
Abstract
Significance:
Lymphedema is chronic limb swelling from lymphatic dysfunction. The condition affects up to 250 million people worldwide. In breast cancer patients, lymphedema occurs in 30% who undergo axillary lymph node dissection (ALND).
Recent Advances:
Immediate lymphatic reconstruction (ILR), also termed Lymphatic Microsurgical Preventing Healing Approach (LyMPHA), is a method to decrease the risk of lymphedema by performing prophylactic lymphovenous anastomoses at the time of ALND. The objective of this study is to assess the risk reduction of ILR in preventing lymphedema.
Critical Issues:
Lymphedema has significant effects on the quality of life and morbidity of patients. Several techniques have been described to manage lymphedema after development, but prophylactic treatment of lymphedema with ILR may decrease risk of development to 6.6%.
Future Directions:
Long-term studies that demonstrate efficacy of ILR may allow for prophylactic management of lymphedema in the patient undergoing lymph node dissection.

Scope of review
A preventative strategy has emerged in attempt to decrease the frequency of lymphedema after axillary lymph node dissection (ALND). This microsurgical procedure was first described in 2009 by Boccardo et al., as Lymphatic Microsurgical Preventing Healing Approach (LyMPHA). 1 The approach has been performed at a growing number of cancer centers over the past 5 years and is now most commonly termed immediate lymphatic reconstruction (ILR). 1 –10 Following ALND, afferent lymphatic vessels that have been disrupted during axillary lymph node excision are identified and microsurgically anastomosed to adjacent veins.
This review performs an analysis of the recently expanding literature to assess effect of ILR at reducing the risk of lymphedema.
Translational relevance
This study investigates the utilization of ILR in reducing lymphedema risk.
Clinical relevance
Prophylactic management to decrease lymphedema rates can increase patient quality of life and decrease morbidity. This study assesses the effect of ILR in reducing the lymphedema risk.
Background
Lymphedema is defined as chronic limb swelling from lymphatic dysfunction. This condition affects up to 250 million people worldwide. 11 Lymphedema is associated with significant impacts on quality of life and has a high health cost burden. 12,13 Fluid, adipose, and fibrosis from inflammation result in progressive limb enlargement. Patients experience recurrent cellulitis, pain, and impaired extremity function as a result. 14 –16 Unfortunately, there is no cure for this progressive disease 14,15,17
Breast cancer is the second most common form of cancer in females, affecting in 1:8, and breast cancer-related lymphedema is the most frequent etiology of lymphedema in the United States. 8,11,18,19 Sentinel lymph node biopsy was developed to decrease the morbidity of axillary sampling during oncologic surgical management in select patients; however, this procedure still carries up to a 6% risk of lymphedema. 5,7 ALND is performed for locally advanced breast cancer or biopsy-proven metastases to the axillary nodes. 20 Lymphedema occurs in 30–52% of patients who undergo ALND, and persistent symptoms of lymphedema affect up to 20% of breast cancer survivors. 5,7,8
Nonsurgical management of lymphedema is primarily with compression and complete decongestive therapy. 21,22 There is no effective pharmacological treatment to date. Surgical management includes excisional and physiologic procedures. Excisional procedures are skin/subcutaneous excision, suction-assisted lipectomy, and the Charles procedure, which consists of radical subcutaneous resection and skin grafting. 23 –25
Physiologic procedures include vascularized lymph node transfer and lymphovenous bypass. 26 –34 Conservative and operative management can improve arm volume and slow progression. However, progressive limb enlargement from interstitial fluid retention, fibrosis, and adipose deposition over time are difficult to reverse and cannot be cured. 23,35,36
MATERIALS AND METHODS
This systematic review is compliant with the recommendations specified in the Cochrane Handbook for Systematic Reviews of Interventions (Version 5.1.0) and is reported in agreement with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. 37
Search strategy and selection
A systematic literature search was performed using PubMed Central, EBSCO, and Ovid MEDLINE for original studies describing the incidence of lymphedema in patients who had ILR after ALND for breast cancer treatment. All dates through February 16, 2021 were included. The search strategy is listed in Table 1. References of returned studies were also reviewed for pertinent articles. A hand search of articles was also performed to ensure inclusivity of all studies through our described systematic review algorithm, but no additional studies met inclusion criteria.
