
Abstract
Significance:
With the increasing diabetic population worldwide, diabetic foot ulcers (DFUs) are a significant concern. This study aimed to compare the efficacy of skin substitutes, biomaterials, and topical agents with standard care.
Recent Advances:
A meta-analysis was conducted using Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. PubMed, EMBASE, and Web of Science were searched using the following keywords: diabetes mellitus AND skin graft OR tissue replacement OR dressing OR drug. Two independent reviewers performed data collection and quality assessment of the eligible studies. The primary outcome was the 12- to 16-week healing rates and the secondary outcome was recurrence rates.
Critical Issues:
Thirty-eight randomized controlled trials, including 3,862 patients, were analyzed. The studies exhibited low heterogeneity (τ2 = 0.10) without significant asymmetry (Egger's test, p = 0.8852). After pooling direct and indirect estimates, placenta-based tissue products exhibited the best wound healing probability (p-score = 0.90), followed by skin substitutes with living cells (p-score = 0.70), acellular skin substitutes (p-score = 0.56), and advanced topical dressings (p-score = 0.34) compared with standard of care. The recurrence analysis showed significant improvement in the intervention group compared with the control group (11.21% vs. 15.15%).
Future Directions:
This network meta-analysis provides the relative effectiveness and rank of biomaterials and topical dressings in DFU healing. The results could help clinical decision making.

Scope and Significance
Diabetic foot ulcers (DFUs) are associated with an increased risk of lower-extremity amputation, which significantly impacts the patient's quality of life, health care burden, and life expectancy. Although there is a wide variety of available treatments, the efficacy of these remedies in healing DFUs is still unclear. The aim of this meta-analysis is to understand the effectiveness of the skin substitutes, biogenic materials, and topical agents in treating DFU.
Translational Relevance
Biomaterial wound dressings are diverse, and new products with different mechanisms are discovered every day. Some products keep the native composition of the extracellular matrix and contain growth factors and cytokines that modulate the inflammation process and promote wound healing, whereas some acellular dermal matrix traps and binds the recipient's own cells and growth factors, which support neovascularization and tissue regeneration. The other mechanisms, including antimicrobial, immunomodulation, increase tissue oxygenation, and collagen synthesis had also been described. Understanding the mechanisms of the biomaterials can promote new drug development and design of combination therapy.
Clinical Relevance
The management of DFUs requires multidisciplinary approaches, including patient education, blood glucose control, offloading, revascularization, wound care, and tissue replacement. Surgeons can choose a biomaterial or topical dressing to promote wound healing based on its effectiveness, cost, and patient preferences. Understanding the rank of healing effectiveness among different treatments can support the clinical decision making.
BACKGROUND
DFUs are the most frequent complication of diabetes mellitus. DFUs are defined as ulcerations of the foot associated with neuropathy and/or peripheral arterial disease of the lower limb in patients with diabetes. 1 DFUs are associated with an increased risk of lower-extremity amputation, which significantly impacts the patient's quality of life, health care burden, and life expectancy.
As the diabetic population increases worldwide, health concerns about DFUs increase. The 10th edition of the International Diabetes Federation Diabetes Atlas states that ∼537 million adults (20–79 years old) were living with diabetes in 2021, and 6.3% of people with diabetes will develop at least one foot ulcer. 2 –4
The management modalities for DFU include patient education, blood glucose control, appropriate wound care, mechanical pressure offloading, reduction of infection, wound debridement, use of dermal substitutes or other biogenic materials, and revascularization in patients with simultaneous peripheral artery disease. 2,5
Due to the heterogeneity of DFUs, treatments can be improved even with the currently available comprehensive treatments. Many adjuvant wound therapies and products have been developed, including negative-pressure wound therapy, biologic skin substitutes, advanced dressings, and topical medications. Although the wide variety of available treatments is a positive factor, the efficacy of these products in healing DFUs is unclear, making decisions about treatment strategies challenging.
A Cochrane review 6 showed favorable therapeutic effects of skin grafts and tissue replacements used in conjunction with standard care. However, the low number of eligible studies limited definitive conclusions. Another meta-analysis by Gordon et al. 7 in 2019 demonstrated that biologic skin substitutes were 1.67 times more likely to heal DFUs by 12 weeks compared with standard care. However, these reviews were limited to skin substitutes and did not include topical medications and dressings, which are widely used.
Additionally, comparisons among the products are sparse. Thus, in this meta-analysis, the efficacies of various skin substitutes, biogenic materials, and topical agents for treating DFU were quantitatively analyzed, incorporating the results of multiple randomized controlled trials. In addition, we aimed to compare the interventions with standard care. To facilitate clinical decision making, recurrence rates and the costs for healing patients are also discussed.
METHODS
Research protocol and search question
The search protocol was based on the following PICO question: for patients with DFUs (population of interest), do different skin substitutes and topical agents provide higher wound healing rates compared with standard care or among the products (comparator). The review protocol was developed as indicated by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement guidelines and was registered with PROSPERO (ID: CRD42022338341). PRISMA NMA Checklist was documented in Supplementary Appendix SA1. Only randomized controlled trials were included in the analysis.
