
Abstract
Objective:
This umbrella review aims to summarize and evaluate the evidence from current systematic reviews/meta-analyses (SRs/MAs) on the effectiveness of stem cell therapy for diabetic foot (DF).
Approach:
We conducted a comprehensive search in four databases for SRs/MAs that included randomized controlled trials (RCTs) on stem cell therapy for DF. Two separate researchers independently evaluated the methodological quality and evidence quality of the SRs/MAs that were included in the study. We conducted a quantitative synthesis of all RCTs included in the SRs/MAs to obtain objective and updated conclusions. Egger's test and sensitivity analysis are used to examine the reliability of the results.
Results:
This umbrella review includes eight SRs/MAs, and their methodological quality and evidence quality were all deemed unsatisfactory. Out of the 8 SRs/MAs, 26 RCTs were included, with a total corrected covered area of 21.4%, indicating a high degree of overlap. The test of super-significance did not yield any significant results. Our updated meta-analysis suggests that DF patients can benefit from stem cell therapy, as indicated by effectiveness in measures, including healing rate, amputation rate, ankle-brachial index, transcutaneous oxygen pressure, ulcer size reduction, complete healing time, pain-free walking distance, rest pain score, and new angiogenesis rate.
Innovation:
This study conducted a comprehensive evaluation and reanalysis of the current evidence regarding the effectiveness and safety of stem cell therapy for DF, which is the first of its kind.
Conclusion:
Based on the existing evidence, stem cell therapy is effective and safe for patients with DF.


INTRODUCTION
Diabetic foot (DF) is one of the most common complications of diabetes. Once infections and recurrences occur in DF patients, wounds are prone to deteriorate, leading to sepsis and an increased risk of amputation. 1 DF constitutes a significant contributor to disability and mortality among individuals with diabetes, 2 with as many as 20% of diabetic patients necessitating hospitalization due to this condition. 3 Evidence indicates that ∼4–10% of individuals with type 2 diabetes may experience the development of diabetic foot ulcers (DFUs).
Furthermore, the risk of mortality within a 5-year period for those affected by DF is notably elevated, being 2.5 times higher when contrasted with individuals who solely have diabetes. 4 It is estimated that a diabetes-related amputation occurs every 20 s globally. The annual mortality rate for DFUs patients is as high as 11%, and for amputees, it is as high as 22%. 5
Unfortunately, over the past few decades, there has been no improvement in the incidence and disability rates of DF prevention. Traditional DF therapies have also been unsatisfactory. Moreover, standalone interventions or vascular bypass surgeries prove inadequate in tackling the fundamental pathological foundation of widespread blood vessel constriction and blockage in the DF, alongside nerve and tissue impairments. 6
Currently, most treatment methods for DF mainly target a single factor related to wound healing. As a highly promising approach for treating DF, 7 the main advantage of stem cell therapy lies in its ability to comprehensively regulate tissue regeneration by improving the microenvironment. 8
Mesenchymal stem cells (MSCs) and mononuclear cells are the primary types of somatic cells and stem cells utilized in clinical practice, showing great potential as a novel treatment modality for diabetic foot. 9 MSCs can be sourced from umbilical cord, bone marrow, and hair follicles. Mononuclear cells are derived from bone marrow and peripheral blood, and they possess both progenitor cell and stem cell characteristics. In addition, there are adipose-derived stem cells (ADMSCs).
Despite the effectiveness of both somatic cells and stem cells in treating DF, and the existence of some overlapping mechanisms, it is currently unclear which type of cell has a superior therapeutic effect. 10 The mechanisms that contribute to its therapeutic effectiveness involve encouraging the deposition of collagen, instigating the formation of new blood vessels, enhancing lower limb blood flow, and mitigating inflammation. 11
The number of systematic reviews/meta-analyses (SRs/MAs) on the effectiveness and safety of stem cell therapy for DF is increasing. SRs/MAs are considered the most robust evidence, playing a crucial role in identifying, evaluating, and synthesizing research findings for clinical decision-making. 12 However, potential biases in the evidence-gathering process raise doubts about the reliability of SRs/MAs in guiding clinical staff decisions. 13
To address this, our study used an umbrella review methodology to critically assess and scientifically document the quality of SRs/MAs on stem cell therapy for DF. In addition, we conducted a comprehensive analysis of the randomized controlled trials (RCTs) included in these SRs/MAs to obtain updated conclusions. The Summary Graphic Illustration of this study can be found in Fig. 1.
