
Abstract
Significance:
Negative pressure wound therapy (NPWT) has been in practice for decades, proving its utility in many applications, ranging from acutely infected wounds to complex combat wounds and skin grafting. It has been routinely demonstrated that NPWT has superior wound healing outcomes compared with previous standard-of-care therapies. However, the technique involves some challenges related to each of the components that comprise the therapy. The purpose of this article is to highlight the challenges, introduce the recent advancements, and discuss about the future directions in NPWT systems.
Recent Advances:
New techniques and materials have been developed to improve the currently used NPWT systems with promising results when utilized with appropriate indications. Many advancements have been introduced in modes of negative pressure delivery, pumps, interface dressings, adhesive dressings, and tubing technology.
Critical Issues:
An optimal NPWT system would avoid the common problems such as failure to deliver negative pressure due to loss of an airtight seal or tissue ingrowth into the interface dressing causing painful dressing changes and bleeding. Other challenges include infection control and patient pain and discomfort that may contribute to noncompliance.
Future Directions:
Many studies have been performed to evaluate the optimal combination of settings and components in various wounds; however, there is still no clear “best” answer for many specific patient-wound scenarios. Novel and emerging tissue engineering and regenerative medicine approaches could potentially be utilized in the future NPWT systems and thus, this review will discuss some novel ideas for future considerations.

SCOPE AND SIGNIFICANCE
Negative pressure wound therapy (NPWT) is one of the most significant inventions of wound care in recent decades. Today, it is routinely used worldwide playing a vital role in the management of both acute and chronic wounds. 1,2 The purpose of this article is to highlight the challenges, introduce the recent advancements and discuss about the future directions in NPWT systems.
TRANSLATIONAL RELEVANCE
In the 1990s, Drs. Argenta and Morykwas were the first to demonstrate in a porcine model that wounds heal faster when negative pressure is applied into the wound. 3,4 Subsequently, several preclinical and clinical studies have demonstrated how NPWT promotes wound healing by removing exudate, decreasing bacterial load, reducing tissue edema, increasing blood flow into the wounds, and promoting angiogenesis and granulation tissue formation. 5,6 Furthermore, new preclinical studies are being conducted to improve and optimize the use of this technology.
CLINICAL RELEVANCE
NPWT provides faster wound healing. However, the technique involves some challenges such as granulation tissue ingrowth into the interface dressing, which results in painful dressing removal affecting patient compliance. Many attempts have been made to solve the various problems related to NPWT and ultimately improve the currently available systems. 7
BACKGROUND
Since NPWT was invented in the 1990s, it has become one of the most important innovations in wound care and is today routinely used in the treatment of various acute and chronic wounds. 8 –10 NPWT is predominantly indicated for the treatment of complex difficult-to-heal wounds that can be either acute or chronic. In acute wound care, NPWT is utilized when the wound cannot be closed by primary intention because of infection, skin tension, or swelling. Thus, traumatic wounds such as open fractures, lacerations, and severe burns are commonly treated using negative pressure. Other indications include closed incisions where NPWT is used to prevent surgical dehiscence and reduce edema and seroma formation. 11,12
NPWT is also often used in the treatment of skin grafted wounds to increase the graft take. Moreover, it has been shown that NPWT can also be used over fragile cultured epithelial autografts to increase their take. 13 The benefits of NPWT can be seen in many realms of wound care, including combat wounds. During combat, early definitive wound care may simply not be possible. Therefore, the availability of NPWT at Role 2 field hospitals has allowed the soldiers' complex wounds to be temporarily treated while awaiting evacuation to higher level of care. 14
Furthermore, the use of the NPWT has significantly improved the healing outcomes of hand injuries that are also common in military conflicts. Hand injuries, such as burns, have presented long-standing challenges due to the sensitive and functional nature of the hand. 15 Several preclinical animal studies have also shown negative pressure therapy as an effective novel treatment for lymphatic leaks such as from vascular surgery complications and for chronic diabetic wounds by improving lymphangiogenesis. However, the clinical evidence is lacking. 16,17
Conventional NPWT systems consist of an interface dressing (usually a foam or gauze), impermeable adhesive membrane dressing and tubing that connects the interface dressing to a powered suction pump. 18 This device then applies suction through the tubing to achieve a subatmospheric pressure, usually between −75 and −150 mmHg at the wound bed. 19
NPWT promotes wound healing by removing exudate and that decreases tissue edema, increases blood flow into the wound, and stabilizes the wound environment. 20 Negative pressure also causes micro- and macromechanical deformation of the wound tissue. Micromechanical stressors stimulate angiogenesis and granulation tissue formation, whereas macromechanical stressors may facilitate wound contraction. 21
Despite being an efficacious technique, conventional NPWT systems have challenges related to each of the components that comprise the therapy. 22 These components are namely the interface dressing, adhesive dressing, tubing, and the pump device (Fig. 1).
