
Abstract
Significance:
As an essential procedure, wound care comes with acute pain, which is short but high in intensity, causing patients to fear and affecting subsequent treatment. Nitrous oxide (N2O) is used to relieve pain related to wound care; however, evidence regarding its application is conflicting. Thus, this systematic review and meta-analysis was performed to evaluate the efficacy of N2O in wound care–related pain.
Recent Advances:
Randomized controlled trials that investigated the effect of N2O in adults undergoing wound care were systematically searched from PubMed, Embase, the Cochrane Library, Web of Science, Scopus, and ClinicalTrials.gov up to February 2023. The primary outcome was the pain score. Secondary outcomes included patients’ satisfaction and side effects.
Critical Issues:
Through screening the 265 identified articles, seven and six studies were finally included in the systematic review and meta-analysis, respectively. Pooled analysis suggested that there was no significant difference in reducing wound care–related pain between the N2O group and the control group (mean difference [MD], −0.02, 95% confidence interval [CI], −1.46, 1.42; p = 0.98, I 2 = 96%). Subgroup analyses indicated that there was a significant difference in favor of N2O for burns, not for ulcers, and N2O was superior to oxygen and similar to topical or intravenous anesthesia. There was no significant difference in patients’ satisfaction or the incidence of side effects between groups.
Future Directions:
This review suggests that N2O might be effective for pain management in patients undergoing wound care. Caution must be taken when interpreting these results due to the high risk of biased methods in the included studies.

SCOPE AND SIGNIFICANCE
Wound care is an essential part of clinical practice, and the healing of wounds directly affects the quality of life. However, wound care often comes with acute pain, which is short but high in intensity, causing patients to fear and affecting subsequent treatment. Several studies investigated the effect of nitrous oxide (N2O) in conscious patients undergoing wound care and no consistent conclusion was made. Patients started inhaling N2O 2–3 min before the onset of wound care and did not stop until the procedure were completed. Therefore, this review provides a thorough appraisal of the effectiveness of N2O in patients undergoing wound care.
TRANSLATIONAL RELEVANCE
The relief of wound care–related pain is of the utmost importance, given the high incidence of acute pain in hospitals. Opioids remain the mainstay of treatment for moderate and severe pain, with side effects of respiratory depression, constipation, and itching. N2O as an inhalation analgesic and sedative anesthetic has the characteristics of noninvasive and rapid clinical effect, and it might also be combined with other analgesics, which could be largely superior to the currently used single-method analgesia. In the future, medical workers should carefully choose the safest and the most effective analgesic methods based on patient needs and wound conditions in wound care.
CLINICAL RELEVANCE
This systematic review and meta-analysis suggested that N2O might reduce wound care–related pain, especially in patients with burns. It can be used as a safe and readily available noninvasive substitute when intravenous or topical anesthesia is not suitable or contraindicated in wound care. More large-scale randomized controlled trials are needed to evaluate the efficacy of N2O in patients undergoing wound care in the future.
INTRODUCTION
Procedural pain is caused by wound dressing change and debridement. 1 Debridement refers to the removal of nonviable material, foreign bodies, and poorly healing tissue from the wound. It remains an important adjunct to good wound care and is highly valued by surgeons for the removal of tissue with the highest bacterial count, reliable cultures, and identification of osteomyelitis. 2 However, the primary risk of debridement is pain, which is acute and lasts for a short time, and the pain intensity is particularly high, causing patients to fear wound care and subsequent treatment. Studies have pointed out that several routine procedures are the main sources of pain.
