
Abstract
Scope and Significance:
Pressure ulcers are very difficult to treat and pose an economic burden, just below cancer and cardiovascular illness, at 4.82 billion U.S. dollars. It is important to understand the pathophysiology of the condition, risk stratification, and ways of preventing it. Prevention forms the most important aspect of their management. The authors systematically evaluated the existing risk prediction scales and explored the evidence from literature regarding the role of additional factors including body mass index, obesity, subcutaneous tissue thickness, and skin integrity in pressure ulcers. With this review it is hoped that the future management of pressure ulcers will concentrate on the preventable and alterable factors in its pathophysiology.
Translational Relevance:
The review focuses on how adipose tissue thickness can predict the occurrence of pressure ulcer. If adequately proved that a definite thickness of peripheral adipose tissue is efficient in prevention of pressure ulcers, then methods of maintaining the thickness of this tissue will be the next effective strategy in the management of this chronic issue.
Clinical Relevance:
The review addresses the management of pressure ulcers to wound care providers and emphasize on confounding parameters of obesity, subcutaneous tissue thickness, and skin integrity during the treatment regimen of pressure ulcers.
Objectives:
The main objective of this review is to draw a consensus concerning the role of adipose tissue in pressure ulcers, based on the published research. A review of the various preexisting predictive scales for pressure ulcers is a secondary objective to highlight the shortcomings in ulcer management. This review finally aims in the future at paving a way to refine our prognosticating scales for pressure sores based on these results. Accurate preventative injury risk scales are needed so that preventative resources can be directed to the patients for whom they are the most appropriate.

BACKGROUND
Pressure ulcers are one of the most important chronic and recurrent morbidities of bedridden patients. 1 The areas of involvement of these ulcers include bony prominences such as ischial tuberosity, trochanteric regions, gluteal regions in the wheelchair-bound patients, and can also occur in the sacrum, heel, thoracic (posterior trunk), and occipital region in the bedridden patients.
These ulcers based on the depth and structures they involve are further classified based on the guidelines of National Pressure Injury Advisory Panel (NPIAP). 2 Stage 1 involves non blanchable redness of skin that is intact. Stage 2 includes pressure injuries with partial thickness skin loss and exposed dermis. Stage 3: Pressure injury with full thickness skin loss. Stage 4 there is combined skin and tissue loss. Unstageable Pressure injury, though there is full thickness skin and tissue loss the extent of the loss cannot be seen due to eschar or slough. Deep tissue injury (DTI), involves persistent non blanchable purple, maroon, or red discoloration of skin due to prolonged shearing effect at the bone-muscle interface. 2
The ulcers not only pose a challenge to the reconstructive surgeons but can further get complicated by local infections such as abscess, or osteomyelitis, cancer such as Marjolin's ulcer, septicemia, renal failure, and even death. 3
A variety of investigators have come up with different scales in the past to predict the risk assessment of pressure ulcers in such patients. Though there are a wide variety of such tools, only a few of them have stood the test of time. They are namely Braden, Norton, and Waterlow scale in the order of popularity. 4 These scales have tried to impress upon the readers the importance of intrinsic patient factors like general physical, mental condition, body mass index (BMI), and extrinsic factors like major surgery, acute illness, and so on. The disadvantage of this system is being realized recently with regard to certain factors taken into account. According to this system, the BMI is a poor prognosis factor, meaning a patient with higher BMI has higher risk of developing pressure ulcer.
But a factor like BMI has two components contributing to it, namely body weight and height. 5 Out of these two components, body weight is the most variable. The body weight of a person is contributed by bone and soft tissue. The soft tissue that is of utmost importance and variable in distribution is the adipose layer. The amount of adipose tissue present in an individual is subjected to activity, nutrition status, and genetic inheritance pattern of that subject. This tissue is distributed both internally (visceral fat) and peripherally (peripheral fat). 6 If we consider pressure ulcer prone areas like sacrum or gluteal and ischial regions , and others the fat tissue is distributed both above and below the bony prominences. 7 Hence, considering the pathophysiology, it is only logical to hypothesize that the fat tissue (and the other soft tissues) below these prominences provide a cushion or padding, protecting the overlying skin.
The corollary of this statement would be that, if the subcutaneous fat tissue or soft tissue below these prominences are increased by some means (e.g., surgically), the risk of developing pressure ulcers should then decrease ideally.
Even though previous studies recommended fat grafting for chronic ulcers, current studies show the effectiveness of this method in early stages of pressure ulcers and also in preventing advancement of these ulcers. 8 –11 Thus, fat grafting can also be contemplated for stage 1 and stage 2 pressure injuries where the grafting can be done in the layer below the intact dermis. For stage 2, in addition after the grafting the dermis can be resurfaced with biological skin substitutes including skin grafting. So instead of considering body weight in total, it is important to understand that the fat or adipose tissue, which is distributed peripherally and viscerally, should be differentiated and assessed independently. One way of dealing with this is to take other measurements apart from BMI, including skin fold thickness, waist hip ratio, and others into consideration. 12
METHODS
Protocol and registration
The study is a narrative review that considers all relevant studies with respect to the role of adipose tissue in pressure ulcers.
Eligibility criteria
Human studies including experimental studies published in English related to pressure ulcers were considered for the review purpose. Randomized control trials and clinical trials of studies containing reports correlating pressure ulcers or deep tissue injuries with obesity, BMI, and peak seat interface pressure, correlation of skin integrity or skin barrier and obesity, and effects of fat grafting on pressure ulcers were considered for the study. Human epidemiological and experimental research were included. The intervention tools included in the search were both preventive and treatment strategies.
Information sources, study selection and search
All Studies published in PUBMED database were included for study population under consideration. The study population was searched using Medical Subject Heading (MeSH) terms “pressure ulcers,” “obesity,” “fat grafting,” “skin barrier,” “deep tissue injury,” “BMI,” “skin integrity,” “peak seat interface pressure.” The resulting studies were further shortlisted based on inclusion criteria of clinical trials and randomized clinical trials related to patient-based studies. The resulting article were further checked for duplication and accordingly avoided. The articles selection schema is provided in Supplementary Fig. S1 and listed in Table 1.
