
Abstract
Significance:
Half of all cancer patients receive radiation therapy as a component of their treatment regimen, and the most common resulting complication is radiation-induced fibrosis (RIF) of the skin and soft tissue. This thickening of the dermis paired with decreased vascularity results in functional limitations and esthetic concerns and poses unique challenges when considering surgical exploration or reconstruction. Existing therapeutic options for RIF of the skin are limited both in scope and efficacy. Cell-based therapies have emerged as a promising means of utilizing regenerative cell populations to improve both functional and esthetic outcomes, and even as prophylaxis for RIF.
Recent Advances:
As one of the leading areas of cell-based therapy research, adipose-derived stromal cells (ADSCs) demonstrate significant therapeutic potential in the treatment of RIF. The introduction of the ADSC-augmented fat graft has shown clinical utility. Recent research dedicated to characterizing specific ADSC subpopulations points toward further granularity in understanding of the mechanisms driving the well-established clinical outcomes seen with fat grafting therapy.
Critical Issues:
Various animal models of RIF demonstrated improved clinical outcomes following treatment with cell-based therapies, but the cellular and molecular basis underlying these effects remains poorly understood.
Future Directions:
Recent literature has focused on improving the efficacy of cell-based therapies, most notably through (1) augmentation of fat grafts with platelet-rich plasma and (2) the modification of expressed RNA through epitranscriptomics. For the latter, new and promising gene targets continue to be identified which have the potential to reverse the effects of fibrosis by increasing angiogenesis, decreasing inflammation, and promoting adipogenesis.

SCOPE AND SIGNIFICANCE
Radiation-induced fibrosis (RIF) of the skin is the most common complication resulting from radiation therapy for cancer treatment. While this therapy can be lifesaving from an oncologic standpoint, the collateral damage caused to the skin can result in functional limitations and litany of sequela, including ulceration, atrophy, and necrosis. Microscopic changes to the dermis, including thickening and decreased perfusion, result in poor surgical outcomes when reconstruction or re-exploration of the area is performed. Current therapies for RIF are limited to noninvasive modalities such as physical therapy, topical treatments, or more invasive techniques such as fat grafting. However, cell-based therapies provide hope of improved functional and esthetic outcomes for patients and surgeons alike.
TRANSLATIONAL RELEVANCE
Although many in vitro and animal model studies point to the potential of cell-based therapies to improve treatment of RIF, translating these therapies to common clinical practice presents several challenges. Notably, fibrotic tissue acts as a hostile graft recipient site, and typical lipoaspirate grafting results in frequent complications and poor retention. While adipose-derived stromal cells (ADSCs) have addressed these concerns in part, logistical complications of harvesting a large enough volume of these cells, particularly from specific subpopulations, remain an important area of future consideration.
CLINICAL RELEVANCE
RIF commonly occurs in cancer patients who often require repeated surgical or reconstructive procedures. Fibrotic skin poses a particular surgical challenge due to a lack of perfusion leading to poor wound healing. Consequently, surgical complications following operations on fibrotic skin are more common. Interestingly, the same characteristics of fibrotic skin that create challenges in surgery lead to similar challenges in fat grafting as well, especially concerning fat graft retention. Therefore, recent developments in augmentation of fat grafts with ADSCs and other agents provide a promising future for the increased utility of this therapy for RIF.
BACKGROUND
Radiation therapy
Less than 1 year following the discovery of x-rays in 1895, radiation was used therapeutically by Emil Herman Grubbe to treat a patient with breast cancer. 1 Recognition of radiation therapy's utility in cancer treatment grew rapidly as the intervention became integrated into curative, palliative, preoperative, postoperative, and combination chemotherapy regimens. 2 Today, approximately half of cancer patients receive radiation therapy during the course of their illness, marking the enduring presence of radiation as a pillar of modern cancer treatment. 1,3 The population of 3.4 million radiation-treated cancer survivors is expected to grow to 4.2 million by 2030. 4 While radiation therapy improved recurrence and mortality rates in oncologic pathologies, this medical intervention is not without complications.
Radiation-induced fibrosis
Since Grubbe's era, significant advances in the field of radiation oncology have increased controllability and spatial specificity of radiation therapy. 1 Despite the resulting improvement in safety for patients, significant and unwanted side effects of all forms of radiation therapy persist. One of the most notable long-term sequelae of radiation therapy is radiation fibrosis syndrome. This process most frequently affects the skin and subcutaneous tissue, but has been notably documented in the pulmonary system, gastrointestinal and genitourinary tracts, and any organ system present in the radiation field. 5
When focusing specifically on the skin and soft tissue, chronic effects of radiation therapy include tissue atrophy, alopecia, as well as increased stiffness. Functional limitations, secondary to reduced skin elasticity and mobility, can significantly impact patients' quality of life. Furthermore, vascularity and perfusion of the affected skin are decreased in the chronic stage of RIF, resulting in complications with wound healing as these tissues often undergo repeated surgical procedures either for oncologic recurrence or for reconstructive purposes. 6,7 RIF can also cause undesirable esthetic results, including telangiectasia, induration, ulceration, hyperplasia, atrophy, and necrosis of the dermis. 8
Pathogenesis and molecular basis of RIF
The organ system most often affected by radiotherapy is the skin, making it the most studied organ system in relation to RIF. Skin injury resulting from radiation therapy can be understood in two stages, acute and chronic. While the acute stage can begin within days or weeks of radiation injury, the findings associated with the chronic stage may take 4–12 months to develop and progressively worsens for many years. 9
Initial exposure to ionizing radiation results in DNA damage to cells in the radiation field and the release of reactive oxygen species (ROS) generated from radiolysis of water to hydroxyl free radicals. This acute phase of injury initiates a number of cytokine cascades which triggers a massive inflammatory response, manifesting clinically as erythema, discoloration, or desquamation.
In some cases of more significant damage, atrophy and ulceration can occur. 6,10 The high level of proliferation in hair follicle stem cells and basal keratinocytes makes them particularly susceptible to damage by radiotherapy. 8,11 The damage to these cells, as well as resident fibroblasts, endothelial cells, and epidermal cells, results in the release of cytokines and attraction of neutrophils to the region. The neutrophils proceed to release additional pro-inflammatory cytokines in the area, including tumor necrosis factor alpha (TNF-α), interleukin-1 (IL-1), and IL-6. 7
As a result, the inflammatory process progresses, ROS are released, and monocytes and lymphocytes migrate to the irradiated area. The ROS which are generated directly damage genetic material, inhibiting normal cell function and can induce apoptosis. 12 Monocytes subsequently differentiate to macrophages upon arriving to the damaged tissue. The release of platelet-derived growth factor by macrophages has been shown to stimulate angiogenesis and the migration of fibroblasts, which play an important role in the progression of fibrosis, to the area (Fig. 1).

