
Abstract
Objective:
To evaluate the role of disease-modifying antirheumatic drugs (DMARDs) on wound healing outcomes of patients with autoimmune disease at our tertiary wound care center.
Approach:
Retrospective review of patients presenting to our wound care center between 2014 and 2018 with both chronic wounds and a history of inflammatory disease. Patient demographics, comorbid conditions, and progression to complete wound healing were compared between those taking DMARDs or not at the time of wound onset. The study adheres to the STROBE statement.
Results:
Fifty-eight patients with a total of 296 wounds were retrospectively reviewed. Patients were taking at least one DMARD at wound onset in 217 (73.3%) of these wounds. The average number of DMARDs at wound onset was 1.5 (standard deviation 1.2). Two hundred ten wounds progressed to heal (70.9%), with a median time to healing of 229.5 days (interquartile range 71.0–490.0). Of the 210 wounds that healed, patients taking at least one DMARD had a significantly shorter time to healing relative to patients who were not on any DMARDs (median 190.5 days vs. 340.0 days, p = 0.0156).
Innovation:
Characterizing wound healing outcomes at a tertiary hospital with a dedicated wound care center and analyzing the role of DMARDs in wound healing progression.
Conclusions:
The median time to healing in the studied cohort was 229.5 days, which is much longer than the healing time for noninfected diabetic foot ulcers at our institution. These findings highlight the wound healing challenges posed by underlying autoimmune disease.10

Introduction
It is notoriously difficult to treat chronic wounds in patients with underlying systemic inflammatory disease. Tissue normally progresses through four wound healing stages: hemostasis, inflammation, proliferation and repair, and remodeling. 1 Patients with chronic wounds fail to progress normally through this healing cascade, remaining instead in a chronic state of inflammation. 2,3 This persistent inflammation leads to unrestrained proteolytic activity, which overwhelms the tissue's protective mechanisms and is thought to be one of the pathognomonic features of chronic wounds. 2
Systemic inflammatory disease such as rheumatoid arthritis (RA), systemic lupus erythematous, and vasculitis can perpetuate this proteolytic imbalance with an additive effect on impaired wound healing. The addition of disease-modifying antirheumatic drugs (DMARDs) for the treatment of patients with inflammatory diseases further complicates the healing process. DMARDs are used to attenuate the body's inflammatory response and prevent permanent injury from chronic inflammation. 4 While helpful in combating inflammatory disease, disruption of inflammation can also inhibit the wound healing cascade.
The intricate relationship between pharmacologic treatments of autoimmune disease and potential wound healing complications led to the investigation of DMARDs' postoperative effects and ulcerative complications in patients with autoimmune diseases such as RA. 5,6 Specific DMARDs such as leflunomide and antitumor necrosis factor-alpha (TNF-α) biologic drugs have been associated with increased postoperative complications such as increased wound healing times and increased infection rates in patients with RA. 7,8 Other studies suggest that DMARDs such as methotrexate and anti-TNF-α biologic drugs do not have a significant impact on ulcer healing in patients with inflammatory disease. 9
Existing research points to conflicting conclusions regarding the effect of DMARDs on healing of chronic wounds in patients with underlying inflammatory disease. In this study, we aim to investigate the impact of DMARDs on healing of chronic wounds in patients with inflammatory disease.
Clinical Problem Addressed
Chronic nonhealing wounds are challenging to treat in patients with autoimmune disease. While the advent of DMARDs aids in suppressing the dysregulated immune system, the extent by which wound healing is impaired has not been characterized. Our study demonstrates the positive influence of DMARD therapy in the setting of nonhealing chronic wounds in patients with various autoimmune conditions and comorbidities. The provided evidence addresses an important question regarding the efficacy and safety of DMARD therapy to manage autoimmune disease for wound-care providers when managing nonhealing wounds in this vulnerable population.
Materials and Methods
Retrospective review
All consecutive patients presenting to our tertiary wound care center with a wound and a history of inflammatory disease between the years 2014 and 2018 were retrospectively reviewed. Patients were identified using current procedural terminology (CPT) codes pertaining to inflammatory disease and DMARD use (Table 1).