Search strategies for interrogated databases for immediate lymphatic reconstruction
All studies at the time of this investigation in which ILR was performed concurrently with ALND for breast cancer were included. ILR performed for indications other than ALND for breast cancer (e.g., melanoma) was excluded to optimize homogeneity of the data. Included articles were limited to human adult studies written in English. Duplicate studies were excluded, as were review articles, abstracts, case reports, case series of less than three patients, discussions, commentaries, letters, and editorials. Only observational studies were included in the analysis due to the paucity of randomized controlled trials reporting the effects of ILR after ALND.
Data assessment and collection
All citations identified on initial search were imported into EndNote X9.3.3 (Thomas Reuters, New York, NY). After removal of duplicate articles, the titles and abstracts of the remaining references were reviewed for content pertinence by two independent reviewers (J.A.C. and A.H.H.). Full text review was then performed of the remaining articles to determine articles meeting inclusion and exclusion criteria. Data collection was performed by two reviewers, and disagreements were resolved by consensus. All included studies were independently evaluated using methodological index for nonrandomized studies (MINORS) criteria. 38
Data points of interest included study design, patient demographics, sample size, modality of lymphedema measurement, number of lymph nodes removed during ALND, number of identified transected lymphatics, number of lymphovenous anastomoses, need for adjuvant radiation, incidence of lymphedema, and follow-up. Lymphedema diagnosis was defined by study authors.
Statistical analysis
A random-effects DerSimonian–Laird model for meta-analysis was used given the innate heterogeneity of observational studies. Statistical heterogeneity was estimated using Cochran's Q and I 2 statistic. A forest plot was created as a graphical representation of the meta-analysis, with horizontal lines demonstrating confidence intervals (CIs) and size of marker indicating the study's weight in the meta-analysis. A sensitivity analysis of the data was performed by repeating the random-effects model as a fixed-effect model. Statistical significance was set at p < 0.05. All analyses were performed in IBM SPSS Statistics for Windows, Version 27.0 (IBM Corp., Armonk, NY).
RESULTS
Study analysis
A total of 448 articles were identified using PubMed, EBSCO, and Ovid MEDLINE databases. The process for filtering studies is depicted in Fig. 1. After the 66 remaining studies were evaluated for compliance with set inclusion and exclusion criteria, 6 studies were determined to be consistent with study goals. Common reasons for exclusion of studies included delayed lymphatic reconstruction, nonbreast cancer diagnoses, lymphatic reconstruction performed for indications other than ALND, lack of defined criteria for lymphedema diagnosis, and no follow-up data.

Article selection flow chart for included studies.
Only studies with the most recent longitudinal data were included, resulting in a total of five studies for this review and meta-analysis. Authors of three of the five included studies had published earlier reports on longitudinal data. 5,39,40 The earlier studies from the same groups were excluded. Of the included studies, three (60%) were prospective cohort studies and two were retrospective reviews. MINORS scores indicated moderate to high quality of studies (Table 2).
Methodological index for nonrandomized studies 38 scoring of included studies
Population data
Five studies totaling 251 patients were included. The average age of all patients was 53.8 years; 249 (99.2%) of patients were female. Mean body mass index (BMI) was 27.0 kg/m2. There were 16.0 lymph nodes removed at the time of ALND with 2.8 positive nodes. A total of 178 patients (70.9%) underwent postmastectomy radiation therapy. Patients followed up a median of 22.6 months following ILR.
Lymphedema data
There was an average 2.6 transected lymphatics identified per patient, and a mean 2.4 lymphovenous anastomoses performed. Of the 251 patients, 15 patients (5.9%) developed lymphedema at a median 10.3 months postlymphatic reconstruction (Table 3). The primary comparison group in this study was those who underwent attempted ILR which was aborted intraoperatively. A total of 23 of 156 patients in 3 studies did not undergo lymphatic reconstruction (14.7%). 5,7,39 Reasons for aborting lymphatic reconstruction included inability to find afferent lymphatics, lack of adequate vein for anastomosis, and profound axillary metastatic disease. Of these 3 studies, 2 reported outcomes of the nonlymphatic reconstruction groups, inclusive of 17 patients. 7,39 Five of the 17 patients (29.4%) developed lymphedema during the study period. The weighted proportion of patients who acquired lymphedema after lymphatic reconstruction (6.6% [95% CI 3.9–10.3]; Fig. 2) was compared to those without lymphatic reconstruction (30.5% [95% CI 4.0–68.1]; Fig. 3).