List of studies associating obesity and pressure ulcer
Levels of evidence adapted from American Society of Plastic Surgeons: Level I: High quality prospective cohort study with adequate power or systematic review of these studies; II: Lesser quality prospective cohort, retrospective cohort study, untreated controls from an RCT, or systematic review of these studies; III: Case–control study or systematic review of these studies; IV: Case series; V: Expert opinion; case report or clinical example; or evidence based on physiology, bench research or “first principles.” Table summary: Studies that point out decreased subcutaneous fat thickness as the reason for pressure injury: The literature search revealed five studies that have directly indicated that the reduced subcutaneous fat thickness to be responsible for increase pressure injury. They include studies by Thomas, 24 Allman et al., 22 Jaul et al., 23 Yalcin et al., 25 and Yarkony. 26 One study by Compher et al. 18 reveals the protective nature of fat against pressure injury. BMI and its role in pressure injury: Though previous studies by Pokorny, 16 Yosipovitch et al., 17 Kernozek et al., 14 Cai et al., 13 and Lowe, 15 have suggested increased BMI (>40) to have a detrimental effect on pressure injury by increasing skin breakdown, some studies like Elsner and Gefen, 19 Hyun et al., 20 and Ness et al., 21 have suggested that very low BMI (18.5–19) can also play a causative role in pressure injury. Indirect evidence of protective role of subcutaneous fat: Studies by Marangi et al., 8 Di Caprio et al., 11 Previnaire et al., 9 and Opsomer et al., 10 have demonstrated the protective role of fat grafting in patients prone to pressure injury indirectly suggesting a protective role of subcutaneous fat.
BMI, body mass index; RCT, randomized clinical trial.
Data items and data collection process
The different studies were included in an excel sheet, documenting the name of the authors, level of study, number of patients included in the study, and the inferences.
Summary measures
Since the review is narrative, the summary measures are based on the consensus from the majority of studies considered that were scrutinized by each of the authors.
RESULTS
The result of the studies has been summarized in Table 1. Around 399 articles were screened with the search terms provided. A total of 182 articles were retrieved using the search term pressure ulcer or deep tissue injury and obesity. Altogether, 85 articles were gathered using peak seat pressure and BMI and 116 articles were found after using terms skin integrity or skin barrier and obesity while 15 articles were documented with terms pressure ulcer and fat grafting. Fifteen studies were based on the selection criteria and adjusting for any duplicate studies. These studies were human, experimental or studies based on trials on humans and dealt with pressure ulcers, skin integrity, obesity, fat grafting, or DTI. The studies belonged primarily to level 2–5 in terms of JBI (Joanna Briggs Institute) evidence. The study characteristics and study selection are also depicted. Since the article is a narrative review, a statistical analysis has not been included.
The search revealed mixed results. While there were studies pointing at obesity as a prognostic factor for pressure ulcers and cause a disruption of skin integrity. 13 –17 There were also those who asserted that patients who are malnourished as measured by their low BMI are more prone to develop pressure ulcers. 18,19 Some studies particularly state that BMI: 19–40 appears to be protective to a certain limit. 20,21 Once this limit is surpassed (BMI >40), it increases the risk of developing pressure ulcers.
However, others have reported the importance of malnutrition in the form of decreased subcutaneous tissue thickness and triceps fold thickness, an independent risk factor for pressure ulcers. 22 –26 In a report by Marangi et al., authors have elucidated the importance of the protective effect of fat tissue in preventing pressure ulcers. 8
Discussion of findings and relevant literature
Risk factors associated with pressure ulcers
Etiology and pathophysiology of pressure ulcers
When pressure occludes the capillaries supplying the tissue then owing to hypoxia inflammatory mediators accumulate and causes vessel wall damage causing it to leak proteins. This further causes edema formation due to osmotic pressure and increases the pressure around capillaries causing it to occlude even at lower external pressure. All this leads to aggravation of hypoxia and tissue death and inflammation. The lymphatic system that otherwise evacuates the protein is also compromised because of the increased edema and occlusion pressure of its channels. The dehydrated cells get further irritated. When the pressure is released the necrotic vessel wall slough out, occludes the lumen, and can further enhance the ongoing damage 27 (Figs. 1 and 2).
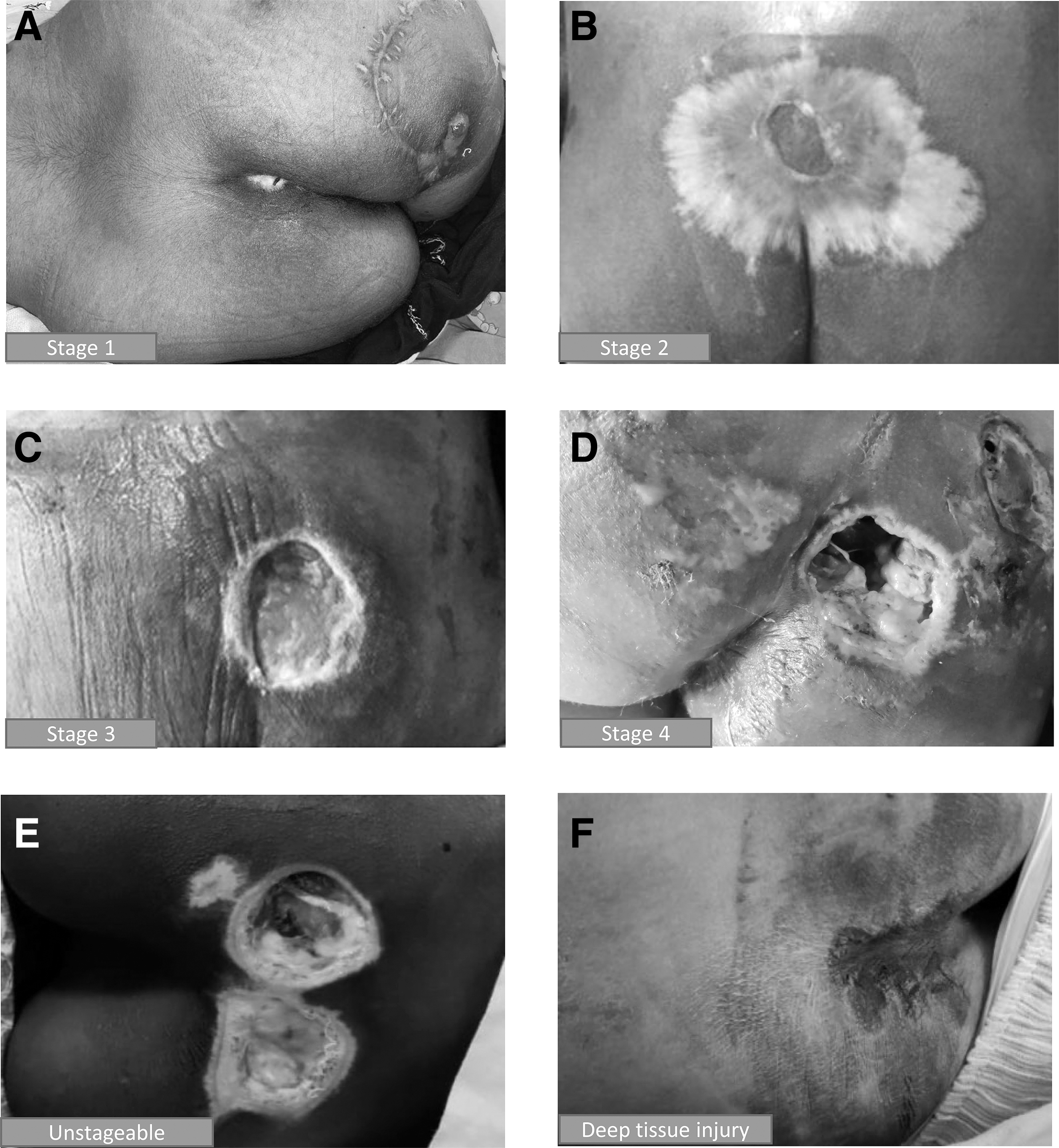
Images of pressure ulcers at different stages at our clinic.

