
Abstract
Significance:
Chronic diabetic wounds on the lower extremities (diabetic foot ulcers, DFU) are one of the most prevalent and life-threatening complications of diabetes, responsible for significant loss of quality of life and cost to the health care system. Available pharmacologic treatments fail to achieve complete healing in many patients. Recent studies and investigational treatments have highlighted the potential of modulating wound pH in DFU.
Recent Advances:
Data from in vitro, preclinical, and clinical studies highlight the role of pH in the pathophysiology of DFU, and topical administration of pH-lowering agents have shown promise as a therapeutic strategy for diabetic wounds. In this critical review, we describe the role of pH in DFU pathophysiology and present selected low-molecular-weight and hydrogel-based pH-modulating systems for wound healing and infection control in diabetic wounds.
Critical Issues:
The molecular mechanisms leading to pH alterations in diabetic wounds are complex and may differ between in vitro models, animal models of diabetes, and the human pathophysiology. Wound pH-lowering bandages for DFU therapy must be tested in established animal models of diabetic wound healing and patients with diabetes to establish a comprehensive benefit-risk profile.
Future Directions:
As our understanding of the role of pH in the pathophysiology of diabetic wounds is deepening, new treatments for this therapeutic target are being developed and will be tested in preclinical and clinical studies. These therapeutic systems will establish a target product profile for pH-lowering treatments such as an optimal pH profile for each wound healing stage. Thus, controlling wound bed pH could become a powerful tool to accelerate chronic diabetic wound healing.


SCOPE AND SIGNIFICANCE
Diabetic foot ulcers (DFUs) are one of the most debilitating complications of diabetes. As the standard of care is based on unspecific wound treatment and fails to achieve complete healing in many DFU patients, there is a need for new molecular therapies. As our understanding of the complex diabetic wound healing pathophysiology is deepening, wound pH has emerged as a promising therapeutic target in DFU. In this critical review, we describe the role of wound pH in the pathophysiology of diabetic wound healing and critically discuss selected strategies for wound pH management.
TRANSLATIONAL RELEVANCE
Recent preclinical and clinical studies using pH-lowering strategies to treat stalled and infected diabetic wounds have shown promising results. However, pH-lowering strategies need to be further investigated to confirm their therapeutic potential. Furthermore, the addition of pH-lowering agents to available wound dressings might be a simple, effective, and inexpensive way to enhance wound dressing performance.
CLINICAL RELEVANCE
A large proportion of patients with DFU do not respond to standard of care. As our understanding of the pathophysiology of diabetic wounds deepens, wound pH has emerged as a molecular target for DFU therapy. The acidification of the wound bed has shown promise for wound healing acceleration and infection control in preclinical and clinical studies. Furthermore, this strategy may reduce the use of antibiotics and could be used for other difficult-to-treat wounds.
BACKGROUND
Diabetes mellitus is an increasingly prevalent chronic metabolic condition characterized by hyperglycemia, resulting from reduced sensitivity or incapability to produce insulin. 1,2 While diabetes can cause several different long-term complications, DFU is one of the most debilitating and prevalent and is responsible for a significant loss of quality of life. 3 DFU is experienced by up to 34% of patients with diabetes with a recurrence rate of 60% after 3 years. 3 Moreover, due to complications such as infections of the wound in more than half of cases, DFU requires amputation in 20% of moderate or severe cases, and increases mortality by a 2.5 times fold. 3 Also, effective treatments of DFU have a significant cost to the health care system, with nearly 80 billion USD attributable to DFU in 2017 in the United States. 4
Despite our deepening understanding of DFU pathophysiology, standard of care of DFU therapy remains unspecific (wet gauze, debridement, antibiosis in case of infection). 5 Currently, the only Food and Drug Administration (FDA)-approved pharmacologic DFU treatment is becaplermin, a recombinant human platelet-derived growth factor (PDGF)-loaded hydrogel, which showed limited clinical efficacy. 6,7 However more recently, new systems such as sucrose octasulfate dressings, autologous leucocyte/platelet/fibrin patches, or the use of negative pressure wound therapy, are now recommended as adjunct therapies to DFU standard of care by the International Working Group on the Diabetic Foot. 5
While showing promising results, the potential impact of these adjunct treatments on diabetic wound pH is not well understood and warrants further investigation. With regard to the high disease burden and the large proportion of nonresponders to standard DFU wound care, new molecular targets are needed to improve wound healing rates in patients with DFU. 5
The pathophysiology of DFU is complex and involves immune pathways and hyperglycemia-associated complications, such as peripheral neuropathies and microvascular diseases. 5 Recent studies have highlighted the importance of wound bed pH in diabetic wound healing and in other types of chronic wounds. 8 –11 In acute wounds, pH moves from neutral to acidic, reaching the natural pH of the skin ranging from pH 4.5 to 5.3 along with the healing process, suggesting that pH might be a potent tool to predict wound healing status (Fig. 1). 9,12,13
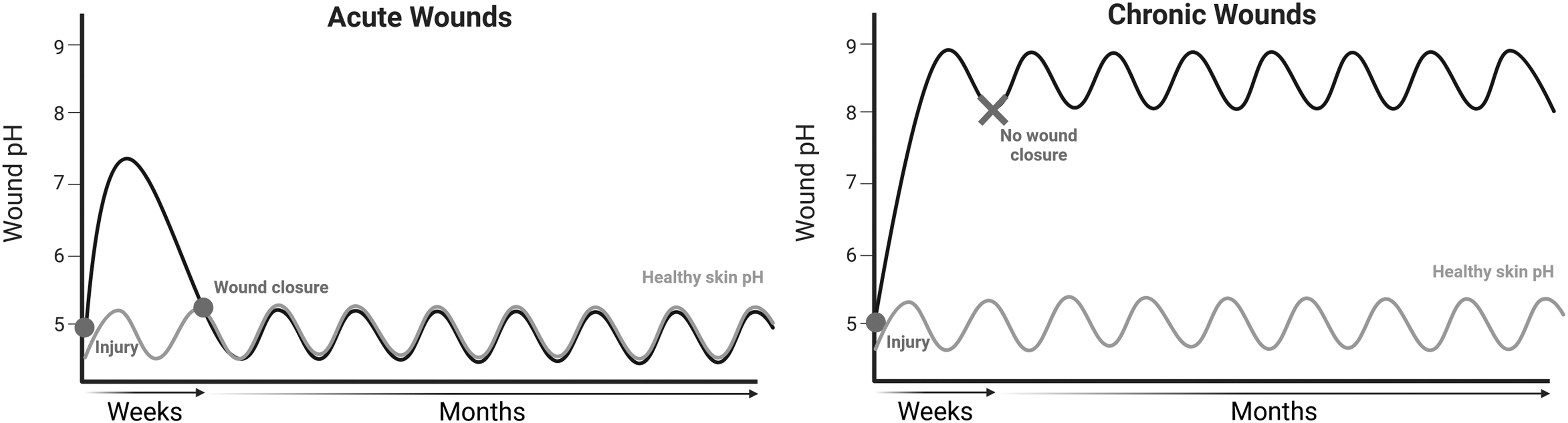
Wound pH values of acute and chronic wounds over time. Chronic wound pH remains alkaline after several weeks with no wound closure, while acute wound pH decreases over a few weeks until wound closure occurs.