A survey indicated that in a French university hospital, 64% of hospitalized patients reported pain during daily minor procedures. 3 Pain as an unpleasant sensory and emotional experience relates to actual or potential tissue damage and has become the fifth vital sign after respiration, temperature, pulse, and blood pressure. 4 As a strong and lasting source of stress, pain seriously affects patients’ sleep and appetite, increases the high metabolism caused by trauma, causes anxiety, anger, depression, and other adverse psychological reactions, and leads to physical and psychological fatigue, which harms wound treatment and healing. 5,6
The most commonly used analgesic procedures include intravenous anesthesia, local anesthesia, and oral analgesics. However, the insufficient analgesic efficacy and obvious side effects of drugs with long postanesthetic recovery may delay healing and reduce patients’ compliance. 7 In addition, most drugs used in general anesthesia often cause respiration and circulation repression in patients. Dependence and tolerance to anesthetic drugs may also occur. 8 N2O appears to be an available method in minor procedures owing to its simple operation and mild side effects. As an inhalation analgesic and sedative anesthetic, it has the characteristics of noninvasive, rapid, and good clinical effect, and it is widely used internationally for acute pain. 9 –11
In recent years, several studies investigated the effect of N2O in conscious patients undergoing wound care such as dressing change and debridement. Patients started inhaling N2O 2–3 min before the onset of wound care and the N2O inhalation did not stop until the surgical procedure was completed. At present no consistent conclusion on the efficacy of N2O in wound care–related pain was made. When trials reach divergent conclusions, a systematic quantitative review of the original clinical trials is a helpful method of assessing the evidence. Therefore, we performed a systematic review and meta-analysis to compare the efficacy of N2O with other analgesic methods in patients undergoing wound care.
METHODS
This systematic review and meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 12 (Supplementary material Table S1 and Supplementary Data S1). The protocol was prospectively registered in the PROSPERO register of systematic reviews (registration number CRD 42023425552), available at https://www.crd.york.ac.uk/PROSPERO/. We made no significant amendments to the original protocol. No formal ethical approval was required.
Search strategy
To define the most appropriate keywords and create an exhaustive search strategy, the search strategy was piloted and refined based on updated Cochrane guidelines. 13 We systematically searched PubMed, Embase, the Cochrane Library, Web of Science, Scopus, and the ClinicalTrials.gov up to February 2023 using the MeSH terms and appropriate corresponding keywords: “Nitrous Oxide,” “Laughing Gas,” “Nitrogen Protoxide,” “Dressing Change,” “Debridement,” and “Wound Dressing.” Then, the references of included studies were screened manually to identify additional references. PROSPERO register of systematic reviews was also searched for ongoing or recently completed reviews. No language or temporal limit was applied. The literature search, study inclusion and exclusion criteria, and data extraction were performed by two authors independently.
Eligibility criteria
Inclusion criteria followed the participants, interventions, comparators, outcomes, and study design (PICOS) framework. 14 Participants: Studies had to be conducted on adults and were focused on wound care (i.e., dressing change and debridement) at whatever wound site (i.e., trunk and limbs). Intervention: N2O inhalation aimed at reducing pain induced by wound care. Comparators: Placebo or other analgesic methods. Outcomes: Included trials had to examine outcomes of patient-reported pain intensity, and secondary outcomes at least following one of the endpoints: patient satisfaction, side effects, and duration of the procedure. Study Design: Interventional studies were included (i.e., clinical trials, controlled clinical trials, and randomized controlled trials). Proceedings, research protocols, and gray literature were excluded.
Meta-analysis was based on trials identified in the systematic review. A separate meta-analysis was performed for each analgesic intervention as long as it involved at least two included studies. No meta-analysis will be conducted if there were fewer than two included studies on the intervention.
Screening and data extraction
Two researchers independently screened the title and abstract of identified studies using Endnote X9 (Thomson Scientific, USA), removed duplicates, and reviewed the full text of the potentially relevant studies. Data on study characteristics (first author, year of publication, country, interventions, controls, adjuvant analgesics, and main outcomes), sample characteristics (number, gender, age, and wound types), narrative summary of findings, and quantitative results were independently extracted by two researchers and entered into an excel data collection form. We would contact the original author by e-mail if data needed clarification or were not presented in the article. Any disagreement or uncertainty regarding eligibility and data extraction was resolved by a third assessor.
