
Abstract
Significance:
Pathologic scarring occurs secondary to imbalances in the cellular mechanisms of wound healing and affects millions of people annually. This review article aims to provide a concise overview of the pathophysiology and management of pathologic scarring for clinicians and scientists alike.
Recent Advances:
Contemporary research in the field has identified aberrations in transforming growth factor-β/small mothers against decapentaplegic (TGF-β/SMAD) signaling pathways as key drivers of pathologic scar formation; indeed, this pathway is targeted by many treatment modalities and translational investigations currently underway. Although intralesional injection of corticosteroids has been the gold standard in the treatment of pathologic scarring, studies show greater treatment efficacy with the use of combination injections such as triamcinolone/5-fluorouracil and triamcinolone/botulinum toxin. Adjunctive therapies including ablative fractional carbon dioxide/erbium-doped yttrium aluminum garnet and non-ablative pulsed-dye lasers, microneedling, and carboxytherapy have shown encouraging results in small cohort studies. Translational investigations involving the use of nanogels, RNA interference, and small molecules targeting TGF-β/SMAD pathways are also currently underway and hold promise for the future.
Critical Issues:
The heterogeneous nature of hypertrophic scars and keloids poses significant challenges in formulating standardized treatment and assessment protocols, thereby limiting the conclusions that can be drawn.
Future Directions:
Rigorous clinical trials into the individual and synergistic effects of these therapies would be ideal before any definitive conclusions or evidence-based treatment recommendations can be made. Owing to the heterogeneity of the pathology and patient population, well-conducted cohort studies may be the next best option.

SCOPE AND SIGNIFICANCE
The aim of this work is to provide a concise overview of the literature regarding key principles of pathologic scarring as well as a comprehensive update on the variety of available treatment modalities and future directions for investigation.
A search of PubMed, Medline, OVID, and Cochrane was performed using the terms “pathologic scar” OR “hypertrophic scar” OR “keloid” AND “treatment” to identify relevant basic science research, clinical studies, and review articles with a focus on contemporary peer-reviewed works published from 2017 to 2023. Of these, publications were then selected for discussion in this review based on significance, generalizability, novelty, and overall relevance to the broader topic.
TRANSLATIONAL RELEVANCE
This review highlights the latest advances in the molecular understanding of pathologic scarring and evaluates data from the most promising translational investigations currently underway. This discussion includes a variety of proteins, gene therapies, growth factors, and inhibitory molecules that show promise as potential targets for novel therapies.
CLINICAL RELEVANCE
Pathologic scar formation affects over 100 million people annually and causes both functional and psychologic issues that limit activities of daily living and quality of life. 1 In addition to compression garments and corticosteroid injection, which have been the mainstays of scar management for over a decade, this review discusses the mechanisms and efficacy of the latest adjunctive modalities currently used in clinical practice.
BACKGROUND
Introduction
Pathologic scarring is a common modern clinical challenge with deep historical roots. Keloids were first depicted in the Smith papyrus in 1700 BC, then described in Nigerian folk art as early as the 13th century, and formally defined in 1806 by Alibert who derived the name from the Greek word for crab claw, chele, in reference to the lesion’s invasion of adjacent tissue. 2 The heterogenous presentation and varying definitions of pathologic scarring make accurate estimations of overall prevalence difficult to estimate. The disease phenotype is dependent on the interaction between wound characteristics, overall health, the environment, and individual genetic as well as epigenetic factors. 3 Importantly, measurements of disease burden differ widely across ethnic groups with studies consistently demonstrating higher incidence in populations of color, that is, individuals of African, Hispanic, and Asian descent. 4 Although both adults and children are affected by the consequences of scarring, children are uniquely impacted by pathologic scar formation because of their underdeveloped immune systems, thinner skin, and vulnerability to severe injuries. 5 Thus, a comprehensive understanding of the clinical and molecular features of pathologic scarring is critical to developing treatments that will meet the needs of all patients with special consideration given to the most vulnerable populations.
The healing cascade
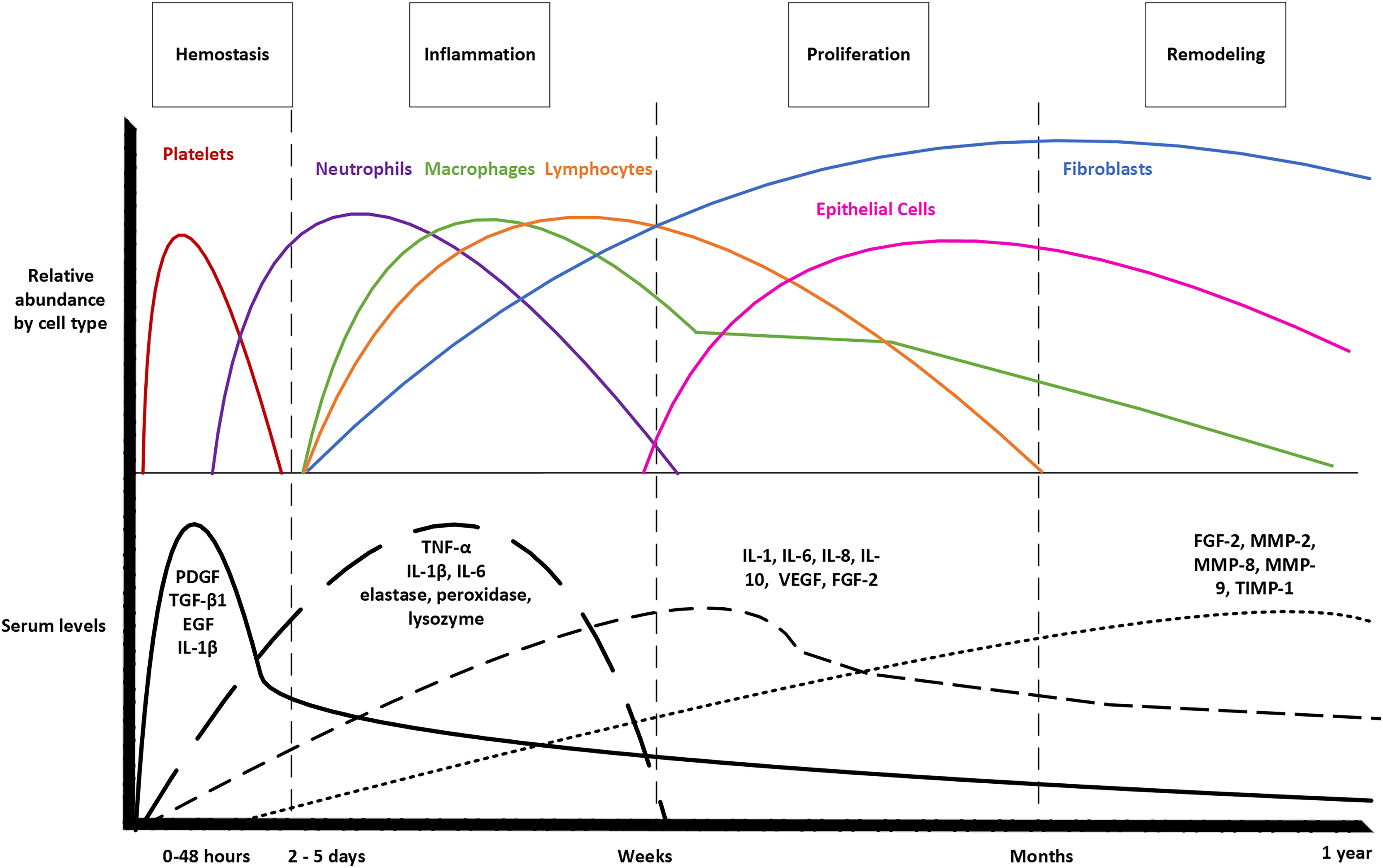
Wound healing begins immediately after acute injury and occurs in three overlapping and interrelated phases characterized by histologic changes in the wound bed. 6 First, the inflammatory phase begins following inciting damage to the capillaries that results in a platelet plug and fibrin clot formation. This temporary matrix stops further blood loss and provides a scaffold for repair; simultaneously, chemokines secreted by platelets stimulate recruitment and activation of a variety of inflammatory and immune cells including neutrophils and macrophages. Second, the proliferative phase is marked by the migration and proliferation of fibroblasts, keratinocytes, and endothelial cells and includes the vital functions of angiogenesis, which restores vascular perfusion to the wound, and re-epithelialization. Indeed, the initial hypoxia within the wound bed, which results from the disruption of normal vasculature, is a key stimulus for the release of growth factors and other regulatory molecules necessary for wound healing. Fibroblasts, once activated in the granulation tissue, then synthesize the extracellular matrix (ECM) that will replace the temporary fibrin scaffold. Some fibroblasts differentiate into myofibroblasts with contractile properties that play a key role in wound contraction and maturation. During the proliferative phase of healing, re-epithelialization occurs secondary to keratinocyte proliferation and migration to the wound edge. Remodeling, the final phase of healing, is a balance between matrix deposition by fibroblasts and myofibroblasts and degradation of the matrix driven by the actions of matrix metalloproteinases (MMPs), which are proteolytic enzymes, and their inhibitors. During remodeling, the ECM within the granulation tissue is reduced and components are modified to resemble normal unwounded dermis more closely; specifically, type III collagen is replaced by type I and elastin is deposited. Transforming growth factor-β1 (TGF-β1) acts as a key regulator of this process by promoting fibroblast migration, proliferation, and collagen deposition as well as inducing the epithelial-to-mesenchymal transition in which epithelial cells assume a fibroblast or myofibroblast phenotype. 6 As wound healing concludes, there is a relative quiescence in cellular activity and a reduction in cell number secondary to apoptosis of myofibroblasts and endothelial cells. In cases of prolonged inflammation in the wound bed, healing continues to proceed along a pathologic pathway with aberrant remodeling resulting in hypertrophic scars (HTS) or keloids in the skin and fibrosis in the internal organs. It is believed that pathologic scarring occurs when granulation tissue continues to expand because of excessive secretion of pro-fibrotic growth factors, resulting in deficient induction of normal cellular apoptosis and matrix remodeling.
