
Abstract
Significance:
The worldwide estimate of burns requiring medical attention each year is 11 million. Each year in the United States, ∼486,000 burn injuries receive medical attention, including 40,000 hospitalizations. Scars resulting from burns can be disfiguring and impair functions. The development of prophylactic drugs for cutaneous scarring could improve the outcomes for burns, traumatic lacerations (>6 million/year treated in U.S. emergency rooms), and surgical incisions (∼250 million/year worldwide). Antiscar pharmaceuticals have been estimated to have a market of $12 billion.
Recent Advances:
Many small molecules, cells, proteins/polypeptides, and nucleic acids have mitigated scarring in animal studies and clinical trials, but none have received Food and Drug Administration (FDA) approval yet.
Critical Issues:
The development of antiscar pharmaceuticals involves the identification of the proper dose, frequency of application, and window of administration postwounding for the indicated wound. Risks of infection and impaired healing must be considered. Scar outcome needs to be evaluated after scars have matured.
Future Directions:
Once treatments have demonstrated safety and efficacy in rodent and/or rabbit and porcine wound models, human testing can begin, such as on artificially created wounds on healthy subjects and on bilateral-surgical wounds, comparing treatments versus vehicle controls on intrapatient-matched wounds, before testing on separate cohorts of patients. Given the progress made in the past 20 years, FDA-approved drugs for improving scar outcomes may be expected.

SCOPE AND SIGNIFICANCE
Burn injuries often result in disabling scars, 1 –5 but few experimental scar prophylactics have been tested in clinical trials on burns. Rather, most have been tested on other types of human wounds. This is likely owing to the greater challenge of treating burns that heal by secondary intention and the larger market for treating surgically closed wounds. Nonetheless, drugs that mitigate surgically closed wound scarring may also prove useful for mitigating burn scars. Here we present a survey of preclinical and clinical studies of experimental pharmaceuticals tested for scar prophylaxis, with an emphasis on burns.
TRANSLATIONAL RELEVANCE
Antiscar treatments can be applied at different points during wound healing. Early post-wound treatments in animal models have suppressed tissue-damaging inflammation, improved healing, and reduced scarring, but risks for infection and delayed healing are present, especially for open wounds healed by secondary intention. Treatments during the proliferation phase can suppress inflammation and fibrotic processes and may reduce scarring, but delayed healing and concave scars are risks. Finally, treatments during the remodeling phase can inhibit fibrotic processes but they may have limited effectiveness. Thus, challenges include the proper dosing regimen and the management of risks for infection and impaired healing.
CLINICAL RELEVANCE
Deep partial-thickness (PT) burns that are not grafted typically heal with scars that cause physical and psychological impairments and costly long-term health care. 6 The same is true of full-thickness (FT) burns that are grafted. Once scars form, treatments for reducing them are only partially effective. 7 Patients would benefit from pharmaceutical prophylactics for cutaneous scarring. 8
BACKGROUND
The need for scar prophylactic therapeutics
Worldwide, burns requiring medical attention are estimated to be 11 million yearly. 1 In the United States, ∼486,000 burn injuries receive medical attention yearly, including 40,000 hospitalizations. 2 Deep burns produce scars that require costly care, are disfiguring, and impair functions.
Deep dermal burns with prolonged inflammation are at high risk for developing hypertrophic scars (HTSs) that are red, raised, and uncomfortable, and may involve contractures that limit function and disfigurements that produce psychological problems. As much as half or more of deep PT burn wounds, regardless of the treatment plan, develop hypertrophic scarring and contracture. 9 Once formed, scars can only be treated with corrective surgery or other modalities that are minimally effective. 10 –16
Although keeping closed wounds covered and moist, such as with silicone sheeting, and reducing their tension, such as with tapes or devices, can improve scar outcomes, these methods are not practical for wounds under tension on mobile tissue that are at high risk for scarring and contracture.
Pharmaceuticals that mitigate burn scarring could also potentially be used on traumatic lacerations (> 6 million/year treated in U.S. emergency rooms) and surgical incisions (∼250 million/year worldwide). 3,4 Approximately 90 million procedures in the United States and Europe yearly could benefit from scar reduction therapy. 17 The market for pharmaceuticals for reducing skin scarring has been estimated to be $12 billion. 5 Consistent with this large market, intellectual property development in the field of scarring is active (Fig. 1).
