
Abstract
Significance:
The standard of care for deep burn wounds is eschar excision and autologous skin grafting within the first postburn days. However, when this is not practical due to medical reasons, unavailable surgical facilities, or lack of donor sites or other coverage, surgeons have used topical cerium nitrate (CN) in a cream with silver sulfadiazine (SSD) for over four decades to convert the eschar into a pliable and protective crust that facilitates the postponement or staging of eschar excision and grafting. CN+SSD treatment is reported to reduce dressing changes, improve patient comfort, and reduce bacterial burden, with unaffected epithelialization and few complications.
Recent Advances:
CN aqueous solutions applied topically alone or together with solid silver dressings in animal models have mitigated wound injury progression, wound microbial burden, and systemic immune dysfunction.
Critical Issues:
CN+SSD cream is not approved by U.S. Food and Drug Administration (FDA) and its efficacy in clinical trials has been challenging to demonstrate. One reason is that CN changes the eschar visibly, introducing unavoidable bias. Also, the market and patient population is small and burn wound presentation is highly variable.
Future Directions:
For use in settings wherein the once- or twice-daily CN+SSD cream dressing changes are least feasible (low-income, military, and mass casualty settings), it may be possible to develop a solid dressing containing cerium and silver that requires infrequent dressing changes. For future clinical studies, the trial design most suited to comparing silver-containing dressings with and without cerium may be paired difference of matched intrapatient wounds.

SCOPE AND SIGNIFICANCE
Topical cerium nitrate (CN) produces a hardened burn eschar that benefits burn management, especially when eschar excision/grafting must be delayed. CN combined with silver sulfadiazine (SSD) cream has been marketed or used in many countries for several decades, and burn surgeons have extoled its benefits in numerous publications. Nonetheless, CN+SSD cream is neither universally used nor U.S. Food and Drug Administration (FDA) approved. Herein, we review the use of CN in burn management, building on Garner and Heppell's excellent 2005 review, 1 highlighting the apparent mechanism of action, recent preclinical and clinical studies, and the potential regulatory pathway for CN-containing solid dressings in the United States.
TRANSLATIONAL RELEVANCE
Treatment of burns with a CN solution bath or CN+SSD cream in animal models has mitigated wound microbial bioburden, systemic inflammatory mediator levels, and burn-induced immune impairment. However, CN baths are not practical clinically and cream dressings require changing at least once daily. Therefore, solid dressings containing cerium and silver, which can be changed every few days and can temporize wounds and facilitate grafting postponement, can benefit patients and caregivers in military, mass casualty, and low-income settings, as well as hospitals.
CLINICAL RELEVANCE
Patients with extensive burns lacking available donor sites usually require allografts or xenografts. However, when these products are not available or patients cannot medically tolerate surgery, CN+SSD can facilitate postponing or staging of eschar excisions. The hardened eschar produced by CN treatment firmly adheres to the wound (for months), limits bacterial colonization, and allows partial-thickness burns to heal and full-thickness burns to be excised when surgery becomes an option. Additional benefits of CN+SSD treatment are fewer dressing changes and improved patient comfort with few complications. CN+SSD is used on partial- and full-thickness thermal burns.
BACKGROUND
Burn injuries
Every year in the United States, ∼50,000 people with burn injuries are hospitalized, 20,000 of them have burns that cover 25% or more of their body surface area, and ∼4,500 of these patients die from their burn injuries. 2,3 There is no published number of patients for whom grafting postponement is needed.