Current procedural terminology codes used to identify patients with inflammatory disease and disease-modifying antirheumatic drug use
Data collected included patient demographics, comorbid conditions, medication information, wound characteristics, treatment regimen (debridement, flaps, etc.), and complications. Electronic laboratory notebook was not used. The Charlson comorbidity index (CCI), a composite score ranging between 0 and 24 that offers estimates of 10-year survival based on underlying conditions, was calculated for each patient. 10 Outcomes of interest were progression to complete wound healing, time to healing, and progression to amputation.
Statistical analysis
Continuous variables were described by means and standard deviations (SDs) or median and quartiles where appropriate. The Student's t-test, Wilcoxon rank-sum test, or Kruskal–Wallis test was used to examine statistically significant differences between continuous variables as appropriate. Categorical variables were described by frequencies and percentages. Chi-square and Fisher's exact tests were used to examine statistically significant differences between categorical variables. Statistical analysis was performed using STATA v.16 (StataCorp, College Station, TX), with significance defined as p < 0.05.
Results
Patient demographics and comorbidities
Fifty-eight patients with a total of 296 wounds met the inclusion criteria for this study. The mean number of wounds per patient was 5.1 (SD 5.6). Average patient age at wound onset (n = 296) was 64.8 years (SD 15.7). A majority of patients were African American (n = 26, 44.8%), followed by white (n = 24, 41.4%). Average body mass index was 29.2 (SD 11.5) and average CCI was 3.7 (SD 2.3). Seven patients (12.1%) were current smokers and 14 (24.1%) had a history of tobacco use. Most patients were insured via Medicare (n = 35, 60.3%) or private insurance (n = 19, 32.8%). Patient demographics and comorbidities are outlined in Table 2.
Patient demographics and wound characteristics
BMI, body mass index; CCI, Charlson comorbidity index; SD, standard deviation.
Immunologic history
The most common autoimmune diseases in the studied cohort were RA (n = 16, 27.6%), pyoderma gangrenosum (n = 13, 22.4%), and vasculitis (n = 9, 15.5%). A majority of patients in the cohort (n = 217, 73.3%) were taking at least one DMARD at the time of wound onset. The overall mean number of DMARDs that patients were taking was 1.5 (SD 1.2). Inflammatory conditions and DMARD usage are outlined in Table 3.
Inflammatory condition and disease-modifying antirheumatic drug usage among patients in the studied cohort
DMARD, disease-modifying antirheumatic drug.
Wound characteristics and healing outcomes
Two hundred ten wounds (70.9%) eventually healed, with a median time to healing of 229.5 days (interquartile range [IQR] 71.0–490.0). Median wound size at presentation was 3.0 cm2 (IQR 0.6–17.7). Wounds that did not progress to healing were significantly larger than wounds that ultimately healed (median 4.5 cm2 vs. 2.4 cm2; p = 0.0214). The majority of wounds were located on the patient's leg (n = 144, 48.6%). Wounds on the ankle and leg were significantly less likely to heal relative to wounds on the toe, foot, or other locations (p < 0.001).
Of the 210 wounds that healed, patients who taking at least one DMARD at wound onset had a significantly shorter time to healing relative to patients who were not on any DMARD therapy (median 190.5 days vs. 340.0 days, p = 0.016). The overall median follow-up was 1006.5 days (IQR 412.5–1844.0). A total of four major lower extremity amputations were required in the studied cohort: three patients (5.2%) required unilateral below-knee amputation (BKA) and one patient (1.7%) required bilateral BKA. Six patients (10.3%) required lower level amputation (e.g., hallux, Lisfranc, metatarsal).
Discussion
The findings of this study demonstrate the complex nature of managing chronic wounds in patients with systemic inflammatory disease as well as the effect of DMARD therapy on wound healing outcomes. Nearly three-quarters of all wounds in the studied cohort ultimately healed (n = 210/296, 70.9%), with a median time to healing of 229.5 days (IQR 71–490). This differs from our institution reporting a 97% wound healing rate with a median time to heal of 30.8 days in patients with noninfected diabetic foot ulcers. 11 There were trends toward higher rates of healing in patients on at least one DMARD, but this finding narrowly missed statistical significance (73.7% vs. 26.3%, p = 0.08).