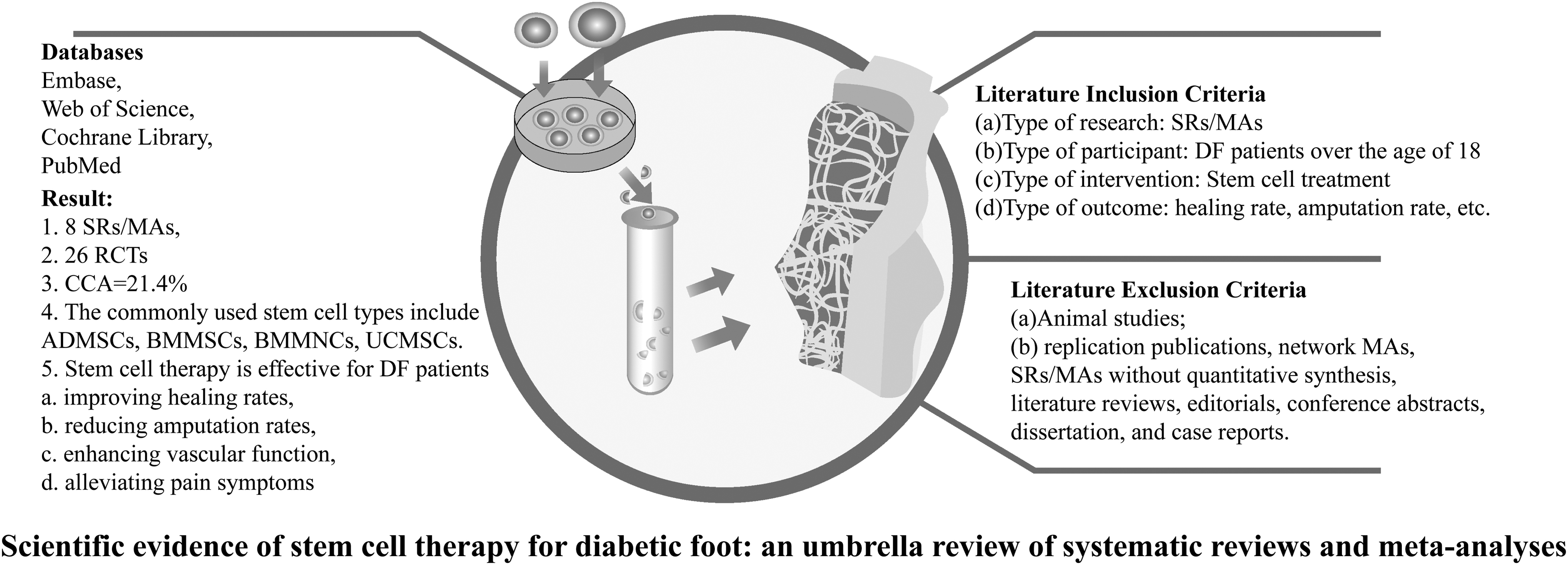
The summary graphic illustration of this study.
METHODS
The methodology of this study followed the preferred reporting items for overviews of reviews (PRIOR) statement, 14 and we followed the methods of Li et al. 15 and Poprom et al. 16 The research protocol for our current umbrella review has been published in the INPLASY database and is registered under the number INPLASY202380037.
Search strategy
Two researchers (referred to as H.S.S. and X.Y.) conducted independent searches of multiple databases, including Embase, Web of Science, Cochrane Library, and PubMed. The search period extended from the inception of these databases up until July 2, 2023. To conduct our search, we used a combination of Mesh terms and free keywords. The Mesh terms used in our search included “Stem Cell,” “Diabetic Foot,” “Systematic Review,” and “Meta-Analyses.” Moreover, we manually reviewed additional references from the identified literature and considered relevant quotes from experts to ensure that any potential missing literature was included. The complete details of the search strategy for all databases in this study can be found in Supplementary Material S1.
Eligibility criteria
Literature inclusion criteria
Type of research: The research is based on SRs/MAs of RCTs that investigate the efficacy and safety of stem cell therapy for DF.
Type of participant: DF patients older than the age of 18, with no restrictions based on race.
Type of intervention: Both the intervention group and the control group receive conventional treatment (CT), which includes regular medication for glucose lowering, blood pressure control, lipid regulation, infection prevention, anticoagulation, neuronutrition, and vasodilation, as well as regular local wound care. In the intervention group, in addition to CT treatment, stem cell therapy was also administered.
Type of outcome: Outcomes assessed in this study included healing rate, amputation rate, ankle-brachial index (ABI), pain-free walking distance, ulcer size reduction, new angiogenesis rate, transcutaneous oxygen pressure (TcPO2), procedure-related complications, rest pain score, complete healing time, and adverse event.
Literature exclusion criteria
Animal studies;
replication publications, network MAs, SRs/MAs without quantitative synthesis, literature reviews, editorials, conference abstracts, dissertation, and case reports.
Publication screening and data extraction
Publication screening and information extraction were carried out independently by our two researchers (referred to as X.Y. and H.S.S.). Initially, duplicate publications were removed using Endnote X20 bibliography management software. Next, an initial screening was performed by reviewing the titles and abstracts of the identified publications. Finally, the full texts of the remaining publications were carefully examined to make the final inclusion decisions. To collect basic information on each SR/MA, a structured data extraction form was used, which included details such as author information, publication year, interventions, and main conclusions.
Quality assessment
Two researchers (referred to as X.Y. and W.J.F.) independently assessed the methodological quality and evidence quality of the included SRs/MAs using the Assessment of Multiple Systematic Reviews 2 (AMSTAR-2) tool 17 and the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system. 18
Statistical analysis
A large number of SRs/MAs focusing on the same area published in a short period of time may contain a large number of replicated RCTs, which may bias the overall results. To assess the potential impact of including the same RCTs, we utilized a measure called corrected covered area (CCA) to determine the extent of overlap. 19 The CCA was calculated using the following formula:
The “N”, “r”, and “c” in the formula stand for RCTs included in SRs/MAs (repetition permitted), RCTs, and included SRs/MAs, respectively.
To determine whether the significance of the combined effect size was due to chance or bias, the results of the dichotomous variables in the included SRs/MAs were tested for excess significance tests. Excess significance bias was assessed by comparing the observed number (O) to the expected number (E). A larger difference between these values indicates a more pronounced bias, and a p-value below 0.10 suggests that a single systematic review/meta-analysis exhibits excess significance. 20
Two independent researchers collected data from all RCTs included in the SRs/MAs conducted for this study. We requantified and synthesized relevant outcome indicators and types of stem cells from the RCTs included in the SRs/MAs. For dichotomous variables, relative risks (RR) and 95% confidence interval (CI) were used as their effect sizes. The pooled effect size for continuous variables was determined using the mean difference and standardized mean difference (SMD) with 95% CI. Heterogeneity was assessed using the p-value and I 2 statistic. If the p-value was >0.10 and I 2 was less than 50%, a fixed effects model was used. Alternatively, if the p-value was less than or equal to 0.10 or I 2 was equal to or greater than 50%, a random effects model was chosen.