HTS and keloids
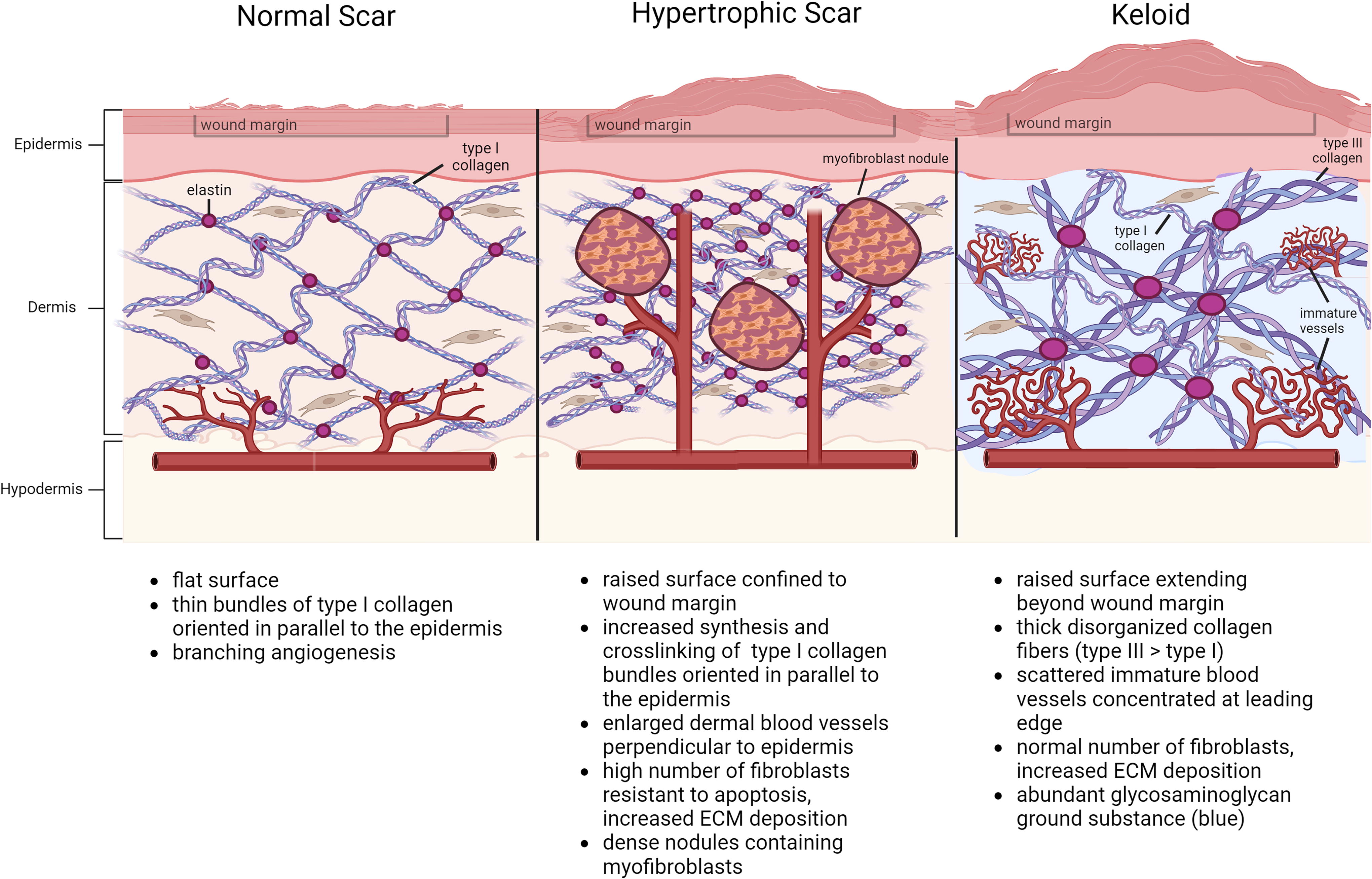
The hallmark of both HTS and keloids is a prolonged healing response to injury, resulting in excessive cell proliferation, vascularization, and collagen deposition (Fig. 1). 7 Although both types of pathologic scars can often present quite similarly, these entities can in fact be differentiated based on clinical, epidemiologic, and histologic differences (Table 1). 6 HTS occur within 4–8 weeks following injury, most often after surgery or burns, and exhibit rapid growth then spontaneous regression over time and most commonly affect regions under high tension such as the shoulders, neck, knees, and ankles. Typically, children are more susceptible to HTS; however, HTS commonly occurs in adults with surgical wounds under tension, including median sternotomy, abdominoplasty, and cesarean section incisions. Conversely, keloids can occur spontaneously or after minor or inconsequential injuries among predisposed individuals and persist without spontaneous regression. Keloids have a predilection for the anterior chest, shoulders, earlobes, arms, and face. Clinically, HTS are confined to the initial wound margins and have lower recurrence rates after excision as opposed to keloids that continue to grow beyond the original borders and have high rates of recurrence. On histology, HTS contain type III collagen bundles that are well organized in parallel to the epidermis and contain nodules of excess myofibroblasts and mucopolysaccharide. Keloids, in comparison, are comprised of disorganized bundles of type I and type III collagen that are relatively hypocellular yet thickened with hyalinized collagen and contain scattered dilated blood vessels without myofibroblast nodules (Fig. 2). 8,9 Though much remains to be discovered regarding the molecular mechanisms of pathologic scarring, emerging differences in the cellular characteristics and expression profiles further underscore the distinction between these two disease entities.
A Comparison of key clinical, macroscopic, and microscopic features of hypertrophic scars versus keloids
α-SMA, α-smooth muscle actin; TGF, transforming growth factor.