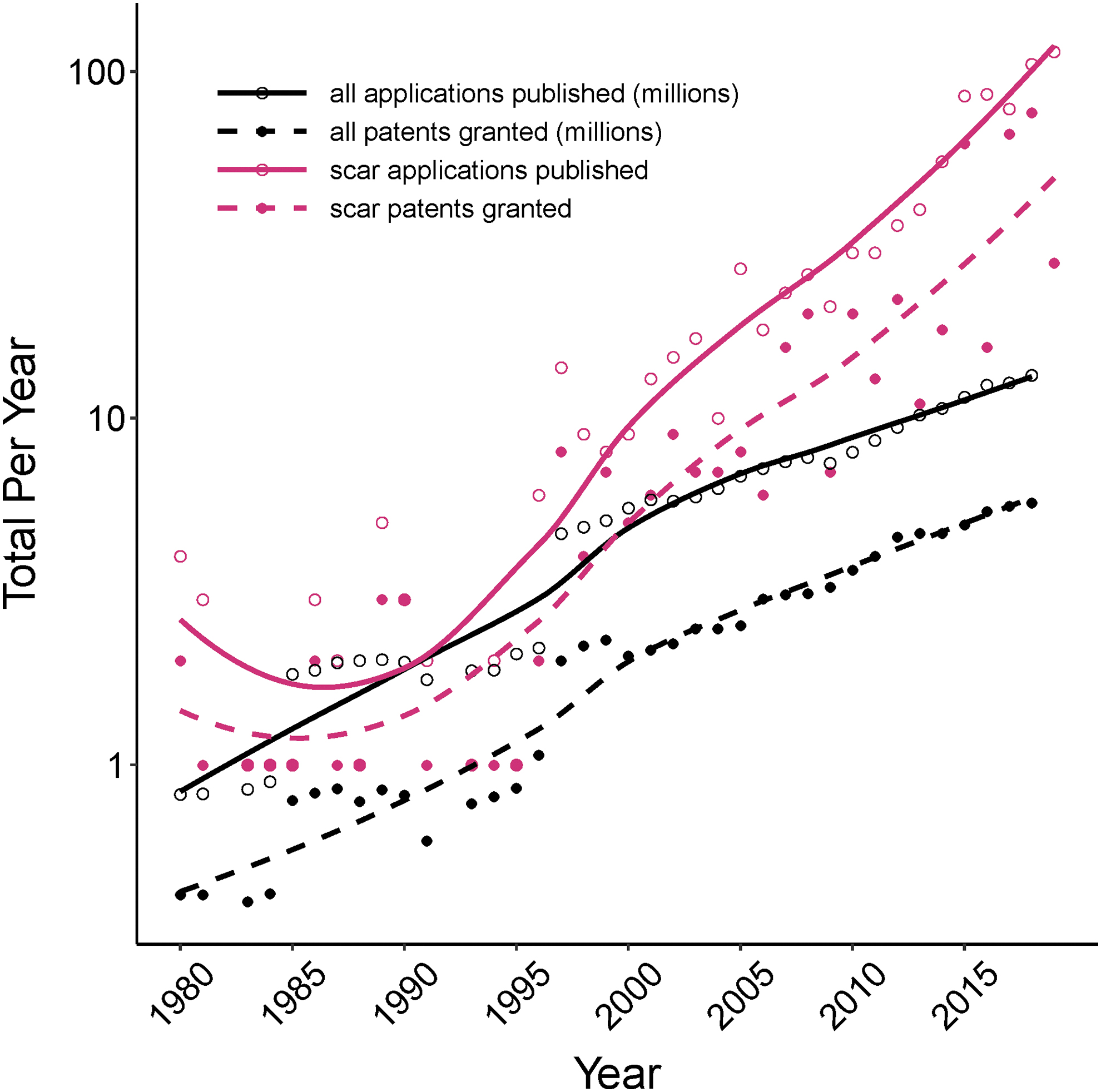
Patents in the field of scar outpace patents in all fields. Patent applications and patents granted in all fields worldwide (solid and dashed black lines, respectively) are shown in millions (WIPO IP Statistics Data Center, Direct and PCT System, updated October 2019). Also shown are worldwide patent applications and patents granted in the field of scarring (solid and dashed red lines, respectively); that is, “scar” or “fibrosis” as title words and “skin,” “cutaneous,” or “dermis” as abstract words in a Google Patents search.
Preclinical studies of scar prophylactic pharmaceuticals
Scar prophylactics have been studied predominantly in murine, rabbit, and porcine models. Numerous and diverse treatments applied at various times postwounding in these models have mitigated contraction, dermal thickness, and other scar parameters. To compile preclinical scar prophylactic studies, we surveyed the literature from 2000 to 2020 (March), which identified 65 studies of ∼55 molecular entities, categorized as small molecules, cells, proteins/polypeptides, and nucleic acids. The great majority of these pharmaceutical and biopharmaceutical treatments—in studies using murine (26), rabbit ear (24), and porcine (14) models—evidenced effectiveness in reducing scars: 14 of 19 for burns, 34 of 34 for excisions, 2 of 2 for incisions, 1 of 1 for ear punch wound, 3 of 3 for splinted excision wounds, and 5 of 5 for wounds closed under tension (Fig. 2, solid circles).