Of the 210 wounds that healed, patients who were taking at least one DMARD at wound onset healed significantly faster than patients who were not on any DMARD therapy at the time of wound onset (190.5 days vs. 340 days, p = 0.016). Furthermore, wounds that healed were associated with a higher number of DMARDs at wound onset compared with wounds that did not heal (1.6 ± 1.3 vs. 1.2 ± 1.1; p = 0.021). Almost half of all wounds were present on the leg (48.8%), further highlighting the multifactorial etiologies involved in the pathogenesis of nonhealing wounds, including autoimmune disease, vasculitis, and vascular pathologies, the latter of which is particularly likely to affect the lower extremities. 12 –14
Wounds on the lower extremity were also significantly less likely to heal when compared with wounds presenting on other locations of the body (p < 0.001). While many factors may play a role in compromised wound healing on the lower extremity, vascular insufficiency and vasculitis are commonly implicated in the pathogenesis. 14
Wound healing in patients with systemic inflammatory disease is compromised by unbalanced proteolytic activity that arises secondary to chronic inflammation. 2 The current study reported a lengthy overall median healing time of 7.5 months (229.5 days) in patients with at least one underlying inflammatory condition at our tertiary wound care center. This statistics is particularly alarming when compared with similarly comorbid patients, such as those with noninfected chronic diabetic foot ulcers, who take a median time to heal of 30.8 days at our institution. 11
Our findings corroborate those of a previous study at our institution, which found prolonged healing times in patients with underlying inflammatory disease relative to patients without inflammatory disease (14.6 months vs. 10.3 months, p = 0.07). 15
Wound healing difficulties have been well studied in a variety of specific autoimmune conditions. Lansdorp et al. analyzed outcomes following proctectomy in patients with perianal Crohn's disease and found that 29.4% of patients had persistent perianal wounds for 1 year after proctecomy. 16 Spencer-Vaele et al. reported the case of a 28-year-old female who developed a venous ulcer secondary to Wegner's granulomatosis and took 2 months for complete healing of the wound. 17
While the previous studies investigated chronic wounds in patients with underlying autoimmune disease, other studies have investigated wound healing in patients with underlying autoimmune disease who have undergone orthopedic procedures. Garner et al. compared wound healing outcomes following orthopedic procedures between patients with a history of RA and patients without a history of inflammatory joint disease and found a significantly higher rate of failed healing in the RA group (p < 0.02) although the time to healing was not significantly different between groups (p > 0.10). 6 Furthermore, disease duration has been associated with increased odds of delayed wound healing in patients with RA undergoing orthopedic procedures. 18
While existing evidence overwhelmingly indicates the negative effect of autoimmune disease on wound healing outcomes, there is more controversy surrounding the effect of DMARDs on wound healing. Healed wounds in the studied cohort had significantly shorter time to healing in patients who were on at least one DMARD (p = 0.016) and wounds that ultimately healed were associated with a higher number of DMARDs at wound onset relative to nonhealing wounds (p = 0.021). These findings suggest that DMARDs may improve wound healing outcomes in patients with chronic inflammatory disease.