Cellular abnormalities
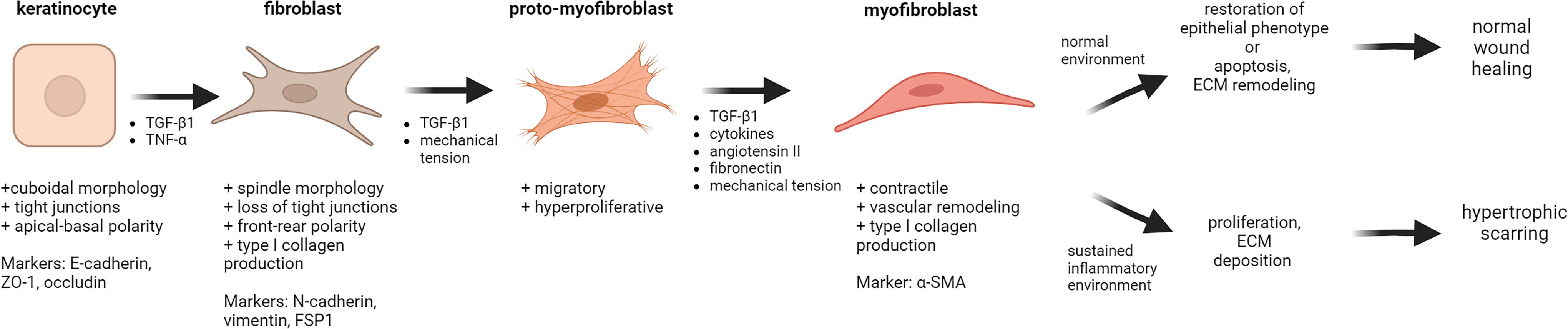
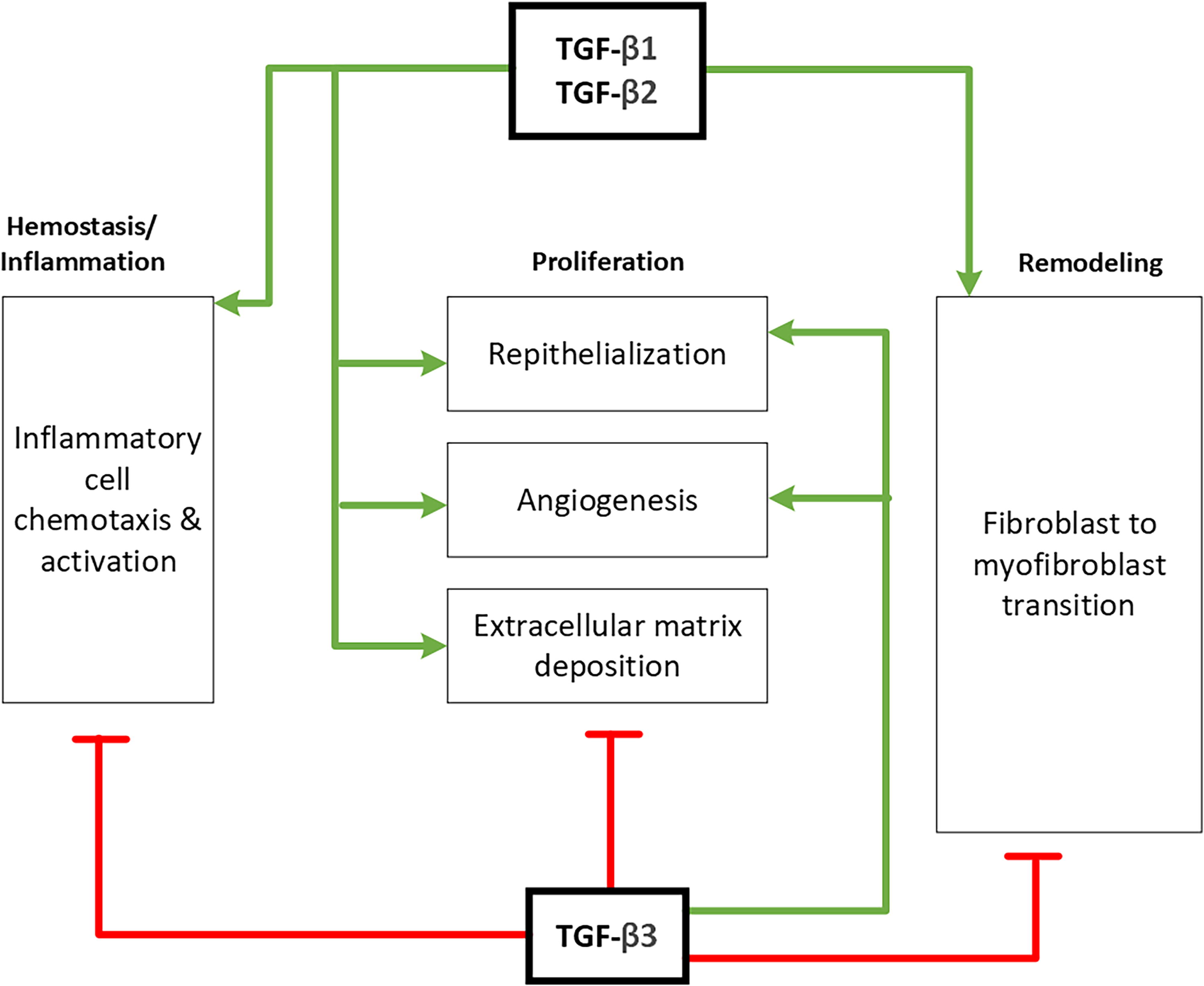
Alteration in fibroblast phenotype is the common thread underlying HTS and keloid formation. Soon after acute injury, platelet degranulation results in the release of inflammatory cytokines and growth factors, which then serve to recruit the variety of cell types required for healing including neutrophils, macrophages, mast cells, fibroblasts, epithelial cells, and endothelial cells. In normal wound healing, exposure to inflammatory factors, namely TGF-β1 and tumor necrosis factor-α (TNF-α), prompts keratinocytes in the wound bed to temporarily adopt fibroblast-like features, including spindle morphology and loss of tight junctions. This reversible phenotypic transition is necessary to enable keratinocyte migration to the wound edge for re-epithelialization and generation of fibroblasts and myofibroblasts for ECM deposition and wound contracture. 10 In pathologic healing, however, it is theorized that prolonged exposure to pro-inflammatory signaling molecules impairs this reversal, thus resulting in persistent fibroblast activity and scar formation (Fig. 3). 11 Fibroblasts isolated from pathologic scars not only exhibit an increased and prolonged expression of growth factors, most notably TGF-β1 and platelet-derived growth factor (PDGF), but also demonstrate increased numbers of growth factor receptors that respond exuberantly when activated. 7 Fibroblasts exposed to inflammatory molecules and mechanical stress further differentiate into myofibroblasts that express high levels of α-smooth muscle actin (α-SMA) and exhibit highly contractile properties as well as increased collagen production that results in dysfunctional remodeling. 12 The TGF-β family of polypeptides comprises three isoforms, TGF-β1, -β2, and -β3, which are highly conserved among mammals and play pivotal roles in both normal and pathologic wound healing. Each isoform has a distinct function in orchestrating this process, which can vary depending on complex signaling interactions and the phase of healing—indeed, there is much contradiction and debate on this topic in the literature. In general, TGF-β1 and -β2 stimulate collagen synthesis and prevent matrix degradation in the early phases of wound healing, whereas TGF-β3 appears in later stages and serves to regulate TGF-β receptor activity, thereby reducing ECM deposition (Fig. 4). 7 Inappropriately strong and persistent expression of TGF-β1/2 is characteristic of both types of pathologic scarring albeit with subtle differences. Keloid fibroblasts demonstrate overexpression of both TGF-β1 and -β2 with low expression of TGF-β3, whereas those from HTS have significantly lower TGF-β2 levels. 8 Administration of exogenous TGF-β3 or neutralizing antibodies to TGF-β1/β2 reduced postoperative scar formation in animal models; however, multiple clinical trials of recombinant TGF-β3, neutralizing antibodies against TGF-β1/β2 (fresolimumab, metelimumab), and inhibitors of TGF-β1/β2 (mannose-6-phosphate) have failed to demonstrate satisfactory efficacy. 13,14 Similarly, estradiol has also been shown to accelerate wound healing and promote collagen homeostasis via reduction of pro-inflammatory cytokines including TGF-β1 and TNF-α, however, clinical trials studying intralesional injection of estradiol-based agents for scar treatment have thus far demonstrated inadequate results. 15,16
A molecular understanding
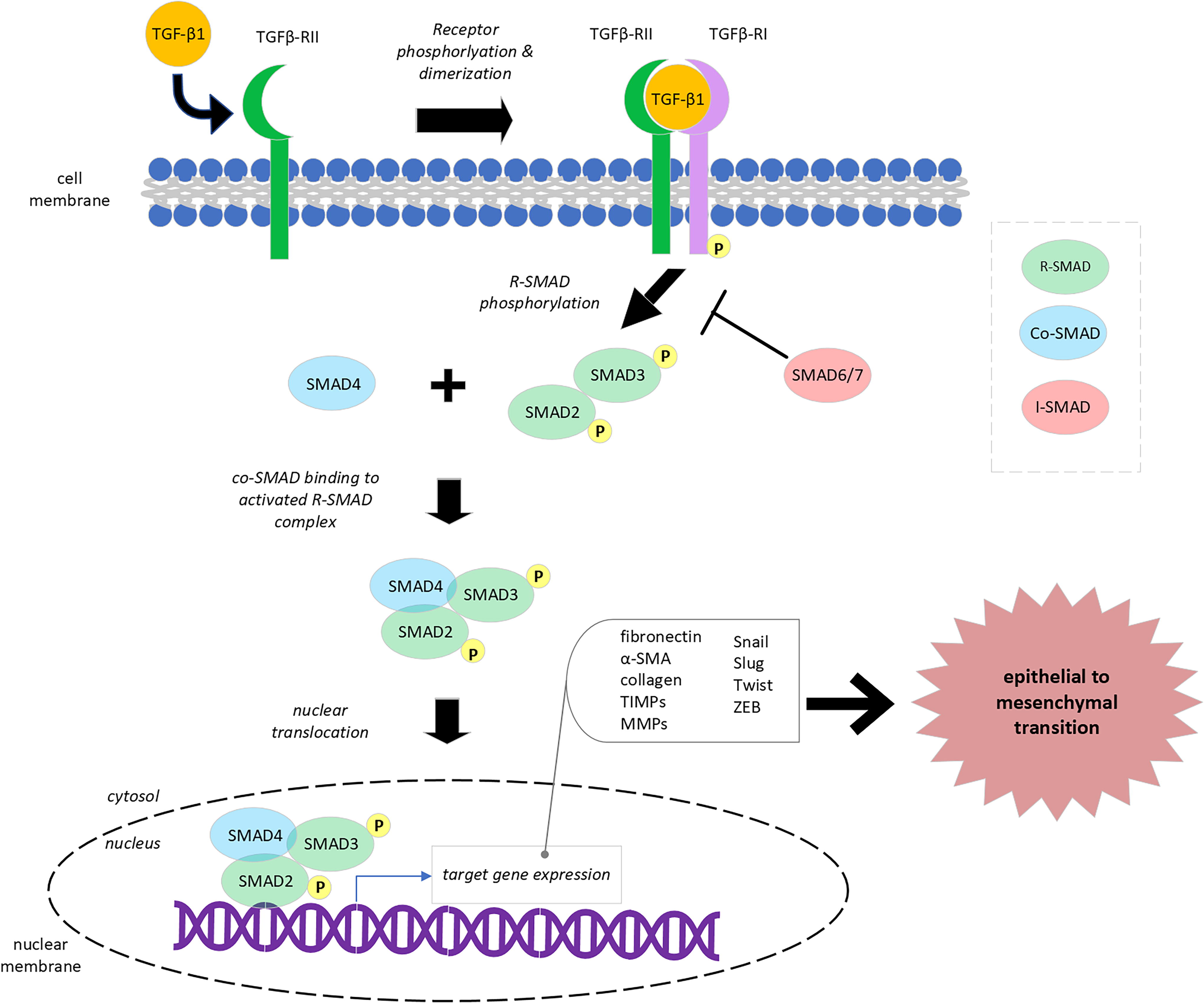
