
Abstract
Objective:
To develop an efficacious and efficient method for treating chronic wounds using “nanosheet” that improves the survival and localization of transplanted cells without prior seeding to optimally derive the regenerative potentials of uncultured stromal vascular fraction (SVF) cells.
Approach:
We propose a method whereby the wound is covered by uncultured SVF cells using the nanosheet [porous poly(
Results:
The placement of the nanosheet improved the grafted cell retention rate at day 10 timepoint by 5 folds, and the wound area was the smallest in the wounds treated with SVF cells plus nanosheet in comparison to the other groups. Collagen deposition and epidermal growth factor were significantly higher in the wound beds treated with SVF cells with the nanosheet, offering some mechanistic insights.
Innovation:
Porous poly(
Conclusion:
The use of the nanosheet is an effective way to improve the transplanted SVF cell retention and accelerate the overall wound closure.
INTRODUCTION
In recent years, cell therapy has emerged as one of the new strategies for treating wounds, especially those that are refractory or chronically nonhealing. Compared with the conventional approaches, cell therapies boast of some major advantages, including the mitigation of major surgical procedures and subsequent donor-site morbidities. One of the major etiological factors that contribute to the chronicity of wounds is decreased functions of the key cells involved in wound healing, namely, fibroblasts and keratinocytes. 1,2 Reduced mitotic activities of those cells, with reduction in extracellular matrix (ECM) synthesis and growth factors needed for the wound regeneration and repair, and concurrent increase in the activities of matrix metalloprotease that breaks down ECM are observed in chronic wounds. 1,2 The wound therefore remains open and susceptible to infections and secondary complications. The restoration of cell functions is key to successful wound closure, and cell therapies, in which cells of wound healing are transplanted onto the wound, are compelling methods for achieving this. Indeed, previous studies have demonstrated that cell therapies fasten wound closure time or enhance some of the processes/stages of wound healing to aid the overall wound healing. 3 –6
The selection of cells is an important step in cell-based therapies, as it determines the preparation procedures, requirement for FDA approval, and treatment outcomes. 7 –9 For instance, utilization of cultured cells in clinical settings requires FDA-approved facilities and techniques, as well as a lengthy culture period. 9 At present, keratinocytes, fibroblasts, and adipose-derived stromal vascular fraction (SVF) cells are used in clinic for wound treatments. Keratinocytes and fibroblasts are isolated from skin biopsy of patient or donor sources, expanded by cell culturing, and typically stored by freezing prior to application. 7 The preparation of these cells therefore faces two major challenges: risk of contamination during cell culturing and diminished cell viability due to cryopreservation. 10 While SVF cells can be stored through similar procedures for future use, they can also be prepared on demand, as they can be obtained directly in large quantities from adipose tissue through liposuction without cell cultures. This minimizes cell manipulation, increases cell yield and viability, and decreases the preparation time, giving them potential legislative and practical advantages over the use of cultured keratinocytes and fibroblasts.
In terms of efficacy, each of the cell types has been shown to fasten the overall healing time when applied on chronic wounds both in animal models and patients. 11 –17 Autologous keratinocytes can be expanded into a sheet of epidermis and used as a skin graft to seal the wound, and cultured allogenic keratinocytes have shown to fasten wound closure rate when applied on chronic leg ulcers. 11 –13 Fibroblast cells used in chronic wound treatments are predominantly allogenic fibroblasts, and the clinical evidence thus far demonstrated limited effects with cryopreserved fibroblasts but some improvements in the wound closure time when prepared fresh. 14 –16 As mentioned above, diminished effects of cryopreserved cells result from a combination of low cell viability (about 50% compared with nonfrozen cells) and impaired cell activities (2–30% protein synthesis and growth factor release compared to nonfrozen cells), which in turn hinder their successful colonization and regenerative activities. 14 –16 The preparation of allogenic fibroblasts in sufficient quantity without cell culturing would, however, require a large source of skin, posing a major practical challenge that likely limits their realistic on-demand use in clinic. SVF cells may be an attractive alternative, especially to allogenic fibroblasts; a previous study has found that uncultured SVF cells can promote proliferation and collagen synthesis by diabetic fibroblasts in vitro. 7 Indeed, SVF cells accelerated wound closure in patients with diabetes, demonstrating clinical efficacy comparable to that of freshly prepared allogenic fibroblasts. 17 Together, data from the prior studies indicate that SVF cells would work well to functionally substitute fibroblast cells in wound therapies. The exact mechanism by which SVF promotes wound healing is not well known. SVF contains a variety of fat cells and mesenchymal stem cells (MSCs). In particular, SVF is a rich source of adipose-derived stem cells (ADSCs) known to have multidirectional differentiation potential and to secrete various growth and inflammation factors. 18,19 Previous studies demonstrated that ADSCs can accelerate the healing of refractory wounds, 20,21 marking them to be a major functional player in SVF-based cytotherapy. Importantly, it was shown that the uncultured SVF accelerates wound closure at a similar rate to purified, cultured ADSCs in vivo despite containing a smaller number of ADSCs. 22 This result indicates that similar therapeutic outcomes can be expected from uncultured SVF cells to that of purified ADSCs, further attesting to the suitability of SVF cells for wound cytotherapy.