However, the pH of chronic diabetic wounds has been reported to typically stall an alkaline range of 7.15–8.9, even sometimes exceeding 9 in clinical studies; and higher values are likely correlated with more severe wound stages and infection (Fig. 1). 9,10,14,15 For example, over a 12-month period, Dissemond et al. measured the pH of chronic wounds from several etiologies in 49 patients, including 12 diabetic patients. In diabetic patients, wound pH ranged from 6.42 to 8.17, with a mean value of 7.39. 11 Another study investigated the pH of DFU wound exudate in 55 patients and found pH values ranging from 6.5 to 8.5. 14 Moreover, wound pH strongly increased with time in full excisional wounds of diabetic mice. 16 Also, wound bed acidification improved healing rates in diabetic wounds in both animal model and humans (see Wound pH-modulating therapeutic and diagnostic systems in diabetic wound healing section below). 12,17
While the role of wound pH in the wound healing process has been investigated since the year 1942, 18 there has been growing interest in wound pH as an etiologic factor and therapeutic target in the last two decades. In this critical review, we will discuss the role of pH in the pathophysiology of DFU and provide a selection of recently reported pH-modulating strategies with preclinical and clinical studies.
Discussion of Findings
Pathophysiology of diabetic wound healing
DFU is related to hyperglycemia-induced systemic complications, such as peripheral neuropathy and peripheral microangiopathy, responsible for the loss of protective sensation and impaired blood flow to the extremities, respectively. 2,3 When these neuroischemic conditions are concurrent with repetitive traumas to the extremities, skin breakdowns can occur leading to difficult-to-treat open wounds. 3
Acute wound healing involves a dynamic process that encompasses coordinate and overlapping phases, namely hemostasis, inflammation, proliferation, and remodeling. 19 –22 Platelets activate the coagulation process that results in the formation of a thrombus. Activated platelets release proteins, which induce migration and adhesion of neutrophils and monocytes. They also release prohealing growth factors such as PDGF and transforming growth factor-β (TGF-β). 19,22 –24 Resolution of the inflammation phase leads to the proliferation phase, where differentiation from proinflammatory M1 macrophages to anti-inflammatory M2 macrophages occurs, leading to stromal cell proliferation, angiogenesis, and formation of granulation tissue. 19 –22
Concurrent with tissue granulation, keratinocytes migrate from the wound edges to completely cover granulation tissue, which leads to wound reepithelialization and thus finalizes the proliferation phase. 22 Finally, the remodeling phase is characterized by normal tissue restructuration and mature scar tissue formation. 19
Due to the complexity of the physiologic process, changes in the wound microenvironment can slow the healing process down and lead to an impaired wound healing process. 2,20,25 In diabetic patients, hyperglycemia and the induced neuroischemic changes are key factors in pathophysiologic alterations in the wound microenvironment, thus leading to wound healing failure, chronicity, and a high risk of infections. 8,25