Pictorial representation of stages of pressure ulcer formation.
However, capillary blood pressure is usually <32 mm Hg in critically ill patients owing to hemodynamic instability and comorbid conditions; thus, even lower applied pressures may be sufficient to induce ulceration in this group of patients. 28
External pressure, 29 tissue tolerance, 30 and duration of pressure are the principle factors that decide the occurrence of pressure ulcers. The intensity and duration of external pressure over skin results in pressure ulcers. The other factor influencing the process is tissue tolerance. While body weight, sensory perception, activity, and mobility decide the intensity and duration of pressure, factors like age, nutrition status, incontinence, friction, skin shear, body temperature, use of medications, and blood pressure decide the tissue tolerance. 31
Factors leading to pressure ulcers
Risk factors for developing pressure sores can be intrinsic and extrinsic. 32 Intrinsic factors include, motor diseases, sensory disturbances, neurological diseases, malnutrition, dehydration, hypo perfusion, and trophic disturbances. 33 –35 Extrinsic factors include, trauma, inadequate movement, amputations, moisture, sheer, lack of attention to positioning, and physical restraints. 36 –39 Back support for lying down is also an important extrinsic risk factor. An air mattress with alternating pressure is proven to be better than a normal mattress or spine board. 40
Moisture is a chief extrinsic factor that affects the tissue tolerance. Moisture causes maceration, 41 changes the environment pH, and causes milieu conducive for infections. 42 Moisture-associated skin damage is a known clinical condition. 43 Patients with this condition come with signs and symptoms of chronic pain, itching, burning, and present with erosions of skin. Moisture-related skin damage is associated with occurrence of dermatitis, fungal or bacterial infections of skin, and pressure sores. 44 A number of factors may exacerbate or precipitate moisture-associated skin damage. There might be excessive perspiration, increased metabolism in dermis, alteration in skin pH, atopy, deep body folds, dermal thinning, or increased sebum production. 45
The factors can also be extrinsic like irritants that can be biological or chemical in nature, mechanical skin stress like sheer, friction, or pressure, skin infections like fungal, environmental factors like humidity, incontinence that can be fecal, urine, or both. 46 Studies relate the importance of moisture and skin moisture content to the development of pressure ulcers. Lower skin moisture content, alteration in skin pH, and decrease in sebum secretion in stratum corneum have led to increase in the incidence of pressure ulcers. 7
Patients positioned in an angle experience sheer forces between the mattress and their skin interface. The gravity forces are counteracted by the frictional force at the level of skin interface. The deeper tissues like subcutaneous tissue, muscle, and bone get displaced in the direction of the force much more and face the risk of ischemia due to devascularization as the vascular supply gets deformed in between the skin and deeper planes 47 –49 (Fig. 3).
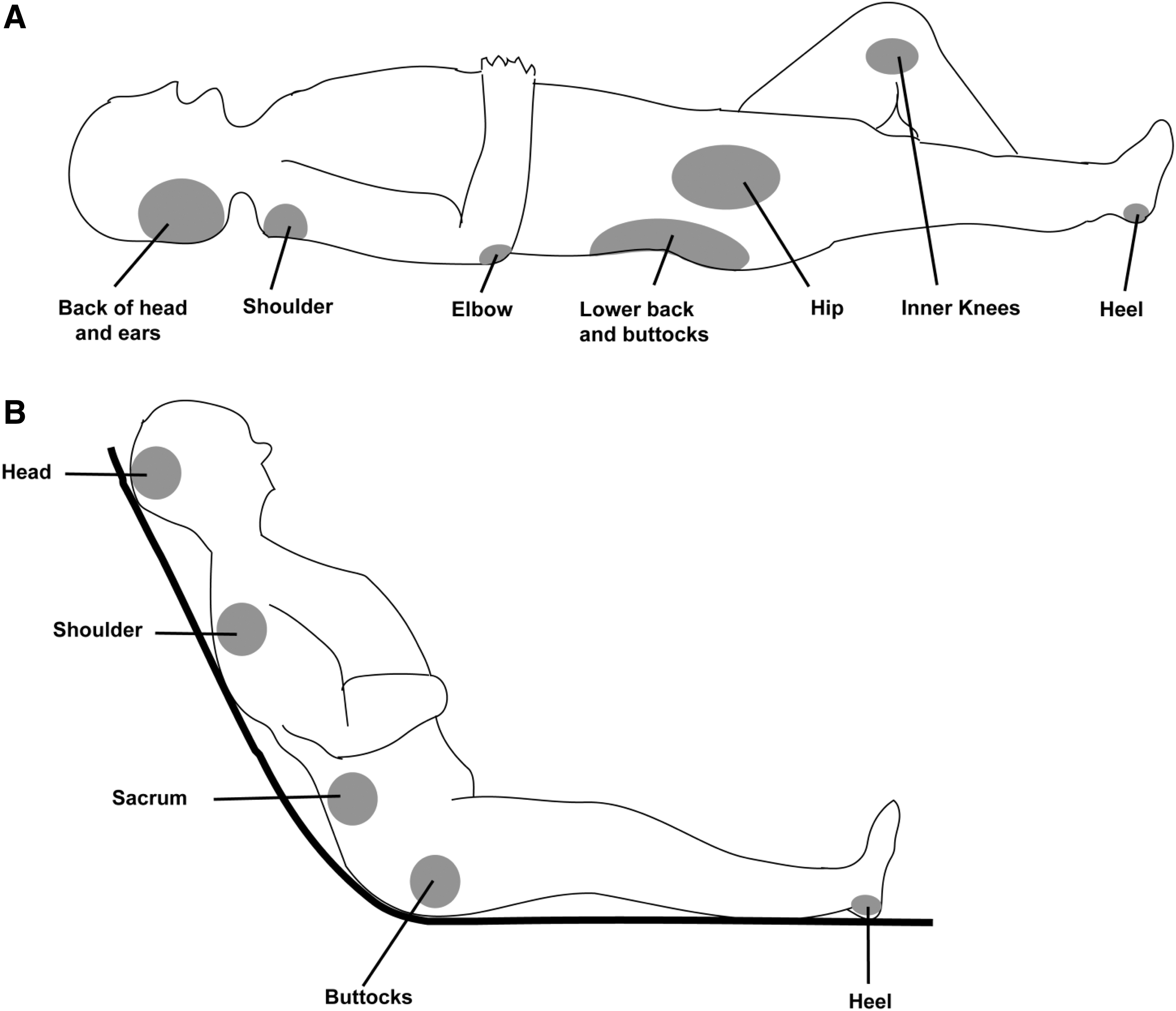
Pictorial representation of sites of pressure ulcer formation.
