
Abstract
Significance
: Diabetic foot ulcers (DFU) are a mounting problem with the increasingly frail population. Injuries that would otherwise heal are kept open by risk factors such as diabetes, obesity, and age-related conditions, which interferes with the natural wound healing processes.
Recent Advances:
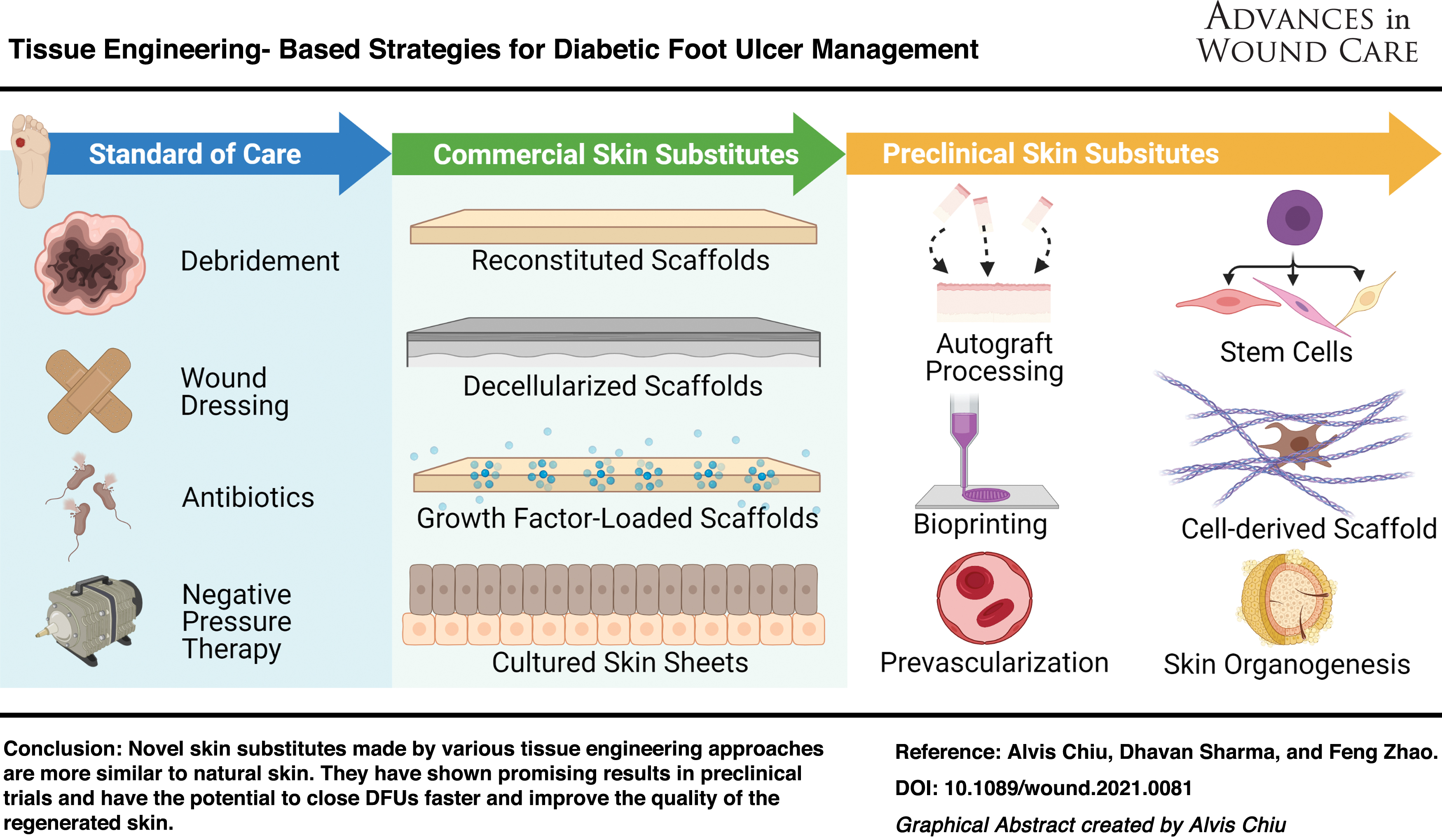
This review summarizes recent advancements in the field of tissue engineering for the treatment of DFUs. FDA-approved approaches, including signaling-based therapies, stem cell therapies, and skin substitutes are summarized and cutting-edge experimental technologies that have the potential to manage chronic wounds, such as skin printing, skin organogenesis, skin self-assembly, and prevascularization, are discussed.
Critical Issues:
The standard of care for chronic wounds involves wound debridement, wound dressings, and resolving the underlying cause such as lowering the glycemic index and reducing wound pressure. Current DFU treatments are limited by low wound closure rates and poor regrown skin quality. New adjuvant therapies that facilitate wound closure in place of or in conjunction with standard care are critically needed.
Future Directions:
Tissue engineering strategies are limited by the plasticity of adult human cells. In addition to traditional techniques, genetic modification, although currently an emerging technology, has the potential to unlock human regeneration and can be incorporated in future therapeutics.

SCOPE AND SIGNIFICANCE
Diabetic foot ulcers (DFU) are a major health care burden worldwide. In this article, various tissue engineering approaches to manage DFUs are reviewed. As skin substitutes for chronic wounds have been extensively assessed in the past, 1,2 more recent tissue-engineered therapeutics are the focus. These novel treatment modalities include growth factor therapies, stem cell therapies, three-dimensional (3D) bioprinting, and in vitro skin organogenesis. Their fabrication methods, modes of action, and healing outcomes are also discussed.
TRANSLATIONAL RELEVANCE
Wound healing is a complex process, which generally is divided into four temporal stages: (1) coagulation, (2) inflammation, (3) granulation tissue formation, and (4) re-epithelialization and extracellular matrix (ECM) remodeling. Dysregulation in any of these stages may inhibit successful wound closure, resulting in the development of ulcers. Unfortunately, achieving simultaneous wound closure and skin function regeneration of foot ulcers in diabetic patients is still a major challenge as psychologically harmful scars could affect treatment outcomes. In addition, the field is limited by a lack of a standardized wound healing measure by which to compare the efficacy and outcome of treatments. Identifying these gaps in research will benefit future research decisions.
CLINICAL RELEVANCE
The prevalence of diabetes in the elderly across the world is estimated to be more than 134.6 million, and this number is expected to jump to as high as 252.8 million by 2035. 3 The estimated annual incidence of foot ulcers among diabetics is 6%, 4 with recurrence rates ranging from 30.6% to 64.4% from 1 to 3 years. 5 Therefore, new therapies for DFUs are critically needed to minimize human suffering, productivity loss, and medical costs.
PATHOPHYSIOLOGY OF CHRONIC WOUNDS: KEY DIFFERENCES IN IMMUNE FUNCTIONING
The key difference between normal, acute wounds and nonhealing, chronic wounds occurs at later stages of inflammation (Fig. 1). The immediate immune response in nonchronic wounds consists of the of release of proinflammatory cytokines, production of antimicrobial peptides, and recruitment of phagocytic cells for pathogen elimination. 6 This primary response is continued by switches of macrophages from the proinflammatory (M1) phenotype to the regenerative (M2a, M2b, M3, M4) phenotypes, a key prerequisite for wound closure, which advances wound healing to the proliferative stage and then the remodeling stage. 7 In chronic wounds, healing does not follow the defined trajectory and is arrested at the late inflammatory stage. Unlike in normal wounds, where bacterial contamination is eventually cleared by the primary immune response, this arrested stage temporarily forms an equilibrium with the resident bacteria, resulting in a nonhealing ulcer, which can last for months or even years.

Key Differences in Immune Functioning between Acute and Nonhealing Chronic Wounds. Nonhealing chronic wounds develop a low-grade chronic inflammation that prevents the successful granulation tissue formation and wound closure. Color images are available online.
The pathogenesis of chronic wounds is driven by many factors and possible mechanisms. Some of these factors are (1) inadequate clearance of contamination, (2) insufficient production of regenerative growth factors and cytokines, which prevents granulation tissue formation and keratinocyte proliferation, and (3) a prolonged inflammatory stage with a sustained presence of proinflammatory cells and proteases that breakdown growth factors and ECM fibers. 8
Comorbidities, such as age, obesity, and diabetes, are risk factors for DFUs (Fig. 1). As age increases, a recurrent exposure to foreign antigens can stimulate systemic chronic inflammation 9 that entails enhanced levels of circulating proinflammatory cytokines 10 and effector T cells. 11 Diabetic patients also show high levels of proinflammatory cytokines and an increased population of memory and effector T cells, and even higher levels of such respondents were detected in patients with DFUs. 12 Additionally, macrophages fail to undergo phenotypic switch from proinflammatory to regenerative phenotype in obese and diabetic patients 6 due to increased interleukin (IL)-6 and tumor necrosis factor (TNF)-α levels. 13 Similarly, the higher leptin levels found in type 2 diabetic 14 and obese 15 individuals promote proinflammatory T helper cell polarization, 16 leading to a “chronic low-grade inflammation” phenotype, 17 which is unable to curtail bacterial contamination. High blood glucose levels also lead to the synthesis of reactive oxygen species (ROS) mainly through impaired mitochondrial glucose oxidation. 18
Even though ROS are critical for wound healing, excess ROS can impede healing by oxidizing DNA, proteins, and lipids. 19 The increase in ROS is especially taxing on cells with a limited capacity to regulate their glucose intake, such as endothelial cells (ECs), Schwann cells, and neurons, leading to cell death. 20 The resulting vascular insufficiency and nerve damage in the lower limbs cause ischemia and repeated trauma to the foot as the patient fails to sense pain. 21 The chronic inflammation eventually leads to immune exhaustion and failure to generate an efficient immune response that resolves infections and promotes wound closure. 22
Besides the immunological deficiencies, the prolonged inflammation also causes cellular changes that make the wound microenvironment unfavorable for healing. A prolonged inflammatory stage, caused in part by comorbidities, leads to the breakdown of regenerative growth factors that are responsible for directing the various cellular behaviors needed to close a wound. In healthy, acute wounds, platelets release growth factors, including epidermal growth factors (EGF), insulin-like growth factors (IGF), platelet-derived growth factors (PDGF), transforming growth factor (TGF)-α, and TGF-β. 23 Notably, both PDGF and TGF-β chemotactically attract fibroblasts, while PDGF stimulates re-epithelialization and revascularization, and reduces protein degradation. 24 EGF promotes the migration and proliferation of keratinocytes, fibroblasts, and ECs. 25 Macrophages produce fibroblast growth factors (FGF), which also induces fibroblast activation and proliferation. 26
Both macrophages and keratinocytes release vascular endothelial growth factors (VEGF) and damaged ECs also release FGF to increase angiogenesis to supply the wound with oxygen and nutrients. 27 In combination with TGF-β, FGF accelerates keratinocyte migration. 28 Fibroblasts are responsible for the secretion of proteases such as matrix metalloproteinases (MMPs) and their inhibitors, 29 which control the synthesis and degradation of ECM fibers as well as the aforementioned growth factors. 30 The absence of healing instructions from growth factors delay wound healing.