Incidence of lymphedema events in patients who underwent immediate lymphatic reconstruction.

Incidence of lymphedema events in patients who did not undergo immediate lymphatic reconstruction.
Characteristics of studies included in systematic review of immediate lymphatic reconstruction
The funnel plots for included studies evaluating lymphedema development after ILR (τ = 1.0, p = 0.32, Fig. 4) and without lymphatic reconstruction (τ = 1.00, p = 0.32, Fig. 5) were symmetric in appearance.

Funnel plot of included studies evaluating lymphedema development after immediate lymphatic reconstruction at the time of axillary lymph node dissection. τ = 0.40, p = 0.32.
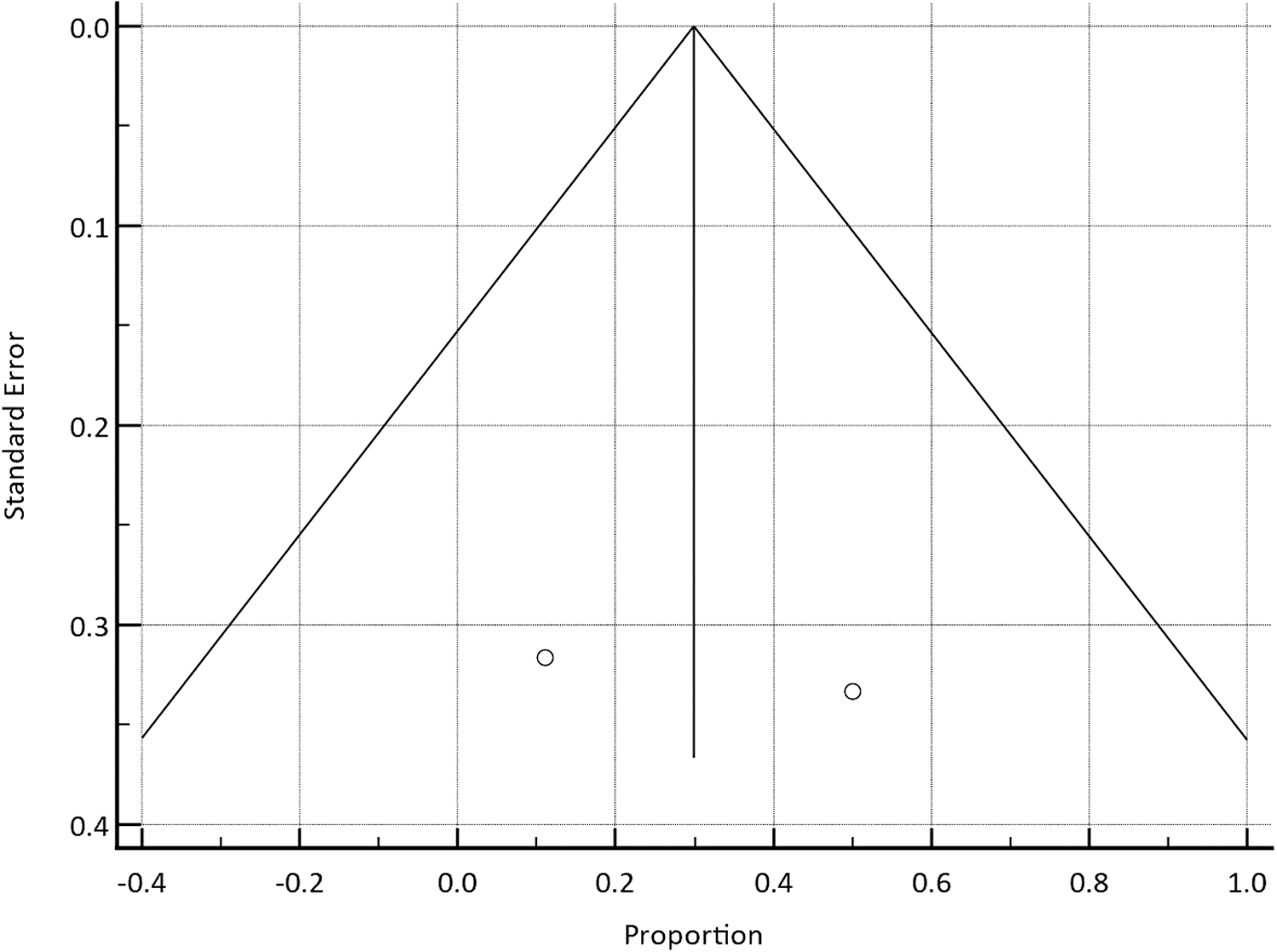
Funnel plot with included studies evaluating lymphedema development without immediate lymphatic reconstruction. τ = 1.00, p = 0.32.
