
Abstract
Significance:
Diabetic foot ulcers (DFUs) are associated with high morbidity, mortality, and health costs. Standard care (SC) associated with nonsurgical offloading is the mainstay treatment for DFUs, but it has high recurrence and infection rates. Metatarsal head resection (MHR) has been proposed as an effective surgical offloading technique for the treatment of plantar neuropathic DFUs, but with no evidence synthesis yet.
Recent Advances:
Based on PRISMA guidelines, a meta-analysis was conducted to assess the efficacy of MHR. Four electronic databases were searched for. Eleven studies met the inclusion criteria with a total of 477 patients (494 feet and 593 neuropathic forefoot ulcers). The studies included three retrospective comparative studies and eight case series.
Critical Issues:
Meta-analytical results of comparative studies on recent noninfected DFUs showed MHR having significantly better rates of healing, time to healing, ulcer recurrence, and infection than SC. Failure to heal, recurrence, and infection rates were 4 times higher in the SC group than in the MHR group, and the amputation rate was two times higher in the SC group than in the MHR group. The outcomes of the meta-analysis of case series on chronic and recalcitrant ulcers treated with MHR were similar.
Future Directions:
Considering the natural history of DFUs treated conservatively and the satisfactory outcomes with a significantly low complication rate of MHR, physicians should consider the use of MHR more often and include this technique in the early management of DFUs.
Scope and Significance:
DFU impose great public health burden around the globe. Standard of care using in-office debridement and topical agents is the usual mainstay of treatment. However, such conservative care is known to result in high rates of ulcer recurrence and complications. In this systematic review, we quantitatively investigate the outcomes of a surgical off-loading technique, the MHR in the treatment of chronic plantar neuropathic wounds.
Translational Relevance:
Many biochemical factors are implicated in the complex process of wound healing. In the case of diabetic neuropathic ulcers of the forefoot, additional mechanical factors induced by the presence of diabetic neuropathy lead to high pressure loads of the metatarsal heads on the plantar skin. With time, such chronic loads could favor ulcer formation. Removal of the causal mechanical factor could alleviate the pressure and allow wound healing.
Clinical Relevance:
Neuropathic plantar ulcers are difficult-to-heal wounds and chronicity is associated to frequent hospitalizations, higher rates of amputation, and mortality. Early removal of the indirect causal agent, the resection of the metatarsal head, after failure of a well-conducted conservative standard of care could be a needed solution for wound healing and consequently a potential for reducing complications and costs.

Background
Diabetic foot ulcers (DFUs) are severe complications of diabetes that are associated with high morbidity, mortality, and health costs. 1 –6 The development of plantar foot ulcers in patients with diabetes is attributed to peripheral sensorimotor and autonomic neuropathy. Diabetic neuropathy leads to high plantar pressure, gait instability, and foot deformities, which increase the risk of developing ulcers. 7 –11 Moreover, multiple risk factors have been associated with the development of DFUs, which include male sex, duration of diabetes (>10 years), high body mass index, peripheral vascular disease, and advanced age. 12 –16
Conservative treatment, which includes wound care, sharp debridement, frequent dressings, and tight glycemic control, is the standard of care (SC) for the treatment of DFUs. 17 Offloading, which is often combined with SC, increases healing rates and decreases the recurrence of neuropathic DFUs. 18 For example, total contact cast (TCC) is effective in treating noninfected and nonischemic plantar diabetic foot wounds, 19 with healing rates ranging from 72% to 100% over a mean course of 7 weeks. 20 However, many reports have shown high recurrence rates when using SC alone or combined with TCC, with frequencies ranging from 40% to 60%. 20 –23 In contrast, surgical offloading, which is commonly used for the treatment of chronic and recalcitrant DFUs, seems to yield good-to-excellent outcomes. 24,25 For instance, metatarsal head resection (MHR) has better outcomes than SC. 26 –28 The procedure aims to definitively remove plantar pressure induced by prominent metatarsal heads. 29,30 A lower risk of major amputation has been demonstrated when MHR is performed at an early stage. 31 Evidence synthesis of surgical offloading with MHR has not been conducted. Thus, this meta-analysis (MA) aimed to quantitatively collect relevant data to evaluate the efficacy of MHR in the treatment of neuropathic DFUs.