In summary, to close chronic wounds, three etiologies must be addressed: (1) clearance of bacterial infection, (2) restoration of regenerative growth factor and cytokine production, and (3) elimination of prolonged inflammation. However, for DFUs, even with successful reactivation of endogenous healing pathways, fibrosis often occurs in the healed skin, and the underlying ischemia and/or neuropathy is often unaltered. This article focuses on tissue engineering approaches for augmenting growth factor and cytokine production and immunomodulation. Newer methods designed to improve functionality and vascularity of healed skins are also introduced.
CURRENT APPROACHES FOR CHRONIC WOUNDS
Chronic wounds are normally managed by multi-pronged means, including debridement, dressings, and topical creams. While the strategy for standard-of-care treatments is to maintain a clean wound to prevent infection and facilitate endogenous wound healing, newer tissue engineering approaches introduce new cells and growth factors to stimulate healing. As the comorbidities have negative systemic impacts on the healing capacity of the patient's cells, relying on endogenous cells poses a risk. Many approaches that replace the growth factors, ECM, and/or cells in chronic wounds through tissue-engineered constructs have yielded better healing outcomes and faster wound closure rates than the standard of care.
Standard of care
Current standard-of-care treatments for DFUs include surgical debridement, appropriate dressings, wound offloading, controlling active infection, and reducing the glycemic index. 31 Surgical debridement, also known as sharp debridement, is a primary response in wound management, which removes necrotic and devitalized tissues surrounding the callus, thereby promoting granulation tissue formation and wound bioburden reduction. 32 Following surgical debridement, it is crucial to select an appropriate wound dressing. Generally, wound dressings should maintain a moist environment to promote granulation tissue formation, epidermal migration, and angiogenesis, however extra absorbing property is required by some wounds to remove excess wound exudates. 33,34 Therefore, no single dressing can be used as a universal material for all chronic wound types. Although a wide spectrum of dressings has been developed for wound management, they alone are insufficient for successful closure of chronic wounds. 35
After debridement, wound site protection and antibiotic treatments are often used. Plantar shear stress, the horizontal component of ground reaction forces, and the vertical plantar pressure are major factors that contribute to poor healing of chronic wounds at the sole of the foot, including some DFUs. 36 Shielding DFUs against plantar shear stress and pressure is a critical component of wound care as it significantly reduces chances of ulcer recurrence. It can be achieved through footwear modification using orthopedic walkers or total contact casting, a gold standard device in DFU management. 37 The fiberglass/plaster-based casting is designed to relieve pressure on the vulnerable areas of the foot that experience higher pressure through evenly distributing the weight. For DFUs located elsewhere on the foot, a vacuum pump has been utilized to reduce wound pressure. This negative pressure therapy has been known to stimulate wound contraction, granulation tissue formation, neoangiogenesis, epithelialization, and removal of excess wound exudates.
Several clinical studies indicated that inclusion of negative pressure besides standard of care in DFU patients showed superior healing outcomes, especially in reducing amputation rate and adverse events. 38 Moreover, a recent study involving swine model indicated that negative pressure therapy increased nearly three-fold the expression of VEGF at the negative pressure-treated site, signifying its potential role in promoting angiogenesis. 39 Also, bacterial infections are a known predictor of poor healing as well as amputation, 40 and broad-spectrum empiric antibiotics are used for mild-to-severe DFU conditions. 32 Furthermore, controlling blood glucose level as a standard of care is widely accepted to improve patient immune response and reduce bioburden. However, it is still unclear whether intensive or conventional glycemic control has a beneficial or detrimental effect on treatment outcomes of DFUs. 41
Adjuvant therapies for the nonhealing chronic wounds
Several adjuvant therapies have been shown to enhance the therapeutic outcome of DFUs. These include nonsurgical debridement agents, wound dressings, topical agents, oxygen therapy, growth factor treatment, acellular grafts, as well as tissue-engineered skin grafts.
Nonsurgical debridement techniques include autolytic debridement, enzymatic debridement, and mechanical debridement, which offer various advantages such as cost-effectiveness and pain reduction. By providing a balanced moist environment in wounds, some hydrogels can facilitate autolytic debridement through recruitment of host cells and secretion of endogenous proteolytic enzymes. 42 Besides hydrogels, clostridial collagenase ointments have been known as the most common enzymatic debridement agent. 43 Maggot and larval-based debridement can reduce bacterial contamination as well as improve fibroblast migration and skin perfusion. 44 Versajet™, a mechanical debridement system that uses high-pressure steam of sterile normal saline, has also been used as an alternative to surgical debridement in lower-extremity DFUs. 45
Several wound dressings and topical agents have recently been in practice as adjuvant treatment options. Alginate dressings are the most common absorbent products, which can absorb large volume of wound exudates, while preserving a moist microenvironment. These dressings have been proved to be more effective than traditional dressings, such as moistened gauze, Vaseline gauze, and hydrofiber, in healing DFUs. 46 Nonconventional topical compounds, phenytoin, and honey, have also shown a significant reduction of wound area and bacterial infection compared with control saline treatment. 45 Since DFUs are associated with impaired oxygenation due to ischemia, topical or systemic oxygen delivery has been studied to promote healing. Although there is insufficient evidence to conclude that topical or systemic oxygen therapy enhances DFU healing in particular, the topical or systemic oxygen therapy can enhance the DFU healing, 45 a novel hemoglobin spray that transports oxygen from atmosphere to hypoxic wounds through diffusion has shown effectiveness for faster wound closure. 47,48 However, as the innate healing ability of DFU patients is compromised by comorbidities, new approaches delivering cells and/or growth factors in tissue-engineered constructs have been clinically shown to be more efficacious than the standard care. 49,50
Growth factor therapies
Since chronic wounds are caused in part by the lack of regenerative growth factors and cytokines, 51 one way of reversing this problem is to simply administer the bioactive signals to the wound. Growth factor therapies directly increases the concentration of deficient cytokines, growth factors, or other proteins in the wound bed. These therapies aim to overcome the dysregulated signaling caused by the degradation of growth factors, to upregulate signals instructing angiogenesis, cell proliferation, and wound regeneration. 51 This section reviews growth factor products that are commercially available or currently being evaluated at the preclinical stage.
Endogenous growth factors
Platelets contain a whole host of growth factors involved in every stage of wound healing in their α-granules, which release their contents after degranulation at wound sites, making them an ideal source of endogenous growth factors. 52 Among others, PDGF and TGF-β are chemotactic and mitogenic toward inflammatory cells, and FGF toward fibroblasts. 53 Both PDGF and EGF promote re-epithelialization, and VEGF induces angiogenesis. 53 Platelet-rich plasma (PRP) is a fraction of blood plasma containing a high concentration of platelets. 54 It is obtained by centrifuging blood twice, first to separate blood plasma from red blood cells, then the platelet-rich fraction from the platelet poor. Thrombin is then added to artificially degranulate the α-granules. The gel product can act as a tissue sealant and close chronic venous ulcers. 54 The platelets in PRP provide growth factors in natural ratios, and the gel promotes fibroblast proliferation and tissue vascularity, 52 resulting in better wound healing compared with standard of care. 55 PRP has also been further engineered by adding hyaluronic acid (HA) 56 or pressing the PRP into membranes 49 to improve its efficacy.
Newer blood-derived products, such as “platelet-rich fibrin” 57 and “concentrated growth factor,” 58 have been made with more advanced centrifugation techniques, creating larger, denser, and more potent fibrin matrices, but the underlying technology and mechanism of action remains largely the same. It has been shown that concentrated growth factor treatment closed chronic wounds smaller than 10 cm2 within 3 months. It has also improved the closure of wounds larger than 10 cm2. 58
Exogenous growth factors
Due to the limited supply of autogenic growth factors, exogenous recombinant growth factors are being used as off-the-shelf-products. 59 Growth factor therapies for DFUs are delivered through solutions, gels, creams, and ointments externally. 60 However, they are broken down by wound proteases and cannot penetrate the intact skin surrounding the lesion. The barrier function of the periwound skin and exudation in the wound bed limit the in vivo efficacy of topical applications of growth factors. 61 These factors may be responsible for the conflicting efficacy data for growth factor therapies seen in preclinical trials. 62 Therefore, current growth factor treatments often rely on high doses and frequent daily administrations. To reduce the frequency of administration and improve efficacy, tissue engineers have developed functionalized scaffolds as delivery systems that can sustain the release of growth factors while increasing their stability. 60
Growth factor-functionalized scaffolds serve as both a 3D structural support for host cell infiltration and a growth factor delivery system. Growth factors can be loaded into the scaffold, such as gelatin, by absorption or encapsulation during the scaffold fabrication process. 63 The only FDA-approved growth factor-based product for DFUs is Regranex®, which delivers recombinant human PDGF in a sodium carboxymethylcellulose gel. 64 The addition of recombinant PDGF to standard care increased the complete wound closure rate at 20 weeks by 15%. 65 Besides Regranex, EGF 66 and FGF 62 -functionalized hyaluronic and chitosan scaffolds have also shown sustained growth factor release and improved healing of wounds in diabetic rodents.
A recent approach using silk fibroin-based microparticles sustainably released insulin for up to 28 days in diabetic rats and improved wound healing. 67 Another study conjugated stromal cell-derived growth factor-1 to an elastin-like peptide, which allowed the fusion protein to self-assemble into nanoparticles, thereby improving its stability in wound fluids. 68
In diabetic mice, the conjugated growth factor induced more vascularization than the unconjugated control. Despite the promising results of growth factor functionalized scaffolds, some evidence suggests that the delivery of one growth factor alone may not be sufficient. 69 This may be due to the different roles each growth factor plays in wound healing and their complex spatiotemporal expression patterns.
