
Abstract
Significance:
Venous leg ulcers (VLUs) are the most common venous disease, mainly presenting as open skin lesions on the legs or feet and are an important concern in clinical care settings.
Recent Advances:
Comprehensive tactics were employed to search electronic databases PubMed, Embase, guideline databases, and society websites were searched for Clinical Practice Guidelines (CPGs) on VLU care. The basic information, recommendations for the VLUs, methodological quality, and reporting quality of VLU's CPGs were extracted and captured in Excel. The quality of each CPG was independently assessed by four researchers using AGREE II instrument and the RIGHT checklist.
Critical Issues:
This study included 19 CPGs with a combined 23 recommendations. The assessment of VLUs was summarized based on the recommendations of VLUs in 11 major items; six on VLU's diagnosis and six on therapeutic strategies of VLUs. The identified CPGs were of mixed quality, and the highest score based on the scope and purpose was 82.85 ± 11.66, whereas the lowest mean score based on the editorial independence by AGREE II was 59.93 ± 21.50. Regarding the RIGHT checklist, field one (basic information) had the highest reporting rate (84.33%), whereas field five (review and quality assurance) had the lowest quality of CPGs (41.11%).
Future Directions:
This evidence map provided new perspectives in the presentation of evidence. In addition, the evidence map collected and evaluated the characteristics of published CPGs. Thus, the evidence map enhances our knowledge and promotes the development of trustworthy CPGs for VLUs.

INTRODUCTION
Venous leg ulcers (VLUs) are the most common venous disease, mainly presenting as open skin lesions on the legs or feet. They occur in areas affected by venous hypertension 1 and painful lower extremity wounds lasting more than 4 weeks. The prevalence of VLUs in the general population is 1% and 3% to 4% in individuals over 65 years of age. 2,3 VLUs are characterized by slow healing and high recurrence. Generally, it takes an average of 6 to 12 months for VLUs to heal. However, an average of only 60% of patients will heal in 12 weeks. 4 Up to 7% of patients with VLUs remain unhealed after 5 years of treatment due to variability in clinical practice. 5 Once healed, 75% develop a recurrence within 3 weeks.
At the same time, 50% to 70% develop a recurrence within 6 months. 6 Longer healing time and recurrence of VLUs are major challenges affecting individual health and quality of life. The effects of VLUs on the quality of life of patients include reduced mobility, pain, social isolation, loss of self-esteem, anxiety, and depression. 7 Furthermore, the management of chronic wounds, particularly VLUs, is costly. In Australia, the estimated health care costs of VLU treatment exceed $3 billion per year. 8
A recent study shows that the mean cost of treating VLUs in the United Kingdom exceeds 7,600 pounds per wound per year. 9 The burden and cost of VLUs are expected to rise sharply due to the increase in the older population and the high prevalence of diabetes, chronic cardiovascular disease, and obesity. 10 In conclusion, more attention should be focused on managing and treating VLUs.
Clinical practice guidelines (CPGs) are systematically formulated principles that include recommendations to optimize patient care in specific clinical situations. 11,12 Currently, several organizations conduct their CPGs and publish recommendations. Well-developed and evidence-based CPGs clinically improve the treatment of VLUs. However, different organizations may publish conflicting recommendations for CPGs, leading to inconsistencies and raising concerns about the quality of CPGs. Therefore, this study comprehensively reviewed and systematically assessed the quality of CPGs by evaluating and collating the quality and recommendations for the VLUs.
Evidence mapping systematically collects existing evidence in relevant research fields. It conducts comprehensive analysis, scientific evaluation, integration, and condensation. At the same time, it concisely and intuitively presents its research status, problems, development directions, and evidence gaps. 13 Evidence mapping provides high-quality evidence for policymakers while identifying research gaps to guide future research by systematically presenting and analyzing relevant evidence in a particular research area. 14 This study presented the CPGs based on diagnosis, therapeutic strategies, and recommendation conflicts for VLUs using evidence-mapping methods.
METHODS
Design
The systematic review was performed following the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA 2020) statement (Supplementary Data SD1).
Search strategy and selection criteria
CPGs were searched in PubMed, Embase, and Web of Science using medical subject headings and keywords. CPGs were also searched in guideline databases, including, but not limited to, National Guidelines Clearinghouse (NGC), National Institute for Health and Care Excellence (NICE), Scottish Intercollegiate Guidelines Network (SIGN), and Guidelines International Network (GIN). Finally, reports of CPGs in the reference lists of eligible guidelines were also searched.
Inclusion criteria for the CPGs were as follows: (1) meeting the definition by the Institute of Medicine 15 ; (2) recently published; (3) written in English.
Data extraction
Two reviewers independently extracted data on the characteristics of the included CPGs using a standard data extraction form. The extracted data included the title, publication year, organization, version, development location, funding, method of forming recommendations, and recommendations for VLU screening, diagnosis, prevention, and treatment. The extracted data were cross-checked, and a third reviewer arbitrated any disagreements.
Quality assessment
The methodological quality of included CPG was evaluated by four researchers based on the Guidelines Research and Evaluation Tool (AGREE II). An independent review of the quality of each CPG that met the eligibility criteria was conducted based on the Reporting Items for Practice Guidelines in Health care (RIGHT) guidelines.
AGREE II instrument comprises 23 items in six domains (scope and purpose; stakeholder involvement; rigor of development; clarity of presentation; applicability; and editorial independence) and two full evaluation entries for the CPG (overall quality assessment and whether to recommend CPG). 16 Each item describes a specific question of the quality evaluation, and the reviewer evaluates the quality of CPG. A score of 1 (strongly disagree) indicates that the CPG does not meet the item description, whereas a score of 7 (strongly agree) indicates that the CPG meets the description very well. Furthermore, the item scores by each reviewer were finalized, and the domain scores were calculated 16 : The standardized score was calculated using the following formula: (score obtained−minimum possible score)/(maximum possible score−minimum possible score) × 100%.