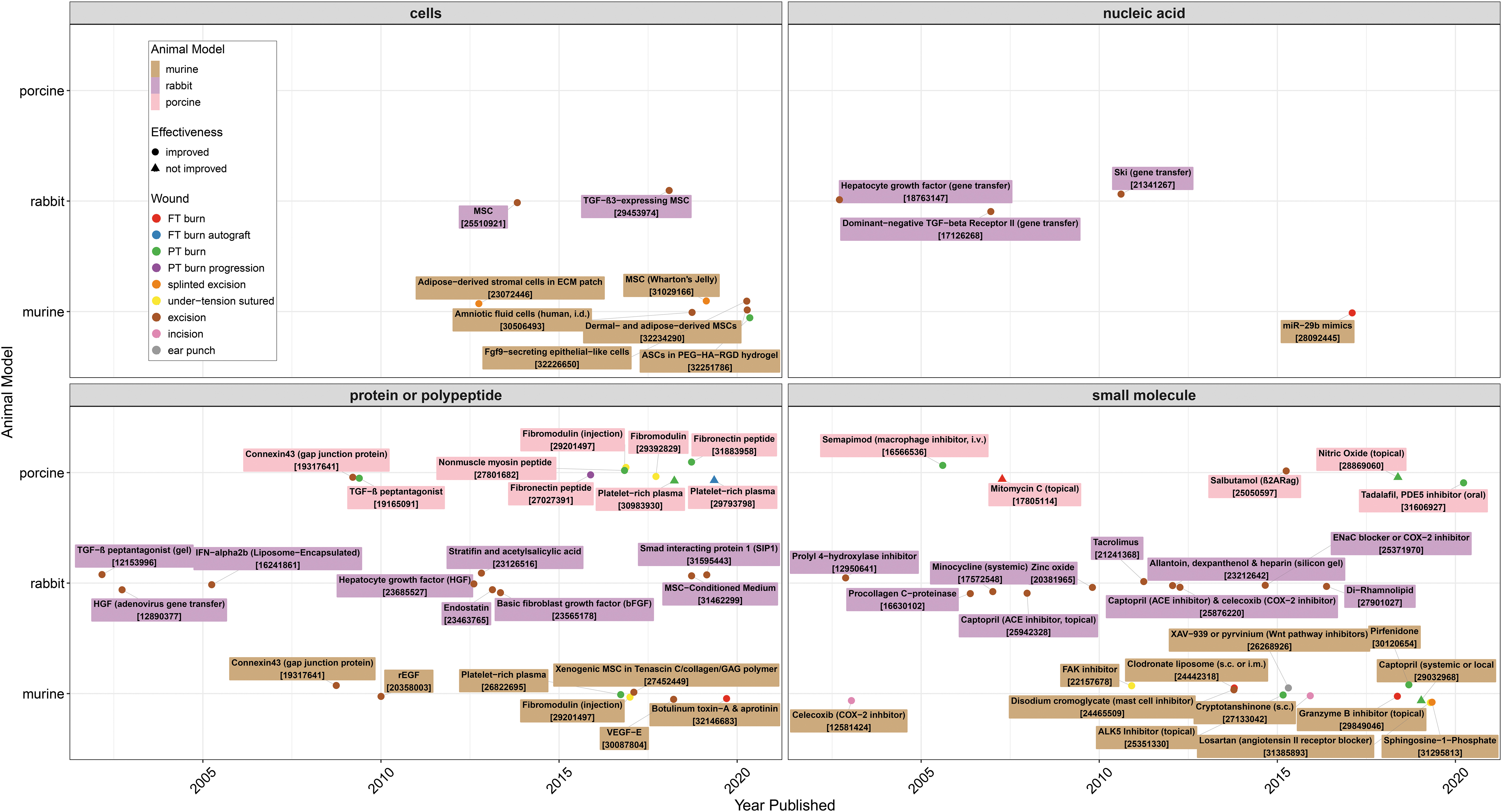
Animal model studies of prophylactic treatments for scarring. PubMed was searched using Boolean terms (Supplementary Data) that resulted in >500 records (in English) from 2000 to 2020 that were manually curated to include studies of pharmaceutical or biopharmaceutical scar prophylactics (PMID numbers are shown in brackets 18 –80 ). The R package easyPubMed was used to facilitate the literature survey. 81 PMID, PubMed identifier.
Porcine wound models, the closest models of human wound healing, are typically used as the final animal efficacy test before human trials. The porcine studies shown in Fig. 2 that reported efficacy in reducing scarring (10 of 14 studies) are summarized in Fig. 3, categorized by the type of wound on which the pharmaceutical was tested (i.e., burn or other wounds) and showing the route of administration (intravenous [i.v.], topical gel, oral, or intradermal [i.d.]), the outcomes, and the schedule of dosing.
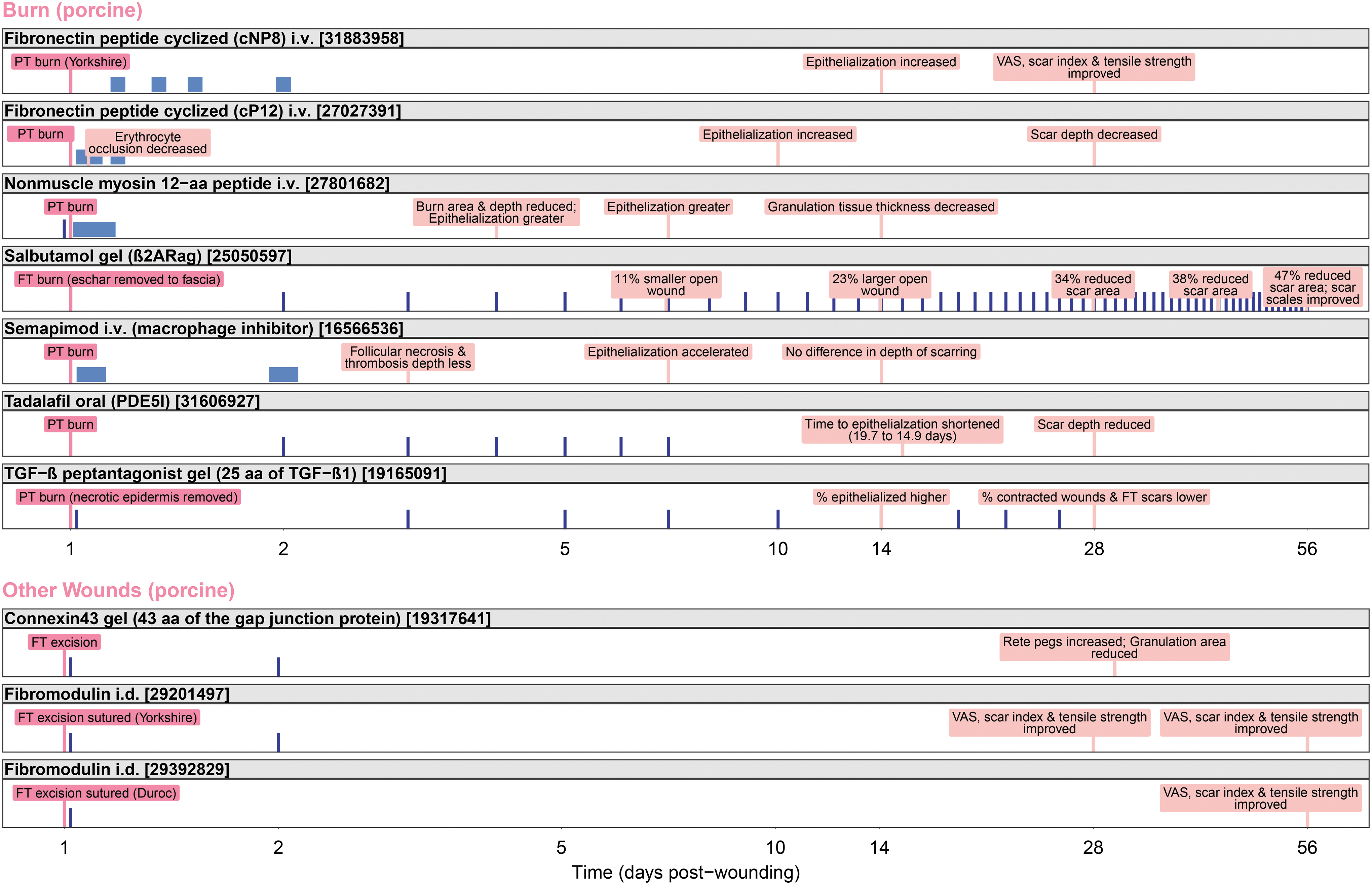
Porcine studies of scar prophylactic treatments showing efficacy: routes of administration, time courses, and scar outcomes for burns and other wounds. Wounds are pink, treatment times are dark blue, and the outcomes are salmon. The light blue rectangles indicate i.v. infusions. PMID numbers are shown in brackets. Days postwounding with wounding on day 1 are shown on a log10 scale. i.v., intravenous.