Materials and Methods
Search strategy
An electronic search was conducted on the following databases from inception to June 2018: PubMed, EMBASE, Cochrane Library, and Google Scholar. Specific Boolean terms were used, which were as follows: (ulcer OR ulceration) AND (diabetes OR diabetic) AND resection AND metatarsal AND (foot OR feet). No language or date limitations were imposed.
Criteria for study selection
Studies with relevant outcomes were selected for inclusion. Only studies with comparative design or cohorts and those that used the dorsal approach to MHR were included. Moreover, studies on single, multiple MHR and pan metatarsal head resection (PMHR) were considered. However, review articles and case reports were excluded.
Screening and selection of studies
Three reviewers (K.Y., C.A., and N.K.) independently screened all studies that were retrieved. After the deletion of duplicates, the titles were first checked. Then, the abstracts were screened. Articles with abstracts that were likely relevant were retrieved. The reference list of every study included was checked for any additional potentially relevant articles. Disagreement on eligibility was resolved by a consensus decision.
Unit of analysis, types of outcome measures, and definition of outcome
The unit of analysis was the number of ulcer, independently of the number of MHRs performed to treat a single ulcer. The primary outcome was healing rate. The secondary outcomes were time to healing, ulcer recurrence rate, ulcer transfer rate, and infection rate. Ulcers that developed after surgery were categorized as recurrent ulcers or transfer ulcers. Recurrent ulcers were defined as those that developed after MHR at the same site as the original ulcer. A transfer ulcer was defined as one that developed beneath a metatarsal head at a different site from the previously treated site.
Complicated ulcers were defined as chronic (>6 months), recalcitrant, or recurrent and infected ulcers resistant to SC. Noncomplicated ulcers were defined as recent (<6 months) ulcers with no infection (Texas 1A/2A or Wagner 1/2 classification).
Data collection
This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 32 for case–control studies and the Meta-analysis of Observational Studies in Epidemiology (MOOSE) statement 33 for case series.
Data extraction
A data extraction sheet was used to report and summarize all relevant details of the studies. Initially, one author (K.Y.) extracted the data, which was later reviewed by other authors to obtain accurate data. Disagreements were resolved by a consensus decision. The predefined demographic data of the patients were extracted. Data about ulcer type, size, duration, surgical treatment, and follow-up duration were obtained. All primary and secondary outcomes were assessed and recorded.
Quality assessment
To identify the potential sources of bias correlated to the study design, the quality of the studies was assessed using the Joanna Briggs Institute (JBI) critical appraisal tools. Both the JBI critical appraisal checklist for case–control studies and the JBI critical appraisal checklist for case series were used accordingly. 34
Data analysis
Statistical analysis was conducted based on treatment type and study design. Effect size MA was used to assess for significant between-group differences in the case–control studies. A two independent proportion test was used to compare the frequencies of outcomes between two independent groups. Proportion MA was used to assess the weighted frequencies of outcomes in the case series. Heterogeneity was assessed using the inconsistency test (I 2 ). If the I 2 value was more than 50%, the random-effect estimate was reported.
Results
Search results
The electronic search yielded 27 references, of which one duplicate was removed. Sixteen studies were excluded: 10 studies did not report the primary outcome, two review studies, two case reports, one study reported MHR outcomes following the plantar approach, and another study reported about the outcomes of MHR for osteomyelitis without ulcers. After checking the references of the remaining 10 relevant studies, another relevant study was found. In total, 11 studies met the inclusion criteria (Fig. 1). Three were case–control studies (comparative design) and eight case series. The basic characteristics of the 11 studies are shown in Table 1.