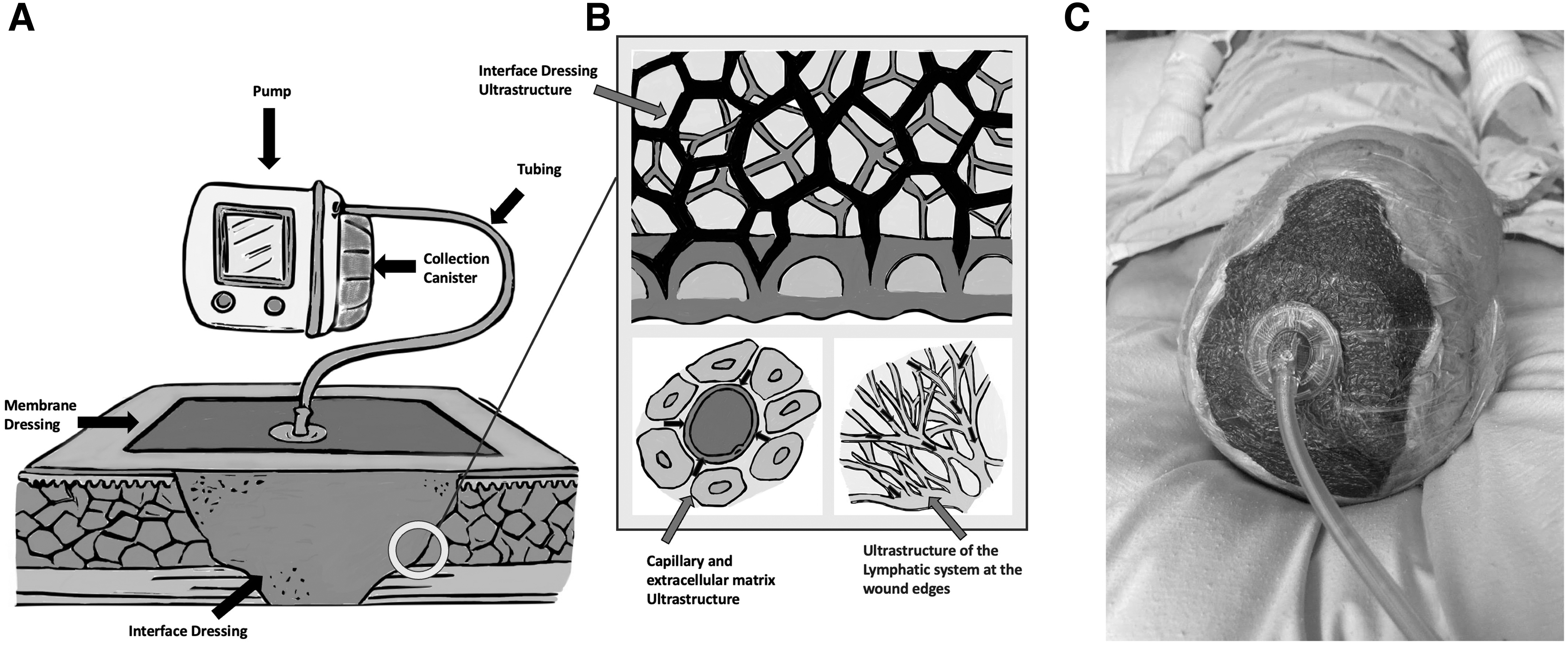
Conventional NPWT system and its components.
Although NPWT promotes tissue regeneration and granulation tissue formation, tissue ingrowth into the interface dressing remains a persistent problem in many devices. As granulation tissue forms within the wound bed, it additionally migrates into the interface dressing, as if it was acting as a scaffolding for tissue healing. 23 When the interface dressing is removed, it tears the granulation tissue off from the wound bed, causing additional trauma and significant pain and discomfort to the patient.
Although this may be an additional act of “debridement,” it removes a layer of newly developed tissue and can cause significant bleeding as well as pain and trauma to the patient if appropriate anesthetic, whether local or general, is not utilized, especially for larger or more complex wounds. 24 Removal of the interface and the adhesive dressings are not the only sources of pain to the patient.
Although many patients do not complain of pain associated with the negative pressure, pressure that is too intense, or pressure that is improperly synced with the specific interface dressing being used can cause additional discomfort. 23,25,26 Various modes of negative pressure delivery have also been utilized to decrease patient discomfort, such as variable NPWT; however, other modes such as intermittent NPWT have been associated with increased discomfort. 27
Patient pain and discomfort contribute not only to the overall experience of wound healing, but it may also contribute to noncompliance. 28 The cumbersome and ergonomic disadvantages of some NPWT devices alongside their frequent lack of cosmetic discretion, the frequent necessity of dressing changes (although improved from standard daily dressing changes), and frequent troubleshooting required due to poor adhesive functionality on skin and anatomically challenging areas lay the grounds for self-discontinuation or outright patient refusal of this therapy. 29
Some devices may be noisy, which may also decrease patient compliance. Further exacerbating factors include the need to keep the pump device charged or connected to a power source, as well as outpatient troubleshooting the device and its associated components—a process that is unfamiliar to the majority of patients. 30 The lack of experience and unfamiliarity with specific NPWT devices by clinical staff might also contribute to decreased compliance and effectiveness. In addition, duration of NPWT therapy remains without universal standardization.
Wound characteristics, such as size, location, type, and presence of infection, impact the planned duration of NPWT. Prolonged NPWT use puts the patient at risk for superimposed infection from the sponge material, damaged periwound skin, prolonged emotional/physical trauma and pain at the wound site, worse outcomes, and higher costs. It is imperative that when NPWT is considered for any wound, that health care provider team has an end-goal in mind for when NPWT will be discontinued, and definitive measures should be pursued. 31
An additional complication of NPWT includes the fact that the interface dressing is a foreign material that is being introduced into a wound bed. The presence of foreign materials, cellulose gauze, polyurethane (PU), and polyvinyl alcohol (PVA) interface dressings in contaminated wounds may contribute to bacterial colonization of the wound and act as a nidus for infection. In such situations, additional surgical debridement may be necessary to clear the wound of harmful bacteria. 32
Should the interface dressing be retained in the wound bed, it can become heavily encapsulated and adherent to the surrounding soft tissues. In many reported cases, repeated surgical procedures and even reconstructive surgery with prolonged antibiotics were required for wound healing. 33,34
Besides the interface dressing there are also problems related to the adhesive dressing and the tubing. When setting up the NPWT system, establishment of an airtight seal using the adhesive dressing is essential. Sometimes, especially in anatomically difficult areas the adhesive fails, which results in loss of negative pressure. Pain related to frequent dressing changes has also been reported as a reason for decreased patient satisfaction. 30 Challenges related to the NPWT tubing include additional discomfort or pressure ulcer formation. 35
To solve the challenges related to currently available NPWT systems and make them more convenient to use for both wound care providers and patients, many research studies have been conducted and have paved the way for technological advancements and innovation. The purpose of this article is to review recent developments in NPWT and to discuss various solutions to the problems related to the current devices and techniques, as well as discuss potential future directions.