Visualizes the progressive effects of radiation on the skin, from immediate (far left), effect after days (middle left), effect after weeks (middle right), to the long-term formation of chronic RIF after months and years (far right). Corresponding text descriptions below detail the changes occurring in each timeframe. RIF, radiation-induced fibrosis.
These fibroblasts, along with the macrophages that stimulate their migration, and native endothelial and epidermal cells, secrete transforming growth factor β1 (TGF-β1), a growth factor/cytokine which appears to play a principal role in the pathogenesis of RIF. Increased TGF-β1 levels are detectable within hours after radiation exposure. 13 TGF-β1 promotes fibrosis through binding to the transmembrane serine and threonine kinase receptors TGF-β receptors I and II (TβRI and TβRII) and inducing phosphorylation and activation of the intracellular Receptor-associated Suppressor of Mothers against Decapentaplegic (R-Smads). 14 Upon activation/phosphorylation, R-Smads join with a co-Smad (Smad4) to form heteromeric complexes before translocating to the nucleus to act as a transcription factor for several profibrotic genes (Fig. 2). 15,16
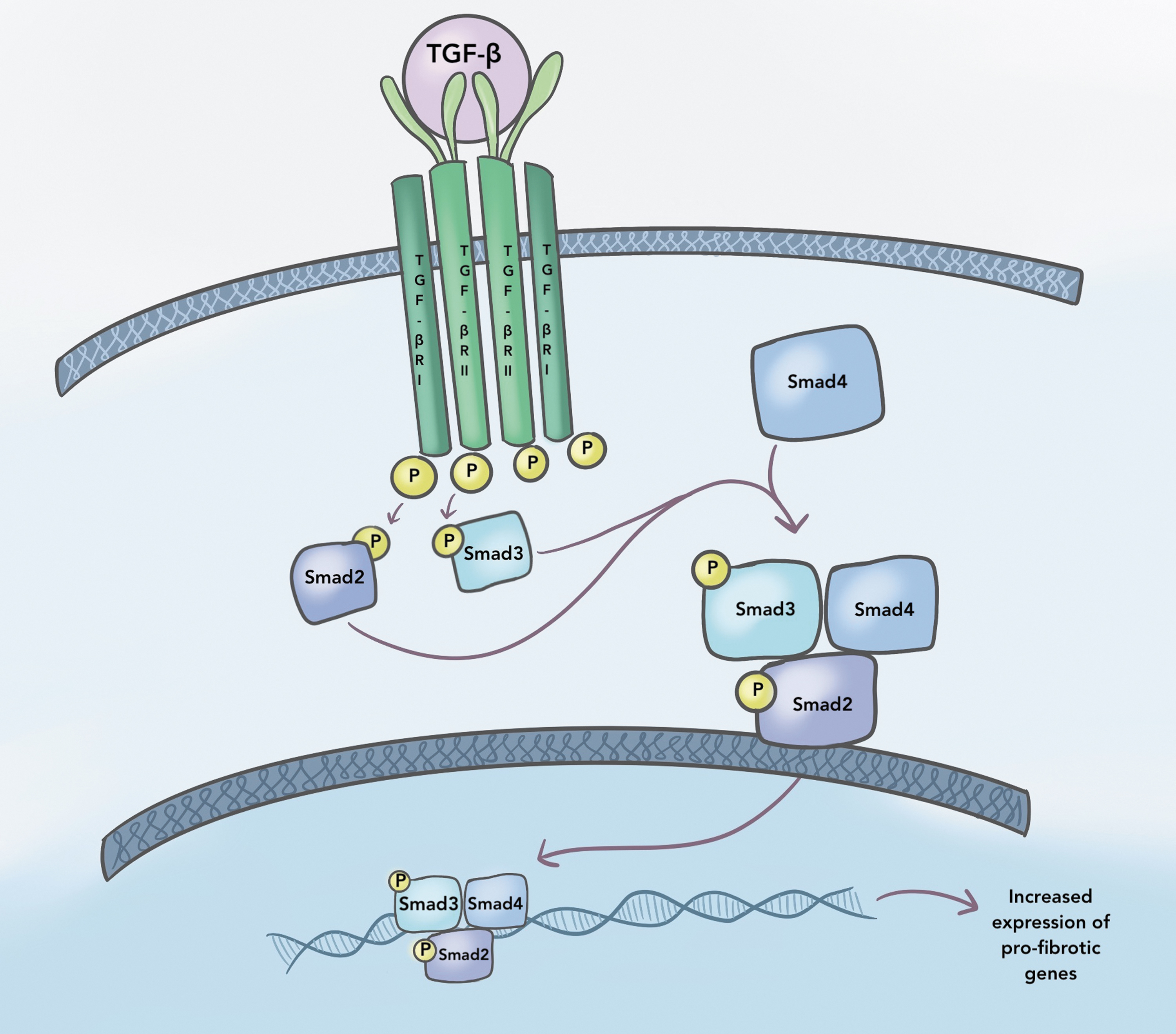
Depicts the TGF-β signaling pathway, an important pro-fibrotic pathway in RIF. TGF-β is secreted by fibroblasts and macrophages in tissue damaged by RIF. TGF-β binds to the transmembrane receptors TβRI and TβRII, which subsequently induces phosphorylation of intracellular Receptor-associated Suppressor of Mothers against Decapentaplegic (R-Smads). These R-Smads are also known as Smad2 and Smad3, as denoted in the figure. The R-Smads join with a co-Smad (Smad4) to form heteromeric complexes. These complexes translocate to the nucleus and act as a transcription factor for profibrotic genes. TGF-β, transforming growth factor β.
Through this pathway, the downstream profibrotic effects of TGF-β1 are numerous and play a large role in the pathogenesis of the chronic stage of RIF, which can involve scarring, retraction, hair loss, and changes in pigmentation. In some cases, hyperplasia, atrophy, ulcers, or skin tumors may emerge. 17 –19 One of the primary ways TGF-β1 mediates the formation of fibrosis is through the activation of fibroblasts to myofibroblasts.
