
Abstract
Objective:
This study is the first prospective within-patient self-controlled research seeking to investigate the safety and efficacy of 595 nm pulsed-dye laser (PDL) for the treatment of cleft-lip scars.
Approach:
This prospective, randomized, self-controlled study is based on the clinical records of the patients who received laser-assisted treatment due to bilateral cleft-lip scars. The bilateral scars were randomly assigned to the 595 nm PDL group with five consecutive sessions at 2-week intervals or control group in a blinded manner of evaluators, with subsequent follow-up for 6 months after the final treatment. Clinical efficacy and safety outcomes were evaluated by Vancouver Scar Scale (VSS), Patient Scar Assessment Questionnaire (PSAQ), and other objective evaluations.
Results:
A total of 18 patients were included. The 595 nm PDL-treated sides showed statistically significant improvement in VSS after treatment at follow-up compared with the baseline (p < 0.05). Interestingly, the 595 nm-PDL-treated side achieved significantly better improvement in scar pigmentation and pliability (p < 0.05). Though there was statistically significant difference between two groups (p < 0.05), the gap in overall PSAQ is not obvious. And comparison by area and coloring evaluation (E/M index) also suggests that the responses of scars to treatment by PDL were slightly improved (p < 0.05).
Innovation and Conclusion:
It is the first time to apply the 595nm PDL for cleft-lip scars. It would be a better choice for the early treatment of red scar with proliferative tendency after cleft-lip surgery.

INTRODUCTION
Cleft lip and palate (CLP) are one of the most common birth defects, and are repaired by surgery at an age of ∼3–6 months. 1 Although surgical repair can solve the appearance and partial functional defects of patients with CLP, postoperative scarring is still a negative factor affecting the operation effect. 2 It has been reported that any trauma that reaches the dermal reticular layer will develop scars. With an incidence as high as 5%–37%, hypertrophic scars are more common in Asians than in Caucasians. 3 In China, 91.4% of deep burn wounds and 44.6% of surgical incisions will develop hyperplastic scarring postoperatively. 4
Moreover, cleft-lip scars are at increased risk of scar hypertrophy due to the repetitive movements of the upper lip compared with the sites of other scars. 5 Severe scar contracture will lead to severe deficient sagittal development in the mid-face, which performs as a class III malocclusion. 6,7 In addition, it has a negative effect on the psychology of these patients. 8,9
Therefore, there has been a continuing effort to treat scars after cleft-lip surgery in an appropriate way to improve their appearance. Although silicone gel has been proven to deliver effective improvements with lower complication rates, they may still cause rashes and eating by mistake especially in children. And it is also difficult to insist on using it for a long time.
The 595-nm pulsed-dye laser (PDL) is a method based on the principle of selective photothermolysis, which has been widely used to treat port-wine stain (PWS) lesions. The method involves the use of light of an appropriate wavelength that is absorbed well by the target issue vessel and has sufficiently short pulse duration to spatially confine the thermal injury while producing a specific vascular and collagen fiber injury without damaging the surrounding normal tissues.
It has already been used in chest scar, which achieved great appearance improvement. 10,11 On the other hand, it was confirmed that the number and size of blood vessels of lip scars and the expression of vascular endothelial growth factor were significantly higher than those of normal skin. 12 This shows that abnormal blood vessels could be closely related to the pathophysiology of lip scars. This technique may inhibit scar hyperplasia by introducing a safe treatment procedure for damaging the dermis capillaries and fibroblasts.
However, up to now, no sufficient prospective studies have examined the effectiveness of the 595 nm PDL for the treatment of cleft-lip scars. This study is the first prospective within-patient self-controlled research seeking to investigate the safety and efficacy of 595 nm PDL for the treatment of cleft-lip scars.
MATERIALS AND METHODS
Study design and data collection
This study is based on the records of the patients treated for bilateral cleft-lip scars using a 595 nm PDL laser at the department of Oral & Cranio-Maxillofacial Surgery between June 2020 and June 2022. This study was conducted prospectively from data obtained for clinical purposes and was in accordance with the Declaration of Helsinki.
