
Abstract
Significance:
Orofacial structures are indispensable for speech and eating, and impairment disrupts whole-body health through malnutrition and poor quality of life. However, due to the unique and highly specialized cell populations, tissue architecture, and healing microenvironments, regeneration in this region is challenging and inadequately addressed to date.
Recent Advances:
With increasing understanding of the nuanced physiology and cellular responses of orofacial soft tissue, novel scaffolds, seeded cells, and bioactive molecules were developed in the past 5 years to specifically target orofacial soft tissue regeneration, particularly for tissues primarily found within the orofacial region such as oral mucosa, taste buds, salivary glands, and masseter muscles.
Critical Issues:
Due to the tightly packed and complex anatomy, orofacial soft tissue injury commonly implicates multiple tissue types, and thus functional unit reconstruction in the orofacial region is more important than single tissue regeneration.
Future Directions:
This article reviews the up-to-date knowledge in this highly translational topic, which provides insights into novel biologically inspired and engineered strategies for regenerating orofacial component tissues and functional units.


SCOPE AND SIGNIFICANCE
Orofacial structures are implicated in common pathologic and iatrogenic processes, and to date, regeneration has been challenging and inadequately addressed due to unique and highly specialized cell populations, architecture, and healing microenvironments. 1 –5 This review aims to explore biomaterial advancements in orofacial soft tissue regeneration within the last 5 years, focusing on the oral mucosa, taste buds, salivary glands (SGs), masseter muscles, as well as the functional units of the tongue and soft palate (Fig. 1). Of note, gingiva, which is also unique to the oral cavity, will not be covered in this study because of existing comprehensive reviews. 6

Clinically challenging and physiologically unique soft tissues within the orofacial region. Tissues of interest in this review are labeled and depicted in color, including the oral mucosa, taste buds, salivary glands, masseter muscles, tongue, and soft palate. Other craniofacial structures are depicted in grayscale. (Figure created with
TRANSLATIONAL RELEVANCE
Biomaterials used for bone, cartilage, nervous tissue, and epidermis have been extensively reviewed in nonfacial structures, such as the upper and lower limb, and are also applicable to orofacial tissue. 7 However, no recent reviews have elucidated the role of biomaterials in reconstructing certain tissues, such as oral mucosa, SGs, and taste buds that are only found within the oral cavity and contain highly specialized cells. 2 –5 In response, this article aims to provide an overview of this largely underaddressed area to accelerate bench-to-bed translation of current biomaterial advancements.
CLINICAL RELEVANCE
Orofacial structures are indispensable for speech, eating, and swallowing, with impairment disrupting whole-body health through malnutrition and poor quality of life. Moreover, damaged or absent tissues in the orofacial region can be secondary to congenital, malignant, iatrogenic, autoimmune, infectious, and traumatic etiologies. Therefore, the orofacial region is an exciting frontier for biomaterial applications due to its functional importance and clinical challenges. By identifying biomaterial candidates and determining avenues for further investigation, this review article aims to bridge the knowledge gap between recent benchtop discoveries and biomaterial usage in clinical practice.
BACKGROUND
In recent years, a spectrum of innovative biomaterial and tissue engineering strategies have been investigated for soft tissue regeneration, which commonly combine the usage of scaffolds, bioactive molecules, and cells. 2,8 –10 Scaffolds are three-dimensional constructs synthesized from organic matrix (e.g., collagen, fibrin) or synthetic polymers [e.g., polyglycolic acid (PGA], poly-lactic-co-glycolic acid (PLGA)] that provide mechanical support and recapitulate matrix architecture, and thus recreate a local microenvironment that promotes cell adhesion and proliferation, modulates cellular differentiation, and encourages long-term remodeling. 1,8,10 Meanwhile, bioactive molecules (including but not limited to growth factors, small-molecule drugs, ions, and endogenous, foreign, or synthetic proteins) could promote local cell proliferation and differentiation, and may also suppress pathologic inflammation and fibrosis. 2,10