DISCUSSION
The traditional NPWT system consists of four main parts: the interface dressing (sponge or gauze), an adhesive dressing, tubing, and a pump that provides the negative pressure for the system (Fig. 1). New techniques and materials have been developed to improve the currently used NPWT systems with promising results when utilized with appropriate indications. Hereunder, we highlight developments related to all of the different NPWT system components.
Interface dressing
The most commonly used interface dressing for NPWT is the standard black foam made from a reticulated open-cell foam (ROCF) PU (Fig. 1B). Benefits to this foam include a pore size (most commonly 400–600 μm) allowing for microdeformation stimulating cell proliferation and subsequent granulation, contraction of the foam as the wound contracts, and being nonabsorbent but allowing exudate to pass through. 36,37 Downsides to this foam are that it may harbor microbes and cause pain, discomfort, and bleeding during dressing changes resulting from tissue ingrowth into the sponge. In addition, the interface dressing might cause foreign body reactions when incorporated in the wound tissue. 38
Gauze is another commonly used interface dressing in NPWT systems. Gauze dressings are frequently used in place of foams, and it has been indicated that gauze-based NPWT systems are also effective. 39 In general, foams are more absorbent, whereas gauze fillers are more malleable and conformable. Although more affordable gauze allows NPWT to be used in the absence of foam sponge, the aforementioned issues still persist. These problems have triggered research and development efforts to improve the currently used technologies. 40,41
White foam dressing
White foam, made of PVA with pore size of 250 mm (such as V.A.C.® Whitefoam™ Dressing or Invia® White FoamNPWT), is preferred over the standard black foam for superficial surface wounds, tunneling wounds, or wounds with undermining. 42 The PVA foam is useful in situations where granulation tissue ingrowth is minimized, such as in wounds with skin graft. It does not stimulate granulation tissue formation due to its increased density, which restricts tissue ingrowth. 43 The increased density also increases the tensile strength of the foam, making it ideal for use in wounds with tunneling.
Decreased tissue ingrowth and increased tensile strength makes dressing changes more comfortable for the patient. The PVA foam is also hydrophilic due to the hydroxyl group in the PVA molecule, which contributes to its excellent performance in water absorption and retention. 44 This is an important consideration if the wound has copious exudate that subsequently prolongs wound healing.
Antimicrobial interface dressing
NPWT is frequently utilized as an adjuvant therapy for controlling wound infection along with wound debridement and antibiotic use. A novel NPWT technique has been developed, which utilizes a silver-containing PU open-cell foam. Silver is widely recognized for its antimicrobial activity and is regularly used in dressings for infected wounds. 45 In a randomized double-blinded clinical trial with 66 patients, open contaminated traumatic lower-extremity wounds were randomly treated with conventional PU foam NPWT (n = 31) and with silver-impregnated PU foam NPWT (n = 35).
The results demonstrated that the silver-impregnated NPWT group showed significantly lower bacterial culture positivity. In addition, the silver-impregnated NPWT was shown to be effective against methicillin-resistant Staphylococcus aureus. This NPWT modality also shows promise as a temporizing measure while these wounds are being prepared for definitive management. 46 In addition, polyhexamethylene biguanide (a cationic polymer with antimicrobial and antiviral properties) pre-impregnated gauze have been used as an interface dressing in NPWT systems. 41
Liner dressings
To inhibit tissue ingrowth into the interface dressing, nonadherent liner dressings are being used as a wound contact layer before the interface dressing. They are useful if there are blood vessels at the wound bed or concerns that the interface dressing is difficult remove. The liner dressings are also beneficial if significant wound contraction is expected due to rapid formation of granulation tissue. 47 Commonly, liner dressings also have antimicrobial properties to prevent and control infection. An example of this is the Acticoat™ flex, which is a silver dressing liner characterized by a nanocrystalline structure providing rapid release of silver ions to the wound. 48
It has been shown to be effective when used in combination with NPWT in the management of chronic infected wounds with large defects, such as in complex breast abscesses. Another liner dressing alternative is a one coated with a fatty acid derivative DACC (dialkyl carbamoyl chloride, Cutimed Sorbact®), which contains strong hydrophobic qualities. 49 It is the hydrophobic interaction with wound pathogens, which also contain hydrophobic characteristics that allow irreversible binding to the dressing and subsequent removal of pathogens from the wound. These dressings allow for the avoidance of local antiseptic or antibiotic ingredients, which allows avoidance of certain adverse toxic effects or development of microbial resistance. 50
Longer duration dressings
Normally the NPWT interface dressing is changed every 24 h to 72 h. To increase wear-time, longer duration interface dressings have been developed. Closed-incision negative pressure therapy (ciNPWT; Prevena™ Therapy, 3M) has been developed to be used on closed incisions to provide protection, remove exudate, and aid in closure. 51 These dressings can typically be kept in place for 7 days and has been shown to decrease the risk of surgical site infections and other postoperative complications because of its underlying mechanism.
The ciNPWT mechanism normalizes stress distribution surrounding the closed incision, enhances the apposition of incision lines, and increases lymphatic clearance. These lead to decreased rates of wound dehiscence as well as decreased risks of hematoma and seroma formation. 51 Longer duration between dressing changes can increase patient compliance, with one example able to be left on for up to 14 days (PICO System, Smith and Nephew). 52 It should be noted that closed incision NPWT is unique, data and time to dressing changes are not comparable with open wound data.