Infections of burn wounds
Over the past several decades, the survival of burn patients has significantly improved due to the use of topical antimicrobials and early eschar excision and grafting. 4 Burn shock was the leading cause of death after major burns in the 1960s, but as the management of burn shock improved, the leading cause of mortality has become infection, which is responsible for up to 50% of burn-related deaths. 5
Once the skin barrier is disrupted, microorganisms from the environment enter and the wound becomes colonization with gram-positive normal skin flora such as Staphylococcus aureus and Streptococcus species, usually within the first 48 h unless topical antimicrobial agents are used. 6,7 By days 5 to 7, gram-negative bacteria appear, such as Pseudomonas aeruginosa, Enterobacter species, Proteus, and Escherichia, which originate from respiratory or gastrointestinal flora. 7 Later, yeast and fungi can emerge and are an ominous sign associated with increased mortality. 8,9 The most common bacteria isolated from colonized burns in a prospective study of 49 burn patients were S. aureus (23%); Proteus mirabilis (22.7%); Streptococci species (15.9%); P. aeruginosa (4.5%); and Escherichia coli, Salmonella, and Klebsiella species (3.4% combined); and the total body surface area (TBSA) burned correlated with bacterial growth. 6
Infections can delay healing and contribute to the pathological immune dysfunction caused by large TBSA burns that is associated with sepsis and multiple organ dysfunction syndrome. 10,11
SSD cream in burn management
SSD cream was introduced in 1968 and has been considered the gold standard in topical burn treatment for >40 years (Fig. 1). 8,12,13 SSD continuously deposits silver ions on the burn surface. 7 To be effective, it must be applied in a layer at least 3.175 millimeters thick every 24 h. 14 It forms a yellow-white “pseudoeschar” that can obscure visualization of the burn as it heals or may be mistaken for the true eschar of a deeper burn. 7

Timeline of introduction of burn therapies and the researcher credited with the introduction.
CN and SSD cream in burn management
CN (2.2%) compounded with SSD (1%) in a cream was introduced in 1976. 15 Since then, the pliable protective crust resulting from CN+SSD treatment has been repeatedly reported to adhere well to the underlying tissue, resist infection, 16 and facilitate the postponement of eschar excision and grafting when patients are too ill to withstand surgery, donor sites or other types of coverage (allografts or xenografts, etc.) are not available, or surgical facilities are inaccessible. 17 Additional benefits that have been reported are fewer dressing changes, less soak through of exudate, less labor-intensive care, and greater comfort for patients. 1,17 –19 Pain scores have been reported to be reduced for CN+SSD versus SSD: 0.6 versus 1.2; −0.60 (95% confidence interval [CI] −0.70 to −0.50)—giving moderate certainty of evidence. 20
Systemic complications from topical application of CN are uncommon because absorption is essentially nil. 15 However, a rare potential complication is methemoglobinemia, which results from absorbed nitrate being reduced to nitrite that oxidizes the heme Fe2+ of hemoglobin to Fe3+ to create methemoglobin, which is unable to reversibly bind oxygen. 21,22 As the methemoglobin content of red blood cells increases, functional anemia and tissue hypoxia can occur. 23 Clinical manifestations depend on the level of methemoglobin. Cyanosis is often the first sign, and with rising methemoglobin levels, dyspnea, headache, and dizziness can occur. Further elevations in methemoglobin can lead to arrhythmias, acidosis, seizures, coma, and death. 24
The incidence of methemoglobinemia in 170 burn patients treated with topical CN+SSD cream was retrospectively evaluated. 25 A total of 10% of patients had methemoglobin levels >3% on arterial blood gas, and 2% had levels >10%. Most of these cases did not exhibit clinical symptoms of methemoglobinemia. Five patients were treated with methylene blue, which acts as an artificial electron acceptor for reduction of methemoglobin. 25
Another potential complication is the possible buildup of silver and cerium in the liver. A severely burned infant treated with CN+SSD for 3 months had a large amount of silver in the liver and kidney, but cerium was only detected in liver in a trace amount. 26
Few complications were observed in 853 burn patients treated with CN+SSD (Flammacerium) at the Burn Centre of Martini Hospital in The Netherlands, between 2009 and 2014. 27
Regulatory status of CN+SSD cream
Although CN+SSD is not FDA approved, it is marketed under the trade name Flammacerium (Alliance Pharma PLC, United Kingdom) in Europe and Dermacerium in South America (Silvestre Laboratories, Brazil). Marketing authorization for the cream is in effect in Belgium, Luxembourg, The Netherlands, France, and Spain (European Medicines Agency, Article 57 product data); it is used on a named-patient basis in the United Kingdom. 1,28 Market authorization was issued in 1983 in The Netherlands (Registration Number: RVG 09707) where the cream is categorized as a cutaneous antibacterial agent.