While quiescent dermal fibroblasts undergo low levels of gene transcription and translation with few interactions with nearby cells, myofibroblasts upregulate expression of contractile proteins that promote tensile interactions with neighboring cells and extracellular matrix (ECM) proteins. 20 Myofibroblasts uniquely express a component of anchorage molecules, α-smooth muscle actin, which is associated with the formation of focal adhesions. 21 Myofibroblasts additionally are known to play an important role in the homeostasis of the ECM. 8
When TGF-β1, among other factors, induces fibroblast differentiation into myofibroblasts (Fig. 3), increased secretion of proteins such as collagen, fibronectin, and proteoglycans into the ECM begins. 7 In addition to promoting the secretion of ECM proteins, TGF-β1 also reduces matrix metalloproteinase activity within myofibroblasts, particularly metalloproteinase-2, -9, and -1, which impair ECM degradation. 6,10 The increase in contractile force between myofibroblasts and their ECM, as well as increased deposition of ECM proteins, promotes tissue stiffness and thickness, contributing to the pathological presentation observed in RIF. 22

Illustrates the transition from fibroblast to myofibroblast. Quiescent dermal fibroblasts (far left) undergo low levels of gene expression and do not contribute to excessive deposition of ECM proteins. When these fibroblasts are exposed to TGF-β, mechanical tension, and other factors, the transition to pro-myofibroblasts (middle) and finally to myofibroblasts occurs. Myofibroblasts (far right), in comparison to quiescent fibroblasts, are characterized, in part, by increased focal adhesions, cytoplasmic actin stress fibers, and α-SMA. These cellular components contribute to the clinical presentation of RIF. ECM, extracellular matrix; α-SMA, α-smooth muscle actin.
In addition, TGF-β1 further contributes to the progression of fibrosis by activating the interferon γ response and the release of TNF-α and IL-1. 22,23 Activation of these profibrotic pathways is believed to persist for years after initial exposure to radiation. 8 Support for this hypothesis has been demonstrated by increased levels of type I and III collagen, as well as TGF-β1, up to 20 years following radiation therapy. 24
Tissue changes in radiation fibrosis
Vasculature
Chronic fibrosis results in changes to the rich vasculature of the dermis. Radiation most significantly affects smaller arterioles and capillaries, resulting in decreased microvascular network density and pericapillary fibrosis. 8,25 Histological changes in vessel morphology and permeability have been suggested, including endothelial hyperplasia and swelling, as well as perivascular fibrosis. 8,24,26 In the acute stage following radiation therapy, vessels become obstructed with fibrin and leukocytes within hours of radiation exposure. 7,8,27
The resulting decrease in perfusion to the tissue and lower oxygen delivery results in expression of collagen type 1 alpha1, which further exacerbates fibrosis, and ultimately can lead to atrophy. 8,28 While the resultant hypoxia stimulates neovascularization, these are often irregular and easily occluded capillaries that cannot effectively reperfuse the tissue. 8 Overall, blood flow to irradiated skin has been shown to be significantly reduced compared to nonirradiated skin. 29,30
Cellular consequences
The combined effect of these cellular changes in the area results in significant impacts on the form and function of the affected tissue. The fibrotic process can impede vascular and lymphatic drainage, resulting in decreased perfusion and subsequent hypoxia. 31 This process can make the affected tissue susceptible to ulceration and poor wound healing. Furthermore, these changes in tissue affected by RIF are particularly unideal for surgery, resulting in delayed healing and increased complication rates. 32,33
DISCUSSION
Current therapeutic options
Physical therapy
Physical therapy for those who have undergone radiation therapy aims to improve functionality by physically manipulating the treated area. The goal of this treatment is to improve range of motion through reduction of scar tissue adhesion, ultimately improving patient quality of life. Treatment regimens often include guided stretches, exercise, and massage. 34 Studies have demonstrated that the addition of physical therapy to treatment regimens improves quality of life, particularly for breast cancer, as well as head and neck cancer, patients who are at higher risk to suffer contractures in the shoulder and neck area following radiation that can impair movement at the corresponding joints. 35,36
One study found that patients who had undergone radiation therapy reported decreased erythema, pain, pruritus, induration, and skin toughness after 1 month of mechanical massage treatment. 37 Another study indicated that deep friction massage may decrease spasms that can result from radiation fibrosis. 38 While physical therapy can be useful in treatment of mechanical limitations associated with RIF, no evidence has shown that physical therapy alone can slow the progression of RIF on a cellular level.
Deferoxamine
Deferoxamine (DFO) is an iron-chelating agent naturally produced by Streptomyces pilosus. 39 Systemic administration of DFO is FDA approved and has previously been utilized clinically in the treatment of hemochromatosis and thalassemia. 31,40,41 After preclinical studies demonstrated locally administered DFO to increase vascular endothelial growth factor (VEGF) production, interest in the agent's utility to improve wound healing, particularly for RIF, emerged.
DFO is thought to act through inactivation of prolyl 4-hydroxylase (PHD), by sequestering iron which acts as its necessary cofactor. PHD constitutively degrades hypoxia-inducible factor 1 alpha (HIF-1ɑ), and in PHD's absence an increased amount of HIF-1ɑ results in increased VEGF transcription. 42 This pathway is hypothesized to result in the improved vascularization of irradiated mouse tissue when treated with topical DFO. 3,43 In addition, DFO's sequestration of iron is thought to reduce iron-catalyzed ROS and free radical formation. 44
These mechanisms are thought to contribute to the findings that local administration of DFO onto irradiated mouse skin can enhance vascularization and increase fat graft retention while reducing dermal thickness. 45 Another study demonstrated that collagen fibril disorganization can be decreased in irradiated mouse skin by transdermal DFO application. 46 These results indicate the potential of DFO to diminish and prevent the skin fibrosis resulting from radiation therapy.