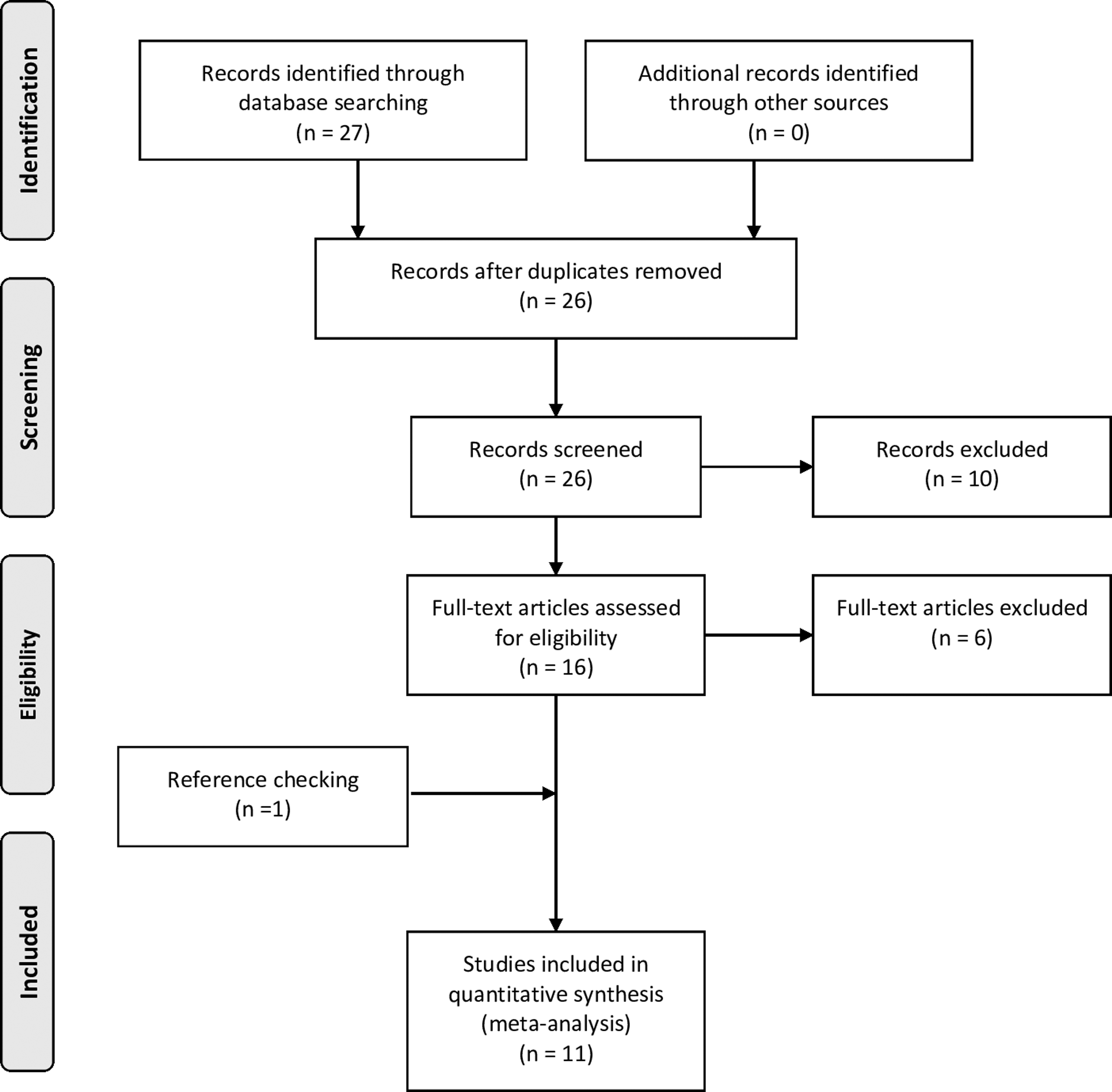
PRISMA Flow Diagram.
Characteristics of included studies
MHR, metatarsal head resection; PMHR, panmetatarsal head resection; SC, standard care; CNU, chronic nonhealing ulcers; *: ulcerations did not probe to bone, and none had concomitant infection or ischemia; NR, not reported.
Characteristics of the patients and ulcers
The total pooled sample comprised 477 patients with 494 feet and 593 neuropathic plantar ulcers. A total of 514 plantar ulcers were treated with MHR, while 89 ulcers (from the 3 comparative studies) received standard nonsurgical medical care. In addition, in the study of Wieman et al. about ulcers with unknown infection status, 101 (20.7%) of 492 remaining ulcers were considered infected. However, the most common ulcers in the case series were chronic and recalcitrant, with high rates of subclinical infection. None of the ulcers was infected in the three comparative studies.