In the United States, where CN+SSD cream originated, 15,29 some burn centers have used it since the1970s. 25,30 After the World Trade Center attacks on September 11, 2001, the FDA issued emergency use authorization. 31 In 1999, the cream (Flammacerium) was designated an orphan drug for the “prevention of mortality in severely burned patients”; orphan drug status gives the sponsor incentives for development (e.g., tax credits and fee waivers). On route to FDA approval, in the early 2000s, Flammacerium was tested in a large prospective randomized clinical trial, and compared with SSD, 31 for the treatment of severe burns (TBSA+age >90 and predicted mortality >80%); the trial was powered to detect a 20–30% reduction in mortality. 1 However, results were never reported.
CN aqueous solution baths
CN administered alone through a single 30-min aqueous bath was reported to benefit burn patients and caregivers in an observational study. 32 The patients (64 patients, aged 16–74 years with 30–90% TBSA burns) were bathed in CN solution (0.04 M) within 4 h of admission to a Swiss hospital (Kantonsspital, Basel). Sixty-one of the 64 patients survived, which far exceeded the expected survival compared with historical data. 32 Reported benefits included the ability to delay eschar excision and grafting due, at least in part, to the firmly adherent eschar. In addition, the wounds were noted to be clean and odorless and to accept skin grafts readily, with epithelialization as expected and pressure on caregivers minimized. 32
CN effects in animal models
Aqueous CN
Besides clinical observations of benefits of CN solution bathing, in animal models CN aqueous solutions have mitigated burn sequelae: edema, 33 immunosuppression, damage-associated molecular patterns (DAMPs) in circulation, 34 cytokines in wound tissue and circulation, 34,35 the lethality of burned skin, 36 wound bioburden, 34 and wound progression. 37
Aqueous CN combined with solid silver dressings
In recent studies using a rat model, burns were treated with a 30-min CN aqueous bath followed by a solid silver dressing that was overlaid with a CN wet compress for 2 days as compared with the control (water bath and wet compress overlying the silver dressing). On day 7, the CN treatment lowered proinflammatory cytokines and chemokines, neutrophils, and skin flora in the wound tissue, as well as burn-induced DAMPs in circulation. 38 Thus, the combination of the CN treatment and the solid silver dressing reduced wound inflammation and resident flora and circulating DAMPs, an indicator of systemic inflammation.
CN was initially used to treat burns because of bacteriostatic activity in vitro against a broad spectrum of bacteria with minimum growth inhibitory concentrations of 1–10 mM. 1,39 However, some results were conflicting, possibly because cerium ions were inactivated by binding to proteins or phosphates, 40,41 or silver's antimicrobial activity predominated. 1,41 –43 Recently, full-thickness burns in a rat model were contaminated with P. aeruginosa and then bathed in CN solution, covered with Silverlon™ (a solid silver dressing), and overlaid with a CN wet compress; the pathogen was reduced ∼1 log versus the control without CN.*
CN+SSD cream
CN+SSD cream has recently been compared with SSD cream in a rat burn model. The creams were applied topically to ∼20% TBSA burns immediately and then twice daily for 28 days. Wound size (on days 7, 14, 21, and 28) between the two treatments did not differ. 44
DISCUSSION
Cerium's hypothesized mechanism of action
Cerium is a lanthanide and a rare-earth element (although not rare). It was originally investigated because of its abundance, ease of purification, and nontoxicity. 1 Although it forms a variety of salts, cerium nitrate [Ce(NO3)3] has been principally used in wound treatment 1 (Fig. 2). Cerium (Ce3+) has an ionic radius similar to calcium (Ca2+) but a stronger electronegativity 45 and, therefore, can displace calcium from biological molecules (as can other lanthanides), altering biological processes. 1,17,46
Chemical structure of CN. CN, cerium nitrate.
In producing the hardened eschar, cerium ions have been postulated to bind to pyrophosphate, 47 releasing calcium and pyrophosphate's inhibition on the formation of hydroxyapatite crystals (Ca5(PO4)3). 1,48,49 Images of the so-called calcified eschars after CN+SSD treatment are shown in Figs. 3 –6.

Scald to the lower limb of a 71-year-old male.