Aberrations in TGF-β isoform expression and signaling are largely mediated via the small mothers against decapentaplegic (SMAD) signal-transduction pathway (Fig. 5). 17 Binding of TGF-β1 to the type II cell-surface receptor (TGFβ-RII) results in dimerization with and phosphorylation of the type I receptor (TGFβ-RI), which then activates receptor-regulator SMAD 2, 3, and 4 proteins (R-SMADs) via phosphorylation—specifically, SMADs 3 and 4 are key intermediaries of increased autocrine stimulation in HTS fibroblasts. 17 Activated R-SMADs join with common-mediator SMADs, and this entire complex translocates to the nucleus, where it recruits transcription factors to activate expression of target genes, many of which are key drivers of fibrosis. Inhibitory SMAD 7 (I-SMAD) provides negative feedback to this mechanism by forming stable bonds with activated TGFβ-RI, thus preventing R-SMAD phosphorylation, activated complex formation, and downstream gene expression. 18 The relevance of this pathway to pathologic scarring is underscored by studies demonstrating decreased ECM deposition by keloid fibroblasts via downregulation of SMAD3 and upregulation of SMAD7. 17
Disequilibrium
In addition to excess anabolic activity, deficiencies in catabolism during the final maturation phase of wound healing further contribute to the abnormal phenotype of HTS and keloid fibroblasts. MMPs are a highly conserved family of cation-dependent proteinases that are vital to connective tissue remodeling in the last stage of wound healing and after wound closure. MMP expression in fibroblasts is regulated largely by cytokines and growth factors, namely, interleukin-1β (IL-1β), PDGF, epidermal growth factor (EGF), and TNF-α, which are secreted by immune cells secondary to complex cell–cell interactions (Fig. 1). 7,19 MMPs also cleave chemokines and are necessary mediators for negative feedback of the inflammatory cascade. Specifically, MMP-9 predominates in early wound remodeling via the breakdown of native collagen types IV and V as well as elastin and fibronectin followed by MMP-2 degradation of denatured collagen products. 7 A disintegrin and metalloproteinase with thrombospondin motifs (ADAMTS) is a superfamily of proteoglycanases that regulate ECM turnover and maturation. 20 Tissue inhibitors of metalloproteinases (TIMPs) are a family of endogenous MMP inhibitors that are expressed by a variety of cells in the wound bed and have specific targets. For example, TIMP-1, an inhibitor of MMP-1, is produced by keratinocytes, fibroblasts, smooth muscle cells, and endothelial cells and can be found in healing excisional and burn wounds, specifically around blood vessels. TIMP-3 is most notably expressed in granulation tissue by macrophages, keratinocytes, fibroblasts, and endothelial cells and is a significant inhibitor of MMP-1, -2, -3, -9, and -13 as well as ADAMTS. 20 Interestingly, HTS and keloid tissue samples demonstrate high levels of MMP-2 and relatively low MMP-9 as compared with normal skin tissue, which suggests an imbalance rather than an absolute deficiency in MMP isoforms in pathologic scar formation. 21 Apoptosis is a necessary component of normal healing and is required for the transition from granulation tissue to mature scar formation; normally, apoptosis of myofibroblasts occurs 12–20 days after injury as epithelialization and collagen deposition commence. As mentioned previously, HTS are hypercellular with a high percentage of myofibroblasts, which persist for a far longer period than in normal skin or scars. It is theorized that the aberrant cellularity and matrix deposition seen in pathologic scarring are largely driven by delayed maturation secondary to chronic dermal inflammation in the wound bed.