In DFU, the inflammation phase likely appears to be the most affected one, as DFU is characterized by a persistent low-grade inflammation leading to an unfavorable environment for physiologic wound healing. 6,21 Even when skin is intact, diabetic patients exhibit a proinflammatory baseline state, which results in higher proinflammatory cytokine concentration and more immune cells in the dermis with a higher M1 to M2 macrophages ratio. 6 These immune cells secrete proteolytic enzymes called matrix metalloproteases (MMPs), whose main function is to degrade and reshape the extracellular matrix (ECM). The abundance of immune cells in DFU has been associated with an overactivity of the MMP-9 isotype, therefore, leading to reduced angiogenesis and reepithelialization, and a stalled healing process. 6
Moreover, higher concentration of reactive oxygen species (ROS) in diabetic wounds have also shown to reduce angiogenesis, induce ECM modification, and affect fibroblast and keratinocyte proliferation and migration. 6 Finally, hyperglycemia-induced neuropathies dysregulate the secretion of substance P and other neuropeptides associated with diabetic wound healing. 6,26 As a result, a typical signature of diabetic wounds is an increased ratio of M1 to M2 macrophages, increased levels of proinflammatory chemokines and cytokines, alterations in neuropeptide concentrations, and decreased levels of prohealing growth factors. 27
Role of pH and its management in diabetic wound healing
In the last two decades, there has been a growing interest to study the role of wound pH in diabetic wound healing. 9 Intact skin is slightly acidic with pH ranging from 4.5 to 5.3, due to organic acid secretion from epithelial cells. 13 When the skin is damaged, acute wounds exhibit a slightly alkaline pH as the exposed underlying tissues have a pH of 7.4. 13 Then, the natural skin acidity is restored during the healing process (Fig. 1). 12
However, in contrast to acute wounds, the pH of chronic diabetic wounds increases over time toward alkaline values (Figs. 1 and 2). 11,14,16,28 These increased pH values are likely caused by the chronic inflammation in diabetic patients and the influx of interstitial fluid into nonhealing wounds. 14,27 Moreover, when infected, the wound pH generally becomes more alkaline because of secreted bacterial enzymes such as urease (degrading urea in ammonia) and uricase (degrading uric acid), which increase wound pH. 9 Furthermore, it seems that pH within chronic wounds bed is not homogeneous but presents centripetally increasing pH values, where the center of the wound exhibits higher pH values than the periphery, which is closer to the intact skin. 29
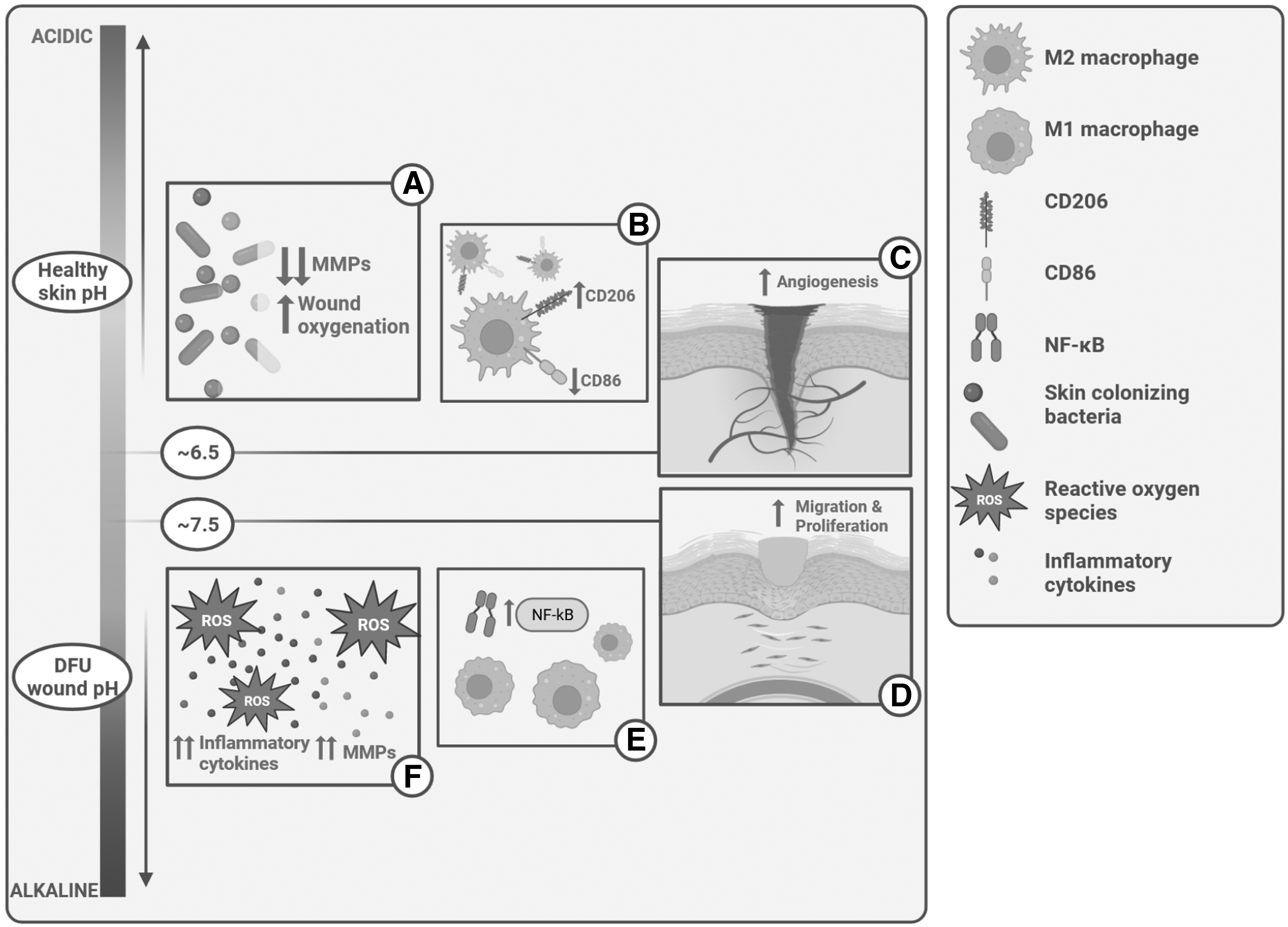
Impact of pH on the pathophysiology of diabetic wound healing. Acidification of the wound significantly reduces MMPs' activity and increases the wound oxygenation through the Bohr effect
Wound oxygenation
The presence of oxygen within the wound site is required for a physiological wound healing process, as it constitutes a vital element for stromal cell growth and ECM synthesis. 9,10,30 In DFU, hyperglycemia-induced micro- and macroangiopathies are responsible for a decreased blood flow, leading to a reduced oxygen supply into the wound bed. 6 The high pH values observed in DFU also play a role in the decreased wound oxygenation due to the Bohr effect, where oxyhemoglobin affinity for oxygen decreases in low pH environment. 30 Therefore, Leveen et al. suggested that acidification of the wound could promote the oxygenation rate by increasing the amount of oxygen released. 30 They showed that a shift in 0.6 units of pH could almost double the available oxygen, allowing a better wound oxygenation to promote wound healing (Fig. 2A). 30
Additionally, a better wound oxygenation could reduce MMP-9 activity, as observed in wounded diabetic mice treated with hyperbaric oxygen therapy. 31 Nevertheless, while hyperbaric oxygen therapy is commonly used for wound healing, its impact on wound pH remains unclear and warrants further investigation.
