
Abstract
Significance:
Obesity affects one-third of the U.S. population and lymphedema is a chronic disorder without a cure. The relationship between obesity and lymphedema has important implications for public health.
Recent Advances:
Extreme obesity can cause lower extremity lymphedema, termed “obesity-induced lymphedema (OIL).” OIL is a form of secondary lymphedema that may occur once an individual's body mass index (BMI) exceeds 40. The risk of lymphatic dysfunction increases with elevated BMI and is almost universal once BMI exceeds 60. Patients with OIL also may develop areas of massive localized lymphedema (MLL).
Critical Issues:
Individuals with OIL are in an unfavorable cycle of weight gain and lymphatic injury. As BMI increases lymphedema worsens, ambulation becomes more difficult, and BMI further rises. The fundamental treatment for OIL is weight loss. Resection of areas of MLL and lower extremity volume reduction are performed when the BMI is lowered to <40 to reduce complications and recurrence.
Future Directions:
The mechanisms by which obesity causes lymphedema are still being elucidated. Although lymphatic function can improve following weight loss, it is unclear whether lymphedema may be completely reversed.

SCOPE OF REVIEW AND SIGNIFICANCE
Obesity is a major public health problem that affects at least one-third of the U.S. population. Lymphedema is an incurable progressive condition. Recently, severe obesity was recognized to cause lower extremity lymphedema, termed “obesity-induced lymphedema (OIL).” Obesity and lymphedema have a reciprocal relationship and each condition worsens the other. This review presents the most current understanding of OIL since the senior author's previous reviews on this topic 1 to enhance the management of this often misunderstood condition.
TRANSLATIONAL RELEVANCE
The clinical observation that obesity is a risk factor for developing lymphedema after cancer treatment, and that severe obesity can independently cause the disease, has led to basic research in this field. Animal models have recapitulated the negative effects of obesity on lymph flow and uncovered mechanisms by which obesity damages lymphatic function. Weight loss and pharmacological inhibition of lymph-mediated fibroadipose deposition have been shown to be beneficial experimentally. These observations may be translated to humans in the future.
CLINICAL RELEVANCE
Obesity leads to several comorbidities that can be improved after losing weight. Unlike other problems associated with obesity, however, lymphedema may not be reversible following weight loss. Consequently, obese patients must be counseled that they are at risk for potentially irreversible lymphedema once their body mass index (BMI) exceeds 40. Subjects at risk for OIL, or who already have the condition, are managed with weight loss. Operations to reduce leg volume or remove areas of massive localized lymphedema (MLL) are performed only after patients have achieved their lowest possible BMI.
BACKGROUND
Obesity and lymphedema have a reciprocal relationship. Obesity increases the risk and morbidity of lymphedema and can cause the disease. Lymphedema, in turn, results in subcutaneous adipose deposition that contributes to obesity. The relationship between the two diseases has important consequences for public health. Obesity affects one-third of the U.S. population (6% have a BMI >40), 2 while 1/1,000 Americans have lymphedema. 3
The negative effects of obesity on lymphatic function were first recognized in patients who develop upper extremity lymphedema following breast cancer treatment. BMI is the variable most closely associated with lymphedema after axillary lymphadenectomy and radiation; the greater the BMI, the more likely the patient develops lymphedema. 4 Elevated BMI also increases the morbidity of established lymphedema. Obese individuals with lymphedema are more likely to have infection, hospitalization, and moderate or severe leg overgrowth, compared with normal-weighted patients. 5
Our group has shown that extreme obesity can independently cause lymphedema and named the condition OIL. 6 Lymphatic dysfunction can occur once a patient's BMI exceeds 40; the risk is 6% if the BMI <50 and 90% when the BMI is >60 (Fig. 1). 7 The BMI threshold to cause OIL in nonambulatory patients with neuromuscular disease is lower; these patients can develop OIL once their BMI exceeds 30. 8 OIL can predispose patients to localized areas of overgrowth termed MLL. 9 Sixteen percent of patients managed in our Lymphedema Program have OIL. 10

The risk of OIL correlates with BMI and requires lymphoscintigraphy for definitive diagnosis.