Risk of bias and certainty of evidence
Risk of bias was assessed by two independent researchers using the revised Cochrane Collaboration Risk of Bias Tool to examine potential bias from the randomization process, allocation concealment, performance and detection bias, missing outcome data, measurement of the outcome, and selection of reported results for all randomized trials. 15 The certainty of the evidence of meta-analysis comparisons was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach. The GRADE approach considers study limitations, indirectness, inconsistency, imprecision, and publication bias to rate the certainty of the evidence. 16
Primary and secondary outcomes
Patients’ perception of wound care pain was the primary outcome, defined as pain during wound care or the overall experience of wound care–related pain.
When no point of time was specified, we classified it as pain during the procedure. When pain was assessed at several time points, we only extracted pain score immediately after the procedure. The primary outcome was expressed using the mean on a visual analog scale (VAS) or numeral rating scale (NRS) of 0–10 with standard deviation (SD). Conversion was applied when necessary (e.g., when expressing the pain as mean on 0–100 or median). All other wound care–related outcomes reported across studies were marked as secondary outcomes. The definition for each outcome above was the same as that used in each included study.
Data synthesis
All analyses were completed in Review Manager software (version 5.3; Nordic Cochrane Center, Cochrane Collaboration). The differences were shown as the risk ratio (RR) with 95% confidence interval (CI) of the dichotomous outcome and the weighted mean difference (MD) with 95% CI of the continuous outcome. Where possible, heterogeneity was assessed by reporting 95% prediction intervals and the I 2 statistic. I 2 values of 0–49.9%, 50–74.9%, and >75% were, respectively, considered to have low, moderate, and high heterogeneity. 17 Contrary to the estimated pooled mean effect size, the prediction interval represents the dispersion of the effects. Statistical significance was considered p < 0.05. When there were >10 studies included in the meta-analysis, meta-regression was conducted. Publication bias was appraised by visually examining a funnel plot when ≥10 trials were available. 18
Sensitivity analysis
Sensitivity analysis involved exploring the role of outliers and influential studies, conducting by omitting one study at a time, and investigating the impact of individual studies on the overall pooled estimate.
Subgroup analysis
The following subgroup analyses were performed to explore heterogeneity in the meta-analysis estimates. These included different wound types (burns or ulcers), different comparators (placebo, intravenous anesthesia, or topical anesthesia), and different time points (during or after procedure).
RESULTS
Overall, the search strategy rendered 265 articles; 184 studies were screened at the title and abstract phase and 11 full texts were assessed. Four studies did not meet the inclusion criteria and were excluded; thus, seven studies 19 –25 were included in the systematic review. One 24 article included in the systematic review was not eligible for inclusion in the meta-analysis, as N2O was used both in the intervention group and in the control group. Therefore, six studies 19 –23,25 were finally included in the meta-analytic process (Fig. 1).

Flow chart of study selection.
Study characteristics
The included studies were published between 2008 and 2020, with sample sizes ranging from 30 to 240; 330 patients were included in the intervention arm and 211 patients were in the control arm. The included trials were conducted in five countries: two in France, 19,20 two in China, 21,24 one in Brazil, 22 one in Switzerland, 23 and one in Iran. 25 All participants of studies contained males and females. All the included studies were randomized controlled trials, of which four 20,21,24,25 were parallel and three 19,22,23 were crossover design. Three trials 19,20,23 were open label, two 22,24 were single blinded, and two 21,25 were double blinded.
Two trials included multiple groups, of which one trial 19 included N2O group, morphine group, and morphine plus N2O group, and the other trial 25 included N2O group, gabapentin group, ketamine group, and dexmedetomidine group. Two trials 21,22 compared N2O with oxygen, and four trials compared N2O with other analgesic methods (local anesthesia 20,23 and intravenous anesthesia 19,25 ). The study setting was in the clinic in one trial 23 and in the burn center in one trial, 24 and the remaining 19 –22,25 were at the hospital. The wound types included burns 21,22,24,25 and ulcers. 19,20,23 The characteristics and outcomes of included studies are presented in Table 1.