While the inflammatory phase of wound healing is prolonged in patients with autoimmune disease, DMARDs may offset the damage secondary to widespread inflammation allowing for progression of wound healing. 2,4 These findings are consistent with reports suggesting that certain biologic DMARDs and TNF-α inhibitors may aid in the healing of chronic ulcers. 9,19 A study done at our own institution suggested that the use of TNF-α inhibitors may be preferred to steroids or cyclophosphamide in treating lower extremity ulcers in patients with RA. 9
Existing studies present conflicting evidence with respect to the effect of DMARDs and other anti-inflammatory medications on the risk of surgical site infection (SSI) and delayed wound healing. While some studies conclude that these medications are associated with a slightly increased risk of SSI and delayed wound healing, 6,19 other studies suggest that DMARDs do not increase SSI risk in patients with autoimmune disease who are undergoing elective orthopedic procedures. 7,18,20,21 Bibbo and Goldberg found no increased risk of SSI following elective foot and ankle surgery in RA patients on TNF-α inhibitors compared with without therapy. 20 Furthermore, Talwalkar et al. reported no SSIs in a retrospective study of patients with RA who were receiving TNF-α inhibitor therapy following elective orthopedic surgery. 21
In contrast, Ito et al. estimated a 6.5% SSI rate in RA patients on biologic DMARD therapy undergoing large joint surgery. 22 These findings were supported by Garner et al., who reported an increased risk of SSI in RA patients on corticosteroids in comparison with RA patients who did not receive perioperative corticosteroid treatment. 6 While there is debate regarding wound healing and DMARD use, there is consensus regarding certain agents such as leflunomide, which is thought to be more detrimental to wound healing. 5,8,12
In a cohort of patients with RA undergoing elective orthoprdic procedures, Fuerst et al. found that leflunomide therapy was associated with increased postoperative wound healing complications relative to other DMARDs. 8 These findings are further substantiated in case reports of delayed wound healing outcomes and skin ulcerations in patients taking leflunomide. 12,13 Although delayed wound healing is an uncommon complication reported with TNF-α inhibitor use, conflicting evidence suggests that other adverse effects such as vascular insufficiency secondary to vasculitis may contribute to delayed healing in patients on these medications. 14
Limitations
One of the major limitations of this study is its small sample size. While the findings of this study indicate that DMARD therapy may improve wound healing outcomes, subsequent investigation using a larger cohort may substantiate the trends noted in this cohort. Another limitation of this study is the potential for recall bias. Furthermore, time to healing was calculated based on wound onset date, which was often collected at a patient's first visit in the wound clinic. Instances in which wound onset date relied on a patients' memory of when they first noticed their wound may have introduced recall bias into our analysis.
Innovation
The effect of DMARD therapy on wound healing outcomes is unclear. These agents suppress the immune system and therefore also suppress the inflammatory phase of wound healing, which could theoretically prolong wound healing. In our study, however, DMARD therapy appeared to have a beneficial effect not only on time to healing but also on progression to wound healing (Fig. 1). These findings demonstrate the need for further investigation into the role of DMARDs in wound healing in a larger cohort.