Moreover, transplantable cell therapeutics, particularly those with multi- or pluripotent cell populations, are particularly promising on account of their versatility, ease of use, and applicability to multiple organ systems. However, concerns, including tumorigenicity, poor cellular survival and retention, and limited cell availability are obstacles that have to be overcome. 11,12 Consequently, significant research has been dedicated toward identifying noninvasive and readily available sources of tissue-specific stem cells, as well as developing in vitro techniques for bolstering therapeutic efficacy, including scaffold seeding, specialized culture, genetic engineering, and most recently organoid culture. 1,9,11,13 Of note, approaches frequently combine cells, scaffolds, and dissolved molecules to effectively control the regenerative environment and local cell behavior; however, this may complicate comparison of different treatments.
Orofacial structures such as the tongue, taste buds, SGs, and oral mucosa are unique clinical targets due to their highly specialized tissues and compact architecture. 2,14,15 Unfortunately, orofacial pathology affects a wide spectrum of patients, with current management inadequately addressing functional disability and risk of severe outcomes. 2,9 For example, cleft lip and palate is the third most common congenital deformity, affecting 1/2000 of live births and presenting as a wide spectrum of malformations in the soft palate, hard palate (Fig. 2), lip, and alveolus. 16 Disappointedly, surgical correction of cleft lip and palate leaves up to 30% of young patients with persistent speech deficits secondary to pathologic fibrosis and incomplete muscle regeneration. 17,18
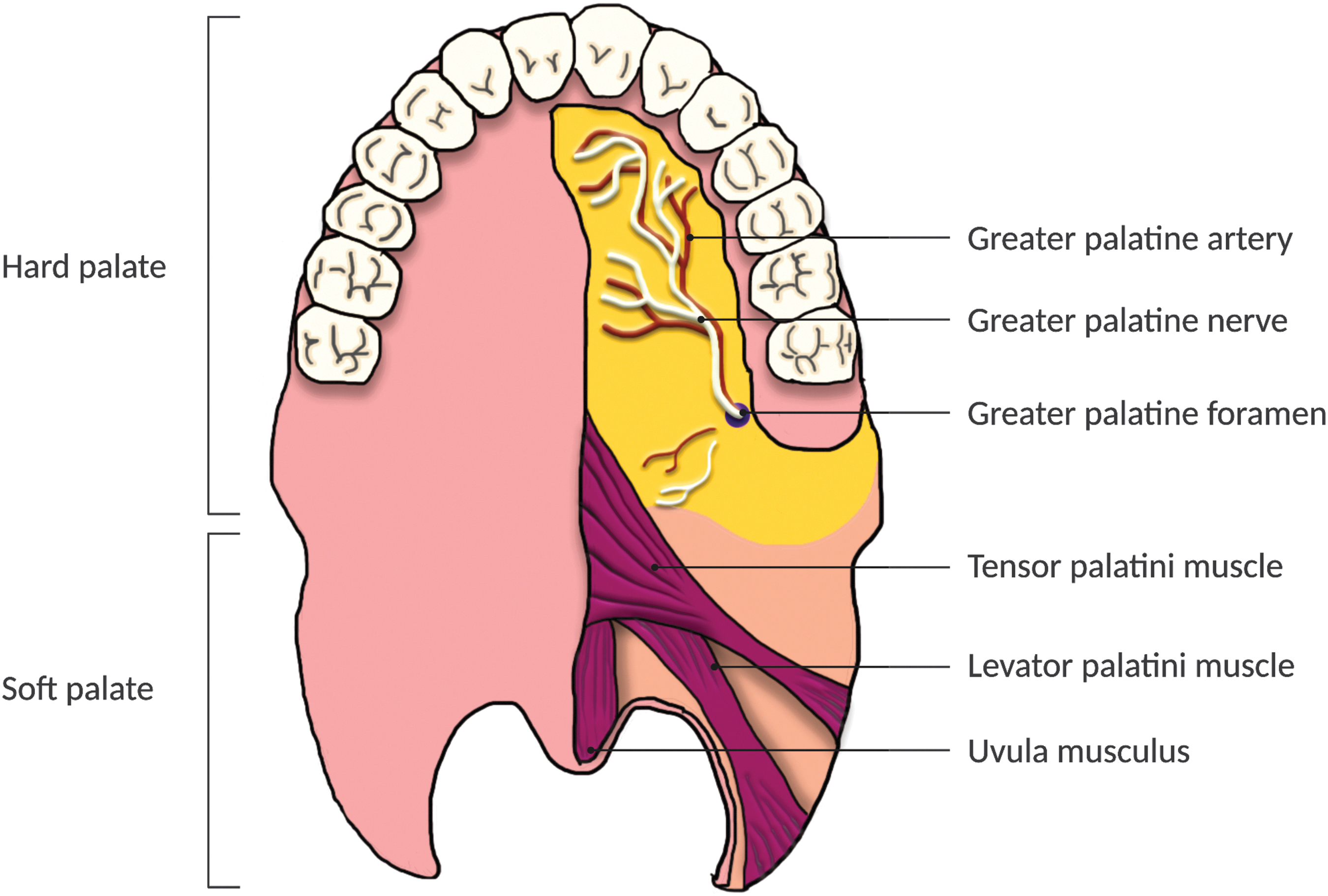
Palate anatomy. The palate consists of the anterior hard palate (containing palatine and maxilla bone), and the posterior soft palate (comprised entirely soft tissue). Neurovasculature enters the oral cavity superiorly through foramina and inferiorly from the pharynx. The soft palate uniquely contains a number of muscles (including the tensor/levator palatini and uvula musculus) as well as a connective tissue attachment for muscles named the palatine aponeurosis (not depicted), which are covered within the oral cavity by mucosa. Minor salivary glands are also found within the mucosa. Cleft palate defects commonly involve the soft palate, with more severe cases progressing anteriorly to impact the hard palate and/or lip. (Figure created with
Another example is surgical resection of head and neck squamous cell carcinoma, the 6th most common cancer worldwide affecting mucosa of the tongue, palate, floor of the mouth, buccal mucosa, oropharynx, and larynx, 19 which leaves large lingual and oral mucosal defects that can be further complicated by difficult closure and radiation/chemotherapy-induced fibrosis and injury of mucosa, taste buds, SGs, and nerves. 1,9,19 Last but not least, Sjogren's disease causes chronic autoimmune destruction of SGs and carries increased risk for dental caries, intraoral infections, and mucosal lymphoma. 20 Early intervention slows but does not reverse disease progression, leaving many patients with dry mouth requiring daily medication or artificial saliva. 21
Moreover, orofacial anatomy is complex and compact, with injuries damaging numerous interrelated tissues that must all be reconstituted for functional recovery. 2,15 For instance, the tongue requires intact musculature, mucosa, taste buds, vasculature/lymphatics, and sensorimotor/autonomic innervation to perform its physiologic roles in swallowing and taste sensation (Fig. 3). 1,9,22 The oral cavity is also a nonsterile, warm, humid environment that supports dense microbial growth, and the balance of commensal and potentially pathogenic microbes significantly affects treatment outcomes. 15,23 Moreover, oral mucosa is repeatedly exposed to foreign molecules/pathogens and mechanical insults through eating, and both oral and facial tissues experience continuous tension and motion. 15,24
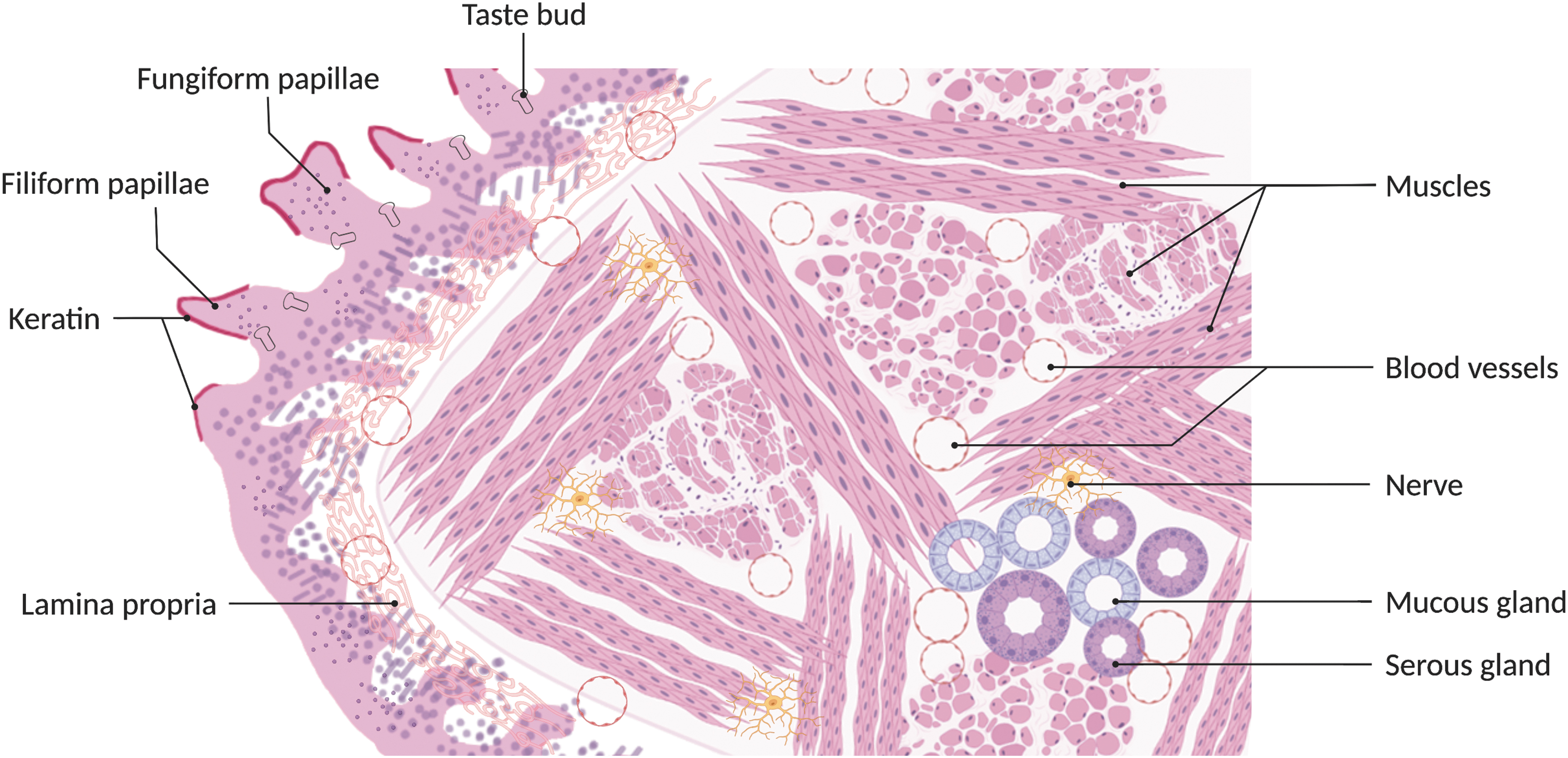
Tongue architecture. The superficial tongue is covered by oral mucosa, with a keratinized epithelium containing projections called papillae (subdivided into filiform, fungiform, and circumvallate papillae [not depicted]), interpapillary pits housing unipotent epithelial stem cells, and taste buds containing specialized taste receptor cells. Deep to this are numerous muscles that enable complex movement, supplied by rich vasculature and motor innervation from multiple cranial nerves. Afferent nerve fibers convey information regarding taste (from taste buds) and general sensation, and also coalesce into numerous cranial nerves. (Figure created with
Tissue for wound closure is also scarce due to compact anatomy, and orofacial scars frequently experience high tension with subsequent craniofacial deformation, particularly in young patients. 25 Lastly, facial structures hold paramount esthetic significance and thus impose strict standards on regenerative approaches, small changes in tissue color, texture, or function may be unacceptable for the patient. 9,26 Thus, regeneration of the orofacial region presents unique considerations.