Characteristics of included randomized controlled trials
N group, nitrous oxide group; C group, control group.
Risk of bias and quality of evidence
One trial was classified as having low risk of bias, four provided some concerns, and two were classified as high risk of bias. Bias due to blinding of participants and personnel, blinding of outcome assessment, and allocation concealment were of the greatest concern. The risk of bias and details for judgment of bias are shown in Figure 2 and Supplementary material Table S2, respectively. The quality of evidence was low for pain scores and moderate for other outcomes, as presented in Table 2. Publication bias was not conducted due to the limited number of included studies.

Risk of bias assessment.
Summary of GRADE evidence profile
GRADE, quality of evidence grade; CI, confidence interval; RCT, randomized controlled trial; RR, risk ratio; SMD, standardized mean difference.
Data reported as downgraded because of some concerns of bias.
Substantial heterogeneity (I 2 = 97%) was found.
Data reported as downgraded because of wide CI or inadequate studies.
Primary outcome
Seven studies in the systematic review explored patients’ perception of wound care–related pain, of which two 19,20 assessed pain immediately after the procedure, and five 21 –25 explored overall pain experience. Two studies 24,25 assessed pain at several time points. Different tools were used to assess wound care–related pain, including the VAS 19 –23,25 and NRS. 24 Three trials 21,22,25 explored the wounding dressing, two 20,23 were debridement, and two 19,24 referred to all the wound care–related pain. VAS results were not analyzed in one study, 19 as incomplete data were available. Ultimately, the pain score was available in five studies. 20 –23,25
Pooled analysis suggested that there was no significant difference in reducing wound care–related pain between the N2O group and the control group (MD, −0.02; 95% CI, −1.46, 1.42; p = 0.98; Fig. 3), with significant heterogeneity (I 2 = 96%). Sensitivity analysis was conducted by omitting one study in each turn, and heterogeneity was significantly changed when Claeys et al.’s study 20 was excluded (p = 0.002; I 2 = 0%). Subgroup analyses were performed to examine the influence of different wound types, control groups, and time points on the pain score.
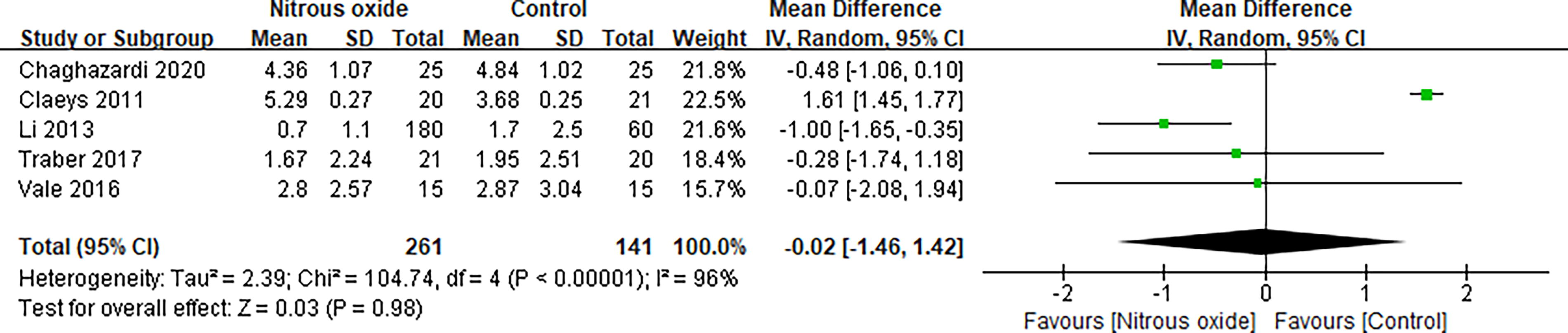
Forest plot for the pain score.