Inflammasomes and immune activation
Complex interactions between immune and nonimmune cells, as well as the activation of inflammasomes, multimeric protein structures that mediate the innate immune response to cellular stress, have been implicated as drivers of pathologic scar formation. Neutrophils and M1 macrophages infiltrate the wound bed within minutes after injury and trigger the release of inflammatory molecules, which then usher in the next phases of healing. Specifically, the nucleotide-binding oligomerization domain, leucine-rich repeat and pyrin domain-containing-3 (NLRP3) inflammasome is responsible for the production of IL-1 and IL-18, which induce fibroblast activation and ECM deposition. 22 As the transition from the inflammatory to the proliferative stage of healing occurs, macrophages transition from the pro-inflammatory M1 phenotype to the anti-inflammatory M2 phenotype. M2 macrophages serve to further promote angiogenesis and epithelialization, remodel ECM, and downregulate inflammatory cascades. 22 IL-10, a key anti-inflammatory cytokine produced by macrophages, functions via downregulation of T cells and sequestration of pro-inflammatory cytokines including IL-6 and IL-8. Phase I/II clinical trials have demonstrated potential efficacy of recombinant human IL-10 for scar healing; however, phase III trials have not been conducted. 14
Dysregulation of the NLRP3 inflammasome has been implicated in pathologic wound healing, including diabetic wounds and keloids, as well as a variety of other clinical entities, including pulmonary, cardiac, hepatic, metabolic, and autoimmune diseases. Both in vitro and in vivo studies have demonstrated higher levels of NLRP3 in keloid and HTS fibroblasts, with concomitantly increased expression of its activator Notch1 and its products IL-1 and IL-18, as well as downstream expression of the inflammatory transcription factor nuclear factor kappa-light-chain-enhancer of activated B cells (NFκB). 22 Upregulation of Notch1 in keloid fibroblasts can result in resistance to autophagy and negative signaling feedback resulting in persistent expression of NLRP3; although NLRP3 is pivotal for M1 macrophage polarization, numerous studies have demonstrated a predominance of M2 macrophages in keloids. As a potential explanation for this finding, Huang et al. propose that NLRP3 expression in M2 macrophages is pro-fibrotic via a “noncanonical inflammasome pathway,” wherein IL-4 prompts further macrophage differentiation into the M2a subtype, which is known to promote fibroblast and endothelial activity. 22
Our understanding of the complexities of wound healing biology continues to evolve and will remain of great interest to clinicians and scientists alike for years to come. Although investigations are ongoing into these mechanisms and the varying ways they can be manipulated for therapy, it already appears evident that early interventions focused on facilitating rapid healing and minimizing inflammation will be paramount in the treatment and prevention of pathologic scars.
DISCUSSION: TREATMENT STRATEGIES
A wide array of treatment modalities for HTS and keloids have been trialed, with varying outcomes reported in the literature. The range of proposed treatments, each with their own constraints and rates of success, speaks to the difficulty in obtaining consistent results and formulating a consensus regarding best practices. Our literature search identified promising topical and injectable agents, ranging from botulinum toxin (BTX) and 5-fluorouracil (FU) to autologous skin components, as well as therapeutic laser, radiation, and shock wave modalities that have demonstrated satisfactory results in small cohort studies.
Topical therapies
Topical application of silicone gel or sheeting is considered the first line for the treatment of mild HTS and can be offered prophylactically to patients with a tendency toward pathologic scarring. It is hypothesized that silicone dressing hydrates and occludes the wound, resulting in impaired capillary activity, thereby downregulating TGF-β2 and downstream collagen deposition. 23 A meta-analysis by Wang et al. (2020) examined 6 randomized controlled trials (RCTs) with a total of 375 patients of all ages and found that topical silicone reduced postoperative scar pigmentation and height and improved pliability scores. Of note, silicone gel and sheet therapy were comparable in efficacy to each other and to other non-silicone topical treatments, including topical methylprednisolone, petrolatum, and onion extract. 23
Intralesional injections
Intralesional injection of corticosteroids for the treatment of pathologic scarring and contracture was first described in 1966 by Dr. Lynn Ketchum. Although triamcinolone acetonide (TAC) remains a popular injectable therapy today, the addition of adjunctive drugs including 5-FU, botulinum toxin type A (BTA), bleomycin (BLM), and verapamil (VER) has shown to be an efficacious and safe tool in the scar treatment armamentarium. 24,25 TAC primarily works in the treatment of pathologic scars via its anti-inflammatory and antimitotic effects, which inhibit fibroblast growth, endothelial budding, and ECM synthesis while also promoting degeneration of collagen and fibroblasts. 5-FU is a pyrimidine analog that inhibits thymidine synthase and is commonly used as a chemotherapeutic agent because of its potent inhibition of nucleic acid synthesis and cell proliferation. In pathologic scars, 5-FU has been shown to inhibit fibroblast and endothelial proliferation and type I collagen production secondary to TGF-β1 signaling. BTA is a neurotoxin naturally produced by Clostridium botulinum that reduces tension on the wound edge when injected into pathologic scars which results in reduced TGF-β1 expression and causes fibroblast cell cycle arrest in the quiescent G0 and G1 phases. BLM, isolated from Streptomyces verticillus, is a commonly used antibacterial, antiviral, and antitumor agent because of its potent inhibition of DNA, RNA, and protein synthesis. When injected intradermally, BLM is toxic to keratinocytes and eccrine epithelial cells and reduces collagen cross-linking via inhibition of lysine oxidase. Lastly, VER is a calcium channel blocker and has been shown to increase pro-collagenase synthesis in keloid, HTS, and normal fibroblasts with downstream actin polymerization, conformational changes, and ultimately apoptosis. Furthermore, it has been suggested that intra-keloid VER injection inhibits IL-6, TGF-β, and vascular endothelial growth factor (VEGF) signal transduction. 25
A scoping review of intralesional corticosteroid injection in both adults and children examined 38 RCTs and concluded that the trials were so heterogeneous, and incomplete reporting within the articles was so pervasive, that adequate data synthesis could not be conducted. 26 Approximately 97.4% of the RCTs used TAC, although dosing, treatment frequency, and outcome measures varied widely.