In addition, the quality of CPGs was evaluated using the RIGHT checklist. The RIGHT checklist comprises 22 items in seven broad areas: basic information, background, evidence, recommendations, review and quality assurance, funding, declaration and management of interests, and information. 17 Four reviewers evaluated each item based on its reporting content using “Yes” (information about the item is presented completely), “Partial” (information about the item is presented partially), and “No” (information about the item is completely missing).
Grading recommendations
The evidence was graded according to the recommendations of Guyatt et al. 18 (Table 1), with “high,” “medium,” or “low” ratings given to the three core components of the respective studies: study quality, risk of bias, and benefit versus risk.
Grading recommendations
Data synthesis and analysis
Statistical analysis
The average scores of each domain were calculated after methodological quality evaluation of the CPGs using the AGREE II. Based on the standardized score, CPG was classified as “strongly recommended” for overall scores >60%, “recommended with modifications” for scores between 30% and 60%, and “not recommended” for scores <30%. 19 At the same time, the number of RIGHT checklist items reported in each CPG and the number of CPGs that reported single RIGHT checklist items represented the reporting quality. The CPG had a high quality if the number of Yes was over 70% and of low quality if the number of Yes was below 40%. Data were analyzed using SPSS 12.0 software (VERSION).
In addition, the consistency among researchers (0 = untrustworthy, 1 = completely reliable) was evaluated using the intra-class correlation coefficient (ICC). ICC >0.75 indicated high consistency. ICC between 0.45 and 0.75 indicated good consistency, while ICC <0.4 indicated poor consistency. 20 All statistical analyses were performed using SPSS software version 22.0.
Quality mapping
The CPG's recommendations, including VLU prevention, screening, and treatment strategies, were summarized using descriptive analyses. All analyses were performed, and bubble plots were generated using Microsoft Excel 2019 (Microsoft Corp, Redmond, WA,
RESULTS
CPG search and characteristics
Our search generated 14,738 reports. After removing duplicates, 9,981 articles were screened further. In the end, 19 full-text articles 21 –39 met the eligibility criteria (Fig. 1) and were included in the final analysis. Among them, 10 CPGs were original versions, 22 –24,26 –29,33,35,36 and the rest were updated from original CPGs. 21,25,30 –32,34,37 Ten CPGs focused on VLU practices, three focused on venous ulcer practices, two focused on chronic venous disease practices, and the rest focused on practices for wound and skin, respectively. Of the 19 eligible CPGs, two 21,25 were developed by professional CPG development organizations, six 23,26–27,29,36,38 were developed by the professional vascular society, and five 22,24,31 –33 were developed by the professional wound society. The remaining six CPGs 28,30,34,35,37,38 were developed by the medical centers or health systems. An overview of the characteristics of the CPGs is presented in Table 2.
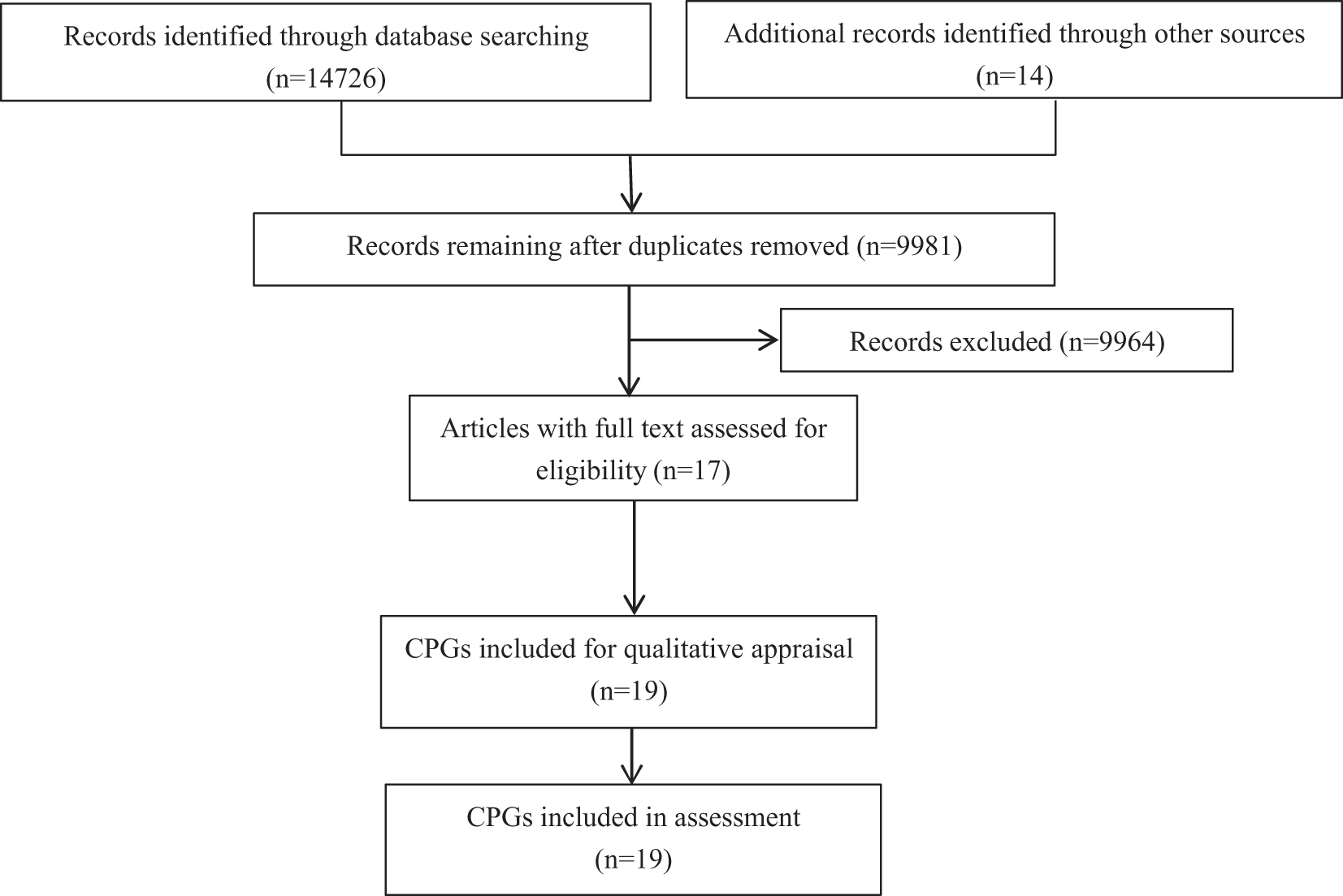
Flowchart of selection process for CPGs. CPG, Clinical Practice Guideline.