ROCF with through holes
The addition of a novel reticulated open cell foam with through holes (ROCF-CC) to the NPWT with instillation dwell time (NPWTi-d) has shown improved results as far as increased granulation tissue formation and improved wound debris removal. 53 Through holes refer to large holes in the ROCF, which help facilitate removal of thick wound exudate. An example of this system is Veraflo™ Cleanse Choice Complete™ Dressing. The use of ROCF-CC with NPWTi-d has been shown to successfully and more rapidly remove thick exudate, dry fibrin, wet slough, and other similar infectious materials from the wound bed.
This system can be utilized in large complex wounds not appropriate or possible for surgical debridement, or when there is stubborn nonviable tissue remaining on the wound surface. Another study showed similar positive outcomes with more rapid development of healthy granulation tissue after utilization of NPWTi-d with ROCF-CC over an average range of 5–14 days 54 (Fig. 2).
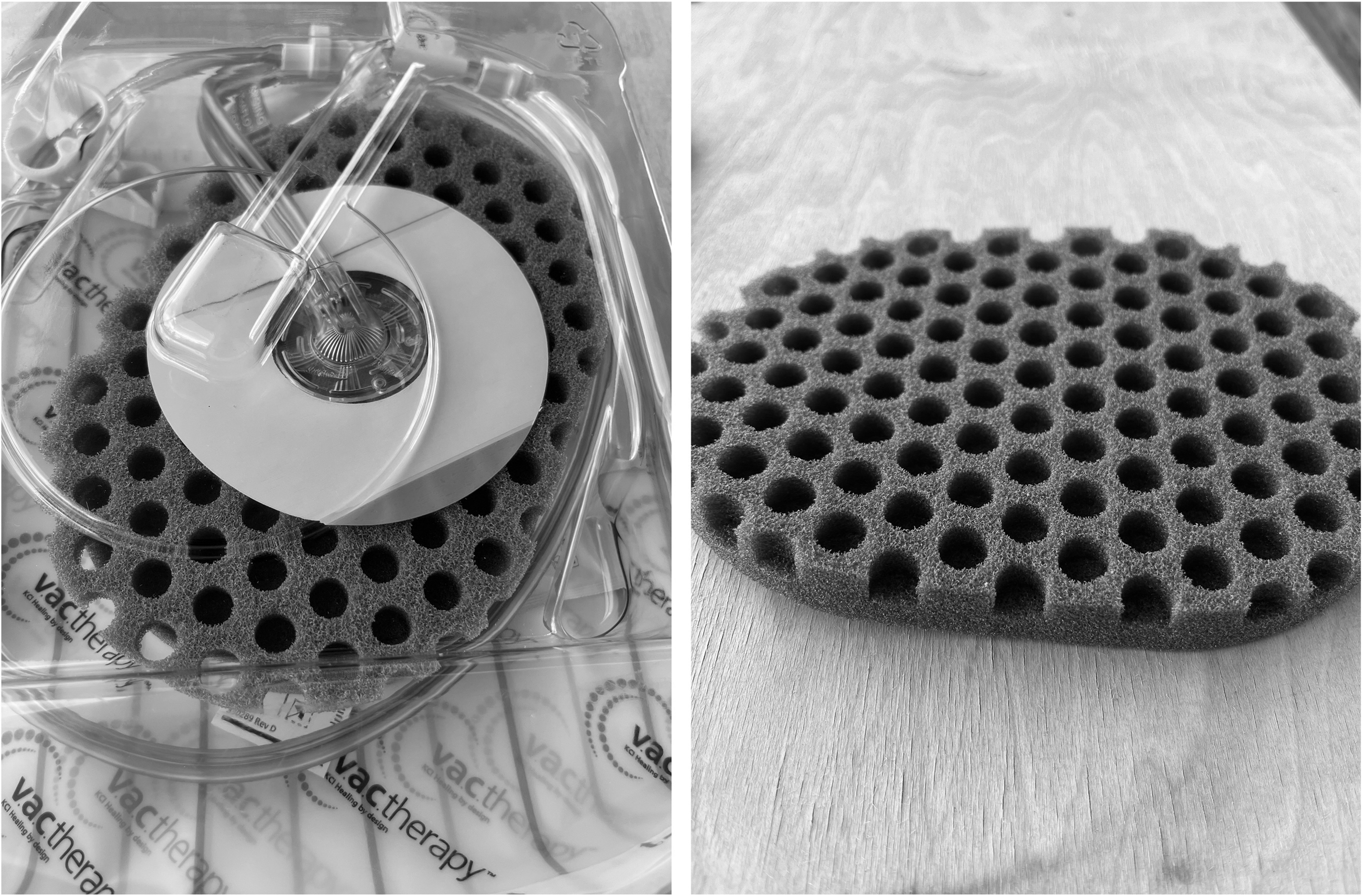
ROCF-CC. The large holes in this foam allow for increased granulation tissue formation within the holes forming a comedone appearance. The ROCF-CC foam in the picture is utilized in NPWTi, where saline or HOCl is infused into dressing and aspirated as part of foam. ROCF-CC, reticulated open-cell foam with through holes; NPWTi, NPWT with instillation; HOCl, hypochlorous acid.
Adhesive dressing
Maintaining an airtight seal in NPWT is of utmost importance. An inadequate seal can lead to a loss of negative pressure and ultimately failure of therapy, causing complications such as desiccation, contamination, or failure of closure. 55 Therefore, alarm systems are important in the management of seal issues. While inpatient, any seal malfunction with the NPWT will cause the system to alarm, prompting nursing evaluation and subsequent physician notification for adjustment as necessary. Mobile applications have also been developed to help health care professionals and patients to better manage NPWT systems.
These applications are particularly useful for patients with outpatient NPWT devices. 56 Another potential concern is periwound maceration. Skin maceration occurs when skin is in contact with liquid or moisture for too long. Maceration is undesirable because it causes pain and discomfort. Furthermore, it can decelerate wound healing and make skin more vulnerable to infection. 57 Wounds in anatomically difficult regions such as the anogenital area or the axilla often present challenges to maintaining a sealed vacuum system (Fig. 3). These regions are often tenuous due to moisture, irregular contour, increased movement, and excrement.