Eligible criteria and outcomes
Eligible studies met the following criteria: (1) included patients with DFUs who underwent wound treatments, such as skin substitutes, biogenic materials, topical dressings, or medications; (2) provided detailed information about treatments, such as brand names and materials; (3) interventional studies published in English available in all databases until January 2022; and (4) reported primary outcomes of interest, including wound healing rates at 12–16 weeks and recurrence rates. The recurrence rate was evaluated for subjects whose ulcer healed during the treatment phase and recurrence was observed during the follow-up period. If a study provided wound healing rates at both time points, the one claimed as the primary outcome was chosen.
Relevant exclusion criteria included: (1) single-arm follow-up studies, case reports, case series, reviews, basic science experiments, and animal or cadaver studies; (2) studies that only focused on cost-effectiveness or other perihealed parameters (e.g., amputation rate, recurrence rate); and (3) studies reporting chronic wounds not limited to DFUs. The primary outcome was healing rates. The secondary outcome was recurrence rates after healing.
Search strategy and study selection
We searched PubMed, Embase, The Cochrane Library, and Web of Science for articles in a systematic approach utilizing a combination of keywords and Medical Subject Heading terms adjusted for each database. The whole search query of different databases was provided in Supplementary Appendix SA2. The most recent search was performed in December 2021. Recursive searches using bibliographies of obtained articles were also performed. Two reviewers (Y.L. and A.C.-Y.C.) independently evaluated titles and abstracts for eligibility and full-text evaluation. All disagreements between reviewers were resolved through discussion and a consensus was finalized by a senior plastic surgeon (D.-H.C.).
Data collection and quality assessment
The following data were extracted by the two reviewers: study characteristics (author, year of publication, region of study, data source, study design, period of study), study arms, sample size, proportion of fully healed ulcers, time to complete healing, inclusion criteria, and specific definitions of each treatment arm. Demographic data, including patient age, sex, body mass index (BMI), glycated hemoglobin (HbA1c) level, wound size, and Wagner's degree of the wound, were also obtained. Electronic laboratory notebook was not used.
The risk of bias and study quality were assessed independently by the two reviewers using the Cochrane risk-of-bias tool for randomized trials (RoB 2). GRADE assessment was performed to evaluate confidence in effect estimates. All discrepancies were resolved by discussion (Figs. 1 and 2).

RoB 2 traffic light plot bias assessment for each RCT. RCT, randomized controlled trial.
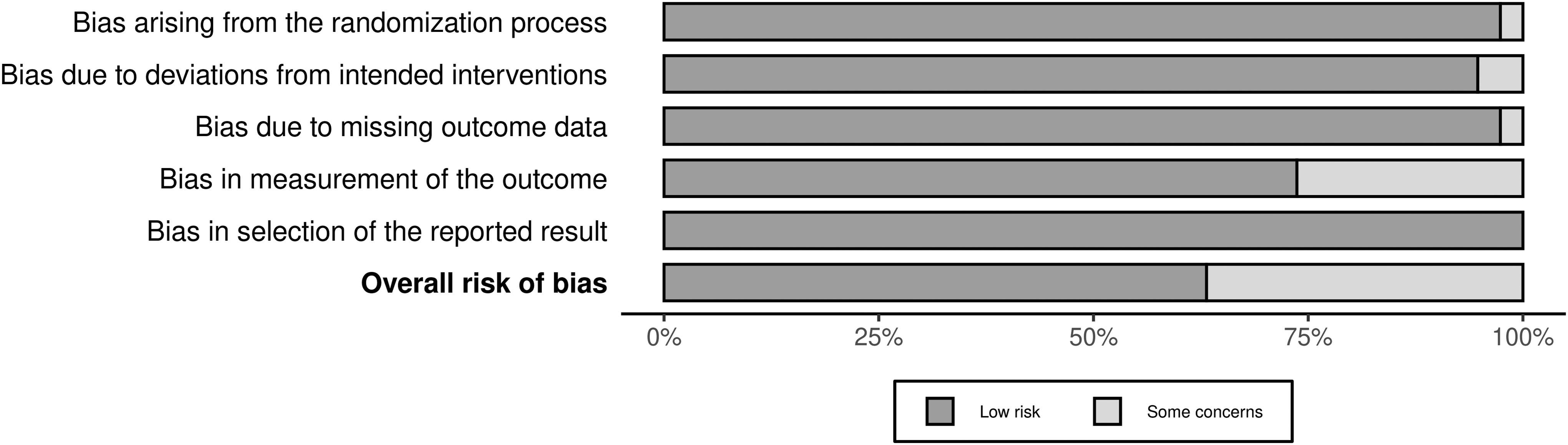
Weighted summary plot of the overall types of bias encountered in the randomized controlled trials.