A common limitation in cell therapies, however, is the low retention rate of implanted cells at the grafted site; the cells undergo apoptosis or migrate out of the wound site soon after transplantation.
8,9,23,24
In order to harness the full regenerative potential of the cells, they must be retained at the wound site for sufficient amount of time for proliferation, differentiation, and release of growth and signaling factors. Common practices for localizing and supporting the transplanted cells have been to seed cells onto a scaffold such as sheets of hyaluronic acids or cover cells with a dressing such as Vaseline gauze.
13
–16
While the former option is an effective method for retaining cells at the site, it requires cell culturing and lengthy preparation, and the latter option does not seem to serve adequately for the purpose of the cell localization. Recent years saw the emergence of a novel strategy whereby therapeutics and cells are delivered through nanostructures. In particular, sheets of poly(
Taken together, we hereby propose the following method of treating chronic wounds that is optimized for clinical outcomes, as well as the ease of clinical application, cost-effectiveness, and low invasiveness. This method comprises a direct application of fresh, uncultured SVF cells harvested from fat tissue using a nanosheet as a cellular scaffold. This method should enable us to harness the full regenerative potentials of SVC cells by ensuring their long-term localization and survival without needing cell seeding/culturing. We hypothesize that the nanosheet will enhance the therapeutic effects of the SVFs and further promote wound healing by providing a more permissive environment to the cells in the wound beds.
In the present study, we first conducted two preliminary experiments to characterize the adhesiveness/cell holding ability of the nanosheet and its biocompatibility with SVF cells. In the second part of the study, the efficacy of the proposed method in treating refractory wounds was evaluated on chronic wounds created by inflicting a full-thickness skin wound on db/db mice, a well-established model of impaired wound healing. 30,31 The wound was treated with nanosheet only, SVF cells only, or nanosheet with uncultured SVF cells, and their respective effects on wound healing were assessed after 10 days on the following parameters: wound closure, reepithelialization, cell proliferation, vascularization, and collagen deposition. Furthermore, the gene expression levels of hepatocyte growth factor (HGF), epidermal growth factor (EGF), and vascular endothelial growth factor (VEGF) in the wound beds were studied to establish the possible mechanism by which the SVF-nanosheet therapy regulates wound healing.
INNOVATION
Chronic wound care lacks definitive therapies and needs more efficacious and less invasive solutions. Cell therapy has shown some clinical promises, but its use has been limited by legislative and practical challenges associated with obtaining and culturing cells. One way to avoid those problems is the use of uncultured SVF cells; however, lack of an effective method for retaining the transplanted cells has limited its efficacy. Using nanotechnology, we developed a “nanosheet” (Fig. 1) 32 that can hold transplanted cells with van der Waal forces, which uniquely enables the long-term localization of freshly harvested uncultured cells after transplantation without prior seeding.
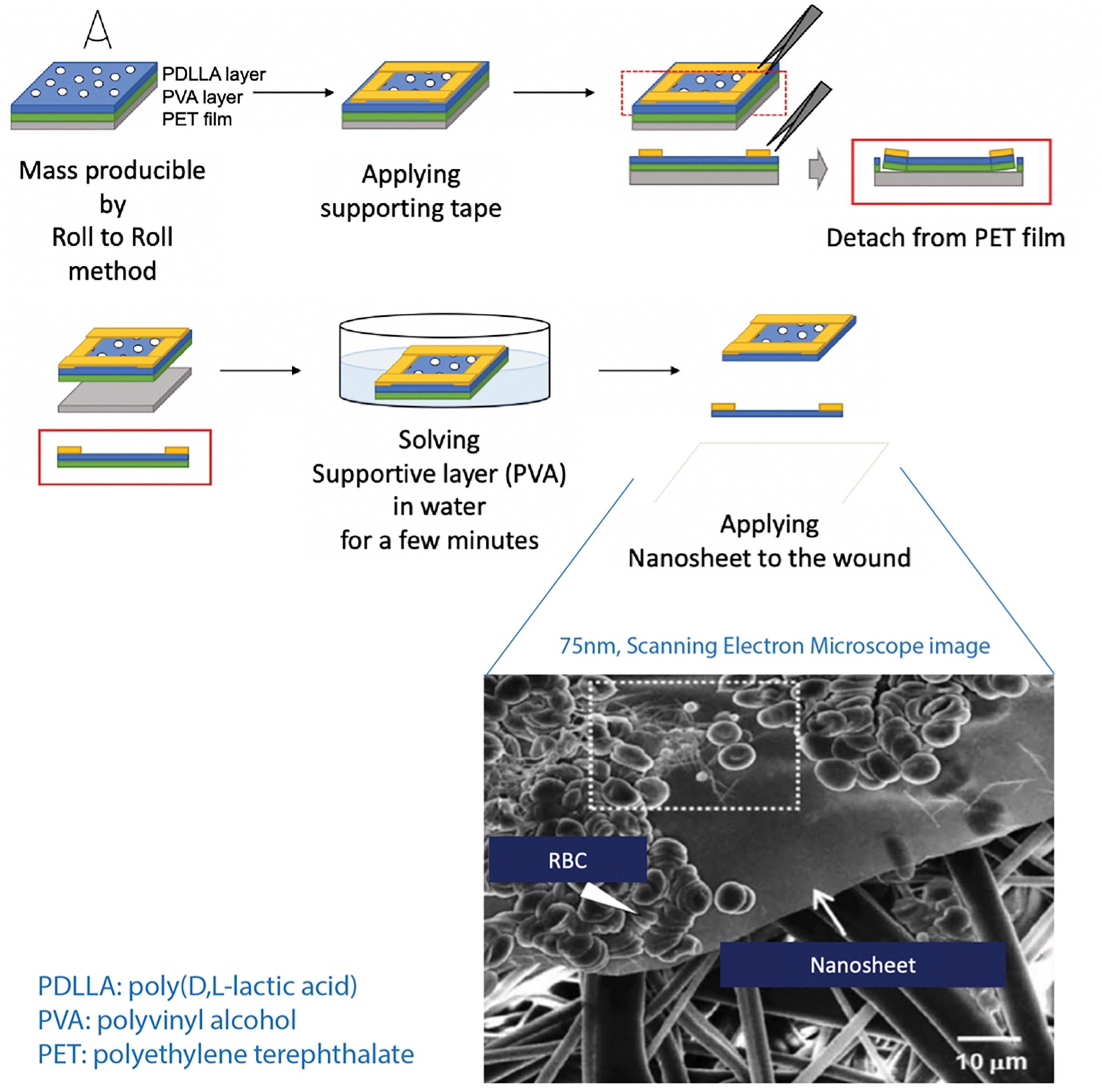