Pressure ulcers may also involve deep tissue, occurring in the subcutaneous fatty tissue in the presence of intact skin. It is different from the superficial ulcer by the fact that the damage progresses from the muscle to the epidermis instead of in the reverse manner. This makes the early detection more complex in such ulcers. This special type of pressure ulcers occur because of chronic compression of soft tissues under bony prominences in patients with sensory motor disturbances 50 (Fig. 4).
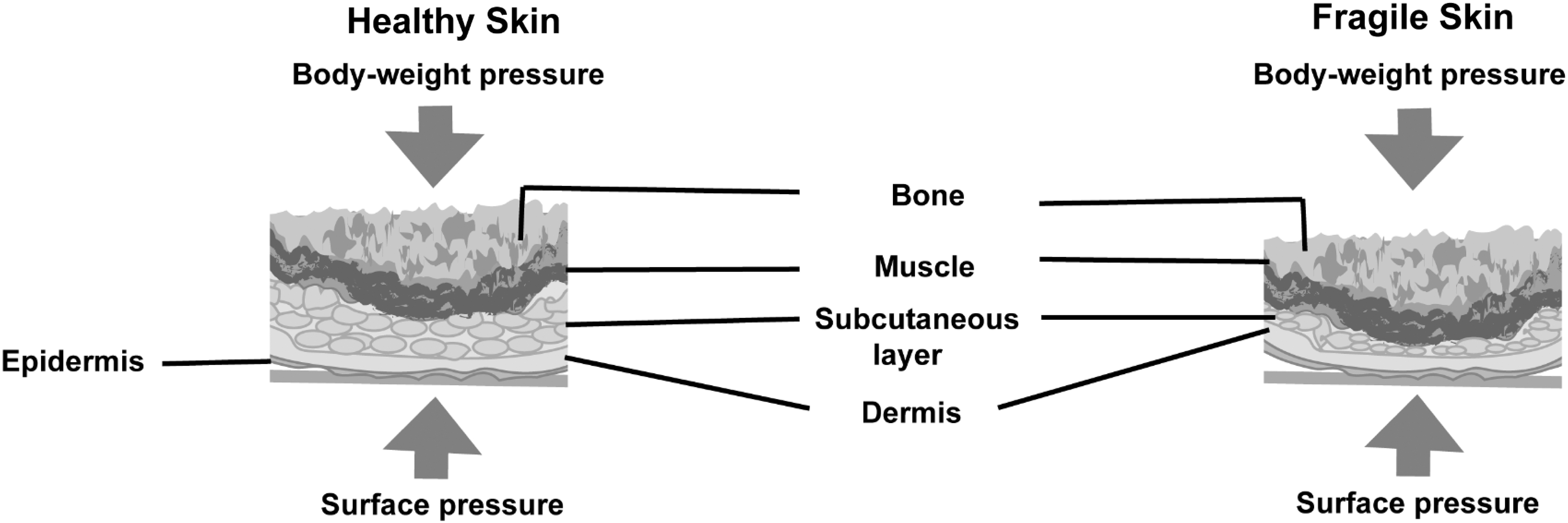
Effect of difference of pressure on healthy skin (well-nourished individual) with normal subcutaneous fat and fragile (malnourished individual) skin with thin subcutaneous fat.
Role of skin integrity in pressure ulcer
Skin is homeostatic in nature. The stratum corneum of adult skin replaces the dead epidermal cells with ceramides and network of keratin fibers. 51 The hydrophobic layer thus formed then protects the underlying soft tissue and prevents water loss. The lipid layer of skin is considered protective as it maintains moisture and prevents drying and loss of water. 52
An intact skin hence protects the body from pathogens, water loss, and irritants. It helps in temperature regulation through vasoconstriction, shivering, vasodilation, and sweating. Resident bacteria are normally present over epidermis. Overgrowth or undergrowth of bacteria can occur due to excess moisture, alkaline soaps, immunodeficiency status, and antibiotic usage. 53 Moisture exposure due to contact with urine or feces, can macerate the outer layer of epidermis, which leads to weakening and breakdown of epidermis. 54
Aged individuals are more prone to pressure ulcers. Aging causes dermal thinning, epidermal thinning, and loss of dermal papillae resulting in flattening of dermo-epidermal junction. This decreases the threshold for shearing and in turn decreases the possibility for oxygen and nutrition diffusion across membrane. 55 Flattening of rete ridges and dermal papillae cause decreased cohesion of dermal epidermal junction and hence increased skin tear. 53
Age-related loss of subcutaneous tissue is also indicated as a definitive risk factor for the development of pressure ulcer. 56 The thinner subcutaneous tissue is also responsible for increased risk of sheer and pressure injuries. 57 The elderly is at higher risk of injury also due to decreased sensory receptors. Occurrence of ulcer is determined by state of consciousness, mobility, and self-caring and ulcer promoting factors. Therefore, the key to preventing pressure ulcers is to accurately identify at-risk individuals quickly, so that preventive measures may be implemented.
Scales and their definitions used in predicting pressure ulcers
Braden, 58 Norton, 59 and Waterlow 60 scales analyze different intrinsic and extrinsic risk factors for predicting pressure ulcer occurrence in susceptible individuals (Table 2).