The Cochrane risk-of-bias tool for randomized trials (RoB 2) consists of five domains: (1) bias arising from the randomization process, (2) bias due to deviations from intended interventions, (3) bias due to missing outcome data, (4) bias in the outcome measurement, and (5) bias in selection of reported results. Each domain is composed of a series of “signaling questions,” and the response options are: yes, probably yes, probably no, no, and no information. After answering the signaling questions a risk-of-bias judgment was reached and one of three levels was assigned to each domain: low risk of bias, some concerns, or high risk of bias. An overall judgment is presented. The plots were converted using Risk-of-bias VISualization (robvis). 8
Classification of the intervention
Due to the lack of consensus in classification systems, biologic skin substitutes were organized both into product brands and broadly into five main groups based on product composition and style, as follows: placental-based tissue products (PBTPs), skin substitutes with living cells (SSLCs) (e.g., Hyalograft, Apligraf®), acellular skin substitutes (ASSs) (e.g., Graftjacket®, Integra), and advanced topical dressings (ATDs). ATDs include a wide range of products, including gels, ointments, and dressings (e.g., Medihoney®, platelet-rich plasma [PRP] gel). Not like aforementioned skin substitutes, ATDs are commonly used daily or weekly for wound care and are surely much cheaper. Any standard care that included conventional dressings, such as paraffin gauze (e.g., Jenolet), foam dressings, hydrogels, and alginate dressings, were categorized as standard of care (SOC). The classification of interventions is shown in Table 1.
Classification of biomaterials and topical medications for diabetic foot ulcer treatment
The product costs per treated wound were estimated according to previous studies and current market information 55,56 : $: 0–1,000 USD; $$: 1,000–2,000 USD; $$$: >2,000 USD.
PRP, platelet-rich plasma.
Statistical analysis and quantitative data analysis
We performed network meta-analysis using the “metafor” (version 3.4-0,
Network meta-analysis models were estimated with a frequentist approach derived from graph theoretical methods. The raw data were transformed into a contrast-based format and used to estimate the odds ratios and 95% confidential interval (CI) for each pairwise comparison. Our pairwise comparison comprised direct and indirect comparisons. Direct comparison indicated that both interventions were compared in a single study, which was also known as a “head-to-head” clinical trial. Indirect comparison indicated that the treatment effect was computed according to trials with the identical comparators (e.g., the treating effect of PBTP vs. ASS from PBTP vs. SOC and ASS vs. SOC studies). 9
These data were utilized to perform a network meta-analysis using random-effects modeling by adding the estimated heterogeneity τ 2 , based on the DerSimonian–Laird estimator, to the variance of each comparison. Direct comparisons were visualized in the form of network graphs, with vertices demonstrating treatments and thickness of edges corresponding to the number of studies. Funnel plots were constructed to assess publication bias and small study effects.
For the binary outcome assessment, we calculated a pooled odds ratio with 95% CI to summarize the relative healed probability of each treatment. The results were visualized using a forest plot with SOC as the reference group. The treatment ranking was generated using p-scores, which is equivalent to the SUCRA score, ranging from 0 to 1. 10 A higher p-score indicates a higher probability of being the best treatment option. I 2 values increase with larger pooled samples. Thus, we used τ 2 to measure heterogeneity, with 0.04, 0.16, and 0.36 corresponding to low, moderate, and high degrees of heterogeneity, respectively.