The mean age of all the patients was 58.6 ± 3.8 years. The mean follow-up period was 25.9 ± 21 months. Three studies 26,27,35 reported the HbA1c level of the patients, with a pooled mean of 8.1% ± 0.6%. Four studies 24,28,30,36 have shown the mean duration of preoperative ulcer, with a pooled mean of 27.5 ± 33.7 weeks.
Table 1 shows the types of ulcer treated, which were categorized using various classification systems. MHR or PMHR was performed after a long and unsuccessful conservative treatment in all eight case series, in which most ulcers were categorized as complicated. The ulcers included in the comparative studies were categorized as noncomplicated.
Quality appraisal outcomes
The JBI critical appraisal checklists were used in the studies. None of the patients had a score less than 7 out of 10 (Tables 2 and 3).
Joanna Briggs Institute critical appraisal checklist for case control studies
Joanna Briggs Institute critical appraisal checklist for case series
Outcomes
Data about the outcomes obtained from individual studies are shown in Table 4. Table 5 depicts the summary of the meta-analytical results.
Summary of individual study results
M, metatarsal bone; SC, standard care; OM, osteomyelitis; WB, weight-bearing; NWB, nonweight-bearing.
Summary of meta-analytical results
NA, not available; CI, confidence interval.
Any MHR (except PMHR)
Five studies 28,31,37 –39 that included 295 ulcers showed a weighted healing rate of 93.6% and a mean healing time of 58 ± 19 days. Four studies 26,28,31,36 that included 269 ulcers yielded a weighted infection rate of 5%. The clean sample of Armstrong et al. 26 and the clean subgroup sample of Griffiths and Wieman, 28 which included a total of 51 ulcers, produced an infection rate of 7.1% (95% confidence interval [CI] = 0.018–0.155). Johnson and Anderson 36 have reported that 1 (5.5%) of 18 infected ulcers was associated with osteomyelitis and was treated with MHR and antibiotics for 6 weeks.
Seven studies 28,31,35 –39 that included 350 ulcers had a weighted recurrence rate of 4.2%. Six studies 28,31,35,36,38 –40 that included 395 ulcers treated with MHR demonstrated a weighted transfer ulcer rate of 16.3%. When combining all 8 case series, the weighted amputation rate was of 4.2%. In the study of Wieman et al., 31 two of the 13 patients who underwent an amputation had uncontrolled infection while the remaining exhibited severe ischemia.
Pan metatarsal head resection
Three studies 27,30,40 with a total of 82 PMHR yielded a healing rate of 92.1% and an infection rate of 8.6%. The clean samples of Armstrong et al. 27 and Petrov et al. 40 with a total of 66 ulcers showed an infection rate of 13.2% (95% CI = 0.022–0.608). In the study of Giurini et al., 30 of the 15 ulcers that were infected and treated with MHR and antibiotics, none showed signs of infection during the last follow-up. Only one study 27 has reported a healing time of 8.6 ± 3.9 weeks. The weighted recurrence and amputation rates were 16.5% and 4%, respectively.
MHR versus SC
Three case–control studies compared MHR (n = 92) and SCR (n = 89). 24,26,27
The weighted healing rates of the MHR and SC groups were 93.1% and 62.6%, respectively. The two independent proportion test yielded a difference of 28.4%, which is in favor of the MHR group (p < 0.0001). The weighted infection rates of the MHR and SC groups were 12.5% and 49%, respectively. The two independent proportion test yielded a difference of 34.4%, which is in favor of the MHR group (p < 0.0001).
The mean time to heal was 19.7 ± 6.5 days in the MHR group and 75.5 ± 25.1 days in the SC group. In the MHR group, the effect size difference in time to heal was −0.94 (95% CI = −1.392 to −0.486, I 2 = 49.5%, p < 0.0001).
The weighted recurrence rate of the MHR and SC groups were 6.8% and 28.9%, respectively. The two independent proportion test yielded a difference of 21.6%, which is in favor of the MHR group (p = 0.0002).