Basic information of CPGs
The methodological quality and reporting quality of CPGs
The ICC between the four reviewers in the study was 0.87 (95% CI: 0.82–0.93). The AGREE II standardized domain scores for each CPG and their overall assessment are shown in Table 3 and Supplementary Appendix Table SA1. The highest score based on the scope and purpose domain was 82.85 ± 11.66. The lowest mean score based on the editorial independence domain was 59.93 ± 21.50. The score of domain five (applicability) was 70.64 ± 19.27, which was also relatively low. A total of 19 CPGs were divided into three levels based on the overall assessment of each CPG. The different levels of the CPGs were represented by three different colored spheres.
Standardized scores of guidelines by AGREE II instrument
RNAO, Registered Nurses Association of Ontario; WHS, Wound Healing Society; ESVS, European Society for Vascular Surgery; AWMAI&NZWCS, The Australian Wound Management Association, Inc.&The New Zealand Wound Care Society; SIGN, Scottish Intercollegiate Guidelines Network; SAS&VSAVF, Clinical practice guidelines of the Society for Vascular Surgery&the American Venous Forum; ICSI, Institute for Clinical Systems Improvement; AAWC, Association for the Advancement of Wound Care; EWMA, European Wound Management Association; ISTAP, International Skin Tear Advisory Panel; EVF&IUA&CDERT, The European Venous Forum&The International Union of Angiology&The Cardiovascular Disease Educational and Research Trust (UK); EDF, European Dermatology Forum; UB, University of Bonn; R, Recommended; RM, Recommended with modifications; NR, not recommended.
Eleven CPGs 21,24 –26,29,33–34,36,37 –39 (represented by 11 green spheres) developed by RNAO (Registered Nurses Association of Ontario), AWMAI&NZWCS (The Australian Wound Management Association, Inc.&The New Zealand Wound Care Society), SIGN (Scottish Intercollegiate Guidelines Network), SAS&VSAVF (Clinical practice guidelines of the Society for Vascular Surgery&the American Venous Forum), ESVS (European Society for Vascular Surgery), EWMA (European Wound Management Association), Health service, EVF&IUA&CDERT (The European Venous Forum&The International Union of Angiology&The Cardiovascular Disease Educational and Research Trust [United Kingdom]), and EDF scored higher than the remaining CPGs and were recommended for clinical practice.