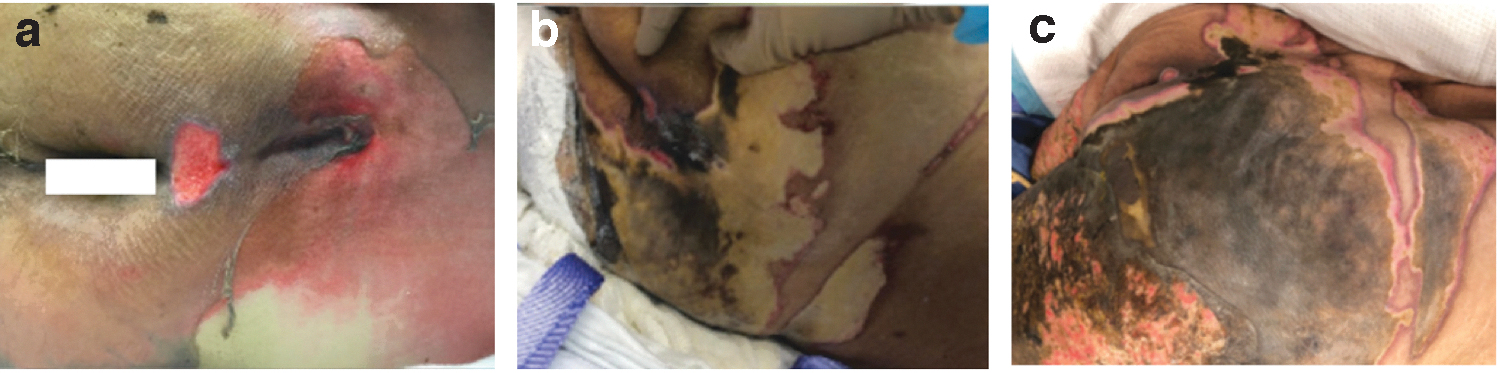
Third-degree burn (house fire) to the sacrum of an 85-year-old male.
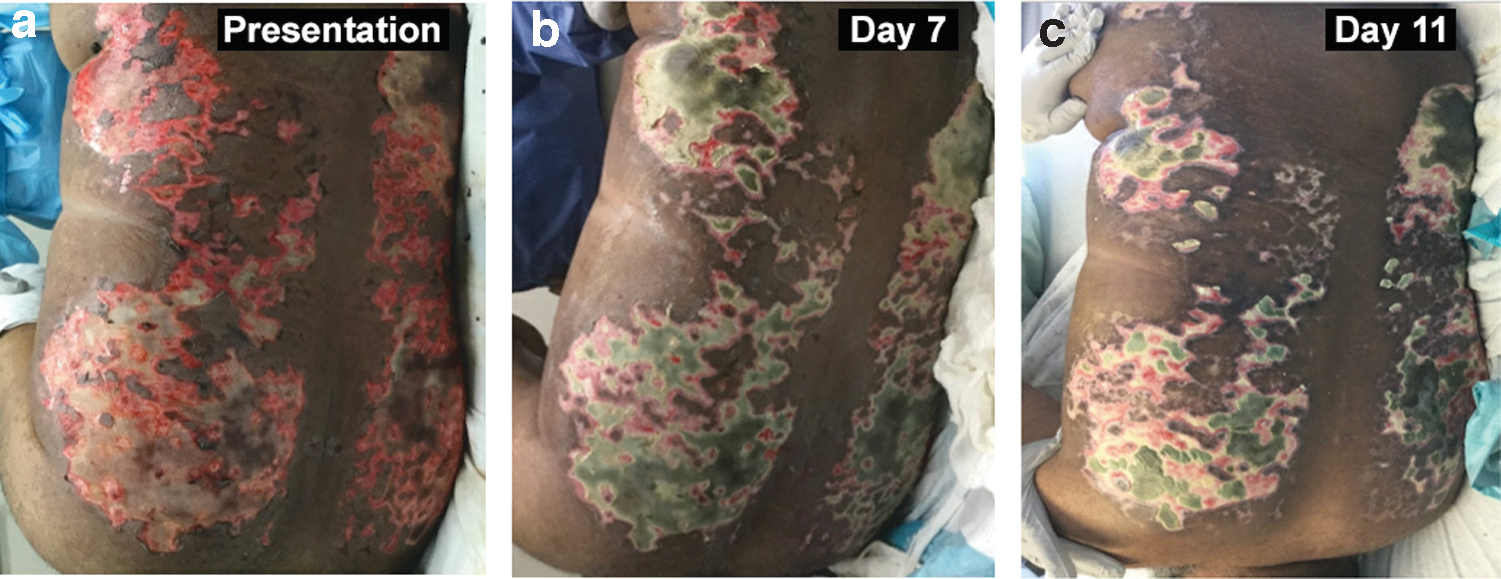
Thermal burns to the back of a 53-year-old male.