The weighted amputation rate of the SC group was twice than that of the MHR group (9% and 4.3%, respectively); however, the result was not significantly different (p = 0.1).
Discussion
Main findings
To the best of our knowledge, this is the first meta-analysis on the efficacy of MHR in treating neuropathic DFUs. The meta-analytical results of noncomplicated recent DFUs in the comparative studies showed that MHR/PMHR had significantly better healing outcomes and lower complication rates than SC. In fact, failure to heal, recurrence, and infection rates were four times higher in the SC group with a significantly longer time to healing. Furthermore, similar meta-analytical outcomes were observed when analyzing the case series of the chronic and recalcitrant ulcers treated with MHR/PMHR (Table 5). The healing time following MHR/PMHR yielded from the case series was substantially longer than that generated from the comparative studies (8.28/8.6 weeks vs. 2.8 weeks); that could be explained by the predominant type of treated ulcers (complicated vs. noncomplicated).
Interpretation of the results
When examining the literature related to conservative management, poor outcomes were often reported. For instance, based on weighted results from the control arms of 10 intervention trials, Margolis et al. 41 reported healing rates of 24.2% after 12 weeks in four trials and 30.9% after 20 weeks in six trials. Later, the same group demonstrated ulcer healing rates of 47% 42 and 68% 43 after 20 weeks. Veves et al. 44 demonstrated a healing rate of 38% at 12 weeks following SC. Ince et al. 45 reported healing rates of 59.8% at 12 weeks and 71.0% at 20 weeks, but for the subgroup of patients with DFUs that lasted for more than 6 weeks, only 39% of ulcers healed after 12 weeks and 56.3% after 20 weeks. Most studies included both chronic and recent ulcers and that might have introduced bias considering the better healing rate of recent wounds.
Nonsurgical offloading such as total cast was found to be one of the very few SC therapies that is backed up by evidence. 46 However, the high healing rate following the use of TCC does not withstand over time with reported high rates of long-term recurrence. 19,20 For example, Pound et al. demonstrated a recurrence rate of 40% within a mean period of 4.5 months after using TCC, 21 and Armstrong et al. 4 calculated a 3-year recurrence rate of 60%. These authors have used the term remission instead of healing. In summary, only half of DFUs have healed after 5 months of SC, yet, with a recurrence rate of 40% among the patients who recovered within the first year. In addition, 2 years of orthotic therapy was found to reduce ulcer recurrence from 79% to 15% 47 whereby our recurrence results ranged between 4.2% and 6.8% following MHR, and 16.5% after PMHR. It should be noted that in the case of customized foot wear are dampened by the fact that large numbers of patients do not adhere to the recommended treatment. 48
Since most ulcers, mainly from the case series, treated with MHR/MPHR, were chronic and recalcitrant to conservative treatment, one can argue that a significant number did not heal owing to an existing subclinical infection. Thus, the incidence of preoperative infection was likely higher than the reported value and consequently, a higher incidence of postoperative infection would have been expected. However, our study had demonstrated very low rates of postoperative infection supporting the effectiveness of the MHR procedure. By contrast, in some case series of clean ulcers, the postoperative infection rates of infected ulcers treated with MHR/PMHR and antibiotics were lower than those of infected ulcers treated with MHR/PMHR alone. These findings could be also attributed to the likely presence of subclinical infection in some of the presumed clean ulcers. Further studies are needed to assess the effect of adding antibiotics to MHR when treating DFUs. Wieman et al. 31 have shown that preoperative infection was a predictive factor of postoperative infection and amputation. These authors stated that 75% (9 out of 12) of the patients who developed infections had infected ulcers before surgery. Nevertheless, clear conclusions could not be drawn from their study since the number of infected ulcers before surgery was not reported.
The amputation rates were significantly higher after treatment of severely ischemic limbs. 49 Wieman et al. 31 have reported that 84.2% (11 out of 13) of major amputations were performed in patients who had either inoperable vascular pathology or failed vascular reconstruction, while the other two patients had uncontrolled infections. Interestingly, no significant difference was observed in amputation rates between the SC and MHR groups in this review. As mentioned by Armstrong et al., 27 the causes of this phenomenon is difficult to identify, considering the improvement in time to healing and low proportion of patients with infection in the MHR group. Although our results were not significant, the incidence of amputation in the SC group was two times higher than that in the MHR group. Thus, further studies with a larger sample size are warranted to identify significant differences between groups.