Six CPGs 22,27–28,31–32,35 (represented by six yellow spheres) developed by WHS2006 (Wound Healing Society), SVA&AVF, ICSI (Institute for Clinical Systems Improvement), AAWC (Association for the Advancement of Wound Care), WHS2015, and ISTAP (International Skin Tear Advisory Panel) were recommended with modifications.
Two CPGs 23,29 (represented by red spheres) developed by ESVS and Clare Williams were not recommended (Fig. 2).
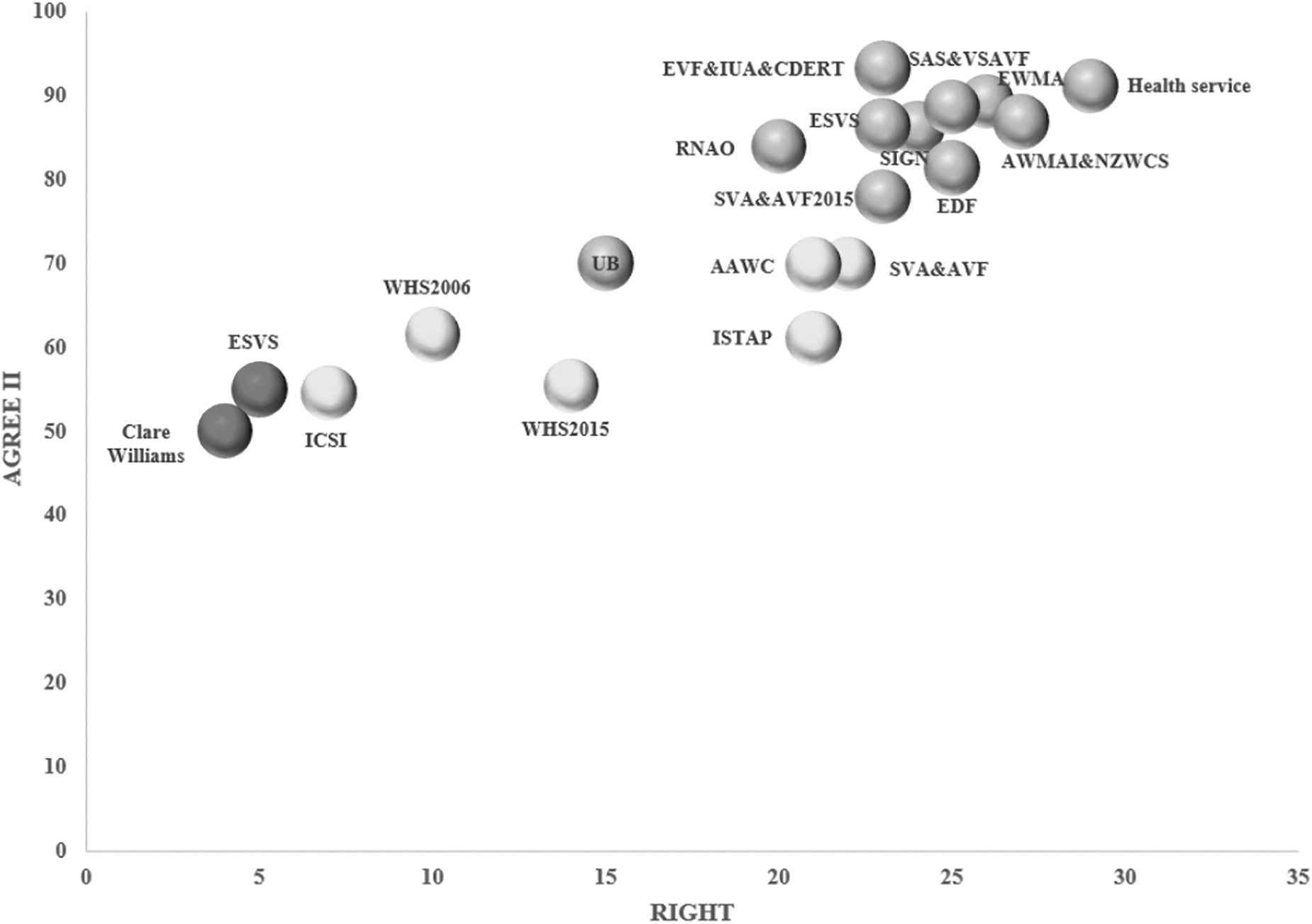
Grading and analysis of reporting and methodological quality of CPGs. RNAO, Registered Nurses Association of Ontario; WHS, Wound Healing Society; ESVS, European Society for Vascular Surgery; AWMAI&NZWCS, The Australian Wound Management Association, Inc.&The New Zealand Wound Care Society; SIGN, Scottish Intercollegiate Guidelines Network; SAS&VSAVF, Clinical practice guidelines of the Society for Vascular Surgery&the American Venous Forum; ICSI, Institute for Clinical Systems Improvement; AAWC, Association for the Advancement of Wound Care; EWMA, European Wound Management Association; ISTAP, International Skin Tear Advisory Panel; EVF&IUA&CDERT, The European Venous Forum&The International Union of Angiology&The Cardiovascular Disease Educational and Research Trust (UK); EDF, European Dermatology Forum; UB, University of Bonn.
Based on the RIGHT checklist, most CPGs were of moderate to high quality (Supplementary Appendix Table SA1). CPGs on health service reported the most items (29 items) in the RIGHT checklist, followed by EWMA (26 items). Based on the seven domains of the RIGHT checklist, field one (basic information) was the most reported (84.33%), whereas field five (review and quality assurance) was the least reported (41.11%) (Fig. 2).
Summary and recommendations for VLUs
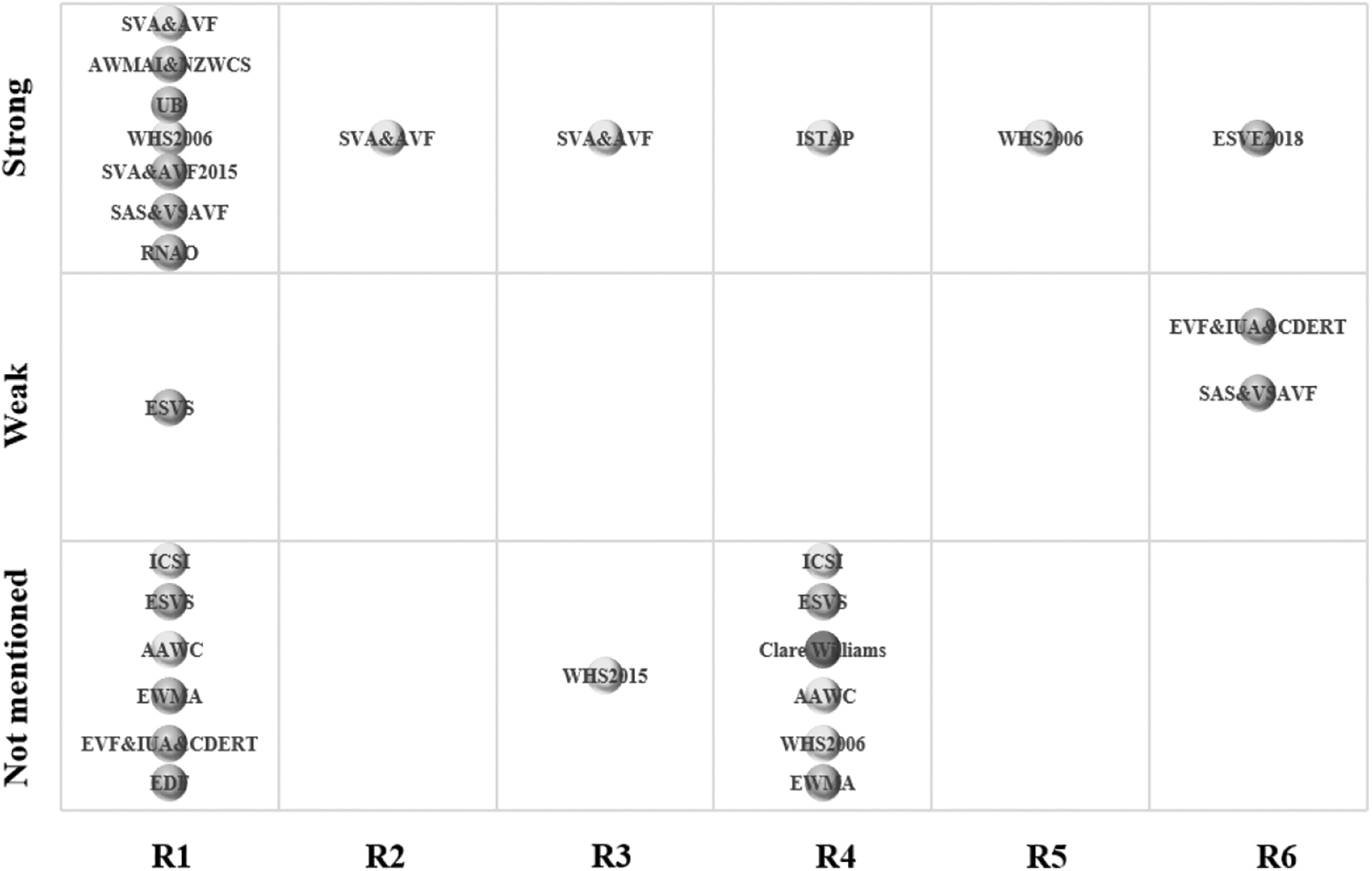
The y-axis in the bubble chart represents the strength of the recommendation, which was divided into strong, weak, and not mentioned. The x-axis represents different recommendations for CPGs. The VLU recommendations in the CPG, including assessment, diagnosis, and therapeutic strategies, were summarized.