Commercially available skin substitutes
Whereas functionalized scaffolds are designed primarily to slowly release exogenous growth factors, skin substitutes stimulate chronic wound healing by providing proregenerative microenvironments. The diversity of skin substitutes makes it difficult to compare different types of substitutes and determine the optimal treatment, as the studies on commercially available products have been reported to be moderately biased and are often done between two products only, 2 often generating contradictory evidence. 70 A comprehensive guide of commercial skin substitutes for chronic wound treatment has been published recently by Snyder et al. 2 As the inclusion of cells imposes significant manufacturing, regulatory, and logistic hurdles, commercial skin substitutes are summarized in this study according to cellularity: acellular and cellular.
Acellular skin substitutes
The first skin substitutes were patches of protein matrices designed to augment the chronic wound ECM and prepare the wound bed for skin graft integration. 2,71 The healing-conducive extracellular environment drives advancement through the natural stages of wound closure. Collagen is one of the most widely used biomaterials for acellular skin substitutes. It restores equilibrium to the wound microenvironment by inhibiting the release of MMPs and other proteases responsible for perpetuating the chronic wound state. 72 The collagen fibers also mimic native healthy extracellular environments and provide arginine–glycine–aspartate (RGD)-binding sites 73 that promote cell adhesion, migration, proliferation, and angiogenesis. 74 Collagen scaffolds have been reconstituted from various processed animal tissues (Fig. 2). Available since the 1980s, Integra® Dermal Regeneration Template is sourced from bovine tendons and infused with shark-derived chondroitin sulfate, 74 which promotes cell proliferation and migration 75 and also modulates inflammation. 76
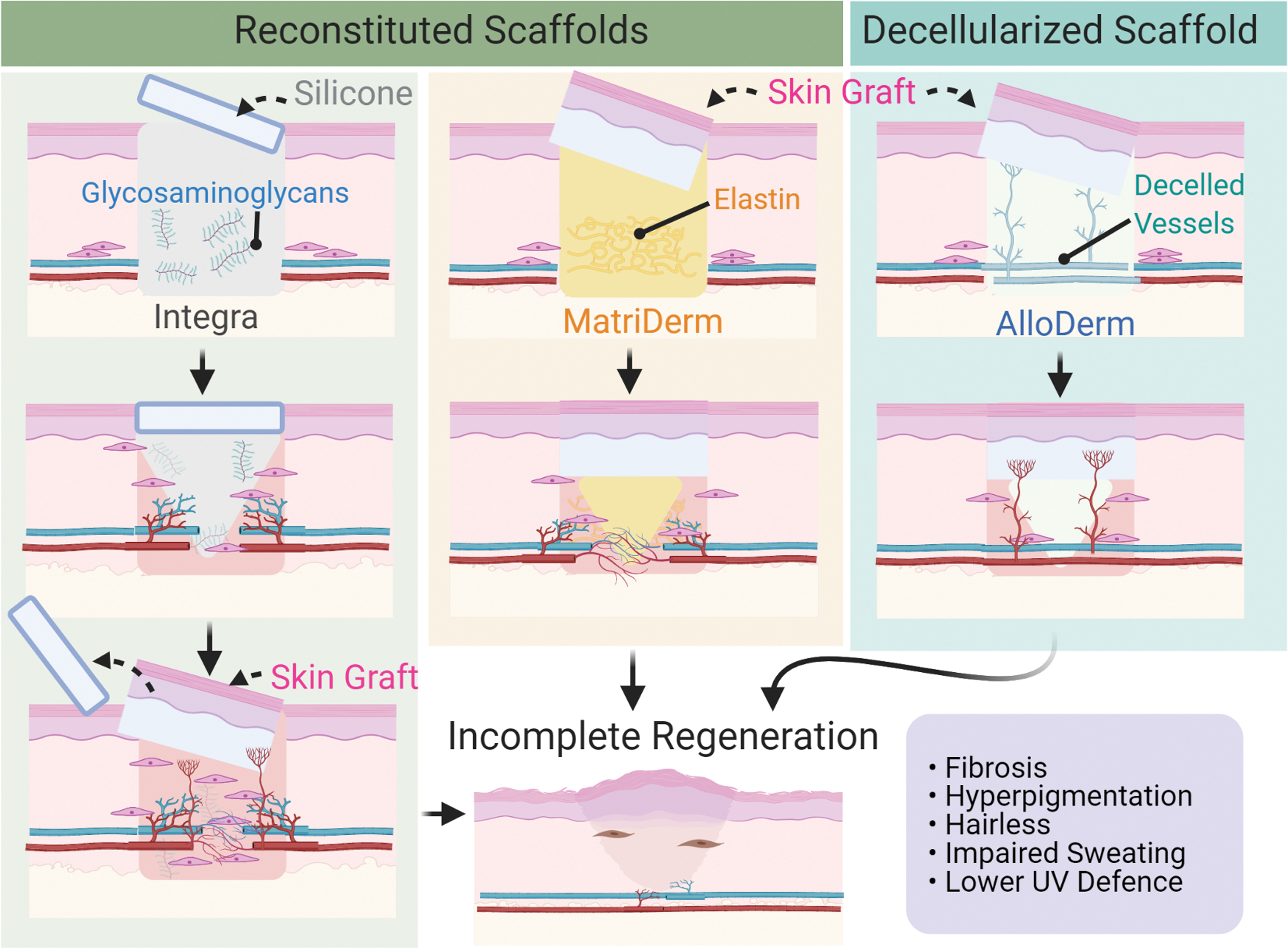
Modes of Action of Acellular Skin Substitutes. Integra® facilitates the growth of a vascularized neodermis under the protection of a transparent silicone cover. MatriDerm® allows rapid angiogenesis in its matrix and accelerates anastomosis of the graft with the host. 78,79 The MatriDerm strategy is a one-step procedure by implanting the skin with the MatriDerm, but Integra requires a two-step procedure for the replacement of the silicone with a skin graft after sufficient vascularization. 74 AlloDerm® possesses vascular architecture, which are colonized by host cells for rapid anastomosis. 85 Color images are available online.
The collagen fibers are chemically crosslinked by glutaraldehyde into a porous scaffold. It is then covered by a protective transparent silicone film, 77 which allows for visual inspection of the healing wound. 74 Another similar product used for chronic wounds is MatriDerm®. It is made of bovine dermis collagen fibrils coated with bovine ligament elastin that provides mechanical strength and also promotes angiogenesis. 78,79 Besides these two products, there are countless other acellular skin substitutes in the market, each with their own strengths and weaknesses depending on the therapeutic properties of their components. In a randomized clinical study, collagen dressings were changed two or three times a week for DFUs and resulted in a higher rate of complete healing (82.4% vs. 38.5%, p = 0.022) and faster wound closure compared with a polyurethane foam dressing. 80
More recently, skin substitutes made by decellularizing allogeneic and xenogeneic skin have attracted much attention for research. 2,81 The aforementioned skin substitutes, such as Integra®, were fabricated by supplementing a homogeneous biomaterial scaffold (collagen) with a select few therapeutic ingredients (chondroitin sulfate). However, native ECM is a heterogeneous scaffold with cell-instructive architecture made of various compounds, such as collagen, glycoproteins, and proteogylcans. 82 The structural and chemical complexity of ECM makes faithfully reproduction through chemical synthesis challenging. 82 The decellularization strategy aims to leave a relatively intact skin ECM scaffold to serve as a skin substitute while eliminating graft immunogenicity and eschewing chemical crosslinkers that can cause cytotoxicity and impede tissue remodeling. 83,84 Available in the United States, AlloDerm® (Fig. 2) preserves not only the dermis, but also the structural elements of blood vessels, which can be rapidly taken over by host ECs. 85
Alternatively, CGPaste®, a decellularized skin paste from Korea, has the advantage of being able to be spread over has been used for small, but deep chronic wounds, which are unsuitable for skin grafting, for a mean healing time of 2.4 weeks and a success rate of 71%. 86 More recently, Derma-Gide®, a porcine decellularized matrix, has been approved by the FDA and is reported to be efficacious for DFUs with a mean heal time of 2.7 weeks. 87 However, complete re-epithelization of wide defects using only decellularized or reconstituted scaffolds is still hard to achieve, and hyperpigmentation and fibrosis still occur after wound closure (Fig. 2). 86 This urged the inclusion of cellular components in skin substitutes with attempts to improve the quality of the healed skin as well as the wound closure rate.
Cellular skin substitutes
The first cellular skin substitutes were cultured epidermal autografts made of keratinocytes. Unfortunately, grafting of these keratinocyte sheets alone led to blistering in addition to scarring and wound contracture due to the lack of a dermal–epidermal junction that bound the epidermis to the dermis, which made it extremely susceptible to friction. 88 The proteases in the wound site also reduced the uptake of epidermal grafts to 30%–80%. 88 To overcome these issues, cultured dermal autografts of fibroblasts were used in conjunction (Fig. 3A). In this bilayered construct, the epidermal–mesenchymal crosstalk contributed to epidermal stratification, dermal–epidermal junction formation, higher tensile strength, augmented cytokine and growth factor secretion, and increased angiogenic properties. 89 The crosstalk was mediated by mostly paracrine signaling. The bilayered construct secreted different levels of IL-6, IL-8, VEGF, and IGF-1 compared with single-cell-type constructs, leading to differential expression of genes such as bone morphogenic protein, FGF1, and PDGF. 89 Collagen IV also appeared at the dermal–epidermal junction of bilayered constructs, but not in single-cell-type constructs, indicating that both cell types are needed for basement membrane deposition.

Schematic of Cell-based Therapies.