DIAGNOSIS
History
Before OIL can be diagnosed, other potential causes of lymphedema are ruled out. Individuals are asked about risk factors for primary lymphedema (e.g., family history of the disease). If an individual developed swelling before adulthood or before becoming obese, then they likely have primary lymphedema. Obese patients who have had lymph node radiation, lymphadenectomy, or penetrating trauma to the inguinal region have secondary lymphedema from the injury. Patients are queried about travel to areas endemic for filariasis to rule out an infectious cause of lymphedema. Individuals with OIL typically state that they were previously healthy and had either a normal (<25) or overweight (25–30) BMI as a teenager and young adult. As the individual gained weight they noted swelling of their extremities, followed by a worsening cycle of weight gain and lower extremity enlargement.
The most important risk factor for OIL is the patient's maximum BMI history. Individuals who currently or previously had a BMI >40 can develop the disease; the likelihood is much higher if a patient has had a BMI >60. 7,11 A history of cellulitis of the extremities also suggests possible underlying lymphatic dysfunction because lymphedema predisposes individuals to infection. Obesity affects both extremities and thus patients with OIL complain of bilateral symptoms. An obese individual with unilateral findings is less likely to have OIL.
Physical examination
OIL is difficult to diagnose by physical examination because an obese leg with or without lymphedema appears similar. The Stemmer sign (inability to pinch the skin on the dorsum of the foot proximal to the second toe) is 92% sensitive and 57% specific for the diagnosis of lymphedema. 12 This test, however, is less-sensitive in obese patients (higher false-positive rate) because their feet have increased subcutaneous adipose tissue. 12
Imaging
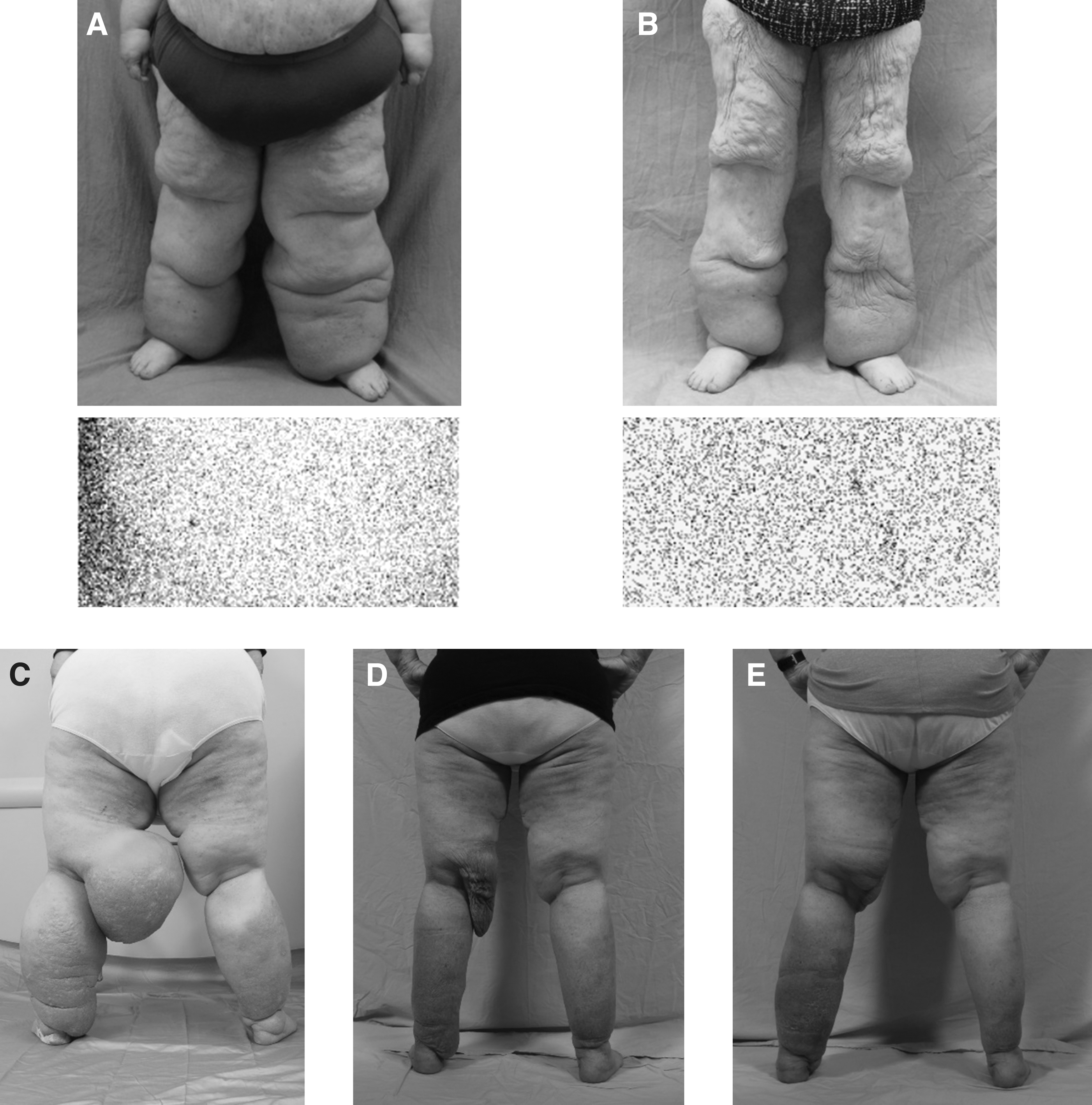
Although the likelihood of OIL can be predicted by BMI, 7 definitive diagnosis requires lymphoscintigraphy. 6,7,11 This test is 96% sensitive and 100% specific for lymphedema 13 and all patients being evaluated for OIL have this study. Lymphatic dysfunction is defined as delayed transit of radiolabeled colloid to regional lymph nodes, dermal backflow, presence of abnormal nodes, and/or tortuous collateral lymphatic channels. 14 –16
CLINICAL FINDINGS