Vitamin E and pentoxifylline
Finally, several studies have focused on the use of the antioxidant alpha-tocopherol (Vitamin E) alone or in conjunction with the anti-inflammatory pentoxifylline to improve tissue compliance in cancer patients who have undergone radiation therapy. 47,48 The combination of these two therapies is thought to work by reducing the large inflammatory response following radiation in addition to blocking TGF-β signaling in irradiated tissues. 49
Fat grafting
While fat grafting has long been used as a method of providing volume restoration in the setting of reconstructive surgery, renewed interest in the use of this tool for therapeutic treatment of RIF emerged in 2007 when a study by Rigotti et al reported symptomatic and esthetic improvements in 20 breast cancer patients with RIF following autologous fat transfer. These patients exhibited neovessel formation, improved hydration, and regeneration of healthy tissue in the treated area, leading to an explosion in interest regarding this therapy and the molecular mechanisms behind it. 50
Since this study, these results have been reproduced and expanded upon by a number of clinical research articles. 51 –54 One group, Salgarello et al, found reduced radiation-related complications in patients undergoing breast reconstruction when fat grafting was used, first in a case study of two patients, and later in a retrospective review of 16 patients. 55,56 An additional large prospective clinical study followed 65 postmastectomy patients who had undergone radiation therapy and received tissue expanders and fat grafting as part of their breast reconstruction and were found to have reduced capsular contracture and improved skin quality with this approach. 57
These clinical results have been corroborated in animal models, where fat grafting in irradiated mice has been shown to decrease thickening of the dermal layer and improve collagen organization. In addition, increased skin perfusion and improved vascularity have been demonstrated in this model. 27 While initial evidence suggested that physical or dilutional effects associated with fat grafting were responsible for the therapeutic benefits, recent evidence has pointed toward ADSCs as the responsible agent. 8,58 –60
Irradiated fields present as hostile graft sites
Although the utility of fat grafting in treatment of RIF demonstrates great promise, the preexisting radiation damage to the tissue in the graft site presents several challenges to this treatment modality. Irradiated tissue is suboptimal as a recipient due to hypo-vascularity, inflammation, and fibrosis. 27,61 This environment can result in necrosis of the graft and promote additional inflammation in the area, further exacerbating fibrosis, calcification, cyst formation, and infection. 62 –64 Fat graft volume retention in a radiated site has been shown to be lower than in healthy tissue. 61 Approaches to overcoming challenges presented by the recipient site include preconditioning of the area before fat grafting, as well as to changes to the processing and augmentation of harvested fat. 24
DFO preconditioning
In 2018, Flacco et al found that pretreating irradiated tissue with DFO before fat grafting resulted in improved fat graft volume retention, vascularity, and perfusion, as well as decreased dermal thickness. 45
Vitamin E supplementation
A study by Abbas et al integrated vitamin E and pentoxifylline into fat grafts in mice to demonstrate that vitamin E treated grafts had improved dermal thickness and collagen density in mice. 65 This study also showed that vitamin E improved fat graft retention. 65
Serial fat transfer
Panettiere et al attempted to improve fat transfer outcomes in radiated breast tissue using a “serial fat transfer technique,” involving multiple sessions of lipofilling. 53 In 20 clinical patients with irradiated reconstructed breasts, this study found improved functional and cosmetic outcomes compared with a control group which underwent only one round of lipofilling. 53
Adipose-derived stromal cells
To address the uniquely hostile graft site presented by RIF, one technique developed to augment the volume retention and benefits of autologous lipotransfer is the enrichment of fat grafts with ADSCs, a method coined “cell-assisted lipo-transfer” (CAL) (Fig. 4). Whole adipose tissue contains both adipose progenitor cells, as well as multipotent stem cells, that can differentiate primarily into osteogenic, adipogenic, myogenic, and chondrogenic lineages (Fig. 5). Several other lineages have also been reported in the literature. Stem cells have been noted to possess several qualities, including capacity for self-renewal, long-term viability, and multilineage potential, which make them appealing in the setting of fat grafting, particularly to treat RIF. 66 ADSCs represent a comparatively readily available and easily obtained population of mesenchymal progenitor cells, as those obtained from bone marrow are in shorter supply and harvested with more difficulty.
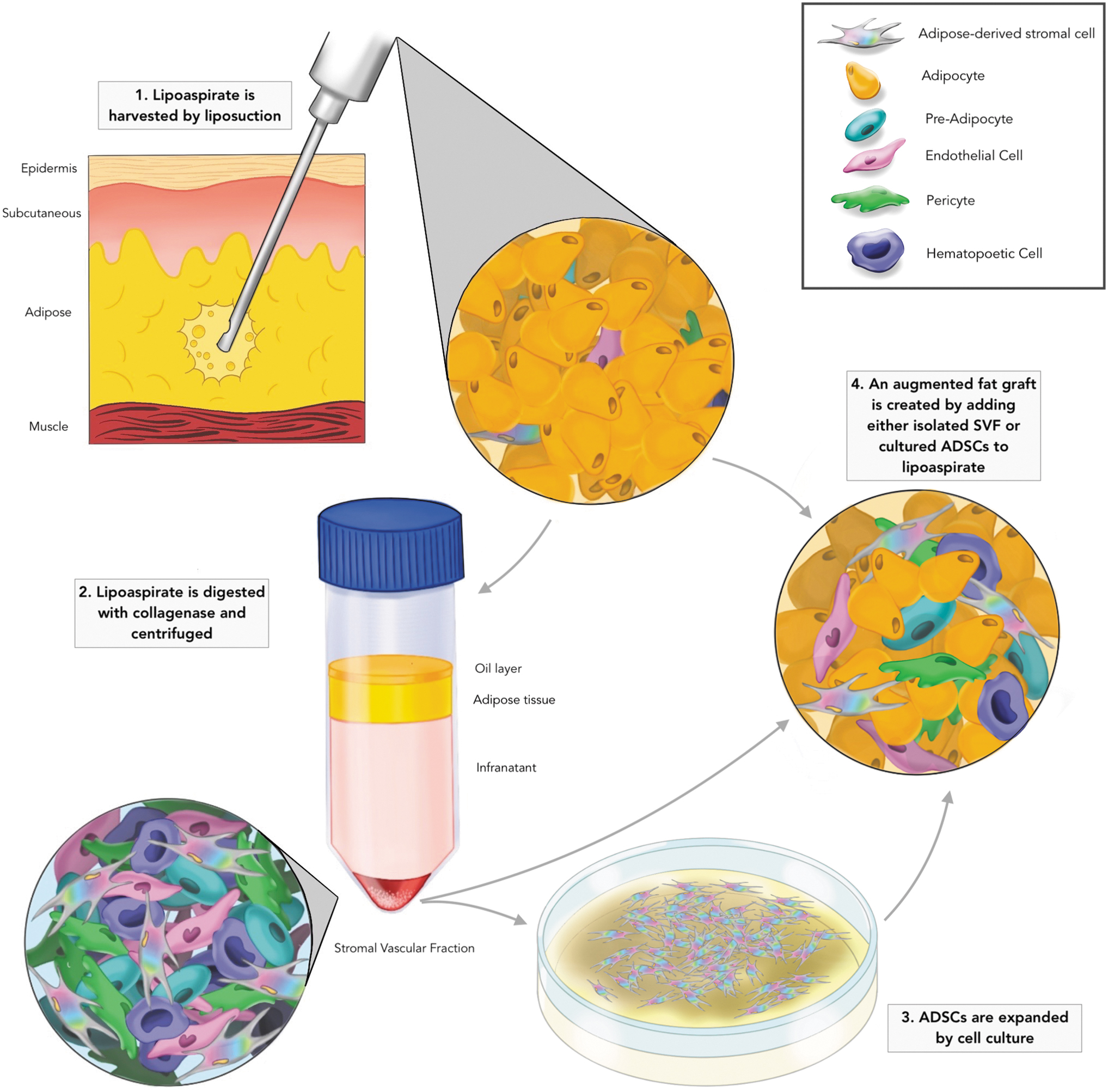
Illustrates the process of creating a fat graft augmented with either ADSCs or the stromal vascular fraction. At point 1, lipoaspirate is harvested by liposuction from the adipose tissue. This lipoaspirate is processed, at point 2, by a digestion with collagenase and centrifugation. The resulting product separates into four identifiable layers, the oil layer, adipose tissue, infranatant, and the stromal vascular fraction (in descending order). The stromal vascular fraction (which includes a heterogenous mix of preadipocytes, endothelial cells, pericytes, hematopoietic cells, and ADSCs) is at that time isolated and either directly added to lipoaspirate or expanded by cell cultured (point 3) to specifically increase the number of ADSCs. One or both of these products are added to lipoaspirate to create an augmented fat graft, seen at point 4.