The schematic of the nanosheet cellular scaffold production. A MicrogravureTM coater was used to create porous nanosheets. A water-soluble sacrificial layer was created on a roll of PET film by coating the film with an aqueous solution of PVA (10 mg/mL) at a gravure rotating speed of 30g and a line speed of 1.3 m/min for 5 min. The solvent was then evaporated by heating the film for 5 min at 80°C. Then, the entirety of the PVA layer was coated with a 1:1 polymer blend solution of PS and PDLLA (total polymer concentrations = 20 mg/mL in ethyl acetate). After submerging the films overnight in cyclohexane, ultrasonication was performed to remove the PS region. The resultant PDLLA film with a macroporous structure (average pore diameter = 4 μm) was cut into pieces. Standard size of the pieces was 2 cm × 2 cm. The PVA layer was then dissolved in deionized water to produce a free-standing porous nanosheet. PET, poly(ethylene terephthalate); PVA, poly(vinyl alcohol); PS, polystyrene; PDLLA, poly(
CLINICAL PROBLEM ADDRESSED
Delayed or nonhealing wounds or chronic wounds are a highly prevalent clinical problem, affecting up to 8.2 million people in the United States alone. 33 They occur most commonly as a comorbidity to diabetes, venous insufficiency, peripheral arterial diseases, immune deficiencies, and dementia and cause an array of secondary complications including functional loss, infections, and amputation. 34,35 Chronic wound care is both cost- and labor-intensive, with the average healing time exceeding 12 months for leg ulcers and up to 70% of patients experiencing recurrence. 34,35 Current therapeutic options are mostly conservative and often leave wounds incompletely healed in the context of impaired healing in these conditions. Surgical interventions are required in severe cases, which may cause further morbidities. 36 –38 Chronic wound treatment therefore critically demands a new approach that is more efficacious and cost-effective with reduced treatment burden on patients.
MATERIALS AND METHODS
Animals
Twelve-week-old male BKS.Cg-Dock7m +/+ Leprdb/J “diabetic” mice were purchased from Jackson Laboratories (Bar Harbor, ME, USA). All procedures of this study were approved by the Institutional Animal Care and Use Committee (IACUC) of Brigham and Women’s Hospital and performed under the institutional guidelines for the care and treatment of laboratory animals.
Nanosheet preparation
From Polysciences, Inc. (Warrington, PA), porous poly(
A MicrogravureTM coater ML-120 (Yasui Seiki Co., Ltd., Kanagawa, Japan) was used to create porous nanosheets while using a gravure coating method. A water-soluble sacrificial layer was created on a roll of PET film by coating the film with an aqueous solution of PVA (10 mg/mL) at a gravure rotating speed of 30 rpm and a line speed of 1.3 m/min over 5 m in length. The solvent was then evaporated by heating the film for 5 min at 80°C. Then, the entirety of the PVA layer was coated with a 1:1 polymer blend solution of PS and PDLLA (total polymer concentrations = 20 mg/mL in ethyl acetate). After submerging the films overnight in cyclohexane, ultrasonication for 30 s (US-1, SND, Nagano, Japan) was used to remove the PS region while in cyclohexane. The resultant PDLLA film with a macroporous structure (average pore diameter = 4 μm) was cut into pieces. The standard size of the pieces was 2 cm × 2 cm. The PVA layer was then dissolved in deionized water to produce a free-standing porous nanosheet.
