
Abstract
Significance:
Hypertrophic scars (HTS) and keloids are common after thermal injuries and other trauma to deep regions of dermis of the skin. These abnormal scars can cause contractures and the thick masses of scar tissue that result in functional and cosmetic impairment. Management of these dermal fibrotic conditions includes a wide range of medical and surgical treatments, which can be time consuming, only partially effective, and often uncomfortable for patients.
Recent Advances:
The molecular pathophysiology of HTS has become more understood over the past two decades, where thermal injury to the reticular dermis results in an inflammatory response, fibrogenic growth factor release, and the formation of a dermal scar with increased collagen and proteoglycan composition in an abnormal morphology. Lasers are becoming a widely used form of treatment for these types of scars; however, the evidence for the beneficial effects of laser treatments and the understanding of their mechanism of action are still evolving.
Critical Issues:
Paradoxically, laser delivery of thermal energy to the skin is suggested to improve scar remodeling and wound healing, yet HTS is a well-recognized complication of excessive thermal energy delivered by laser treatments. This review aims to examine the current evidence for the use of lasers for HTS, and to investigate the molecular mechanisms where re-injury of a burn scar from laser treatment could result in overall improvements in scar quality.
Future Directions:
Improved design of clinical trials for the treatment of scarring in the future will evolve from new methodology and models of HTS in animals and humans.
Edward E. Tredget, MD, MSc, FRCS

Scope and Significance
Fibrotic scarring, including hypertrophic scars (HTS) and keloids, is difficult to treat; however, laser therapy has become an increasingly common treatment. With different authors using an assortment of lasers to treat scars with varying success, their underlying mechanisms of action and biological properties are not well understood. This review provides an overview of the types of lasers, potential applications, and current deficiencies in understanding, as related to laser treatments for scar management in clinical practice.
Translational Relevance
Laser therapy is a relatively newer treatment for fibrotic scarring and dermal disorders, and understanding of its mechanisms of action is still evolving. There remains a lack of robust, large, controlled studies on laser treatments for HTS after burn injury. As more recent investigations and information become available, an update on laser treatment advances is essential to further our knowledge of appropriate types of lasers for serious scarring and their therapeutic regimens.
Clinical Relevance
As stated earlier, HTS are a serious and difficult dermal fibroproliferative disorder, very common after deeper injuries to the skin for which current forms of treatment are only partially successful, often prolonged, and uncomfortable. More efficient, successful, and directed therapy for HTS would be a major advance in their treatment.
Background
Burns: hypertrophic and keloid scars
Burn trauma is one of the leading causes of severe scarring worldwide, hospitalizing ∼500,000 people annually in the United States alone (2016). 1 Greater than 70% of burn injuries develop pathologic scars, including HTS or keloids (Fig. 1 2), causing functional disabilities, cosmetic deformities, and decreased quality of life. 3 Scar management remains a significant challenge faced by patients and their physicians. Scar treatment and the management of chronic wounds are a major burden for health care systems, and while cost estimations are wide ranging, they are estimated to be $5–$24.3 billion for hospitalized patients and $9.9–35.8 billion for outpatient costs in the United States alone. 4

Morphology of keloids in a 12-year-old child following a scald burn and HTS in a 28-year-old woman following a burn injury. HTS, hypertrophic scars. Permission was granted from original journal and authors.
HTS and keloids are dermal forms of fibroproliferative diseases where abnormally dense extracellular matrix (ECM) production in the healing dermis creates functional impairment, particularly when these scars occur in regions such as the shoulders, elbows, hands, neck, face, ears, or central chest. Normal wound healing consists of four stages: hemostasis, inflammation, proliferative, and tissue maturation/remodeling phase. 5 Although HTS and keloids often arise from tissue injuries affecting the reticular layer of the dermis, they are distinctly different (Table 1). HTS appear to develop from injuries to the deep dermis, which often take longer than 3 weeks to reepithelialize. Keloids, however, may occur spontaneously, do not regress over time, and often extend beyond the borders of the initial wound. HTS appear 4–8 weeks after skin injury and have a distinctive histologic pattern of wavy parallel collagen fibers and fiber bundles. Long-term follow-up of HTS patients 2 years postinjury shows that, despite improvements in wound healing, many patients experience decreased quality of life due to a significant number of scar-related complications, including functional and cosmetic impairments, which have substantial psychosocial impacts. 6
The features of keloids and hypertrophic scars in morphology, histology, and cellular and molecular mechanisms
HTS, hypertrophic scars.