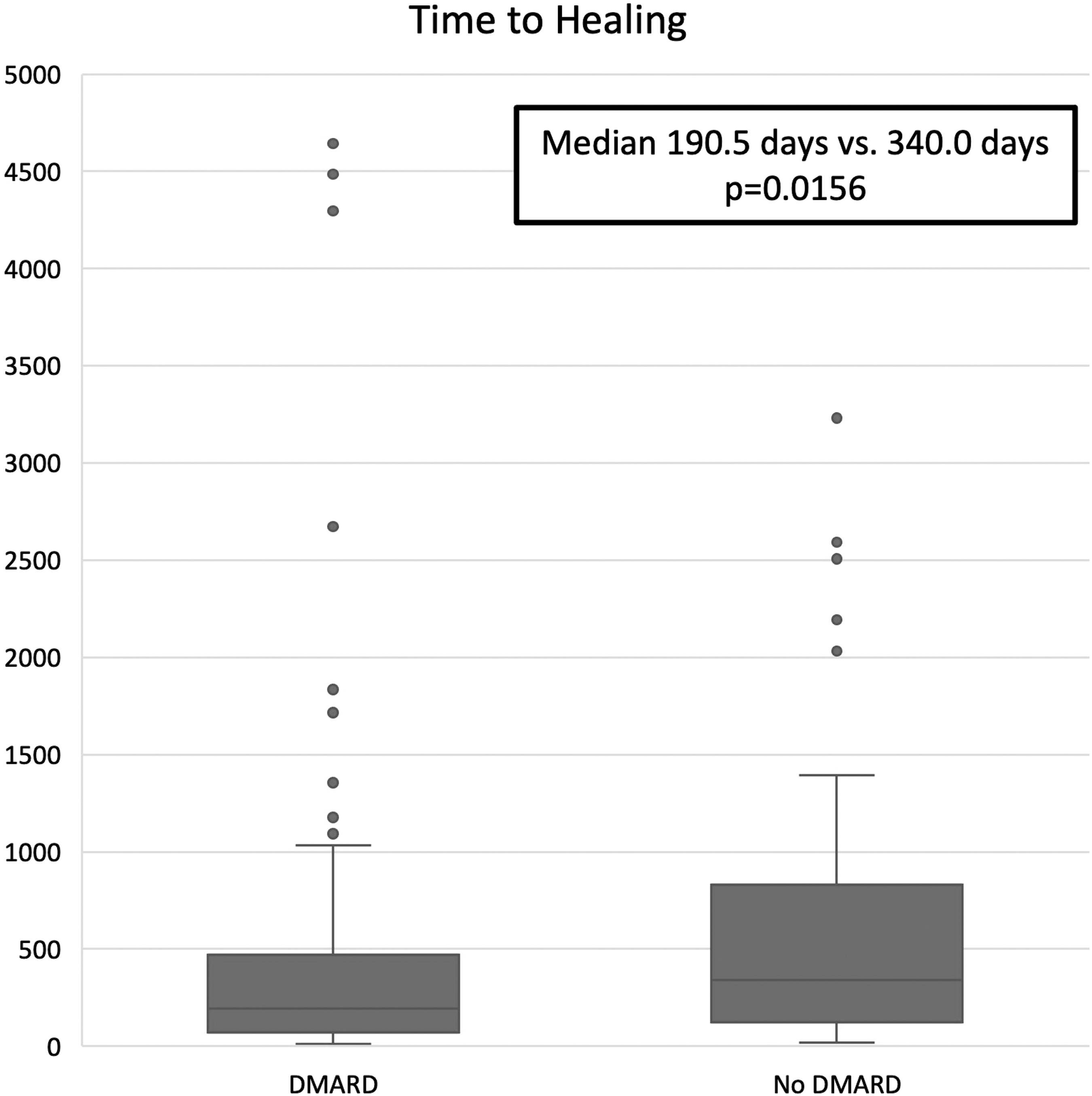
Median time to heal in patients who were either taking DMARDs at wound onset or not. Median time to heal in those taking DMARDs at wound onset was 190.5 days (IQR: 70.0–469.0). Median time to heal in those who were not taking DMARDs at wound onset was 340.0 days (IQR: 124.0–829.3). DMARD, disease-modifying antirheumatic drug; IQR, interquartile range.
Key Findings
In the studied cohort, 70.9% of all wounds healed and median time to healing was 229.5 days.
Patients who were taking at least one DMARD at wound onset healed significantly faster than patients who were not on any DMARD therapy at the time of wound onset (190.5 days vs. 340 days, p = 0.016).
Wounds that healed were associated with a higher number of DMARDs at wound onset compared with wounds that did not heal (1.6 ± 1.3 vs. 1.2 ± 1.1; p = 0.021).
Footnotes
Authors' Contributions
Kunal M. Kirloskar, MS, provided substantial contributions to the acquisition of data, ensuring accuracy between chart review and data collection, interpretation of results, article drafting and review, and final approval of the version to be published.
Paige K. Dekker, BA, provided substantial contributions to the acquisition of data, ensuring accuracy between chart review and data collection, interpretation of results, article drafting and review, and final approval of the version to be published.
Julianne Kiene, MS, provided substantial contributions to the acquisition of data, ensuring accuracy between chart review and data collection, article drafting, and final approval of the version to be published.
Suzanne Zhou, BS, contributed to the acquisition of data, ensuring accuracy between chart review and data collection, article drafting, and final approval of the version to be published.
Jenna C. Bekeny, MD, contributed to the study design, acquisition of data and analysis and interpretation of findings, article drafting and review, and final approval of the version to be published.
Ashley Rogers, MD, contributed to the study design, article review, and final approval of the version to be published.
Elizabeth G. Zolper, MD, contributed to the study design, acquisition of data, article review, and final approval of the version to be published.
Kenneth L. Fan, MD, contributed to the study design, article review, and final approval of the version to be published.
Karen K. Evans, MD, led the study design and provided substantial contributions to the interpretation of results, article review, and final approval of the version to be published.
Carol Deane Benedict, MD, contributed to the study design, article review, and final approval of the version to be published.
Helena B. Pasieka, MD, contributed to the study design, article review, and final approval of the version to be published.
Christopher E. Attinger, MD, provided substantial contributions to the study design, article review, and final approval of the version to be published.
Acknowledgments and Funding Sources
None declared. There are no financial disclosures, commercial associations, or any other conditions posing a conflict of interest to report for any of the above authors.
Author Disclosure and Ghostwriting
No competing financial interests exist. The authors reported no proprietary or commercial interest in any product mentioned or concept discussed in this article. The content of this article was expressly written by the authors listed. No ghostwriters were used to write this article.
About the Authors