OIL affects the lower extremities and the risk increases with elevated BMI: BMI <40 (0%), 40–49 (17%), 50–59 (63%), 60–69 (86%), 70–79 (91%), and >80 (100%) (Table 1). 7 Two-thirds of the patients have a history of infection, and lymphoscintigraphy shows abnormalities bilaterally (75%) or unilaterally (25%). 5,10,11 Gender, comorbidities, and duration of obesity do not play a role in the development of OIL. 11 OIL also can affect the upper extremity; the patient with the highest BMI history in our cohort (105) had arm lymphedema by lymphoscintigraphy (his BMI at the time of the study was 60). 17
Increasing body mass index predicts the risk of lymphedema
From Greene and Sudduth. 7
MLL of the lower extremity is present in 60% of patients with OIL and involves the thigh (94%; 2/3 bilateral, 1/3 unilateral), genitalia (18%), and suprapubic area (12%). 9 The probability of patients with OIL developing MLL is directly related to their BMI: BMI = 40 (4%), BMI = 50 (15%), BMI = 60 (40%), BMI = 70 (75%), and BMI = 80 (92%) (Table 2). Patients with OIL and a BMI >61 have 21 times greater odds of developing MLL versus a BMI <61. 9
Elevated body mass index correlates with the development of massive localized lymphedema
From Maclellan et al. 9
PATHOPHYSIOLOGY
Several mechanisms may explain the development of OIL. The upper limbs should be more resistant to developing the condition than the legs because adipose deposition in obese patients affects legs more than arms. Lymph drainage from the upper limbs also is closer to the central venous circulation. Transporting lymph proximally from the legs against gravity is more difficult.
Lymph transport depends on the function of the lymphatic vasculature (clearance) and the volume of lymph produced by the tissues (load). One hypothesis to explain OIL is that the lymphatics in the extremity are normal, but are unable to transport the increased volume of lymph. As the patient's BMI rises, the amount of lymph produced by the leg increases, while ambulation/muscle contraction to transport the fluid decreases. Clinical evidence supporting this theory is the observation that nonambulatory individuals develop OIL at a lower BMI than ambulatory patients. 8 Because this patient population is unable to walk and has nonfunctional lower extremity muscles, a lower BMI “second hit” is necessary to overwhelm lymph transport. Excessive pressure from the weight of the tissue and/or progressive skin folds might also reduce lymphatic flow by collapsing lymph vessels.