Pathophysiologic features of HTS
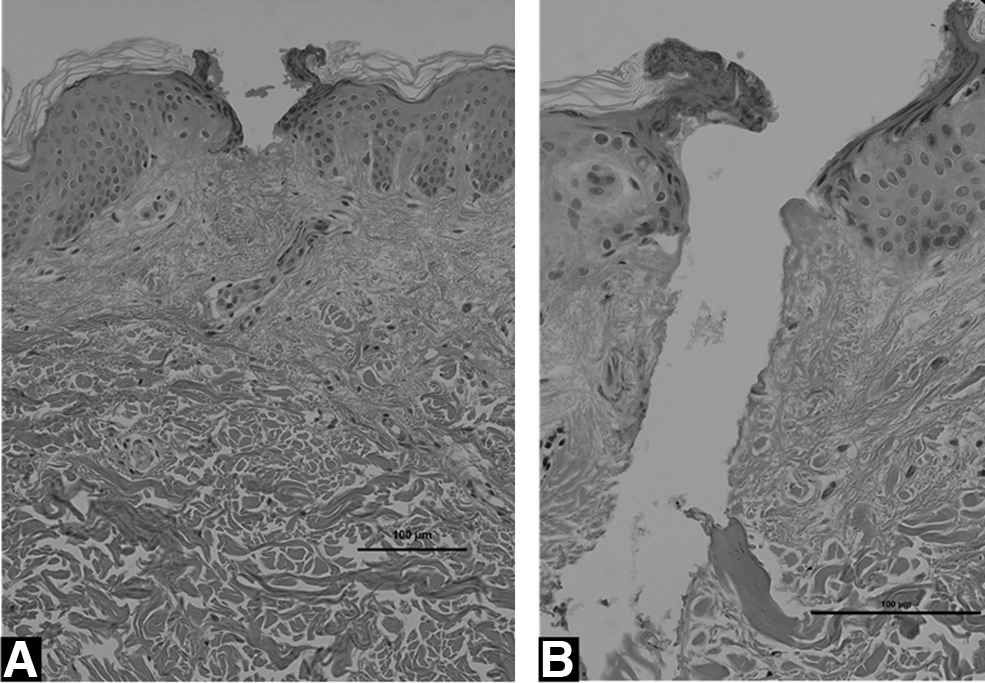
Histologically, HTS have thickened epidermis and dermis and lack rete ridges compared to normal skin (Fig. 2). It is hypercellular and hypervascular, and has significant changes to collagen bundle orientation. Picrosirius red staining utilizes newer methodologies to provide a more objective measure of treatment outcomes of collagen bundles. The dermis of normal skin shows a typical basket-weave pattern, while HTS have densely packed collagen fiber bundles in a parallel orientation, whereas keloids have more dispersed, dense bundles (Fig. 3). Histologic images can be assessed by Fourier analysis to determine the collagen orientation index (COI), where 0 corresponds to a random orientation of collagen found in normal skin, whereas 1 corresponds to abnormally parallel collagen typical of HTS. Picrosirius red staining also demonstrates an increased collagen type III:I ratio (Fig. 3). Novel subpopulations of peripheral blood mononuclear cells from blood circulation enter the tissues after burn injury, where they express profibrotic cytokines and mediators contributing to the HTS. 7 Healthy skin contains a collagenous matrix morphology that includes proteoglycans such as decorin, which is required for tightly packed collagen fibers and fiber bundles and is abundant in normal skin. 8 However, in human HTS, as well as in mouse models of HTS where transplanted human skin develops HTS-like features, decorin is reduced by about fivefold compared to unwound skin, and thus its reduction appears to play a key role in HTS formation.

Histological characteristics of HTS include thicker epidermis and dermis

Picrosirius Red staining of HTS and normal skin. Normal skin has basket-weaved appearing collagen bundles
As illustrated in Fig. 4, when a progressively deeper wound is created in lateral hip skin, once the depth extends into the deep dermis (beyond ∼0.56 mm in thickness), a red, raised, hypertrophic-like scar develops, as described by Dunkin et al., in 113 normal volunteers. 9 This suggests that superficial wounds can heal with minimal scar; however, beyond a critical depth, HTS commonly forms. This is relevant to laser therapy, as it remains elusive how microthermal columns penetrating deep into the skin after ablative laser treatment can result in a regenerative wound healing process, while avoiding the classic deep dermal injuries and the molecular changes of HTS. These factors include fibroblast proliferation, accumulation of myofibroblasts, infiltration of M2 macrophages and fibrocytes, and increased fibrogenic cytokines such as transforming growth factor (TGF)-β and its type II receptors. Ultimately this cellular milieu activates deep dermal fibroblasts leading to increased synthesis of abnormal matrix proteins, including type III collagen, high molecular weight proteoglycans such as versican and aggrecan, and less leucine-rich, small molecular-weight decorin, which is dramatically different than normal skin. 10,11

Superficial injuries to the papillary dermis of the skin often lead to normal wound healing with little residual scarring; however, deeper injury to the reticular dermis results in a greater and prolonged inflammatory response, often resulting in HTS. 12 When the ECM deposition by fibroblasts exceeds degradation by matrix metalloproteinases (MMPs), a net accumulation of ECM occurs, contributing to the inelastic and thick scar, which are features commonly seen in HTS. 13,14 Our research group has found that deep dermal fibroblasts likely contribute to HTS, showing similar characteristics to HTS fibroblasts by producing more TGF-β1, versican, and collagen, and less collagenase and decorin, and expressing more α-SMA. 15 Fibronectin produced by fibroblasts is also significantly higher in HTS. 16 Elastin in the ECM shows significant reduction in HTS, contributing to wound contraction and matrix stiffness. 17
Investigators using classic protein extraction and quantitation methods found the ratio of type III/type I collagen is increased in HTS compared to normal skin. 18,19 More recently, using confocal microscopy to quantitate immunofluorescent images, Oliveira et al. demonstrated increased type III collagen synthesis in the deep dermal region of immature HTS in burn patient's biopsied longitudinally using site-matched normal skin and normotrophic scars. 20 In contrast, nonhypertrophic or normotrophic scars taken from the same patient at the same time points had significantly less type III collagen when compared to HTS. 19 During wound healing, investigators have documented increases in type III and type I collagen within the first week after burn injury, peaking at about 6 months postinjury and declining to a normal turnover rate by 2–3 years. Suggestions that laser therapy improves scar by inducing type III collagen messenger RNA (mRNA) are inconsistent with these well-controlled studies and appear to be based on changes in gene expression, which are subject to post-translation modification or are limited by sampling techniques and lack of within-patient controls. Similar technical limitations exist in multiple studies of type I and III in HTS fibroblasts in vitro. 18