Sensitivity analysis
Results were confirmed using a fixed-effect model. The weighted proportion of patients who developed lymphedema after lymphatic reconstruction (6.6% [95% CI 3.9–10.3]) was compared to patients without lymphatic reconstruction (29.9% [95% CI 11.5–54.9]).
DISCUSSION
Lymphedema is a difficult problem to treat. It can progress over time through four stages. Stage 0 is defined as subclinical lymphatic dysfunction with a normal examination. Stage 1 is characterized by edema that improves with extremity elevation. Pitting edema is present in stage 2 without resolution of swelling during arm elevation. Finally, edema becomes nonpitting during stage 3 because of fibroadipose deposition. 41 Physiologic procedures may be combined with excisional procedures to address the fluid, adipose, and scar elements of arm expansion. However, the inflammatory process involved in lymphedema is difficult to reverse, and no cure exists. 23,24,42,43
The results of this systematic review indicate that ILR decreases the risk of breast cancer-related lymphedema. The weighted proportion of patients who developed lymphedema after ILR (6.6%) was lower than those without lymphatic reconstruction (30.5%). The frequency of lymphedema in individuals that did not have ILR was consistent with the previous literature. 8,44
ILR has promising results, but the expected benefits of a new emerging procedure need to be weighed against the risks. ILR has not been shown to add any additional morbidity to the lymphadenectomy, but there is additional operative time that improves with experience. 5,40 Despite this increase in operative time, a cost-utility analysis demonstrated ILR after ALND to be a cost-effective procedure in decreasing the rates of lymphedema. 45
During embryologic development, lymphatic vessels bud from veins. 46 Lymphatic capillaries transport extracellular fluid from peripheral tissues, and the proteinaceous lymph flows through lymphatic collecting vessels and ultimately through lymph nodes. Lymph within the lymphatic system is ultimately returned to the circulatory system through the thoracic duct into the subclavian vein. 47
ALND disrupts the afferent lymphatic vessels that drain into the axillary lymph node basin. ALND is performed for locally advanced breast cancer or biopsy-proven metastases to the axillary nodes. It involves excising axillary lymph node levels I and II. 40 The methods of ALND in the included use varied approaches to removing the lymph node basin. If axillary dissection is being performed without sentinel node biopsy preceding during the same operation, axillary reverse mapping (ARM) can be performed.
ARM involves injecting isosulfan blue subdermally in the brachial fascia. 5,40 This stains the afferent lymphatics and lymph nodes that are critical for upper extremity drainage. Lymphatic channels that connect to those blue nodes that require resection during the axillary dissection based on their anatomic location are then anastomosed to adjacent veins using ILR. If a sentinel node biopsy is performed before ALND doing the same operation, isosulfan blue often is injected in the breast along with technetium99 to help identify the sentinel nodes. If intraoperative pathological frozen sections indicate the need for axillary dissection, then fluorescein isothiocyanate with albumin can be used to identify afferent lymphatics for ILR because lymphatic blue staining can be from the breast injection. 39
During ILR, the cancer treatment status is not affected because: (i) these lymphatic vessels would be left in place regardless of whether ILR is performed because the standard anatomic axillary dissection is followed, (ii) the patients would receive postmastectomy radiation therapy for concerning histological features, and (iii) the lymphatic vessels that are anastomosed are reestablishing lymph flow coming from the arm (not from the cancer site).
ILR reestablishes a continuous path for lymph flow in the limb by drainage directly into the venous system at an earlier point than the subclavian vein, which is a normal physiologic recipient site of lymph. This technique involves identifying disrupted afferent lymphatics by utilizing isosulfan blue, indocyanine green, or fluorescein. 2,6,48,49 Using a surgical microscope, a branch from the axillary or thoracodorsal vein is then anastomosed to the disrupted lymphatic vessel (Fig. 6).

Immediate Lymphatic Reconstruction to prevent lymphedema performed after axillary lymph node dissection. (Left) Top left arrow shows the pectoralis major muscle and white arrow exhibits the axilla. The black box and arrow depicts the lymphovenous anastomosis. (Right) Under the surgical microscope, the disrupted afferent lymphatics (right arrow) are identified with isosulfan blue dye and anastomosed to a vein branch (left arrow).