Subgroup analyses were conducted based on treatment comparisons to evaluate heterogeneity within studies. Sensitivity analyses were also performed in the presence of serious bias, significant heterogeneity, or estimated effect size in different diagnosis groups. The outlier studies were detected by “NMAoutlier” module. Further network meta-analysis was conducted after excluding these studies. The result would be compared with the original analysis, which included all studies meeting the criteria, to see if there's significant impact of certain studies.
RESULTS
Literature search and selection process
The database search yielded 1,393 articles. After the removal of duplicates and screening titles and abstracts, 82 full-text articles were reviewed for eligibility, and 38 studies were included in the quantitative synthesis. Figure 3 shows the PRISMA flow diagram for the clinical literature search.
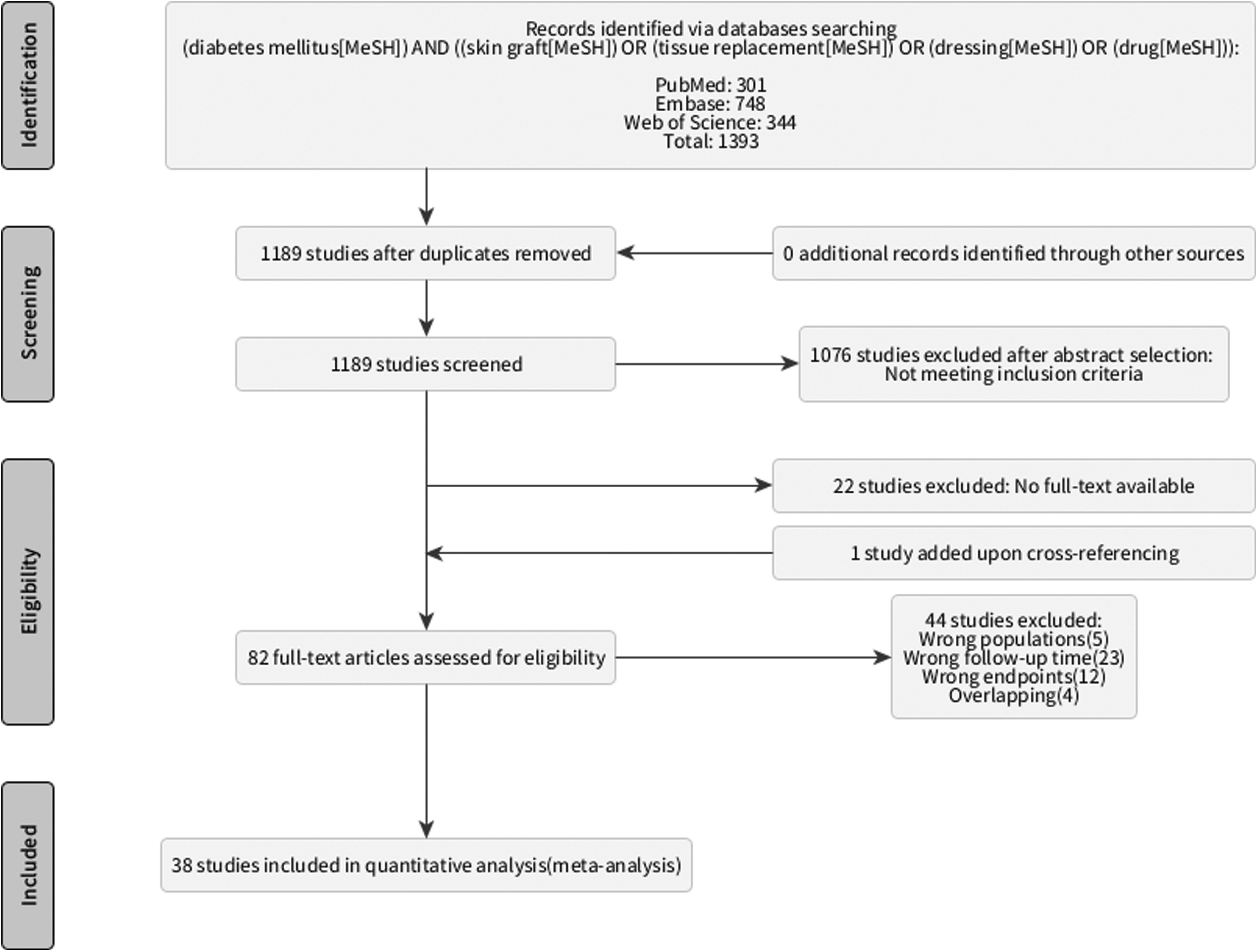
PRISMA flow diagram of the number of records identified, screened, assessed, included, and excluded, and the reasons for exclusion. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses.
Study characteristics
Our network meta-analysis included 38 randomized controlled trials (RCTs) with a total of 3,862 patients. All studies were active comparator studies, with 16 articles comparing ATD and SOC11–26, 1 article comparing SSLC and ATD27, 6 articles comparing ASS and SOC28–33, 5 articles comparing PBTP and SOC34–38, and 11 articles comparing SSLC and SOC35, and 39–48. Table 2 shows the characteristics of the participants in each study group and the primary outcome of each study; the classification system is also listed.
Characteristics and wound healing rate of included studies
This study utilized University of Texas Treatment-Based Diabetic Foot Classification System (UTDWC), we redefined it into Wagner's classification.
In these studies, they did not present the exact classification of the wound, but we used the description of inclusion and exclusion criteria to determine the grade.
FCG, formulated collagen gel; HSAM, hypothermically stored amniotic membrane; N/A, not applicable.
Among the enrolled studies, the profiles of the participants were presented in the Supplementary Appendix SA3 according to intervention classification. Generally, the participants were mostly male (around 70%) with type 2 diabetes (88%), 55–65 years of age, mild-to-moderate obesity (BMI 30–35 kg/m2), and had small- to medium-sized neuropathic ulcers (mean: 3.80 cm2, range: 1.0–26.6 cm2).
However, as for the grading of the ulcer, 34 of 38 studies have disclosed their inclusion criteria of it and 4 have not. Among the 34 studies, 19 included only Wagner grade I (partial- or full-thickness ulcer) patients, 14 included both Wagner grade I and II (deep ulcer extended to ligament, tendon, joint capsule, or bone without abscess or osteomyelitis) patients, 1 study included grade II and III (deep abscess formation or osteomyelitis) patients, and no study included grade IV (forefoot gangrene) or V (extensive gangrene) patients. In all, the patient characteristics were similar among studies and the intervention categories, which minimize the bias and facilitate the quantitative meta-analysis. Supplementary Appendix SA4 was the descriptions of different treatment options.
Methodological quality
The network graph demonstrates the structure of our network meta-analysis (Fig. 4). When the data were pooled, low heterogeneity was observed (τ 2 = 0.10). Subgroup analysis revealed moderate heterogeneity for SSLC versus SOC and ASS versus SOC (τ 2 = 0.24 and 0.24, respectively) and low heterogeneity for PBTP versus SOC, ATD versus SOC, and SSLC versus ATD (τ 2 = 0.05, 0.00, and 0.02, respectively) (Fig. 5). Egger's test revealed no significant asymmetry (p = 0.8852), indicating no publication bias, as shown in Fig. 6.
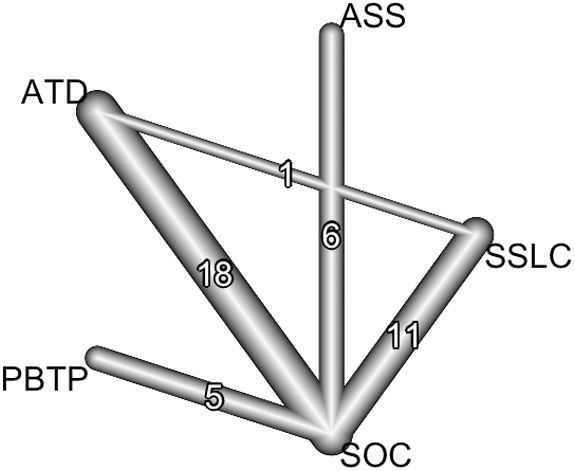
The network graph demonstrating the structure of our network meta-analysis.