Mast cells increase in HTS compared to normal skin and mature scars, and release fibrogenic growth factors. 21 In HTS, mast cells have fewer intercellular gap junctions and less connexin proteins, which is unique in the fibrotic nature of these scars. 22 Dermatopontin is a noncollagenous protein in the ECM, binding small proteoglycans, decorin, and collagens, 23 which is also decreased twofold to threefold in HTS based on mRNA expression. 24
Discussion of Findings and Relevant Literature
Lasers as a treatment for scarring
Standard treatments for HTS and keloids include pressure garments, silicone gels, topical and intralesional corticosteroids, calcium channel blockers and 5-fluorouracil, radiation, cryotherapy, surgical excision, and/or skin grafting, as well as laser therapy. 25 –27 Although historical articles on the use of various lasers to treat HTS showed promise, they often consisted of small case series, animal studies, or expert opinion. 28 –35 More recently, a number of more robust studies have been performed, including large case–control series, and randomized, controlled trials, 36 –58 which provide greater evidence for the use of lasers in the treatment of HTS. However, many investigators recognize that no adequately powered, randomized control trials, which control for spontaneous natural improvements in HTS after burn injury, and which utilize improved, objective outcome measures, exist as of yet. 59
Laser is an acronym for “Light Amplification by Stimulated Emission of Radiation.” Laser treatment stimulates the wound site by using photothermal energy to initiate the cellular response within scar tissue and remodel dermal collagen and elastin. Lasers differ in their radiation sources, but their emission is a single, fixed wavelength of light energy, which is unidirectional and coherent. The photothermal principle of lasers is the absorption of energy by chromophores in the skin, which generate heat and can cause a targeted inflammatory response, 59 cellular death, and tissue ablation. 60,61 Many types of lasers have been used in scar treatments, differing in wavelength and/or depth, including carbon dioxide (CO2), neodymium-doped yttrium aluminum garnet (Nd:YAG), erbium-doped (Er) YAG, and pulse dye laser (PDL). Fractional photothermolysis produces focused laser beams to create a three-dimensional pattern of microthermal treatment zones (MTZs) (Fig. 5). Nonablative lasers penetrate the epidermis, directing energy to the underlying dermis, whereas ablative lasers photocoagulate the epidermis enroute to the underlying dermis and are therefore more painful and capable of penetrating to greater depths within the dermis with greater risks of photodamage with excessive energy. 62 An example of laser treatment is a 12-year-old girl who developed severe HTS after a grease splatter burn, as seen in Fig. 6.
Fractional CO2 ablative laser treatment of a mature scar on a low setting vaporizing shallow MTZs through the epidermal layer only in

Grease splatter burn wounds in a 12-year-old female healed with HTS.
A laser beam that hits the surface of skin may reflect, scatter, absorb, or transmit at each layer. 63 While there is minimal light scattering in the epidermis, the high concentration of collagen fibers in the dermis causes significant scatter which is inversely proportional to the wavelength of laser light. 64 The laser photons are targeted to specific chromophores in the dermis, including melanin, hemoglobin, water, amino acids, and bilirubin, depending their absorption coefficient. 65,66 Fractionated ablative lasers create MTZs in specific geometric patterns, causing skin inflammation and subsequent remodeling, but are spaced by surrounding zones of uninjured tissue. 65 Lasers selectively use photons of specific wavelengths to target tissue, which generates increased temperatures within the tissue. At 60–70°C, collagen and other structural proteins denature; at 70–80°C, nucleic acids denature and cell membranes are made permeable; at 70–100°C, coagulation necrosis occurs, denaturing proteins; and above 100°C, water in tissue vaporizes and ablation occurs. 67
Nonablative lasers penetrate the epidermal layer, leaving it intact, while producing columns of coagulated tissue in the dermis with denatured collagen to stimulate wound healing. 66 These MTZs heal by reepithelialization and with renewed dermal collagen synthesis in a potentially more normal ratio of type III and I collagens, causing morphologic improvement in the structure of the collagen bundles (Fig. 2). 66 Investigators suggest that laser injury induces type III collagen and is associated with more normal morphology as a result 68 ; however, as discussed earlier, immature HTS have more type III collagen compared to non-HTS matched in the same patient at the same time postinjury. These confusing findings may be due to technical limitations of measuring mRNA for type III collagen or using isolated histological measurements, which are complicated by post-translational modifications as well as limitations in sampling technique and adequate controls as discussed by Oliveira et al. 20