Although patency of the lymphovenous anastomosis is assessed intraoperatively by milking the dye across the anastomosis, only the study by Boccardo et al., assessed the lymphovenous anastomosis with lymphoscintigraphy in a subset of patients at least 1 year postoperatively. 5 Patients are followed for evidence of lymphatic dysfunction (clinical, bioimpedance, perometry). Those who exhibit swelling begin compression.
Obesity is an independent risk factor for acquiring lymphedema after ALND. 6,8 A BMI greater than 30 kg/m2 triples the risk of lymphedema after ALND. 50 Obese individuals that develop lymphedema exhibit more morbidity, infections, hospitalizations, and greater limb volume compared to those with normal BMI. 51 The mean BMI for patients in this study who underwent ILR was 27 kg/m2. Only one article included in this study set a BMI cutoff of 30 kg/m2 for patients to be offered ILR. 5
There is no consensus on whether there should be a BMI threshold to perform the procedure. Considering that 70% of patients do not acquire lymphedema after ALND, targeting high risk patients increases the potential benefit from the procedure.
There are several limitations to this systematic review. Only 5 articles met inclusion criteria, and the sample size was low with 24–88 patients per study in the treatment group. None of the investigations provided level I evidence. There is a lack of a consistent control group in the studies as only two articles reported lymphedema rates in patients who had ALND without ILR. The funnel plots, particularly the control group, have limited definitive conclusions because of the small sample size.
The outcome variables and measurements were also not uniform. Lymphoscintigraphy, volumetry, bioimpedance, and perometry were variably used in addition to clinical assessment. The length of follow-up in the studies is also potentially problematic. The average onset of lymphedema is 1 year postoperatively. 8 Approximately 75% of patients develop lymphedema within 3 years after lymphatic injury. 44
Three of the five articles that were included had median follow-up of less than a year. 6,7,39 Due to this short duration of follow-up, it is expected that a greater number of those patients will develop lymphedema over time. The precise risk reduction from ILR will therefore be higher than 6.6%. Three of the five articles included in this meta-analysis were released within the past year, which attests to the increasing emergence of this procedure throughout institutions.
As more data are published and longer term follow-up is available, a clearer picture will be established on the true efficacy of the procedure and whether more precise selection criteria are required. Long-term outcomes are particularly important as aging is also a risk factor for lymphedema as there is progressive lymphatic stasis over time. 52 –54
In summary, this is a comprehensive systematic review of the most current literature of ILR, the emerging technique to decrease the risk of breast cancer-related lymphedema. The preventative approach of ILR has the potential to change the management paradigm for lymphedema. Evidence from the systematic review of the literature supports performing ILR after ALND in the treatment of breast cancer. ILR was found to decrease the risk of lymphedema from 30.5% to 6.6%. Of the five studies included, however, none provided level I evidence. The lack of long-term follow-up indicates that the 6.6% risk of developing lymphedema after ILR will likely rise over time. Once lymphedema is established, treatment is challenging. Considering that the morbidity of ILR is low, the benefits of performing ILR outweigh the risks based on the best clinical data available at this time.
KEY FINDINGS
Lymphedema occurs in nearly 30% of patients after ALND in the treatment of breast cancer.
There is no cure for lymphedema, and it is difficult to treat.
ILR is an emerging microsurgical procedure to prevent lymphedema. Disrupted afferent lymphatic vessels are anastomosed to veins immediately after lymph node dissection.
This systematic review of literature demonstrates that performing ILR can decrease the risk of lymphedema to 6.6%.
Footnotes
AUTHORs' CONTRIBUTIONS
All authors provided significant contributions to study idea design, data acquisition and analysis, article writing, and article edits. The authors agree with the submitted form of this article.
ACKNOWLEDGMENTS AND FUNDING SOURCES
The authors acknowledge all previous, current, and future lymphedema researchers in their pursuit of improving patient lives. This article was not specifically supported by any funding sources. Author Aladdin H. Hassanein is supported by grants from the Department of Defense DOD-W81XWH2110135, American Association of Plastic Surgeons, and the Plastic Surgery Foundation.
AUTHOR DISCLOSURE AND GHOSTWRITING
The authors have no financial interests or commercial associations to disclose. No ghostwriters were involved in this article.
ABOUT THE AUTHORS