The study protocol was approved by the Research Ethical Review Committee of Shanghai Ninth People's Hospital (SH9H-2021-T357–2). All treatment procedures performed were part of the routine care, in which patients were verbally informed regarding the clinical procedure. Treatment was completed after the patient's legal representative had read and signed an informed consent form. The patients were evaluated by different groups of observers at each follow-up.
Study population
The clinical records of patients who matched the described inclusion criteria were selected for the retrospective investigation. The analyzed data included postoperative wound healing, scar assessment and postoperative pain perception.
The following are the inclusion criteria: Patients under symmetrical bilateral cleft-lip repair Patients without any systemic condition Treatments performed and followed up by the same operator
The bilateral scars for each patient were of the same condition and randomly assigned to be treated with 595-nm PDL or the control and were followed up 6 months after their final sessions. A random allocation was created using block randomization blind envelope to assign the treatment modality of each side. Because of the lack of previous data, the sample size was determined based on feasibility considerations rather than a power analysis.
Treatment protocol
Initially, the patients' skin was cleaned before treatment. For the PDL (Vbeam Perfecta PDL, Syneron-Candela, American) treatment, half a pulse duration of 0.45 ms with a fluence of 4–6 J/cm2 was delivered with cryogen cooling at a spot diameter of 10 mm. The spot overlap rate was 20%, and the dynamic cooling device was set at 20/20 ms.
The target scars underwent five laser treatments with a 2-week interval, and the first session started 1 week after the removal of stitches. The therapeutic method was determined based on the doctor's clinical experience. Before treatment, all wounds were checked to ensure that they were free of swelling and exudation. In addition, it is also recommended that all patients avoid sun exposure.
Clinical assessment
All patients were photographed using a digital camera (EOS 600D; Canon, Tokyo, Japan) under identical lighting conditions at pretreatment and up to 6 months after treatment. Efficacy of scar improvement was assessed by Vancouver Scar Scale (VSS), 13 Patient Scar Assessment Questionnaire (PSAQ, Table 1), in which low was very satisfactory. 14
Patient Scar Assessment Questionnaire
Small scores reflect good scar quality.
The primary outcome was the change in the VSS grading scale at each follow-up visit. The PSAQ documented their degree of satisfaction and symptoms. Blanching of the treated scar was assessed by three groups of plastic surgeons in a fully blinded manner. Moreover, the scar area, erythema, and the scar color index were also evaluated by 3dMD photogrammetry system (3dMD, LLC, American), VISIA (Canfield Scientific, American), and skin spectrophotometer (SV; Cyber Derm, New Darlington, PA) respectively.
The skin color was presented as E index (red)/M index (black). EI reflects the condition of facial capillaries and intuitively reflects the degree of inflammation. Adverse responses after treatment (blistering, purpura, or crusting) and side-effects (change of pigmentation, scar formation, or infection) were also monitored.
Statistical analysis
The obtained data were imported into GraphPad Software for statistical analysis, the measurement data were expressed as mean standard deviation (
RESULTS
Patients
Eighteen of the 20 patients completed the research. Two patients were lost to follow-up because of COVID-19. Twelve males and 6 females aged 6 months to 31 years were ultimately enrolled. There was no significant difference in mean VSS score at baseline between the two sides (5.50 ± 0.96 vs. 5.78 ± 1.09, p = 0.462 > 0.05). During the treatment period, there were no serious complications such as wound disruption, hyperpigmentation or hypopigmentation, blistering, or ulceration.
Only one male patient developed transient purpura, which recovered after 1 day. The details are shown in Table 2 . In our study, eight people have bilateral cleft lip with bilateral alveolar cleft. We statistically analyzed the VSS score of the patients with or without alveolar cleft before treatment, and found that there was no significant difference in scar ( Table 3 ).
Demographic information of the 18 patients
The Vancouver scar scale scores of two groups (alveolar cleft and no alveolar cleft) before treatment
Clinical evaluation
At the final follow-up visit, the 595 nm-PDL-treated scar side demonstrated superior efficacy compared with the control side after five sessions of treatment each, whereas both sides showed significant improvement in VSS score from baseline (Table 4 ). At the first follow-up, the relative changes of VSS scores from baseline in laser group and control group were 0.707 ± 0.075 and 1.010 ± 0.076 respectively, and the differences were statistically significant (p < 0.05), which was similar in the other two follow-ups.