Subgroup analyses based on pairwise comparison demonstrating the heterogeneity between studies.
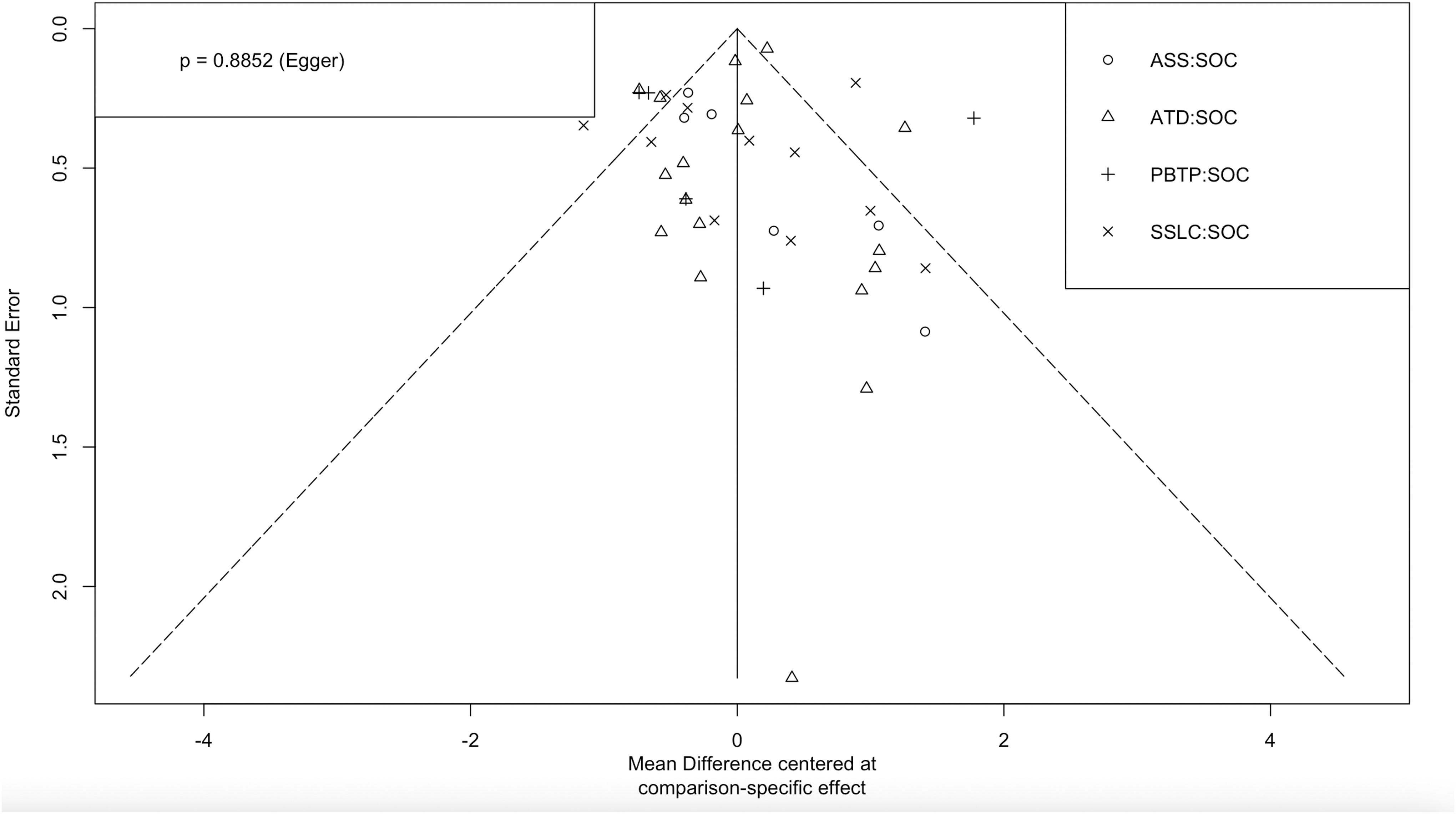
Funnel plot assessing publication bias and small study effects.
Wound healing probability
Twelve-weeks' crude wound healing rates for PBTP, SSLC, ASS, ATD, and SOC were 72.0%, 53.8%, 61.8%, 48.1%, and 33.2%, respectively. The crude healing rates at 16 weeks were 58.0% at PBTP, 51.0% at ASS, 64.8% at ATD, and 37.5% at SOC group; there was no study including the 16-week wound healing rate of SSLC. The wound healing rates reported in each study are summarized in Table 2. The consistency in the direct, indirect, and network comparisons of each treating arm is shown in Table 3. After pooling direct and indirect estimates, PBTP exhibited the best wound healing probability (p-score = 0.90), followed by SSLC (p-score = 0.70), ASS (p-score = 0.56), and ATD (p-score = 0.34) compared with the wound healing probability of SOC (Fig. 7).