Fractional CO2 ablative lasers cause photothermolysis, which induces a wound healing response to the thermal tissue damage, resulting in some restoration of rete ridges, increased mucin deposition in the epidermal-superficial dermis region, formation of new dermal collagen, and tissue repair. 69 Ablative fractional laser resurfacing in human skin shows a persistent collagen remodeling response lasting at least 3 months. 70 Fractional laser resurfacing causes an initial inflammatory response with marked elevated levels of proinflammatory cytokines, followed by increases in several MMPs and later by induction of both types I and III collagen. 71 These changes after CO2 laser treatment include an upregulation of genes such as COL12A1, which is a homotrimer found in association with type I collagen and thought to modify the interactions between collagen I fibrils and the surround matrix. Also, an increased expression of fibroblast growth factor 7 (FGF7) is associated with tissue remodeling, upregulation of heat shock proteins such as HSPB3, chemokines, including CXCL12 and CCL8, and proinflammatory cytokines, including interleukin 1 alpha (IL-1α). 59,72
The histological effects of laser resurfacing in scars are of importance to understanding the benefits of treatments at a molecular level. Figure 5 illustrates the effects of CO2 laser in the penetration of epidermis and superficial and deep dermis. After CO2 laser resurfacing, IL-1β has been shown to increase from day 1 to more than 6,000-fold compared to the baseline level, and declines rapidly between days 6 and 8, 73 and mRNA levels of tumor necrosis factor alpha (TNF-α) peaked on day 6, with a rapid drop by day 8, similar to IL-1β. Both cytokines are involved in the tissue repair process, in part, by inducing MMPs. After laser treatment of HTS, MMP-1, MMP-3, and MMP-9 arising from cells in the tissues or from blood-borne monocytes are elevated up to 6 months post-treatment. 74 Others have found improvements in HTS post-treatment associated with degradation and remodeling of collagen and other ECM proteins 73 through increased MMP-9 proteolytic activity also. 75
Types of Lasers and their Applications
Fractional CO2 laser
Fractional CO2 lasers ablate the skin in a grid-like pattern of MTZs, and stimulate a response termed selective photothermolysis. The zones of thermal injury are generally <500 μm in width, with controlled depth and density, to allow for rapid repair from the induced thermal injury from nearby uninjured tissue. 76 Water is the targeted chromophore in ablative laser treatment, which absorbs laser light at 10,600 nm in the skin where proteoglycan binding of water leads to a high percentage of water in the dermis, a common feature of HTS. 77 Although water also comprises 90% of the epidermis, CO2 lasers specifically target collagen in the dermis to stimulate wound healing and attempt to avoid high rates of epidermal damage. 76,78 CO2 lasers have also been shown to increase the regenerative capacity of adipose-derived stem cells by activating redox pathways, in turn increasing cell proliferation and secretion of angiogenic molecules. 79 In a multicenter and site-controlled study, 22 patients with HTS, who received 3 treatments of fractional CO2 laser, showed sustained and significant improvement of elasticity, thickness, and appearance, causing the HTS to resemble a mature scar. 80 In a study of 27 patients after three treatments of fractional CO2 laser, the most significant improvements were found in pigmentation, pliability, and height. 78 Patients typically have redness lasting at least 4–6 weeks post-treatment; however, the more powerful ultrapulse CO2 fractional laser commonly leads to skin recovery within 7–10 days after application, 62 which is generally faster in comparison to other ablative laser treatments. Clinical experience with a prototype diode laser with a wavelength of 1,500 nm, fluence of 5 mJ/cm2 to create microscopic treatment zones, results in the continuity of the epidermal cell layer being restored within 24 h. 81 In addition to epidermal regeneration, increased collagen III production and myofibroblasts were present after 7 days post-treatment. 81 Other studies also suggest that fractional CO2 laser treatments increase type III to type I collagen in mature burn scars, as well as restoring the collagen orientation more toward that of normal skin. 59 As reviewed earlier, some of these laser-induced increases in type III collagen are features found in immature HTS and thus the paradox remains unresolved in terms of how this is beneficial in HTS based on our current understanding. In a comparative study, ultrapulsed fractional CO2 laser significantly improved scar tone, texture, and appearance, 36 while utilizing cooling devices to prevent excess thermal damage to surrounding skin from/by the nearby thermal columns.