Skin barrier and pressure ulcer: pressure sore risk prediction scales
CVA, cerebrovascular accident; DM, diabetes mellitus; MS, multiple sclerosis.
Braden scale takes into consideration those factors that can extend the period of external pressure like sensory disturbance, activity and mobility and those that can affect skin integrity like moisture, shear, nutritional state and friction forces. 58
The Norton scale includes patient related risk factors like advanced age, mental status, additional illness, skin condition, general medical condition, mobility and incontinence. 59
The Waterlow scale considers both intrinsic (weight with respect to height, age, sex, appetite, body habitus, skin type, continence, neurological deficit) and extrinsic factors (major surgery, acute illness, medications like sedatives). 60 The factors are given scores of 1–4 (Table 2). When these scores were analyzed, we found that the nutrition parameter is based on subjective scale and hence their validity is questioned. The factor does not take in to account the triceps fold thickness 61 or arm girth. 62 Neither has the scale taken into account waist-hip ratio or waist circumference 63 to measure the visceral adiposity index, 64 which is important with respect to the pathology of pressure ulcer.
In addition, patients with lipodystrophy might have more fat in the pressure ulcer susceptible regions (gluteal regions) than other sites requiring specific measurements in these regions in addition apart from the arm regions, which normally reflect the general fat distribution.
While the above scales give views regarding the prediction of high-risk category of patients, the European Pressure Ulcer Advisory Panel (EPUAP) scale grades the pressure sore depending upon the depth of involvement of the ulcer, related to skin and tissue changes. 2,65 The EPUAP, is an adoption of National Pressure Ulcer Advisory Panel (NPUAP), system introduced in the United States to ensure a uniform standard classification system of pressure ulcers for clinical practice and management.
Critical issue and summary of evidence
Obesity, BMI, and subcutaneous fat and its implications on pressure ulcers
Obesity is defined as accumulation of excess fat to the extent of causing disease. 66 Obesity is also suspected to be one of the factors influencing pressure ulcers, though much patient-based studies have not been conducted in this direction (Table 1). Traditionally, obesity is measured in terms of BMI. Individual with BMI above 30 is defined as obese. 67 BMI has high specificity (0.9) but low sensitivity (0.5). 68 Although BMI is comparable to gold standards of body fat measurements, it cannot distinguish between lean and fat mass or give information about body fat distribution. Studies have shown that BMI might not be an actual reflection of obesity. 69 People of different age and gender having same BMI might have different amounts of fat in their body as revealed by studies. 70,71
In elderly people, there is loss of muscle mass and BMI might underestimate obesity in this population. The most accurate direct method of assessing fat distribution and quantity is dual energy X ray absorptiometry (DEXA). 72 The main disadvantage of this imaging is that it is very cumbersome and expensive. Therefore, clinicians generally resort to anthropometric measurements. 73 While subscapular and abdominal fat gives an idea of central obesity, thickness of biceps or triceps folds evaluates peripheral obesity.
Visceral adiposity is predicted by waist circumference, waist hip ratio, and waist height ratio. Although all these measurements correlate with body fat, they need to be adjusted to ethnicity, environmental and medical factors. Bioelectric impedance 74 is another method to measure fat distribution but is influenced by the prediction equation employed and the device used. The quadratic equation relating the BMI with percentage of body fat is expressed as follows: Body fat (%) = 3.76 BMI-0.042–47.8. It was reported that percentage body fat is independent of BMI as seen in the study that the percentage of fat in women was 10.4% as compared to that of men with similar BMI. They thus concluded that the BMI and percentage fat relation is dependent on age and gender. 75
There is no measure of obesity pertaining to pressure ulcer occurrence in the high-risk population. The importance of obesity or the fat distribution has not been clearly researched to know their role in pressure ulcers.
While studies such as Baugh et al., 76 has agreed that obesity is a risk factor for pressure ulcer by increasing the pressure on load-bearing soft tissues by the higher body mass, other studies like Compher et al., 18 suggested that the increased fatty layer may be protective by redistributing high interface pressures. This was based on a prospective study that had 3,788 patients and collected details regarding obesity and malnutrition. In the 378 patients who ultimately developed pressure ulcers it was found that malnutrition posed an even higher risk when compared to obesity with respect to these pressure ulcers. The authors thereby concluded that obesity might be protective for this pathology. Reports by Berlowitz et al. 77 and Casimiro et al. 78 had also suggested protective effect of higher BMI.
In another work, Hyun et al. 20 studied 2,632 patients and associated BMI with risk for pressure ulcers. Four groups of patients of different BMI categories—underweight, normal, obese, and very obese were included in the study. The demographics, Braden score, body weight, and the pressure ulcer occurrence were considered from their medical records. Their conclusion was that BMI <19 and BMI >40 carry the highest risk for pressure ulcers. The study stated that obesity contributes to decreased mobility in intensive care units (ICUs) and this in turn leads to pressure on the overlying skin.
Ness et al. 2 1 had studied 2,479 patients, based on audits and clinical records conducted a retrospective cohort study. Regression analysis between BMI, malnutrition and pressure ulcers were done. Similar conclusions were drawn: BMI <18.5 and BMI >40 lead to increased risks for pressure ulcer. Contrary to the traditional belief that obesity contributes to increased risk of development of pressure ulcers, the studies concluded that the category of patients with malnutrition have more tendency to develop them when compared to healthy individuals and obese individuals with BMI <40. The study also concluded that morbidly obese patients of BMI >40, had over three times the odds of developing pressure ulcers when compared to the healthy weight patient.
Further, a malnourished morbidly obese patient is eleven times more likely to develop pressure ulcers. 21 Obesity has often associated with other comorbidities like diabetes, hypertension, and cardiovascular diseases. Each of these conditions can influence the prognosis of pressure ulcer.