It is also worth noting that orofacial tissues also possess prohealing mechanisms. Healthy saliva supplies growth factors and moisture to encourage wound regeneration within the oral cavity. 15 Generally, orofacial tissues receive robust blood supply, with lower levels of hypoxia observed in recovering wounds compared with nonfacial skin. 27 More importantly, oral mucosa demonstrates markedly superior regenerative capacity than skin, for which a number of mechanisms have been proposed. 28,29
In summary, factors such as nonsterility, exposure to foreign substances, abrasion and stress, constant movement, and potential for complicated and disabling injury inform the need for orofacial biomaterial therapies. Simultaneously, decoding the native healing mechanisms unique to orofacial tissues may also inspire development of novel biomaterials for functional recovery. Since investigation is still in infancy, most strategies are limited to preclinical animal testing, which is primarily done in rodent and rabbit models that provide affordable and relatively rapid (few days to weeks) results. 30 To the best of our knowledge, only a few acellular grafts and human amniotic membrane (hAM) have been tested in humans, primarily for oral mucosal regeneration, although this may change as the field evolves. 31 –33
DISCUSSION
Oral mucosa
Tissue characteristics
The oral mucosa consists of three tissue layers from superficial to deep: [1] stratified squamous epithelium, [2] lamina propria, and [3] submucosa (Fig. 4). 3 The surface epithelium serves as a barrier protecting deeper tissues from infection, trauma, and dehydration. Depending on location and mechanical stress, the surface epithelium can be nonkeratinized (such as in the floor of the mouth and in the check lining) or keratinized (such as in the anterodorsal surface of the tongue and hard palate). 28,34

Oral mucosa architecture. From superficial to deep: stratified squamous epithelium [keratinized depending on location and consisting of stratum corneum, granulosum, spinosum, and basale], basement membrane, lamina propria [containing ECM, vessels, nerves, fibroblasts, and immune cells], and submucosa [containing ECM, vessels, and nerves, as well as adipose tissue depending on location]. (Figure created with
Epithelium is further divided into four cell layers from superficial to deep: the stratum corneum, granulosum, spinosum, and basale (Fig. 4). 3 Notably, the stratum basale replenishes all epithelial cells lost to the environment and consists of a single layer of mitotically active cells in the deepmost epithelium. 3 These cells are attached through hemidesmosomes to an underlying basement membrane, which provides a connective tissue interface to the lamina propria. 3
The lamina propria facilitates nutrient exchange and mechanical anchoring of the mucosa, and consists of elastin and collagen type I and III matrix, vasculature, nerves, fibroblasts, and immune cells. Lastly, deep to the lamina propria is the submucosa, which similarly contains collagenous/elastic matrix, nerves, and vasculature, as well as SGs, muscle, and adipose tissue in certain anatomic regions. 3
Oral mucosa heals more rapidly and displays less inflammation and scar formation than other stratified squamous epithelia, which can be attributed to a variety of reasons. 15,28,29,35 –38 First, oral mucosal keratinocytes migrate into wounds and proliferate more rapidly than epidermal keratinocytes, 37,39 which is partially attributable to local growth factors supplied by saliva 37,40 and baseline expression of transcriptional networks that are typically only activated after injury. 35 Second, oral wounds display attenuated increases in vascularity yet decreased hypoxia and hypoxia-inducible factor 1-alpha expression compared with the skin, which may ultimately discourage scar formation. 27,36,40
Third, injured keratinocytes in mucosal wounds experience a faster-onset, faster-offset, and overall attenuated inflammatory response that helps prevent pathologic fibrosis. 15,36 –38,40 Fourth, oral keratinocytes express different tight and gap junction profiles at baseline and during wound healing. 28,39 Lastly, injured keratinocytes in mucosal wounds appear to undergo apoptosis through the intrinsic pathway, versus extrinsic in the skin. 29 Future investigation on oral mucosa wound healing may draw upon these mechanisms.
Clinical challenges
Although oral mucosa heals better than the skin, clinical challenges in its regeneration are still undeniable. Chronic mucositis secondary to radiation and chemotherapy is debilitating and increases the risk of severe infection, 41 while current management displays limited efficacy and entails symptomatic pain control, oral hygiene, and nutrition. 42 Larger wounds secondary to excision, invasive dental procedures, or significant trauma are painful and usually require adequate coverage due to the nonsterile oral environment. 15,19 Even small mucosal defects from routine dental work, minor injury, or ulcers are associated with marked discomfort. 43
Overall, the ideal goals of oral mucosa injury treatment vary depending on chronicity and seriousness of injury; acute mild lesions expect rapid and painless recovery, larger defects require complete closure to prevent infection and facilitate reepithelization, and chronic mucositis entails a conservative plan for acceptable barrier regeneration and prevention of future injury. 41 –43 Auto- or allografts facilitate reconstruction when primary closure is contraindicated 2,44,45 ; however, the current options do not fully satisfy clinical demands. Split-thickness grafts are the first-choice autograft, with application hindered by limited size and availability due to oral cavity geometry. 46
Meanwhile, skin transplants integrate poorly in oral mucosa and potentially result in esthetic consequences and limited healing in medically compromised patients due to differing properties from oral mucosa. 2,44,46 It is also worth noting that the mechanical requirements of grafts may vary depending on differences in epithelial keratinization and local tissue stress. 46 Therefore, there is an impetus to develop novel regenerative strategies for oral mucosa.
Acellular grafting materials
Acellular grafts, including decellularized extracellular matrices (ECM) and man-made constructs, possess the marked advantages of convenient storage, procurement, and application and have been tested clinically as exciting “off-the-shelf” options for wound coverage (Fig. 5)

Scaffold preparation for orofacial soft tissue regeneration. Arrows depict typical preparation steps. Scaffold are assembled out of synthetic/engineered materials or mammalian ECM (derived from xenogeneic, allogeneic, or autogenic tissues). For ECM, decellularization preserves native architecture to some degree, while further processing enables additional delivery modalities, including glues, gels, sheet-like grafts, and sponges. Autologous cells may be seeded on engineered or native tissue-derived scaffolds. On the other hand, allogeneic cells are a unique and viable option for minimally immunogenic progenitor cell populations–for example, those in human amniotic membrane. (Figure created with
Decellularized tissues contain native bioactive molecules that can direct local cell phenotype and differentiation as well as facilitate recruitment; sterilization methods can also preserve the architecture and mechanical properties to some degree. 2,10,47 For example, an acellular xenograft composed of decellularized porcine small intestinal submucosal (SIS) matrix reduced wound area and collagen I expression compared with nontreatment in a rat lingual defect model. 48 Meanwhile, Camacho-Alonso et al. reported that rat lingual wounds treated with a hydrogel of decellularized porcine urinary bladder matrix exhibited faster and more complete reepithelization, less myeloperoxidase activity, and earlier resolution of inflammation and revascularization. 49 Moreover, the absence of reported infection or requirement for graft reapplication further supported the clinical use of these acellular grafts for oral mucosal defect closure. 33
As an example of synthetic polymer-based constructs, PGA sheets secured to wounds with fibrin glue provide easier and more rapid coverage than traditional grafts while demonstrating low immunogenicity and good hemostasis, barrier function, adhesion, and resorbability in multiple anatomic sites. 50 However, in a rabbit lingual defect model, PGA sheets delayed wound reepithelization compared with primary closure. 51 In addition, in patients receiving PGA and fibrin closure after oral mucosa excision, PGA sheets detached after 3–6 weeks and wounds healed with mild scarring. 50,52 Thus, the usage of PGA constructs for oral mucosa closure warrants further investigation.