Infection control
The low pH in the inflammation phase of acute wound healing acts as a protective mechanism against bacterial growth. 32 The alkaline pH values in DFU could therefore be an important contributor to the high infection rate of diabetic wounds, which affects up to half of patients with DFU. 3 While the vast majority of pathogenic bacteria can grow when pH is alkaline, bacterial growth, proliferation, and adhesion are reduced at lower pH values. 17,33 Acidification of the wound pH below 6, therefore, promises to impair microbial growth and potentiate the efficacy of local antiseptics like iodine and silver when incorporated inside wound dressings. 9,17 Furthermore, bacterial end products like ammonia, which is toxic for tissues, can be neutralized by low pH environment, through protonation and formation of nontoxic ammonium. 30
Macrophage activity and differentiation
The most impaired phase of wound healing in DFU is the inflammation phase. DFU is characterized by a higher ratio of M1 to M2 macrophages within the wound site, causing a persistent and inefficient state of inflammation. 6 Acidification of the environment promises to counter this imbalance by promoting macrophages' polarization into the anti-inflammatory phenotype M2. 34 –36 Indeed, an acidic environment induces macrophages polarization into anti-inflammatory M2 phenotype, while an alkaline environment induces polarization into proinflammatory M1 phenotype (Fig. 2B, E). 34 –36
In addition, acidification of the wound site may reduce inflammation by decreasing tumor necrosis factor-α (TNF-α) secretion. 9,35 While the mechanism behind acid-induced M2 polarization in not fully understood, it is thought to be attributable to the activation of pH-sensing G protein-coupled receptors (GPR), like GPR4 and GPR65, which leads to increased expression of cyclic adenosine monophosphate (cAMP) and inducible cAMP early repressor. 34,37 Based on these findings, wound acidification may favor macrophage polarization into the M2 phenotype and thus promote the resolution of the inflammation phase.
Activity of endothelial and stromal cells
Wound pH has an impact on a variety of nonimmune cells, including endothelial cells, fibroblasts, and keratinocytes, which are essential for angiogenesis and reepithelialization. Acidification of the wound site promotes von Willebrand factor glycoprotein multimerization, a key element in vascular regeneration. 35,38 This multimerization results in the tubularization of endothelial cells and angiogenesis. 38 Therefore, as blood flow is restricted in DFU because of small and large vessel disease, reducing the wound pH might increase wound oxygenation through neoangiogenesis, in addition to the Bohr effect described above (Fig. 2A, C).
Fibroblasts and keratinocytes are two skin cell types required for tissue growth and wound closure. 9,10,35,39 While both cell types can tolerate large pH range from 6.5 to 10.5, fibroblasts' and keratinocytes' proliferation and migration pH are optimal at neutral to alkaline pH values between 7.5 and 8.5 (Fig. 2D). 39 Indeed, a neutral pH range appears optimal for wound closure in nondiabetic mice. 39 Potentially, the advantages of alkaline pH values on stromal cell proliferation and migration are counterbalanced by an increased risk of infection. 40
Proteolytic enzyme activity
Because of the chronic inflammation in DFU, the activity of proteolytic enzymes is increased. 9,10 Their overexpression in DFU is responsible for the degradation of the ECM and growth factors, and thus contributes to impaired wound healing. 9,10 The high pH values observed in DFU contribute to increases in cathepsin-G, elastase, MMP-2, MMP-9, and plasmin activity, whose optimal pH value is around 8 (Fig. 2F). 9,10,33,40,41 On the other hand, an acidic environment decreased their activity, suggesting that a more acidic environment may reduce the activity of the overexpressed proteases and be beneficial for DFU healing (Fig. 2A). 41
As our understanding of the importance of wound pH in the regulation of diverse mechanisms implied in wound healing is deepening, there is a growing consensus that pH is an emerging therapeutic target in diabetic wound healing. 12
Wound pH-modulating therapeutic and diagnostic systems in diabetic wound healing
Commercially available pH-modulating and pH-sensitive products
The idea of using acid agents as adjuvant therapy for chronic wound healing emerged in 1942, when Dugal and Laugier observed a fastened wound healing process by topical application of oxalic acid on uninfected rabbit wounds. 18 Even though the researchers did not understand the underlying mechanism, they hypothesized that the pH-lowering property of oxalic acid might play a role in the accelerated wound healing rate. 18
Several devices reported to modulate wound pH are commercially available for use on chronic wounds, including some indicated for diabetic wounds (Table 1). 42 –73 They use pH-modulating components such as polycarboxylates, 42 –45 acidifying enzymes, 46 –50 medical-grade honey, 54 –59,71 polymers that degrade into acidic products, 60 –63,69 –71 and acid-releasing systems. 64 –67,71 We also identified one pH-sensitive dressing for diagnostic purposes. 72,73 It is important to note that high-quality peer-reviewed clinical studies are currently lacking for these products, and that studies with a control group are needed to compare their performance with standard of care.
Selected commercially available devices with reported pH-modulating or pH-sensitive properties
For more information on honey-based commercially available products, the reader is referred to exhaustive reviews from Hossain et al. 52 and Scepankova et al. 53
FDA, Food and Drug Administration; PHI, polyhydrated ionogen.
Low-molecular-weight pH modulators
More recently, topical applications of pH-lowering agents in preclinical and clinical studies showed promising results in various types of wounds. In this study, we are presenting preclinical and clinical studies using pH-lowering agents such as acetic acid, 74 citric acid, 12,75 hypochlorous acid, 76 and phosphoric acid, 12 for the treatment of diabetic and nondiabetic wounds (Table 2). These studies suggest that the use of these often inexpensive, relatively nontoxic when diluted, easily available acids may have beneficial effects on wound infection status and healing kinetics.
Selected clinical and preclinical study using low-molecular-weight pH modulators
Calculated using https://www.wolframalpha.com (Wolfram Research, Champaign, IL) from https://www.wolframalpha.com/input?i2d=true&i=2M+HOCl+pH
Sim et al. investigated the healing potential of wound bed acidification using 0.01 M citric acid and 0.01 M phosphoric acid solutions in nondiabetic mice with a saline control. 12 The acid solutions were adjusted to pH 4 and 6 for both acids and were either applied every day or every 2 days, while the saline was applied every 2 days. 12 The results showed that the application of acid solutions increased reepithelialization, wound closure rate, and collagen levels of noninfected wounds. 12 However, the application frequency did not impact the wound healing rate.