For burns, the treatments include peptides (nonmuscle myosin, 60 transforming growth factor [TGF]-β, 66 and the fibronectin-derived cNP8 and cP12 21,49 ) and small molecules (salbutamol, 82 semapimod, 67 and tadalafil 29 ). Among the peptides, the route of administration varied: i.v. infusions were used for fibronectin and nonmuscle myosin peptides, and topical gel was used for TGF-β peptantagonist. 66 Among the small molecules, the route of administration also varied: topical gel for salbutamol, i.v. infusion for semapimod, and oral for tadalafil. Along with the varied routes of administration, the frequency and duration of dosing also varied (Fig. 3, top panel).
The i.v. treatments (semapimod, 67 fibronectin peptides, 21,49 and nonmuscle myosin peptide 60 ) were only administered over the first 2 days postburn. Such short-term i.v. administration of the fibronectin-derived peptide cP12 (starting as late as 4 h postburn) to PT burns reduced the occlusion of blood vessels by erythrocyte clumps by at least 50%, which was associated with faster healing (day 10) and reduced scarring (day 28). 21 In addition, daily oral tadalafil (vasodilator) in the first week postburn accelerated epithelialization (from average of day 19.7 to 14.9) and reduced scar depth (day 28). Overall, these short-term treatments appeared to reduce burn wound progression that was largely associated with improved scar measures (except for semapimod), including reduced granulation thickness for nonmuscle myosin (day 14), less scar depth for tadalafil (day 28), and less scar depth or better scar quality and tensile strength for the fibronectin peptides (day 28).
The longer term topical gel burn treatments—salbutamol (β2 adrenergic receptor agonist) daily for 2 months 42 or TGF-β peptantagonist 66 every other day for 1 week, then twice weekly for 3 weeks—also reduced scar area, thickness, appearance, and/or contraction at 1 or 2 months postinjury.