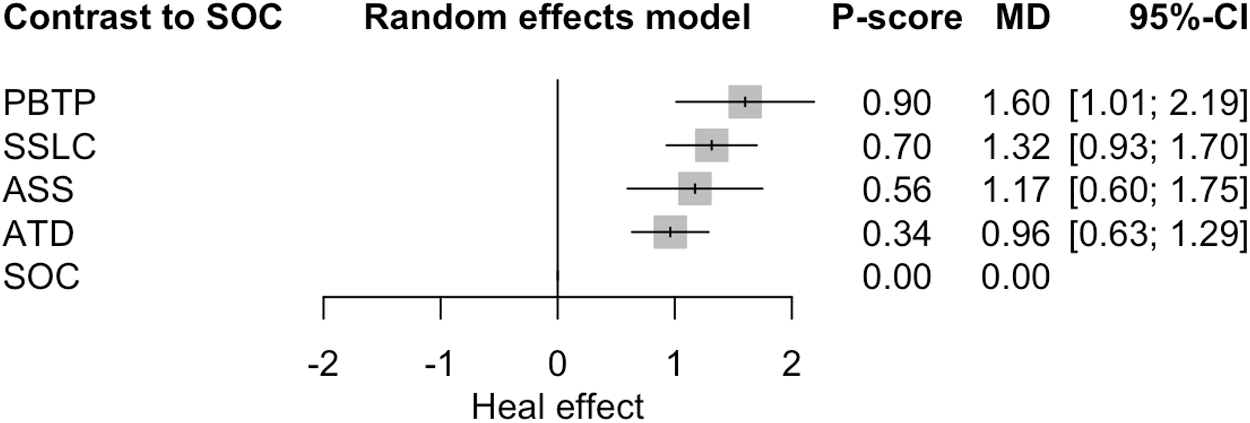
Forest plot demonstrating the odd ratio of healing probability compared with SOC and ranking of treatment arms by p score. SOC, standard of care.
The consistency in the direct, indirect, and network comparisons of each treating arm
Sensitivity analyses
We performed sensitivity analyses after using the “NMAoutlier” module and determination of publication bias. In these analyses, there was no prominent outlier detected. However, almost all studies used SOC as comparator and only one head-to-head study comparing SSLC to ATD. After exclusion of this particular study “Landsman 2018,” the treatment ranking remained the same, with p-score of 0.90, 0.69, 0.56, and 0.35 in the order of PBTP, SSLC, ASS, ATD, respectively. We further excluded “Moon 2019” due to relatively higher risk of bias to conduct more precise sensitivity analyses. No significant heterogeneity or inconsistency was found, and the ranking of treatment remained the same, with p-score of 0.90, 0.67, 0.57, and 0.37 in the order of PBTP, SSLC, ASS, ATD, respectively (Supplementary Appendix SA5).
Recurrence rates
Recurrence rates were evaluated in 11 of the 38 studies (Table 4). The recurrence status was assessed after reaching primary endpoint (wound healing), and the time point of clinic follow-up to observe for any signs of healed ulcer recurrence and safety assessments was also documented in Table 4. All 11 studies compared biomaterial products with SOC. The overall pooled recurrence rate of the intervention group was 11.21%, which might be related to the follow-up time after wound healing.
Recurrence rate of the healed ulcers of included studies
T: time point of assessment after primary endpoint achieved (weeks).
The healing rate here means the initial wound healing rate as the primary outcome of the studies.
The recurrence rate was evaluated for subjects whose ulcer healed during the treatment phase.
Based on the pooled results, the intervention group had a lower risk of recurrence than the SOC (11.21% vs. 15.15%). We also conducted a meta-analysis on this specific subgroup to estimate the odds ratio of recurrence. The result demonstrated that compared with the control group, intervention group generated decreased risk of recurrence (Fig. 8). Nevertheless, the follow-up time of each study varied, so the quantitative result may not be eligible, while the trend of this result may be reasonable.

Forest plot demonstrating the odd ratio of recurrence risk compared with SOC.
DISCUSSION
There is a growing need for wound dressings to heal DFUs more efficiently and effectively. Our meta-analysis, which combined both direct and indirect comparisons, provides an overview and ranks the healing effectiveness of various products regarding complete wound closure within 12–16 weeks. These studies had similar patient characteristics and relatively low risk of bias, which made the quantitative analysis result more convincing.
Our study demonstrated that PBTP achieved the best healing outcomes when compared with other biomaterials. This result was derived from five studies through the indirect comparison (Table 3 and Fig. 7). Amniotic membrane wound dressings have been used for over a century as an alternative biomaterial in reconstructive surgery. 49 PBTP contains a single epithelial cell layer, a thick basement membrane, and an avascular stroma, making PBTP an ideal biological graft. Human amniotic membranes can assist in wound healing by supporting cell migration into the healing tissue. 50 In addition, placental tissues are immune-privileged; the antigens in placental tissue do not evoke an inflammation response. The PBTPs keep the native composition of the extracellular matrix and contain growth factors, chemokines, and cytokines that modulate the inflammation process and promote tissue repair. 51
A recent systemic review by Lakmal et al. 52 included 12 studies (8 RCTs, 2 prospective, and 2 retrospective studies) and showed that DFU healing time was shorter for amniotic membrane allografts compared with healing times in response to conventional methods. However, the heterogeneity among studies precluded further meta-analysis. Our study compensated for this issue by setting stricter inclusion criteria.