In many cases, CO2 laser treatment appears to require greater penetration than the default parameters to reach the deeper levels of HTS that have been suggested are necessary for successful therapy. To overcome this, stacked interrupted laser drilling HTS in two passes has been suggested to achieve higher clinical efficacy. While more treatment sessions are recommended for optimal results, a 30% reduction in scar firmness after a single treatment session has been found. 82 However, in a study of 118 burn patients, investigators found that after one treatment session, scar improvement occurs over 2 years as the skin regenerates its collagen and elastin. 83 It is important to note that greater penetration of thermal and other forms of injury to the dermis can be associated with the development of HTS (Fig. 4), so the mechanism by which this possibly hazardous approach of multiple lasers passes to extend their depth of penetration is effective remains unclear. After CO2 laser treatment with a fluence of 100 mJ/cm2, there was increased expression of chemokines CXCL12 (127% on day 3) and CCL8 (144% on days 3 and 5), 59 which may play a role in tissue reorganization. 84 In a clinical study of 171 patients, there was a significant negative correlation between the duration of the scar and magnitude of scar improvements after laser treatment, suggesting that earlier intervention with laser treatment for HTS may improve the degree of scar remodeling. 39
Fractional CO2 laser has been suggested to remodel densely packed collagen fibers and replace them with newly synthesized, randomly orientated collagen bundles and reduced vascularity. 75 Moderate to severe acne scars considered hypertrophic have shown a 40% reduction of scar area after treatment with fractional photothermolysis. 40 However, the optimal density of fractionated laser-induced microcolumns needed to show for significant improvement in color and texture for HTS appears to be a high density of ablative microcolumns approaching 20% of the tissue area. 85 After a single treatment of fractionated ablative CO2 laser, investigators have found that collagen induction is 40–50% more pronounced than fully ablative laser resurfacing. 41
Although there are significant histologic differences seen in HTS after ablative laser treatment, there can be limitations in patient satisfaction rates due to pain, pruritus, and pigmentation changes. 75,86 However, in a retrospective 6-month study of laser therapies, major adverse effects were considered rare and an accepted trade-off for improved remodeling of scar tissue. 87 The outcomes of fractional CO2 laser treatment appear to be reproducible, and hypopigmentation maybe be avoidable by “feathering” the treatment area. 88 Although other nonablative lasers have been suggested to require less downtime for patients, they often require multiple treatments and a higher overall cost. In a randomized control trial using a nonablative laser on normotrophic, hypertrophic, and atrophic burn scars, improvements in HTS were smaller, suggesting the limited depth of penetration of HTS with nonablative treatment maybe a factor. 51 Thus, based on cost, effectiveness, and treatment outcomes, fractional CO2 laser therapy has been suggested to deliver superior long-term outcomes.
In pediatric burns with HTS, ablative fractional CO2 laser therapy is less widely accepted; however, a recent study suggests that clinically significant improvements in pediatric HTS treated with lasers are immediate and less invasive than alternative therapies. 38 The ablative fractional CO2 laser has shown therapeutic improvements in range of motion in function-limiting scar contractures in children 1 month post-treatment. 87
Long pulsed Nd:YAG laser
Nd:YAG is a nonablative laser, with a synthetic solid crystal pumped by a high-intensity lamp delivering long pulses converted to heat in the tissues. The Nd:YAG laser utilizes a quality-switched (Q-Switched) function that creates concentrated laser beam pulses of high-intensity light with a wavelength of 1,064 nm. 89 Although this laser has been used for dark birthmarks and scars, tattoos, age spots, and moles, the Nd:YAG laser appears to suppress angiogenesis in pathological scars. 43,90 The long-pulsed Nd:YAG laser allows for safer laser treatment in a variety of skin types because it is weakly absorbed by melanin, resulting in fewer pigmentary alterations. 91,92 In a previous study measuring fibroblast collagen production 20 h after treatment with the Nd:YAG laser, a significant decrease in collagen production was found without affecting cell proliferation. 93 At 1,064 nm, the Nd:YAG laser (energy density of 75 J/cm2, exposure time per pulse of 25 ms, and repetition rate 2 Hz) shows potential to target hyperpigmented and dyschromic burn scars and appears selective for arterial blood vessels deeper in the scar, due to a relatively higher absorption of oxyhemoglobin compared to deoxyhemoglobin. 94
A frequency-doubling crystal may be inserted into the Nd:YAG laser beam to halve the wavelength to 532 nm, emitting a deeply penetrating (4–6 mm) green light, poorly absorbed by hemoglobin, melanin, and water. 95 These Q-Switched Nd:YAG lasers have a wavelength of laser light of 1,064 nm, and appear to have minimal adverse reactions making them safest for use in patients with dark complexion as the longer wavelength is minimally absorbed by melanin. 96 A comparative study was conducted in Egypt, including 60 darker skin colored patients, using Q-switched Nd:YAG laser for pigmented lesions at 8–10 J/cm2 for dermal lesions and 2.5–5 J/cm2 for epidermal lesions in up to 6 sessions. 42 The Nd:YAG laser appeared to be effective and safe treatment for more deeply pigmented skin lesions in these higher risk patients, with 56.7% showing an excellent response. 42
In a large retrospective cohort study, an Nd:YAG laser set at 1,064 nm has shown greater improvement in HTS compared to keloids following treatment every 3–4 weeks for 1 year. 43 The use of Nd:YAG lasers have been a more common treatment for cellulite or skin tightening for facial rejuvenation rather than HTS or keloid scars. 97 –99 However, in a retrospective chart review and photographic analysis, the 1,064 nm picosecond Nd:YAG showed significant improvement in early HTS with minor hypertrophy and hyperpigmentation as assessed using the Vancouver Burn Scar Scale. 44 Nd:YAG shows promise as a combination therapy with other lasers to suppress the redness and pigmentation of scarring as well as aid in skin tightening and rejuvenation.