Correlation between diabetes and pressure ulcers
Diabetes is considered to be a significant risk factor for development of pressure sore in post-operative and critical care settings. 79 It is well known that persons with diabetes are at increased risk of neuropathic and arterial insufficiency-related foot and leg ulcers. In addition, a number of studies have explored the association of diabetes with pressure sores. 80,81 A diabetic foot ulcer is also influenced by pressure, but it occurs on the walking surface of the foot. Ulcers due to pressure on the back of the heel of a person with diabetes are pressure injuries. In a meta-analysis in 2017 it was found that patients with diabetes have 1.77 times risk of developing pressure ulcers in the perioperative period compared to patients without diabetes. 82 Hospital-acquired foot ulcers, an important cause of increased morbidity and cost of treatment have also been found to have significant association with diabetes. 83
Sensory loss due to diabetic neuropathy and decreased tissue perfusion due to vasculopathies have been thought to be the etiology of pressure sore in diabetics but exact cause–effect relationship is yet to be established. 84 Moreover, these pressure ulcers once formed are more difficult to heal since diabetes impairs wound healing and tissue remodeling. 85 Thus, there needs to be an improved awareness about this risk factor among health care workers. This also implies an improved assessment of patients with diabetes for possibility of development of pressure ulcer, inclusion of diabetes as a risk factor in scores for hospital-acquired pressure ulcers and timely and comprehensive management of these patients.
Hypertension and pressure ulcers
Ahmed et al. studied the effects of hypertension on wound healing and found that there was a significantly higher delay in healing of surgical sites of total hip arthroplasty patients when compared with normotensive patients undergoing this surgery. 86
The evidence regarding hypertension as a major factor in pressure ulcer formation is scarce and the opinion largely divided. A cross-sectional study of the general practitioners database of United Kingdom was performed and it was found that pressure ulcers had an inverse relation with hypertension. 87 The most probable cause for this appeared to be that patients with hypertension had decreased longevity, and as increased age is directly proportional to risk of pressure ulcer formation so it is possible to have obtained an inverse relation in this study. Contrary to this, a separate study concluded that there was a directly proportional relationship between pressure ulcer formation and hypertension. 88 This study was conducted on cross section of 78 patients admitted in ICU so there was a chance of other factors besides hypertension also being responsible for this inference.
They divided the study group into normotensive and hypertensive groups and assessed the risk of pressure ulcer formation as per the Norton, Braden, and Waterlow scales. Its only when they used the Waterlow scale that a significant association between risk of pressure ulcers and hypertension was detected. This could also mean that the Waterlow scale is a better scale for screening patients at risk of pressure ulcers as it is the only one that takes clinical evaluation and age into consideration. The probable reason for the increased risk was a high chance of injury to brain, kidneys, and heart owing to vascular pathology that would contribute to pathophysiology of pressure ulcer. 88
Pressure ulcers in cardiovascular diseases
Patients with advanced heart disease can develop pressure ulcers due to hypotension and decreased oxygenation. 89 This leads to muscle necrosis that results in predisposition to DTI. Certain studies have also documented the left ventricular ejection fraction (LVEF) to be an independent risk factor for pressure injury. 90 The study stated that a 5% decrease in LVEF can have the same risk as that of 10 years of increased age. Patients who develop hypotension in the course of their cardiac disease can also develop pressure ulcers either because of hypoperfusion or concomitant use of vasoconstrictors as a part of their management. 91
Certain studies quote about 29.5% patients who underwent cardiac surgery to be associated with pressure ulcers. 92 They have also documented that patients with preoperative atrial fibrillation have increased incidence of pressure ulcers and hemodilution may result in increased catabolism and inflammation hypoalbuminemia in cardiac surgical patients. The fall in albumin level to an extent of causing interstitial edema affects wound healing. 93 Pressure ulcers are found in up to 75% in patients with serum albumin levels below 3.5 mg/dL, 16% in patients with higher serum albumin levels. 94
Weight of adipose tissue can exert adequate pressure to cause occlusion of capillaries and hence decreased tissue perfusion. 15 In patients with high BMI, due to thinner capillaries, afferent and efferent arterioles take longer time to reach post-occlusive hyperemia in their tissue. Therefore, these patients are subjected to longer duration of tissue perfusion deficit when compared to others. However, adipokines induce stratum corneum replacement and help in the activation of keratinocytes. 95 Leptin, a mitogen factor for keratinocytes, promotes fibroblast activation and collagen synthesis. 96 The subcutaneous fat provides a cushion to prevent the pressure effects from causing damage to skin integrity. 18
Prevention of pressure ulcers
Prevention is the best means to manage pressure ulcers and the nursing care fraternity is a huge boon both in inpatient care and home care.
Dry and clean skin
It is necessary for the skin to be kept clean and dry to prevent skin peeling and consequent pressure ulcer formation. 97
Padding of pressure points
Appropriate padding or offloading of pressure points is imperative in preventing pressure ulcers. When wheelchairs are used for mobility of patients it should be custom fitted and padded in strategic high-pressure zones to prevent ulcers. Pressure mapping technologies have been very helpful to understand the various pressure trigger points and their results have been implemented in the custom-made wheelchairs built specifically for pressure ulcer and high-risk patients. A 30° tilt wheelchair has been designed based on the results analyzed using this technology. 98 Although this analysis may not be very helpful in bedbound patients it can still evaluate at risk sited for development of ulcers. They can also be used to evaluate the pressure relieving positions on established wounds.
Repositioning
Any patient at risk for development of pressure ulcers must be planned for repositioning that has to be individually tailored. The repositioning should also take care to prevent sheer and hence lifting is preferred over dragging the patient. 99
Pad dressings of wounds
Sacral and heel area-specific foam pads are available for dressing. 100 If the edge of these dressings is firm, they can also form pressure points. Such dressings should be discouraged from use. Silicone-adhesive foam dressings may decrease pressure ulcer risk. 101
However, dressings that trap heat can increase the risk of pressure ulcer formation. 102 The role of thermal conductivity of dressings in prevention and treatment of mattress pads like egg crate mattresses. Sheep skins are suitable for greater areas to provide pressure offloading. Silk-based bedlinens are favored over cotton as they produce less friction. 103 Polymeric membrane dressings, which limit inflammation when applied over intact skin, have been successfully used for prevention of DTIs and to resolve stage 1 pressure ulcers. 102,104
Nutrition
Apart from management of skin environment, a patient's nutrition also plays an important role in pressure ulcer prevention. The caretaker has to ensure a positive Nitrogen balance with vitamin and mineral supplementation in the patients and hence encourage protein-rich diet to them. 105 Prealbumin estimation from time to time enables one to assess the short-term adequacy of nutrition while albumin estimation assesses the same in long term.
Use of fat grafts and role of adipose stromal cells in pressure ulcer treatment
Marangi et al. 8 performed fat grafting for stage I DTI pressure ulcers, reversed tissue injury and hence prevented pressure ulcer occurrence in those patients 8 –11 (Fig. 5). The authors attributed the protective ability of fat grafting to the adipocyte stem cells and the changes in the fatty tissue layer.