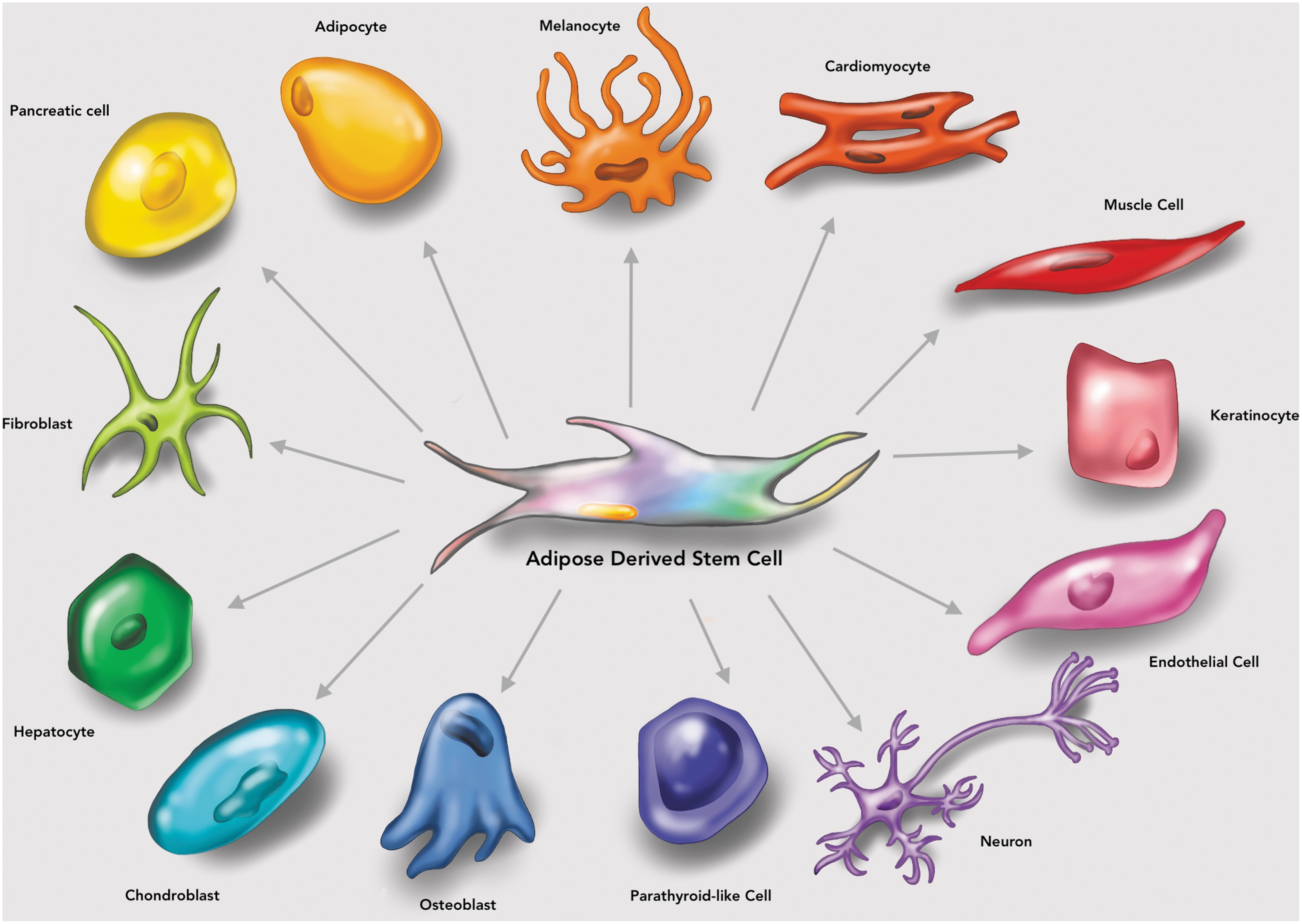
(lineages) ADSCs are multipotent progenitor cells that can differentiate into a variety of lineages, as depicted in Fig. 5. ADSC, adipose-derived stromal cell.
Studies have indicated that during the process of liposuction, the resulting lipoaspirate contains a relatively low proportion of ADSCs compared to whole fat, potentially contributing to the volume retention concerns and necrosis complications in fat grafting. 67 This technique aims to enrich lipoaspirate with additional ADSCs and ultimately improve clinical outcomes.
Indeed, CAL has been demonstrated to increase fat retention and improve cosmetic outcomes clinically. 68,69 Microvasculature has been detected more prominently following CAL, indicating its potential effect of increasing angiogenesis. 68 Animal studies have demonstrated decreased dermal thickness, lower collagen density, improved structural quality, and increased vascularity when CAL was utilized in RIF compared to whole fat graft. 8 In this mouse model, irradiated skin treated with CAL was also found to be less stiff and have improved elasticity compared to radiated skin treated with normal fat grafting. 61 Another study utilizing a rat model demonstrated that ADSCs promote hair follicle and sebaceous gland regeneration, in addition to having anti-inflammatory, antifibrotic, and antiapoptotic effects in RIF. This study also found that ADSCs can have a protective effect against the formation of RIF (Fig. 6). 70

Demonstrates the numerous beneficial effects associated with treating irradiated skin with a fat graft containing ADSCs. Findings in typical irradiated skin include epidermal thinning, atrophy of the hair follicles and sebaceous glands, dermal thickening, increased collagen density and linear collagen organization, and decreased vascularization. The addition of a fat graft containing ADSCs to irradiated skin has been shown to decrease dermal atrophy, promote hair follicle and sebaceous gland growth, decrease dermal thickness, decrease density, and increase basket weave organization of collagen, improve fat graft retention, and improve vasculo- and angiogenesis.