One of the earliest bilayered products, from 1997, was the TissueTech Autograft System® that combined two existing products, Hyalograft 3D® (the dermal compartment) and Laserskin® (the epidermal compartment). 90 However, the product was later discontinued. Apligraf® is a similar product, except that the cells are not autologous, but from allogeneic neonatal foreskin keratinocytes and fibroblasts (Fig. 3A). 91 Although Apligraf was clinically effective in treating DFUs, immunologically inert, and did not trigger acute rejection responses, the cells were short lived and completely eliminated in 4 weeks. 91,92
Limitations of skin substitutes
Commercial skin substitutes face several challenges when closing DFUs. For instance, the neodermis generated by using Integra has no skin appendages because it fails to regenerate hair-inductive epithelial cells for de novo hair follicle regeneration, and lacks nerve endings and elastic fibers in the healed skin (Fig. 2). 93 Similarly, autologous or allogeneic cellular skin substitutes cannot eliminate fibrosis and the lack of appendages. 2 Consequently, skin substitutes, whether acellular or cellular, are still associated with poor cosmetic outcomes, low ultraviolet protection, absent temperature regulation, and scar contractures. 24 Since DFUs are usually covered under footwear, esthetics and UV protection outcomes have not been prioritized. Nonetheless, scars may indirectly effect DFU outcomes through the mental state of the patient. Ngaage and Agius 94 suggested that scars may exacerbate depression and anxiety, which are already widely prevalent in DFU patients. 95 Also, the perception of inefficacy of DFU skin substitutes resulted from poor cosmetic outcomes may be generalized to a perception of inefficiency of diabetic medication, leading to poor medication adherence. 96 Currently, no research has been published on the effect of DFU healing outcomes on diabetes medication adherence.
Besides therapeutic efficacy, cost is another important concern for health care product design. The cost and the therapeutic efficacy of skin substitutes may not always correlate. 97 A recent health care economics study found that due to the product cost and the number of applications required to close a DFU, acellular skin substitutes may end up being more cost-effective than cellular ones. 97 For example, DermACELL® (a decellularized skin substitute), Integra, and Apligraf cost $2001, $3335, and $4169 per patient, respectively, but displayed 68%, 51%, and 58% DFU closure rates at 16 weeks, seemingly suggesting that the decellularized skin substitute is superior in price and efficacy. But, as the healing rates were simply cited from clinical trials with varying operationalizations of therapeutic effect, patient populations, and quality, a conclusion about the “best” product for DFUs cannot be accurately drawn. These confounding factors remain a challenge when comparing skin substitutes and need to be overcome by large-scale multicenter randomized controlled trials.
Since cellular skin substitutes were made with a heterogeneous population of stem cells, progenitor cells, and differentiated cells harvested from patients, constructs made solely from stem cells with their superior differentiation potential, healing capacity, and fabrication simplicity are under investigation.
Stem cell therapies
Stem cells are a relatively new cell source in treating chronic wound healing and are highly valued for their proliferative, self-renewal, and differentiation capacity. The most common stem cells for the treatment of chronic wounds are mesenchymal stem cells (MSCs), derived from bone marrow and adipose tissue in clinical trials, 98 and chosen for their therapeutic effects and ease of harvesting. 50 Other types of stem cells being studied include induced pluripotent stem cells (iPSCs) and embryonic stem cells, which faces tumorigenicity concerns and ethical issues, respectively. 99 The strategies summarized in this section focuses on tissue-engineered constructs using the two most popular and promising stem cells: MSCs (Fig. 3C) and iPSCs (Fig. 3D).
Mesenchymal stem cells
Often referred to as the “drugstore” or “medical signaling” cells by researchers, MSCs drive chronic wound healing by improving the wound microenvironment through paracrine signaling (Fig. 3B). 100 These adult stem cells naturally participate in wound healing 101 and localize to wound sites in response to injury. 100,102 Once at the site, they secrete chemokines that lower the level of proinflammatory signals being sent out by immune cells and MSCs, 101 and promote the switch of macrophages from the inflammatory M1 phenotype to the anti-inflammatory M2 phenotype through paracrine signaling and cell–cell contact, 103,104 which direct the healing process toward tissue regeneration instead of fibrotic repair. 105 MSCs also decrease the amount of infiltrated immune cells and the level of proinflammatory cytokines associated with fibrosis, such as IL-6, IL-1, and TNF-α (Fig. 3). 106 The growth factors secreted by MSCs, including VEGF, EGF, HGF, FGF, and many others, drive various steps of wound healing: cell migration, proliferation, angiogenesis, and re-epithelialization. 101,107 –109 Furthermore, MSC-derived exosomes have recently been found to stimulate pancreatic regeneration in induced type 1 diabetic rats. 110 There are also reports of MSCs reversing femoral neuropathy in rodents, 111 differentiating into various wound-resident cells, 112 and secreting collagen III (Fig. 3), 113 signifying MSCs’ promise for DFU treatment.
Numerous randomized controlled trials have shown that overall autologous and allogeneic adipose or bone marrow-derived MSC therapies are more efficacious than standard care for DFUs, although not all patients were receptive to MSC therapy. 50,98 Autologous in this case refers to MSCs harvested from the patient, expanded outside of the body, and reintroduced into the body. However, most MSCs in clinical trials are delivered through injections of cell suspensions. 114 This approach results in low cell survival, and inadequate cell retention at the DFU site. 101
To further improve the efficacy of MSC therapies, tissue engineers have focused on designing new cell delivery methods 98 and cell culture conditions with the aim to optimize growth factor production, cell proliferation, cell engraftment, and cell survival through manipulating extracellular factors. Delivering MSCs in scaffolds made of biomaterials, such as HA, fibrin, 115,116 collagen, or a mix thereof, 117,118 have been found to prevent MSC death and accelerate healing in chronic wound animal models. For more insight into biomaterial design, Khademhosseini and colleagues 119 have succinctly summarized the physical and biochemical properties of various biomaterials for tissue regeneration. More recently, a self-healing hydrogel made from N-carboxyethyl chitosan and adipic acid dihydrazide with HA-aldehyde, was developed to be injectable and crosslinkable in situ, making MSC delivery easier while preventing the cracking problem of past hydrogels. 120 The scaffold successfully protected MSCs from the inflammatory microenvironment and promoted M2 macrophage activation.
Aside from the scaffold on which the MSCs are seeded, the culture condition has been augmented with extracellular signals, such as neurotrophin-3, EGF, 121 or FGF, 121 and hypoxia, 122,123 to improve cell proliferation and angiogenic properties after implantation. In a recent study, Yang et al. 124 preconditioned MSCs in timolol, a beta blocker indicated for hypertension, in hypoxia on an Integra scaffold in conjunction with daily timolol administrations. The preconditioning improved wound epithelialization, lowered proinflammatory cytokine, IL-1B, and IL6 levels, and improved immunomodulation and angiogenesis compared with unconditioned MSCs in genetically diabetic db/db mice.
Although the delivery of MSCs in tissue-engineered constructs have successfully reduced the inflammatory response and upregulated regenerative signals in DFUs, MSCs exert their therapeutic effects mainly through mobilizing wound-resident cells and not through cell differentiation. 125 The efficacy of MSCs is also compromised by age 126 and diabetes 127 -associated changes such as accumulated DNA damage and oxidative impairment. 126 These alterations impact relevant MSC functions: cell proliferation, paracrine signaling, and immunomodulatory properties. 127 Recently, Zhang et al. discovered that donor-specific variation in MSC immunomodulation and cell proliferation is caused by IFN-γ and NF-κB signaling impairment. This may explain the lack of therapeutic efficacy in some patients. 128 iPSC therapy is emerging as an alternative stem cell therapy that can directly replace wound-resident cells and mitigate the effect of aging and diabetes on stem cells.
Induced pluripotent stem cells
Compared with MSCs, iPSCs can be harvested from skin, hair follicles, and other tissues, negating the need for invasive procedures of extracting adipose tissue or bone marrow tissue. 129 The pluripotency of iPSCs is generally utilized to generate difficult-to-harvest cell types deficient in DFUs (Fig. 3D). For example, human iPSC-derived ECs and iPSC-derived smooth muscle cells (SMCs) have been shown to increase perfusion and vessel density through angiogenic paracrine signaling and cell incorporation in new blood vessels. 130 iPSC-derived neural crest-like cells were examined for treating diabetic neuropathy in streptozotocin diabetic mice, and have demonstrated capability in improving motor and vascular functions (Fig. 3). 131
Remarkably, harvesting primary cells from chronic wound beds of diabetic patients, converting them to iPSCs, and then differentiating them back into somatic cells can reverse the influence of diabetes on those cells. 132 iPSC-derived fibroblasts, 132 EC progenitors, 133 SMCs, 134 and MSCs 135 from DFU patients are reported to acquire epigenetic modifications, which enable them to perform as well as nondiabetic cells. Similarly, iPSCs from older donors are comparable to those from younger donors in differentiation potential, senescence, and function due to resetting of epigenetic markers. 136 The rejuvenation effects of the dedifferentiation process suggest that iPSC-derived MSCs may outperform ex vivo expanded MSCs, especially with older patients. More studies are needed to clarify the benefits of this approach in DFUs.
Initial iPSC trials were also limited by cell engraftment and survival. 130 Similar strategies used for MSCs have been applied to iPSCs, and scaffolds for iPSC-derived cells are in development to maximize iPSC survival in the hostile chronic wound microenvironment. Tissue-engineered constructs using iPSCs for chronic wounds are mostly vascularized, with hiPSC-ECs and hiPSC-SMCs incorporated in scaffolds, such as collagen, 134 HA, 133 and electrospun polycaprolactone/gelatin scaffolds. 137 Those materials successfully increased cell survival and retention at the wound site while boosting angiogenesis and M2 macrophage count. Later studies have investigated the effect of a collagen HA hydrogel crosslinked in situ, and found an increase in cell viability and a maintenance of VEGF, FGF, and PDGF secretion compared with a collagen hydrogel. 138 Another strategy used by the same group examined the effect of collagen fibrillar density, which altered the mechanical strength of the scaffold, on iPSC-SMC paracrine signaling. 139 They found that incubating the cells in a dense collagen fibrillar scaffold made from plastic compression in a rolled configuration promoted cell proliferation and migration and increased the secretion of VEGF, IL-10, TGF-β, and IL-8 compared with a flat configuration, as the rolled configuration created a physiologic hypoxia gradient that upregulated angiogenic genes. 139
The rejuvenation ability of iPSCs makes it possible to outperform other cell therapies, as therapies without a dedifferentiation step remain debilitated by diabetes and age. This is critical as all DFU patients have late-stage diabetes and the mean age of the patients is 59.3 years. 140 Therefore, iPSC-MSC or iPSC-SMC therapies are likely to have higher therapeutic output than traditional MSC therapies in DFU patients. Unfortunately, iPSCs are currently still limited by teratoma formation for clinical trials, 141 so most of the research outcomes have not been translated to humans yet, and likely will not be until the malignancy can be brought down to safe levels. 140 Alternative approaches have focused on producing tissue-engineered constructs that mimic native skin structure.