Cell-based grafting materials
Cell-based therapies show promise in rodent models for managing deeper and less well-defined defects. Systemic intravenous administration of allogeneic bone marrow-derived mesenchymal stem cells (BMSCs) and endothelial progenitor cells significantly reduced radiation-induced mucositis area and lingual ulcer size, promoted subepithelial angiogenesis, prevented basal cell apoptosis, and protected lingual epithelium against breakdown. 42 Moreover, systemic application of xenogeneic human gingival-derived mesenchymal stem cells (GMSCs), a less invasively obtained cell source easily isolated from discarded tissues in dental procedures, improved lingual papillae (i.e., mucosal projections) regeneration in 5-fluorouracil-induced mucositis (Fig. 6). 53
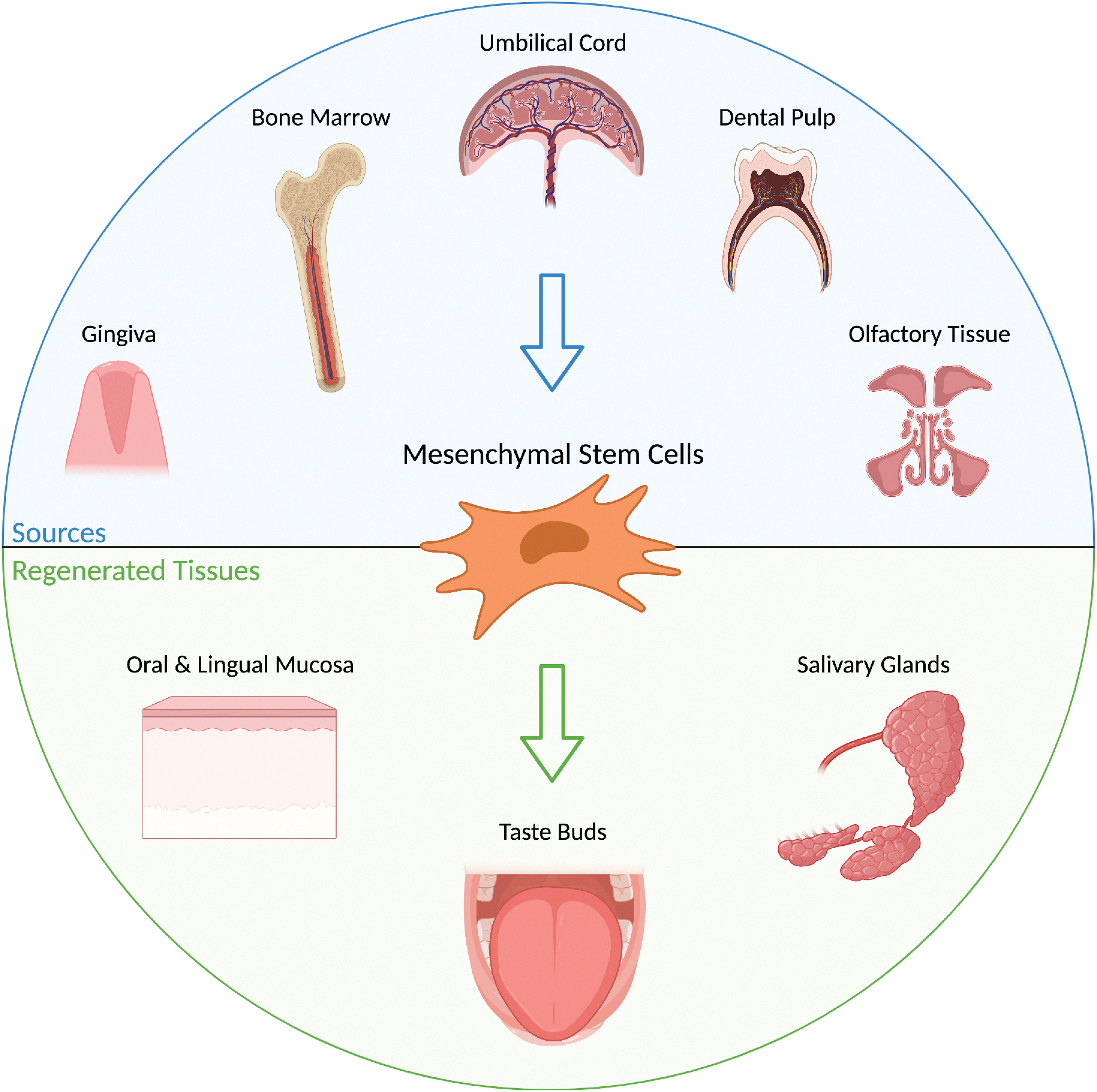
Sources and applications of mesenchymal stem cells for orofacial soft tissue regeneration. Mesenchymal stem cells are successful derived from murine bone marrow and olfactory epithelium, as well as human umbilical cord, dental pulp leftover from dental procedures, and gingiva. These cells encourage regeneration of radiation and chemotherapy-injured oral and lingual mucosa, salivary glands, and taste receptor cells and associated neurons. (Figure created with
Although MSCs, in theory, can replace lost tissue through implantation and differentiation into parenchymal cells, their long-term survival and retention are often poor and complicated by inflammation or the absence of endogenous stem cell populations. 13,54,55 Meanwhile, more and more research suggests that MSCs secrete numerous bioactive paracrine molecules, which modulate local host cell migration, proliferation, differentiation, and inflammatory response. 11,13,30,54 –58 Likewise, limited integration of transplanted MSCs or MSC-derived organoids with native tissue, 56 as well as concerns for MSC or host tumorigenesis, 11,12 present additional longitudinal challenges.
Another important consideration is that MSCs derived from different embryonic origins or tissues can exhibit varying therapeutic properties. For instance, craniofacial BMSCs proliferate more rapidly than those from long bones. 57 Similarly, craniofacial tissues contain unique stem cell populations that facilitate in vivo regeneration of specialized structures such as oral mucosa, taste receptor cells (TRCs), and masseter muscle. 17,57,59,60
Novel research into these craniofacial-derived MSCs may yield exciting findings for orofacial regeneration but also present unique challenges in terms of donor tissue availability and donor-site morbidity, as well as the amount, type, and bioactivities of the isolated cells. 61 –63 It is worth noting that exosomes, extracellular vesicles, and conditioned medium partially recapitulate MSC paracrine signaling and circumvent the difficulties of live cell transplantation. 54,64 –69 Therefore, the impact of MSCs on healing outcomes requires further investigation.
Implantable scaffolds are the most common vehicles for cell delivery (Fig. 5). Successful examples include autologous fibrin sheets that are seeded with human fibroblasts and mucosal keratinocytes to accelerate reepithelization and inhibit pathologic fibrosis of rat lingual mucosal wounds 70 and porcine SIS extracellular matrix that is seeded with human GMSCs to suppress rat mucosal wound collagen I expression, contracture, and scarring. 48 These grafts confer a physical barrier and contain tissue-derived ECM and growth factors, which encourage healing. 48 Undoubtedly, orofacial soft tissue regeneration frequently requires specialized biomaterials due to varying success with strategies studied in other organ systems. For example, skin grafts applied to mucosal defects demonstrate poor integration, functional recovery, and even taste bud loss in adjacent mucosa. 2,44,46,66
On the other hand, decellularized colonic or bladder mucosal matrix appears to accelerate oral mucosal healing and suggests that niche matching for developmental or tissue origin may improve outcomes. 48,49 More dramatically, some structures such as TRCs even require unique signaling molecules to undergo proper differentiation and maintenance. 59 Recreating a regenerative environment for complex craniofacial tissues thus necessitates a comprehensive understanding of orofacial wound pathophysiology and cellular niche.
Of note, hAM is one of the most studied cell-based grafts and consists of simple epithelium, basement membrane, stroma, and varying numbers of viable mesenchymal stromal cells and growth factors. 33 Clinical usage of hAM for coverage of mucosal defects secondary to excision, mandibular vestibuloplasty, and oronasal fistulae consistently accelerates wound reepithelization and hemostasis and reduces perceived pain. 31 –33 Human amniotic membrane can be cryopreserved to maintain some number of viable native cells. 33,71
Alternatively, by utilizing advantageous techniques of irradiation, hyperdrying, and glycerol preservation, hAM can be sterilized for extended preservation. 33,71 Excitingly, preserved hAMs, including hyperdried membranes, demonstrate similar efficacy in human mucosal wounds of the cheek and tongue. 71 As hAM undergoes increasing clinical usage and commercialization, optimization of processing and application methods will minimize high production costs and maximize patient impact. 31 –33
However, concerns of cell-based graft materials include immunocompatibility and off-target differentiation of transplanted stem cells, including striking neovascularization and tumorigenesis. 11,42 Nevertheless, autologous or allogeneic cell therapies may provide much-needed treatment options for chemotherapy and radiation-induced mucositis.
Regenerative molecules
Bioactive molecules include growth factors, synthetic peptides, and pharmacologic compounds. For example, preinjection of transforming growth factor (TGF)-β3 15 min before mechanical mucosal injury accelerated reepithelization, suppressed scarring, and promoted submucosal expression of hyaluronic acid and elastin at 6 weeks postinjury. 72 TGF-β1 also promotes lingual wound contraction and subsequent α-smooth muscle actin expression in fibroblasts, and can be suppressed by matrix metalloproteinase 8. 73 However, off-target effects can complicate growth factor treatment. 74 Another molecule, SV peptide, is a seven-amino acid sequence within the endogenous osteopontin protein that is rapidly metabolized and specifically encourages oral mucosal wound closure by upregulating keratinocyte and fibroblast motility and promoting skeletal muscle myofiber reconstitution, which may benefit deep orofacial defects implicating underlying musculature. 74 Extensive details can be found in previous review articles. 15,30
Others
Besides endogenous molecules, traditional medicinal plant extracts and laser therapy are popular but demonstrate unclear treatment efficacy. Extracts of Matricaria recutita and Centella asiatica, copaiba oleoresin, and the plant-derived compound bixin all accelerated reepithelization of rat oral mucosal wounds. 49,75,76 Copaiba oleoresin and bixin also reduced acute inflammation, and bixin promoted fibroblast proliferation, 75,77 whereas repeated studies of aloe vera extract in murine mucosal wounds were inconclusive. 78,79
Meanwhile, photobiomodulation therapy is a novel approach that directs high-power lasers at the borders of mucosal ulcers with the intent of stimulating cellular metabolism and inhibiting inflammation, 43,80 –83 although it cannot be properly classified as a biomaterial and poses uncertain clinical benefits and thermal injury risk. 83 Future studies may elucidate specific pathways for both plant-derived and laser therapies and help confirm early findings.
