery of multiple bioactives using composite biomaterial and nanodelivery systems. It is evident that the most accurate assessment of these therapeutics will be in slow-to-heal, potentially ischemic, wounds in diabetic rodents or large animals that provide the best representation of human ulcers.
GF and cytokine delivery systems as antiscar treatments
The impact of GF and delivery systems on cutaneous scarring has not been extensively investigated. This may, in part, be due to the high use of models that utilize rodents, which heal with minimal scarring due to the lack of tension provided by their loose skin. 171 In rodents, the minimal scar size and hair regeneration around the wound limit the use of macroscopic assessments such as scar scales. 74 Most preclinical studies have, therefore, evaluated the impact of the delivery system on scarring processes and the quality of skin repair using histological analyses.
Excess inflammation is a hallmark of excessive healing. Neutrophil and macrophage levels were investigated in wounds treated with fibrin hydrogels delivering VEGF-A-encapsulated macromers, showing no increase relative to untreated wounds. 153 Scarring is also characterized by a lack of remodeling, with impairments in the maturation of the blood vessels, differentiation of the epidermis and reorganization of collagen fibers.
FGF-2 and FGF-7 within a collagen membrane, and VEGF-A macromers in a fibrin hydrogel, were reported to increase epidermal differentiation in healed wounds in rodents, as evidenced by increased suprabasal and squamous cell production of keratin 10 and involucrin and pronounced hair follicle formation. 117,153,155
Blood vessel maturation is measured by evaluating the association of endothelial cells with pericytes. Vessel maturity was increased following treatment of rodent wounds with collagen membrane containing FGF-2 and FGF-7, fibrin-HA hydrogel containing VEGF-A-NPs, and fibrin matrix delivering FGF-2 and PlGF. 122,137,155 In addition, more mature blood vessels were noted following treatment of rat burns with FGF-2-laden microspheres in a composite alginate sponge. 134
Collagen remodeling, with collagen I to III ratios and thickening fibers organized in a “basket-weave” pattern approaching that of unwounded skin, was also observed following burns in rats treated with liposomes encapsulating FGF-2. 120 Similarly EGF-loaded liposomes increased the tensile strength of healed incisions relative to liposome and saline controls. 121 These analyses show greater translatability, and similar histological and biomechanical analyses are performed in human scar therapy trials. 74
As rodents heal with very little fibrosis or scarring, large animal models may better represent scarring in humans. For example, skin wounds in the Duroc pig produce raised, hyperpigmented scars with collagen organization similar to that in hypertrophic scars. 172 By contrast, horses are the only animal, other than humans, to naturally develop fibroproliferative skin lesions known as exuberant granulation tissue (EGT), which are reminiscent of keloids. 173 Administration of a viral GF and cytokine to equine limb wounds before bandaging led to faster resolution of EGT formation, with greater blood vessel integrity observed relative to the hydrogel alone. 170 To our knowledge, no GF or cytokine delivery systems have been trialled in the porcine scarring model.
These findings indicate that scar prevention is also dependent on timely progression through the phases of the wound healing response. Once again therapies must suppress inflammation, relieve hypoxia, and control granulation tissue and epidermal repair so as to support scar remodeling. This will also likely require the phasic delivery of multiple bioactives using composite biomaterial and nanodelivery systems. Further research is, however, required as to the impact of different biomaterials on scarring processes, as well as optimization of dosage and timing of GF and cytokine delivery. Assessment of these parameters would ideally be conducted in large animals that exhibit excessive scarring more like hypertrophic scars or keloids in human.