NOVEL APPROACHES FOR CHRONIC WOUNDS
Recent advancements in tissue engineering have combined cells, growth factors, and scaffolds to create more sophisticated skin substitutes for chronic wounds. The complex interactions among cells, signals, and scaffolds better recapitulate skin nativity than treatments with separate components. Several experimental approaches to treating wounds has the potential to be used on DFUs: (1) 3D bioprinting aims to recreate the architecture and cell distribution of the skin to generate skin appendages and reduce fibrosis, (2) self-assembled constructs replace synthetic scaffolds with autologous patient-specific scaffolds and growth factors, and (3) skin organoids (Fig. 3C) recapitulate the embryonic developmental pathways to regenerate lost skin appendages. These tissue engineering strategies reproduce different aspects of healthy skin and pave the path for affordable and effective DFU treatments.
Skin bioprinting
Skin bioprinting is an emerging strategy of applying principles of 3D printing to skin tissue engineering. Skin substitutes often have poor cosmetic outcomes. Some of this is due to the unnatural distribution of cells in the graft and failure of the graft to integrate and vascularize upon integration. 142 The unnatural cell distribution can be caused by overlaying 2D skin substitutes over 3D wounds. Restoring the proper layering of the skin through various bioprinting methods can augment the proliferation and migration of multiple cell types, 143,144 leading to better healing outcomes.
In situ skin printing is a promising innovation that aims to print the missing skin parts directly onto the wound site. 143 This technology can overcome the limitation of some cell therapy approaches, such as cell sprays, which are unable to deliver specific cells to specific sites. First, a hand-held laser scanner is used to scan the wound site, and a 3D model of the wound is generated. Then, the printer arm pathway needed to fill the deficits is calculated, and the wound is split into layers corresponding to the dermis and the epidermis (Fig. 4A). The correct type of cells and scaffolds are then printed to fill up the wound to the appropriate level (Fig. 4B), before switching to another cell type. The printing system is based on inkjet printing, where a pressure source pushes the cell delivery system through the nozzle. The bioinks are keratinocytes or fibroblasts embedded in a fibrinogen and collagen matrix, with respective cell types being stores in different cartridges, akin to the color inks of traditional printers. 143
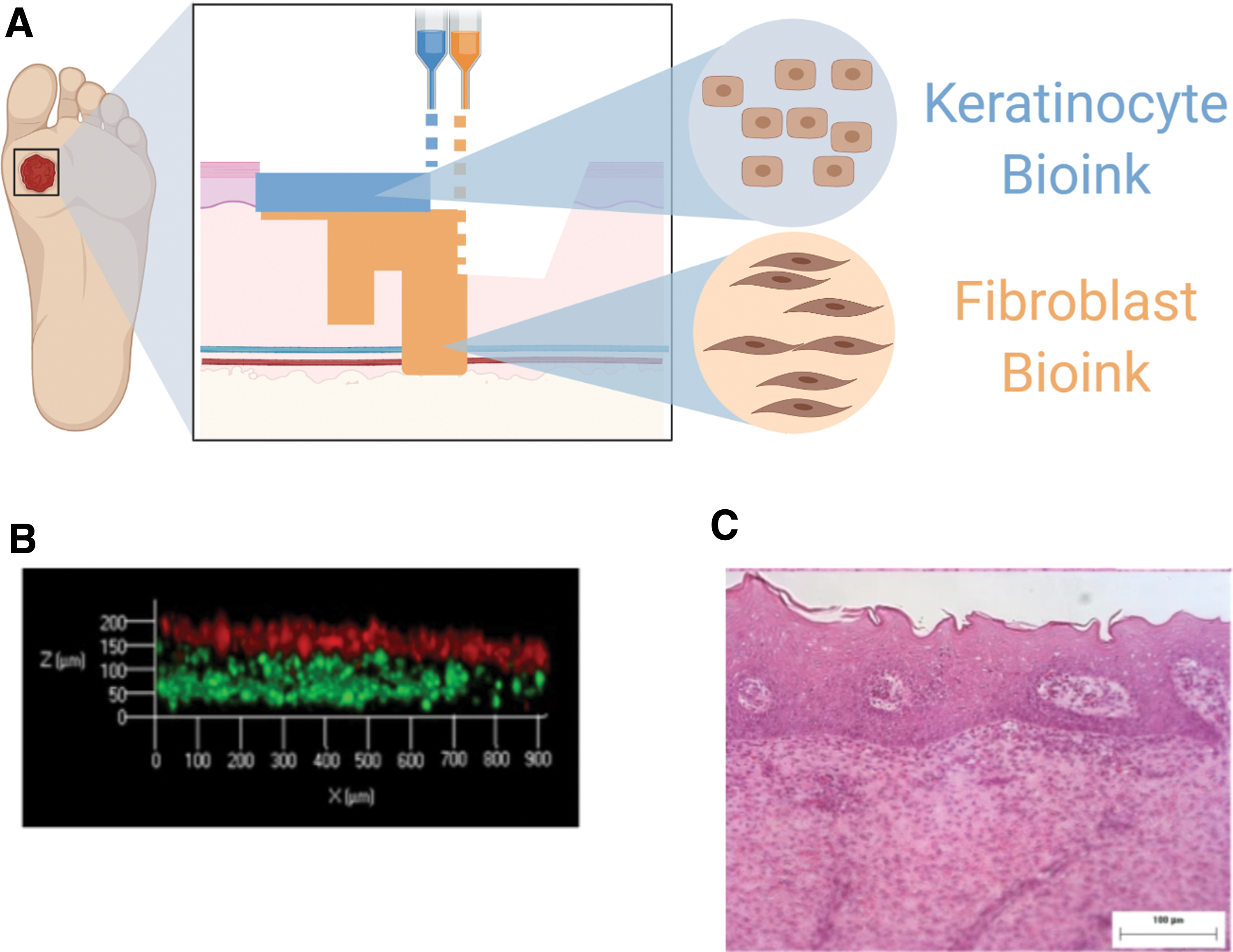
Schematic of in situ Bioprinting.
In a porcine excisional wound model, 3D in situ bioprinting with autologous cells showed promising results. Re-epithelialization occurred after 2 weeks and thickened and pigmented after 4 weeks. Histological staining showed the formation of papillary dermis, stratified epithelium, and rete pegs (Fig. 4C), which are missing in scar tissue. 143 Albanna et al. believed that in situ bioprinting yielded superior outcomes compared with cell spraying because the bioprinting method allowed the dermal fibroblasts, and epidermal keratinocytes are printed in such a way that the cells are spatially distributed according to the unique wound topography, matching the surrounding layers of tissue. Perhaps due to the lack of hair follicle stem cells, no hair follicles were regenerated.
Takeo et al. recently published a protocol for expanding hair follicle stem cells capable of regenerating entire hair follicles. 145 Incorporation of such cells may aid skin appendage growth. Also, melanocytes have been incorporated into bilayer cellular constructs and shown to grant UV protection. 146 To our knowledge, inclusion of skin appendages or melanocytes in in situ bioprinting has not yet been attempted and are promising directions for future research. Another avenue for future research is using lineage-specific subpopulations of fibroblasts that are predisposed to skin regeneration. 147 However, skin bioprinting uses many exogenous materials to create bioinks, and approaches that rely solely on cell-secreted, autologous materials may be more beneficial for chronic wounds.
Skin self-assembly and organogenesis
Skin bioprinting is limited in cell variety and scaffold biocompatibility. The skin tissue consists of immune cells, nerve cells, melanocytes, fibroblasts, ECs, keratinocytes, hair follicle cells, and sweat gland cells, with distinct subpopulations, of which, only a few cell types are presented in skin substitutes. The closing of chronic wounds using a selected few cell types of the native skin results in missing functions due to the absence of the cells constituting higher-order structures that maintain specific functions such as temperature control, UV protection, physical sensation, and mechanical properties. The biomaterials used in scaffolds for skin substitutes or in bioinks for skin bioprinting are mostly exogenous and may compromise ECM functions such as growth factor binding and interfering with cell-to-cell signaling, cell proliferation, and innervation. 148,149 Modular tissue-engineered constructs using microtissues and cultured organoids have been developed to regrow the cellular and extracellular composition of native skin.
Whereas skin bioprinting embeds cells inside crosslinked bioinks like pouring cement, modular tissue engineering creates microtissue building blocks out of cells like bricks. In the traditional “top-down” approach, cells are seeded in scaffolds in bulk. The modular “bottom-up” approach fabricates microtissues to construct a larger 3D structure or modular tissues. Fibroblasts have been embedded in gelatin microspheres to create dermal building blocks. 150 These building blocks were packed into a maturation chamber to allow for cell–cell signaling and ECM interactions, which facilitated the degradation of the original gelatin scaffold and its replacement by fibroblast-secreted ECM (Fig. 5). The in vitro engineered ECM had similar mechanical properties to native ECM.