The relative changes of Vancouver scar scale scores from baseline were compared between the two groups at each follow-up
Interestingly, two out of four aspects (pigmentation and pliability) improved more obviously after laser treatment. The levels of decrease in VSS from baseline were significantly different between the two regimens at the follow-up visit (p < 0.05, Fig. 1).
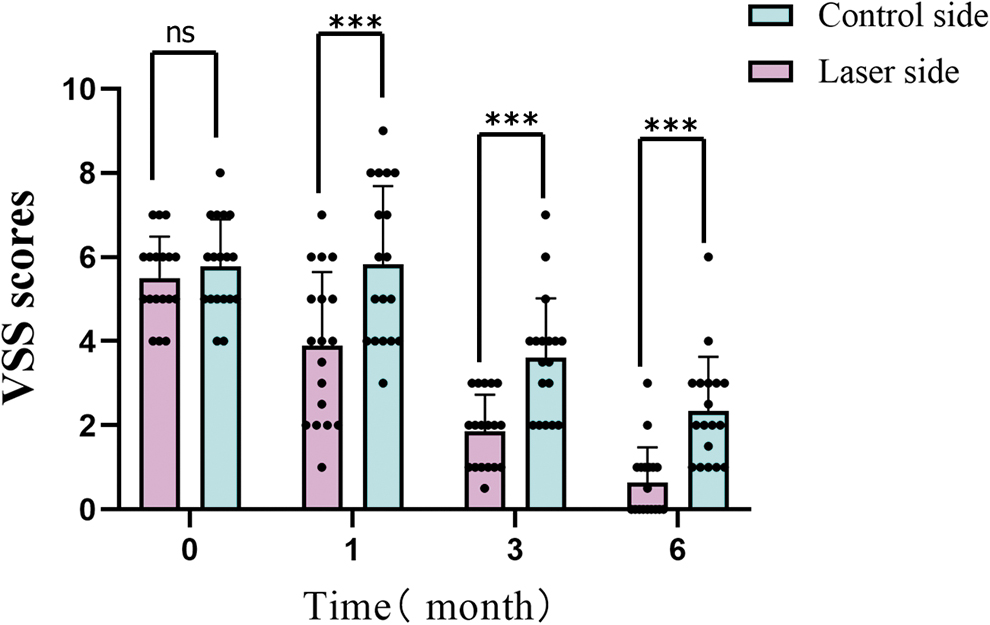
Comparison of decline trend (total VSS scores) charts between the two groups at different follow-up time (0 represents the baseline; 1,3,6 represents the 1-month, 3-month, and 6-month follow-up after the last treatment (ns indicates no significant difference with the control group, p > 0.05; ***indicates significant difference with the control group, p < 0.001). VSS, Vancouver scar scale.
For the improvement of cleft-lip scar, patients were slightly satisfied with 595 nm PDL treatment than the control side (mean ± SD) of satisfaction scores (1.89 ± 0.96 vs. 3.94 ± 1.35; p < 0.05; Fig. 2). As for the scar area, the average was significantly smaller on the laser side than on the control side (24.20 ± 10.95 mm2 vs. 31.19 ± 14.51 mm2 respectively; p < 0.05; Fig. 3). There was a significant difference in the comparison of the EI, whereas there was no significant difference in MI (Fig. 4).
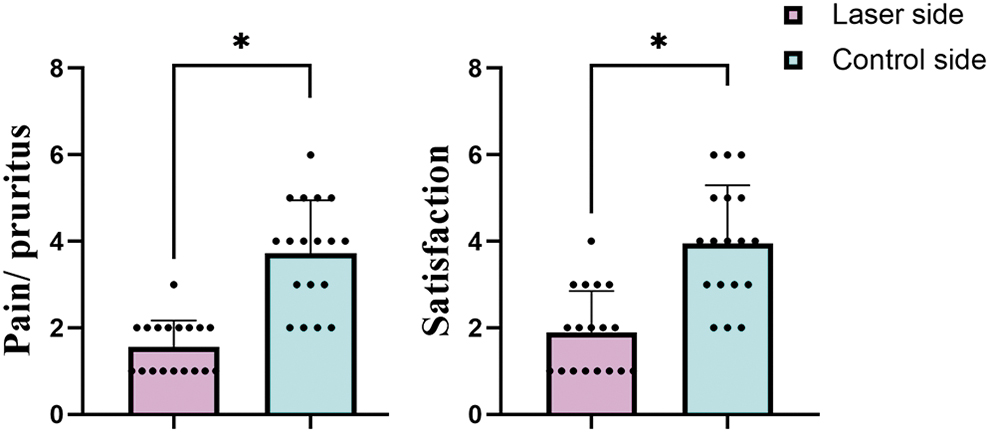
The PSAQ scores of two groups at the 6-month follow-up (*indicates significant difference with the control group, p < 0.05). PSAQ, Patient Scar Assessment Questionnaire.