NPWT placed in anatomically difficult regions.
The traditional adhesive drape is usually derived from PU containing acrylic adhesive colloquially called “1–2 tape.” Multiple challenges exist with this dressing. 58 The first challenge is that the stiffer outer layer that is removed second is somewhat clunky, leading to poor contour adherence to an irregular surface when initially applying. This can lead to crevices and creases under the adhesive resulting in air leaks.
In addition, this adhesive dressing cannot be redone once applied if the user wants to redo the initial application or inadvertently sticks the dressing to itself or other unintended areas. Periwound skin can be sensitive in nature and subjected to medical adhesive-related skin injury from the application and removal of adhesives. 59 It has been shown that adhesives remove superficial epidermal cells that can compromise the inherent barrier function, subjecting the patient to worsening insensible water loss, infection, and/or skin breakdown. 60
Therefore, a balance must exist between an atraumatic removable adhesive that is not only strong enough to hold negative pressure and stick to naturally moist areas, but also flexible enough to conform to anatomically challenging areas. Applying these dressings can often require certain tricks to ascertain an airtight seal. Providers that have become proficient in applying NPWT adhesives dressings have used liquid adhesives (such as Mastisol®, Cavilon™, and Benzoin) to increase adhesion between skin and dressing, ostomy powder to dry excess moisture, ostomy paste to fill crevices in skin and around wound, as well as small adhesive strips (i.e., 5 cm) in irregular contoured areas. 61,62
A recent advancement in adhesive dressings used for NPWT has been developed, which contains the standard PU film with an adhesive silicone-acrylic hybrid drape that allows for repositioning after initial placement (Dermatac™). This dressing has been shown to be reliable in creating an airtight seal for NPWT in anatomically challenging areas, as well as to decrease patient discomfort during removal, and to reduce clinician application time. 58
Tubing
The third element in an NPWT system is the tubing that connects the airtight dressing to the vacuum pump. The proximal end of the tubing contains a port within an adhesive dressing, colloquially called the “lily pad” to be placed over a small opening (∼1–2 cm) created in the NPWT dressing. 2,63 Challenges may arise with the tubing, which must be discussed. First, if the dressing is on a pressure bearing region (i.e., sacrum), the tubing may cause a pressure injury to the patient's skin.
It is recommended to bridge dressings to a nonpressure bearing region to prevent these injuries from occurring. Commonly, bridging is made after applying the initial wound dressing, by first protecting the skin with the adhesive dressing, applying the standard PU foam bridge over that, followed by an additional piece of adhesive dressing with the port at the distal end (Fig. 4). 64 In addition, there are specifically designed bridge dressings that are available for ease of use.

Bridge dressings.
Bridging helps to avoid pressure injuries and also helps to prevent blockages in the tubing, often caused by kinking under the patient. If a blockage alarm is encountered and the tube has been effectively troubleshot (i.e., no kinking and no active clamps) there may be debris such as sloughing tissue or clot obstructing the tubing. This can often be solved by excising the port from the NPWT dressing and replacing it with a new lily pad and tubing system. 65
It is worth mentioning that not all tubing systems are universally consistent, and some are quite sensitive to positional changes in relation to the wound. Technology exists within that vacuum, facilitated by specially designed tubing that can measure pressure between the wound and the device, compensating for changes in pressure delivered and pressure measured at the wound (Sensa T.R.A.C™, 3M). McNulty et al. demonstrated a significant decrease (up to 7–10 × ) in actual pressure achieved when devices without regulated pressure feedback (RPF) were raised 90 cm above the wound. Systems that do not have RPF are limited as they do not reliably sense pressure delivered at the wound. 66
Negative pressure and pumps
Today there are multiple different NPWT pumps available that vary in their properties and size. Numerous vacuum pumps offer customization in amount of pressure applied as well as how it is delivered (Fig. 5).

NPWT pumps. Two main variations of pumps:
Vacuum pumps
Since its initial debut in the 1990s, the wound vacuum pump device has undergone several iterations over the years. Its overall transformation has primarily focused on more compact devices that deliver equivalent negative pressures, although the ability of the device to alter the amount of negative pressure applied to the wound and the way in which it is delivered cannot be overstated. Today, there are many devices on the market that are the size of a cell phone and can fit into a pocket.
Although these devices lack the technological innovation of the much larger and more cumbersome inpatient devices, they afford more discretion and allow the patient to go about their daily activities without advertising their ongoing wound care. 67,68 These portable devices sometimes have a predesignated life span without needing to be recharged; such innovation is purposeful, increases device compliance, and additionally is meant to indicate time of removal of the entire device and its components. 69
In contrast, larger systems, compared with the outpatient models, are popular in inpatient settings due to the diverse customization within its various settings. This tunability allows clinicians to tailor their provided care to the wound of interest. 70 Despite the pros and cons of the numerous devices on the market, they all succumb to common pitfalls, including need for troubleshooting, need for a source of electrical power, and device malfunction.
It is important to know the availability of the various NPWT devices carried by the hospital or institution so that therapy can be appropriately tailored. If available NPWT devices are limited and leads to subpar patient care and outcomes, consideration should be given to investing in additional varieties by the institution utilizing them.
Delivery of negative pressure
Although continuous pressure therapy (cNPWT) is the most traditionally used setting, intermittent (iNPWT) and variable (vNPWT) also exist. cNPWT delivers a constant pressure set on the device throughout the treatment. In iNPWT and vNPWT, the device alternates between two settings: In iNPWT, a set subatmospheric pressure alternates with atmospheric pressure (0 mmHg), whereas vNPWT (or cyclical therapy), alternates between two set subatmospheric pressures without returning to 0 mmHg (e.g., −125 and −50 mmHg). In both iNPWT and vNPWT, the time periods spent during each pressure setting can be adjusted. 71,72 A graphic depiction of each is displayed in Fig. 6.