For FT excision wounds, as with burn wounds, treatments on only days 1–2 postinjury reduced scarring: fibromodulin protein (has roles in wound healing) injected intradermally or connexin43 (gap junction protein) peptide gel applied topically improved scarring at 1–2 months postinjury. For connexin43 gel, two topical applications on postsurgical days 1 and 2 increased rete pegs and reduced granulation tissue area on day 30. 27 For fibromodulin, two i.d. injections, one at the time of surgery and another on day 2, into the edges of excision wounds that were then sutured under tension, improved the appearance and tensile strength of scars on days 28 and 56 (Yorkshire pig). 79 In addition, only a single i.d. injection with fibromodulin at the time of surgery improved scar appearance and tensile strength 2 months later (Duroc Pig) 37 (Fig. 3, bottom panel).
Overall, the porcine studies suggest that treatments of either PT burns or FT excision wounds (either open or sutured closed under tension)—for only 2 days postinjury—can decrease progression and/or reduce inflammation and fibrosis, which translates, 1 or 2 months later, into reduced scarring. In addition, treatments with gels over a longer term, daily, or every other day, can inhibit scarring, as for salbutamol (FT burns) or TGF-β peptantagonist (PT burns).
Clinical studies of scar prophylactic pharmaceuticals
Burns
Interventional clinical trials for treating burn injuries to mitigate scarring listed on
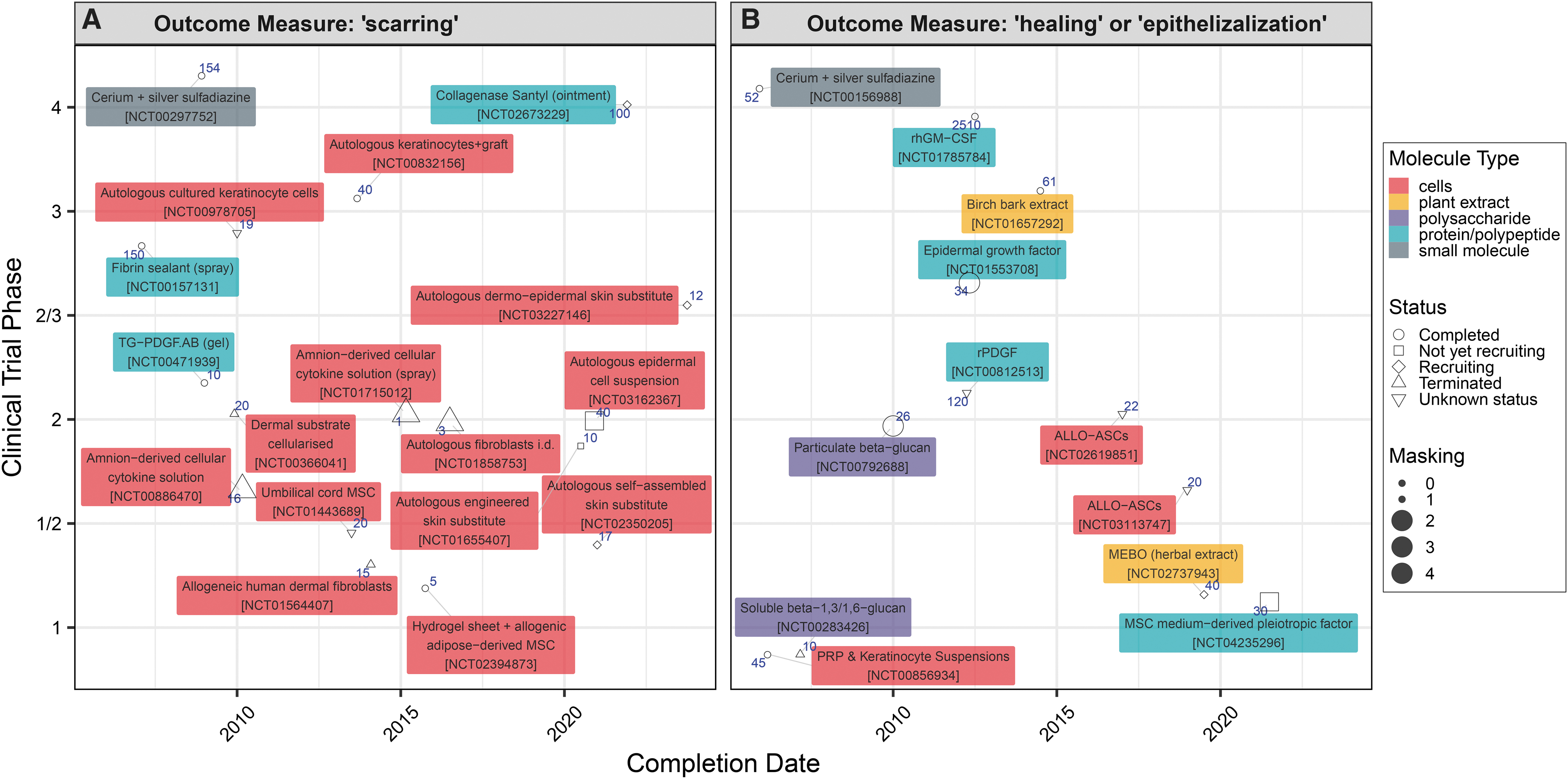
Studies listed in
Another 12 studies also have “burns” as the Condition and “drug” or “biological” as the Intervention but instead of “scarring” have “healing,” “epithelialization,” or “reepithelialization” as the outcome measure (Fig. 4B).
Of the 29 studies listed in Fig. 4A and B, 22 have a study design that is either “Open Label” (62%) or single-blinded (i.e., masked; see symbols). Only 7 studies were double-blinded or more. This may be owing to the noticeable effects of the treatments on the wounds (e.g., collagenase and cerium nitrate) or the characteristics of the treatment make it difficult to design a suitable placebo (e.g., autologous cultured keratinocytes or dermo-epidermal skin substitute).
Overall, the 29 interventional studies in Fig. 4A and B for treating burns to mitigate scarring or accelerate epithelialization tested different molecular classes: 16 cell based (55%), 2 plant extract (6%), 2 polysaccharides (6%), 7 protein/polypeptides (24%), and 2 small molecules (6%).
Skin wounds in general
