
Abstract
Objective:
A few studies have focused on the quality of life (QoL) of patients with chronic non-responsive pressure skin ulcers. The aim of this study was to assess how correct treatment (advanced wound care [AWC] dressings alone or vacuum assisted closure [VAC] therapy alone) changes the QoL of these patients.
Approach:
One hundred six patients with chronic non-responsive pressure skin ulcers, who had previously used galenic dressings, applied without proper therapeutic indication, were included in this study. We administered the WOUND-Q, at time 0 and after 1 month of appropriate therapy, to assess patient-reported outcome measures. Group 1 consisted of 30 patients treated with advanced dressings, Group 2: 22 patients treated with VAC therapy, and Group 3: 30 patients continuing conventional galenic dressings (Control group). Statistical analysis allowed us to analyze QoL changes over time and to compare WOUND-Q Group 1 and 2 deltas with those of Group 3. The study followed the STROBE statement.
Results and Innovation:
In all the scales evaluated (Assessment, Drainage, Smell, Life impact, Psychological, Social, Sleep and Dressing), there were significant improvements in mean values for Groups 1 and 2. Kruskal-Wallis tests with Dunn's multiple-comparisons tests and Brown-Forsythe and Welch Analysis of Variance tests demonstrated significant differences between deltas of Group 1 and Group 2 compared with those of Group 3 for most scales analyzed.
Conclusions:
Administration of the WOUND-Q demonstrated that the application of advanced dressings alone or VAC therapy alone positively affects the QoL of patients with chronic nonresponsive pressure wounds, in comparison with galenic dressings alone. The WOUND-Q has been shown to be a valid tool in studying changes in QoL of these patients.

INTRODUCTION
A skin ulcer is defined as a loss of skin tissue that is not prone to spontaneous healing. A wound that has failed to heal within 4 weeks is defined as chronic. 1 It can involve underlying soft tissues and might worsen a patient's quality of life (QoL) to a variable degree depending on its stage. 2
The prevalence of skin ulceration is very high: in the United States, over 6.5 million people suffer from this condition. 3 The trend is increasing due to an aging population and the prevalence of comorbidities and risk factors (smoking, atherosclerosis and obesity) in the general population. 4 About 20% of ulcers remain unhealed after 2 years. This percentage drops to 8% when considering them after 5 years. 5
An ulcer approach starts with an accurate multidimensional and multidisciplinary patient evaluation among medical specialists; this is essential to achieve optimal treatment goals. The etiology of skin ulcers can be heterogeneous and include: vascular diseases (arterial, venous or both), neoplastic conditions, traumatic events, continuous pressure forces, etc. 6
A correct diagnostic flow chart can guide physicians toward the exact etiological diagnosis. 7 An ulcer approach depends on the patient's health status, the wound etiology and on other features such as the wound depth, margins, areas of necrosis or fibrin, bacterial infection, and exudate (type and quantity). 8 Local treatments may include conventional dressings, surgical techniques (skin grafts, flaps), 9 advanced wound care (AWC) dressings such as alginates, hydrocolloids, semipermeable films, hydro polymeric polyurethane foams, hydrogels, resorbable biocompatible dressings, etc., 10 vacuum assisted closure (VAC) therapy, 11 bioengineering, and regenerative medicine techniques (growth factors and adipose-derived stem cells). 12 –15
CLINICAL PROBLEM ADDRESSED
Chronic wounds are a challenging problem for both patients and caregivers. 1 The suffering experience includes both physical and psychological aspects. Skin ulcers can cause pain, unpleasant odors, and reduced mobility. They can also lead to social isolation and further impairments in everyday life activities. 16 There can be a financial impact on the patients due to the price of dressings, medical supplies, and frequent trips to the hospital's outpatient clinic. 10
Skin ulcers are the expression of an underlying condition and they do not tend to heal until the underlying cause is properly addressed. Some diseases, such as immunological conditions (e.g., vasculitis), vascular diseases, diabetes mellitus etc., can rarely be eradicated. Therefore, even if these conditions are controlled, it is not possible to guarantee the patient disease-free days.
Consequently, in some cases even with the best dressings, ulcers tend not to heal and their management can only have a palliative effect. Health-related quality of life (HR-QoL) evaluation can help the management of chronic wounds, reporting the patient's perspective of the disease and its treatment. 17 –20 Many studies in literature investigated the etiology, staging, and treatment of skin ulcers. Only a few of them focused their attention on the QoL of those patients who are unlikely to heal. The aim of this study was to assess how correct treatment changes the QoL of patients with chronic non-responsive pressure skin ulcers.