CPG recommendations on VLU assessment
Fifteen CPGs 21–22,24 –35,39 contained 11 major recommendations (Fig. 3 and Supplementary Appendix Table SA2). The summary of recommendations is as follows:
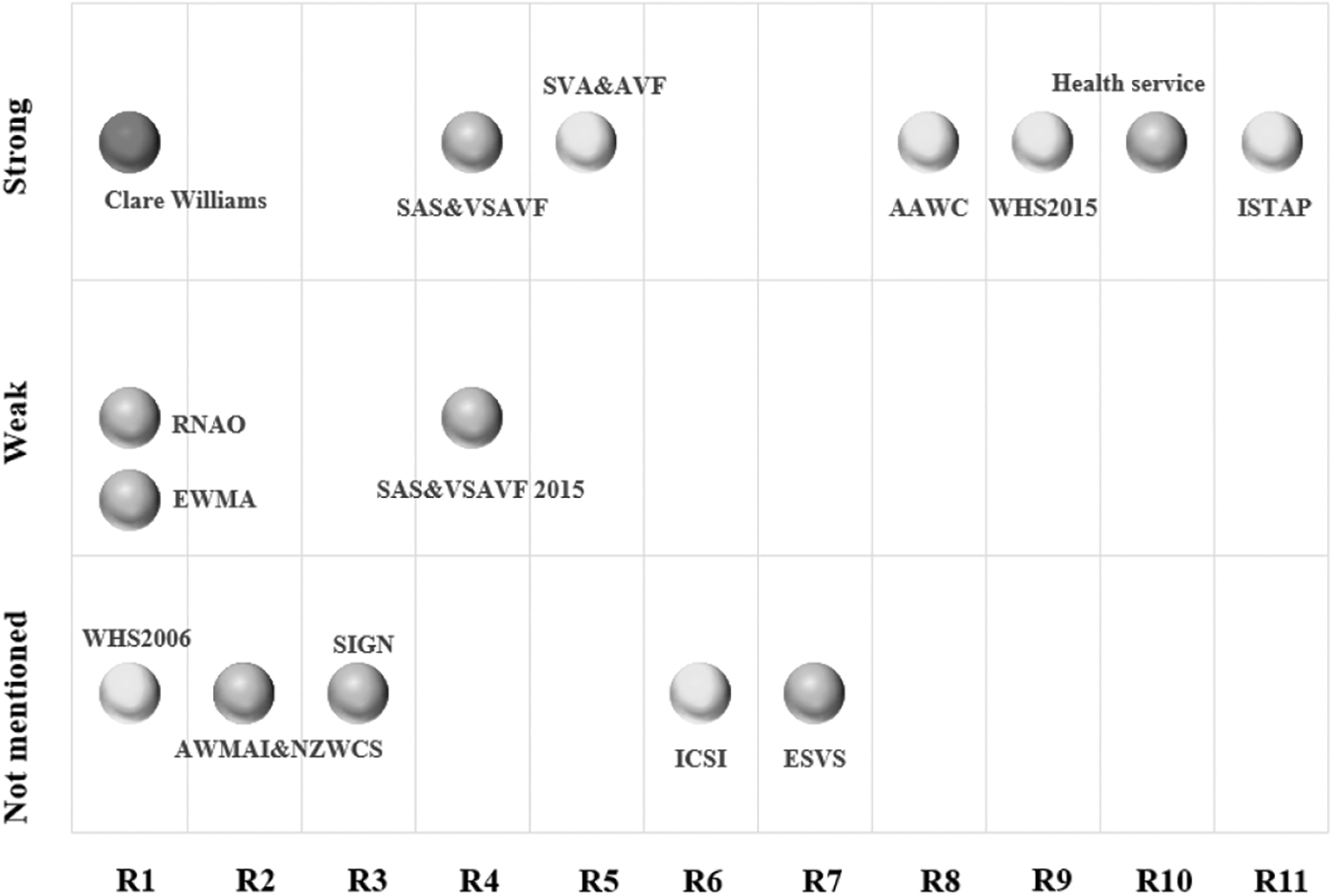
CPGs recommendations on VLU's assessment.