Since the pressure induced by the metatarsal head is a major factor for the development of neuropathic plantar ulcers, momentary offloading, such as that in TCC, does not relieve plantar pressure. Hence, the high recurrence rate after nonsurgical offloading is not surprising. We argue that bone-induced pressure should be definitively removed via surgical interventions, such as MHR. The results of this review should prompt other researchers to investigate the efficacy of other surgical offloading techniques, such as metatarsal osteotomy. These surgeries are considered minor procedures as they can be performed under local anesthesia. Considering that the natural history of recurrent and recalcitrant ulcers is so dismal and the outcomes of MHR are satisfactory, physicians should consider the use of MHR more often and incorporate this technique in the early management of DFUs. Our results concur with other evidence-based surgical outcomes on the efficacy of conservative surgery in treating diabetic forefoot ulcers. 50 –53 Yammine and Assi demonstrated that a period of 12 weeks could be considered a reasonable cutoff value to consider surgical treatment for patients with nonhealing DFUs. 52
Limitations
The present study had some limitations, primarily related to the study design of the included studies. Although three comparative studies had a retrospective study design, they were of good quality as the baseline characteristics of the patients and ulcers were similar between the groups. Numerous factors and comorbidities could have affected the healing rate of DFUs, which consequently might have impacted our results. All included studies used the dorsal approach; however, a study comparing dorsal and plantar approaches rendered similar healing times but with higher incidence of postsurgical complications through the plantar approach. 54
Another possible limitation is the lack of data about the accurate status of the arteries in the peripheral lower limb. Peripheral artery disease is considered a predictor of nonhealing. 35 However, most patients in this review had no clinical signs of severe ischemia. In contrast, the incidence rate of ulcer transfer after MHR was relatively high, and this could be a disadvantage of the procedure. A disadvantage could be the development of a flail toe following MHR; however, no walking limitation, new deformity, or novel ulcer was observed in one study reporting such outcomes. 24 Unfortunately, none of the included studies discussed explicitly the management and outcomes of newly developed ulcers. The change in the parabola of the metatarsal heads could have contributed to the increase in pressure at the sides of the resected head. 55 In a recent meta-analysis, Yammine et al. reported a transfer rate of only 10.3% after metatarsal osteotomy in patients with infection-free DFUs. 50 Another limitation that might have impacted the results is the use of different postoperative protective devices. While some authors used TCC in the postoperative period, others prescribed pneumatic walkers or protective footwear. Moreover, the time period for nonweight-bearing varied between studies. Such heterogeneity in postoperative management might have affected our results.
Conclusion
The MHR technique demonstrated significantly faster healing time, better healing rate, and lower infection and recurrence rates than SC among patients with recently developed noninfected ulcers. Similar meta-analytical outcomes were generated from the case series of recalcitrant ulcers treated with MHR. This procedure was found to be a reliable and efficient surgical offloading technique. Considering the natural history of DFUs treated with SC, the use of this surgical offloading technique at an earlier stage could be justified. Further large-sampled randomized trials should be conducted to support the results of this review.
Take-Home Messages
Neuropathic plantar ulcers of the forefoot are difficult-to-heal wounds where the results of the standard of care are not optimal.
Removing the pressure load by resection of the corresponding metatarsal head was found to generate significantly better outcomes than SC.
Failure to heal, recurrence, and infection rates were four times higher in the SC group than in the resection group. The amputation rate was two times higher in the SC group than in the resection group.
Outcomes from case series on chronic and recalcitrant ulcers treated with resection were very good.
Footnotes
Authors' Contribution
K.Y. designed the research. K.Y., N.K. and C.A. screened and selected the studies. K.Y. extracted the data then reviewed by N.K. and C.A. K.Y. performed the data analysis. K.Y., N.K., and C.A. wrote and reviewed the article.
Author Disclosure and Ghostwriting
No competing financial interests exist. The content of this article was expressly written by the authors listed. No ghostwriters were used to write this article.
About the Authors