As the treatment was palliative in those patients, we did not want to consider the degree of ulcer improvement, rather the impact of the AWC dressings alone and VAC therapy alone, according to the skin ulcer treatment guidelines, 21 –24 on QoL. Most patient-reported outcome measures (PROMs) questionnaires focus on a specific type of wound. 25 –32 We chose to use the WOUND-Q questionnaire to gain an objective assessment of QoL improvements by breaking down the physicians' subjective interpretations evaluating PROMs in chronic non-responsive pressure ulcer patients.
Wound-Q: Italian translation
The WOUND-Q questionnaire is a scientifically validated multidimensional questionnaire that is beneficial in describing the QoL of patients suffering from any type of wound independent of anatomical location and being suitable for clinical trials, economic evaluations, and clinical practice.
17,33
–35
WOUND-Q, being a PROMs-based test,
34
reports the status of a patient's health condition directly from a patient's point of view without any other interpretation.
36,37
The questionnaire investigates four domains: Wound characteristics and wound perception; HR-QoL; Experience of care; Wound treatment.
Wound characteristics and perception investigate aspects including bleeding, odors, holes, swelling, edges, color, drainage, pain, depth, and size. HR-QoL impact investigation focuses on: relationships, social life, ability to be independent, ability to move, sleep and psychological aspects. The relationship with the wound care team, office staff and general satisfaction with dressings can also be studied. 38 Each domain has multiple scales also functioning independently. 39 The questionnaire is composed of 13 scales, including a total of 111 questions, each with 4 possible answers. Figure 1 shows the domains investigated and the scales composing the questionnaire.
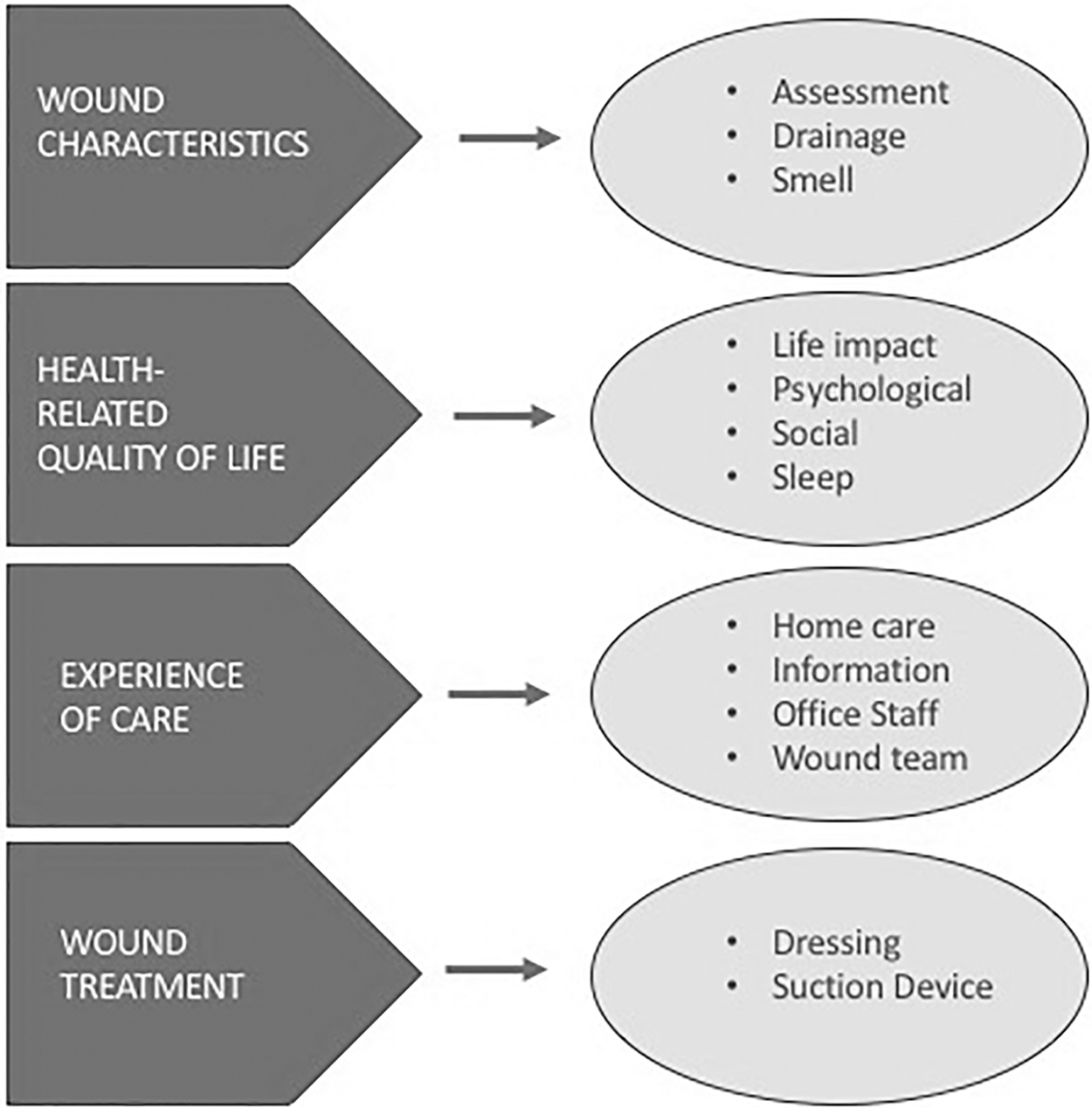
The WOUND-Q scales and domains investigated.
As there was no WOUND-Q Italian version yet, it was necessary to translate and validate WOUND-Q into Italian. We began the validation process following each step established by the questionnaire's creators. In the first step, two separate Italian translations (forward translation) of the questions and answers were performed by two fluent English-speaking native Italian speakers. The second step required mediation of the two Italian translations to create a single version. A reverse translation (back translation from Italian to English) was performed by a fluent Italian-speaking native-English professional translator who had not taken part in the previous translation processes. The Q-Portfolio team then provided a review of the reverse translation. Only a few language corrections were made during the back-translation review. The last step required the administration of the questionnaire to at least 10 people to confirm that the Italian version was fully understood. Following the questionnaire administrations, no grammatical misunderstandings were reported. The Q-Portfolio team approved the Italian version of the WOUND-Q questionnaire and granted us permission to use the test for this observational prospective study.