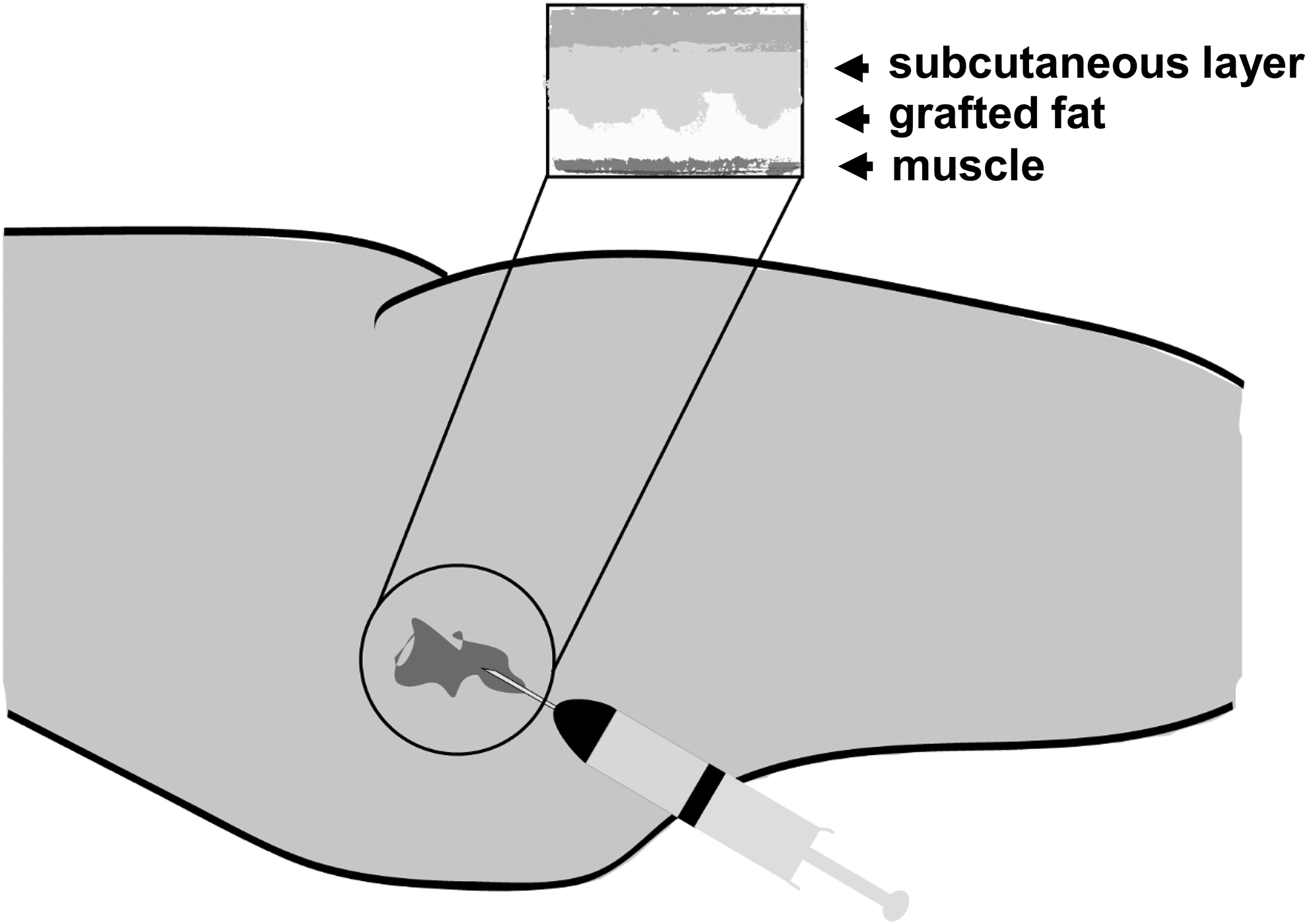
Fat graft for malnourished individuals with thin subcutaneous fat as a surgical technique to prevent pressure sores.
Our group has used quantitative methods by using computational three-dimensional methods to find out the statistical difference between the use of fasciocutaneous flaps that consists of predominantly fat and musculocutaneous flaps consisting of fat and muscle, in sacral pressure ulcers. 106 Systematic review shows significant difference in recurrence in the usage between fasciocutaneous and musculocutaneous flaps in the treatment of sacral pressure sores. 95 Vathulya et al. emphasized that it is important to match the depth of the defect rather than the use of muscle flaps to get increased blood supply to reconstruct such complex site healing. 107
In these ulcers, the principal soft tissue covering over the sacrococcygeal vertebrae is comprised anatomically of subcutaneous fat. It was found that even though flaps are time tested methods for surgical management of this pathology these methods did not show any statistical difference in the time frame with respect to recurrence. 107 The study revealed the importance of fat tissue in the management of pressure ulcers by acting as a cushion. Benefits of these fat grafts and adipose stem cells are due to decreased inflammatory reaction; higher production of extracellular matrix; and factors like vascular endothelial growth factor (VEGF), transforming growth factor beta (TGFβ), and epidermal growth factor (EGF) that aid in wound healing. 108
Since BMI may not predict the fat distribution as seen in previous studies, persons with same BMI might present with different subcutaneous tissue thickness and hence may face different degrees of risk with regards to developing pressure ulcers.
Ultrasonography (USG), a methodology that uses ultrasonic probe to analyze the various tissue planes can help us in measuring subcutaneous tissue thickness, we can use them to determine the need for fat grafting in these patients as a preventive measure. 109
In one of the methods, fat was harvested from abdomen, hips, and crural regions wherever the expected subcutaneous tissue thickness measured with USG is not less than the expected values based on normal BMI using the logistic regression equation: BMI = 16.99 + 0.39 times subcutaneous tissue. After pressure mapping, the fat was transplanted in to the subcutanoeus plane of areas prone to pressure ulcers including elbow and heel areas. 10,109 Algorithms addressing the pressure ulcer prevention before ulcer formation and management strategies post-ulcer formation have been discussed in Figs. 6 and 7. These algorithms have discussed cases based on BMI and skin thickness where fat grafting might lead to better outcomes.

Suggested therapy regimen for patients with high risk of developing pressure ulcer.