Taste buds
Tissue characteristics & clinical challenges
Taste buds are highly specialized chemoreceptor structures that detect and differentiate pleasant versus aversive chemical stimuli within food. 4 Taste buds are primarily concentrated on the surface of the tongue and soft palate, while recent studies report ectopic taste receptors located in the larynx, SGs, gastrointestinal tract, and adipose tissue where they are proposed to modulate pathophysiologic processes. 14,84,85 Each taste bud is a round cluster of 50–100 columnar epithelial TRCs that sense external stimuli through surface receptors and transduce signals to afferent nerves (Fig. 7). 4,14,84,86 Mature TRCs are subdivided into three types based on morphology and function: type I glial cells, type II sweet/bitter/umami detectors, and type III sour detectors. 4,22 Taste buds maintain a specific ratio of mature TRC types, which live on average for 8–12 days before replacement by newly differentiated cells. 4
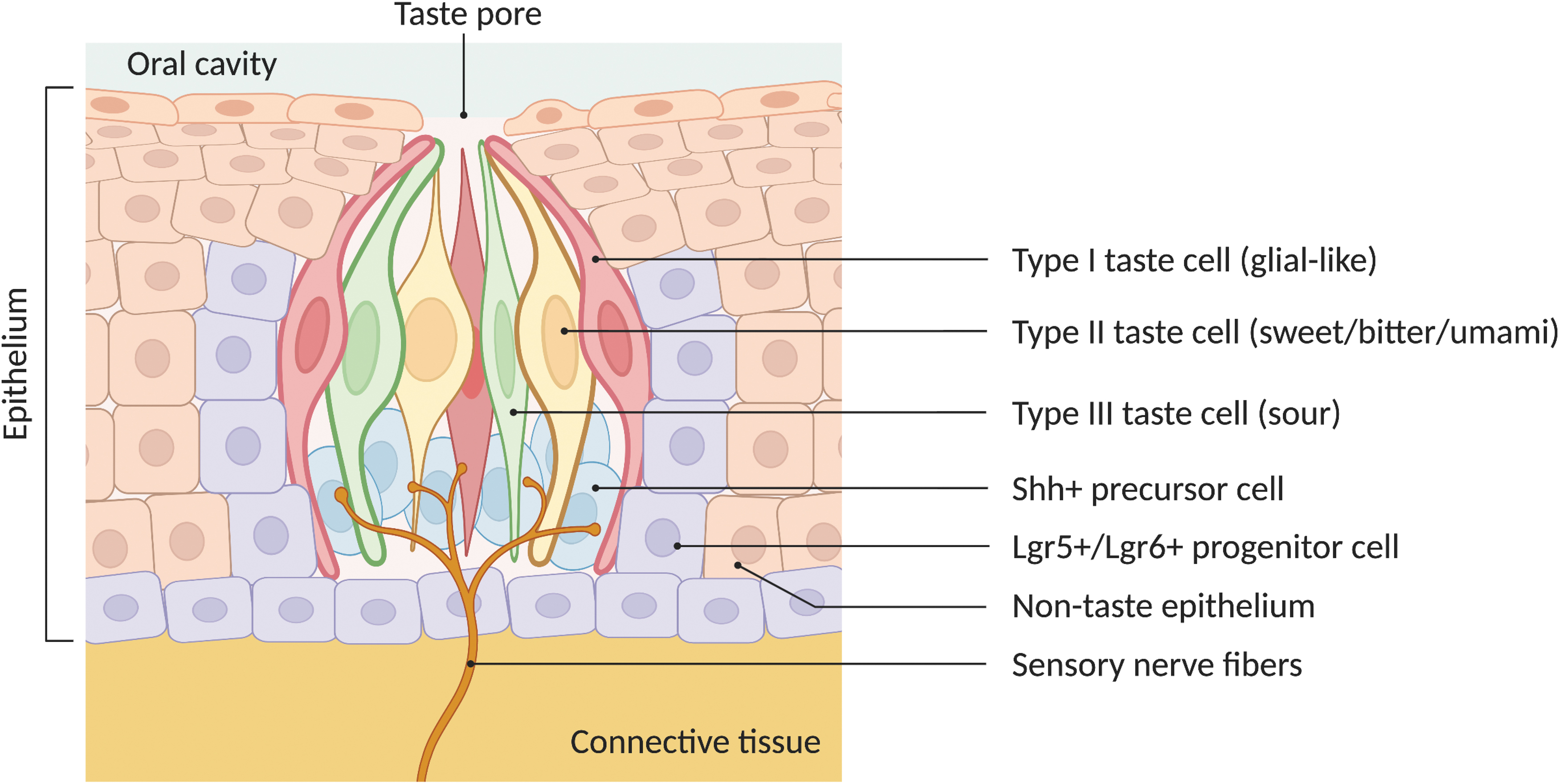
Taste bud architecture. Each taste bud contains 50–100 taste receptor cells and maintains a specific ratio of mature cell types: type I glial cells, type II sweet/bitter/umami detectors, and type III sour detectors. Taste receptor cells are replaced every 8–12 days by taste progenitor cells expressing leucine-rich repeat-containing G protein-coupled receptor 5 (Lgr5) or Lgr6, which subsequently differentiate into precursor cells expressing Shh. Taste receptor cells function to transduce chemical stimuli into neuronal signals, which are transmitted through sensory nerves. (Figure created with
TRC injury through irradiation, chemotherapy, or surgical procedures results in dysgeusia. For instance, local radiation for head and neck cancer or chemotherapy for other malignancies can disrupt taste sensation through impaired TRC turnover. 22,87 Otherwise, lingual defects occur from excision or trauma, and subsequent reconstruction with traditional autografts demonstrates poor taste bud regeneration, while skin-derived grafts can even induce taste bud loss in noninjured lingual mucosa. 66
Meanwhile, gustatory nerve injury secondary to surgical procedures (e.g., tympanoplasty) induces sensory neuron loss with subsequent TRC involution. 88 Moreover, taste bud recovery after nerve resection is slow and inconsistent: buds reappear at the earliest of 5–8 months, and ∼40% of patients experience persistent ipsilateral ageusia after 2 years. 88,89 Chronic dysgeusia is disabling, whereas acute dysgeusia may also be complicated by anorexia and subsequent malnutrition and poor wound healing. 66 Therefore, novel regenerative or protective taste bud therapies are needed to improve patient outcomes and long-term wellbeing.
Taste bud healing relies on progenitor cells capable of differentiating into all three types of mature TRCs. These progenitor cells are characterized by the expression of leucine-rich repeat-containing G protein-coupled receptor (Lgr)5 or Lgr6, and differentiate into precursor cells, which express sonic hedgehog (Shh) (Fig. 7). 22,59,86,90 –92 Meanwhile, neuronal support is necessary for TRC development and function. 86,93 –96 At the molecular level, R-spondin (Rspo)2 is a protein selectively expressed by gustatory ganglion neurons that functions as the ligand of Lgr5 and its homologs Lgr4 and Lgr6. 86,97 Systemic administration of exogenous Rspo2 or its homolog Rspo1 promoted differentiated TRC regeneration in mice after glossopharyngeal nerve transection. 86 However, Rspo proteins are not necessary for the proper differentiation of Lgr5 and Lgr6-positive stem cells, at least in vitro. 59
Meanwhile, Shh is expressed by both neurons and taste bud epithelial cells 98 and inhibits the embryonic formation of taste bud primordia but reverses to promote TRC differentiation immediately after birth and throughout adulthood in mice. 99,100 Particularly, ectopic Shh expression redirects differentiation of lingual epithelial precursors to form taste-bud-like structures containing all mature types of TRCs, even in lingual areas natively devoid of taste buds. 99 In addition, continuous administration of hedgehog signaling pathway inhibitor, sonidegib (aka. Odomzo), eliminated most taste buds in fungiform and circumvallate papillae. 101
Cell-based TRC therapies
Lgr5 and Lgr6-positive progenitor cells can successfully recreate three-dimensional taste organoids in vitro, which contain all types of mature TRCs and a native-like combination of proliferative progenitor and nonproliferative intragemmal cells. 59 Organoids can also recapitulate the gene expression profile of native circumvallate papillae when cultured with Rspo, Wnt3a, and Noggin. 102 Nevertheless, the prognosis of transplanted organoids is unknown, and further research is needed to pave the way for in vivo translation.