Inflammation from excess subcutaneous adipose may destroy lymphatic vasculature and also contribute to OIL. This mechanism is supported both clinically and experimentally. Patients with OIL continue to have lymphatic dysfunction after significant weight loss to a BMI below 40. 18 Obesity in humans impairs lymphatic drainage of macromolecules, which promotes inflammation. 19 Animal studies have shown that obesity impairs lymphatic transport, damages and reduces lymphatic vessels, and increases inflammation. 20 –22 Obese mice also exhibit decreased lymphatic gene expression (e.g., LYVE-1, PROX-1, VEGFR3) in endothelial cells. 23 Recent studies show that elevated inducible nitric oxide synthase causes nitrosative stress that injures lymphatic vessels. 24 Animal models have illustrated that weight loss can improve lymphatic dysfunction. 25,26
The pathophysiology of MLL is unclear. As BMI continues to rise, skin folds might obstruct lymphatics resulting in localized overgrowth. 8 The thighs might be preferentially affected because there is more skin laxity compared with the distal extremity. Histologically, MLL is different than typical lymphedema, which exhibits subcutaneous fibroadipose tissue with inflammation. 27 MLL histologically appears similar to well-differentiated liposarcoma (WDL) because widened septa resemble the fibrous bands of WDL. 28 MLL, however, does not exhibit significant nuclear atypia present in WDL. 28
MANAGEMENT
Patients with OIL are initially treated like other individuals with primary or secondary lymphedema. They are prescribed compression garments as well as pneumatic compression. Individuals are advised to avoid incidental trauma that might lead to cellulitis. The infection rate is higher in patients with OIL (58%) compared with patients with other causes of lymphedema (24%). 10 Exercise is encouraged because it helps lower BMI and encourages muscle activity to promote lymph transport. 29