A network meta-analysis conducted by Yang et al. (2021) demonstrated that combined TAC-BTA and TAC-5-FU injections were superior to single agents alone; however, in those patients for whom the side effects of these agents were intolerable, the use of TAC in combination with silicone gel was advised. 25 Injections of TAC and BTA have been shown to be safe and effective for the treatment of pathologic scars in children; BTA injection was found to not only improve scar erythema and thickness but also improve the associated pruritus and pain. 27 Artzi et al. investigated the use of Tixel, a novel thermomechanical system, for the delivery of TAC-5-FU in children and found it to be both efficacious and safe with significant reduction in Vancouver Scar Scale (VSS) after eight treatments. 28 Clinical trials comparing VER with TAC for the treatment of keloids and HTS have demonstrated adequate results and fewer adverse events with VER injection; however, TAC has significantly superior results in terms of pliability, height, and vascularity as well as lower recurrence after excision. 29,30
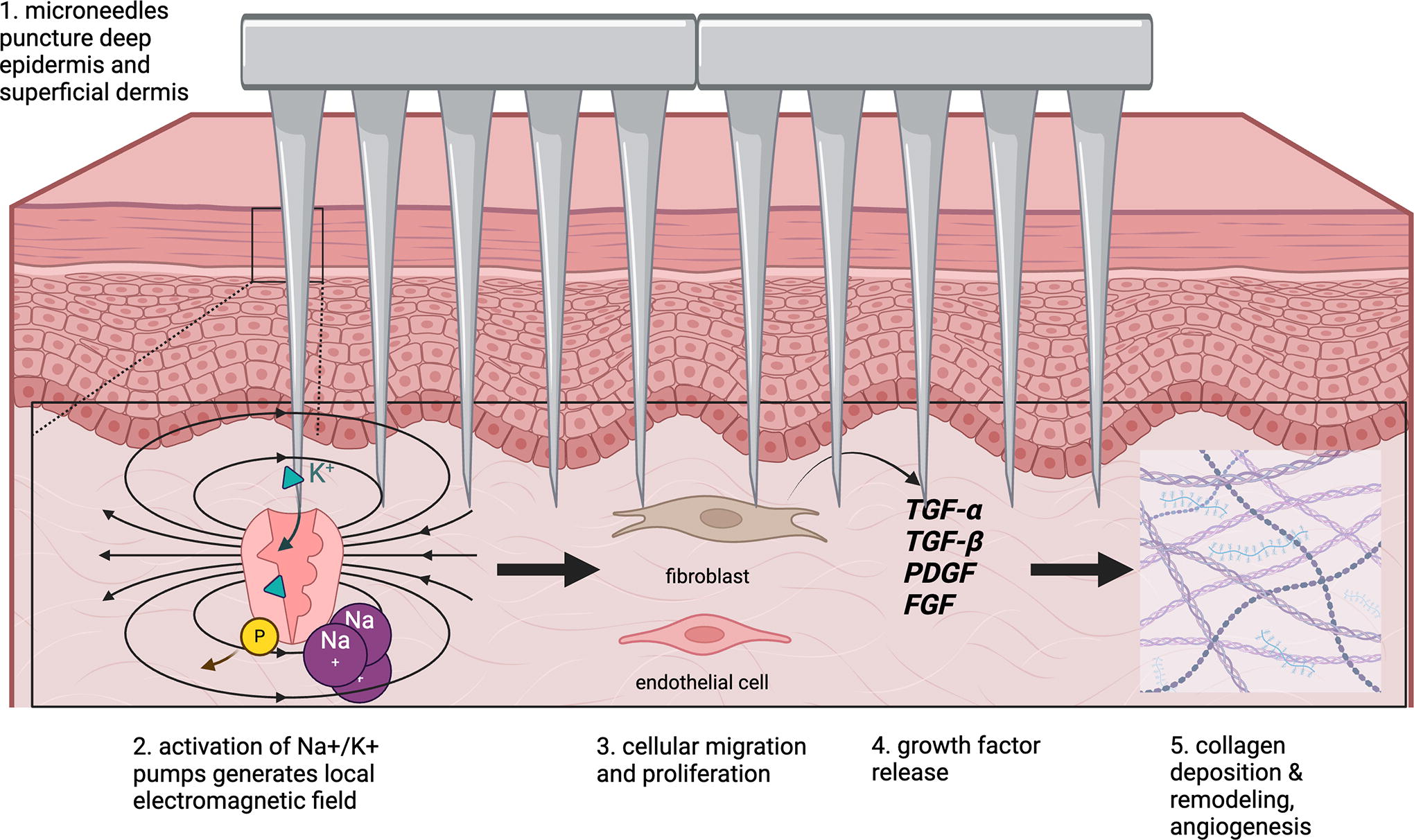
Microneedling (MN) has shown potential as a useful adjunct to pharmacologic therapies in the treatment of scars via mechanical effects on fibroblasts and ECM remodeling. Specifically, for the treatment of scars, microneedles puncture through the stratum corneum into the deep epidermis and superficial dermis to activate endogenous Na+/K+ pumps, thereby generating a local electromagnetic field that stimulates epithelial and endothelial cell migration and growth factor release, resulting in neovascularization and collagen remodeling (Fig. 6). 31,32 A systemic review by Juhasz et al. (2020), which examined 58 studies regarding MN for the treatment of scars, found that the procedure produced satisfactory clinical improvement in many scar types, including HTS and keloids, and was reportedly better tolerated than laser resurfacing with minimal adverse effects, especially in Fitzpatrick skin types IV-VI; MN can also be used in combination with other therapies to administer intralesional medications such as TAC and to enhance penetration of topical agents. 33
Autologous cell therapy
Intralesional injection of autologous stem cells, adipose cells, skin suspensions, and platelet-rich plasma (PRP), as well as percutaneous collagen induction (PCI), have recently emerged as promising treatments for hypertrophic scarring and keloids.
Autologous fat transfer (AFT), also known as lipofilling, was first described as a treatment for scarring in 1983. The utility of AFT in scarring lies in its volumizing properties as well as its rich milieu of growth factors and cells, which importantly includes mesenchymal stem cells. 34 Among their many properties, adipose-derived stem cells (ADSCs) have been shown to downregulate TGF-β1 and SMAD activation. This cross talk is bidirectional, however, and TGF-β1 exerts its own pro-fibrotic effects on ADSCs thereby promoting differentiation into a myofibroblast-like phenotype. The role of ADSCs in wound healing is further complicated by secreted growth factors, such as fibroblast growth factor 2 and hepatocyte growth factor, which have powerful paracrine and autocrine effects that promote healing and reduce scar formation. 35 In vitro, coculturing human fibroblasts with microfat promoted cell proliferation and migration and was associated with lower expression of fibrosis-related genes. Yu et al. transplanted human HTS fibroblasts to nude mice, injected microfat into the scars, and harvested them 4 weeks later. 36 Scars treated with microfat showed more normative collagen fiber organization compared with control scars; microfat-treated scars also showed less fibrosis-related gene expression. Clinically, AFT has shown mixed results in the treatment of pathologic scars. A multitude of case series demonstrating both treatment successes and failures have been reported in the literature; however, the small sample sizes and lack of control groups limit the conclusions that can be drawn regarding the practical utility of AFT in scarring. 35
Autologous skin cell suspensions (ASCS) entail the application of an epithelial cell suspension over a wide area with the goal of prompting early re-epithelialization and are under investigation as a potential therapeutic option for the treatment of scars. A systematic review of five trials (n = 347) conducted by Bairagi et al. found a significant decrease in time to re-epithelialization of pediatric partial thickness burns and adult split-thickness skin graft donor sites treated with ASCS. 37
PRP injection and PCI have also been reported in the literature as adjunctive therapies for pediatric scarring, however, definite conclusions cannot yet be drawn in the absence of higher-powered studies with adequate control groups and randomization. 37,38
Laser therapy
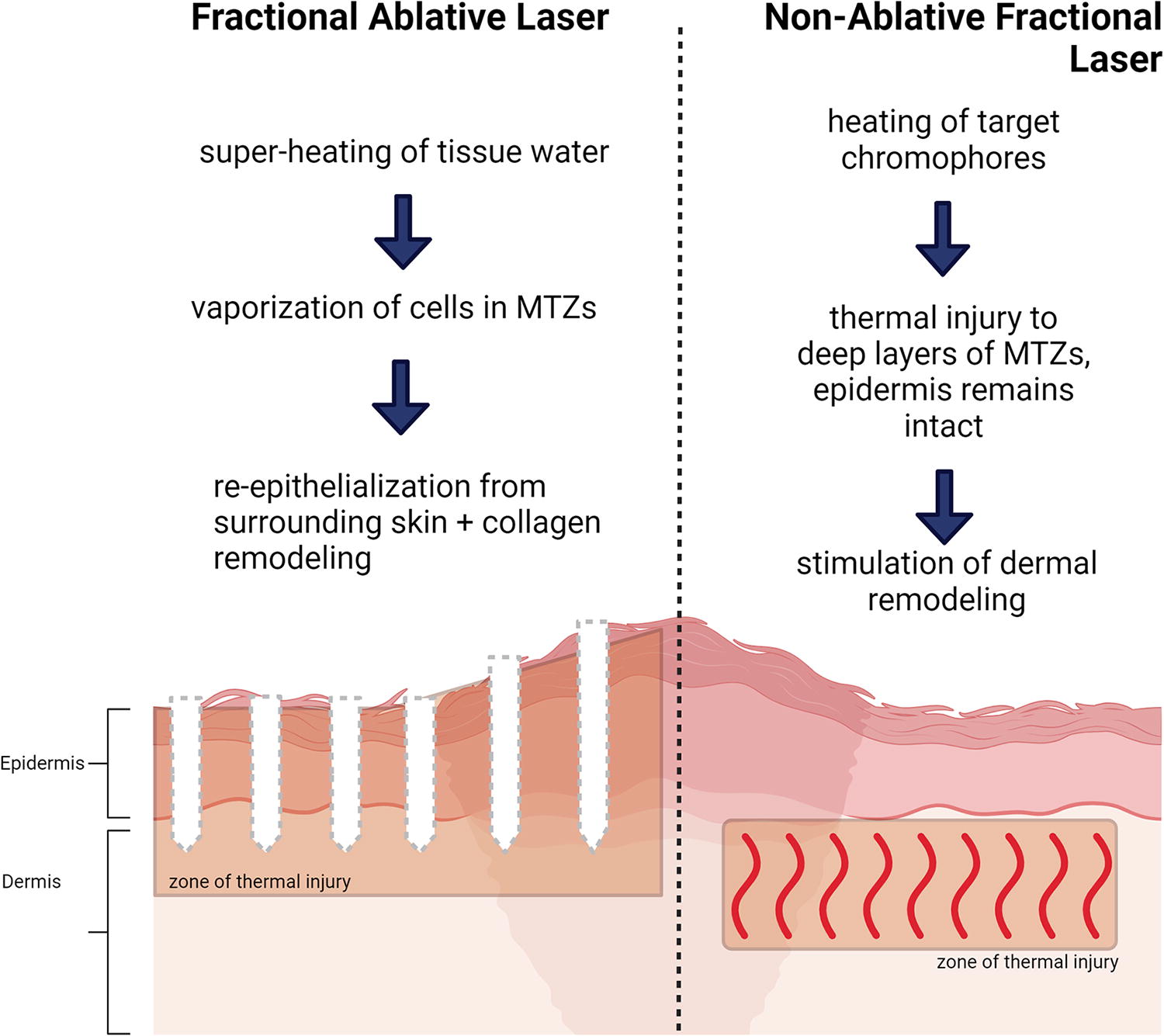
Over the past decade, a variety of laser therapies have shown promising results in the reduction of scar tissue volume, possibly by promoting collagen reorganization within HTS. Fractional lasers were first described in 2004 and have since revolutionized the field of skin resurfacing. The basic underlying principle of fractional lasers is the use of microscopic columns of thermal damage, termed microscopic thermal zones (MTZs), to jumpstart tissue regeneration and remodeling of the interval regions of normal skin. 39 Fractional lasers used for scar treatment are classified as ablative or non-ablative based upon impact on the stratum corneum, which is dependent on wavelength. Ablative fractional lasers, namely fractional carbon dioxide (CO2, 10,600 nm) and erbium-doped yttrium aluminum garnet (Er-YAG, 2,940 nm), have longer wavelengths that are absorbed by tissue water, causing complete vaporization of cells in the MTZs while leaving the surrounding area intact to provide a scaffold for tissue regeneration and remodeling and promote migration of epithelial cells into the ablated MTZs. 40 Ablative lasers have demonstrated high efficacy but have a significant side effect profile including post-procedure pain, longer recovery, scarring, hypopigmentation, and increased risk of infection, which may limit their practical utility. Non-ablative lasers were developed to mitigate these complications by using shorter wavelengths that do not disrupt the stratum corneum. Examples include the 585 nm and 595 nm pulsed-dye laser (PDL), the pulsed potassium titanyl phosphate (532 nm), and the neodymium yttrium aluminum garnet (1,064 nm) lasers. An advantage of these non-ablative lasers is that they have specific targets, such as oxyhemoglobin, with narrow absorbance ranges, thereby stimulating dermal remodeling via controlled heating of deep tissue with reduced damage to surrounding healthy tissue (Fig. 7). 39,40