MATERIALS AND METHODS
One hundred six consecutive patients older than 18 years of age suffering from non-responsive, for at least 40 days to conventional treatments with grease gauzes and antiseptics (Povidone-iodine or hydrogen peroxide), chronic pressure skin ulcers, who had never used advanced dressings, afferent to our Wound Care Unit were enrolled in this prospective study.
We excluded: patients who were not mentally competent, patients with uncompensated diseases or those who needed further treatments (e.g.: patients with uncompensated mellitus diabetes, patients who were candidates for angioplasty, etc.), patients who had failed to complete at least one administered test, and patients who had not followed instructions as directed by wound care center staff.
We decided to exclude all of these patients because all of the conditions cited earlier could have led to bias in the interpretation of the data. None of these patients had previously been followed up in a specialized wound care center, but they had used conventional dressings to manage chronic ulcers without achieving any visible improvement for at least 40 days before the first visit. No concomitant adjunctive therapies such as Hyperbaric Oxygen or HBO were performed. At time 0, each patient was examined by a plastic surgeon and a wound care center nurse.
A thorough medical history, focused on highlighting pathologies related to ulcer formation, was conducted: immobility, diabetes, vasculitis, lymph stasis, venous insufficiency, etc. All patients in whom the underlying diseases were in a compensatory stage and did not require pharmacological and surgical treatments to compensate for the disease were included in the study.
In cases of suspected infection, a culture examination was performed. If this was positive, antibiotic therapy was prescribed by our wound care unit infectious disease specialist if appropriate. If necrosis was present, debridement was performed on an outpatient basis (if debridement was not feasible on an outpatient basis, the patient was hospitalized).
After debridement, according to the characteristics of the ulcer, the most suitable dressing was applied according to the international reference guidelines. We administered the Italian version of WOUND-Q in a calm environment in paper form at time 0 (the day on which the patients made their first visit to our wound care clinic and were prescribed the proper application of an advanced dressing or VAC therapy) and at time 30 (after 1 month of appropriate therapy).