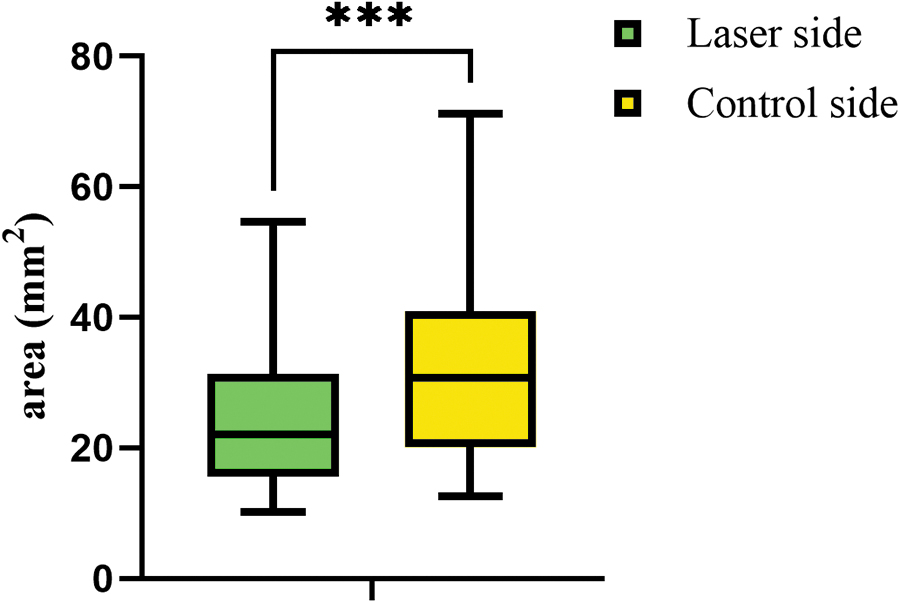
Comparison of the surface area between the two groups (***indicates significant difference with the control group, p < 0.001).

Comparison of scar color between two groups.
Typical case
A 20-year-old male with bilateral cleft-lip nasal deformity underwent a secondary operation. Figure 5 also demonstrates the improvement in the appearance of scar tissue after laser therapy. The right lip scar was treated with a PDL 5 times after removing the sutures. Although some improvement was observed in control side, a slightly prominent improvement in pigmentation and pliability was noted on the laser-treated side of the scar.

Clinical photographs revealed the improvement of cleft-lip scarring by 595 nm PDL treatment.
DISCUSSION
Scarring is an important complication that has physical, psychological, and cosmetic impacts on patients, especially for those with cleft lip. There is a tendency toward hyperpigmentation and scar formation after skin injury, with a greater risk in Asians. It is suggested that scar treatment should be initiated earlier in Asians to prevent the proliferation of pathological scar. 15
Treatment of scars currently includes surgery, corticosteroids, pressure garments, tamoxifen, and interferon therapy, with different treatment regimens resulting in varying degrees of recurrence. Most of the literature on keloid treatment suggests that a high rate of recurrence (50%–70%) is expected. A more effective method is required for inhibiting scar hyperplasia. 16 –18
JAMA expert consensus believes that 6 months after surgery is the early stage of scar hyperplasia, and it is also the time when scars enter maturity stage. 19,20 Intervention when the scar is not yet stable can significantly shorten the process of unstable stage of scar and improve the prognosis of scar. The early starting point was that the wound healing and re-epithelization were basically completed.
Epithelization usually occurs about 14 days after the skin is injured. At this time, new blood vessels react vigorously, and the density of blood vessels is about 7.5 times that of normal tissue. 21 When the blood vessels cannot effectively resolve, hypertrophic scars will be caused. Therefore, laser therapy was selected in this study for about 1 week after suture removal.