Negative pressure delivery modes. Pressure graphs showing negative pressure on the y-axis in relation to time on the x-axis comparing the different modes:
In the original study by Morykwas et al. in 1997, they demonstrated that at a continuous pressure of −125 mmHg, blood flow increased at a rate of 4 × . At pressures of −400 mmHg, blood flow actually fell below baseline. 3 Based on these study results, many institutions, physicians, and manufacturing companies preferentially use a default of −125 mmHg for most wounds. However, various studies have demonstrated higher rates of blood flow at higher pressures. One prospective randomized study found that −300 mmHg generated a 5 × increase in cutaneous blood flow when used with standard black reticulated PU foam. 73
Although this study did not evaluate clinical wound healing, it may be extrapolated that higher rates of blood flow facilitate faster and more optimal wound healing. Unfortunately, higher pressure is accompanied by potentially increased patient discomfort, which may preclude these settings. Furthermore, higher negative pressure settings may actually impede blood flow in certain wounds or wound areas. Borgquist et al. demonstrated that at 0.5 cm from a wound edge, blood flow actually decreased by up to 30% from baseline at settings as low as −75 mmHg, despite an increase in blood flow at the center of the wound.
This should raise caution in using NPWT in wounds with concern for ischemia or hypoperfusion injuries. 69 Further caution may be warranted depending on the patient's physiology. For example, in a patient with a low mean arterial pressure (MAP) with a wound in which NPWT is applied, the wound may have a compounded risk for ischemia: not only does the low MAP predispose the entire wound to poor healing due to decreased oxygen and nutrient delivery, but also the NPWT may further disrupt blood flow to areas of the wound in an already at risk state. 74 Furthermore, specific location of the wound may prompt caution when using certain pressure settings.
For example, although −125 mmHg is a preferred setting for many wounds, there have been reports of cardiac rupture in deep sternal wounds at this pressure. 75 Hemodynamic changes and physiological derangement have both been raised as concerns when using negative pressure at higher settings. Although there does not appear to be any studies specifically looking at systemic physiological derangements in humans using NPWT, several porcine studies have been published that have not demonstrated significant changes to parameters such as cardiac output, MAP, pulmonary artery pressure, systemic vascular resistance, or central venous pressure when using NPWT. 75,76
Interestingly, Morykwas et al. also demonstrated more robust granulation tissue using iNPWT compared with cNPWT by about 40%. 3 It is thought that the repeated change in pressure allowed in both settings promotes tissue remodeling and healing to a greater extent than cNPWT. 16 With frequent and repetitive mechanical stimulation, these shearing forces stimulate the release of growth factors, cell division, and granulation tissue formation.
Many porcine studies have demonstrated that vNPWT appears to be superior to both iNPWT and cNPWT in terms of cellular proliferation and blood vessel density, leukocyte infiltration, and granulation tissue formation. 23,72,77 In addition, iNPWT and vNPWT may be less worrisome in wounds where hypoperfusion and ischemia are of greater concern; repeated alleviation in pressure prevents continuous tissue ischemia in the wound bed and at the edges. 70
However, patient discomfort still persists in both of these settings. The discomfort associated with iNPWT is largely due to the drastic changes in pressure with a return to atmospheric pressure. In vNPWT, since the wound is always under subatmospheric pressure regardless of the settings, this mode may cause less discomfort whereas still affording the benefits of repeated mechanical stimulation. 78
NPWT with instillation
NPWT with instillation (NPWTi) is another variation that may afford improved wound outcomes compared with standard therapy. Typically, this technology is only available in acute care and rarely in other settings. With instillation therapy, the NPWT device infuses a predetermined solution into the interface dressing and wound bed prior negative pressure returning and evacuating all fluid.
Several options for instillation fluid may be used with NPWT, most commonly normal saline or an antiseptic solution such as hypochlorous acid solution, hypochlorite solution, or acetic acid solution followed by saline solution for infected wounds. However, antiseptic solutions should be used cautiously given the risk of cytotoxic effects with longer duration use. 79
Biofilms remain an obstacle to optimal NPWT. They reduce the effectiveness of the therapy due to the creation of a slimy barrier between the sponge and the wound bed. 80 NPWTi has been associated with reduction in biofilm and bioburden in many studies, both in vitro and in vivo. For example, in a study done by Goss et al. evaluating NPWTi using Dakin's solution in post-debridement bioburden in chronically infected lower extremity wounds, they found a statistically significant reduction in the absolute bioburden of the treatment group wounds (10.6 × 106 vs. an increase in control group of 28.7 × 106, p = 0.016). 81
A separate study by Yang et al. demonstrated a mean reduction in quantitative biofilm bacteria of 48% in the treatment group (NPWTi with sodium hypochlorite 0.125%) versus 14% in the control group (p < 0.05), although there was no significant difference in wound healing at 1 week. 82
Further tuning affords the ability to set a dwell time (NPWTi-d) so that the wound bathes in the solution as opposed to undergoing simple irrigation. Lessing et al. demonstrated in porcine models that NPWTi-d with saline is associated with improved granulation tissue thickness by up to 57%, faster wound filling rates, and greater overall reductions in wound area and perimeter when compared with cNPWT, iNPWT, and vNPWT. 70 Although these results sound promising, other studies failed to show any difference between NPWTi-d and cNPWT in time to wound healing, proportion of healed wound, number of surgeries required for wound debridement, and reinfection rates. 83,84
However, Lessing et al. utilized instillation, which they separate from irrigation. They describe instillation as a period of time without pressure where the solution instills into the wound bed, followed by a soaking (dwell) time, then continuation of pressure. 68 Davis et al. and Lavery et al. utilized a continuous irrigation mode, wherein the pressure and the solution were simultaneously delivered in a constant manner. 83,84 In a retrospective cohort-controlled study by Kim et al., they found that NPWTi-d using variable instillation—similar to Lessing's described method—was associated with shorter hospital stay, shorter time to a definitive surgical procedure, higher percentage of wound closure, and improvement in culture burden compared with cNPWT.