Scald burn to the right torso of a 69-year-old male.
The anti-inflammatory and wound-progression inhibitory activities of CN have been suggested to result from displacement of calcium from proteins and alteration of calcium-dependent processes extracellularly (since cerium does not cross mammalian cell membranes). 1,50 These perturbed calcium-dependent processes could potentially involve calmodulin, complement, calcium channels, S100 proteins, the lipid protein complex burn toxin, 51 blood clotting, 52 and many others. 1,53 –55
The anti-inflammatory effect of cerium, demonstrated in animal models, has also been suggested by a clinical study that compared two site-matched deep dermal burns, one treated with CN+SSD and the other with SSD. The CN+SSD-treated wounds showed lower leukocytic infiltration. 47
Clinical evidence of cerium's benefits
Prolonged treatment with SSD can produce a macerated eschar. However, the hardened eschar after CN+SSD treatment remains adherent for many weeks, presents an apparent barrier to microbial colonization/infection, requires fewer dressing changes, improves patient comfort, and facilitates grafting postponement. These observations of CN treatment have been reported by numerous clinicians for several decades. 7
In early clinical studies that lacked controls, additional potential benefits of CN+SSD treatment were reported: improved survival and lower colonization/infection. Animal model studies have also demonstrated that CN can lower inflammation and mitigate wound progression. However, these effects of CN observed in controlled animal studies and uncontrolled clinical trials have yet to be supported by strong clinical evidence.
A major issue in the clinical evaluation of CN+SSD versus SSD is formation of the greenish-yellowish and relatively dry eschar that makes it impossible for clinicians or patients to be blinded; thus, the study design is necessarily open label with inherent bias. 18,56 Additional imprecision is due to the difficulty in balancing group characteristics and the enrollment of too few participants with event rates (e.g., infection, mortality) that are too low to provide sufficient statistical power. 57 Clinical studies of CN+SSD versus SSD are summarized in Fig. 7 and discussed hereunder.
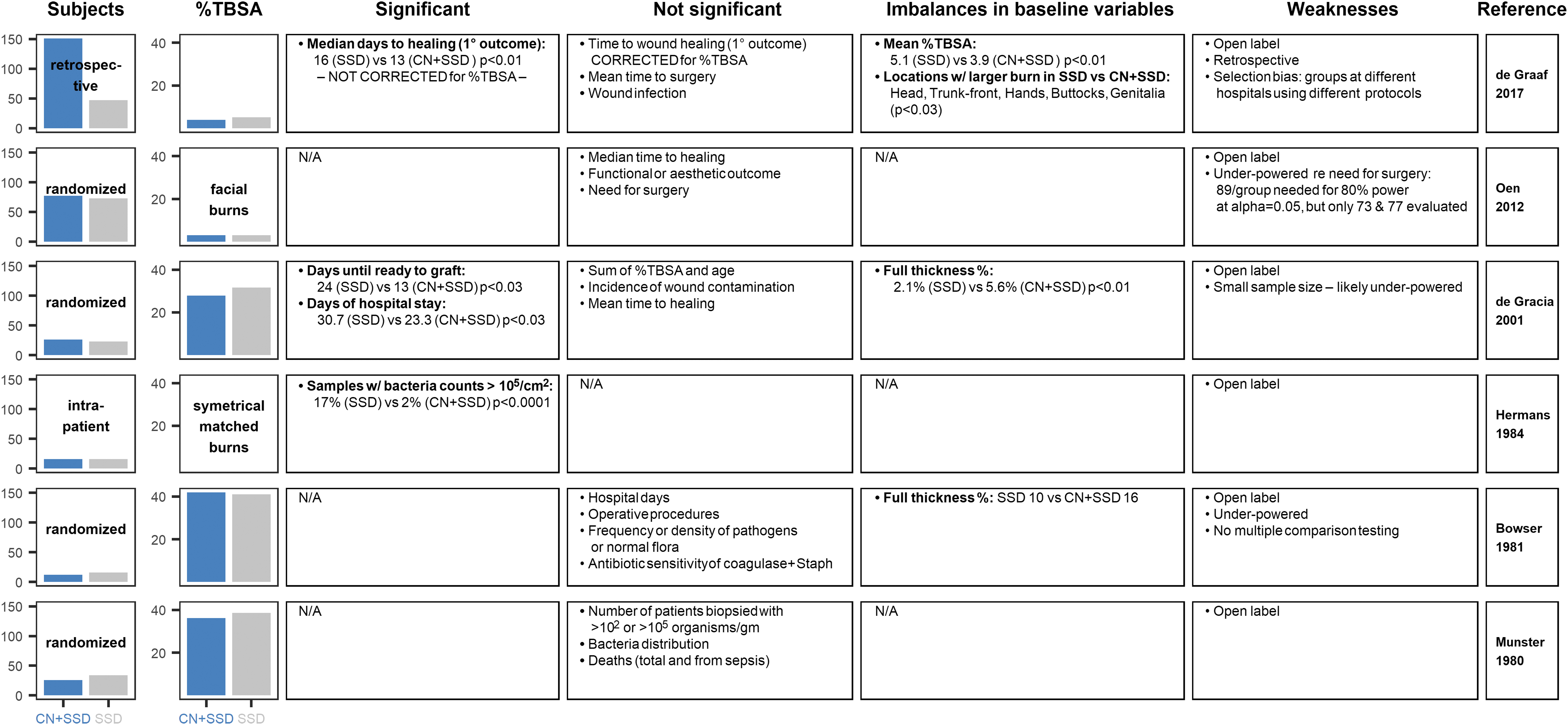
Summary of clinical trials comparing CN+SSD with SSD creams.
Bacterial colonization/infection
Early uncontrolled clinical studies of CN+SSD reported that it decreased bacterial colonization, gram-negative colonization, and pseudomonal infection in particular. 1,15,29,58 –60 However, these findings mostly have not been replicated in controlled studies that are thought to be confounded by error in sampling across large wounds, including of only infection-suspected areas, as well as by the potential inherent bias in sampling calcified versus noncalcified wounds. 57,60