In cases of significant heterogeneity, subgroup analysis was conducted to investigate potential sources of heterogeneity, and the grouping method is based on the type of stem cells. Sensitivity analyses were conducted to assess the robustness and reliability of the portfolio results. All of the above statistical analyses were performed using R 4.3.1 and Cytoscape 3.8.1.
RESULTS
Literature search and selection
According to the search strategy of this study, a total of 218 potential publications were obtained through 8 databases, and we first removed 64 duplicates. After reviewing the titles and abstracts of publications, we excluded 98 records. The remaining 17 records were retrieved for full-text evaluation. Finally, eight publications 21 –28 were included. The study selection process is depicted in Fig. 2, illustrating a flowchart. Supplementary Material S2 contains a list of the excluded literature.
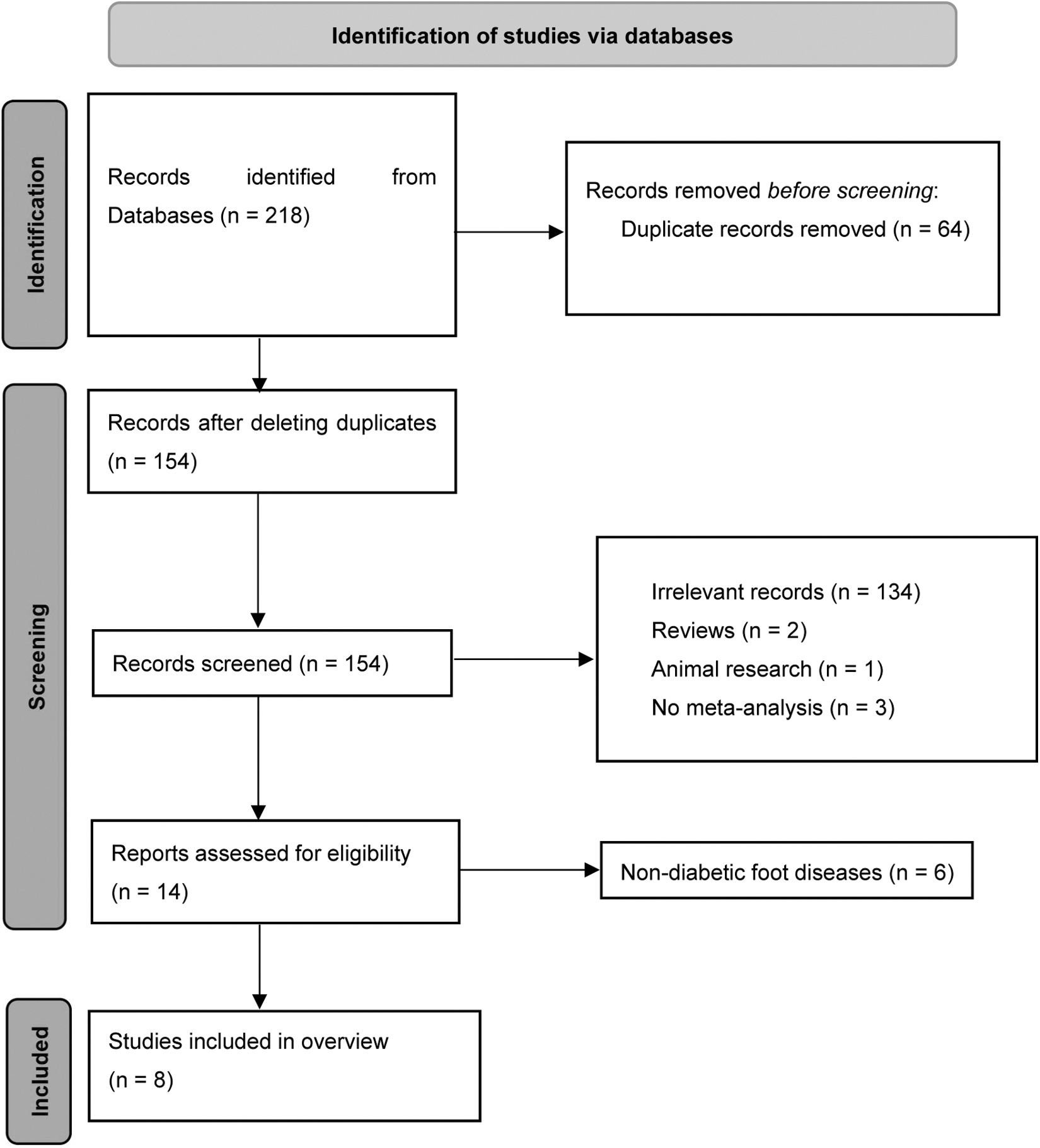
The flowchart of the screening process.
Description of included SRs/MAs
The eight SRs/MAs included in this study were published between 2017 and 2023, indicating substantial research interest in the topic. Table 1 presents the characteristics of these SRs/MAs. Among them, seven SRs/MAs were published by Chinese and one SR/MA was published by Irish researcher. To sum up, all SRs/MAs analyzed in this study were published in English. To summarize, this study incorporated a total of 26 RCTs 29 –54 within the SRs/MAs, and the corresponding relationships between SRs/MAs and RCTs can be found in Supplementary Material S3. Among these RCTs, the highest frequency of use was observed with ADMSCs and peripheral blood-derived mononuclear cells (BMMSCs) (n = 6), followed by bone marrow-derived mononuclear cells (BMMNCs) (n = 4) and human umbilical cord mesenchymal stem cells (UCMSCs) (n = 4), as shown in the corresponding diagram in Fig. 3.