Assessment and clinical investigations should be undertaken by a health care professional(s) trained and experienced in leg ulcer management (Weak, 21 Strong, 30 Not mentioned 22,33 );
Assessment for VLUs: All patients presenting with a leg ulcer should receive a comprehensive assessment by a health professional trained in the assessment and management of VLUs, which includes patient history, examination of the leg, vascular assessment, biochemical analysis, microbiology and histopathology, nutritional assessment, pain assessment, and psychosocial, quality of life, and social assessments (Not mentioned 24 );
The leg should be assessed for signs of venous disease (Not mentioned 25 );
We recommend that all patients with VLU be classified on the basis of venous disease classification assessment, including Clinical–Etiology–Anatomy–Pathophysiology (CEAP), revised Venous Clinical Severity Score, and venous disease-specific quality of life assessment (Strong 26,39 );
The venous procedural outcome, including impact on VLU healing, should be assessed (Strong 27 );
The extent of necrotic tissue in the wound bed (T), presence of inflammation or infection (I), evidence of any surrounding maceration (M), and the edge (E) of the ulcer (Not mentioned 28 ) should be described;
The ChronIc Venous Insufficiency Questionnaire (CIVIQ), Aberdeen Varicose Vein Questionnaire (AVVQ), and Venous Insufficiency Epidemiological and Economic Study on Quality of Life (VEINES-QOL) used to measure the health outcomes in patients with varicose veins. (Not mentioned 29 );
Validated measures such as wound depth (Not mentioned 31 );
If significant wound improvement does not occur within 3–6 weeks of initiating a treatment plan, reevaluation of the patient and consideration of other treatment options should be considered (Strong 32 );
Several (more than twice daily) skin assessments at the skin device interface in patients vulnerable to fluid shifts and/or exhibiting signs of localized or generalized edema should be performed (Strong 34 );
A full holistic skin assessment should be conducted at the first visit or on admission to the clinical setting, and ongoing inspection of the skin should be incorporated into an integrated and documented daily care regimen to ensure changes in health status/skin integrity of patients are identified (Strong 35 ).
CPG recommendations on diagnosing VLUs
Eleven CPGs 21–22,24,26–27,29,31 –33,36–37 had six major recommendations on VLU diagnosis (Fig. 4 and Supplementary Appendix Table SA3) as follows:
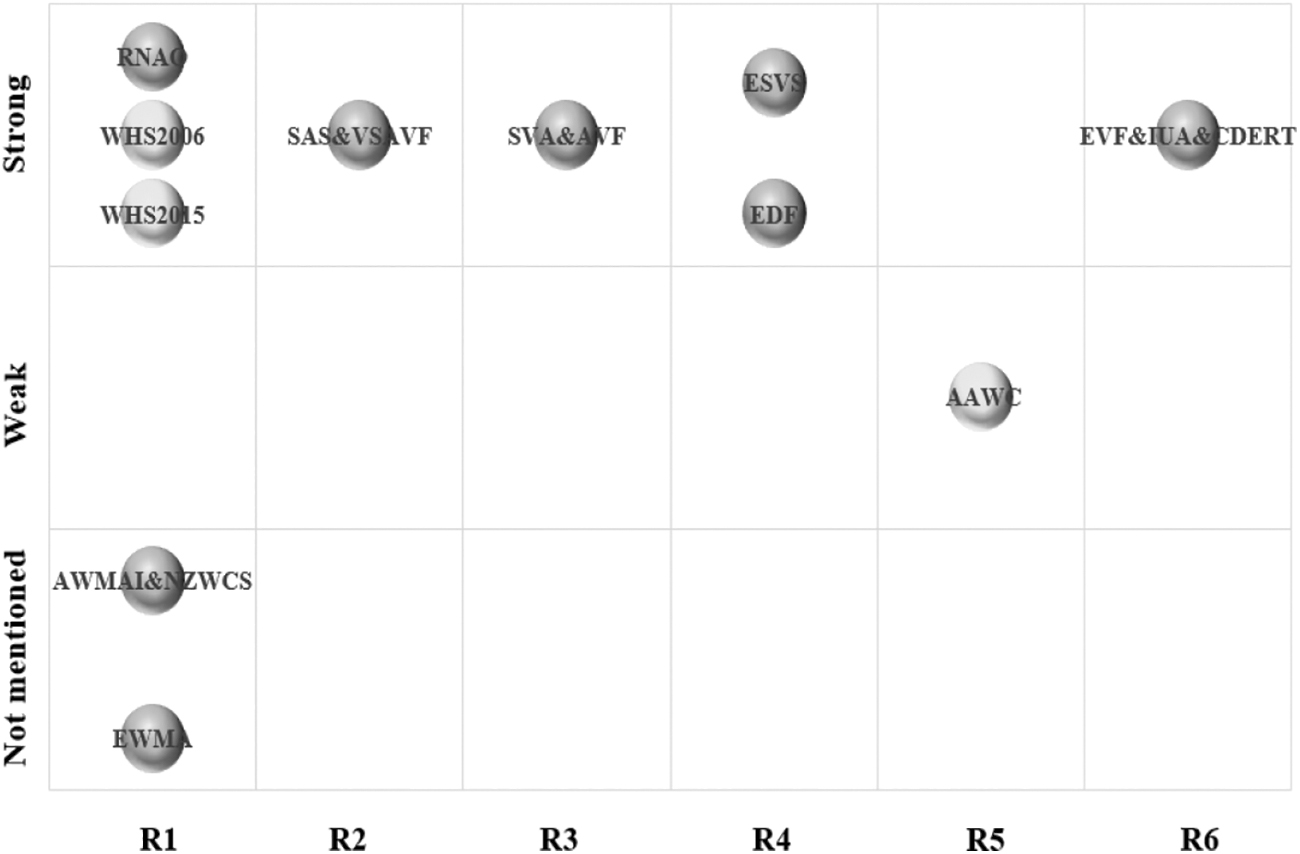
CPGs recommendations on VLU's diagnosis.