Bioactive TRC molecules
To date, bioactive molecules have been used to promote TRC regeneration and protect from taste bud injury in animal models. Exogenous systemic Rspo rescued mature TRCs in denervated rodent taste buds in vivo and in ex vivo culture of papillae tissue, 86 whereas Shh protein successfully reprogrammed lingual epithelial progenitor cells and induced ectopic formation of taste buds containing all differentiated TRC types. 99 Preventative strategies, such as using NAD-dependent deacetylase Sirtuin 1 inhibitors to modify the oxidative injury response and bolster cell proliferation, reduced lingual ulcer area in irradiated mice and partially rescued lingual epithelium thickness, and was also associated with mitigated loss of Lgr5-positive stem cells. 87
However, additional study is required for these molecules' clinical translation, especially regarding potential off-target and/or safety concerns. For example, Sirtuin 1 regulates many genes involved in cellular metabolism and homeostasis and has been shown to exert strong cardioprotective effects. 103 Likewise, Rspo dysregulation is implicated in the development of gastrointestinal tract malignancies. 104
Integrated TRC and nerve regeneration
It is worth noting that TRC reconstitution alone is insufficient for functional taste bud recovery, 88 and TRC/neuronal interfacing must also be restored. Le-Kim et al. engineered TRCs and neurons to self-assemble using surface molecules into multicellular clusters in vitro, capable of transducing bitter stimuli into neuronal signals within a few seconds and with an average transmission duration of 5 min. 105 Of similar note, in a critical-sized rat lingual defect model, purified gingival MSC-derived extracellular vesicles delivered in decellularized SIS matrix increased expression of markers specific to neurons, mature TRCs, epithelial stem cells, and taste bud progenitor cells. 66 Thus, integrated regeneration of TRCs and neurons will likely afford the greatest restoration of clinical taste sensation.
Salivary glands
Tissue characteristics & clinical challenges
The salivary system includes three pairs of major SGs ([1] parotid, [2] submandibular, and [3] sublingual), as well as ∼1,000 minor glands in the oral mucosa. The major SGs consist of a network of branching ducts that terminate into secretory acini, which can be serous, mucous, or mixed. 66 At the cellular level, SG epithelium comprises ductal, myoepithelial, and acinar cells (Fig. 8); acinar cells produce saliva, which is secreted by contraction of myoepithelial cells enveloping the acinar cell clusters. Secreted saliva undergoes modification as it travels through small intercalated ducts, striated ducts, and finally larger excretory ducts into the mouth (Fig. 8). Altogether, these structures enable the production of around 1.5 L of saliva daily. 106
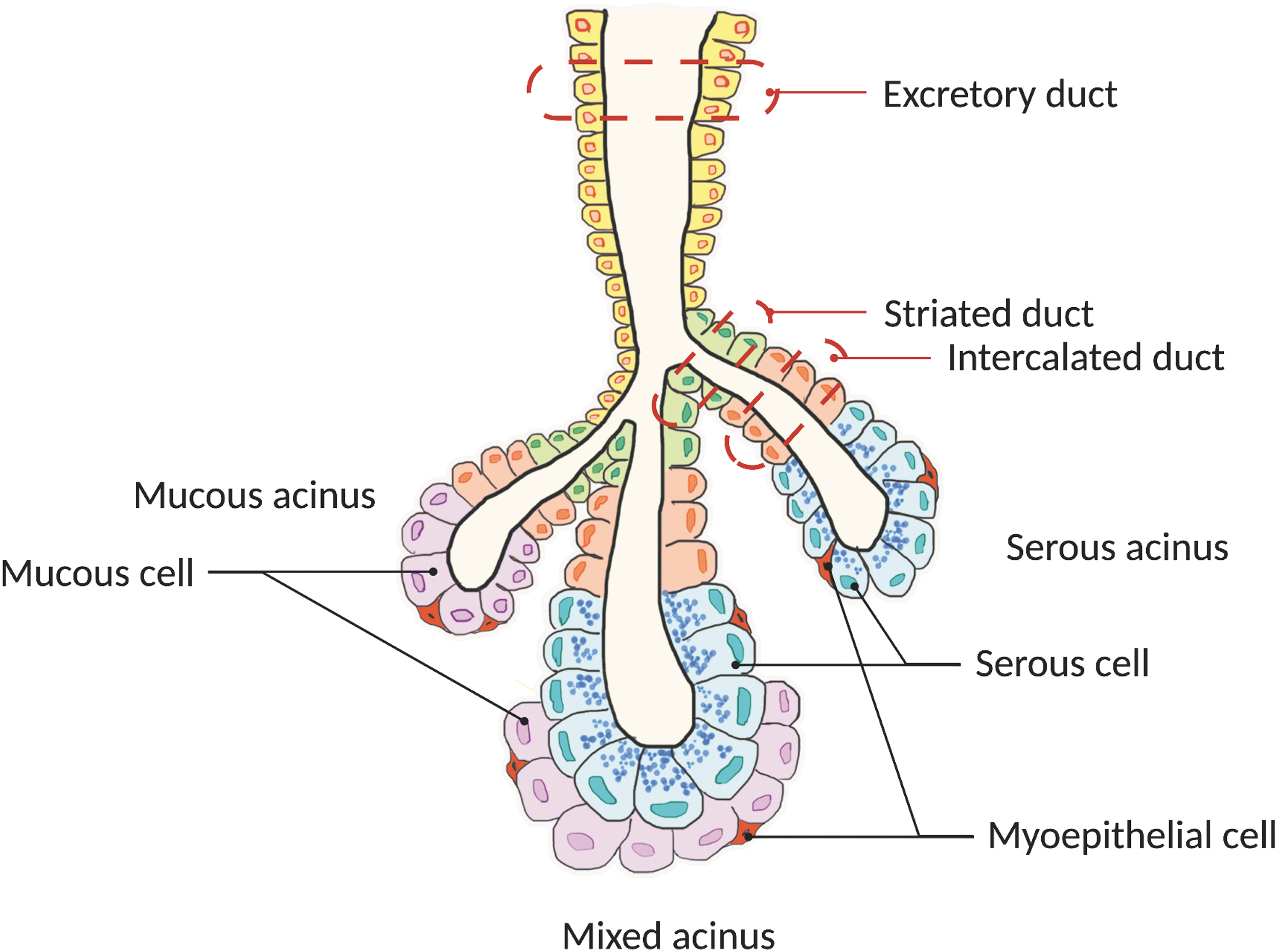
Salivary gland architecture and cell populations. Salivary glands consist of branching ducts that terminate into secretory acini (serous, mucous, or mixed). Gland epithelium comprises ductal, myoepithelial, and acinar (subdivided into mucous and serous) cells. Acinar cells produce saliva, which is secreted through the contraction of myoepithelial cells enveloping the acinar cell clusters. Secreted saliva undergoes further modification as it travels through small intercalated ducts, striated ducts, and finally larger excretory ducts into the mouth. (Figure created with
By secreting saliva into the oral cavity, SGs keep the mouth moist, initiate digestion, and maintain oral hygiene. On the other hand, hyposalivation increases the risk of dental caries and oral infections. 21 Radiation therapy for craniofacial malignancies as well as autoimmune diseases, such as Sjogren's syndrome and chronic graft-versus-host disease, can lead to SG injury that diminishes saliva generation, 9,56 whereas aging is another common cause of xerostomia with a reported prevalence between 20% and 30% in older aged individuals. 107 Disappointingly, current management strategies, including lifestyle changes and artificial saliva supplementation only provide temporary and often inconsistent relief.
Cell-based strategies
The structural complexity and healing dynamics of SGs make spontaneous regeneration difficult. 13,56 Thus, stem or progenitor cells obtained from parotid and/or submandibular glands 62,108 –111 are investigated for in vivo transplantation. 13 Excitingly, SG stem cells transplanted into radiation-damaged rodent SGs formed local ductal structures with increased acinar cell surface area. 62,63 However, isolating sufficient autologous cells from an injured gland is the major obstacle to this procedure.