At this stage, the scar was in the proliferative phase, and the inflammatory reaction had subsided, with formation of granulation tissue, proliferation of a large number of capillaries, active proliferation of fibroblasts, and formation of a large number of collagen. The tissue was well tolerated, and it was suitable for PDL treatment at 595 nm, and the patient could tolerate laser.
Given the developments in laser technology, the application of diverse lasers shows remarkable improvements in those treatments. Currently, the PDL is the best choice for early scar treatment, improving scar vascularity, color, height, texture, and pliability. In 1995, a 585 nm PDL was first applied to treat the red hypertrophic scar of the chest and was found to relieve congestion, reduce scar thickness, and improve scar softness, all of which resulted in significant improvements in clinical parameters. 22
The 595 nm PDL selectively photothermolyzes targeted vessels with minimal damage to surrounding tissue, producing microvascular destruction and leading to ischemia, which may deprive a scar of nutrients or may impair the proliferation of fibroblasts. 23,24 It is considered to be the first choice for the treatment of PWS. However, there is a lack of high-level clinical evidence for early intervention treatment of scars.
Moreover, 595 nm PDL had less adverse reactions, painless, noninvasive and was convenient for nursing. To alleviate postoperative discomfort, a uniform cold air cooling level was used during the treatment sessions throughout our study. Therefore, 595 nm PDL was a safe technique to treat cleft-lip scars.
In this randomized, self-controlled study, the treated side showed significantly better improvement than the control side at the follow-up visit (p < 0.05, Table 4). In addition, PDL treatment was associated with a significant reduction in scar height (0.08 ± 0.26 vs. 0.67 ± 0.57, p < 0.001) and pliability (0.42 ± 0.49 vs. 1.31 ± 0.52, p = 0.003).
Degrees of subjective satisfaction for associated indications (pain and pruritus) were also higher on the treated side. A significant difference of EI and skin color between the two groups was observed after the last visit (p < 0.05). During the follow-up, we also found that the scar area on the treatment side was significantly smaller than that on the control side, indicating that 595 nm PDL therapy could effectively inhibit the hypertrophy of scars (p < 0.001).
Until now, the majority of published studies have used the VSS to assess the effect of various treatment modalities for scars. However, detailed meaningful differences could be missed using only a comparison of post-treatment VSS scores. Therefore, objective evaluation was added to this study to better evaluate the cicatrix.
STUDY LIMITATIONS
There are some limitations in this study. First, the number of enrolled patients is smaller. Second, as a novel technology, longer-term efficacy should be followed. Third, in this work, we did not address the relationship between alveolar cleft and biomechanical tension and scar in the later period. This constitutes a serious weakness.
INNOVATIONS
Scars are one of the most common complications after cleft-lip surgery. The 595 nm PDL has been regarded as the gold standard of the treatment for PWS. However, the evidence for early scarring treatment has so far been inadequate. It is the first time to apply the 595 nm PDL for cleft-lip scars after surgery.
KEY FINDINGS
In the context of the limitation of this study as addressed, the following findings are of interest:
595 nm pulsed dye laser can achieve certain curative effect in the treatment of postoperative scar of cleft lip, which is more advantageous in the pigmentation and pliability of scar.
The 595 nm pulsed dye laser would be a better choice for bright red scars with proliferative tendency.
Meanwhile, the 595 nm pulsed dye laser is noninvasive, convenient for nursing, and worthy of promotion and application in clinic.
Footnotes
AUTHORs' CONTRIBUTION
C.H.S. analyzed and interpreted the patient data regarding the scars treated by 595 nm PDL and the transplant and was a major contributor in writing the manuscript. ZXR analyzed the data. P.H., S.L.Y., and Z.G.Y. performed the laser treatment of the scars. C.M. operated the cleft-lip repair. All authors read and approved the final manuscript.
AUTHOR DISCLOSURE AND GHOSTWRITING
The authors have no conflict of interest to declare.
FUNDING INFORMATION
This work was supported by the Clinical Research Program of the 9th People's Hospital affiliated to Shanghai Jiao Tong University School of Medicine (Funding number: JYLJ202001).
ABOUT THE AUTHORS