Measurements of ankle–brachial pressure index (ABPI) (Strong, 21–22,32 Not mentioned 24,33 );
Duplex scanning for follow-up of patients after venous procedures who have symptoms or recurrence of varicose veins (Strong 26 );
Selective computed tomography venography, magnetic resonance venography, contrast venography, and/or intravascular ultrasound are recommended for patients with suspected venous leg ulceration (Strong 27 );
Duplex Ultra Sound examination should be the gold standard in the diagnosis of Chronic Venous Disease (Strong 29,37 );
Differential diagnosis or seeking appropriate consultation should be made to determine the cause of ulceration (Weak 31 );
Hand-held Doppler or color flow duplex ultrasound examination (Strong 36 ) could be used for diagnosing VLUs.
CPG recommendations on VLU's therapeutic strategies
Eighteen CPGs 21–22,24 –39 provided six recommendations (Fig. 5 and Supplementary Appendix Table SA4):
CPGs recommendations on VLU's therapeutic strategies
Early use of compression (Strong, 21–22,24,26–27,38,39 Weak, 29 Not mentioned 28–29,31,33–34,36–37 );
Therapeutic trial of appropriate compression and wound bed moisture control before cellular therapy (Strong 27,39 );
Routine ultrasound therapy should not be applied for venous leg ulceration (Strong, 27 Not mentioned 32 );
Choice of wound dressings should not be provided for venous leg ulceration (Not mentioned, 28 –33 Strong, 35 Weak 39 );
Cytokine growth factors are yet to demonstrate their effectiveness in treating VLUs (Strong 32 ).
We suggest venoactive drugs in addition to compression for patients with pain and swelling due to chronic venous disease, in countries where these drugs are available (Strong, 29 Weak 26,36 ).
DISCUSSION
This is the first systematic review of CPGs for VLUs using AGREE II and RIGHT checklist. The review investigated the gaps of assessment, diagnosis, and treatment of VLUs using an evidence map (Supplementary Appendix Table SA5). A total of 19 CPGs were identified in the current international review of CPGs for VLU care, and the quality of the identified CPGs' varies. Furthermore, there were inconsistent scores for each domain of the CPGs. All the CPGs had high-quality scores regarding the scope and purpose, whereas all the CPGs had lower-quality scores regarding editorial independence. The scores of domain five (applicability) were also low. Multiple recommendations of VLUs for most CPGs were consistent. However, there were also some conflicting recommendations in the CPGs for VLU care.
Many CPGs provide varied recommendations for VLU evaluation. Regular ulcer assessment was crucial in monitoring treatment effectiveness and healing goals. Regular ulcer assessment was recommended by five CPGs (RNAO, WHS2006, Clare, Williams, and EWMA): that assessment and clinical investigations should be undertaken by a health care professional(s) trained and experienced in leg ulcer management. The health care professional assessing the patient with a VLU must be experienced in leg ulcer management. This is because the type of leg ulcer diagnosis should be based on a thorough clinical history and physical examination. Therefore, this will help to identify the underlying cause of the leg ulcer and any associated diseases.
In addition, it is expected that individual nurses have appropriate education and experience to know that there are different types of ulcers, including venous, arterial, diabetic, rheumatoid, or malignant. The patient should be referred to an appropriate specialist in case of doubt over the etiology of the ulcer. Furthermore, RNAO CPG suggested routine assessment at 6-month intervals for resolving and healing VLUs. 21
This assessment must be performed by a vascular surgeon, angiologist, or dermatologist for vascular evaluation or, in cases of long-term healing failure, by a dermatologist for a further diagnostic workup to rule out other differential diagnoses. 33 SAS&VSAVF CPG recommends the assessment of clinical outcomes after therapy for varicose veins and more advanced chronic venous disease using the revised Venous Clinical Severity Score (VCSS). VCSS is a valuable tool for assessing change of clinical symptoms of venous disease over time with or without intervention. 38 Recently, VCSS was revised to increase its sensitivity and value in interpreting the language of venous disease. Emphasis has been placed on updating terminology, simplifying the application, and eliminating ambiguity, with special consideration given to the use of language from quality-of-life instruments. 39
At the same time, the CIVIQ, AVVQ, and VEINES-QOL were used to measure the health outcomes in patients with varicose veins. A systematic review 40 of the literature about quality-of-life scales in chronic venous disorders comprising leg ulcers reported that CIVIQ and VEINES-QOL emerged as being thoroughly validated instruments.
It was recommended that venous procedural outcomes, including impact on VLU healing, be assessed. Studies of the venous procedural outcome predict which patients may benefit from surgery, while successful treatment of leg ulcers requires an interdisciplinary team to make the correct diagnosis, assess vascular supply, and identify other modifiable factors to optimize healing. 41 ICSI CPG recommended that wound assessment should describe the extent of necrotic tissue in the wound bed (T), presence of inflammation or infection (I), evidence of any surrounding maceration (M), and the edge (E) of the ulcer. It was also recommended that validated measures that include wound depth should be used.
A comprehensive and detailed wound description should be provided to document the healing process better. Based on the frequency of wound assessment, Health service CPG recommended more frequent (greater than twice daily) skin assessments at the skin device interface in patients vulnerable to fluid shifts and/or exhibiting signs of localized or generalized edema should be conducted.
Furthermore, WHS 2015 recommended that if there is no significant wound improvement within 3–6 weeks of initiating a treatment plan, reevaluation of the patient and consideration of other treatment options should be considered.
VLU's diagnosis plays a supporting role in the management and care of VLUs. Five CPGs (RNAO, WHS2006, AWMAI&NZWCS, WHS2015, and EWMA) recommend that the ABPI is an invaluable tool for assessing the severity of the peripheral arterial disease (PAD). The ABPI is widely used in clinical practice as a noninvasive method to detect the presence and severity of PAD. In addition to visual inspection of the ulcer, many studies highlight the importance of making an objective etiological diagnosis by measuring the ABPI, pedal pulse palpation, and a thorough clinical and physical assessment.