Stromal vascular fraction cell harvesting
SVF cells were harvested from the inguinal fat pad of 12-week-old male BKS.Cg-Dock7m +/+ Leprdb/J “diabetic” mice (Jackson Laboratories). Briefly, adipose tissue was harvested from this diabetic mouse and minced mechanically. Then, the tissue was incubated with 0.1% collagenase A (Roche Diagnostics GmbH; Mannheim, Germany) at 37.8°C for 40 min on a shaker. After discarding floating debris, the cell suspension was filtered through a 100-nm nylon mesh (BD Falcon, Becton Dickinson, Oxford, UK) and centrifuged at 1300g for 5 min. The stromal cell pellet was resuspended in Dulbecco’s minimum essential medium F12 (Gibco, Carlsbad, CA). Dead cells were visualized with trypan blue, and the cells were counted under a light microscope. Cell yield is summarized in Table 1.
SVF harvesting from inguinal fat from diabetic versus wild-type mice
SVF, stromal vascular fraction.
Nanosheet and cellular spreading characterization
To investigate the relative adhesion of the nanosheets in the context of cell seeding, the following experiment was conducted. A measure of 1 μL of mouse blood was placed on a plastic Petri dish and covered with nanosheet (N group) and Tegaderm® (3M, St. Paul, MN, USA) (T group) without applying an intentional pressure (placed on the dish with minimal force). The gross, diffused blood area on the dish after the application was photographed digitally (WG-40, Ricoh Company, Ltd., Tokyo, Japan) and measured by ImageJ (National Institutes of Health, Bethesda, MD, USA). In addition, the cells were observed under 20× power field of the microscope (BX53 Biological Microscope, Olympus Corporation, Tokyo, Japan).
Green fluorescent protein-labeled adipose-derived stem cell survival
In order to assess the viability and retention rate of the grafted cells at the wound sites, 12-week-old C57BL/6 were given a single, 0.8 cm diameter full-thickness skin wound on their dorsum, and 1.0 x 106 green fluorescent protein (GFP)-labeled adipose-derived MSCs (GFP+ ADSCs) (Cyagen Biosciences, Santa Clara, CA, USA) in 50 μL of medium were placed on the wound site with a respective dressing (Fig. 3A). The two groups were GFP+ ADSCs grafted with nanosheet (GN group) and GFP+ ADSCs without nanosheet (control group) (n = 6 for each group). The GN group had two nanosheets placed; one sheet directly on the wound, deep to the GFP+ ADSCs, and the other immediately superficial to the GFP+ ADSCs (Fig. 3A). Both groups received the DuoDERM®/sponge/Tegaderm® dressing as described below. DuoDERM® (ConvaTec, Berkshire, UK) was sutured to the skin as a splint at the wound corners by 4-0 Vicryl. A hydrophobic sponge (Eptsealer®, Nitto Denko, Osaka, Japan) was applied over DuoDERM to prevent the wound from drying and to maintain physical contacts of the dressing. These were covered by MultiporeTM dry for stabilization and Tegaderm® most superficially for maintaining the moisture. Tegaderm® was the only material changed at every observation made on 0, 5, and 10 post-operative days (POD).
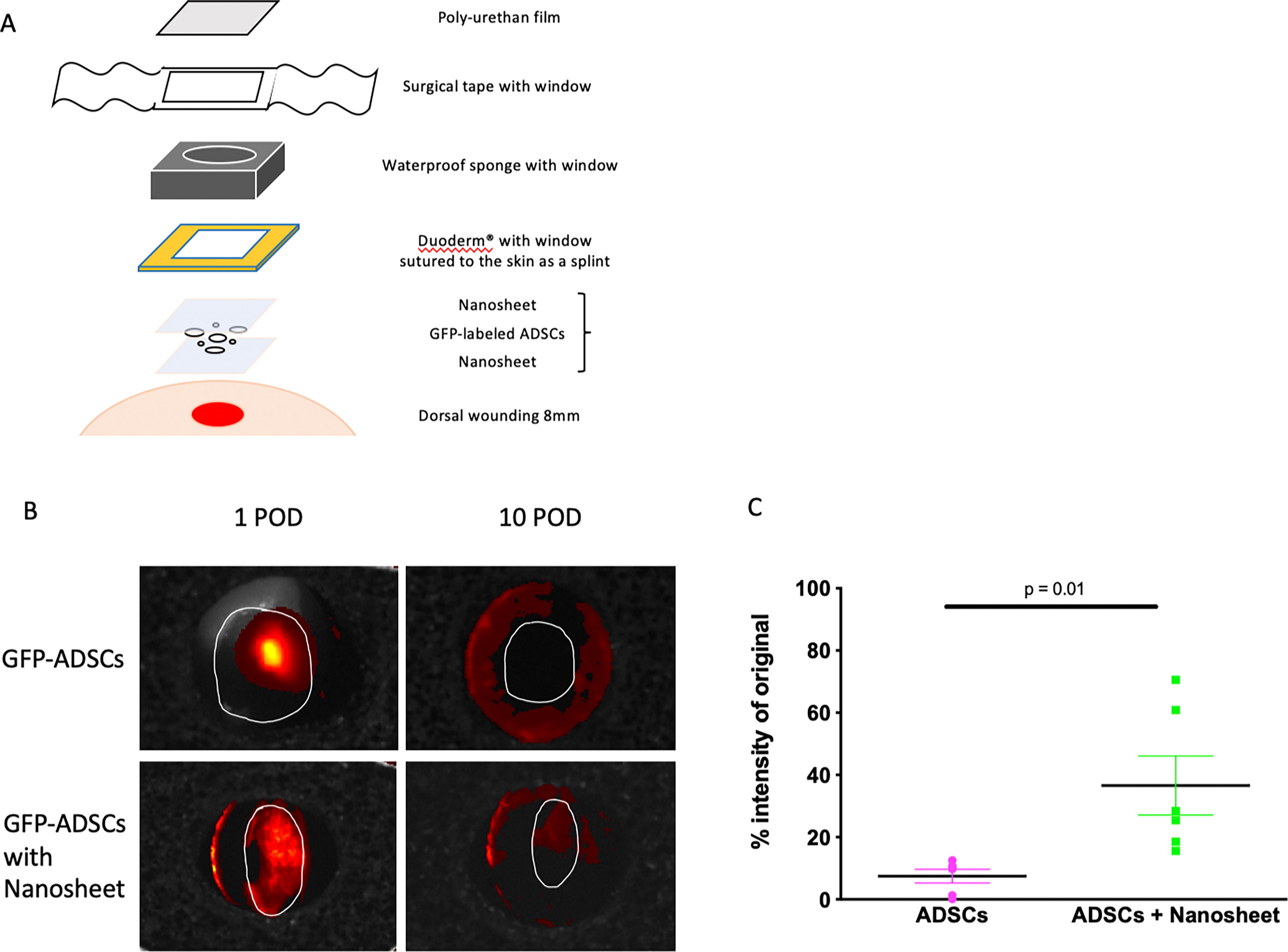
Cell survival test. For confirming whether and how long the nanosheet can hold cells on the grafted wound, GFP-labeled adipose-derived stem cells (GFP+ ADSCs) grafted on the wound
The grafted GFP+ ADSCs were traced by a bioimaging camera, IVIS (PerkinElmer, Inc., Waltham, MA, USA) on 10 POD. ImageJ was used to measure the area with high signal intensity relative to the rest of the wound (native cells). Grafted cell retention percentage (GCR%) in the wound was calculated as follows to quantify retention and viability of grafted cells:
Rapid SVF transplantation model
A total of 32, 12-week-old male BKS.Cg-Dock7m +/+ Leprdb/J “diabetic” mice were used in this in vivo experiment cohort. Additional nine diabetic mice were used as SVF cell donors. The experimental animals were randomly assigned to one of the following four groups (n = 8 in each group): control group (C) without any treatment, nanosheet group (N), uncultured SVF grafted group (S); and uncultured SVF grafted with nanosheet group (SN). Under general anesthesia using isoflurane, dorsal hair was removed from the mice by hair clipper. A single, 0.8-cm-diameter circular, full-thickness dorsal skin, including the dartos fascia, was excised to create a wound on each mouse’s dorsum using scissors. Either no cells or uncultured SVF cells (1.0 × 106 SVF cells in 50 μL of medium) were grafted onto the wounds of C and N groups, and S and SN groups, respectively. On 0, 5, and 10 POD, a digital photograph was taken from directly above the wound (10 cm from the wound), and the wound area was measured by ImageJ. Macroscopic wound closure (%) was calculated by comparing the wound area at days 5 and 10 timepoints to the area at day 0 timepoint. A schematic of this experimental method is depicted in Figure 1.
HISTOLOGY
On 10 POD, all the mice were euthanized, and a specimen of the wound was taken from each mouse and processed for histological evaluations. For the evaluation of collagen deposition in the wound site, specimens were stained with Masson Trichrome staining according to conventional procedure. Under the 20× power field, the blue areas at the wound borders were identified and considered as newly formed collagen and subsequently quantified using ImageJ. Reepithelialization was quantified by measuring the width of the area covered by the epithelial cells superficial to the wound from the outermost edge of the wounds on an IHC (immunohistochemistry)-stained longitudinal cross-section of the wound at POD 10. To evaluate angiogenesis in the wound beds, specimens were stained with goat anti-mouse CD31 antibody (AF3628, R&D Systems, Minneapolis, MN, USA) as the primary antibody and goat IgG VisUCyte HRP (horseradish peroxidase) polymer antibody (VC003, R&D Systems, Minneapolis, MN, USA) as the secondary antibody. The average number of CD31-positive vessels in the 10 randomly selected, nonoverlapping high-power fields spanning the wound beds was counted using ImageJ.
For assessing cell proliferation, rabbit anti-mouse anti-Ki67 antibody (ab15580, Abcam, Cambridge, UK) and goat anti-rabbit IgG H&L (HRP) antibody (ab205718, Abcam) were used as the primary and secondary antibodies, respectively. Ki-67-positive nuclei and total nuclei were counted under 40× magnification by ImageJ, and then the ratio of positive nuclei/total nuclei was calculated. Of note, electronic laboratory notebook was not used.
STATISTICAL ANALYSES
All the statistical analyses were performed by R (The R Foundation for Statistical Computing, Vienna, Austria), including evaluation of normality and equal variance. Tukey–Kramer tests were performed on all the subjects with appropriate normality and equal variance confirmation. All data were expressed as mean ± standard deviation. The value of p < 0.05 was considered statistically significant.