Dressings used up to this point were discontinued. The control group continued to use galenic dressings. At both times of administration, standardized digital photos with a centimetric reference were taken. Digital photos were then exported in software (ImageJ), which allowed the calculation of areas with a global pixel-centimeters conversion. Anonymity of the test was ensured, assigning each patient a code. Each patient signed a written consent form and was aware of this clinical investigation.
Two patients died, 6 patients were excluded due to lack of follow-up, and 16 patients presented at least 1 exclusion criterion during the study.
A total of 82 patients with chronic non-responsive pressure ulcers completed the study answering all the questions on the test (Fig. 2). The first 52 patients who consecutively flocked to our Wound Care Unit were placed in the experimental groups, and the next ones in the control group. Patients were divided into three groups depending on the treatment they were subjected to, according to the guidelines:
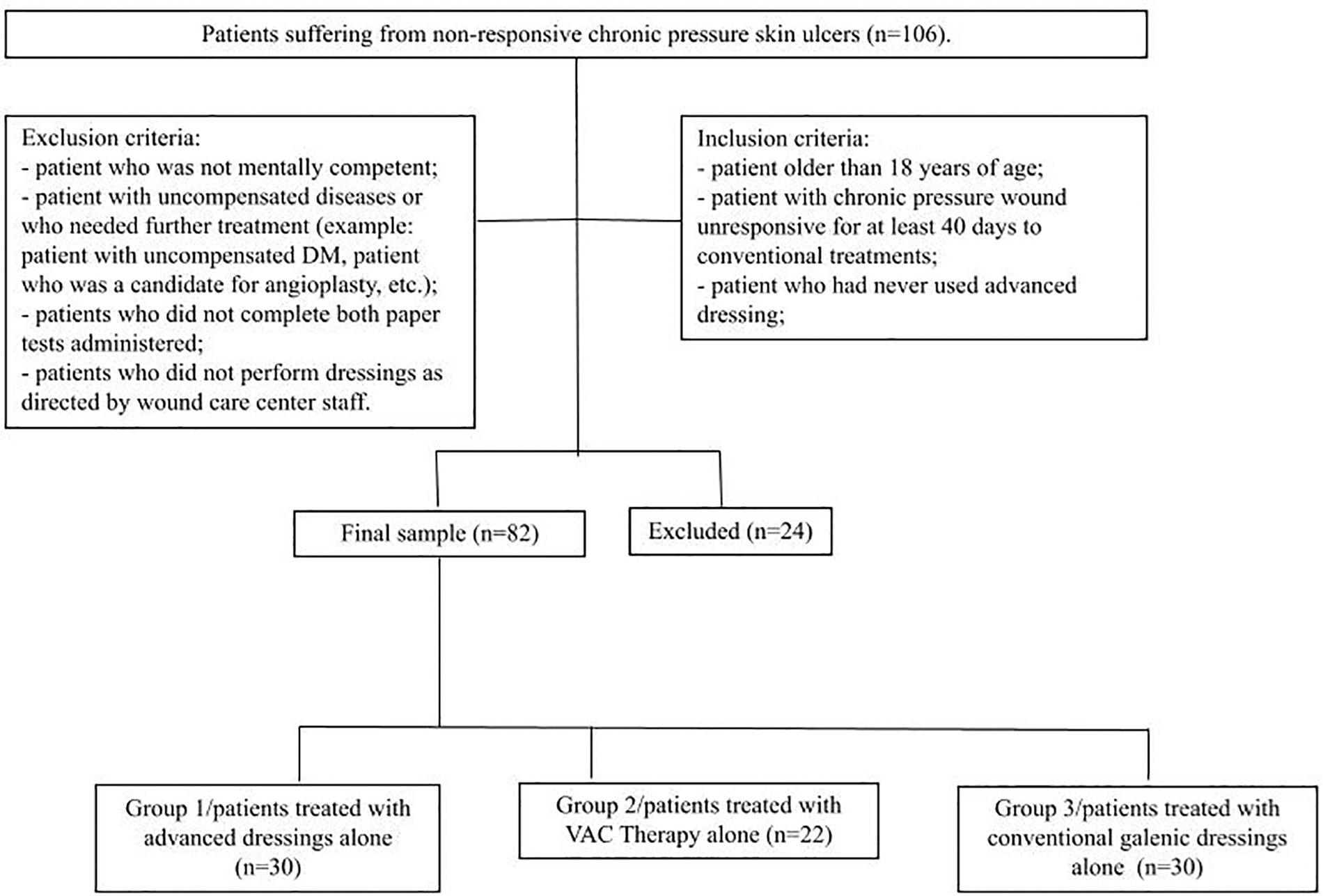
Flow diagram describing patient enrollment. DM, diabetes mellitus; VAC, vacuum assisted closure.