The network diagram illustrating the connections related to “SRs/MAs-RCTs-Types of stem cells.” Red represents SRs/MAs; blue represents RCTs; green represents types of stem cells. RCTs, randomized controlled trials; SRs/MAs, systematic reviews/meta-analyses.
Characteristics of the systematic reviews/meta-analyses
ABI, ankle-brachial index; ADMSCs, adipose-derived stem cells; CT, conventional treatment; DF, diabetic foot; BMMNCs, bone marrow-derived mononuclear cells; BMMSCs, bone marrow-derived mesenchymal stem cells; BMTRCs, bone marrow-enriched tissue repair cells; MNCs, mononuclear cells; MSCs, mesenchymal stem cells; PBMNCs, peripheral blood-derived mononuclear cells; PBMSCs, peripheral blood mesenchymal stem cells; TcPO2, transcutaneous oxygen pressure; UCMSCs, human umbilical cord mesenchymal stem cells.
In addition, information regarding the source, cultivation, and application can be found in Supplementary Material S4. The CCA value was determined to be 21.4%, illustrating a significant level of overlap among the included studies. Each SR/MA included a varying number of RCTs, ranging from 4 to 19. The sample sizes of the individual studies within these SRs/MAs ranged from 151 to 683. In addition, the risk of bias for the included SRs/MAs was evaluated using different assessment tools. Specifically, the Cochrane RoB (1.0) was utilized for 6 SRs/MAs, and the Jadad Scale was applied to 2 SRs/MAs.
Results of SR/MA quality assessment
Methodological quality
According to the evaluation results of AMSTAR-2, the methodological quality of seven SRs/MAs included in this study was determined to be very low, and one of the SRs/MAs was assessed as being of low quality. The main factors contributing to the poor methodological quality of the included SRs/MAs were the lack of study protocol registrations (Item 2, 1/8, 12.5%) 25 and publication exclusion lists (Item 7, 0/8, 0%), and inadequate reporting of funding sources (Item 10, 0/8, 0%) (Fig. 4).
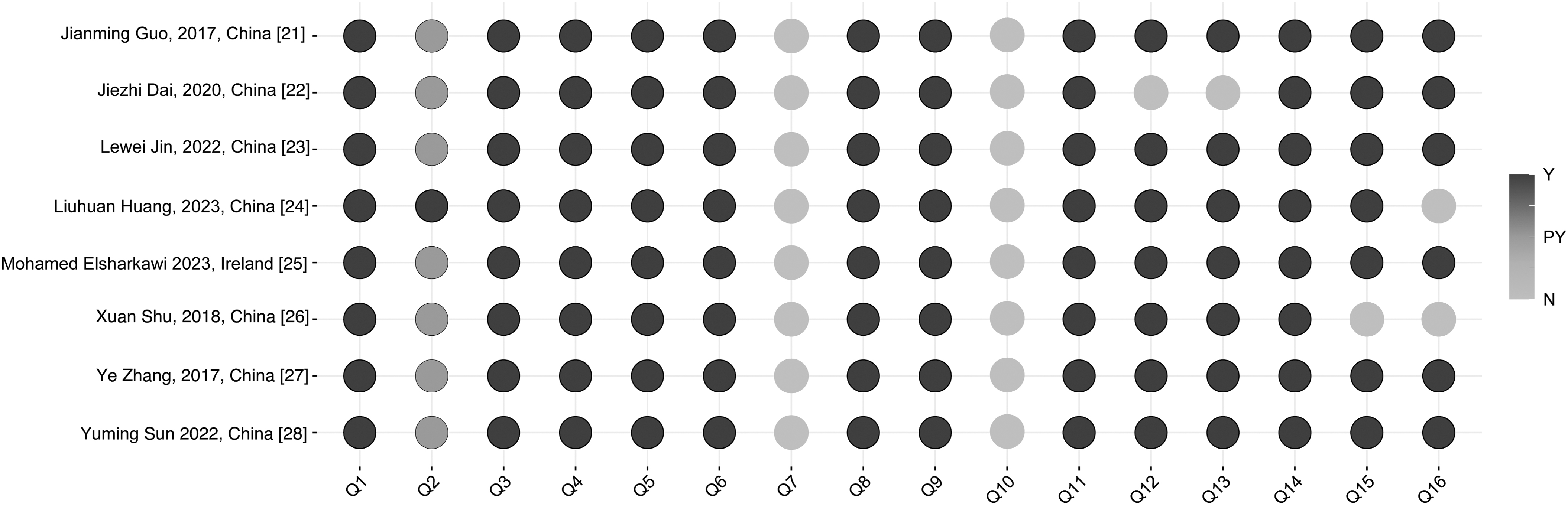
Results of the AMSTAR-2. Y, yes; N, no; PY, partially yes. AMSTAR-2, Assessment of Multiple Systematic Reviews 2.
Evidence quality
Thirty-one outcomes related to stem cell therapy for DF were derived from the incorporated SRs/MAs. The results of the GRADE assessment showed that of the 31 outcomes, there were 4 high-quality (4/31, 12.9%) evidence, 6 moderate-quality (6/31, 19.4%) evidence, 12 low-quality (12/31, 21.4%) evidence, and 9 very low-quality (9/31, 43.3%) evidence. The main reasons for the unsatisfactory quality of evidence included imprecision (20/31, 70.1%) and publication bias (17/31, 54.8%). Details were listed in Table 2.
Results of certainty of quality
H: high; M: moderate; L: low; VL: very low.
Summary of included outcomes
In this study, we have condensed the outcomes encompassed in the SRs/MAs. and no significant excessive impact was found in the related outcome indicators, as shown in Table 3.