Definitive management of OIL requires treating the underlying cause of the disease, which is the patient's weight (Fig. 2). We refer patients to a bariatric surgical weight-loss center. While a minority of individuals are able to lose significant weight by diet and exercise, most benefit from a surgical weight-loss procedure. Reducing the patient's BMI is the only way to stop the vicious cycle of inflammation, adipose deposition, further lymphatic damage, enlarging extremity size, and the development of MLL (Fig. 3). Wounds involving MLL typically are chronic and will not heal unless the patient loses weight or the area of MLL is resected. We also recommend obese patients with a BMI >40 who do not yet have OIL by lymphoscintigraphy to lose weight before they develop the potentially incurable condition. Unlike other comorbidities that are reversible with a reduction in BMI (e.g., diabetes, hypertension, hyperlipidemia), OIL may not be curable.
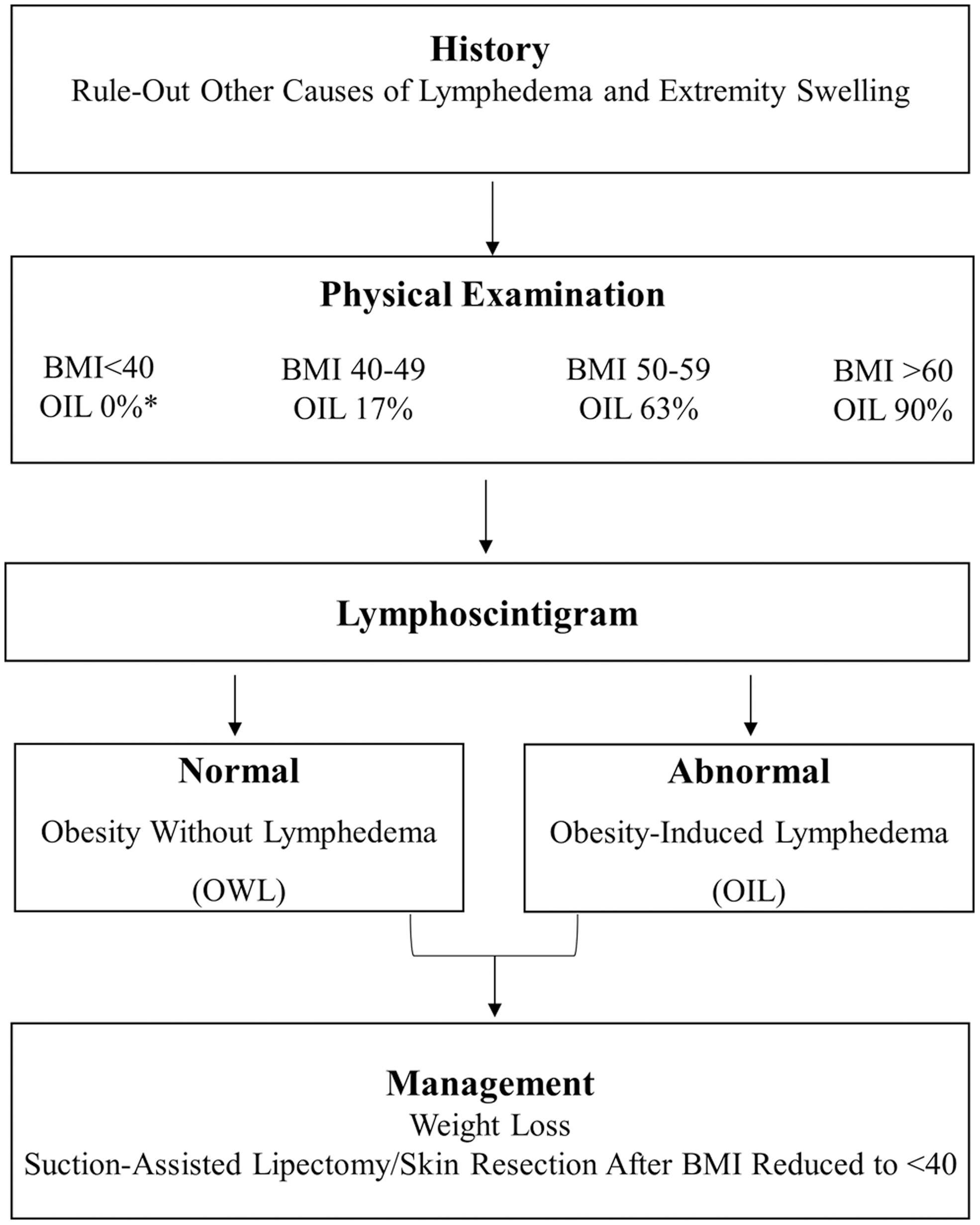
Treatment algorithm for OIL. Diagnosis requires lymphoscintigraphy and definitive management in weight loss. *Nonambulatory patients can develop OIL with a BMI <40.
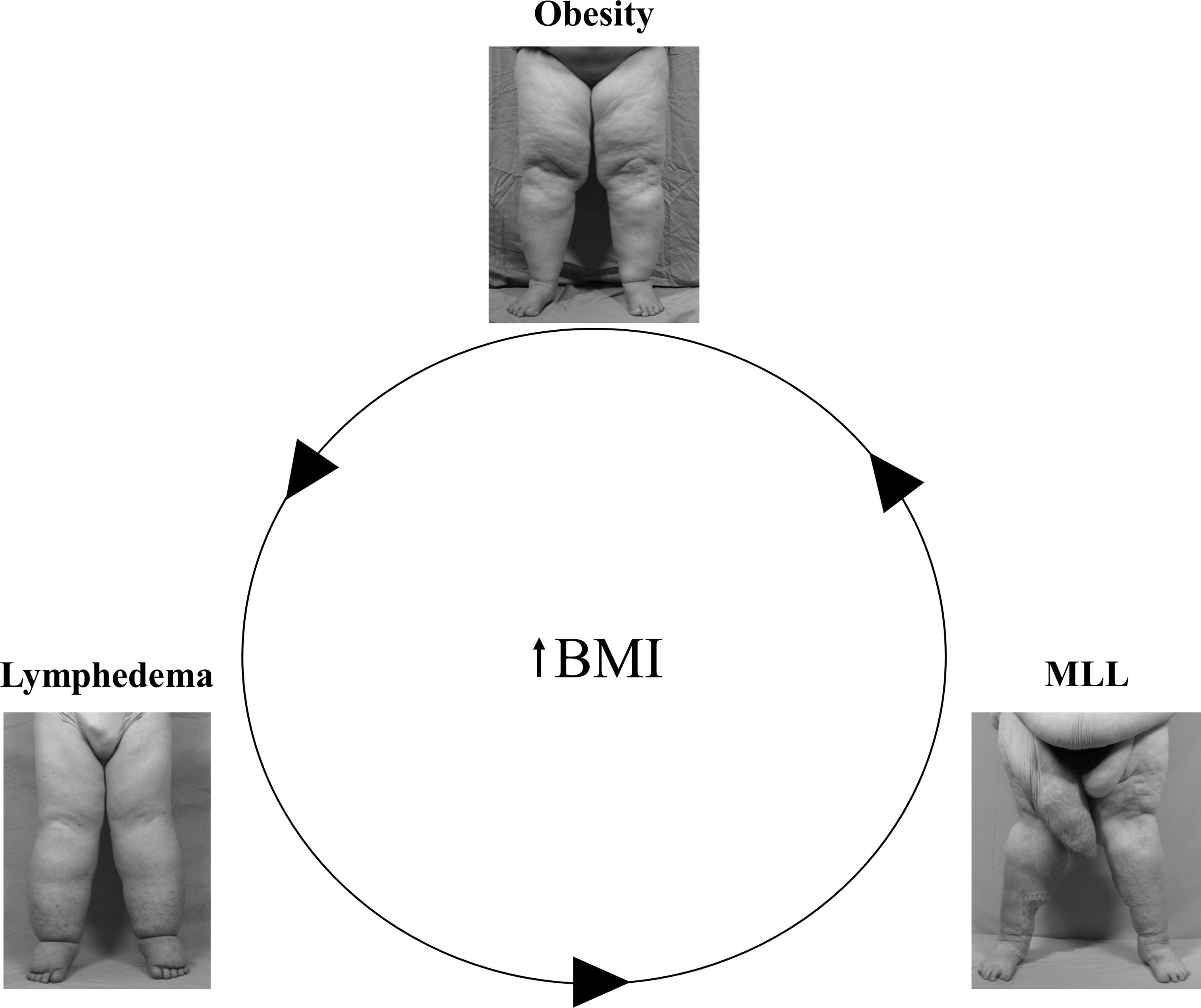
Obesity and lymphedema negatively affect each other. Obese individuals who develop OIL enter a vicious cycle of subcutaneous adipose deposition of their legs, which causes further damage to their lymphatics. Lymphedema worsens, MLL develops, which further increases their obesity. The only way to break the cycle is weight loss.
Resection of excess skin and subcutaneous tissue is not considered in patients with OIL until they have lost weight and their BMI is <40 (Fig. 4). Following weight loss, most patients will have a satisfactory reduction in the size of their legs and areas of MLL. 9,18 If an excisional procedure is indicated, the intervention is significantly facilitated. In addition, because the patient's BMI and lymphatic function are improved, the risk of recurrence is much lower. Our