Summary
Healing of the skin requires phasic production of GFs and cytokines, and their dysregulation can lead to impaired or excessive healing. Direct administration of GFs and cytokines to skin ulcers, burns, and surgical incisions increased closure rates and improved scar aesthetics, but underwhelming results mean that only three products have progressed to clinical use. To address the limitations associated with direct protein administration, delivery systems have been developed from natural and composite biomaterials. The findings from this review indicate that biomaterials can provide differential GF and cytokine release kinetics, and extend protein half-life in the presence of proteinases or wound fluid. The incorporation of GFs or cytokines into a biomaterial, in most instances, also increased the reparative functionality of that biomaterial, particularly in acute wounds in rodents. There was, however, limited evidence to suggest that the delivery systems would offer greater efficacy as wound or scar therapeutics, as most studies do not compare the product to direct administration of the same proteins. It was also unclear which GF or cytokine delivery system could, or should, be tailored for specific wound indications, as only a few were assessed in models that exhibit impaired or excessive healing, and no comparisons between different natural or synthetic biomaterials were made. In addition, no studies examined the retention of GFs or cytokines within the biomaterial or the wound site nor did they evaluate the immunogenicity for delivery system components. As such, there is insufficient evidence to conclude whether GF and cytokine delivery systems will offer greater clinical success than the direct therapies that were originally trialled.
To increase the likelihood of GF and cytokine delivery systems succeeding in clinical trials, it is important that they are rigorously tested at the preclinical stage (Fig. 6). Interventions must be carefully designed for a specific wound indication, and phase of healing at which the healing response has stalled. Appropriate biomaterials, proteins, drugs, and cells must then be chosen to address that wound complication. The fabrication method(s) selected must allow for both tailored delivery of the GFs, cytokines, and drugs and physicomechanical support for delivered or invading cells. Delivery systems should then be assessed in vitro, for their ability to protect GFs and cytokines within a proteolytic environment, prevent systemic protein leakage and the induction of immunogenicity, and to support the migration, growth, and differentiation of their skin cell targets.
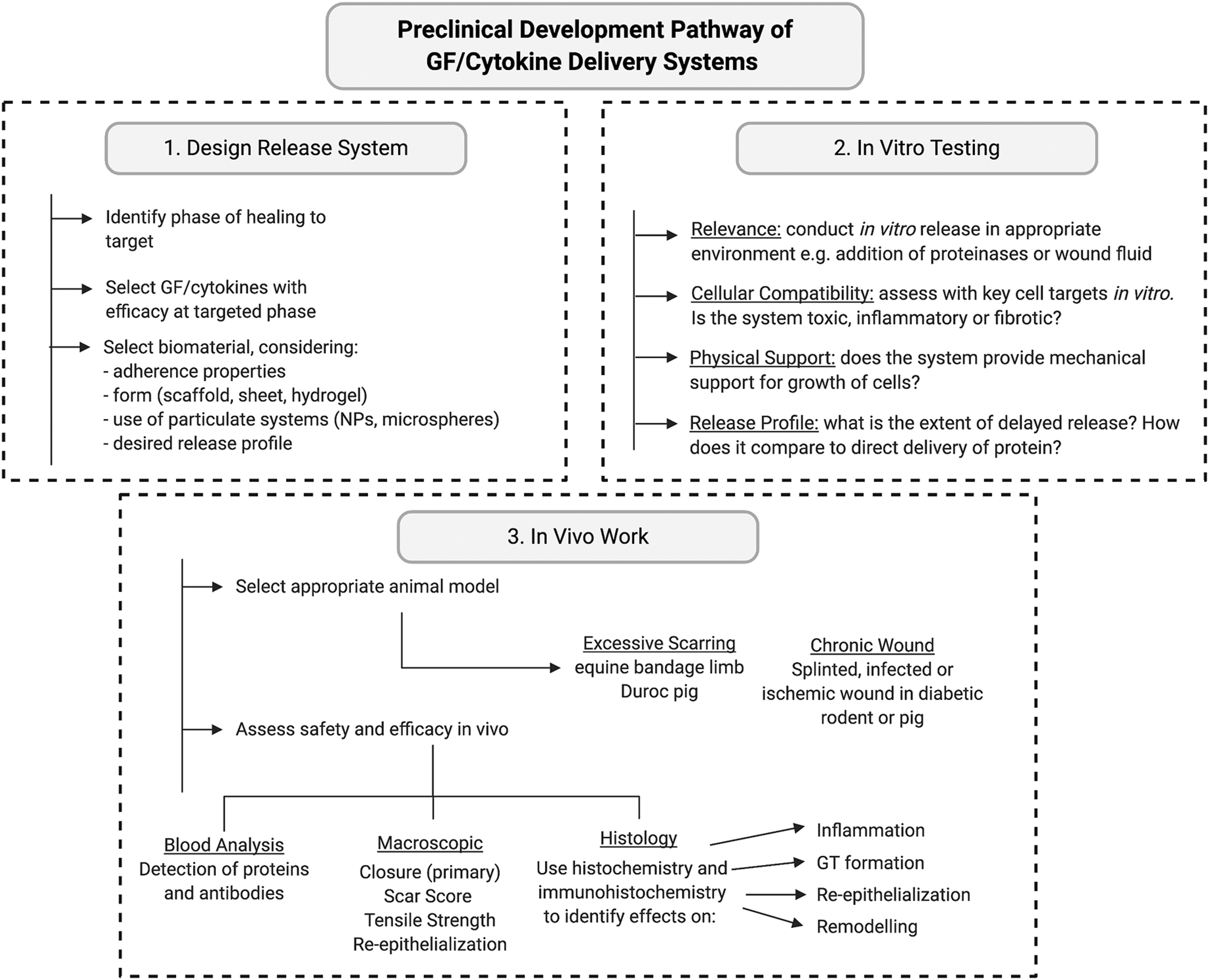
Proposed preclinical development pathway for biomaterial-based GF and cytokine delivery systems. Pathway includes three stages: design of the release system with regard to selection of wound indication, desired GF and/or cytokine release profile, biomaterial, and fabrication methods (1), in vitro testing in proteolytic environments and with skin cells (2) and in vivo work in clinically relevant chronic wound or excessive scarring models with macroscopic and histological readouts of healing and scarring outcomes along with blood analysis of protein and antibody levels (3). Note that testing should be conducted in comparison to direct protein administration.