To further complicate NPWTi-d, the solution being delivered is not standard; any solution can be used if it is compatible with the components of the NPWT device. 85 Some studies use saline, whereas others have used antimicrobial solutions or antibiotic-based irrigant, and some studies fail to specify what was used. Owing to the wide nature of variables for NPWTi-d, an expert multidisciplinary panel has recommended normal saline as the preferred solution with a dwell time of 10–20 min followed by 2–4 h of negative pressure at −125 mmHg for the majority of wounds.
Antimicrobial solutions were recommended for wounds with acute infection for the first 24–48 h. 86 The irrigation or instillation rate can also be adjusted, contributing to the overall difficulty in managing these systems and knowing which combination of variables is optimal. 70,83 –86
Future perspectives
Over the past decade there have been many advancements in NPWT as described in this review article. In comparison with the NPWT systems 20 years ago, the current technologies enable patients to be mobile and the dressings can be left on the wounds for longer periods of time allowing the use of the NPWT even at home. In addition, modalities such as NPWTi and antimicrobials have been introduced. Regardless, there is still room for improvement and future NPWT systems should focus on solving the issues related to the current technologies. Novel and emerging tissue engineering and regenerative medicine approaches such as various biomaterials and smart dressings with sensors could potentially be utilized in the future NPWT systems.
NPWT without the filler material
The biggest issues with todays' NPWT systems are related to the interface dressing, most commonly foam or gauze. Platform wound device® (PWD®) is a novel single component NPWT dressing that eliminates the need for the interface material. The PWD consists of an impermeable embossed membrane with an integral adhesive. 87 A suction pump is connected to the underside of the membrane with tubing. Once the suction pump is started, the embossed membrane is pulled into contact with the entire surface area of the wound.
The embossed pyramids in the membrane provide primary distribution channels for negative pressure and the wrinkles in the redundant membrane provide secondary channels. 88 The lack of the interface dressing decreases the pump capacity requirements and, therefore, the PWD can operate at much lower negative pressure than other devices. In a recent preclinical study, it was demonstrated that the PWD accelerated wound healing, reduced tissue necrosis, inflammation, and bacterial burden in the treatment of full-thickness wounds at pressure level of −50 mmHg. 89
Another preclinical study in pigs compared the PWD with conventional NPWT systems in the treatment of both excisional wounds and incisions. The study indicated that there was no difference in wound healing between the NPWT systems with the interface dressing and the PWD. Furthermore, the PWD is transparent enabling monitoring of the wounds without dressing removal. This commercially available technology has also been validated in a clinical setting and has been cleared through the U.S. Food and Drug Administration 510k pathway as a class II device 90 (Fig. 7).
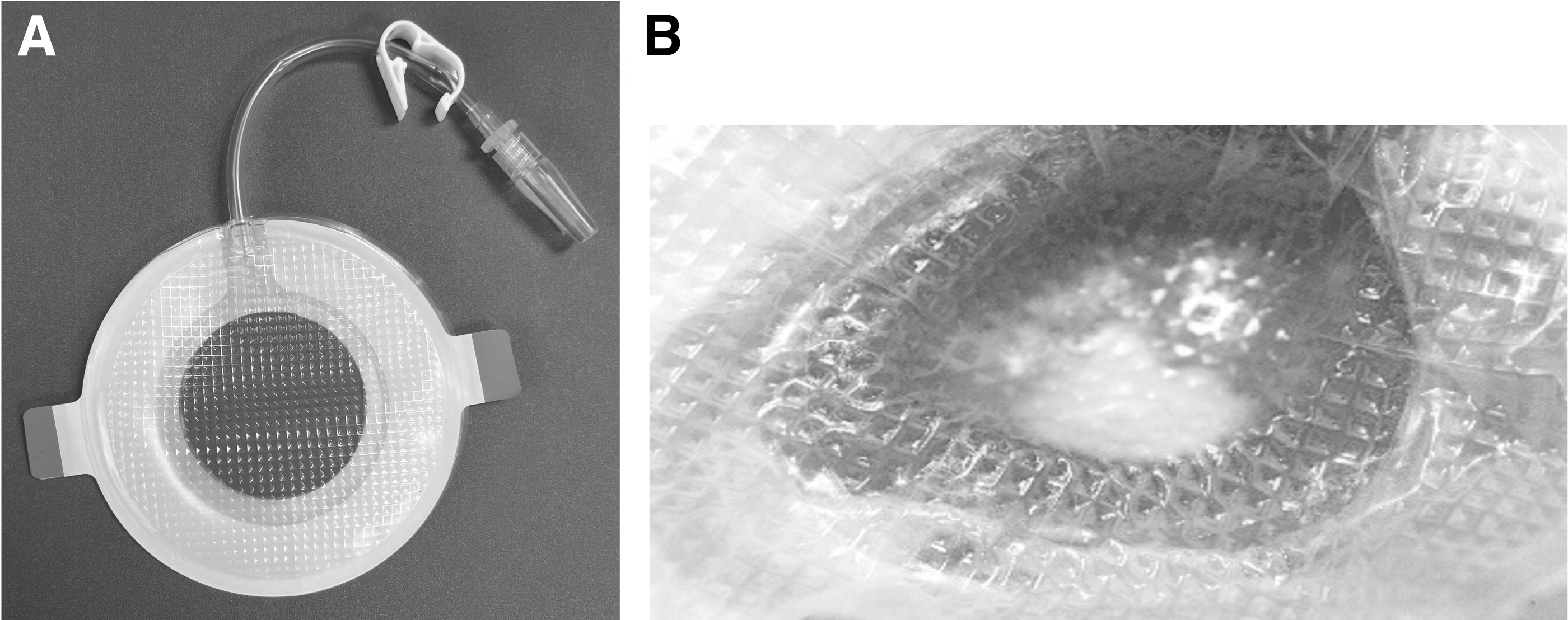
Platform wound device® (PWD®). A foamless interface dressing designed to reduce the risk of dressing incorporation and improve ease of application.