A 7-year study found that the Nd:YAG laser at 1,064 nm with a pulse duration of 5 ms has similar efficacy and shorter recovery and treatment times to CO2 lasers with lower costs; however, this research was focused on facial rejuvenation rather than scarring. 100 Comparison between PDL and Nd:YAG laser treatments on HTS has shown significant improvements (36–38%) in scars, but no significant difference between laser types. 101 Patients undergoing three to eight treatments at 3- to 6-week intervals of hyperpigmented scars using 1,064 nm Nd:YAG picosecond laser showed a decrease in the melanin index by 39%. 45 In a retrospective, case-controlled study, a combination treatment of CO2 laser and Nd:YAG laser in minor linear surgical scars appeared to be a favorable alternative then monotherapy with a fractional CO2 laser, particularly with improvements in pigmentation. 46 A 1,064 nm Q-switched Nd:YAG laser was used to treat hypertrophic and keloid scars with low fluency at 1- to 2-week intervals. 47 This study showed decreased pigmentation, vascularity, pliability, and scar height. A limitation of Nd:YAG appears to be the increased number of treatment sessions required, lower predictability of outcomes, and lack of histological evidence of improvements, which appeared to be extremely variable from patient to patient. Unfortunately, there is little objective research of the effect of Nd:YAG on HTS treatment and more studies are needed.
Er:YAG laser
Er:YAG laser is an ablative fractional laser used to treat acne scars, rhytids, facial aging, and melasma. It generally uses a wavelength of 2,940 nm and is gentler when it is used in a fractionated pattern compared to the CO2 laser, making it useful for thinner skin. 102 However, the lack of “pure ablation” caused by the erbium laser raises the concern for reduced collagen remodeling due to the lack of dermal penetration, compared to the fractional CO2 laser. 88 In a large and controlled trial, burn scars treated with Er:YAG laser significantly improved viscoelastic deformity, skin roughness, and wrinkle depth. 48 The therapeutic effect of Er:YAG laser on wound healing has been examined in diseased periodontal tissue 2 or 6 weeks following initial therapy, which failed to show a beneficial effect of Er:YAG laser treatment in collagen maturation or wound healing. 49 Tissue samples taken 3 days after fractional Er:YAG laser had significantly increased mRNA expression of MMP1, 2, and 3, chemokines (CXCL1, 2, 5, and 6), and interleukins (IL-6, IL-8, and IL-24). 50 The Er:YAG laser with a pulse stacking technique showed histological alterations and shifts in gene expression related to epidermal inflammation, differentiation, and tissue remodeling. 50 Tissue samples taken 3 days after treatment using fractional Er:YAG laser therapy had reduced expression of MMP3 and 9, chemokines (CXCL1, 2, 5, and 6), and IL-8. 103 Er:YAG laser treatment showed anti-inflammatory effects, dermal remodeling, and increased epidermal differentiation.
The Sciton laser™ is an Er:YAG system, capable of skin resurfacing with two modalities, full field and fractional. At 1,319 nm, the pulsed energy laser targets fibroblasts in the dermal layer to stimulate collagen remodeling, and appears to improve scars, skin tone, and texture. 104 This laser uses a large-area pattern generator to evenly distribute the laser's path, preventing any region of the skin from overheating. 102 The Er:YAG laser uses up to 50 ms pulses at up to 40 W, and thermally targets fibroblasts in the dermis to stimulate collagen production. 102 In a randomized control trial, a nonablative 1,540 nm fractional Erbium-glass laser was used to target superficial and deep layers of burn scars, showing continuous improvement of HTS in histology. 51 After a 6-month follow up, the epidermis contained rete ridges similar to normal skin compared to the flattened dermal-epidermal junction at baseline, as well as collagen structure changing from thick parallel bundles to dense interwoven fibers with higher vascularization. 51
In another randomized control trial, the effects of long pulse Nd:YAG and fractional Er:YAG lasers were compared for facial rejuvenation. Both lasers significantly improved esthetic improvement scores, periorbital wrinkling, nasolabial folds, dyschromia, and skin laxity after three treatments associated wounds; however, Nd:YAG had significantly lower downtime for recovery. 52 Therefore for facial rejuvenation, Nd:YAG is the favored laser treatment. Acne and postburn scars also have a significant improvement following the treatment by Nd:YAG laser with lower cost, recovery time, and treatment period compared to Er:YAG and CO2 lasers, 100 although both nonablative and ablative laser treatments may yield skin rejuvenation based on the skin condition. However, studies have reported that the nonablative lasers are below the threshold of vascular injury needed to stimulate scar remodeling. 105 Thus, although preservation of the dermis is often an advantage in the short term with Nd:YAG lasers, the effects seen may not be sufficient for optimal long-term improvement.
Pulsed dye laser
Pulsed dye laser photons at 585–595 nm targets hemoglobin present in blood vessels, achieving selective photothermolysis, which is used for the resolution of the proliferative phase of wound healing. 106 Hemoglobin absorbs the energy produced by PDL, causing coagulation necrosis within blood vessels and tissue hypoxia. PDL has a lower wavelength and higher energy than Nd:YAG laser, causing the absorption of the energy by the hemoglobin to convert it into darker methemoglobin, acting as a chromophore. PDL energy downregulates connective tissue growth factor (CTGF) in cultured keloid fibroblasts. 107 CTGF is a strongly profibrotic growth factor, and is highly expressed in HTS and keloid scars. On this basis, PDL is purported to be useful for erythema and pruritus in HTS.