There was a significant difference in favor of N2O for burns 21,22,25 (MD, −0.68; 95% CI, −1.10, −0.26; p = 0.002, I 2 = 0%), whereas there was no significant difference for ulcers 20,23 (MD, 0.81; 95% CI, −1.02, 2.64; p = 0.39; I 2 = 84%; Fig. 4). Pooled analysis showed that in reducing wound care–related pain, the effect of N2O was superior to oxygen 21,22 (MD, −0.91; 95% CI, −1.53, −0.29; p = 0.004; I 2 = 0%), and was similar to topical anesthesia 20,23 (MD, 0.81; 95% CI, –1.02, 2.64; p = 0.39; I 2 = 84%) and intravenous anesthesia 25 (MD, –0.48; 95% CI, −1.06, 0.10; Fig. 5). In addition, the pain score during the procedure in the N2O group 21 –23,25 (MD, −1.62; 95% CI, −6.80, 3.57; p = 0.54; I 2 = 100%) was not significantly different from that in the control group, while the pain score post procedure in the N2O group was significantly lower than that in the control group 21 –23,25 (MD, −0.65; 95% CI, −1.06, −0.24; p = 0.002, I 2 = 0%; Fig. 6).
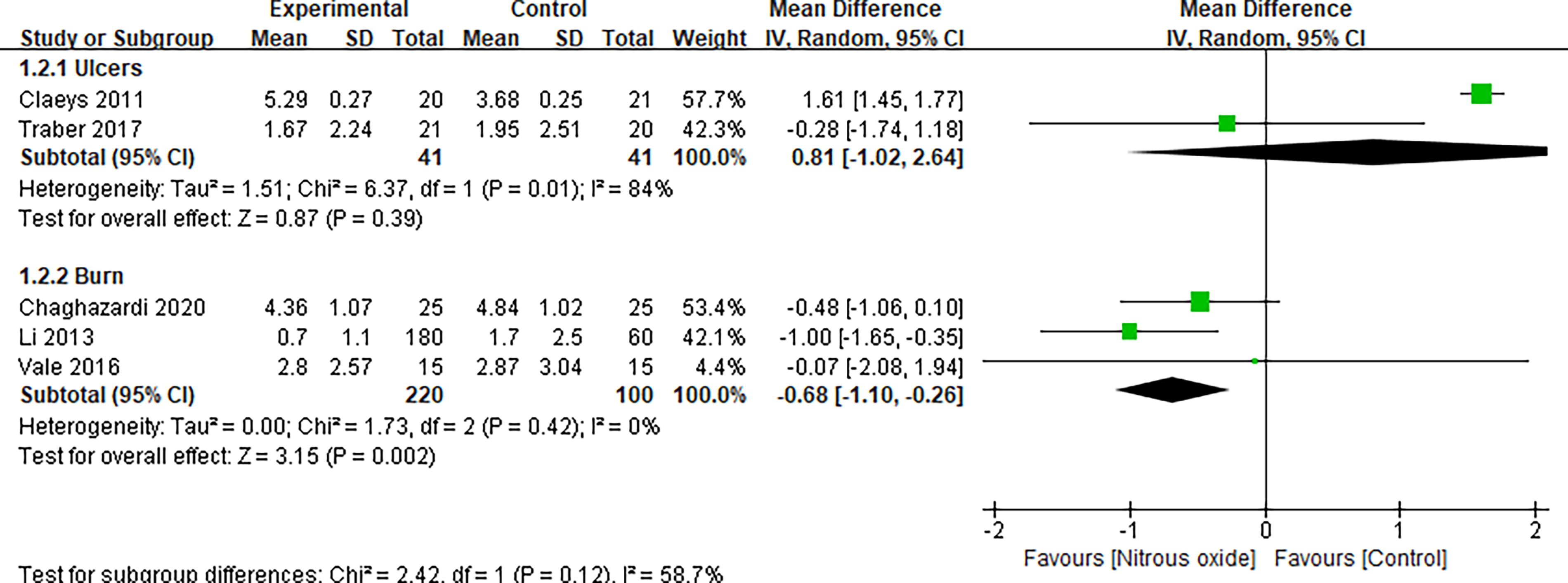
Forest plot of subgroup analysis for pain score by different wound types.