Accordingly, MSCs are undergoing study as an alternative stem cell source for SG regeneration as preliminary animal and human studies suggest that intravenous injection slows autoimmune glandular destruction and enhances saliva flow after injury; MSCs were also successfully isolated from a broad spectrum of tissues, including but not limited to bone marrow, umbilical cord, dental pulp, and olfactory tissue (Fig. 6). 58,64,67 –69,112 –115 Intravenous delivery of BMSC-derived exosomes exhibit similarly promising effects. 68
Regenerative scaffolds and materials
In recent decades, biocompatible materials have catalyzed significant breakthroughs in SG organoid culture and transplantation. 56 Numerous materials were derived from endogenous matrix and growth factors and used for the formation of SG-like organoids, which can subsequently be transplanted for parenchymal restoration. 56 For example, fibrin hydrogels chemically conjugated to trimers of laminin-111 peptides or modified with a combination of laminin-1 peptides and human growth factors [vascular endothelial growth factor and fibroblast growth factor (FGF)9] significantly enhanced SG regeneration in vivo. 116,117 Additionally, a scaffold coating of catechol-conjugated hyaluronic acid imitated the hyaluronic acid-rich niche of embryonic submandibular glands and successfully directed the differentiation of SG progenitor cells into functional acinar and myoepithelial cells. 118
Other materials such as chitosan 119,120 and neurturin-containing laminin matrices 121 can promote native ECM reconstitution, and some synthetic polymers such as polyacrylamide gels, 122 elastin electrospun nanofiber, 123 and PLGA/PGA-sebacate nanofibers 124 can boast customizable mechanical properties and architecture (Fig. 5). A notable and persistent challenge is ensuring the long-term integration of transplanted organoids with native tissues.
Masseter muscle
Tissue characteristics and clinical challenges
The masseter is a large and powerful muscle of mastication, which inserts at the zygomatic bone, zygomatic arch of the temporal bone, and mandibular ramus (Fig. 9), 17 whose injury is uncommon but devastating for chewing function and nutrition status. 125,126 The typical causes of masseter injury include trauma, congenital deformity, surgery, and inherited musculodegenerative conditions. 125,126 The masseter and several other orofacial skeletal muscles derive from pharyngeal arches, unlike somites for limb and trunk skeletal muscles. 17,60 Compared with somite-derived skeletal muscles, the masseter displays poor regenerative capacity and is particularly susceptible to fibrofatty infiltration and slow myofiber regeneration, 17,60 which may be partially attributable to fewer total and proliferating myoblasts in the healing masseter. 60

Masseter muscle anatomy. The masseter consists of two heads (superficial and deep), which attach superiorly to the zygomatic bone and the zygomatic arch of the temporal bone, and inferiorly to the mandible. Branches of the facial nerve course in close proximity, and the parotid gland is located superficial to the muscle. Of note, the masseter is the most powerful muscle of mastication and contributes significantly to chewing. (Figure created with
Native regenerative cell populations
Injured masseter muscle recruits satellite and fibro/adipogenic progenitor cells that are phenotypically distinct from those of somite-derived skeletal muscle. 60 Generally, myogenic satellite cells (SCs) localize between the basal lamina and sarcolemma of myofibers, and are normally quiescent but respond to injury by proliferating and differentiating into myoblasts, which subsequently fuse into mature myofibers (Fig. 10). 17 SCs in the masseter belong to the mesoderm posterior bHLH transcription factor (Mesp)1)/ISL LIM homeobox (Isl)1 lineage, and undergo more active proliferation but delayed differentiation in vitro compared with those from the limb. 17,18,60 Interestingly, transplanted masseter SCs were equally effective as limb cells in limb muscle regeneration, which may be attributable to activity modulation of the recipient local environment. 17

Satellite and fibro/adipogenic progenitor cells: location and response to injury. Myogenic SCs are located between the basal lamina and sarcolemma of myofibers. Although normally quiescent, they respond to injury by proliferating and differentiating into myoblasts, which subsequently fuse into mature myofibers. Fibro/adipogenic progenitors are interstitially located mesenchymal cells. Postinjury, they migrate to damaged muscle, secrete ECM (to provide architectural support for regenerating myofibers) and paracrine factors (such as Wnt-inducible signaling pathway protein-1 and interleukin-10 to promote myogenic SC differentiation), before finally undergoing apoptosis. (Figure created with
Fibro/adipogenic progenitors are interstitially located mesenchymal cells that migrate to damaged muscle, deposit ECM (to provide architectural support for regenerating myofibers), and secrete paracrine factors {such as cellular communication network factor 4 [CCN4; aka. Wnt-inducible signaling pathway protein (WISP)1] and interleukin (IL)10 to promote myogenic SC differentiation} (Fig. 10). 60 Notably, after matrix synthesis, fibro/adipogenic progenitors then undergo apoptosis. 60
Masseter fibro/adipogenic progenitor cells are predominantly neural crest-derived, in contrast to mesoderm-derived progenitors in limb skeletal muscle, and express platelet-derived growth factor receptor alpha and stem cell antigen-1. 60,127 Because they demonstrate a greater tendency for fibrosis, similar to other ectoderm-derived tissues, and can also differentiate into adipocytes in the presence of proadipogenic systemic cues such as diet, 60,127 fibro/adipogenic progenitor cells may be the predominant contributor and promising therapeutic target for the fibrofatty response to masseter injury.
Cellular and acellular grafting materials
Transplanted and engineered cells demonstrate early success in masseter-specific muscle regeneration. For instance, premolar pulp cells that were epigenetically modified with DNA methylation agent 5-aza-2′-deoxycytidine demonstrated enhanced myogenic differentiation, with increased desmin/myogenin expression, myotube formation, and collagen gel contraction in vitro. 128 Local injection of modified cells also improved signs of muscle regeneration in cardiotoxin-damaged masseter and gastrocnemius in mice. 128 However, because neonatal SCs displayed significantly higher proliferative capability but decreased rates of myofiber fusion than their postnatal counterparts, 18 donor age must be a consideration for cellular masseter strategies.
Acellular scaffolds face unique healing obstacles within the masseter, such as the delayed differentiation and myofiber maturation of masseter SCs for which the mechanism is unclear. 17,18,60 Meanwhile, local fibro/adipogenic progenitor cells pose additional difficulties to acellular scaffold usage through excess fibrotic potential and undesirable multipotency. 60,127 Preserving a muscle cellular niche may be particularly challenging within the orofacial region–for example, muscle cells colonized a decellularized skeletal muscle matrix scaffold implanted at the masseter/mandible interface after masseter detachment, but were replaced by bony and cartilaginous tissues adjacent to the mandible. 129 Such considerations highlight the need for masseter-specific regeneration strategies, which may be superior to existing regenerative approaches for somite-derived skeletal muscle.
Myogenic molecules
Myogenic molecules are options for controlling local cell behavior to promote masseter regeneration. For example, by stimulating myogenic cell motility/differentiation, type III collagen expression, angiogenic activity, and differentiation of fibroblasts into myofibroblasts, SV peptide administration in rats mitigates fibrosis, and improves skeletal muscle functional recovery and muscle fiber diameter at 8 weeks postinjury. 74 Growth factors, including but not limited to FGF1, FGF2, FGF6, and hepatocyte growth factor, are also known to activate skeletal muscle SCs, 17 while TGF-β1 encourages myofiber formation in the developing tongue but reverses to inhibit SC activity and promote fibrosis and myofibroblast differentiation in adult wounded skeletal muscle.
Likewise, endogenous myostatin antagonists, such as follistatin and decorin (a proteoglycan belonging to the small leucine-rich proteoglycan family), 17 unsuppress SC proliferation and differentiation by inhibiting myostatin: a TGF-β family protein secreted by skeletal muscle. 126 Therefore, a diverse spectrum of molecules hold potential for bolstering masseter healing, although very few have been specifically tested in the masseter or orofacial healing environment.
Functional units: tongue and palate
Orofacial soft tissue injury commonly implicates multiple tissue types due to the tightly packed anatomy, and thus functional unit reconstruction in the orofacial region is more important than single tissue regeneration. As a result, the challenge of orofacial regeneration lies in not only regenerating individual tissues but also in reconstituting native-like intertissue interfacing and architecture.