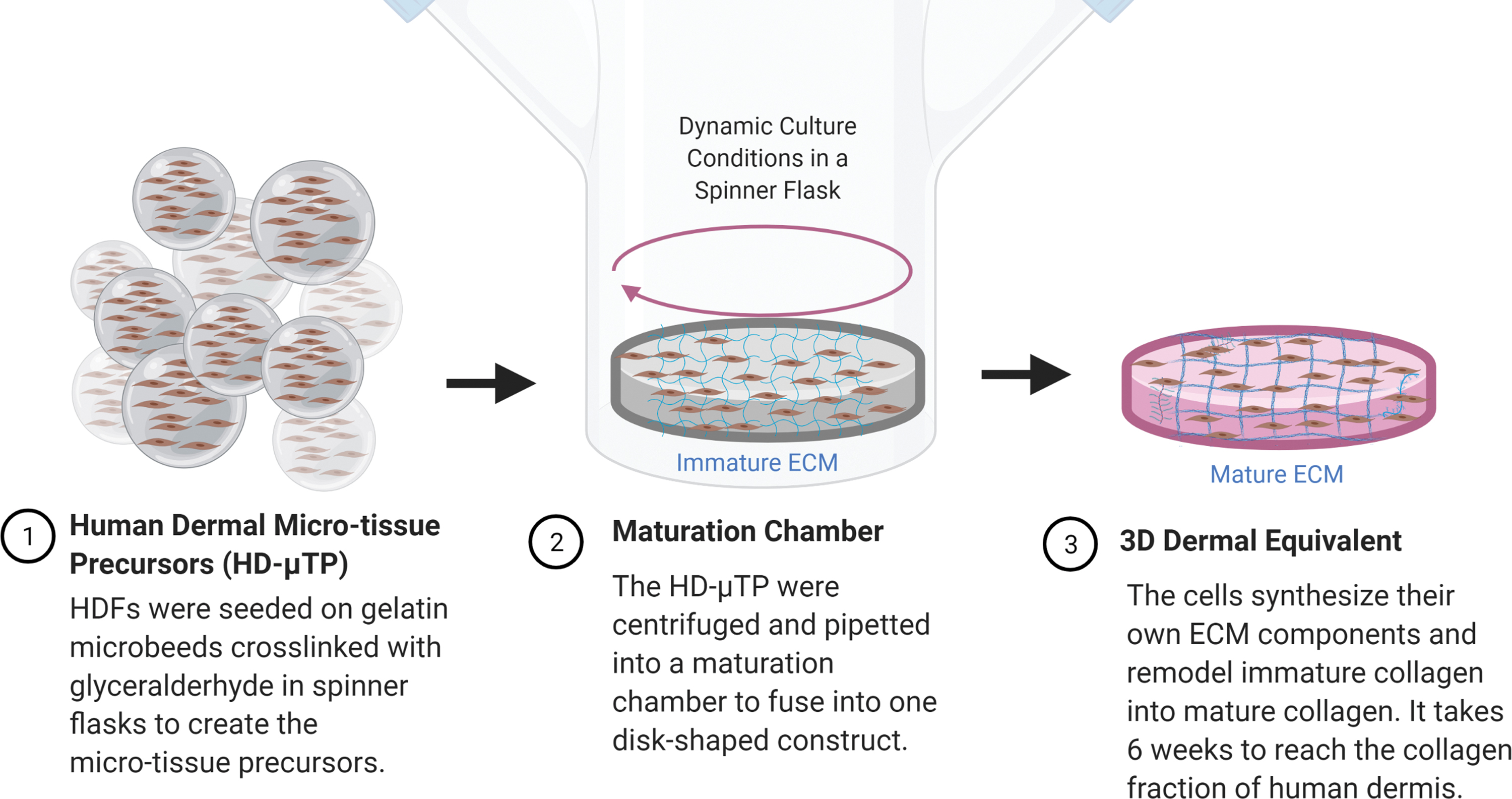
Schematic of the Dermal Microtissue Method. Fibroblasts are seeded in microcarriers of gelatin. These carriers are packed together and matured in a bioreactor over 5 weeks. Eventually, the gelatin is degraded and replaced by fibroblast-derived ECM, creating a completely autologous dermis. 150 Color images are available online.
This construct was also prevascularized by seeding human umbilical vein endothelial cells (HUVECs), which formed an interconnected capillary network after 3 weeks. 151 Seeding adult human keratinocytes also formed hair follicle-like structures. 152 However, the disadvantage of this method is that it takes months to achieve tissue maturation. One study overcame this weakness by generating natural ECM building blocks from decellularized adipose tissue, similar to the aforementioned acellular dermal matrices. 153
Building blocks have also been generated from skin organoids with the purpose of regenerating skin appendages (Fig. 3C). Although hair neogenesis is easily accomplished in rats, it has been a major challenge to overcome with human cells. 154 As seen in the microtissue construct, follicle-like structures often form, but eruption of hair seems to be developmentally constrained in humans and does not occur. 155 Lee et al. 155 recently reported hair generation from a successful organoid culture system for iPSCs. Stepwise modulation of TGF and FGF signaling pathways was used to induce cyst-like skin organoids with a stratified epidermis, fat-rich dermis, hair follicles, sebaceous glands, and sensory neural circuits. Xenograft of the human skin organoids onto nude mice formed planar hair-bearing skin. 155 These skin organoids may allow the generation of de novo hair for chronic wound patients and may potentially reverse the neuropathy of DFUs, as the organoids self-organized into functional skin after implantation. Same as with the microtissues, an intrinsic weakness of tissue maturation-based approaches is the long culture time. Organoid maturation required 4–5 months. 155
In situ skin self-assembly and organogenesis
A recently developed product managed to create organoid-like aggregates from harvested skin. Marketed as SkinTE® and pursuing FDA approval, the “autologous homologous skin constructs” are made from full-thickness skin biopsies (Fig. 6). 156 The dermal and epidermal layers of the biopsy are sectioned with an ultrafine blade and made into a suspension of minimally polarized multicellular aggregates. 157 It is then combined with the stromal vascular fraction derived from the hypodermis and adipose tissue layer of the biopsy. The hair follicles are kept intact as much as possible during sectioning, so these aggregates retain hair follicle stem cell niches as well as their polarity, which helps to maintain their identity and proliferative and differentiation capacities. In addition, since the cells are not cultured ex vivo, the loss of stemness caused by unnatural cell culture conditions is avoided. 158 This allows the processed skin construct to preserve the stem cell populations in the skin in their respective native niches. The expansion occurs in situ after implantation. 159
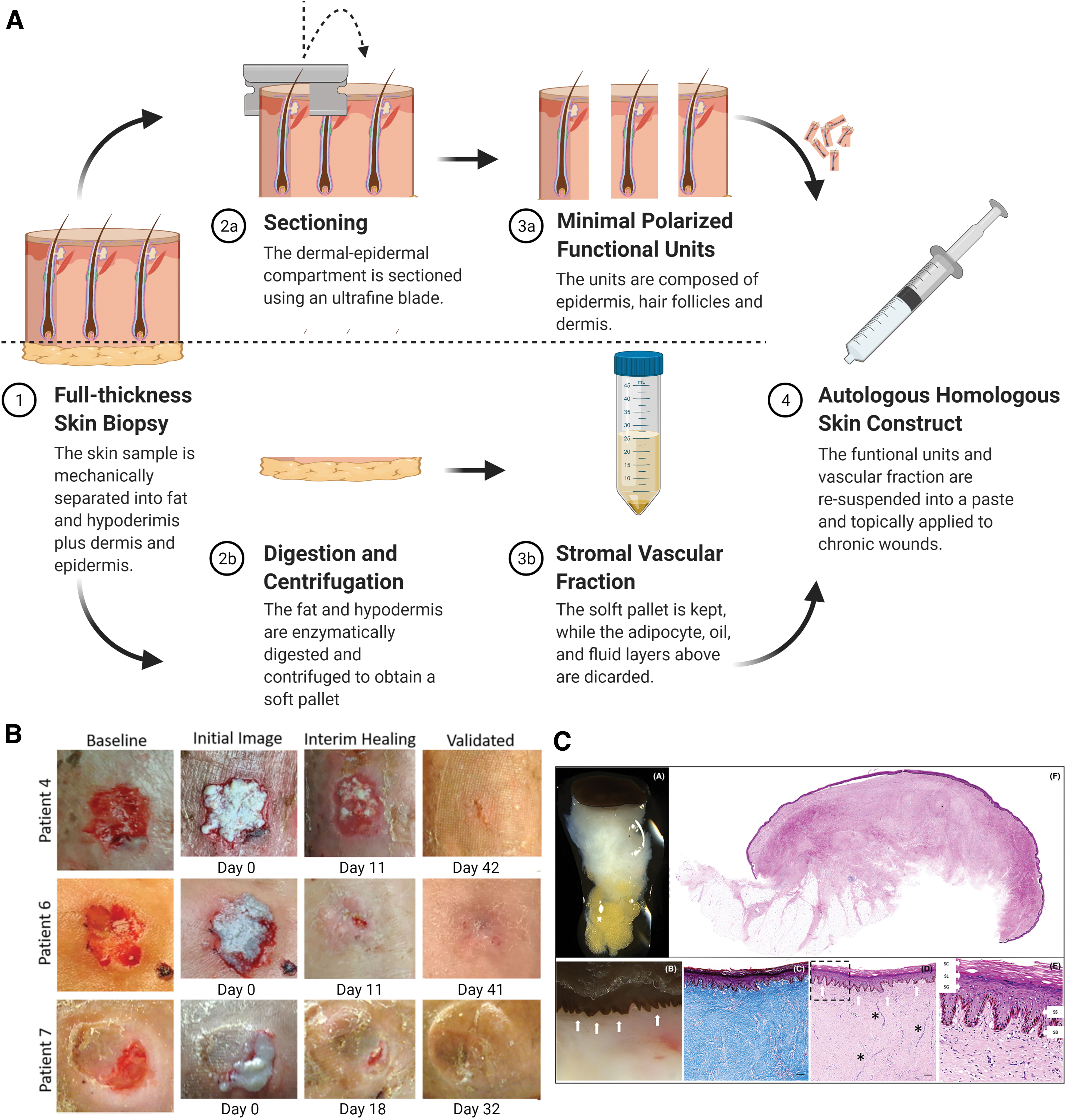
Autologous Homologous Skin Construct Manufacturing Process.
The dispersed stem cell populations self-organize into functional skin with skin appendages and innervation after topical application onto venous leg ulcers, resulting in superior two-point discrimination sensitivity (Fig. 6B, C). 159 One of the inventors of SkinTE, Lough et al. 160 first noticed that in coculture, epithelial stem cells aggregated at the surface, while the stromal vascular fraction-derived MSCs aggregated at the subepithelial position. The polarization interaction among cells triggers them to reorient into epidermis, dermis, and hypodermis, which is theorized to happen in vivo. 161 The minimal processing allows the paste to be ready within 2 days, so the procedure can be done in one hospital visit for inpatients, which lasts 8–11 days 162 on average, bypassing the long maturation time needed for organotypic approaches. 159
Prevascularization of skin tissue constructs
Further attempts to improve wound healing have led to the addition of vasculature in skin products. Commercial products without a circulatory system may result in partial necrosis of the graft and delayed integration time, which is further exacerbated by the ischemic conditions of DFUs. The inclusion of a preformed vascular network is therefore essential to ensure timely nutrient and oxygen delivery to cells distal to the wound bed. Vascular networks are formed in vitro by EC self-organization into capillaries with appropriate supporting cells. Recent strategies for prevascularizing skin constructs include 3D printing and topographical patterning. 144
Capillaries can form and self-assemble in 3D printed scaffolds. Dense microvasculature was generated in 3D gelatin methacryloyl (GelMA) by encapsulated human blood-derived endothelial colony-forming cells and MSCs. 163 The MSCs differentiated into pericytes at the abluminal position, supporting vascular network formation. More recently, Turner et al. 164 combined functionalized scaffolds with GelMA to generate a vascular construct that improved wound healing. GelMA has thermoreversible properties that allows it to stabilize after extrusion on a cool surface. They encapsulated MSCs in the sheath bioink and HUVECs in the core bioink during extrusion bioprinting. The MSCs in the sheath surrounded the HUVECs, in the position that pericytes take in natural blood vessels. The sheath bioink of GelMA was crosslinked with UV for mechanical integrity, while the chitosan–dextran bioink of the core was functionalized with a synthetic cell adhesion peptide and the RGD peptide or the MMP-2 proteolytic peptide. The printed construct was found that cord-like, natural microvascularization formed, and the construct improved healing in a wound scratch assay.