Prospective studies have reported either a greater percentage of gram-negative pathogens in the CN+SSD group in one study 43 or no significant differences in microbial bioburden between the CN+SSD and SSD groups in several studies. 18,30,56 A Cochrane Database review in 2017 concluded, “It is [also] uncertain whether infection rates differ for SSD plus cerium nitrate, compared with SSD alone (low-certainty evidence).” 20
However, one study assessed bacterial counts on symmetrical burns on 16 patients who were left-right matched and randomized to receive SSD or CN+SSD. More viable bacteria counts of >105 per cm2 were found on the SSD-treated (204 samples) versus the CN+SSD-treated (240 samples) sides (17% vs. 2%, p = 0.0001); although details of the sampling method or the bacterial composition were not reported. 16 Burns treated with CN+SSD may resist colonization because they are stabilized by being calcified, adherent, and dry. 16,30
Re-epithelialization
Early observational studies of burns treated with CN+SSD reported that re-epithelialization occurred at the expected rate. 32 In addition, our recent pilot retrospective study of 142 patients (mean TBSA of 9.9%) at MedStar Washington Hospital Center, Washington, DC (Shupp, Moffatt and coworkers), has led us to conclude that CN+SSD successfully temporizes burn wounds and supports re-epithelialization. 61
Another recent retrospective study (de Graaf et al.) at two Dutch burn centers, from 2009 to 2013, evaluated children with partial-thickness scalds up to 10% TBSA (SSD: 47 patients; CN+SSD: 151 patients) and found a significantly shorter median time to healing of 13 days for CN+SSD versus 16 days for SSD (p < 0.01). However, when corrected for the smaller %TBSA of the CN+SSD group, there was no significant difference. In addition, the study was retrospective and analyzed CN+SSD treatment used at one center with SSD treatment used at a different center. 62
As reviewed by Garner and Heppell, 1 an open trial of randomized patients was performed at two burn services in Manila from 1992 to 1993 that compared 30 patients treated with CN+SSD and 30 patients treated with SSD. Patients were >4 months of age with >15% TBSA and a mean TBSA of 28–31%. The CN+SSD group was reported to show an 8-day average earlier wound closure (partial-thickness burns) and an 11-day earlier acceptance of grafts (full-thickness burns) that translated to a 7-day shorter hospital stay. 18 However, this study was biased due to the open-label design (as all others) and is likely underpowered.