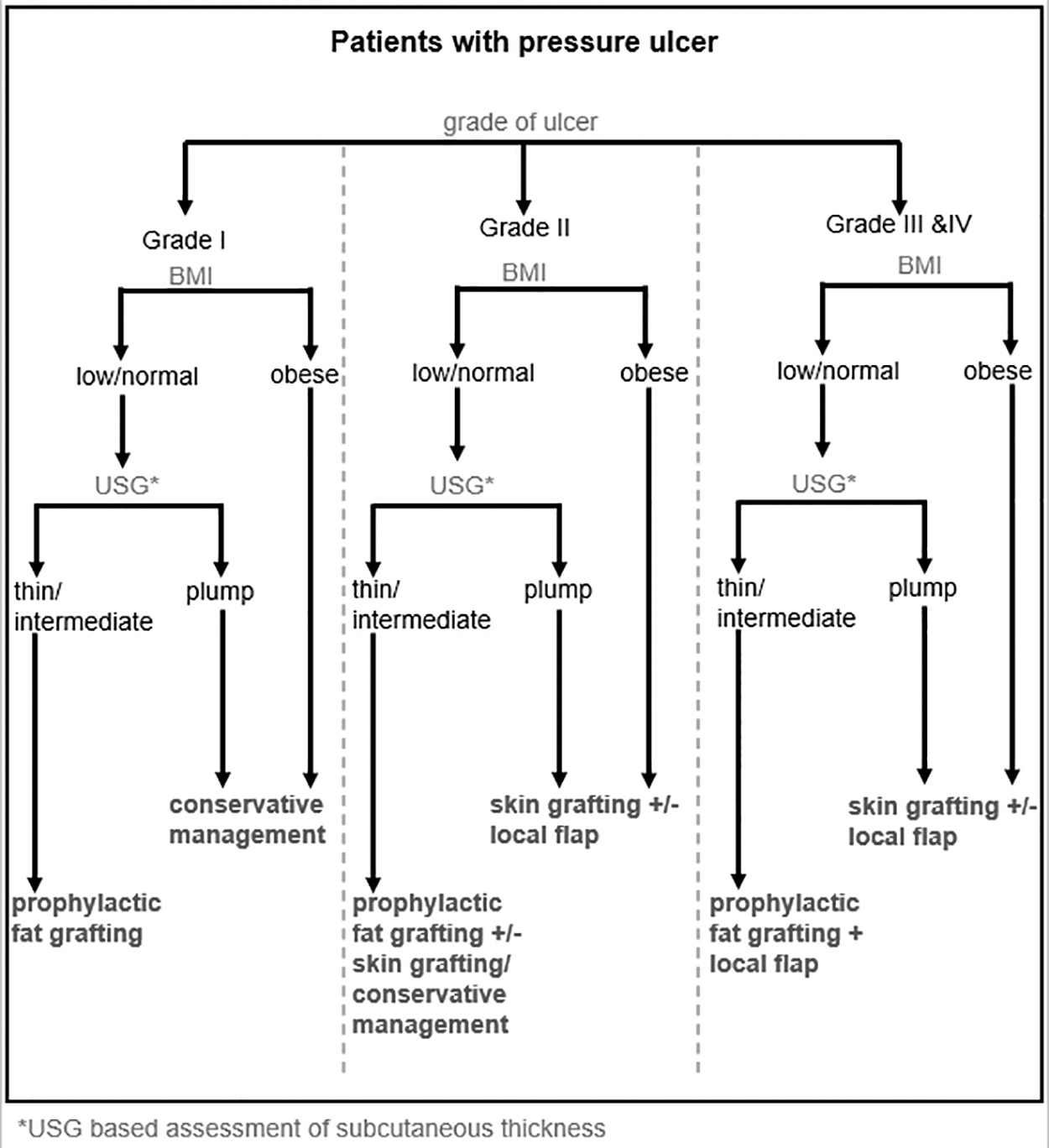
Suggested therapy regimen for patients with pressure ulcer.
The method of fat grafting proposed is as follows. The fat is harvested from abdomen, hips, and crural regions wherever the expected subcutaneous tissue thickness measured with USG is not less than the expected values based on normal BMI using the linear regression equation: BMI = 16.99 + 0.39 X Subcutaneous tissue (expected), as per study of Nadeem et al. 109 The fat is transplanted into the subcutaneous plane in areas prone to pressure ulcers including elbow and heel if required that are documented after a pressure mapping.
Limitations of the review
The limitation of this article is that very few randomized control studies (no level 1 studies) have been published correlating the role of adipose tissue and pressure ulcers. The review is also based on published literature on human and experimental studies in English language only. Also, the study is based on a narrative review and hence a formal meta-analysis of the available limited data has not been performed.
CONCLUSION
Although there are numerous risk prediction tools available in literature for pressure ulcers, there are some pitfalls in the parameters included in them. One such factor is BMI, the reason being, first it not easily measurable in all categories of patients and second, it does not highlight central adiposity and the adipose tissue present in the subcutaneous planes separately. In the current literature, the differentiation between central and peripheral obesity is largely unclassified and hence the interpretation of these studies is incomplete. Additional patient-based studies need to be done to understand the definitive role of subcutaneous adipose tissue in pressure ulcer initiation and progression so that this parameter can be added more accurately into a risk prediction tool. Conducting prospective case–control studies can be a first step in this direction.
TAKE-HOME MESSAGES
The need of the hour in management of pressure ulcers apart from prevention is to modify the previous prognostic scales for pressure ulcers by considering other factors like BMI, and subcutaneous fat.
Review of recently published studies reveal a need for further exploring our search on subcutaneous adipose tissue as a confounding factor for causing pressure ulcers.
Nutritional factors need to be objectively qualified in terms of adipose tissue thickness in the subcutaneous planes; comparison of waist–hip ratio for pressure sores occurring in the sacral, trochanteric and ischial areas; and triceps fold thickness.
Though the role of BMI is evident from literature, that of subcutaneous fat is still not defined.
Further insights can be gained through studies correlating ratio of subcutaneous fat thickness and BMI with the occurrence of pressure ulcers.
Footnotes
ACKNOWLEDGMENT AND FUNDING SOURCES
This work is supported in part by collaborative studies 207/IEC/IM/NF/2019 and 400/IEC/EM/2020 on pressure ulcers between AIIMS-Rishikesh and Indiana Center for Regenerative Medicine and Engineering, University School of Medicine, Indianapolis, IN. We thank Dr. Uddhav Timlisina, The State University New York, Buffalo for helping with the illustrations.
AUTHOR DISCLOSURE AND GHOSTWRITING
No competing financial interests exist. The content of this article was expressly written by the authors listed. No ghostwriters were used to write this article.
ABOUT THE AUTHORS
SUPPLEMENTARY MATERIAL
Supplementary Figure S1
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.