Tongue
Component tissues in the tongue interact and communicate for proper function. The superficial tongue is covered by keratinized oral mucosa, termed lingual mucosa in this region (Fig. 3). Epithelial projections called papillae house superficially located taste buds. In between papillae are also interpapillary pits containing single unipotent stem cells, which replace lost lingual epithelium. 130 Numerous muscles are located deep to the mucosa and arise from SCs that likely share a similar lineage with somite-derived muscles. 1,60 Lastly, extensive deep neurovasculature encompasses multiple cranial nerves and a rich blood supply. 1 Lingual component tissues interface extensively, for example, taste buds transduce signals for neuronal propagation and taste sensation, lingual mucosa protects underlying tissue from mechanical and biochemical insults, and intricate musculature enables swallowing and speech. 9,14,15
Tongue injury occurs in a broad spectrum of scenarios, most commonly secondary to excision of head and neck malignancy, radiation/chemotherapy, and trauma, 9,16,19 whereas the clinical consequences of tissue and functional loss include infection, dysgeusia, speech deficits, and dysphagia complicated by malnutrition and chronic aspiration. Disappointingly, currently available surgical reconstruction and closure do not restore parenchyma, ultimately resulting in fibrosis with impaired tissue movement and sensation. 1 As a result, functional reconstitution is a pressing but daunting task.
Strategies for single-tissue regeneration in the tongue include cellular and acellular grafts. For example, porcine bladder matrix seeded with neonatal myoblasts increased expression of muscle-, neuron-, and vasculature-specific markers in rat lingual muscle defects and restored tongue mass and body weight to noninjured levels. 131 On the other hand, an engineered crosslinked, nanoscale cholesterol-bearing pullulan hydrogel facilitated myoblast adhesion, myofiber regeneration, sustained protein drug release, and eventual resorption in rodent lingual wounds. 132
Among the studies that address inter-tissue communication or functional restoration, genetically modified clusters of TRCs and neurons transduced taste stimuli into nervous signals in vitro. 105 Activated platelet-rich plasma injection into the deep tongue also increased neuron-specific marker expression and reduced wound inflammation and fibrosis in hemiglossectomy young mice on day 14, postoperatively. 133 In patients, a thrombin/fibrinogen biosponge improved oral clearance time, bolus clearance, and frenulum flexibility at >1 year after partial glossectomy defect closure, although the patient quality of life (as measured through functional intraoral Glasgow scale) was unchanged. 134
Despite these advances, there is an overall dearth of tongue biomaterial research. A systematic review in 2021 identified only eight original studies on tongue regeneration within the last 20 years. 1 Given the incidence and morbidity of head and neck malignancy, regenerative strategies for the tongue remain a research area of need.
Palate
Cleft palate is another important and complex clinical target, and surgical reconstruction frequently results in fibrosis and inadequate muscle regeneration, leaving up to 30% of young patients with long-term speech deficiencies and velopharyngeal dysfunction. 17,18 Soft palate muscles are pharyngeal arch derived, with SCs demonstrating delayed myogenic differentiation and increased fibrotic tendency. 17,18,60 Surgical wounds in the area also experience significant tension secondary to compact orofacial anatomy and sparse tissues for closure (Fig. 2), contributing to long-term craniofacial deformation with esthetic and functional consequences. 16,25
Minimal palate-targeted biomaterials were identified in literature. 2,25 Myogenic molecules, such as TGF- β1, FGF, decorin, and fibromodulin, have not been specifically tested in the palatal healing microenvironment, but are proposed to improve healing based on prior studies in limb and trunk skeletal muscle. 25,135
Future considerations for animal models
One additional concern is that many orofacial soft tissue therapies are researched in animal models and thus encounter limitations with clinical translation (Table 1). Rodent and rabbit models are commonly studied since they are inexpensive and easy to handle. However, they exhibit irreconcilable anatomic and histological differences compared with humans. Rodents are significantly less susceptible to posterior palatal and lip/alveolar clefts than humans due to embryonic differences in palatal shelf fusion. 136 Unlike the curved soft palate that terminates in the uvula in humans, the rodent soft palate forms a straighter pharynx and uniquely fuses with the pharyngeal wall or flanks the epiglottis, 136 which may contribute to dissimilar wound biomechanics in this region. Meanwhile, the rabbit palate is elongated and narrower at the rostral and caudal ends. 137
Biomaterial and tissue engineering strategies for orofacial soft tissue regeneration in vivo


Similar strategies utilized for multiple tissue types are highlighted in the same color.
TRC, taste receptor cell.
Histologically, murine oral mucosa is thinner and more keratinized than human tissue and possesses decreased epithelial projections. 138 Rabbit palatal mucosa also exhibits decreasing epithelial keratinization anteriorly, which may reflect the animal's vegetarian diet. 137 Last but not least, the murine oral microbiome displays less richness and interanimal variability than its human counterpart, which may contribute to differing orofacial infection susceptibility due to minimal overlap in bacterial species. 139
Large animal models, such as dogs and pigs, may better simulate orofacial wounds of a more comparable scale. 30 Particularly, minipigs and monkeys possess similar oral mucosal thickness, keratinization, and architecture as humans. 138 However, large animals are currently rarely used for orofacial soft tissue research due to cost, technical difficulty, and more strict facility requirements. Thus, further investigations are warranted to reveal the detailed differences in wound physiology and biomechanics between these large animals and humans.
Undoubtedly, the experimental defects in animal models are poorly representative of real-world injury. 30 Patients seen in the clinical setting may suffer from defects involving multiple tissues, possibly with wide and/or uneven wound margins, and experience significant tension across the wound even after closure. Bearing these concerns, cell-based therapies rooted in animal studies are still variably pragmatic in clinical practice, where donor tissue availability and donor-site morbidity become predominant hurdles. 11,61 –63 As the literature on orofacial soft tissue biomaterials continues to grow, there will be a greater impetus to test promising findings in large animal or human models to confirm real-world efficacy.
SUMMARY
Biomaterials consist of any combination of supporting materials, cells, and bioactive molecules and provide exciting strategies for orofacial tissue regeneration. Orofacial tissues possess profound functional and esthetic significance, but encounter marked barriers to healing, including high mechanical demand, nonsterile environment, and intrinsic cellular limitations. In vitro, in vivo, and early clinical studies demonstrate biomaterials accelerate healing and enable the reconstitution of native-like tissues, including oral mucosa, TRCs, and SGs. Biomaterials also show early promise in promoting masseter muscle, tongue, and soft palate reconstitution but require further investigation due to intricate tissue architecture and stem/progenitor cell behavior nuances.
As a final consideration, clinical translatability remains an important focus. As single tissue regeneration becomes increasingly successful, reconstitution of tissue/tissue interactions and organ architecture will emphasize functional orofacial restoration. In addition, growth factors or allogeneic/autogenic cell therapies may require scrutiny for long-term safety and biocompatibility. 1 Furthermore, scalability and financial solvency are concerns for human-derived or poorly storable biomaterials. 1 Lastly, patient-centric goals such as mobility and sensation may help guide therapeutic priorities for tissues particularly difficult to restore. In summary, biomaterials are increasingly successful in regenerating native-like orofacial tissues and may benefit from future research into functional restoration and clinical translation.
TAKE-HOME MESSAGES
Regeneration of orofacial soft tissues is a pressing and inadequately addressed clinical need.
Orofacial soft tissues are daunting regenerative targets due to nuanced physiology, specialized cellular behavior, and uniquely nonsterile and humid environments.
In the last 5 years, biomaterial advancements encompass novel scaffolds, seeded cells, and bioactive molecules that specifically target orofacial soft tissues.
As single-tissue regeneration becomes increasingly successful, emphasis on clinical translatability (particularly functional unit reconstruction, safety, and scalability) will offer the greatest functional improvements for patients.
Footnotes
AUTHORs' CONTRIBUTIONS
P.H. and C.L. collected and interrelated the data for the work. P.H. and T.L. interpreted the data, drafted, and revised the article. C.L. and Z.Z. established the concept, designed the work, and revised and approved the article.
ABOUT THE AUTHORS
AUTHOR DISCLOSURE AND GHOSTWRITING
The content of this article was written by the authors listed. No ghostwriter was used to write this article.
FUNDING STATEMENT
This study was supported by the American Association of Orthodontists Foundation (AAOF) Orthodontic Faculty Development Fellowship Award, American Association of Orthodontists (AAO) Full-Time Faculty Fellowship Award, University of Pennsylvania School of Dental Medicine Joseph and Josephine Rabinowitz Award for Excellence in Research, and the J. Henry O'Hern Jr. Pilot Grant from the Department of Orthodontics, University of Pennsylvania School of Dental Medicine for Chenshuang Li.