As discussed earlier, TGF-β1 is a fibrogenic cytokine that stimulates fibroblast proliferation and promotes HTS formation during adult wound healing, 108 and decreases with PDL treatment. 109,110 HTS treated with long PDL (595 nm) showed a mean improvement of 55% after the first laser treatment and 80% after the second treatment, measured on a 3-point scar scale. 111 Significant improvement in scar thickness, erythema, and pliability is seen at the 585 nm PDL laser setting, which is more effective in younger scars, <1 year old. 112,113 After two to three PDL treatments plus compression, scar height was lessened and tissue elasticity improved when compared with compression alone. 114 The efficacy of PDL has been tested using pulses ranging from 0.45 to 40 ms duration, 595 nm wavelength, and 7 J/cm2 fluence, and found that the shorter 0.45 ms pulse duration was more effective in decreasing scar size and improving scar texture. 115 A systematic review supports the use of 595 nm over 585 nm-PDL, showing moderate, but limited efficacy of the former over the latter for the treatment of HTS. 116 Two treatments of HTS within 4 weeks using 595 nm PDL with cryogenic spray cooling significantly improved scar pliability and decreased scar erythema-associated symptoms. 117
Traditionally, PDL has been used to improve ecchymosis; however, recent studies have reported hypertrophic or keloid scarring can occur as a complication from the excessive use of PDL. 118 PDL and Nd:YAG laser significantly improved both HTS and keloids with no perceptible difference between the two lasers. 54 Combined PDL and ablative CO2 laser also show significant improvement in HTS and keloids. 53,119 Caution must also be utilized with darker skin-toned patients, as the light energy in PDL can be competitively absorbed by melanin, increasing the risk of dyspigmentation. 120 PDL is used to treat immature, thin HTS <1 cm in thickness, discoloration and pruritus, but does not result in collagen remodeling to the same degree as ablative lasers. 67 Thus, although PDL has demonstrated variable efficacy in treatment of scars, it is necessary to use them with caution when treating patients with darker skin tones as a higher chromophore density predisposes to pigment damage in the skin.
Multiple laser combinations
A number of studies have evaluated the effects of treatment with combinations of different lasers versus monotherapy with a single laser. In a randomized and controlled trial, significant improvements in HTS overall scar profile were seen using CO2 laser ablation compared to the control; however, color and textural changes showed a greater improvement when a combination of CO2 laser ablation and intense pulsed light was applied. 121 In a therapeutic study of keloids, fractional CO2 laser was used, followed by a combination of PDL and Nd:YAG laser 55 ; however, this resulted in only partial improvement in size or thickness, color, and esthetic appearance. Other studies have demonstrated significant improvements in pigmentation, vascularity, pliability, and height after a combination treatment with PDL and Nd:YAG laser on surgical scars. 122 Dermatoscopy and reflectance-mode in vivo confocal microscopy demonstrated low numbers of narrow, horizontally oriented vessels and reduced collagen fibers in an improved, more random orientation, similar to the dermal layer of healthy skin at 1 week after treatment. HTS was significantly improved with no adverse effect after several treatments of combined PDL/Nd:YAG laser. 56 A study of 45 keloid patients receiving a combination of fractional CO2 and Nd:YAG laser showed the most significant clinical improvement than use of either laser alone, which also used a molecular assessment by measuring procollogen I. 123
Laser-assisted drug delivery
Apart from laser treatments, triamcinolone is the most frequently used intralesional corticosteroid for treatment of keloids or HTS. 124 Combination therapy of same-session ablative fractional laser and immediate triamcinolone delivery resulted in an overall significant improvement in HTS. 125 Autologous fat injection before fractional CO2 laser treatment in HTS is shown to significantly reduce pain and itching, while improving thickness, texture, and congestion of scar. 126 A recent study also uses platelet-rich plasma with CO2 laser, which showed to be more effective than laser treatment alone. 127 In this prospective cohort study on HTS, a combination treatment of PDL targeting pruritus and erythema and CO2 laser for texture, thickness, and stiffness showed statistically significant improvements in scar scores. 86 A similar study in larger numbers of patients assessed by a modified scar scale showed rapid, significant, and long-term improvements in HTS treated by combined PDL and fractional CO2 laser. 128 Specific to keloids, treatment with triamcinolone acetonide corticosteroid (TAC) injection with CO2 laser therapy has shown a mean recurrence of 15.4%, while TAC and intralesional cryotherapy have found a 12% recurrence, with no adverse effect reported at 6 months of follow-up. 129 In a randomized control trial with HTS, which used fractional monotherapy alone and in combination with topical corticosteroid following laser treatment, which both showed significant improvement in scar appearance from baseline, but no difference between treatment groups, suggesting for HTS fractional monotherapy is an effective treatment. 130 Other studies reaffirm a strong beneficial clinical effect on HTS treated with PDL combined with fractional CO2 laser and cold compression used immediately after laser treatment, with a mean treatment effect seen by 3 months. 57,58 PDL appears to coagulate blood vessels in the scar by targeting hemoglobin, while the CO2 laser reduced proliferation of fibroblasts and improved abnormal collagen organization. These studies provide strong evidence that combined PDL and CO2 laser therapy for HTS yields higher incremental gains in HTS improvement than monotherapy alone.