RNAO CPG recommended that trained practitioners should do Doppler ultrasound measurements of ABPI. Furthermore, other CPG recommended that clinicians must have sound practical knowledge and experience in using ABPI. A systematic review 42 suggested that the result is reliable when used for measurements by a trained practitioner. Vascular assessment for ABPI is recommended for ulcers in the lower extremities before debridement to rule out a vascular compromise.
In the absence of chronic venous insufficiency and an abnormal ABPI (greater than 1.2 or less than 0.8), arterial etiology should be considered, and a vascular opinion should be sought for further medical assessment. ABPI should be recorded and performed continuously in patients with first or recurrent leg ulcers. The cause of ulceration was determined by differential diagnosis or appropriate consultation.
SAS&VSAVF guideline recommended duplex scanning for follow-up of patients after venous procedures who had symptoms or recurrence of varicose veins. Currently, dual-light scanning is the gold standard for diagnosing patients with varicose veins, given the slight difference in diagnostic accuracy compared with venography. 43 ESVS and EDF guidelines also recommended that duplex ultrasound examination be considered the gold standard in diagnosing Chronic Venous Disease. In addition, SVA&AVF CPG recommended selective computed tomography venography, magnetic resonance venography, contrast venography, and/or intravascular ultrasound in patients with suspected venous leg ulceration. EVF&IUA&CERT recommended a hand-held Doppler or color flow duplex ultrasound examination to evaluate venous leg ulceration.
Therefore, physicians should choose the appropriate clinical diagnostic tool based on the condition of the patient.
Multiple adjunctive therapies have been proposed to treat wound healing in patients with VLUs. SVA&AVF, RNAO, ESVS, AWMAI&NZWCS, SAS&VSAVF, ICSI, ESVS, AAWC, WHS2006, EWMA, EVF&IUA&CDERT, and EDF CPGs recommended early use of compression as a comprehensive wound management program for VLUs. An ABPI measurement must be done before the commencement of compression therapy. 44 The pressure at the ankle should be between 30 and 40 mmHg (less than 30 mm Hg in case of mixed ulcers). In addition, selecting the type of compression must consider the size of the ulcer, the appearance of the wound, the presence of leg deformities, the volume of edema, and the general condition of the patient in daily practice. However, there was no specific evidence to validate the cost of compression in healing patients with VLUs.
There is a need for further research to determine the cost-effectiveness of compression in healing patients with VLUs. The guidelines also recommend management measures to prevent the recurrence of venous ulcers, including wearing compression stockings, regular follow-up to monitor ABPI, discouragement of self-treatment with over-the-counter preparations, and avoiding accidents or leg trauma.
SVA&AVF guidelines recommended that therapeutic trials of appropriate compression and wound bed moisture be controlled before cellular therapy. Cells play a role in normal wound healing, and their presence supports healthy healing physiology, playing a critical role in primary wound healing by regulating immune responses and inflammation. 45
Dressings play a supporting role in the care of VLUs. ESVS guideline recommended that choice of wound dressings should not be provided for venous leg ulceration. The results of the previous study 46 demonstrated that the type of dressing applied beneath compression was not shown to affect ulcer healing. The results of the meta-analysis showed that applying hydrocolloid dressings beneath compression produced no benefit in terms of ulcer healing compared with applying simple low adherent dressings. No conclusive recommendations can be made as to which type of dressing is most cost effective. Decisions on which dressing to apply should be based on the local costs of dressings and the preferences of the practitioner or patient. However, the guideline found no specific dressing selection and cost analysis.
At the same time, there was insufficient evidence to prove that any wound dressing was superior to another in treating ulcers. There is a need to determine which dressing is the better choice for healing wounds.
Limitations and strengths
The strengths of this review are: This is the first study to systematically review CPGs on VLU care and generate an evidence map. The evidence map provides high-quality evidence for decision makers by systematically presenting and analyzing the evidence related to lower extremity venous ulcers while identifying research gaps to guide future research. Furthermore, we critically assessed the quality of CPGs using a combination of AGREE II tool and the RIGHT checklist to identify possible deficiencies in different areas and aspects for further improvement.
This study had several limitations. First, only CPGs published in English were included, limiting the number of entries. Second, despite a relatively comprehensive literature search, some CPG may not be identified. Therefore, it is likely that not all available CPGs were identified and included. Third, assessing the methodological and reporting quality of CPG using the AGREE II tool and RIGHT checklist is a subjective process. There is a possibility of bias, although four researchers independently assessed the eligibility of CPG and used ICC scores to check their reliability and consistency. Last, this study classified the quality and strength of evidence for venous ulcer CPG recommendations using a different grading system based on different coding systems. Therefore, the results in the evidence map should be interpreted with caution.
CONCLUSIONS
In this study, the evidence map included 19 moderate- to high-quality CPG to provide CPG recommendations for evaluating, diagnosing, and treating VLUs. In total, 24 major recommendations were summarized. These recommendations were generally consistent. However, evidence for some clinical issues remains lacking. There is a need for more research on the evaluation, diagnosis, and treatment of VLUs to produce more evidence-based and high-quality recommendations.
TAKE-HOME MESSAGE
This evidence map provided new perspectives in the presentation of evidence.
In addition, the evidence map collected and evaluated the characteristics of published CPGs.
In total, 24 major recommendations were summarized. These recommendations were generally consistent.
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
None declared. No funding was received for this article.
AUTHOR DISCLOSURE AND GHOSTWRITING
No competing financial interests exist. No ghostwriters were used to write this article.
ABOUT THE AUTHORS
Supplementary Material
Supplementary Appendix Table SA1
Supplementary Appendix Table SA2
Supplementary Appendix Table SA3
Supplementary Appendix Table SA4
Supplementary Appendix Table SA5
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.