Forest plot of subgroup analysis for pain score by different controls.
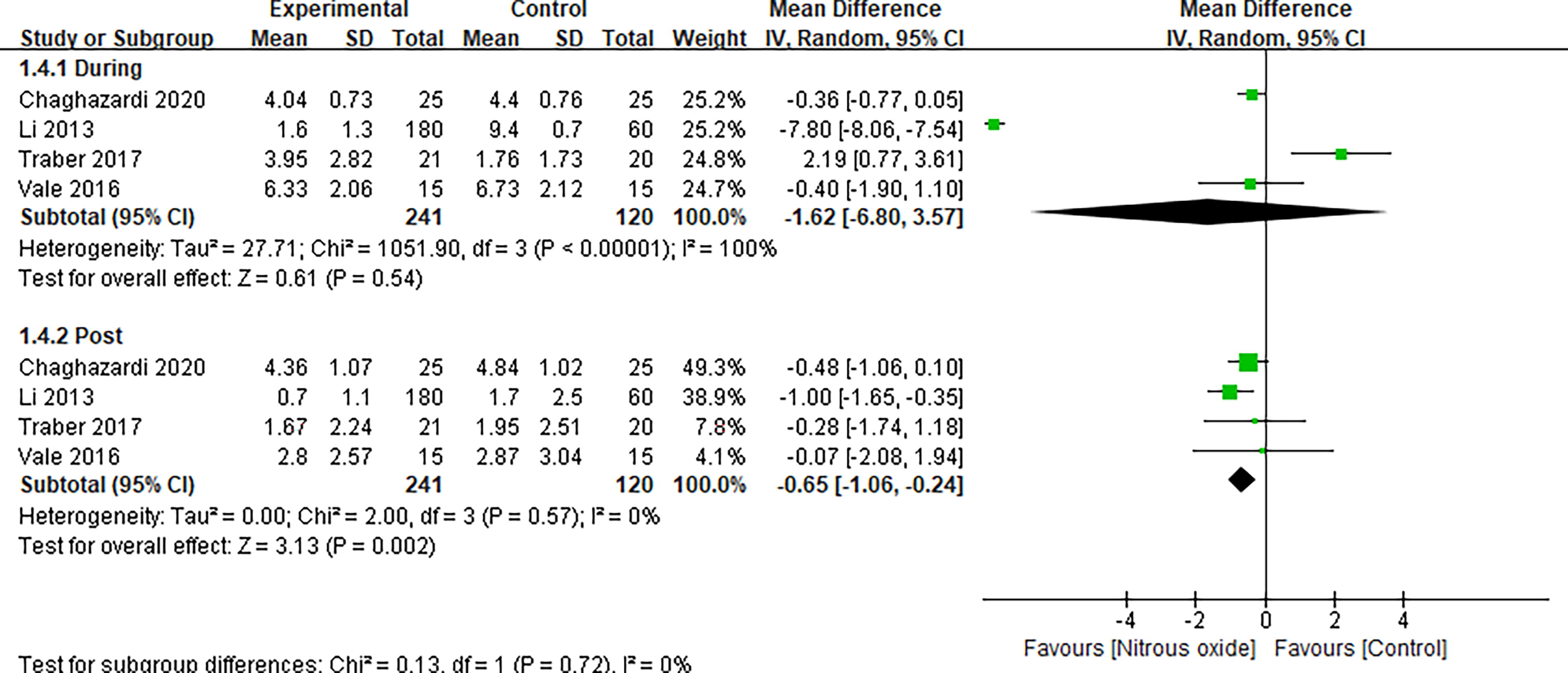
Forest plot of subgroup analysis for pain score by different time points.