Summary of outcome measures
CI, confidence interval; MD, mean difference; O/E, observed number/expected number; OR, odds ratio; RD, risk difference; RR, relative risks; SMD, standardized mean difference.
Effectiveness of stem cell therapy on DF patients
Eight systematic SRs/MAs 20 –27 reported that stem cell therapy can significantly improve the healing rate in patients. At the same time, five SRs/MAs 21 –23,26,27 also showed that stem cell therapy can significantly reduce the amputation rate in patients with DF. Four SRs/MAs 22,25 –27 reported that stem cell therapy can significantly improve measures of ABI and TcPO2 in patients with DF. Two SRs/MAs separately reported that stem cell therapy can improve ulcer size reduction 22,25 and pain-free walking distance 23,27 while reducing rest pain score. One 22 of the two SRs/MAs reported that stem cell therapy can significantly reduce complete healing time. Two separate SR/MA reports have indicated that stem cell therapy can significantly improve the new angiogenesis rate 27 in patients. However, there is no significant difference in reducing surgical complications.
Safety of stem cell therapy on DF patients
Six SRs/MAs 20,22 –24,26,27 have evaluated the safety of stem cell therapy for DF using systematic reviews method. Adverse reactions mainly include pain in the recipient area and leg swelling after stem cell transplantation. However, these adverse effects do not significantly impact the patients' quality of life and do not cause serious harm to their health. Overall, the results of these SRs/MAs indicate that stem cell therapy is safe for patients with DF.
Reassessment of outcomes, including RCTs in SRs/MAs
For the 26 RCTs included in the SRs/MAs in this study, we performed a quantitative synthesis on the relevant outcomes healing rate, amputation rate, ABI, TcPO2, ulcer size reduction, complete healing time, pain-free walking distance, rest pain score, and new angiogenesis rate. The results of the meta-analysis indicate that stem cell therapy has a significant improvement in healing rate compared to the control group (RR = 1.88 [1.68; 2.10], I 2 = 28.6%) (Fig. 5A), and stem cell therapy can also significantly reduce the amputation rate (RR = 0.27 [0.16; 0.44], I 2 = 0%) (Fig. 5B) of patients with DF.
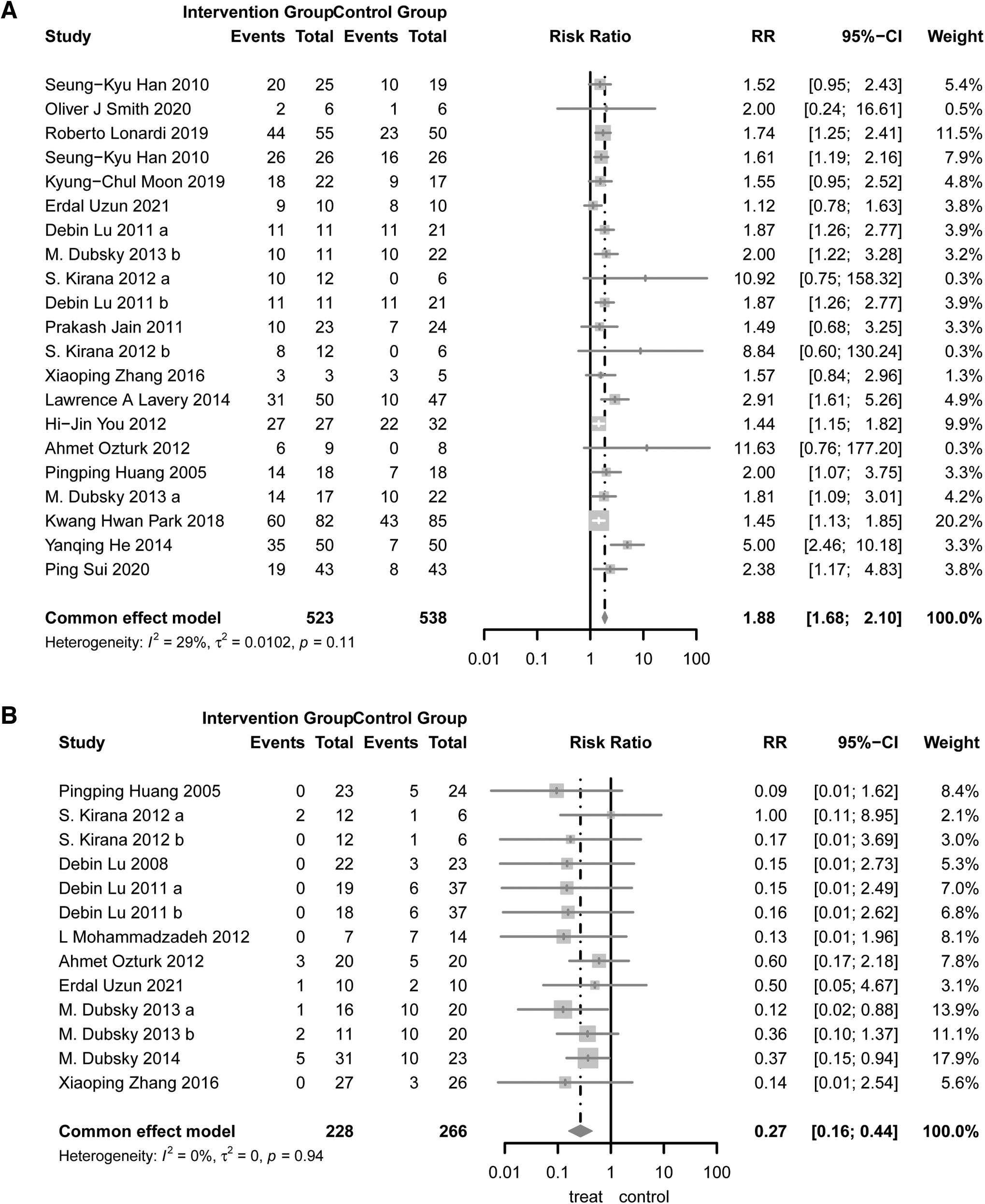
Forest plots of healing rate and amputation rate.