Also, the acid solutions at pH 4 were more efficient than those at pH 6 and the citric acid solutions were more efficient than the phosphoric acid solutions. 12 After 7 days, the citric acid solution at pH 4 showed a wound healing rate of 85.5% compared with 65.0% for saline. 12 This slower healing rate observed in phosphoric acid groups suggests that the acidic environment created by acids with higher buffering strength slows the healing activity of various intricate cellular processes down, and thus affects the wound healing rate. 12
Agrawal et al. used acetic acid for the treatment of nonhealing infected wounds by various opportunistic pathogens such as Pseudomonas aeruginosa and Staphylococcus aureus. 74 The inclusion criteria included failed treatment with saline, povidone–iodine, eusol, and hydrogen peroxide. 74 This clinical study involved 100 patients, among which 25 had an infected chronic diabetic wound, and studied the efficiency of a 1% acetic acid (pH 2.5)-soaked gauze dressing. 74 After 21 days, no patients recorded microbial growth on culture, with 64 out of the 100 exhibiting no growth after only 14 days. 74 Adverse reactions were limited to a stinging sensation when the solution was applied in a few patients. 74 After treatment, all wounds reduced in size and infected skin grafting donor sites spontaneously healed. 74 While these results were promising, the lack of a control group and the missing evaluation of the healing rate call for further studies to corroborate these findings.
Nagoba et al. conducted a clinical study involving 115 patients with infected DFU of Wagner grade I–III that did not respond to conventional therapy. 75 Wounds were treated with a daily 3% citric acid ointment topical application (pH 2.0–2.5), 77 covered with sterile dressing. 75 The results showed that 94% of Wagner grade I DFU were completely healed after 5–30 applications, 94% of Wagner grade II DFU after 6–34 applications, and 86% of Wagner grade III after 16–34 applications. A complete wound healing rate was observed in 92% of patients, and no adverse reactions were reported. 75 As no control group was included in this single-center study, controlled studies are needed to evaluate the potential of this acidifying treatment.
Ragab and Kamal performed a randomized clinical trial, including 60 diabetic patients, and compared the efficacy of a 10% hypochlorous acid solution against 20% hydrogen peroxide followed by povidone iodine, as a wound care agent in treating infected nonhealing DFU. 76 The pH values of these two solutions were not provided in the study. We calculated a pH of around 3.61 for the hypochlorous acid solution. They reported that after 15 days, all wounds treated by the 10% hypochlorous acid solution were free of microbes while only 13.3% in the control group were. 76 Also, there was a stronger decrease in wound dimensions than the control group. 76 The 10% hypochlorous acid solution also showed faster pain reduction, better odor control, and exudate reduction. 76
Wound pH-modulating polymeric dressings
Several dressings based on synthetic or natural compounds have been developed with the aim of modulating the wound bed to promote the different pH-dependent cellular and biochemical processes described above and for infection control (Table 1). Compared with small molecules, polymeric hydrogel-based dressings have tunable properties that have the potential to improve porosity and swelling ability, moisture and temperature control, antimicrobial and mechanical properties, and the capacity to deliver bioactive agents with controlled release kinetics. 78 Natural polymers such as alginate, chitosan, or agarose have gained broad acceptance for hydrogel-based dressings as they show high biocompatibility, low immunogenicity, low toxicity, and low costs. 79,80 In this section, we are discussing the composition and performance of selected pH-modulating wound dressings in development (Fig. 3 and Table 3).
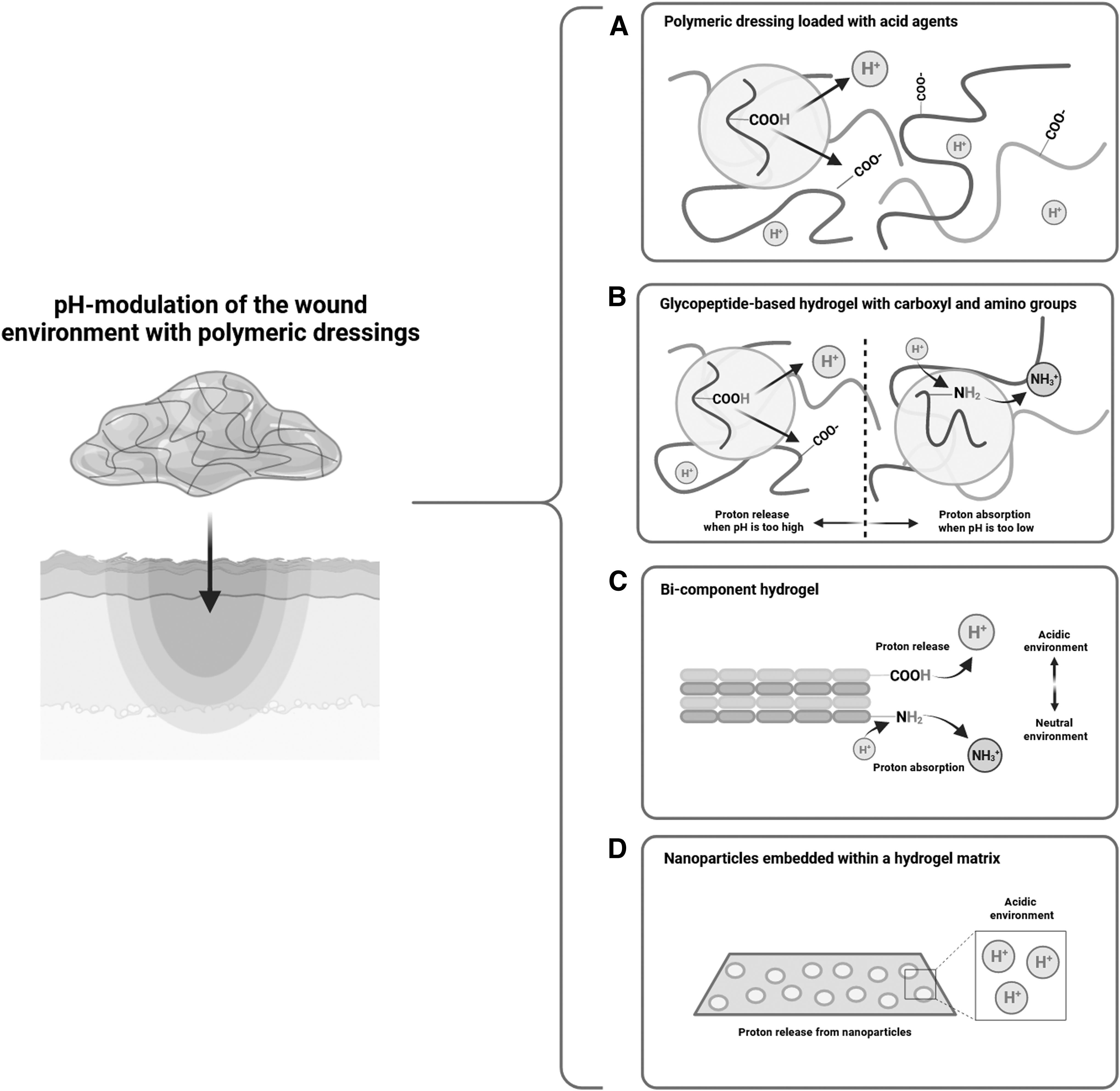
Illustration of pH-modulating mechanisms of selected dressings. Hydrogels loaded with low-molecular-weight acids such as lipoic acid, acrylic acid, or citric acid
Selected polymeric dressings and their pH-modulating mechanisms
2D, two-dimensional; 3D, three-dimensional; CS-MA, methacrylic chitosan hydrogel; DMAEMA2.0, 2% 2-dimethylaminoethyl methacrylate-loaded hydrogel; Gel1, poly(acrylicacid-co-1-vinyl-2-pyrrolidone) hydrogel; Gel2, poly(carboxymethylchitosan-co-acrylamide) hydrogel; GelA, poly(hydroxypropyl acrylate-co-acrylic acid)-magnesium ions hydrogel; GelB, carboxymethyl chitosan hydrogel; HASN, hyaluronic acid single-network hydrogel; HPADN@INS, strontium-crosslinked glycopeptide-based hydrogel, including hyaluronic acid modified with diacylhydrazine adipate or aldehyde and dopa-modified poly(6-aminohexanoic acid) (loaded with insulin); LAMC@Exo, lipoic acid-modified chitosan (loaded with exosomes); PASN, poly(6-aminocaproic acid) single-network hydrogel; VI3.5, 3.5% N-vinylimidazole-loaded hydrogel.