Acquisition/processing of ADSCs
CAL follows a protocol similar to that of basic fat grafting, beginning with the harvesting of adipose tissue through liposuction.
The lipoaspirate is mechanically processed or digested with a mixture of PBS and collagenase I and III to separate the mature adipocytes and connective tissue from the stromal vascular fraction (SVF) or “pellet.” 68 This pellet contains a heterogeneous mix of cells from various lineages, including ADSCs, preadipocytes, premature endothelial cells, mature endothelial cells, hematopoietic cells, and pericytes. 71 The SVF is then isolated, resuspended, filtered, and, depending on use, further processed. 24,68 Studies indicate that ∼10% of the SVF is constituted of ADSCs by flow cytometry. 72 Therefore, SVF has been used for various cell-based therapies, including CAL. 68
However, to isolate and purify the heterogenous mix of ADSCs from SVF, surface immunophenotypes are used as a mechanism to identify and sort subpopulations. Immunomagnetic beads and flow cytometry have both been used to select for and against cell types of interest. 73 –75 ADSCs have also been found to readily adhere to plastic culture flasks, providing another method of isolating ADSCs from the SVF for expansion by culture. 70 Once the ADSCs have been isolated and/or cultured to the desired specificity and volume, they are attached to unaugmented lipoaspirate, which acts as a scaffold to create an ADSC-rich lipoaspirate ready for fat grafting. 13
Some studies have considered the use of the SVF “cell pellet” without additional processing or addition of lipoaspirate. A clinical study involving five patients who had undergone radiation therapy and developed subsequent RIF experienced improved wound healing and pain relief following autogenous SVF cell pellet injection. 72 While use of the SVF in entirety has demonstrated potential benefit over fat grafting alone, implementation of immunogenic beads and flow cytometry has allowed for investigation into specific populations of fibroblasts within the SVF. Recent interest has emerged in characterization of specific ADSC subpopulations within the SVF and the associated benefits of each in RIF treatment.
ADSC subpopulations
As interest in ADSCs has expanded, current research has focused on the identification of subpopulations of ADSCs with various immunophenotypic markers and to define the specific physiologic role of each individual population (Table 1). While research has been done on a multitude of markers, we focus only on those particularly relevant to wound healing and radiation fibrosis below.
General information and potential of notable adipose-derived stromal cell subpopulations
Antifibrotic CD74+
CD74 is a cell surface receptor for macrophage inhibitory factor and has been found to suppress production of amyloid beta and interact with the class II major histocompatibility complex. It also appears on cells showing antifibrotic qualities in tissues and acts as a receptor for cytokine macrophage migration inhibitory factors on the surface of cells. 9,76
CD74+ ADSCs have been shown to reduce skin stiffness, dermal thickness, and collagen production of damaged adipose tissue by increasing levels of hepatocyte growth factor (HGF), fibroblast growth factor 2 (FGF2), and TGF-β3 and decreasing the levels of TGF-β1 in mice. 77 The changing levels of these growth factors allow for there to be a decrease in the production of multiple types of collagen, such as procollagen type 1, collagen type 1, and collagen type 2, as well as a decrease in fibrotic fibroblasts. 77 These qualities of CD74+ ASDCs demonstrate an antifibrotic role that has been observed both in vitro and in vivo. 77
Vasculogenic CD146+
Recent evidence has shown CD146, also known as melanoma cell adhesion molecule, to be a cell-surface receptor that binds with miscellaneous ligands, growth factors, and extracellular matrices. 78 CD146+ ADSCs have been found to improve RIF by increasing vascularization and decreasing dermal thickness and collagen production. 79 The antifibrotic effects of CD146+ ADSCs are modulated by an increase in VEGF, angiopoietin-1, and FGF2 and a decrease in TGF-β1 expression. 79 –81 Fat grafts augmented with CD146+ ADSCs also demonstrated improved graft survival and retention, likely mediated by their increased vascularity. 80,81
Adipogenic BMPR1A +s
Bone morphogenetic protein receptor 1A (BMPR1A) is a protein receptor that specifically binds ligands from the TGF-β superfamily, transmitting signals between the cell membrane and then nucleus. 82 BMPR1A+ ADSCs have been shown to decrease RIF by increasing levels of adipogenic growth factors in fat grafts, which in turn helps with volume retention of the fat graft. 83 In vivo and in vitro studies have demonstrated that when BMPR1A+ ADSCs are activated by the binding of bone morphogenic protein 2 (BMP2), peroxisome proliferator-activated receptor gamma (PPAR-γ) protein expression is subsequently upregulated, which leads to increased adipogenesis. 84
Angiogenic CD248+
CD248, also known as endosialin, is a transmembrane receptor that binds to ligands, including fibronectin, type I collagen, and type IV collagen. 85 CD248+ ADSCs also serve an angiogenic role within wounded tissue. In vivo fat grafting in a mouse model of CD248+ ADSCs resulted in increased expression of several angiogenic genes, including VEGF, FGF2, platelet derived growth factor alpha (PDGFRA), and PDGFRB, and HGF. 86 CD248+ ADSCs have been linked to faster wound healing and increased vascularization thought to be mediated by decreased vessel regression toward the end of the wound healing process. 86 While the vasculogenic effects of CD248+ ADSCs have been observed both in vivo and in vitro, the characterization of CD248+ ADSCs is still widely debated. Some believe CD248 to be a marker for tumor related fibroblasts, while others believe CD248 to be a marker for stromal fibroblasts. 86
Cellular Mechanisms underlying regenerative potential of ADSCs
Despite clinical evidence of their therapeutic potential, the mechanisms underlying the regenerative effect of ADSCs on radiated skin remain unclear. Initial theories suggested that ADSCs simply function by replacing the native irradiated senescent adipose stromal cell population; however, further research has uncovered various alternative pathways that may contribute synergistically to their therapeutic actions. 8,87 These functions include the ability of ADSCs to transdifferentiate, alter the wound environment through paracrine signaling, and to recruit other host stromal cells to the area of injury. Accordingly, two main hypotheses for the mechanism of ADSCs in fat grafting have emerged: the first is that ADSCs differentiate into adipocytes, and the second is that the vascularization and tissue remodeling of fat and surrounding soft tissue are driven by cytokines and growth factors, which are delivered through the paracrine system. 88