According to our definition, SSLC products contain living cells, including keratinocytes and/or fibroblasts within the matrix. 53 SSLC exhibited better healing rates than ASS. The key role of keratinocytes in diabetic wound healing is widely accepted. Nevertheless, cellularized materials are intricate, difficult to manufacture, and more susceptible to host rejection, particularly if the product is not an allograft. 54 Moreover, most SSLCs require specific storage to keep the cells alive. For example, Apligraf should be maintained at 68–73°F and Dermagraft must remain frozen at −103°F ± 18°F. On the other hand, ASS is usually dehydrated or freeze dried and can be stored at room temperature, making these products more convenient and economical. 53
As for the ulcer recurrence, our meta-analysis revealed the patient treated with biomaterials had a lower risk of recurrence than SOC. However, the risk difference is marginal and the follow-up periods varied among studies (4–24 months), therefore, the strength of effect is somehow doubtful. Besides the local tissue durability of the healing ulcer, recurrence might be more related to other factors, such as off-loading devices, blood glucose control, and body weight. The effectiveness of biomaterials in recurrence prevention requires more studies to clarify.
Most previous systemic reviews only focused on skin substitutes, which require graft fixation, short-term immobilization, or even hospitalization. However, some other products, including gels, ointments, and dressings, which we called ATD, are commonly used daily or weekly for DFU wound care and different from skin substitutes. These products may be good alternatives for patients who cannot tolerate surgery or immobilization.
On the other hand, due to different mechanisms of wound healing, such as antibiofilm or anti-inflammation, and different application methods from other skin substitutes, the ATDs can also be combined with other therapies after skin substitute implantation to achieve better healing. For example, as shown in Fig. 9, a patient with a moderate-sized (15 cm2) Wagner II plantar DFU underwent artificial dermis (Integra) grafting initially. After the graft was well taken, the wound seemed to be downgraded to a superficial one, and a macrophage-regulating ointment (ON101) was used daily to accelerate the epithelialization.

Combination of multiple wound treatment strategies
In the real-world clinical practice of DFU care, treatment outcomes depend on both the effectiveness of dressing materials or treatment modalities and multifaceted patient factors, including out-of-pocket expenses and treatment compliance. 55 Therefore, cost-effectiveness and ease of dressing use should be considered when establishing personalized treatment plans for DFUs.
Most chronic wounds have a dynamic healing process due to multiple local tissue and systemic factors. 56 Due to this complexity, establishing general treatment guidelines is difficult. Advanced wound care materials were compared with standard care or other wound care materials in this study. This information can facilitate decision making and enhance clinical outcomes.
Based on the demographic data of the studies included in our review, most participants had small- to medium-sized, Wagner grade I or II DFUs with no active infection. Although there was no clear description of the ulcer etiology in most studies, we could expect they were mainly neuropathic foot ulcers, while these studies had set certain criteria to exclude limb ischemia (Supplementary Appendix SA6).
However, there were still some variations among studies (e.g., ankle brachial pressure index >0.9 or >0.7), whereas some studies did not investigate the precise blood supply or vascularity of the ulcers. Topical intervention is more likely to achieve complete wound healing in the patients with small and superficial DFUs and adequate limb perfusion. For patients with larger DFUs, some surgeons would choose split-thickness skin grafts or flap surgery for wound closure. 47,57 However, it is difficult to conduct an RCT for skin graft or flap surgery, and this is the reason why we did not include these methods in our analysis. The 12-week healing rate is the traditional primary outcome in DFU studies.
However, many studies revealed a substantial increase in healing between 12 and 16 weeks for some biomaterial products. 29,37,38 Therefore, we included studies with 12- to 16-week healing rates as the primary outcomes. Because of the homogeneous patient population and the relative strict outcome of included RCTs, we demonstrated the low risk of bias and heterogeneity of the meta-analysis.
Biomaterial wound dressings are diverse, and new products are discovered every day. However, there is no universal classification system. A classification system was proposed based on cell components. For example, Balasubramani et al. 58 classified skin substitutes into epidermal, dermal, and both epidermal and dermal layers. Kumar 59 proposed a similar classification system, which is widely used. This system includes a new temporary, impervious, dressing material group, and subdivides other groups into single or double-layer groups. However, differentiating products based on the presence of live cells may be important, due to the differences in clinical application, storage, cost, and availability of biomaterial products. 54 Therefore, we followed the recommendation of Davison-Kotler et al. and classified the skin substitutes, except PBTP, based on the existence of living cells into SSLC and ASS.
Furthermore, cost is another major concern when treating patients with DFUs, and some studies evaluated the cost-effectiveness of skin substitutes. A Canadian study 60 comparing skin substitutes as adjunct therapy with SOC considered relevant costs (physician fee, debridement, dressing change) and savings (reduction in minor and major lower-extremity amputations). Assuming a 26-week treatment interval, the study showed that the mean total costs for the skin substitute treatment and standard care were $6,371 and $5,313 (Canadian dollars), respectively, but skin substitute achieved a greater number of ulcer-free weeks (18.96 weeks vs. 12.26 weeks over 26 weeks).