Xia et al. investigated the wound healing performance of a pH-modulating dressing in full-thickness excisional diabetic mice. 35 They developed a glycopeptide-based hydrogel with ammoniated- or aldehyde-functionalized hyaluronic acid and poly(6-aminocaproic acid) (HPADN) to regulate the pH of diabetic wounds (Fig. 3B). 35 The presence of numerous carboxyl and amino groups within the polymer structure allowed the hydrogel to modulate pH values in a neutral–acidic–neutral change sequence, with pH values between 6 and 7 between day 1 and 12. 35 This allowed an acidic environment during the inflammation phase and a progressively neutral pH environment during the proliferation and remodeling phase, to promote the different pH-dependent cellular and biochemical processes throughout the wound phases described earlier. 35
They also loaded the hydrogel with insulin (HPADN@INS) to reduce the local blood glucose level in the wound bed and potentiate the wound healing effects. 35 After only 3 days, HPADN@INS and HPADN groups exhibited a healing rate of 69% and 56%, respectively, while the nondiabetic and diabetic control groups with no hydrogels only showed a healing rate of 41% and 28%, respectively. 35
After 14 days, the HPADN@INS, HPADN, and nondiabetic groups showed almost completely closed wounds, while the diabetic group still had a visible wound area with a 75% healing rate. 35 Furthermore, the application of the hydrogel on diabetic wounds promoted polarization of proinflammatory M1 macrophages into the anti-inflammatory M2 phenotype, reduced oxidative stress, and induced angiogenesis, thus promoting diabetic wound healing. 34 –36 Finally, the hydrogel showed antimicrobial activity against S. aureus and Escherichia coli and exhibited good mechanical and adhesive properties. 35
Liu et al. developed pH-lowering chitosan-based hydrogels in association with lipoic acid (LAMC) and tested this system in diabetic rats with splinted full-thickness excisional wounds to prevent wound contraction. 81,82 This system avoided the use of expensive and cytotoxic photoinitiators and exhibited an antioxidant effect. 82 The authors also loaded the LAMC gel with exosomes (LAMC@Exo) to improve the already existing antioxidant properties of the LAMC hydrogel. 82 The degradation of the hydrogel in a H2O2-, glucose-, and pH-responsive manner is responsible for the conferred pH modulation property of both LAMC and LAMC@Exo hydrogels (Fig. 3A). 82
After 5 days, pH of wounds treated with LAMC and LAMC@Exo hydrogels became acidic around 6.8 and 6.5, respectively, while the pH of control wounds (gauze or methacrylic chitosan hydrogel) increased to more alkaline values exceeding 7.5. 82 Also after 5 days, the wound healing rate was significantly higher in LAMC and LAMC@Exo groups reaching around 25% and 30% healing, respectively, while the gauze and methacrylic chitosan hydrogel groups exhibited a healing rate below 10%. 82
After 21 days, LAMC and LAMC@Exo groups showed a wound healing rate of around 75% and 85%, respectively, while the gauze and methacrylic chitosan groups showed a healing rate around 60%. 82 In conjunction to higher wound healing rates, the LAMC and LAMC@Exo hydrogels showed better biocompatibility than the methacrylic chitosan hydrogel, increased fibroblasts, and endothelial cell proliferation and reduced the amount of ROS as well as advanced glycation end products within the wound bed. 82 Finally, the hydrogels showed good flexibility, swelling, and adhesion. 82
Cui et al. investigated a topical pH-regulating bicomponent microgel ensemble in healthy mice with full-thickness excisional wounds. 83 The ensemble was a network of two hydrogel bead formulations, one poly(acrylic acid) based loaded with magnesium ions (GelA) and one carboxymethyl chitosan based (GelB), allowing for a great number of carboxyl and amino groups (Fig. 3C). 83 Similar to the pH profile induced by Xia et al. 35 and Liu et al., 82 but with different systems, the hydrogel changed the wound pH in a neutral–acidic–neutral manner, with acidic pH values reaching around 6.5. 83
After 12 days, the healing rate for the microgel ensemble was 93%, compared with 68% for the hydrogel-free control group. 83 The authors also successfully induced the growth of a thin layer of adipocytes in the microgel ensemble group, thanks to the loaded Mg2+, maintaining the integrity of the epidermis and acting as a protective layer from the environment. 83 The microgel ensemble promoted macrophage polymerization into the M2 phenotype, enhanced angiogenesis, and increased adipocyte and fibroblast proliferation. 83
Moreover, the ensemble exhibited antibacterial effects against S. aureus and E. coli, showed good mechanical strength, self-healing ability, and swelling capacity. 83
He et al. developed a bicomponent hydrogel with pH-regulating properties and investigated its wound healing performance in healthy mice with full-thickness excisional wounds. 84 The first component is a poly(acrylic acid)-based hydrogel rich in carboxyl groups [poly(acrylicacid-co-1-vinyl-2-pyrrolidone) hydrogel, Gel1] and the second layer is a poly(carboxymethyl chitosan) and acrylamide-based hydrogel rich in amino groups (Gel2) (Fig. 3C). 84 This hydrogel regulated the wound pH in a neutral–acidic–neutral manner, by acidifying the wound around pH 6.5–7, thanks to Gel1 during the early stages and alkalinizing the wound during the late stages with Gel2. 84