first-line surgical intervention is suction-assisted lipectomy to remove excess subcutaneous adipose tissue if the patients continue to have significant morbidity from the size of their legs. If significant skin excess is present, or to treat MLL, a skin and subcutaneous excision is required. Microsurgical operations for OIL are not frequently performed because obesity increases the technical difficulty of the procedure. Lymphatic-venous anastomosis or vascularized lymph node transfer also is unlikely to be successful because patients with OIL have significant subcutaneous fibrosis and inflammation.
Management of OIL is weight loss.
Patients who are not candidates for a surgical weight-loss procedure are advised to lose weight through diet and exercise. If an individual is unable to lower his/her BMI <40 (e.g., not a bariatric operative candidate), and suffers significant morbidity from an overgrown extremity or area of MLL, an excisional procedure can be performed. However, the patient will be at high risk for complications and will have recurrence of the resected tissue unless his/her BMI is able to be reduced to <40 following the procedure.
Take-Home Messages
A BMI threshold of 40 exists at which point lower extremity lymphatic dysfunction can occur.
The risk of OIL increases with elevated BMI; 90% of individuals with a BMI >60 will have the disease.
Patients with OIL, or at risk for the disease, are managed with weight loss.
Operative intervention to reduce extremity overgrowth is considered after patients have reduced their BMI to less than 40.
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
There was no funding source for this work.
AUTHOR DISCLOSURE AND GHOSTWRITING
No competing financial interests exist. No ghostwriters were used to write this article.
ABOUT THE AUTHORS
AUTHORS' CONTRIBUTIONS
Both authors made substantial contributions to the work, drafted and revised the work, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.