Given the few burn scar prophylactic clinical trials, to identify trials of prophylactics against scarring of skin wounds in general (including burns),

Studies listed in
Next, publications in PubMed were searched using keywords related to clinical trials, skin, and scar, which yielded 940 publications. These were manually curated to retain trials of scar prophylactic treatments (i.e., excluding studies of existing HTSs and keloids), which were then organized by wound type—burn, sutured surgical incision, or artificial incision—and by whether the treatments and controls were compared between cohorts (interpatient) or between matching areas of each patient (intrapatient) (Fig. 6). Most of these treatments (13 of 18) are proteins or polypeptides; fewer are cell, nucleic acid, or small molecule treatments (2, 1, and 2, respectively).
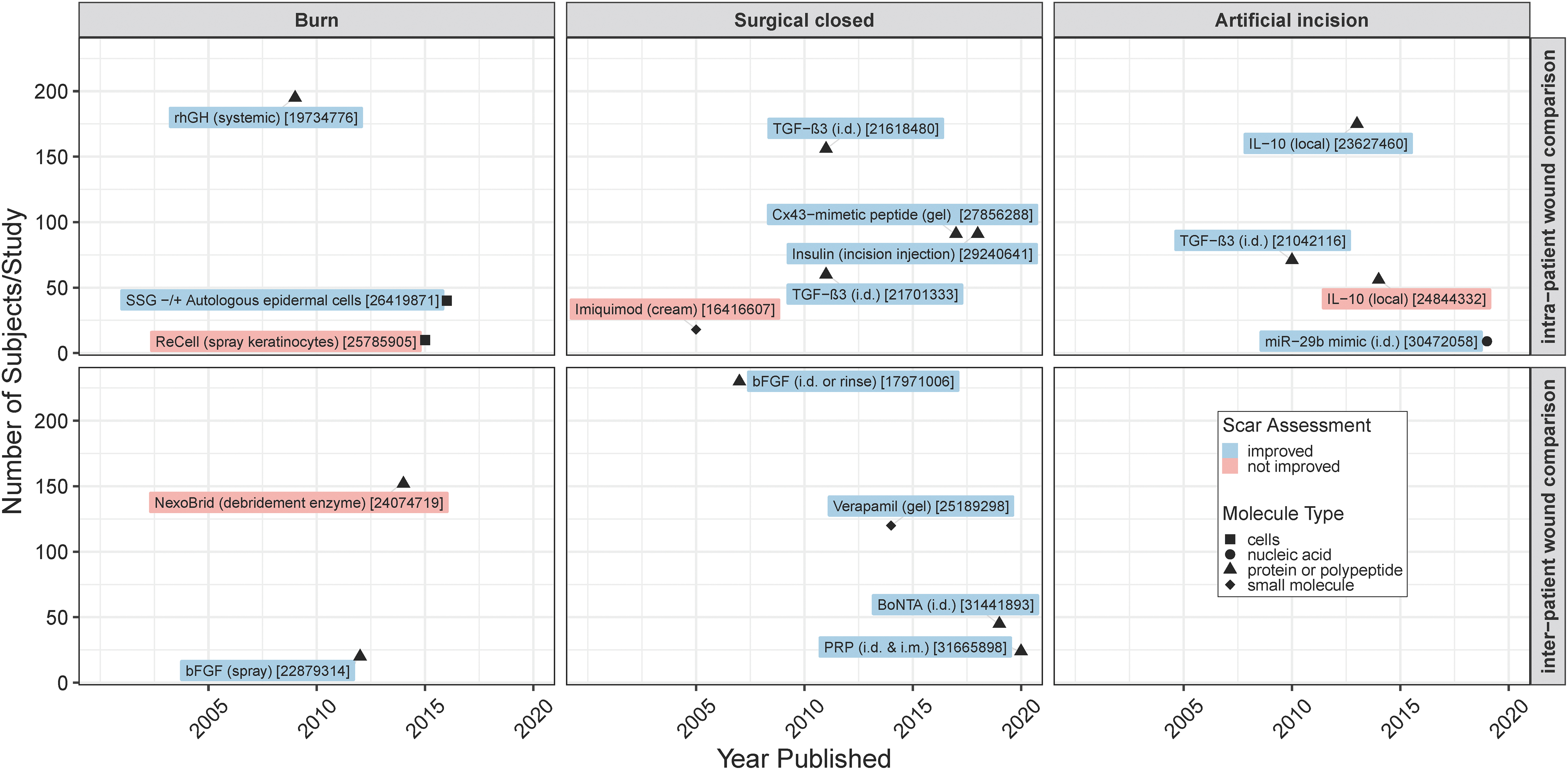
Human skin scar prophylaxis clinical study summary. PubMed was searched for scar[Title/Abstract] AND (skin[Title/Abstract] OR dermis[Title/Abstract] OR cutaneous[Title/Abstract]) AND (“Clinical Study” OR “Clinical Trial” OR “Phase I” OR “Phase II” OR “Phase III” OR “Phase IV” OR subjects OR participants), which resulted in 940 records in English from 2000 to 2020 (April) that were manually curated. PMID numbers are shown in brackets. 82 –101
From the 18 publications of clinical trials given in Fig. 6, the 14 that showed efficacy in reducing scarring (or indicators of scarring) are given in Fig. 7, organized by wound type (i.e., burn, surgical closed, or artificial incision) and showing the route of administration, the time course of treatments, and outcomes. Only 3 of these 14 studies were performed on burns. Most were surgical closed wounds (8) or artificial incision wounds made on healthy volunteers (3).
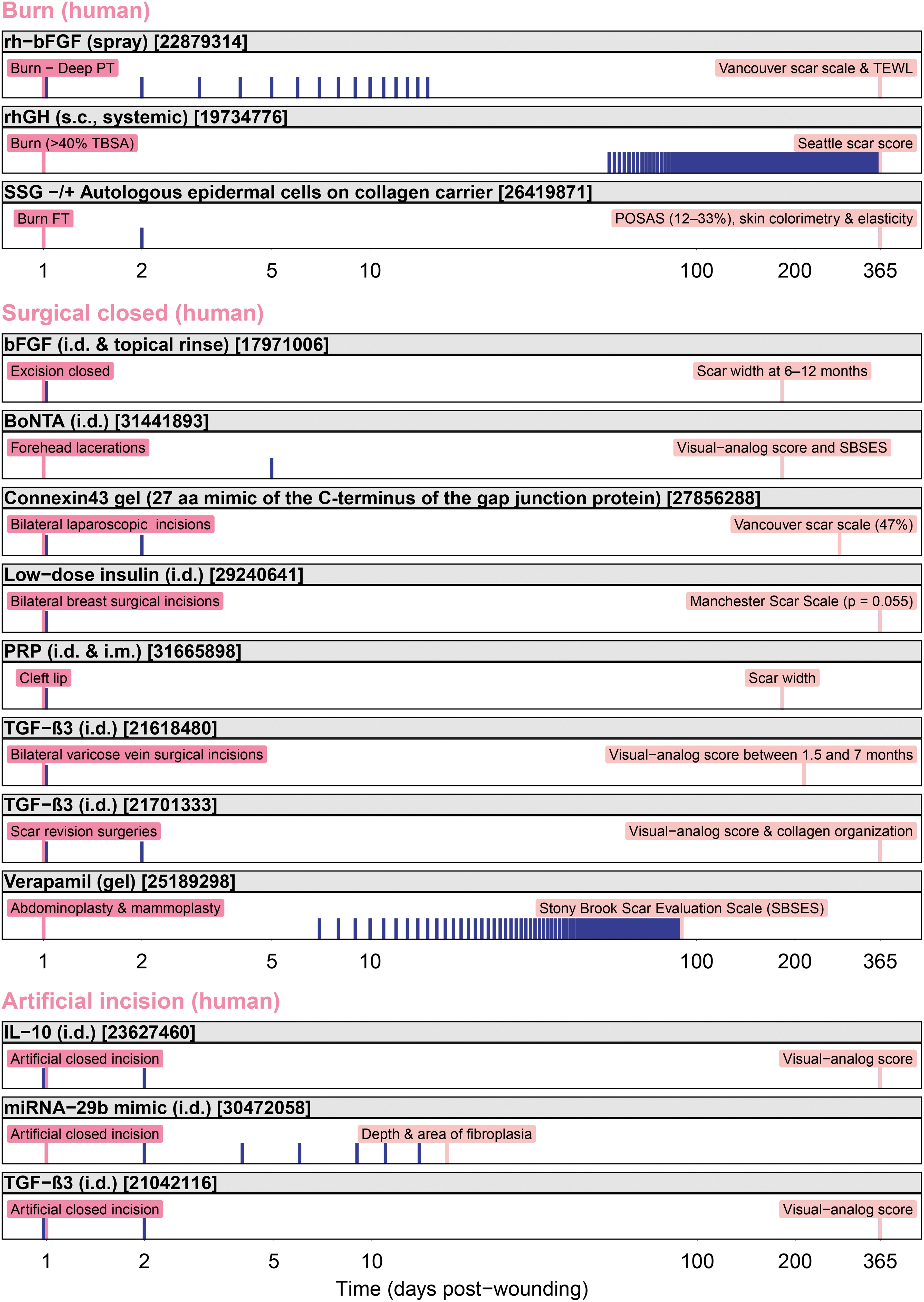
Human skin scar prophylaxis: time course and outcomes of pharmaceutical treatments that showed efficacy. Wounds are pink, treatment times are blue, and the outcomes are salmon colored. PMID numbers are shown in brackets. rhGH was administered to patients after hospital discharge (an average of 7.5 weeks after burn) until 12 months. Days postwounding (wounding on day 1) are shown on a log10 scale. rhGH, recombinant human growth hormone.