In terms of improving vascular function, the reaggregation analysis also indicates that stem cell therapy can significantly enhance patients' ABI (SMD = 1.26 [0.78; 1.75], I 2 = 83.5%) (Fig. 6A), TcPO2 (SMD = 1.40 [0.85; 1.95], 2 = 80.6%) (Fig. 6B), and the new angiogenesis rate (RR = 6.07 [1.73; 21.26], I 2 = 54.8%) (Fig. 6C). Given the significant heterogeneity, we performed subgroup analysis based on race and stem cell type (Supplementary Material S5). Through subpopulation analysis, we found that although the types of stem cells used and the classification of ethnicity can partially explain the source of heterogeneity (the new angiogenesis rate), some comparisons still show high heterogeneity (ABI and TcPO2), which may be attributed to the measurement methods.
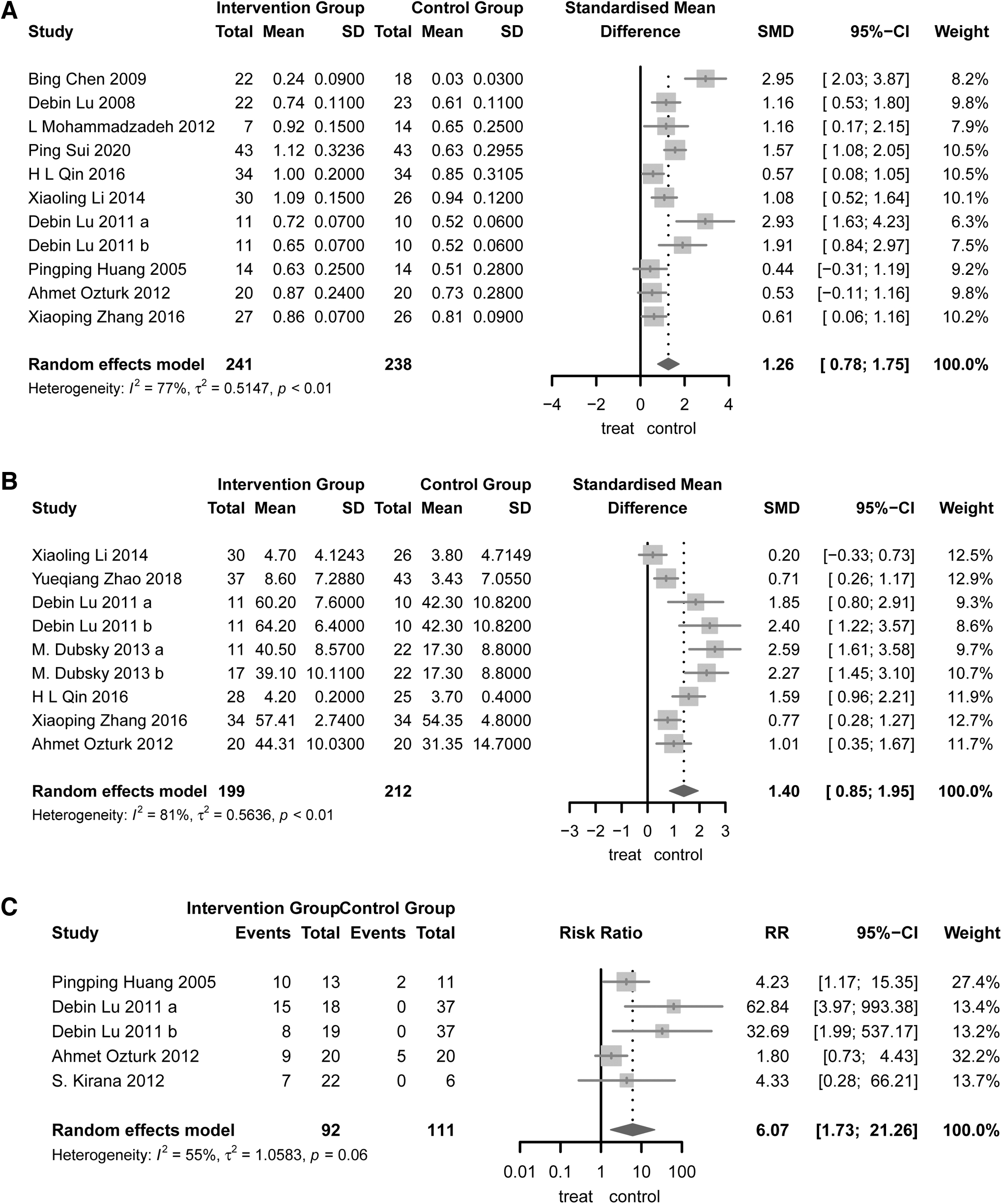
Forest plots of ABI, TcPO2, and new angiogenesis rate.
In the relief of pain symptoms, stem cell therapy can significantly decrease rest pain score (SMD = −1.79 [−2.24; −1.33], I 2 = 0%) (Fig. 7A) while enhancing pain-free walking distance (SMD = 1.27 [0.89; 1.65], I 2 = 0%) (Fig. 7B).In addition, our study also demonstrates that stem cell therapy can effectively reduce complete healing time (SMD = −0.88 [−1.72; −0.03], I 2 = 87.3%) (Fig. 8A), while significantly increasing ulcer size reduction (SMD = −0.89 [−1.43; −0.36], I 2 = 0.0%) (Fig. 8B).