A similar self-assembly strategy has been successfully applied to prevascularize composite skin constructs (Fig. 7). In a recent study, Baltazar et al. 165 combined human dermal fibroblasts, human ECs, and human pericytes in a collagen type I bioink to create the dermal layer of a bilayered construct. The dermal layers were printed layer by layer. Three-dimensional endothelial networks spontaneously arose from the printed ECs and pericytes. Following the network assembling, the epidermal bioink was printed on top of the dermal layers. Upon implantation, the skin constructs self-organized with evenly distributed fibroblasts within the dermal layer. The morphology of the epidermal compartment and the ECM components were found to be similar to native human skin with the epidermal layer-forming basal cells adherent to a basal membrane. Moreover, the rete pegs formed and the human ECs were anastomosed to the mice vasculature. 165
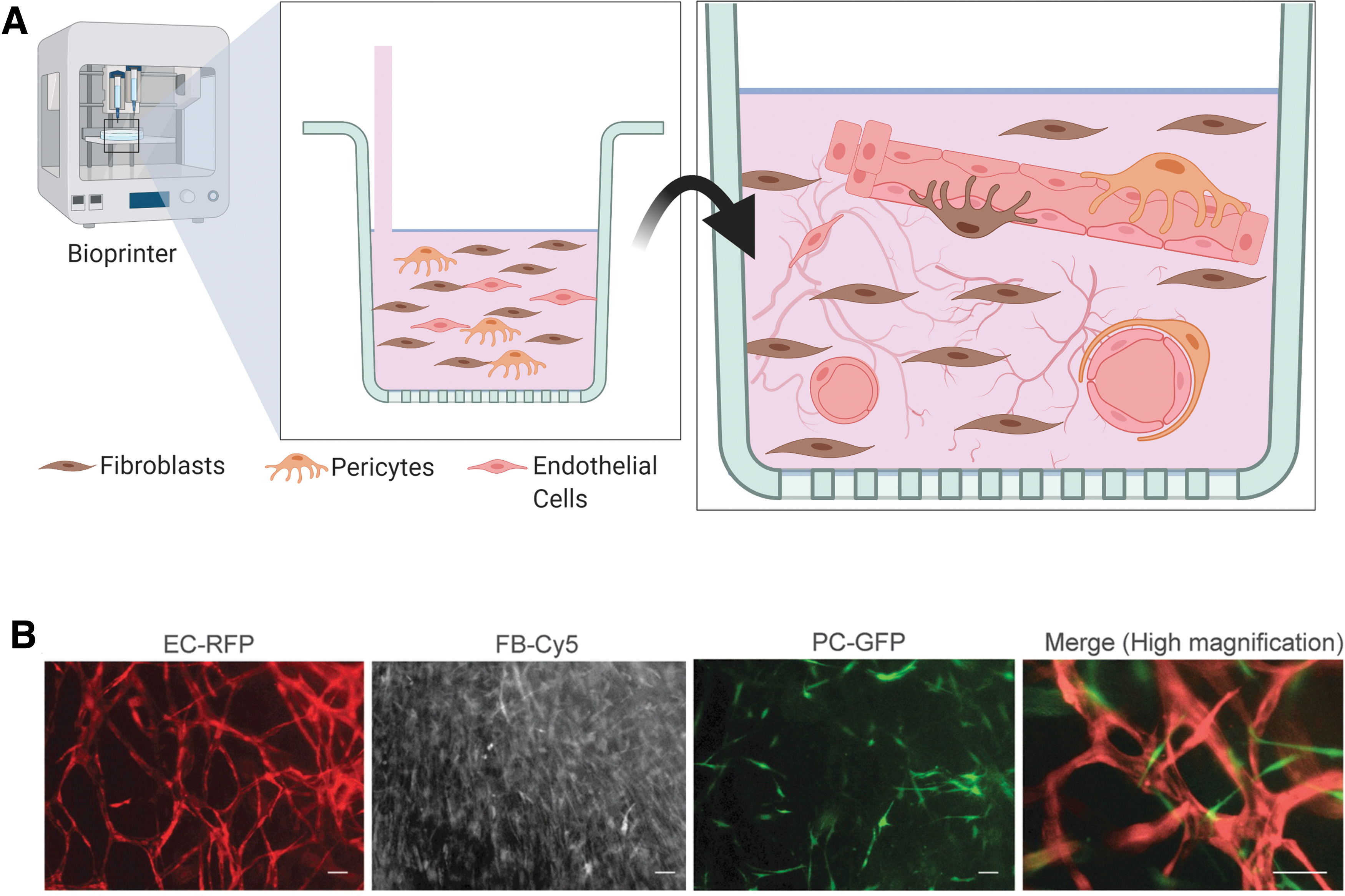
3D Printed Self-Assembled Microvasculature.
Our group have recently developed a 3D prevascularized tissue construct for diverse applications, including DFUs, using cell sheet engineering (Fig. 8). 166 Natural aligned nanofibrous ECM scaffold was obtained by decellularizing cultured human dermal fibroblast sheets. Then, human MSCs (hMSCs) were seeded on the ECM scaffold under hypoxia (2% O2) for 7 days. ECs were then cocultured on top of hMSCs under normoxia (20% O2) for 7 more days. The hMSCs acted as pericytes, supporting vasculature formation and a source of paracrine factors. The ECs formed aligned microvessels with enhanced structure, length, and density compared with randomly organized networks on nanofibrous ECM. This coculture method increased angiogenic factor secretion and decreased intercapillary distance (20 μm). 167 The aligned vasculature is also more structurally physiologic. The construct acted as a bridge between the vasculature of the skin graft and the host by rapidly connecting to both sides and improved the integration of skin grafts in a rat wound model. The fast perfusion of the graft prevented necrosis and fibrosis. 168
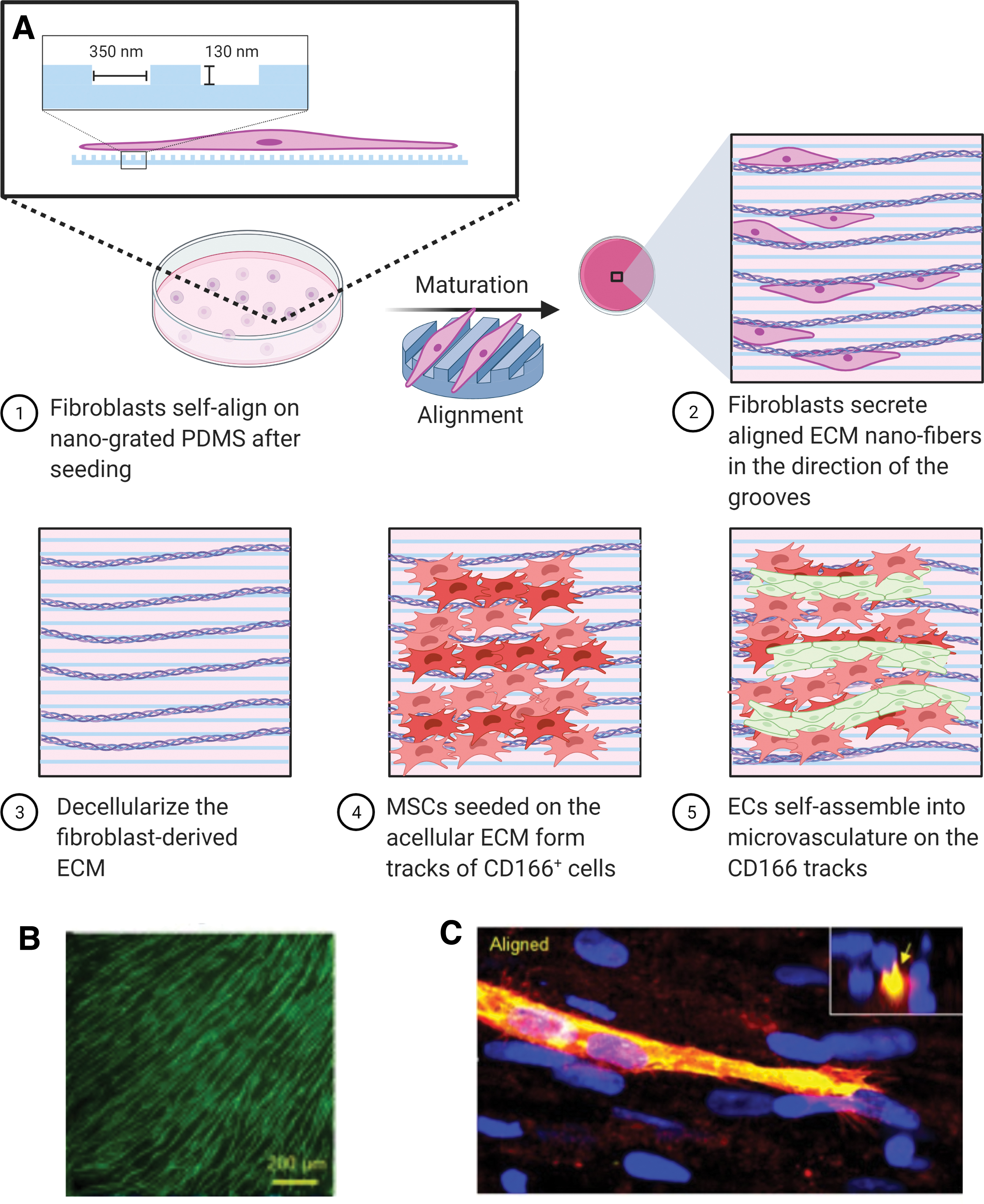
Schematic of creating Aligned Microvasculature.