For burns of >40% total body surface area, recombinant growth hormone (rhGH) treatment systemically (subcutaneous) starting at the time of hospital discharge and continuing for 1 year, improved scar appearance. 84 For FT burns requiring autologous split-thickness skin graft (SSG), the addition of autologous epidermal cells on a collagen carrier to meshed SSG improved scar appearance and elasticity at 12 months. 88 For deep PT burns, daily topical application of recombinant human basic fibroblast growth factor (rh-bFGF) in the form of a spray until complete healing improved scar appearance and transepithelial water loss (TEWL) at 12 months. 91
For surgical incisions, most treatments were i.d. injections administered once at the time of surgery (bFGF, 97 low-dose insulin, 90 platelet-rich plasma [PRP], 98 and TGF-β 96 ) or twice, during surgery, and the following day (TGF-β). 100 Additionally, botulinum toxin type A (BoNTA) was injected on day 5 for forehead lacerations. 95 And, connexin43 (gap junction protein) peptide gel was applied to incisions immediately after bilateral laparoscopic surgery and the following day, 89 whereas verapamil (calcium channel blocker) gel was applied topically twice daily starting at day 7 and continuing for 90 days for treating abdominoplasty and mammoplasty incisions. 83
For artificial incisions made on healthy volunteers, the pharmaceuticals were also injected intradermally at the time of surgery and on day 2 (interleukin [IL]-10 and TGF-β), 85,93 or six times over 2 weeks (miRNA-29b mimic). 87
Overall, there have been fewer successful trials of scar prophylactics for burns (3) than incisions (11, surgical or artificial) (Fig. 7). For deep PT burns, the improvement of scar appearance and TEWL resulting from rh-bFGF applied daily until complete healing may have been owing to accelerated healing. 102 For severely burned children, the scar quality improvement provided by systemically administered rhGH has been speculated to be because of enhanced wound repair or lowered hypermetabolism that diminishes scar blood flow. The improvement in scarring provided by autologous epidermal cells overlaid onto meshed SSG is likely owing to earlier coverage.
For wounds closed by primary intention (surgical or artificial), i.d. injections (bFGF, BoNTA, low-dose insulin, PRP, TGF-β3, IL-10, and miRNA-29b) soon after wounding improved scar appearance at 6 months to 1 year. Additionally, topical application of verapamil gel twice daily from days 7 to 90 improved visual scar assessment at 3 months. And, the connexin43 gel applied only twice improved visual assessment of scarring at 9 months.
The mechanisms of the antiscar activity of these pharmaceuticals are not completely understood but may involve reducing stress on the wound (BoNTA), reducing inflammation and fibrogenesis (TGF-β3, PRP, connexin43 peptide, IL-10, miRNA-29b, and verapamil), and providing growth factors (bFGF, rhGH, and insulin).
DISCUSSION
Pharmaceutical prophylaxis of scarring has been an active research field for more than 20 years. 8,103,104 The drug most well-studied was TGF-β3 (Avotermin) that was evaluated in 13 clinical trials before it failed to meet its primary endpoint in a pivotal phase III trial. 8 Thus, no drug for preventing scars has been approved by the Food and Drug Administration (FDA). Nonetheless, in preclinical and clinical studies, many treatments have mitigated scarring, offering hope for a treatment being clinically available in the not too distant future—despite the fact that no wound healing drug has been approved in 23 years, since FDA approved Becaplermin (Regranex; i.e., recombinant human platelet-derived growth factor) for diabetic foot ulcers. 105 Someday with continued work, tissue regenerative therapies may become a reality (300 years spanned the first attempts at blood transfusions and their routine use 106 ).
Protein/polypeptide and cell therapies (Figs. 4 and 5) have been the most frequently evaluated classes of therapeutics for scar prophylaxis in clinical trials. Fewer trials, only 20%, have evaluated small molecules, although small molecules can have a cost benefit, especially small molecules that have been approved for other indications and can be repurposed. Nonetheless, proteins/polypeptides (e.g., connexin43 peptide, 89 low-dose insulin, 90 TGF-β3, 85,96,100 IL-1093) and cells, 88 despite their costly manufacture, may prove feasible antiscar therapeutics as they have shown some effectiveness when applied to wounds only on the first and/or second day postinjury.