Similarly, a recent preclinical introduced a peel and place dressing that also does not have a foam or gauze. Instead, it consists of a multilayer dressing with a PU manifolding core and a silicone-acrylate combination adhesive tape for the periwound interface. This dressing was also developed to eliminate issues related to the interface dressing and it enables a longer wear-time to decrease frequency of dressing changes and patient discomfort.
The study showed that the dressing reduced the risk of tissue ingrowth and was characterized by low dressing peel force at removal. In addition, the study demonstrated that upon removal, the peel and place dressing decreased the presence of dressing fragments in the wound, significant bleeding, and signs of irritation or infection compared with traditional interface dressings (foam or gauze). It was also shown that wound fill was increased and wound area decreased in the peel and place dressing compared with the conventional foam interface dressing. 91
NPWT with novel biomaterials
Today there are numerous novel biomaterials that have been successfully utilized in wound care. These novel biomaterials can be loaded with wound healing promoting factors or antimicrobial agents and their release properties can be customized. In addition, these scaffolds can be engineered to be biodegradable in the wound. The use of biodegradable interface dressing in NPWT systems could be appealing. The biodegradable foam dressing would negate the need for repeated dressing changes, decreasing the burden on the patient and provider.
In 2011, Liu et al. investigated this idea by developing a biodegradable poly(ɛ-caprolactone) (PCL) foam showing similar function compared with traditional PVA foam in proof of concept testing. 92 Later in 2017, Warner et al. attempted to fabricate various other biodegradable dressings, showing that a copolymeric poly(lactide-co-glycolide) at a lactide:glycolide ratio of 50:50 combined with PCL at either a 75:25 or 50:50 ratio degraded significantly after 21 days of subcutaneous implantation in rats. 93
Three-dimensional printing of biomaterials is another emerging field in tissue engineering that could be utilized in NPWT. This would allow each dressing to be specifically designed for each wound bed, no matter how irregular the contour. Therefore, the need of cutting multiple pieces of foam at the patient's bedside, or stapling multiple pieces together would be avoided. This would also allow for consistent application with each dressing change.
Although bioprinting has found its way into the medical community, the idea of 3D printed NPWT dressings, biodegradable or not, has yet to be published. 94,95 Not only would a 3D printed dressing allow for custom shape, but also custom components specifically designed for each patient. This could include antibiotics, growth factors, or even stem cells. A recent trial of a novel platelet-derived growth factor embedded hydrogel dressing proved promising by showing larger amounts of neovascularization, collagen deposition, and thicker epidermis by day 12 compared with their control in full thickness wounds in a murine model. 96
In addition, a dressing was created using a novel class of antimicrobials called lipophosphonoxins that have been shown to combat antibiotic resistance due to their rapid membrane-targeting mode of action. 97,98 Not only did they demonstrate antibacterial activity while not impairing proliferation of fibroblasts and keratinocytes but also that there was no systemic absorption. Combining their findings with the low propensity for resistance and embedding this into an NPWT foam dressing is a very intriguing and promising idea.
NPWT with biosensors
Smart dressings with biosensors are of recent interest in the wound healing community. It has been demonstrated that at least pH, temperature, oxygen, and moisture have shown promise as potential markers for assessing the status of the wound. 99 Currently, monitoring of the wounds is performed through repeated dressing changes by medical professionals.
This is expensive and time consuming. NPWT systems with incorporated biosensors that could monitor the wound environment and provide real-time information on the status of the wound without the need for opening the bandage would be very beneficial. This would especially be useful in the management of chronic wounds that are often described as being in a persistent inflammatory state sometimes never reaching the proliferation or remodeling state. 100 Owing to their chronicity requiring prolonged care, there exists a need for a smart dressing able to detect when intervention, such as debridement, is needed. 101
TAKE-HOME MESSAGES
NPWT is routinely used in the management of both acute and chronic wounds.
Conventional NPWT systems comprise an interface dressing, adhesive dressing, tubing, and a pump.
There are multiple challenges related to the use of the NPWT.
Research and development projects have been conducted over the years to improve the current technology.
Novel and emerging tissue engineering and regenerative medicine approaches could be utilized in the future NPWT systems.
SUMMARY
NPWT is an efficient treatment modality that is utilized in the management of all kinds of wounds from nonhealing wounds to large traumas and surgical incision. Since its invention in the 1990s the NPWT technology has evolved from hospital-use to out-patient and even home use, and each of its components has had several advancements. Antimicrobial silver-impregnated sponges, open-hole foam that promotes removal of infected sloughing tissue, adhesive drapes that allow for repositioning on initial placement, and devices that allow instillation of various solutions are just a few of these advancements.
Staying up to date with these advancements not only helps the clinician to choose the right device and settings, but also ultimately helps the patient achieve the best wound healing outcome. Although challenges still persist, the future and technological advancements of NPWT—to include creating a bioabsorbable dressing to decrease foreign body reactions and utilizing evolving 3D printing and biosensor technologies to create the ideal negative pressure dressing—remain promising.
ACKNOWLEDGMENTS AND FUNDING SOURCES
Rodney Chan, MD, Victoria Diaz, RN, and Kristin Anselmo, RN are thanked for providing photos to Figs. 1, 3, and 4.
No funding was received to support this work.
AUTHOR DISCLOSURE AND GHOSTWRITING
The authors declare no conflict of interests. No ghostwriters were involved in the writing of this article.
Footnotes
DISCLAIMER
The views expressed in this article are those of the author(s) and do not reflect the official policy or position of the U.S. Army Medical Department, Department of the Army, DOD, or the U.S. Government.
ABOUT THE AUTHORS