After 5 days, the Gel1/Gel2 assembly showed a higher wound healing rate of around 50%, while the wounds treated with only Gel1 or Gel2 showed a wound healing rate around 30% and 40%, respectively. 84 However, after 14 days, the wound healing rate were similar at around 83% and 79%, respectively. 84 The bilayer hydrogel showed good swelling and mechanical properties, as well as a self-healing capacity. 84
Koehler et al. engineered a pH-modulating poly(ethylene glycol)/alginate hydrogel loaded with different concentrations of acrylic acid (Fig. 3A). 85 The effect of the hydrogel on wound healing was assessed in a two-dimensional (2D) cell migration assay (gap closure model) using human dermal fibroblast, adult (HDFa) cell line, and in an alkaline (pH = 8) three-dimensional (3D) wound model using fibroblasts and keratinocytes isolated from juvenile foreskin. 85 In the 2D wound model, the control hydrogel and the hydrogel loaded with up to 1.5% acrylic acid completely closed the gap. 85 In the alkaline 3D wound model, the 0.25% acrylic acid-loaded hydrogel increased the healing rate compared with the control hydrogel. 85 These systems showed good tensile and compressive mechanical strength and adequate swelling properties to take up high amounts of wound exudate. 85
Piva et al. engineered an agarose-based hydrogel dressing loaded with cesium salt of phosphotungstic heteropolyacid nanoparticles that was investigated as an infection control device (Fig. 3D). 86 This system exhibited an acidic surface of pH 3 at 20 wt% nanocomposite, thanks to a very strong Brønsted acidity and had broad antimicrobial properties against E. coli, S. aureus, Candida albicans, and Aspergillus fumigatus. This dressing showed good mechanical properties in terms of stretch resistance, and did not lead to skin irritation in rabbits. 86
Tyeb et al. developed a bilayer agarose film loaded with citric acid, and lowered the pH of a wound exudate model made of horse serum in calcium-containing saline to pH values of 6–7. 33,71 The layers were loaded with 7.5% or 10% citric acid, allowing a better release control and a longer duration in the pH value range of interest (Fig. 3A). 33 When the 7.5% citric acid-loaded layer was in contact with the wound exudate model, pH values reached the desired range of 6–7 after 1 h for a duration of 24 h. 33 In the targeted pH range of 6–7, the film showed bacteriostatic effects on S. aureus and P. aeruginosa, as well as satisfying mechanical and swelling properties. 33
In the same horse serum-based wound exudate model, Milne and Connolly assessed the pH-lowering properties of four hydrogel formulations. 71 The acidic agents used were manuka honey, carboxymethylcellulose, protease-modulating collagen cellulose (Promogran®), and a polyhydrated ionogen (PHI)-coated polymer mesh made of polyethylene gels loaded with metal cations and citric acid (Tegaderm 3M Matrix PHI®) (Fig. 3A). 71 After 20 min, a decrease of the simulated wound fluid pH was observed from around 8.3 to 5.30, 6.65, 5.41, and 4.02, respectively, the most effective one being the PHI-coated polymer mesh. 71 Only the pH-lowering properties were assessed in this study. 71
Based on the results obtained by Schreml et al. indicating that impaired cell migration and proliferation on the wound periphery may be related to acidic values around 6.5, 29 Koehler et al. also investigated the effect of an alkaline poly(ethylene-glycol)-based hydrogel loaded with 3.5% N-vinylimidazole (VI3.5) or 2% 2-dimethylaminoethyl methacrylate (DMAEMA2.0) for wound healing. 87 The pH of the precursor mixture was 8.5 and 10.0 for the VI3.5 and DMAEMA2.0 hydrogels, respectively. 87
In the same 2D wound model than previously, 85 the VI3.5 hydrogel showed higher migration velocity than the control hydrogel and around 60% gap closure compared with 35% for the control hydrogel after 48 h. 87 With the DMAEMA2.0 hydrogel, they observed higher migration velocity than the control hydrogel and almost complete gap closure. 87 In the same acidic 3D wound model (pH = 6.5) than previously, 85 cell ingrowth was enhanced by 46% with VI3.5 hydrogel and by 89% with DMAEMA2.0 hydrogel compared with the control hydrogel. 87 Overall, they exhibited good swelling and mechanical properties. 87
Based on the preclinical studies, it appears that a slightly acidic pH around 6.5 leads to better healing outcomes in diabetic and nondiabetic wounds (Table 4). We were not able to retrieve data on lowering wound pH under 6. More studies are needed to determine the ideal timing and extent for acidification for optimal wound healing. Also, while these investigational systems are promising and could easily be implanted in diabetic wounds' standard of care (Fig. 4), they face important challenges in the translation to the clinic.