The first step in the development of a scar prophylactic is the demonstration of effectiveness in models of incision, excision, or burn wounds—such as the rabbit-ear (naturally splinted) wounds, splinted-excision murine wounds, 107 sutured-under-tension murine and porcine wounds, 37,79,108 and/or porcine excision wounds, and so on. After demonstrating effectiveness, preclinical pharmacology and toxicology studies are needed, with the product administered at multiples higher than the anticipated therapeutic dose—using the same route, dosing regimen, and duration of exposure intended for clinical use—to estimate the therapeutic index (toxic dose/effective dose) and to aid in the selection of the initial clinical starting dose. 109 Once these studies demonstrate safety and the IND application to FDA becomes effective, the clinical trials may begin. 109 The first clinical study may be dose-ranging in artificial wounds in healthy subjects, such as incisions or punch biopsies on the inner upper arm 110 or on abdominal skin that is later removed during abdominoplasty surgery. 111 Treatments can also be evaluated on patients' bilateral wounds, such as after laparoscopy or varicose vein, breast, or abdominoplasty surgery—comparing control and experimental treatments within patients. Such within-patient studies can maximize the use of a limited number of study subjects and minimize between-patient variability. However, within-patient comparisons do not allow assessment of systemic safety, and the results of efficacy and safety at the wound site (delayed healing or infection) may be biased by systemic absorption and/or translocation of the experimental treatment.
The clinical evaluation of scar prophylactics has required multiple trials: For example, avotermin (TGF-β3), connective tissue growth factor (CTGF) antisense, and CTGF small interfering RNA were, respectively, tested in 14, 7, and 6 trials that, respectively, enrolled 1246, 291, and 149 patients (as listed on
In developing a scar prophylaxis treatment, the first indication could be for wounds closed by primary intention, such as surgical sites, because the risk of dehiscence and infection should be less than the risks of delayed healing and infection for open wounds such as burns. Once a closed-wound indication receives FDA approval, a follow-on indication could be sought for treating wounds closed by secondary intention (e.g., administering the treatment early postinjury, during healing, and/or after closure).
Our survey of clinical trials in
SUMMARY
Treatments are needed that can be applied to incision wounds or lacerations after closure and to open wounds as they are healing or soon after they have closed, to promote regenerative healing and mitigate pathological scarring.
The development of antiscar treatments, once proof-of-concept studies in rodents or rabbits are completed, involves porcine models with scars assessed after several months as well as good laboratory practice pharmacology and toxicology studies. Clinical studies can then be implemented on artificial wounds on volunteers and/or wounds on patients. Comparisons between bilateral wounds, with one side receiving the treatment and the other side the vehicle control, are most efficient for demonstrating efficacy (although systemic absorption and/or translocation of the experimental product must be considered). However, to establish systemic safety and confirm efficacy, a cohort of patients treated with the product must be compared with cohorts receiving the vehicle control and the standard of care.
Pharmaceuticals that have successfully mitigated scarring in animal models and clinical trials include proteins/polypeptides, cells, nucleic acids, and small molecules. Such drugs need to be validated for clinical effectiveness at 1 year and even longer after injury. Drugs that lessen the scarring of closed incision wounds may potentially lessen the scarring of wounds like burns that heal by secondary intention. Getting FDA approval for the indication of surgical wounds and subsequently for the indication of burns may provide the necessary large first market as the commercialization incentive.
TAKE-HOME MESSAGES
The development of antiscar pharmaceuticals involves identifying the postwounding window of administration and the proper dose and frequency of the treatments for the indicated wound.
Small molecules, cells, nucleic acids, and proteins/polypeptides have mitigated scarring from a variety of wound types in preclinical and clinical studies.
Porcine excision and burn wounds, splinted murine excision wounds, 107 naturally splinted rabbit-ear excision wounds, and murine and porcine sutured-under-tension wounds 37,79,108 are well suited for preclinical testing of pharmaceuticals for prophylaxis against pathological scarring.
In porcine models of burn wounds, treatments only on postburn days 1 or 2 (fibronectin peptides 21,49 and nonmuscle myosin peptide, 60 intravenously) or during week 1 (daily oral tadalafil 29 ), or over the longer term (salbutamol 42 or TGF-β peptantagonist 66 gel), decreased burn progression and/or reduced inflammation and fibrosis, which translated, 1 or 2 months later, into reduced scarring.
In porcine models of excision wounds, treatments on only postinjury days 1 or 2 (fibromodulin i.d. and connexin43 peptide gel) also reduced scar parameters at 1–2 months. Tensile strength of the scar was also improved after fibromodulin treatment.
In clinical trials that assessed surgical or artificial incision scars, short-term treatments on only postinjury days 1 or 2 (bFGF, connexin43 peptide, TGF-β3, IL-10) improved visual assessments of surgical scars at 6 months to 1 year.
For clinical testing, dose-ranging studies can use artificial wounds in healthy subjects, such as incisions or punch biopsies on the inner upper arm 110 or on abdominal skin that is later removed during abdominoplasty surgery. 111 Efficacy of treatments can then be evaluated on patients' bilateral surgical wounds, comparing placebo and treatments intrapatient. However, separate cohorts receiving the treatment or placebo need to be compared to assess safety.
Getting FDA approval first for the indication of surgical wounds and subsequently for the indication of burn wounds may provide the necessary large first market as the commercialization incentive.
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
PD is supported by the U.S. Army Research Laboratory and the U.S. Army Research Office under contract W911NF1310376 to The Geneva Foundation. KPL is an employee of the U.S. Government. The work presented is part of his official duties and is supported in part by the U.S. Army Medical Research and Materiel Command, Combat Casualty Care Research Directorate, Clinical Rehabilitative Medicine Research Directorate, and the Naval Medical Research Center's Advanced Medical Development program (MIPR N3239815MHX040). Title 17 U.S.C. §105 provides that “Copyright protection under this title is not available for any work of the United States Government.” Title 17 U.S.C. §101 defined U.S. Government work as work by a military service member or employee of the U.S. Government as part of that person's official duties. DoD Disclaimer: The views expressed in this article are those of the authors and do not reflect the official policy or position of the U.S. Army Medical Department, Department of the Army, DoD, or the U.S. Government.
AUTHOR DISCLOSURE AND GHOSTWRITING
The authors do not have any commercial or financial conflicts of interest to declare. This article was written exclusively by the authors without ghostwriters.
ABOUT THE AUTHORS
Supplementary Material
Supplementary Data
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.