Group 1: 30 patients treated with advanced dressings alone (after detersion, patients with grade 3 and 4 ulcers according to NPUAP were medicated with a gelling fiber dressing with Hydrolock® technology covered by polyurethane foam, as a secondary dressing, and covered with sterile gauze);
Group 2: 22 patients treated with VAC Therapy alone;
Group 3: 30 patients still treated with conventional galenic dressings (Control group).
We categorized patients according to sociodemographic characteristics such as sex, age, marital status, occupation, and education and according to existing medical characteristics and novel medical events. Nine questions on the questionnaire were related exclusively to dressings; only Groups 1 and 3 were required to answer these questions.
Nine questions were exclusively related to the use of suction devices, with only Group 2 required to answer. Each question measured the degree of severity with a number. Each scale, composed of different questions, led to a total score for each patient. Each total score was converted using a conversion RASCH scale table provided by the Q-Portfolio team. This conversion linearizes the intervals of values into a score that ranges from 0 (worst) to 100 (best). 40,41
The data were collected in a Microsoft Excel 2007 worksheet. Electronic laboratory notebook was not used. Data were exported to statistical software (Prism-GraphPad) for the descriptive analyses. In every scale, the sum of mean scores, obtained at time 0 and after 1 month of treatment, were evaluated for each group separately to assess their variations over time.
The normal distribution of the sample was evaluated according to the Shapiro-Wilk test. Depending on the gaussian distribution of values, Paired t-test or Wilcoxon matched-paired test were performed to detect any significance of variations over time within each group. Only variations with p < 0.05 were considered significant. Delta values of each scale were calculated for each group.
Kruskal-Wallis tests with Dunn's multiple-comparisons tests and Brown-Forsythe and Welch Analysis of Variance (ANOVA) tests enabled the comparison of deltas for each scale of Group 1 and Group 2 with deltas of Group 3, which represents the control group, assessing the possible significance of variations over time. As analyzing delta over time for “Information,” “Home care,” “Wound staff,” “Office staff” within the three groups was not our aim, we excluded these scales from our comparison analysis. Even if just 23 patients in Group 1, 11 in Group 2, and 25 in Group 3 were treated by a home care nurse, we decided to report all data derived by administration of the Home care nurse scale.
Unpaired t-test with Welch's correction was used to assess any significant differences between Group 1 and Group 3 deltas in the “Dressing” scale. The study was conducted in accordance with local regulations, international standards of “Good Clinical Practice” in the European Community, and the principles of the Declaration of Helsinki. This study followed the STROBE statement.
RESULTS
In all three groups, there was a prevalence of females (59.8%) and of patients older than 60 years (71.9%). These data are in line with the trends described by AIUC in a 2016 Italian analysis. 42 Most of the patients were single or divorced (62.2%), unemployed (74.4%) and had a primary education only (65.8%). The majority of the patients had a body mass index lower than 18.5.
Table 1 shows sociodemographic characteristics of patients belonging to Group 1 (treated with advanced dressings alone), Group 2 (treated with VAC therapy alone), and Group 3 (treated with galenic dressings alone). The patients' medical characteristics and novel medical events over follow-up time are shown in Table 2.
Distribution of patients treated with the application of advanced dressings alone (Group 1), vacuum assisted closure therapy alone (Group 2), and galenic classic dressings alone (Group 3), according to sociodemographic characteristics
BMI, body mass index.
Patients' medical characteristics and novel medical events during the follow-up time
MRSA, methicillin-resistant Staphylococcus aureus.
Table 3 illustrates pre- and post-mean values for all the three groups. The same table shows statistical significance of changes over time calculated through Paired t-test or Wilcoxon matched-paired test. Higher WOUND-Q scores reflected better outcomes. On average, all mean values tended to increase in Groups 1 and 2. In all the scales evaluated (Assessment, Drainage, Smell, Life impact, Psychological, Social, Sleep and Dressing), there were improvements in mean values for Groups 1 and 2. These improvements were statistically significant (p < 0.05).
WOUND-Q means values and changes at 1 month
“*” Indicates the significance of variations.