Remaining controversies in laser treatment of HTS
In a recent systematic review and meta-analysis of fractional ablative CO2 lasers using the Vancouver Scar Scale (VSS), pooled data from 8 studies included 282 patients showed an overall improvement of 29%. 131 This study was limited by the heterogeneity of treatment regiments where many other forms of treatment, including corticosteroids and additional lasers, such as the pulsed dye laser, were also used. The limitations of the VSS as a scar outcome measure include the lack of patient assessment, operator-dependent errors, failure to measure pain and pruritus, and inability to account for changes in pigmentation within large scars. Blinded placebo-controlled trials for scar treatment have found an average improvement in modified VSS of 30% over 6 months post-injury in the placebo group of burn patients, which argues stronger for studies that have more objective outcome measures, which are able to control for spontaneous improvement, and occur naturally in HTS after burn injury. In addition, in a systematic review of laser treatment of HTS following burn injury, it is suggested that the quality of the existing studies in terms of the risk of bias and methodological quality was insufficient to draw definitive conclusions of the benefit of laser therapy. 132
It is important also to consider the age of the scar subjected to laser treatment, where investigators such as Zuccaro et al. found a statistically significant improvement in VSS of HTS <12 months old. 132 In another systematic review, Karmisholt et al., suggested that earlier treatment of HTS <3-month duration during the inflammatory and proliferative phases of wound healing has a greater potential for reducing cutaneous scar formation. 133 However, Issler-Fisher et al. studied scars greater than or less than a 2-year duration and found similar improvements independent of scar age. 83
To improve the quality of design and outcome measures and to avoid potential ethical concerns for nontreated control wounds in human research, animal experiments using the red Duroc pig were conducted where the scars of skin-grafted third-degree burn wounds were assessed after either CO2 or Er:YAG ablative laser treatments. 134 –137 This model is sensitive enough to show statistically significant benefits of pressure garments in terms of scar contraction, hypervascularity, scar stiffness, and collagen fibrillogenesis. 135 –137 In this model, laser treatment increased transepidermal water loss, which returned to normal levels between 24 and 96 h. 137 Microthermal zones of treatment demonstrated significantly increased IL-6 and MCP-1 within 1 h of treatment, but resolved to baseline by 24 h postlaser, whereas slower and more sustained increases in TGF-β1 and TGF-β3 also occurred. 137 In a burn only injury in Red Duroc pigs, Er:YAG treatments demonstrated improvements in a modified scar scoring system. Increased expression of decorin as well as MMP2 and MMP9 mRNA by reverse transcription-polymerase chain reaction and western blotting was demonstrated in the scar biopsies compared to untreated control burn scars with fractional CO2 laser-treated wounds. 135 Scar volume may also be measured in an objective and reproducible way using ultrasound, as illustrated in Fig. 7. However, little difference in outcomes was found in scar properties in this model using the fractional ablative CO2 laser with pulse energies of 20–150 mJ/cm2 assessed by quantitative, objective measures. 134

Scar volume measurements using ultrasound as a newer, objective, reproducible, and quantitative outcome measure for the evaluation of HTS following burn injury.
Future Directions
This type of information supports the need for more clinical investigations using nontreated controls and objective outcome measures.
Summary
HTS and keloids are a result of deep dermal injury and are currently difficult to treat; however, lasers show significant improvement in scar conditions, when used appropriately to maximize benefits. Evidence suggests that treatment of HTS by fractional CO2, Nd:YAG, Er:YAG, and PDL lasers does offer improvements. For skin rejuvenation, tightening, or cellulite, the Nd:YAG laser treatment appears favorable; however, it may be less than ideal therapy alone for HTS or keloid treatment. Fractional CO2 laser has been purported to work at a biological level to reorient newly formed collagen bundles to a more “normal” orientation after re-inducing the wound healing process at a microscopic level. PDL targets blood vessels through hemoglobin; therefore, it appears to reduce pigmentation, pruritus, and erythema. Review of current existing literature supports combined treatment of HTS with PDL and fractional CO2 lasers to achieve the best results in color and texture for fibrotic scars in a minimal amount of recovery time and expense. Overall, ablative fractional lasers have more depth of penetration for HTS with thick morphology, showing better effectiveness with fewer treatments. However, further research in large-scale trials is needed to establish higher levels of efficacy for laser treatment of HTS.
Take-Home Messages
In HTS and keloid treatment, studies combining PDL and fractional CO2 laser therapy have shown the most significant results in vascularity, thickness, and overall outcomes.
In the future, larger scale efficacy trials are needed with more validated objective outcome criteria, which control for spontaneous improvement in HTS.
Also, basic research examining the pathological basis for scar treatment with lasers is required to create more specific therapy to prevent and treat fibroproliferative disorders of the dermis.
Footnotes
Authors' Contributions
L.S. was responsible for review of literature, drafting the review, histology figures, and editing revisions. E.E.T., J.D., and P.K. were responsible for ethics application, providing recommendations, and helping revise and edit the review. This review was supervised by E.E.T. All authors read and approved the final article.
Acknowledgments and Funding Sources
Support has been received from the Firefighters Burn Trust Fund from Edmonton Firefighter Association at the University of Hospital Foundation.
Author Disclosure and Ghostwriting
No competing financial interests exist. E.E.T. and J.D. made recommendations for structure, revision, and editing of the review.
About the Authors