Forest plots of rest pain score and pain-free walking distance.

Forest plots of complete healing time and ulcer size reduction.
According to the biased assessment, the results of the healing rate, amputation rate, and ABI relevant Egger test indicate p-value of 0.0014, 0.0344, and 0.0835, suggesting that there is a certain publication bias in the research. Sensitivity analysis results indicate that the results of other outcome measures are robust (Supplementary Material S6).
DISCUSSION
Stem cell therapy holds immense promise in the field of regenerative medicine and is of significant importance for the treatment of DF. This study provides a comprehensive and critical umbrella review of SRs/MAs in stem cell therapy treatment of DF by using AMSTAR-2, GRADE framework, CCA, excess significance tests to summarize the reliability of current evidence in guiding clinical decision-making and obtain the latest conclusions by using re-meta-analysis.
Summary of included SRs/MAs
As far as we know, this study represents the first comprehensive umbrella review of SRs/MAs focusing on the effects of stem cell therapy on DF. Seventy-five percent of the literature was published in the last 5 years (2018–2023), indicating the increasing interest of researchers in exploring stem cell therapy for DF. In this umbrella review, 9 SRs/MAs were included, which encompassed a total of 26 RCTs. This study has a CCA value of 21.4%, indicating a relatively high degree of literature duplication. This suggests the presence of a similar pool of articles within the current SRs/MAs on the topic of stem cell therapy for DF.
In addition, considering the concentration of publication years in these SRs/MAs, it suggests a consistency in their literature search approach. Based on the reported outcomes, 30 of the 31 (96.77%) indicators demonstrated that stem cell therapy could be beneficial for DF patients, with safety assessments showing no serious side effects. In addition, the excess significance tests showed that none of the dichotomous outcome indicators involved in SRs/MAs in this study was of excess significance.
Summary of the quality of included SRs/MAs
The methodological quality and evidence quality of the included SRs/MAs in this study were found to be the unsatisfactory. Therefore, there may be discrepancies between the inclusion results of the SRs/MAs and the actual outcomes. Only one (1/8, 12.5%) SR/MA has been registered for the research protocol, which could potentially lead to significant modifications during the research process, weakening the standardization, rigor, and transparency of the evidence, thereby increasing the likelihood of selective reporting bias. 55 All SRs/MAs (8/8, 100%) did not include lists of excluded articles. This omission could potentially result in the incorrect exclusion of crucial articles, thereby compromising the accuracy and thoroughness of the reporting. No SR/MA included in the study disclosed complete information about the sources of research funding.
This lack of transparency raises concerns regarding the reliability of the RCT results, as clinical trials funded by industry may be influenced by the interests of the funders, thereby potentially biasing the outcomes.
Only 4 (4/31, 12.9%) outcome indicators were considered to be of high quality according to the GRADE assessment. Imprecision (20/31, 70.1%) and publication bias (17/31, 54.8%) were identified as the key factors leading to the downgrading of the evidence quality. The main reason for imprecision is the insufficient sample size included in the evaluation of each outcome indicator. After all, the included number of patients in the GRADE evaluation of relevant outcome measures leading to imprecise downgrade reasons is insufficient. The high publication bias of the included outcomes can be attributed to the insufficient number of RCTs assessed for each outcome, and assessing publication bias for outcome measures is not meaningful when there are too few included RCTs.
The reestimation of outcomes
While a high CCA value suggests consistent and accurate literature searching, the substantial overlap among the included SRs/MAs indicates that they may not be considered entirely independent and ideal sets of evidence, despite demonstrating no bias through excessive significance testing. Therefore, to avoid errors stemming from overlap and achieve higher quality evidence-based conclusions, it is crucial to extract relevant data from RCTs and reestimate outcome measures. 56 The updated meta-analysis indicates that stem cell therapy has shown significant improvements in the healing rate, amputation rate, ABI, TcPO2, new angiogenesis rate, pain-free walking distance, rest pain score, ulcer size reduction, and complete healing time in patients with DF, and there were no reports of serious adverse events in the RCT.
In our reevaluation, ABI, TcPO2, and new angiogenesis rate exhibited higher heterogeneity, possibly due to the use of different detection devices. Unfortunately, the majority of the original RCTs did not report the relevant detection methods. The results of the reconducted meta-analysis indicate the potential presence of publication bias in the relevant studies. The outcomes of sensitivity analysis suggest that the assessment results are robust. Overall statement, DF patients can benefit from stem cell therapy.
Stem cells are characterized as undifferentiated cells with the capacity to both multiply and specialize into a diverse array of mature cell types, ultimately culminating in the creation of various tissues and organs within the body. 57,58 Traditional treatment methods for DF primarily involve medication and surgical revascularization. Nonetheless, in cases of foot ischemia stemming from arterial stenosis and blockage, relying solely on medication fails to provide a comprehensive solution. Even surgical interventions, which are effective in reestablishing blood circulation, encounter certain complexities. For instance, lower extremity arterial disease prevalent in DF patients frequently affects the arteries in the calf region, and a considerable number of patients experience limitations in distal arterial outflow. 59
Compared to traditional therapies, stem cells can systematically mobilize injured and ischemic tissues and create a favorable wound microenvironment that facilitates wound healing, ultimately promoting the healing of DF, 60,61 and the underlying mechanisms involve promoting angiogenesis, improving neural ischemia and inflammation, and encouraging collagen deposition. 62
Stem cell therapy is expected to become a new approach for treating DF. Currently, the somatic cells and stem cells predominantly used in clinical practice are mononuclear cells and mesenchymal stem cells (MSCs). 9 Mononuclear cells are derived from bone marrow and peripheral blood. They possess progenitor cell and stem cell characteristics and do not require in vitro expansion. Mononuclear cells are used to treat DF by promoting blood vessel formation, reducing inflammation, enhancing epithelial regeneration, and increasing collagen deposition. 53 MSCs can be sourced from umbilical cord, bone marrow, hair follicles, adipose tissue, gingiva, dental pulp, and menstrual blood. They are mainly used to treat DF by promoting blood vessel formation, reducing inflammation period, and increasing type I collagen content. 63 ADMSCs and stromal vascular fraction with adipose stem cells play an important role in the repair and regeneration of chronic wounds after tissue defects. 64
Although somatic cells and stem cells are effective in the treatment of DF and there are some overlapping mechanisms, it is still unclear which type of cells has better therapeutic effects. Further high-quality clinical research is needed to explore this.