These parameters should then be confirmed in vivo within the context of a healing or nonhealing wound. Acute wound models in rodents can allow for mechanistic insight into the effects of the biomaterial and GF/cytokine on key healing processes such as inflammation, reepithelialization, vascularization, and collagen remodeling. It is, however, important that parameters such as complete closure, scar esthetics, and tensile strength, that are translatable to human wounds, also be assessed. Healing should also be evaluated using standardized units of measure and at agreed upon stages of healing. These analyses are most appropriate in cutaneous wounds that exhibit delayed healing, such as in the diabetic rodent, or those with exasperated scarring, such as the Duroc pig.
Should a delivery system prove more efficacious than direct administration of a GF or cytokine when following a preclinical development plan such as that proposed, the findings may then indeed translate to human trials. These products will likely offer greater efficacy, safety, and patentability than direct protein administration. But they will likely be more costly to produce and may face more regulatory hurdles. Whether the clinical benefit generated by such combination therapies will be sufficient to justify the costs associated with their development, and the clinical testing for products that contain more than one bioactive component, will still need to be answered. Future success with GF and cytokine delivery systems as wound healing and antiscarring therapeutics will, however, still depend on advancements in clinical trial design and regulatory requirements, with regard to science-based patient selection, and quality of life-based healing outcomes.
Take Home Messages
GFs and cytokines are critical regulators of skin repair, and their dysregulation can contribute to wound chronicity and excessive scarring.
Direct administration of recombinant GFs and cytokines to skin ulcers, burns, and surgical incisions has led to underwhelming results in human trials.
Delivery systems made from natural biomaterials offer sustained GF and cytokine release, proteolytic protection, and a matrix supportive of wound repair processes.
Delivery systems have proved efficacious in promoting healing of acute, diabetic, and ischemic wounds in rodent models, but have rarely been tested in large animal models or for antiscarring action nor compared to direct protein therapy or other delivery systems.
Further preclinical and clinical testing is required to determine whether GF and cytokine delivery systems will be more efficacious and safer than direct protein administration, and if so, for which skin wound indications.
Footnotes
Acknowledgments and Funding Sources
This work was supported by the Health Research Council of New Zealand (13/774, 17/649) and New Zealand Lottery Health Research (2019-98814).
Author Disclosure and Ghost Writing
The authors do not have any commercial or financial conflicts of interests to declare. The named authors wrote this article and no ghostwriters were used.
About the Authors
Supplementary Material
Supplementary Table S1
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.