RESULTS
Nanosheet improves the distribution and attachment of cells
To assess how the nanosheet may secure cells in place, 1 μL of mouse blood was placed on a plastic dish and covered with a nanosheet (nanosheet group), polyurethane film (Tegaderm group), or nothing (control) without intentional pressing. With the nanosheet, blood cells spread to cover the area 80 times larger (360.9 ± 18.8 mm2) than that with Tegaderm (36.7 ± 6.4 mm2) (p ≤ 0.001) (Fig. 2A,B). The blood cells under the nanosheet were organized in a single-cell layer, without gaps in between cells, whereas the cells under Tegaderm were irregularly clumped together in multilayers (Fig. 2C). In addition, the cells held under the nanosheet were stationary on the dish, while some movements of the cells were observed between the Tegaderm and plastic dish. These observations indicate that application of nanosheet improves the distribution and secure attachment of cells to a solid surface (Fig. 2C).
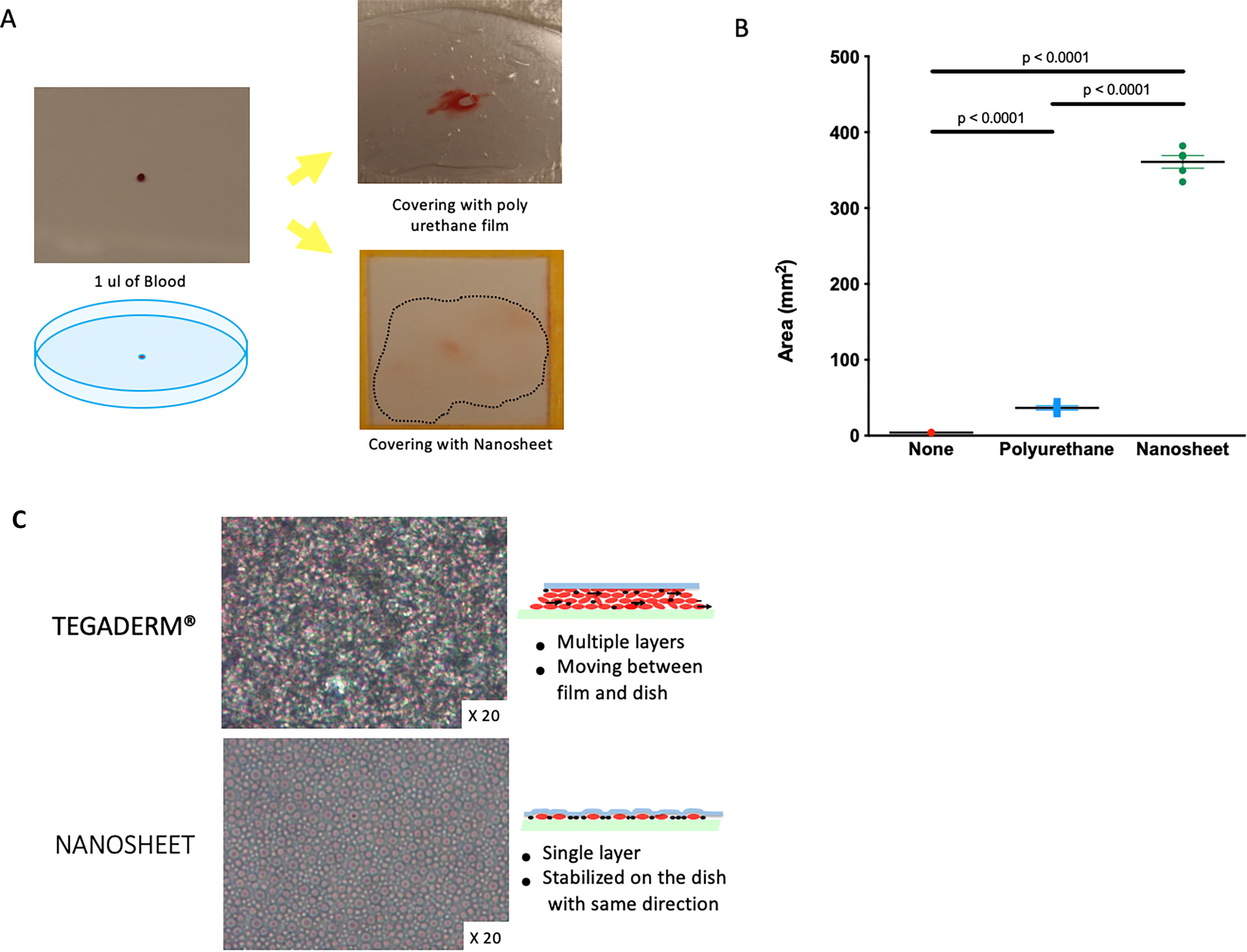
Tight attachment test. 1 μL of mouse blood was put on a Petri dish and covered with the nanosheet (N group) and polyurethane film (T group) without any intentional pressing. The area covered by the diffused blood on the dish after the application was photographed digitally and measured by ImageJ. Cell arrangement was observed under the 20× magnification. N group had 80 times greater area covered by the blood than the T group
Nanosheet placement improves stem cell retention within wounds
The grafted cell retention percentage (GCR%) of the nanosheet group and control group (GFP+ ADSCs) was 36.6 ± 23.3% and 7.49 ± 5.33%, respectively. There were significantly more grafted cells remaining and surviving at the wound site at 10 POD in the nanosheet group compared with the no Nanosheet (p = 0.01) (Fig. 3B,C).