A 2023 systematic review by Worley et al. sought to compare the effectiveness of intralesional injection and laser therapy for the treatment of pathologic scars; the analysis of 25 clinical trials found that intralesional injection was significantly more efficacious than topical or laser therapy. Among the laser options, ablative laser and PDL were most effective, and response to treatment correlated with Fitzpatrick skin type (specifically, laser treatment was most efficacious in Fitzpatrick types I–III and superior to compression therapy in this group). A 2022 Cochrane review of 15 RCTs including both children and adults (n = 604) found low-certainty evidence demonstrating scar improvement following 585 nm PDL therapy but overall found that the available evidence was too heterogenous, and often too conflicting, to draw any conclusions regarding the efficacy of laser treatments over other treatments or no treatment for keloids and HTS. 41
There are, however, a few nonrandomized studies that offer low-certainty evidence in support of laser treatments for pathologic scarring. A retrospective study of 17 children with HTS treated using CO2 laser alone or in combination with PDL found improvement in scar pain and itching from baseline; however, no control group was included for comparison. 42 Similarly, in a study of 30 children receiving fractional ablative CO2 laser surgery to treat hand scarring, hand function and scar appearance significantly improved compared with the patients’ untreated baseline. 43 A retrospective study of 60 patients with burn and scald scars found that a regimen including both PDL and fractional CO2 laser treatments was associated with significant improvement from baseline in measures of pain, appearance (including surface area), and texture. 44 A similar combination treatment regimen in 25 pediatric patients identified similar improvements in appearance and function; at baseline, these patients also had higher plasma concentrations of MMP-2, TIMP-1, and α-1 type I collagen compared with age-matched controls, and it was found that combined laser treatment was correlated with a significant decrease in concentrations of MMP-2 and TIMP-1. 45 A single-institution study that included 77 children with burn scars also found that CO2 laser, alone or in combination with PDL, improved elasticity from baseline in a dose-dependent manner. 46
A 2018 split-scar study assessed the efficacy of low-energy CO2 laser treatment in children under the age of 12 with hypertrophic scarring (n = 23) and demonstrated significant improvements in pain, itching, and scar appearance following three treatments at 1-month intervals. 47 Donnellan et al. assessed the feasibility of treating chronically hypertrophic burn scars with a newer-generation ablative CO2 laser in an outpatient setting (n = 17 patients); all the patients reported that treatment pain was “tolerable” or “very tolerable,” and all reported improvement in pain, pruritis, and/or range of motion at the scar site. 48 A split-scar study using ablative helium–neon laser treatment in 15 children aged 2 to 10 also reported significant improvement following treatment. 49
Ablative lasers have shown some success in improving pathologic characteristics of HTS and, to a lesser degree, keloids. Importantly, one of the adverse effects of cutaneous laser therapy is the induction of scar formation, which may confound treatment outcomes. 40 The heterogeneity in treatment regimens and baseline scar characteristics reported in the literature poses serious limitations as far as drawing any overall conclusions about treatment efficacy. Randomized prospective studies with rigorous standardization and objective assessment of outcomes are needed to further validate the utility of lasers in the treatment of pathologic scarring.
Carboxytherapy
Carboxytherapy involves subcutaneous or intradermal introduction of CO2, which combines with water in tissues to form carbonic acid. The decrease in pH causes vasodilation and increased capillary permeability, which allow for increased delivery of oxygen and growth factors, thus promoting local angiogenesis, re-epithelialization, and collagen remodeling. 50 There is a paucity of clinical trials testing the efficacy of carboxytherapy for the treatment of pathologic scars; however, Delgado-Miguel et al. have recently demonstrated significant improvement in VSS score 6 weeks after two carboxytherapy sessions in 16 pediatric patients with either atrophic or HTS. 51
Radiation
A critical review published in 2022 found that external-beam radiation and high-dose rate brachytherapy were the most used modalities for pathologic scar treatment in adults and have demonstrated moderate success in small cohort studies; however, randomized trials are still needed. 52 Although radiation therapy is widely practiced in the treatment of adult keloids, publications regarding the use of radiation treatment for pathologic scars in children were not found in our literature search. A survey of radiation oncologists suggested that radiation therapies are much less accepted in the treatment of pediatric keloids, possibly because of the concern about the risk of secondary malignancies. 53 Survey respondents reported similar keloid treatment strategies for children and adults. In both populations, most treating clinicians used electron-beam radiation and applied three fraction regimens. Similar proportions of oncologists who treated adults and oncologists who treated children reported administering radiation treatments within 24 hours of keloid excision.
Extracorporeal shockwave therapy
Extracorporeal shock wave therapy (ESWT) harnesses transient short-term acoustic pulses to noninvasively enhance wound healing. ESWT is theorized to function via enhanced stem cell recruitment, anti-inflammatory, and antimicrobial effects; however, the exact mechanism of action remains to be determined. 54 In a mouse model, ESWT significantly accelerated wound closure, promoted leukocyte turnover, and enhanced angiogenesis without mechanically damaging tissues. 55 ESWT is well tolerated, has minimal serious adverse effects, and has demonstrated significant improvements in scar characteristics in small cohort studies. 56 A meta-analysis found that, compared with comprehensive rehabilitation alone, the combination of comprehensive rehabilitation with ESWT was associated with greater improvements in scar itching, pain, and appearance, as well as skin elasticity. 57
Translational investigations
A wide variety of translational investigations currently underway for the treatment of pathologic scarring have shown promising results in animal models, but their clinical utility in humans remains to be determined.