A more recent randomized controlled trial, from 2006 to 2009, of adult patients admitted to Dutch burn centers with acute facial burns evaluated 77 patients treated with CN+SSD and 73 patients treated with SSD; there was no difference in the time to wound healing, the need for surgery, or the functional or aesthetic outcome (at 3–12 months after burn). 56 However, even this study was underpowered as the authors calculated that to identify a 20% difference in the mean number of patients requiring surgery (from 45% to 25%), 80 patients per group (without dropouts) were needed.
For assessing CN effects on burn wound re-epithelialization, one of our groups (Leung) is currently performing studies in a porcine partial-thickness burn model.
Mortality
Earlier studies reported that CN reduced deaths from large burns as compared with historical data. 1,58 –60 However, a prospective study by Munster et al. in 1980 evaluated 60 burn patients, with an average TBSA of 37% who were randomized to either CN+SSD or SSD treatment; the total number of deaths and deaths due to sepsis between the treatments did not differ. 30
Two more recent prospective studies of CN+SSD versus SSD (de Gracia 18 and Oen et al. 56 ) were combined in a Cochrane review meta-analysis. 20 The %TBSA burned for the CN+SSD versus SSD groups was 9.8 versus 9.3 for the de Gracia study and 28 versus 31 for the Oen study. In the combined CN+SSD group, there were 2 deaths in the 108 patients and the combined SSD group had 9 deaths in 106 patients. The relative risk was 0.22 (95% CI 0.05 to 0.99), which is low-certainty evidence because of the wide and fragile CIs resulting from low number of participants and events. 20
As already stated, in the early 2000s, a large prospective randomized clinical trial was undertaken to compare Flammacerium (CN+SSD) and SSD in the treatment of severe burns (TBSA+age >90 and predicted mortality >80%) that was powered to detect a 20–30% reduction in mortality. 1,31 However, the results were never reported. As to whether CN treatment reduces mortality, either no benefit may exist or the heterogeneity of burn patients makes it difficult to construct a well-powered trial. 28
Proposed scenarios for use
The single most important factor in the reduction of mortality from burns over the last several decades has been early eschar excision. 14 When a patient presents with a large surface area burn, the clinician must determine whether early excision and grafting is feasible and whether the patient can tolerate surgery. Patients with large burns may be hemodynamically unstable on presentation, develop burn shock early in their hospital course, or have concomitant traumatic injuries that would limit aggressive excision with inherent blood loss. Any of these scenarios must be addressed before surgical excision of burns, similar to the damage control approach used in trauma. 1,27,63,64 Alternatively, burn patients may have comorbidities that make them unfit for surgery or unable to tolerate general anesthesia.
Patients with extensive burns may only have a small amount of healthy donor skin to cover excised burns. In such cases, the staging of burn excisions can be facilitated by treating the eschar with CN+SSD while donor sites re-epithelialize and can be reharvested. 65 When adequate donor skin is not available, temporary wound coverage of large TBSA burns can be achieved with stored allograft skin, xenografts, and tissue-engineered biosynthetic products. 28 These expensive products are not readily available in many areas of the world, limiting the option of early excision and grafting.
Early eschar excision is also not feasible during military combat or in a mass burn casualty event that overwhelms limited resources. 28 An ideal dressing in these settings would require minimal time commitment from skilled staff, consume minimal resources, and prevent burn wound sepsis. 14 In such situations, CN+SSD is considered an alternative to surgery. However, the once- or twice-daily dressing changes for applying CN+SSD cream are not practical—a solid dressing that delivers cerium and silver would be more practical. Silver-impregnated dressings are lightweight and tolerant to temperature extremes. They have been used to manage burn wound infections in combat and have been stockpiled for mass casualty use by the Biomedical Advanced Research and Development Authority (BARDA), U.S. Department of Health and Human Services (HHS). 66 –68 Other types of solid wound dressings, such as films or hydrogel sheets, may also be suitable for delivering cerium and silver. Such dressings should deliver these metals to the burn for 3 to 7 days, so few dressing changes are needed.