Nanosheet placement with SVF improves wound healing in murine wound model
The average percent wound area of original of the SN group (37.4% ± 12.0%) was significantly smaller compared with the control (66.7% ± 19.0%, p = 0.003), N only (55.98% ± 18.1%, p = 0.03), and S only (51.5% ± 8.7%, p = 0.02) groups on 10 POD (Fig. 4A,B). The S group (20.3 ± 5.4, p = 0.004) and the SN group (18.6 ± 5.6, p = 0.02) had statistically greater numbers of CD31+ vessels in the wound beds than the control group (10.9 ± 5.7) (Fig. 5A,B). Furthermore, the S group (0.26 ± 0.06, p = 0.006) and the SN group (0.23 ± 0.07, p = 0.04) had significantly higher ratios of Ki-6 positive nucleus: total nuclei compared with the control group (0.15 ± 0.07) (Fig. 5C,D). Collagen deposition as a percentage of HPF (high-power field) was significantly greater in the SN group (62498 ± 20362) compared with the control group (41544 ± 13882, p = 0.02), N group (40865 ± 14382, p = 0.02), and S group (37822 ± 12871, p = 0.007) (Fig. 5E,F). The SN group (2.6 ± 0.6 μm) had significantly greater average epithelialization length over the wound compared with the control group (1.7 ± 0.3 μm, p < 0.001) and N (1.99 ± 0.5 μm, p = 0.03) groups and demonstrated a strong trend of being greater compared with the S only group (2.2 ± 0.3 μm, p = 0.07) (Fig. 5G,H).