Secondary outcomes
Satisfaction
The degree of patients’ satisfaction was reported in three trials 20,22,23 with 100 patients. There was no significant difference between the N2O group and the control group (RR, 0.98; 95% CI, 0.78, 1.23; p = 0.87; I 2 = 0%; Supplementary material Fig. S1).
Side effects
Five studies 19 –22,25 reported the overall incidence of side effects, and pooled analysis showed that N2O did not increase the incidence of side effects compared with other analgesic methods (RR, 1.31; 95% CI, 0.76, 2.26; p = 0.34; I 2 = 0%; Supplementary material Fig. S2). Data for nausea and vomiting were available from four trials. 19,21,22,25 Pooled analysis showed no significant difference between groups (RR, 0.95; 95% CI, 0.40, 2.22; p = 0.90; I 2 = 0%, Supplementary material Fig. S3).
Duration of the procedure
The mean duration of the procedure was available in three trials 19,22,23 in the systematic review. The mean time was significantly shorter for N2O versus morphine 19 (16.7 min versus 20 min, P < 0.001), or N2O versus fentanyl 22 (38.8 min versus 43.33 min), and was similar when N2O versus lidocaine/prilocaine cream 23 (29.48 min versus 28.43 min, p = 0.82).
DISCUSSION
To the best of our knowledge, this was the first systematic review and meta-analysis aimed to investigate the efficacy of N2O in adults undergoing wound care–related pain. In addition to placebo (oxygen), our review identified four analgesic techniques in the control group, including fentanyl, morphine, ketamine, and lidocaine/prilocaine cream. The evidence accumulated in this study suggested that N2O could provide better analgesia than oxygen and similar analgesia to other analgesic methods and relieve pain with shorter duration of procedure and mild side effects during the process of wound care.
Wound care is the process of removing dressings, debridement, medication, and bandage for wounds. It is the foundation of wound healing, widely used in burns, ulcers, trauma, and surgical wounds. Efforts are directed at techniques that facilitate wound healing, prevent infection, promote comfort, and meanwhile, maintain optimal function and minimize deformities. 26 However, the whole treatment process is often not feasible due to the limited potency of the analgesic method, especially in patients when extensive or deep wound debridement is intended. It is also known that insufficient pain control is a significant predictor of impaired quality of life. 27,28 Therefore, the availability of a potent analgesic method is critical to the overall success of painful wound care not only because of patient comfort and optimal treatment but also because painful process of debridement and dressing change would jeopardize patients’ adherence to further therapy.
Our findings showed that N2O was not significantly different from other analgesic methods in reducing wound care–related pain, suggesting that N2O might provide adequate analgesia for adults. Subgroup analyses showed that compared with the control group, N2O had a better analgesic effect on burns, 21,22,25 and a significantly lower immediate postprocedure pain score. 21 –23,25 A possible explanation could be that, in addition to pain relief, N2O has sedative and antianxiety properties, so it may increase the patient’s pain threshold, resulting in lower immediate postprocedure pain score. 21 In pooled analysis of two trials for ulcers, the effect of N2O is similar to 5% lidocaine/prilocaine cream during the procedure. 20,23
Traber et al. 23 described that a plausible explanation could be that the oil-in-water-based character of lidocaine/prilocaine cream might be able to macerate the wound and thus allow more effective and deeper debridement with a lower level of pain for the patient. On the other hand, Stahl et al. 29 found the vasoconstrictive effects of lidocaine/procaine cream, which may exacerbate ulcer progression. The 50% N2O/O2 would precipitate its analgesic properties systemically with no topical activity on the wound itself, and can be regarded as an effective substitute when intravenous or topical anesthesia is not suitable or contraindicated in wound care.