Samsell et al. 61 analyzed the cost-effectiveness of eight skin substitutes, including two PBTP, two SSLC, and four ASS, and found that the average cost for treating one DFU varied from $2001 to $14,507 and $1207 to $8791 for the hospital outpatient department and physician's office setting, respectively.
Although the cost is generally correlated with the healing probability according to the classification of treatment products in our meta-analysis (Table 1), the cost of the certain biomaterial did not necessarily correlate with its efficacy, and physicians and patients can choose the most appropriate one according to their local prices.
Regarding the use of biomaterials for DFU treatment, we suggest effectiveness, cost, and ease of use (compliance) as the three key factors for patients. Costs may vary in different countries or insurance systems and compliance is related to individual patient characteristics. Our network meta-analysis, which combined both direct and indirect comparisons, provides an overview and ranks the healing effectiveness of the different treatments to support clinical decision making.
In this review, we included 38 RCTs of the topical treatment of DFU, and nearly 60% of the studies were conducted in the United States. This also reflects the regulation difference between countries or continents, as well as the availability of these products. For example, the well-known product of SSLC Apligraf, did not get the global marketing approval in EU but only received Switzerland's approval. A similar situation also happened to PBTP. A review article published in 2021 found that the United States took 79% of world market while Africa, Asia, and Europe shared the remaining 21%. 62 However, due to the increasing popularity of cell therapy, we believe the application of the advanced biomaterials in DFU care will soon be widespread in the world.
Limitations
There are several limitations to this meta-analysis. First, the vast majority of the included studies used SOC as control group and only one head-to-head study was enrolled, which caused the results largely dependent on the indirect comparisons. Future meta-analysis might be conducted with more product versus product trials to provide stronger evidence. Second, the main SOC comparison group in our study differed slightly in each study, which may impact the results of this study.
Third, many of the included randomized studies failed to blind their participants and/or assessors. This claim is complicated by differences in the appearance of certain skin substitutes and SOC dressings. Complete double blinding may therefore be technically infeasible for this type of study. However, bias can be minimized by employing objective measures for assessing outcomes and using independent assessors of wound closure when possible. Fourth, the included studies in our review were across two decades, and the SOC also changed from time to time, which might lead to some bias (Supplementary Appendix SA7).
For example, the PBTP studies were mostly conducted within recent 10 years and more hydrofiber dressings have been used as SOC lately while some older studies used paraffin gauze, which might lead to lower healing rates. However, which SOC is better or worse is still controversial but remained a confounding factor in this study. Fifth, the majority of the studies had financial disclosures to report that were relevant to the manufacturer of the skin substitutes being tested, whereas other studies included no information about funding sources.
Sixth, the “DFUs” mentioned in this meta-analysis should be classified as neuropathic ulcers, however, the criteria of limb perfusion among studies were not entirely consistent. To focus more on neuropathic ulcers, precise vascularity evaluation is required in the future studies. Lastly, the patient population of the included studies were relatively homogeneous that focused on small superficial wounds, but this could not reflect the real clinical situations, which are usually more complicated. Therefore, our study results should be interpreted with caution when put into clinical practice.
CONCLUSIONS
This network meta-analysis provides the information of the relative effectiveness and rank for the use of biomaterials and topical dressings in DFU healing. In treating small, superficial, and neuropathic DFUs, PBTP had the best healing outcome, followed by SSLC, ASS, and ATD when compared with SOC. Future studies should consider costs and patient compliance for better application in the diverse clinical scenarios.
TAKE HOME MESSAGES
Regarding the use of biomaterials for DFU treatment, the effectiveness, cost, and patient compliance are the three key factors for clinical decision making.
The meta-analysis showed placenta-based tissue products have the best DFU healing effectiveness, followed by SSLCs, ASSs, and ATDs.
Combination of skin substitutes and ATD may improve DFU healing.
In this study, the patient population were homogeneous, which had superficial and small wounds, and the study results required caution when applying to real-world practice.
Footnotes
ACKNOWLEDGMENT AND FUNDING SOURCES
The authors appreciate Enago for professional language editorial services. No funding was received for this article.
DATA AVAILABILITY STATEMENT
All data generated or analyzed in this study are included in this published article. The datasets used and/or analyzed during the current study are available from the corresponding author.
AUTHORs' CONTRIBUTIONS
All authors had full access to the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Conceptualization, Y.L. and A.C.-Y.C.; Methodology, Y.L. and D.-H.C.; Investigation, Y.L., A.C.-Y.C., and D.-H.C.; Formal Analysis, Y.L.; Resources, D.-H.C., Y.-S.C., C.-Y.H., and K.-C.C.; Writing—Original draft, A.C.-Y.C., and Y.L.; Writing—Review and editing, C.-Y.H., D.-H.C. and K.-C.C.; Visualization, Y.L.; Supervision, D.-H.C.
AUTHOR DISCLOSURE AND GHOSTWRITING
The authors have no financial interests to disclose. The content of this article was thoroughly written by the authors listed. No ghostwriters were used to write this article.
ABOUT THE AUTHORS
SUPPLEMENTARY MATERIAL
Supplementary Appendix SA1
Supplementary Appendix SA2
Supplementary Appendix SA3
Supplementary Appendix SA4
Supplementary Appendix SA5
Supplementary Appendix SA6
Supplementary Appendix SA7
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.