Nanogels
Chen et al. used rabbit, rat, and in vitro models to investigate the capacity of hyaluronic acid-modified and verteporfin-loaded polylactic acid nanogels to aid scarless wound healing. 58 These materials were biocompatible and found to enter fibroblasts via endosomal transport. Once inside the cell, the nanogels reduced the expression of Yes-associated protein, which promotes fibrosis and ECM deposition. In a rat model, wounds treated with these nanogels were significantly smaller at day 16 than untreated control wounds; treated wounds also showed a more favorable collagen I/III ratio than untreated wounds. These experiments did not, however, investigate the efficacy of nanogels in wounds that have already closed and scarred (although these materials may prove useful in the prevention of scar formation).
SMAD
The TGF-β/SMAD signaling pathway is a key driver of many features of pathologic scarring and has thus emerged as a promising therapeutic target under rigorous investigation. Indeed, a variety of naturally occurring small molecules, as well as RNA interference and gene therapies targeting this pathway, have shown promise in cell culture and animal models.
As the scientific understanding of the complexities of TGF-β/SMAD signaling continues to grow, more and more attention is being paid to enhancing the existing biologic regulatory mechanisms already in place. Angiotensin-converting enzyme (ACE) is a familiar and essential biochemical enzyme with a variety of functions, in particular, organ fibrosis and scar formation. Both in vivo and in vitro studies have suggested that ACE inhibition may show promise as a safe and effective treatment for pathologic scarring via the downregulation of SMAD2/3 and TGF-β activated kinase 1 pathways. 59 BMP-7 is a member of the TGF-β superfamily, which has been demonstrated to counterbalance the fibrotic effects of TGF-β1 in a variety of organs, including the liver, kidneys, lungs, and heart. Local injection of BMP-7 into thermal injuries of mice has been observed to promote healing and inhibit scarring via attenuation of SMAD signaling and induction of fibroblast apoptosis. 60
Curcumin, a naturally occurring anti-inflammatory compound found in turmeric, has been shown to reduce fibroblast activation and hypertrophic scarring in cell and animal models via suppression of SMAD3 phosphorylation and nuclear translocation. 61 In a similar vein, the flavanol kaempferol is an antioxidant found in tea and broccoli, which has been demonstrated to suppress fibroblast proliferation and excess collagen deposition via competitive inhibition of the TGF-β-RI in vitro and in vivo. 62 The small molecule galangin (3,5,7-trihydroxyflavone) is yet another naturally occurring flavonoid extracted from a plant root, which has been found to have numerous biologically active roles, including potent anticancer and anti-inflammatory properties. Galangin has been found to selectively target a particular kinase on the TGF-β-RI, resulting in dose-dependent downregulation of SMAD2/3 phosphorylation and its target effects in cultured human skin cells and mouse models. 63 Loureirin B is a compound extracted from the Dracaena cochinchinensis tree, which is commonly used in traditional Chinese medicine for the prevention and treatment of pathologic scarring. Further investigation in cultured human skin fibroblasts, as well as rabbit ear scar models, demonstrated that loureirin B suppresses fibroblast proliferation and promotes ECM degradation secondary to increased expression of MMP-1, MMP-3, MMP-9, and MMP-13 via disruption of SMAD2/3 phosphorylation. 64
RNA interference
Numerous genetic and cellular techniques currently under investigation have shown efficacy in the prevention and treatment of pathologic scarring, however, the safety and feasibility of translating these to the bedside remain to be determined.
MicroRNA-29 and microRNA-182-5p have potent anti-fibrotic activity in many organs, including lung, liver, and skin, and have been shown to mitigate inflammation and regulate collagen deposition in cultured fibroblasts and animal scar models. Human incisional skin wounds treated with microRNA-29 demonstrate a significant decrease in collagen deposition compared with placebo-treated incisions and a decrease in fibroplasia, which was not statistically significant in this cohort. 65,66
Cytoplasmic polyadenylation element binding protein (CPEB) and connective tissue growth factor (CTGF) demonstrate pro-fibrotic properties via augmentation of TGF-β1/-β2 and SMAD signaling. Small interfering RNA (siRNA)-mediated knockdown of CPEB 1 or 4 reduced TGF-β and SMAD signaling, as well as gene expression of fibrotic markers (α-SMA, collagen I, and fibronectin) in cultured human THP-1 macrophages (a human leukemia monocytic cell line) and dermal fibroblasts. 67 siRNA inhibition of CTGF has been demonstrated to reduce HTS formation and contracture in animal wound models via a reduction in myofibroblast cell populations and collagen production. 68,69
Knockdown of circular RNA HECTD1, a circular RNA that is more plentifully expressed in HTS than in normal skin, reduces cell migration, proliferation, and invasion, as well as the expression of TGF
There are a multitude of investigational molecules for the treatment of pathologic scarring that target each step of the wound healing process and have shown promise in preclinical studies. Further investigation is needed to assess the translational capabilities of these exciting agents.
CONCLUSIONS AND FUTURE DIRECTIONS
Scar formation is an essential component of the mammalian tissue repair system, yet pathologic scarring is a common clinical challenge that can have significant deleterious effects on normal function and psychosocial well-being. Although our understanding of the molecular mechanisms underlying aberrant scarring (i.e., TGF-β/SMAD signaling pathways) has grown exponentially, the treatment options for HTS and keloids remain limited in scope and unstandardized in practice. The broad variety of therapeutic modalities discussed in this review article speaks to the challenge of safely and efficaciously translating novel biochemical insights to the bedside. Owing to the relatively rare and extremely heterogenous nature of pathologic scarring, it is difficult to predict and standardize treatment protocols. Although well-powered randomized controlled trials to study the individual and synergistic effects of these therapies would be ideal before any definitive conclusions or evidence-based treatment recommendations can be made, because of the heterogeneity of these patient populations, well-conducted cohort studies may be the next best option.
TAKE-HOME MESSAGES
Pathologic scarring is driven by abnormal fibroblast function and matrix remodeling secondary to aberrations in TGF-ß/SMAD signal transduction pathways. Intralesional corticosteroid injection with TAC has been the gold standard for over a decade; however, recent studies have demonstrated improved treatment efficacy when TAC is combined with BTX or 5-FU. Ablative (fractional CO2 and Er-YAG) and non-ablative PDL therapy, MN, carboxytherapy, and radiation have shown some efficacy in improving scar appearance and elasticity in nonrandomized studies. Small molecules and RNA interference targeting key components of the TGF-ß/SMAD axis have shown promise in reducing scar formation in vitro and in vivo animal models; robust investigations are ongoing to translate these findings into practical clinical applications. Further studies with well-standardized treatment regimens and outcome measures are needed to formulate evidence-based recommendations.
SUMMARY
Wound healing is an intricate process that occurs for months to years after injury and is dependent on the balancing of complex interactions between multiple cell types. Pathologic scarring, which occurs secondary to imbalances in these cellular mechanisms, affects millions of people annually and can result in social and psychologic harm as well as physical disability. Children are uniquely susceptible to pathologic scar formation because of their fragile skin and immature immune systems, as well as their vulnerability to traumatic injuries.
Here, we discuss the contemporary literature regarding the molecular mechanisms of pathologic scarring and review promising treatment strategies including topical and injectable agents, MN, laser therapies, radiation, and ESWT. These treatments have demonstrated some success in small studies; however, randomized trials are still needed to draw conclusions or comparisons. Translational investigations are also underway into several potential new treatments that may become available in the future, such as treatment with nanogels, gene therapies, and certain small molecules.
Footnotes
AUTHORS’ CONTRIBUTIONS
S.G.H.: Conceptualization, methodology, investigation, visualization, writing—original draft, writing—reviewing and editing. A.S.: Investigation, writing—original draft, writing—reviewing and editing. O.O.O.: Conceptualization, methodology, supervision, writing—reviewing and editing.
AUTHOR DISCLOSURE AND GHOSTWRITING
The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article. This article was written in its entirety by the listed authors—no ghostwriting services were used.
FUNDING STATEMENT
No external funding was received for this article.
ABOUT THE AUTHORS