QoL, quality of life.
In Group 3, values tended to rise in Assessment, Drainage, Psychological state, Sleep and Social life. Regarding Group 3, improvements in mean values were statistically significant in the Psychological scale only. Regarding the Dressing scale, on average, mean values tended to rise significantly in Group 1 (from 52.47 ± 9.71 to 79.83 ± 12.78 with p < 0.05), whereas they decreased in Group 3 (from 51.67 ± 9.42 to 49.23 ± 17.80 with p > 0.05).
As only 1 month mean values were reported, no comparison could be performed on the Suction device scale. On average, the Group 2 patients expressed a positive opinion about VAC therapy: 67.73 ± 14.86 on a RASCH scale ranging from 0 to 100. Kruskal-Wallis tests with Dunn's multiple-comparisons tests and Brown-Forsythe and Welch ANOVA tests enabled the comparison of deltas for each scale of Group 1 and Group 2 with deltas of Group 3.
Only the comparison of the Psychosocial scale deltas with those of Group 3 were not significant to either Group 1 or Group 2. The comparison of the Sleep scale deltas with those of Group 3 was not significant for Group 2. Regarding the Dressing scale deltas, the unpaired test with Welch's correction showed a statistical significance between Group 1 and Group 3. Statistical significance of comparison of deltas (pre-post) between Groups 1 and 3 and between Groups 2 and 3 for each scale is illustrated in Table 4.
The statistical significance of comparison of the deltas (pre-post) between groups 1 and 3 and between groups 2 and 3 for each scale
“–” Indicates that no comparison can be made.
“*” Indicates significant data.
DISCUSSION
Some patients with chronic nonresponsive pressure skin ulcers are aware that they may never heal. What matters most in these cases, beyond the improvement of the wound (if possible), is the improvement of the QoL. So, in our experience, in approaching these patients, the QoL becomes a priority. The World Health Organization defines “Quality of life” as “an individual perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns.” 43
These outcomes regarding QoL are unmeasurable except through specific questionnaires such as the WOUND-Q. Our administration of this questionnaire to these patients showed that the application of advanced dressings alone or VAC therapy alone positively improves the QoL, from patients' point of view, in comparison with continuing to use galenic dressings alone.
This is demonstrated by our data derived from a comparison of WOUND-Q deltas between Group 1 and Group 2 with those of Group 3 (control group-galenic dressings). As on average patients of Group 3 perceived a worsening in odor control, overall QoL, and given that the improvements achieved with VAC therapy alone and advanced dressings alone in terms of exudate and odor control, QoL, sleep, and impact on social life, are better than in the control group, we suggest their use when dressing these types of patients.
We also observed an improvement in Psychological scale data in Group 3, but this can be assumed to be due to the understanding, the care, and the frequency and quality of dressings gained by patients, who had not previously been cared for by specialists in our wound care center.
This is in line with data expressed by patients in the Office staff scale; they rise significantly over time in all the three groups. Since these data are derived from PROMs, they are not based on chemical or physical experiments, but based on patients' feelings. They represent patients' opinions on their QoL only. This may imply that the patients themselves, feeling the secretions, smell, and wound general improvement, may feel more confident.
This could also help their personal relationships. Patients also have fewer problems in falling asleep, reduced night awakenings, and less difficulty in finding a comfortable position in which to fall asleep. This should be beneficial not only to the patients physically, but also to their psychological state. The strengths of this study are the use of a validated questionnaire (WOUND-Q) and the distribution of patients in comparable samples.
LIMITATIONS
Our study is limited to a small sample and to a 1-month follow-up. This study can be interpreted as a preliminary study on QoL of these patients; further studies with a long-term follow-up are needed. Despite this, we believe that our data also provide a benchmark for comparison with other researchers' results.
KEY FINDINGS
Administration of the WOUND-Q demonstrated that the application of advanced dressings alone or VAC therapy alone positively affects the QoL of patients with chronic nonresponsive pressure wounds, in comparison with galenic dressings alone.
The WOUND-Q has been shown to be a valid tool in studying changes in QoL of these patients.
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
The authors have no financial interest to declare in relation to the content of this article. There were no funding sources. The authors declare no conflict of interest.
AUTHOR DISCLOSURE AND GHOSTWRITING
The authors declare that no competing financial interests exist. No ghostwriters were used to write this article.
ABOUT THE AUTHORS