These novel prevascularization techniques are still at the preclinical stage and associated with allogeneic cell usage. For clinical application, ECs need to be isolated from the patient's skin or adipose tissue to avoid allogeneic reactivity. Immune reaction to allogeneic ECs may lead to endothelial damage and activation of deleterious proapoptotic and proinflammatory pathways. 169 More sources of ECs are needed for the employment of prevascularized constructs. Qin et al. 170 recently reported a culture system for the generation of endothelial progenitor cells from CD34+ cells harvested from peripheral blood, which could serve as a source of ECs for prevascularization.
CONCLUDING REMARKS AND FUTURE PROSPECTS
DFUs and other chronic wounds are an emerging health care crisis, as diabetes, obesity, and population aging increase in developed nations. Tissue-engineered constructs for chronic wound treatment has come a long way. From relatively simple growth factor therapies, skin substitutes, and stem cell therapies, the field has advanced onto 3D printed skin, self-assembled skin, organoid skin, and construct prevascularization. Using tissue engineering technologies to reproduce more aspects of healthy native skin, including soluble factors, ECM, cell–cell interactions, and stem cell niches, has proven to improve healing outcomes (Fig. 9). The challenge that is being overcome with varying success is the restoration of skin function: visual appearance, UV protection, temperature control, hair, and mechanical properties. Fibrotic outcomes of closed DFUs have largely been ignored and should be addressed due to their effects on the mental well-being of the patient.
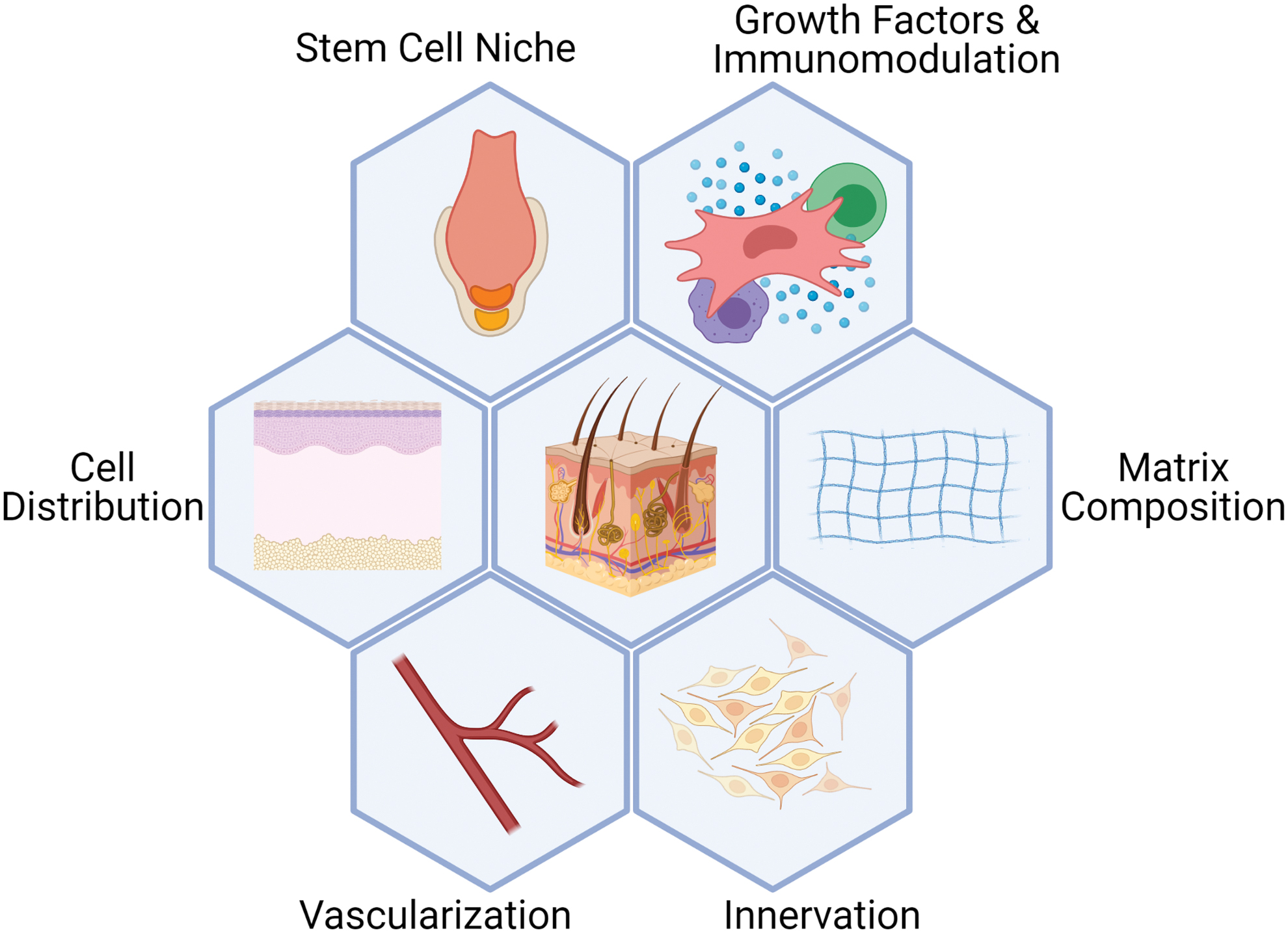
Summary of aspects of skin mimicked with tissue engineering to completely regenerate DFUs. DFU, diabetic foot ulcer. Color images are available online.
The field is impeded by the lack of standardization among clinical and preclinical trials. One study measured the touch sensitivity of the new skin, 159 and a few examined rete peg formation, 143,165 but the majority only measured the rate of wound closure. 58,65,87 Existing scar scales that analyzes attributes such as vascularity, pliability, pigmentation, and thickness, should be used to evaluate and compare DFU treatments. 171 New scales that takes into account other aspects of skin function, such as sensitivity and hair follicle density, should also be developed. As each study or product focuses on only a few of these targets, it is challenging to completely restore skin to a prewound state. Additionally, further investigation on DFU-specific healing is needed as new technologies, such as skin bioprinting, have not been tested on DFU animal models. Therapeutics shown to be efficacious for other types of wounds may not have the same effect on DFUs due to differences in the etiology.
With deeper insights into the molecular mechanisms of wound healing, cellular reprogramming therapies are emerging as the next promising avenue of DFU regeneration. Humans possess the genetic potential to regenerate scarlessly in the right conditions, as evidenced by fetal scarless regeneration, and the regeneration of micrometer-scale full-thickness skin wounds. 172 It has been demonstrated that overexpression of SOX2 using CRISPR/Cas9-regenerated human corneal ECs, which does not occur naturally. 173 Recently, C-Myc-mediated partial reprogramming has been discovered to downregulate profibrotic gene markers in fibroblasts, resulting in reduced scar formation. 174 Also, inhibition of MMP-9 secretion by delivering small interfering RNA in collagen-based scaffolds showed favorable in vitro results, 175 while preventing the expression of Engrailed-1 gene that turned on profibrotic programs in fibroblasts induced the regeneration of hair follicles, glands, and mechanical strength in mice. 147
While SkinTE does have one of the best clinical trial results for DFUs as other approaches are still at the preclinical stages, the autologous cells are still limited by the insidious effects of diabetes and aging, which may limit its therapeutic effects in some patients. 128 Many researchers are developing cellular reprogramming methods using small molecules and growth factors that could be used to rejuvenate diseased cells without viral transduction and the resulting tumorigenicity. 176 Directly manipulating cellular machinery will be necessary as the limit of external stimulation is reached.
SUMMARY
DFUs threaten the livelihoods of thousands and can lead to decreased mobility, infections, amputations, and death. Neuropathy, ischemia, chronic inflammation, and hyperglycemia from diabetes prevents successful wound healing. The present standard care of DFUs through underlying diabetes treatment and maintenance of a sterile moist wound site is often insufficient. Numerous tissue-engineered products have been developed to improve DFU closure rate through growth factor therapies, skin substitutes, and stem cells. Nevertheless, psychologically harmful scars are frequently resulted. Newer approaches emerged to replicate the complex external cues of the skin to promote better regeneration. Skin bioprinting aimed to reduce scar formation by tailoring the distribution of cells to each wound site. Dermal microtissues were made to generate a more natural ECM. Skin organoids grew implantable hair follicles, neurons, dermis, and epidermis.
The autologous homologous skin construct diced and spread a skin graft while preserving the various stem cell niches and appendages of the skin. Construct prevascularization accelerates the perfusion of grafted tissues. These advances resulted in more healthy, functional, sensitive, and esthetic new skin. However, each study invariably characterized wound closure with other disparate properties of the regenerated skin. A new comprehensive index needs to be standardized to measure healing outcomes for better comparison of therapeutics.
TAKE-HOME MESSAGES
Current tissue-engineered products are limited by incomplete wound closure, fibrosis, and the lack of skin appendages.
Novel tissue engineering approaches for DFU treatment include 3D bioprinting, dermal microtissue culture, skin organoids, engineered skin grafts, and engineered tissue vascularization.
Most of the present tissue-engineered constructs were only characterized for their wound closure. Comprehensive skin healing indices need to be standardized to better compare outcomes from various DFU interventions.
These new technologies need to be translated to DFU animal models, and then to clinical trials.
Footnotes
ACKNOWLEDGMENTS
All figures were created with BioRender.com
AUTHORS’ CONTRIBUTION
A.C. contributed to every section, except section 4 of the article. D.S. contributed to section 4. Dr. F.Z. was responsible for editing, proofreading, and corresponding. All authors have reviewed and approved of this article. This work is original and has not been submitted to or published elsewhere.
AUTHOR DISCLOSURE AND GHOSTWRITING
This article was expressly written by the authors listed. No ghostwriters were used. No competing financial interest exists.
ABOUT THE AUTHORS
FUNDING INFORMATION
This study was supported by the National Institutes of Health (R01HL146652) and the National Science Foundation (1703570, 2106048) to Feng Zhao, PhD.