Implementation of pH-modulating and pH-sensitive products in the clinical pathway for DFU. Wound pH assessment can be performed in addition to macroscopic evaluation for both initial wound diagnostic and follow-up for disease staging, evidence-based treatment selection, and the assessment of treatment success. Regarding treatment selection, alkaline wound beds may be preferentially treated with an acidifying wound dressing, and wound pH assessment may help evaluate treatment success at follow-up.
Wound closure and lowest pH achieved for selected dressings in preclinical studies
On a materials level, diabetic wound dressings must fulfill a multitude of functions, including providing a moist wound environment, gas exchange to oxygenate the wound, wound exudate absorption to avoid maceration, high mechanical stability, and thermal isolation. Many of the cited studies have yet to demonstrate these capabilities to enable the development of a clinically viable product. Furthermore, certain studies lack a preclinical proof-of-concept study in an animal model of diabetes.
This limits the evaluation of the potential of these systems as diabetes strongly influences the complex interplay between stromal and immune cell types in the wound healing process. A more general limitation for preclinical studies in diabetic wound healing is the missing consensus regarding which animal model best represents human DFUs in terms of pathophysiology. 88
Diagnostic and theranostic systems
Wound pH has already been used as a wound biomarker to engineer pH-responsive systems, mostly hydrogels and flexible electronics, for wound monitoring and for infection control (Table 5). These technologies can either be focused on diagnostic, therapeutic, or a combination of both (theranostic) systems.
Examples of pH-sensitive mechanisms for bioactive agents delivery
Adapted from Han et al. 96
As wound pH is a promising biomarker for wound healing rate, the use of pH-sensitive dyes is one of the most straightforward ways to monitor the wound pH. 73,89 Some of these diagnostic devices are able to give a quick optical approximation of the wound pH value within a few seconds to a few minutes by using colorimetric dyes. 73,90 This optical strategy has limitations such as the subjectivity of the color interpretation and potential interferences by chromogenic substances such as hemoglobin.
Wound pH can also be assessed using small pH electrodes encapsulated in flexible materials, 91 or fluorescent dyes for point-of-care wound diagnostic, allowing for more accurate pH values. Our group recently reported a fluorescent pH-sensitive alginate wound dressing that detected pH values in a clinically relevant range in excisional mouse wounds. 89 Some of these dressings demonstrated good performance in patients with chronic wounds, including DFU, 73 or in an infected porcine wound model, 92 where pH tends to become more alkaline. For a detailed discussion on pH-sensitive diagnostic wound dressings, the reader is referred to a recent perspective from our group (Fu et al.). 27
Wound pH can also be used as a trigger for drug release in pH-sensitive drug delivery systems, through hydrogel swelling, 93 degradation, 94 and internal interactions between the loaded drug and the other components of the dressing (Table 5). 95 Swelling is generally due to the pH-dependent protonation and deprotonation of the functional groups in the material components. 96 Consequently, a phenomenon of charge repulsion can occur, increasing the pore size to release drugs. 96 Also, increased pH values can lead to the degradation of the 3D polymer network, leading to a weakened hydrogel matrix and drug release. 96 Both synthetic and natural antimicrobials as well as nanoparticles, cells, and other bioactive agents have been used in these systems for infection control and wound healing promotion. 96 For a comprehensive discussion on pH-responsive systems for drug delivery and associated mechanisms, the reader is referred to a recent review (Han et al.). 96
Eventually, because pH can be used as a biomarker and a trigger for drug release, pH-sensitive theranostic dressings are being developed currently. Most of these systems are bioelectronic flexible films that can simultaneously measure wound pH and release antimicrobial agents like cefazolin through an electroresponsive electrode, 97 ciprofloxacin from oxidation of silicon microparticles, 98 or thrombin-derived c-terminal peptide-25 through contraction and water expelling from electroactive hydrogels. 99 Also, wound pH can be obtained through wireless technologies and directly read on a smartphone, 97,99 –101 or by simple visual monitoring. 98 Some of these systems showed promising results for wound healing monitoring and healing in preclinical studies, 97,102 and in a diabetic mouse model. 99
SUMMARY
Wound pH is closely related to the status of DFU. Wound pH-associated processes such as dysregulated macrophage activity, impaired stromal cell migration and proliferation, protease overactivity, and bacterial growth negatively influence diabetic wound healing. Modulating wound pH using small molecules and engineered hydrogel dressings improved wound healing kinetics in preclinical models of diabetic wounds and in clinical studies with patients with DFU. Wound pH is therefore an emergent target in DFU with a high potential to yield novel molecular topical therapeutics for DFU.
TAKE-HOME MESSAGES
DFU is one of the most debilitating and life-threatening complications of diabetes with limited pharmacologic options.
Alkaline wound pH affects different cellular and biochemical processes involved in wound healing and the risk of microbial growth.
Preclinical studies in diabetic and nondiabetic mice showed that pH modulation increased the healing rate of wounds.
High-quality clinical studies are warranted to explore the full therapeutic potential of wound pH modulation in DFU.
ACKNOWLEDGMENTS AND FUNDING SOURCES
All figures were created with BioRender.com. S.M. gratefully acknowledges funding from the Natural Sciences and Engineering Research Council of Canada (Discovery Grant, RGPIN-2022-04384) and the Fonds de recherche du Québec—Nature et Technologies (Établissement de la relève professorale—Communauté métropolitaine, 330153).
Footnotes
AUTHORs' CONTRIBUTIONS
L.-P.T.: investigation, visualization, and writing—original draft. M.-L.A.-H.: visualization, and writing—review and editing. K.C.: visualization, and writing—review and editing. G.M.: visualization, and writing—review and editing. B.R.F.: conceptualization, project administration, supervision, and writing—review and editing. S.M.: conceptualization, project administration, supervision, funding acquisition, and writing—review and editing.
AUTHOR DISCLOSURE AND GHOSTWRITING
B.R.F. has equity in Limax Biosciences and is a consultant for Amend Surgical. All the other authors declare no conflicts of interests with regard to this critical review. Ghostwriting was not used.
ABOUT THE AUTHORS