Implications for future research and clinical practice
Stem cell therapy is still in the clinical research stage and is currently not established as a standard treatment DF, 65 and we hope to provide evidence for its clinical application through high-quality clinical research. In future published SRs/MAs, researchers should enhance the credibility and scientific rigor of the results by providing a registration of research protocol, along with lists of excluded literature and funding sources. High-quality SRs/MAs were based on well-executed and large-scale clinical trials. To enhance the evidentiary quality and improve the clinical relevance of RCTs in the field of stem cell therapy, it is recommended to adopt the Consolidated Standards of Reporting Trials 2010 (CONSORT 2010). 66 These standards play a crucial role in improving the reporting and transparency of RCTs, thereby facilitating better clinical decision-making.
In addition, this study includes 5 RCTs that utilized ADSCs and BMMSCs, respectively. When selecting clinical stem cell types, it is important to consider not only their clinical efficacy but also the availability and supply of different stem cells (e.g., ease of acquisition, good manufacturing practices, and extensive in vitro proliferative capacity). 67 In addition, clinicians need to account for transplant immunology. Autologous stem cell transplantation holds preference due to its ability to circumvent immunogenicity issues, bolster the survival rate of cells on ulcerated surfaces, and mitigate several ethical concerns. 68 In the RCTs included in this study, 17 RCTs utilized autologous stem cells.
However, allogeneic stem cells are sometimes an effective alternative because under high-glucose conditions, autologous primary stem cells may not be obtainable in sufficient quantities. 38 There is currently insufficient clinical evidence to determine which treatment approach is more effective. To better utilize stem cells in conjunction with new cutting-edge technologies, further research is needed.
Strengths and limitations
As the first systematic umbrella review evaluating stem cell therapy for DF, this study used AMSTAR-2, GRADE, CCA, and tests of super-significance to summarize and assess the evidence for the efficacy of stem cell therapy in DF. Furthermore, this study highlights apparent limitations in current SRs/MAs and RCTs, which may enhance the quality of future clinical research. However, the methodological assessment in this study is subjective. Although our assessment underwent analysis and review by independent researchers, it is crucial to acknowledge that different researchers may hold distinct perspectives on each item, which could result in diverse outcomes.
CONCLUSION
Based on the existing evidence, stem cell therapy is effective for patients with DF, as it can promise in improving healing rates, reducing amputation rates, enhancing vascular function, and alleviating pain symptoms. The commonly used stem cell types in the current RCTs include ADMSCs, BMMSCs, BMMNCs, and UCMSCs. In addition, stem cell therapy has a high level of safety. Given the methodological quality and evidence quality of the supporting SRs/MAs, it is prudent to approach this conclusion with caution.
TAKE HOME MESSAGES
As the first systematic umbrella review evaluating stem cell therapy for DF, this study used AMSTAR-2, GRADE, CCA, and tests of super-significance to summarize and assess the evidence for the efficacy of stem cell therapy in DF.
This study highlights apparent limitations in current SRs/MAs and RCTs, which may enhance the quality of future clinical research.
This study also included a survey of commonly used clinical stem cell types.
Footnotes
AUTHORs' CONTRIBUTIONS
G.B.L., W.J.F., and H.S.S. proposed the research design. H.S.S. and X.Y. conducted literature search, publication screening, and data extraction. X.Y. and W.J.F. performed quality assessment. H.S.S. carried out the data analysis. X.Y. conducted article revisions. The authors collectively contributed to and endorsed the final version of the article.
DATA AVAILABILITY
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
ACKNOWLEDGMENTS AND FUNDING SOURCES
The study was funded by the National Natural Science Foundation of China (82274528); Construction Task Book for the Three-Year Action Plan for Accelerating the Inheritance and Innovative Development of Traditional Chinese Medicine in Shanghai (2021–2023) (ZY [2021–2023]-0211); Shanghai Municipal Health Commission Scientific Research Programme Mission Statement (202240228); Three-year Action Plan for Accelerating the Inheritance and Innovative Development of Traditional Chinese Medicine in Shanghai (ZY [2021–2023]-0211); Special Youth Project for Clinical Research of Shanghai Municipal Health Commission (20234Y0162); Clinical Research Talent Training Program of Shanghai University of Traditional Chinese Medicine Affiliated Hospital (2023LCRC06); Four Bright Foundations of Shuguang Hospital Affiliated to Shanghai University of Traditional Chinese Medicine (SGKJ-202301).
AUTHOR DISCLOSURE AND GHOSTWRITING
The authors have no financial interests to disclose. The content of this article was thoroughly written by the authors listed. No ghostwriters were used to write this article.
ABOUT THE AUTHORS
SUPPLEMENTARY MATERIAL
Supplementary Material S1
Supplementary Material S2
Supplementary Material S3
Supplementary Material S4
Supplementary Material S5
Supplementary Material S6
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.