Adipocyte differentiation
Given the multipotent nature of ADSCs, some of their differentiation into de novo adipocytes and endothelial cells likely facilitate their effect on ameliorating cutaneous radiation injury. 87,89 The ability of ADSCs to differentiate into mature adipocytes has been demonstrated in numerous cell-tracking studies. 90 –92 Restoring cutaneous fat may be a potential way through which ADSCs serve to reverse dermal RIF. Recent studies have demonstrated that mature adipocytes can exert both an antifibrotic effect, through the activation of PPARγ, and can promote regeneration. 93,94
Second, differentiation of ADSCs into endothelial cells has also been verifiably demonstrated in numerous studies. 95 –97 Notably, in a rat model of radiation injury, injection of DiI-labeled ADSC into a radiation ulcer resulted in the formation of hybrid neovasculature composed of both host and ADSC-derived endothelial cells. 98 Furthermore, other studies have shown that ADSCs can also take on a pericyte-like role, stabilizing newly formed vessels to further support angiogenesis. 99
Given that ischemia secondary to hypovascularity mediates both radiation injury and fat graft necrosis, as well as the demonstrated benefits of augmenting angiogenesis to improve RIF in skin, the direct promotion of angiogenesis by ADSCs likely plays a major therapeutic role. 3,61,100
Paracrine signaling
An alternative mechanism through which ADSCs are postulated to function is through paracrine signaling. The secretome of ADSCs has been a subject of extensive research and has uncovered various growth factors and cytokines that are thought to catalyze their therapeutic actions. 101
The most extensively studied are their angiogenic, anti-inflammatory, and antifibrotic functions, although many others have also been identified. VEGF, HGF, basic fibroblast growth factor (bFGF), and angiopoietin-1 are all angiogenic growth factors known to be expressed by ADSCs. 80,102 –104 These growth factors can stimulate both host endothelial cells, as well as grafted endothelial cells, from the SVF to proliferate and contribute to capillary tube formation.
It has been shown that the introduction of ADSCs into an ischemic environment, such as a newly transplanted fat graft, results in the secretion of VEGF. 87 A study by Garza et al demonstrated increased expression of VEGF in ADSCs extracted from fat grafts in mice, which correlated with increased vascularity. 88
The antifibrotic function of ADSCs is thought to result from modulation of nearby fibroblasts. Studies have demonstrated reduced expression of TGF-β1 and collagen in dermal fibroblasts cocultured with ADSC, findings which have further been validated in animal studies of radiation fibrosis. 77,104 Reduced expression of TGF-β1 may result in lower chance of fibroblast activation to myofibroblasts. The consequent absence of intercellular contractile forces and excessive ECM deposition may contribute to the decrease in skin fibrosis observed clinically in patients with RIF who are treated with ADSCs. 60
Finally, ADSCs can also serve an anti-inflammatory role through their expression of immunosuppressive cytokines, including IL-10 and prostaglandin E2, and modulation of T and B cell activation. 105 –107 Furthermore, given the oxidative mechanism of radiation-induced soft tissue damage, ADSCs could further reduce inflammation by mitigating ROS generation; studies have shown a capacity to upregulate superoxide dismutase and glutathione reductase in cocultured dermal fibroblasts. 108 In all, ADSCs appear to target many of the pathophysiologic mechanisms of radiation damage through their varied paracrine activities.
Recruitment of host stem cells
A final potential therapeutic pathway of ADSCs is their recruitment of host stem cells to the site of RIF by increasing the release of stromal derived factor-1. 109,110 The release of this homing chemokine is capable of attracting a variety of stem cells, ranging from ADSCs in nearby skin to mesenchymal stem cells from distant bone marrow, to the site of injury. 111,112 Once honed to the site of injury, these distant stem cells can locally exert the therapeutic roles outlined above to the sequelae of RIF.
In summary, ADSCs likely potentiate their therapeutic and regenerative effects on irradiated tissues through a synergistic combination of differentiation, paracrine signaling, and host stem cell recruitment to increase adipogenesis and angiogenesis, minimize fibrosis, and attenuate inflammation in radiation-damaged soft tissues.
Commercial availability and potential
Autologous and allogenic ADSC therapies have generated interest on the regenerative medicine commercial market in recent years. Their attributes of pluripotency, low immunogenicity, and high availability (due to esthetic liposuction procedures) contribute to their therapeutic promise and profitability potential. 113 Interest in the clinical utility of ADSCs extends far beyond the scope of RIF, as recent studies have demonstrated possible therapeutic use in bone regeneration, autoimmune diseases, and neurodegenerative processes. 107,114,115
Numerous and diverse preclinical and clinical trials are currently underway to assess the efficacy of ADSC treatment in diseases such as systemic sclerosis, chronic kidney disease, neurological and degenerative diseases, atherothrombotic diseases, and more. At this point in time, many preclinical investigations have been done in animal models and those done in humans have been limited by sample size. Clinical trials related to ADSC applications are predominantly in phases I and II rather than III and IV. 116
While interest in bringing ADSCs to the commercial market and clinical practice appears abundant, broad availability of ADSCs commercially is yet to come to fruition. Lack of standardization in the harvesting, processing, and storage of these cells has been identified as a contributing factor. In addition, significant adverse effects of SVF therapy have been described, such as macular degeneration, which has increased emphasis on patient safety and oversight as these therapies become available. 113,117
Future directions of cell-based therapy to reverse fibrosis in irradiated tissue
Recent advances in fat graft survival and viability have focused on cell-based therapies utilizing adipocytes or ADSCs. Emerging techniques to augment these cell-based therapies to improve their efficacy have created exciting potential growth in RIF treatment and in the field of wound healing and tissue regeneration more broadly. One of these techniques utilizes platelet-rich plasma (PRP), a popular clinical therapy within orthopedics, reconstructive and esthetic surgery, and dermatology, to enrich adipocytes and ADSC populations.