Opioids remain the mainstay of treatment for moderate and severe pain. However, the incidence of side effects can be as high as 76–92% in patients with acute pain, such as respiratory depression, constipation, and itching. 8,30 One of the biggest problems faced in wound care is that patients may undergo frequent procedures. Thus, patients need to undergo intravenous anesthesia every other day, or even daily, with prolonged fasting and long periods of postanesthetic recovery. 31
The consequences may be malnutrition and delayed wound healing. Dependence and tolerance to analgesics may also occur. 32 Differed from opioids, N2O remained intact in airway reflexes and had no negative effect on respiration. The primary effects of N2O are exerted in the central nervous system, with analgesic action on supraspinal GABA (γ-aminobutyric acid) inhibition and spinal GABA activation. 33 Studies reported that N2O, as an NMDA (N-methyl-D-aspartic acid) antagonist, could be able to inhibit opioid-induced postoperative hyperalgesia and decrease consumption of opioids. 34,35
The duration of procedure was reported in three included trials 19,22,23 in this review. The mean time was significantly shorter for N2O versus morphine (16.7 min vs. 20 min; p < 0.001), or N2O versus fentanyl (38.8 min vs. 43.33 min), and was similar when N2O versus lidocaine/prilocaine cream (29.48 min vs. 28.43 min; p = 0.82). Mraovic et al. 36 found that adding N2O to isoflurane anesthesia significantly shortened the recovery time of patients undergoing laparoscopic assisted vaginal hysterectomy. This property has a positive effect on promoting patients’ recovery, shortening hospital stays, reducing economic burden, and improving satisfaction.
The above characteristics suggested that N2O was better suited for patients who cannot tolerate the side effects of opioids or needed rapid and frequent analgesia. Alternatively, N2O might also be combined with other analgesics, which could be largely superior to the currently used single-method analgesia. In the future, medical workers should carefully choose the safest and most effective analgesic methods based on patient needs and wound conditions in wound care. It is noteworthy that anesthesia is responsible for approximately 1% of N2O emissions in the atmosphere, which is substantial. Hence, N2O should be used by trained people and attention should ideally be paid to scavenge it properly.
Limitations
Two trials included in this systematic review and meta-analysis were at high risk of bias. The main areas of bias were the blinding setting and allocation concealment, because of the different characteristics of N2O and other analgesics. In addition, some of our results may be limited by the low number of trials available for subgroup analyses, which needs larger sample trials in the future so as to increase the reliability of results. In addition, one study 21 included minor patients older than 16 years and we believed that adolescents older than 16 years had complete communication skills and the ability to express their own perception. Furthermore, the overall high risk of bias in the studies, the ratio of N2O to oxygen, the analgesic drugs used in the control group, the severity of the wound, and the operators were all factors contributing to the significant heterogeneity among the included trials.
CONCLUSION
This systematic review and meta-analysis highlights the effectiveness of N2O in reducing wound care–related pain. N2O has rapid onset and may represent a safe and readily available noninvasive substitute when intravenous or topical anesthesia is not suitable or contraindicated in wound care. Caution must be taken when interpreting these results, due to the high risk of biased methods in the included studies and the heterogeneity observed across studies.
TAKE HOME MESSAGES
Insufficient pain control is a sign of impaired quality of life. Regarding the successful performance of wound care, the effectiveness, cost, and patient compliance are the three key factors for clinical decision-making. The findings suggested that N2O might be effective in patients undergoing wound care. However, when interpreting these results, caution must be taken due to the high risk of biased methods in the included studies.
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
This study was supported by clinical medical science and technology innovation project of Jinan (Grant number: 202019025). The funders had no role in the conduct of the research.
AUTHOR CONFIRMATION
As the submitting author, L.T. confirms to have written consent from all authors to submit the article and that all authors accept complete responsibility for the contents of the article. This article has not been previously published.
AUTHOR DISCLOSURE AND GHOSTWRITING
The authors have no financial interests to disclose. The content of this article was thoroughly written by the authors. No ghostwriter was used to write this article.
ABOUT THE AUTHORS
SUPPLEMENTARY MATERIAL
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Table S1
Supplementary Table S2
Supplementary Data S1
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.