Potential of a solid dressing containing cerium and silver
CN combined with solid silver dressings was recently tested in a rat model using three commercially available silver-impregnated dressings: Acticoat™, Mepilex™, and Silverlon. 38 The burns were first soaked in an aqueous CN bath for 30 min and then covered with a silver dressing overlaid with a CN solution wet compress for 2 days. Regardless of the silver dressing (which differed in quantity and chemical or physical form of silver)—the burns treated with CN (vs. water controls) had significantly lower interleukin 1 beta (IL-1β) and growth-regulated oncogene/keratinocyte chemoattractant (GRO/KC) (and there was a trend toward lower interleukin 1 alpha [IL-1α] and macrophage inflammatory protein-1α [MIP-1α]) and bacterial bioburden (resident skin flora in wound biopsies). Thus, CN interfered with neither the antimicrobial activity nor the barrier function of the silver dressings, but rather enhanced their antimicrobial and anti-inflammatory properties. 38
Possible regulatory path for a cerium and silver solid dressing
CN has a long history of safe clinical use for managing burn patients, including those who require the conservative approach of delaying eschar excision and grafting, such as children, elderly, and patients with severe burns or comorbidities. Since the number of such patients and the market for such a product are small and constructing an adequately powered trial is difficult and expensive, the most appropriate regulatory path may be as a humanitarian use device (HUD), which is a medical device intended to benefit not more than 8,000 patients per year in the United States (Section 3052 of the 21st Century Cures Act, Pub. L. No. 114-255). For this path, a humanitarian device exemption (HDE) marketing application is used that is exempt from the demonstration of effectiveness (Sections 514 and 515 of the FD&C Act). Alternatively, a 510(k) marketing clearance can be sought for a barrier dressing (FDA product code FRO, unclassified level of control) that uses a solid silver dressing as the predicate device and demonstrates the known safety of cerium.
SUMMARY
SSD+CN has been used for >40 years and as compared with SSD, it requires fewer dressing changes and evidently provides greater comfort to patients and similar or improved antimicrobial activity and healing. Few complications have been observed. CN is an efficacious and safe alternative to early excision and grafting.
TAKE HOME MESSAGES
CN stabilizes the burn eschar; the yellow-greenish hardened eschar adheres to the underlying tissue and appears to resist infection, as suggested by a study of matched intrapatient burn wounds—samples having bacteria counts of >105 per cm2 were 17% on the SSD side and 2% of the CN+SSD side (p < 0.0001)—whereas other studies of randomized groups of patients treated with CN+SSD versus SSD found no difference in colonization or infection.
The stabilized eschar by CN has been repeatedly reported for many decades to require fewer caregiver hours (e.g., less frequent dressing changes).
Pain scores were reduced for CN+SSD versus SSD: 0.6 versus 1.2; −0.60 (95% CI −0.70 to −0.50) with moderate certainty of evidence. 20
Healing differences between CN+SSD and SSD treatments in randomized clinical trials have not been found.
Clinical studies of CN effectiveness are necessarily open label since CN changes the eschar visibly; therefore, bias is inevitable. Additional imprecision in clinical trials of topical treatments for burns comes from too few participants and event rates. 57
Animal studies have demonstrated that CN mitigates wound progression, suppresses systemic immune dysfunction, and reduces wound bioburden.
CN is an efficacious and safe burn wound treatment.
Footnotes
AUTHORS' CONTRIBUTIONS
R.D. carried out drafting and revising the article, analysis of data, conception, and design. P.D. carried out drafting and revising the article, analysis of the data, conception, and design. L.M. was responsible for revising the article and analysis of the data. K.L. was responsible for revising the article, analysis of the data, conception, and design. J.S. was responsible for revising the article, analysis of the data, conception, and design.
ACKNOWLEDGMENTS AND FUNDING SOURCES
P.D. is supported by the U.S. Army Research Laboratory and the U.S. Army Research Office under contract W911NF1310376 to The Geneva Foundation. K.P.L. is an employee of the United States Government. The study presented is part of his official duties. The views expressed in this article (book, speech, etc.) are those of the author(s) and do not reflect the official policy or position of the U.S. Army Medical Department, Department of the Army, DoD, or the U.S. Government. The authors have no funding information to declare.
AUTHOR DISCLOSURE AND GHOSTWRITING
No competing financial interests exist. The content of this article was expressly written by the author(s) listed. No ghostwriters were used to write this article.
ABOUT THE AUTHORS