Platelets are a well-known component of the hematologic system that remain inactive in their native state. However, when platelets encounter damaged endothelial cells within injured tissue, they are activated to help create a thrombus and prevent further damage to the injured tissue and initiate the first phase of wound healing: hemostasis. 11 These activated platelets release a plethora of growth factors and cytokines to facilitate tissue repair by improving surrounding cells' resistance to oxidative damage while simultaneously promoting angiogenesis. 118 Not only does PRP improve adipocyte survival but also it has been shown to improve ADSC survival and differentiation. 119 –122
Epitranscriptomics is a blossoming field within basic science research to modify RNA expressed by cells, and applications with regeneration secondary to fat grafting is not exempt. Most RNA modifications occur to alter the two main factors affecting adipocyte and fat graft viability that was discussed above: inflammation and vascularity. Yu et al transfected human ADSCs with VEGF modified mRNA (modRNA) and were able to increase levels of cellular proliferation and pro-angiogenesis in vitro and in vivo. 123
Modification of N6-methyladenosine (m6A), N6-adenosine methyltransferases (Mettl3), fat mass and obesity-associated gene (FTO), and alpha ketoglutarate beta homolog 5 (Alkbh5) mRNA within ADSCs has been the focus of numerous ground-breaking studies. Lin et al showed that upregulation of Mettl3 resulted in increased vascular smooth muscle differentiation, and silencing of Mettl3 decreased expression of VEGF, TGF-β1, and granulocyte-macrophage colony-stimulating factor. 124
FTO has been shown to regulate the inclusion of Runt-related transcription factor 1 (RUNX1T1), an adipocyte regulatory factor, and suppressed differentiation of preadipocytes. 125,126 Wu et al demonstrated that FTO regulated cell cycle progression of adipocytes by affecting expression of cyclin A2 (CCNA2) and cyclin dependent kinase 2. 127 Furthermore, Zhang et al showed that PPARγ, a potent and well-studied adipogenic differentiating factor, is a downstream target of FTO during adipogenesis. 128
M6A deletion was found to inhibit adipogenesis by uncoupling protein-2 (UCP2) but, conversely, promoted adipogenesis in the presence of patatin-like phospholipase domain containing 2 (PNPLA2). 129 Most recently, CCAAT/enhancer-binding protein zeta (C/EBPZ) expression inhibits preadipocyte differentiation and increases preadipocyte proliferation, potentially identifying a novel negative regulator of adipogenesis.
Finally, as recent effort to elucidate the specific mechanisms of ADSC subpopulations progresses, future directions of cell-based therapies may be more tailored. With interest growing in the discovery and characterization of ADSC subpopulations, future research may continue to reveal previously undescribed populations of ADSCs.
As technology advances, these novel techniques will drive the identification of new ADSC subpopulations, better define the physiologic roles of current ADSC populations, and develop additional modulating factors to improve the viability and functionality of these ADSC populations. The exciting potential of these stem cell populations and the ability to delve deeper into the transcriptomic modulation of these populations could revolutionize the field of regenerative medicine, wound healing, and tissue engineering to improve the lives of millions of patients worldwide dealing with RIF and any other fibroproliferative disease.
SUMMARY
As radiation therapy has emerged as an effective means of treating cancer, so, too, has associated complications. The most common of these is RIF, which is associated with numerous undesirable clinical features, such as decreased skin perfusion, dermal thickening, and poor wound healing. Fat grafting has gained popularity as a therapeutic approach for preventing and treating these sequelae, after studies reported improved functional and esthetic clinical outcomes associated with its application in RIF. However, while promising outcomes have been reported, radiated skin and soft tissue provides a relatively hostile host site for a graft given decreased vascularity and poor fat graft retention in the RIF-affected area.
Various modalities of improving upon fat grafting as a therapeutic approach have been investigated and reported, including preconditioning the tissue with DFO, supplementing the graft with vitamin E, and using serial fat transfer techniques. Perhaps the greatest interest has been taken in reported use of contents of the SVF, including ADSCs, to augment fat grafts. These techniques have been reported to increase fat graft volume retention, decrease fat graft necrosis, increase angiogenesis, decrease collagen density, decrease dermal thickness, among other clinical benefits.
The cellular mechanisms underlying these observed benefits have not yet been fully elucidated but are thought to be related to the ability of ADSCs to differentiate into various cell lines, act through paracrine signaling pathways, and recruit host stem cells. As this area of research continues to develop, expected areas of further exploration include fat graft enrichment with PRP, incorporation of epitranscriptomics, and increased understanding of the specific roles played by specific ADSC subpopulations.
TAKE-HOME MESSAGES
One half of cancer patients receive radiation therapy as part of their treatment, the most common complication of which is RIF.
RIF results in changes to the skin that can create functional limitations, cause esthetic concerns, and cause increased surgical complications.
Fat-grafting emerged as a possible therapeutic option for RIF in 2007 when Rigotti et al reported symptomatic and esthetic improvements in radiated skin following its application in the affected area.
Various improvements upon this therapy have been proposed, the most notable of which is augmenting the fat graft with ADSCs, which are multipotent progenitor cells.
Augmentation of a fat graft with ADSCs has been shown to improve clinical outcomes, increase perfusion, improve structural quality, decrease dermal thickness, and provide additional positive benefits in the setting of radiation-induced skin fibrosis.
Several subpopulations of ADSCs have been identified and associated with specific therapeutic benefits, providing promise for increased specificity in the future of this field.
Footnotes
AUTHORs' CONTRIBUTION
C.E.B.: Writing-original draft and review/editing (equal); visualization (lead). D.A.: Writing-original draft and review/editing (equal). H.A.L.: Writing-original draft and review/editing (equal). A.A.C.: Writing-original draft and review/editing (supporting). M.G.: Writing-review and editing (supporting). J.L.G.: Writing- review and editing (supporting). A.C.C.: Writing-review and editing (supporting). J.B.L.P.: Writing-review and editing (supporting). M.A.D. Jr.: Writing-review and editing (supporting). M.T.L.: Supervision (equal); conceptualization (equal). D.C.W.: Supervision (equal); conceptualization (equal); writing-review and editing (equal).
ACKNOWLEDGMENTS AND FUNDING SOURCES
Derrick C. Wan was supported by NIH DE027346. Michael T. Longaker was supported by the NIH grant R01 GM 116892, RO1 GM 136659, Gunn/Olivier Research Fund, Stinehart-Reed Fund, and the NIH grant U01 HL099776.
AUTHOR DISCLOSURE AND GHOSTWRITING
No competing financial interests exist. The content of this article was expressly written by the authors listed. No ghostwriters were used to write this article.
ABOUT THE AUTHORS