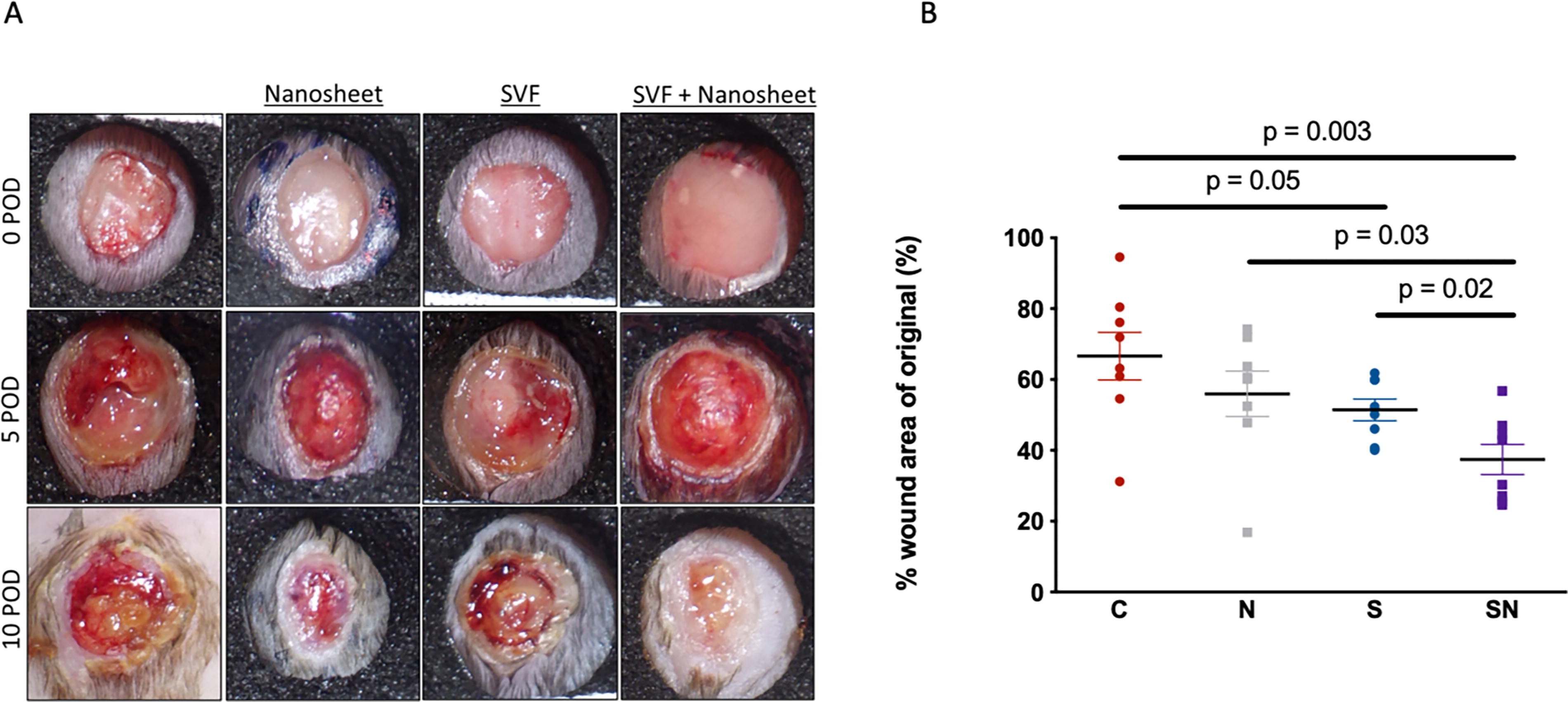
Macroscopic evaluation of wound healing in in vivo rapid transplantation model. Macroscopic photos of wound healing
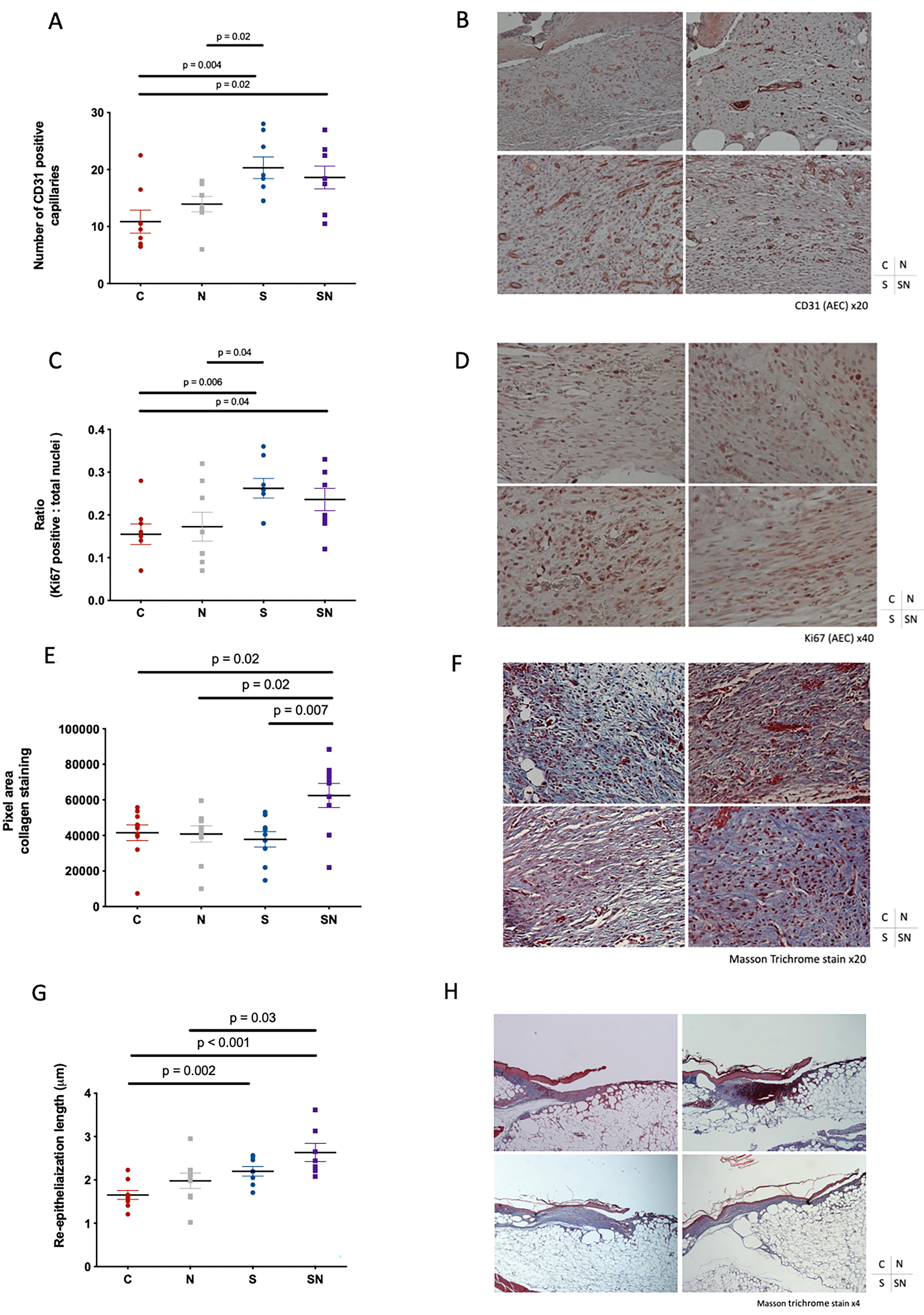
Immunohistochemical evaluation of the wound beds at 10 POD. In CD31 staining to evaluate angiogenesis, S (20.3 ± 5.4, p < 0.01) and SN (18.6 ± 5.6, p < 0.01) demonstrated statistically larger numbers of CD31-positive vessels than C (10.9 ± 5.7)
Nanosheet placement with SVF increases the local concentration of EGF at the wound bed
The relative HGF mRNA expression levels in the wound bed specimen was significantly higher in the SN group (15.24 ± 13.6) than in both the control (1.00 ± 0.9, p = 0.04) and N (0.47 ± 0.18, p = 0.04) groups (Fig. 6A). The relative EGF mRNA expression was significantly greater in the SN group (12.70 ± 8.6) than in the control (1.00 ± 0.94, p = 0.008), N only (1.34 ± 0.87, p = 0.003), and S only (1.92 ± 8.6, p = 0.04) groups (Fig. 6B). The relative VEGF mRNA expression did not increase with the placement of nanosheet with SVF compared with the control group (Fig. 6C).
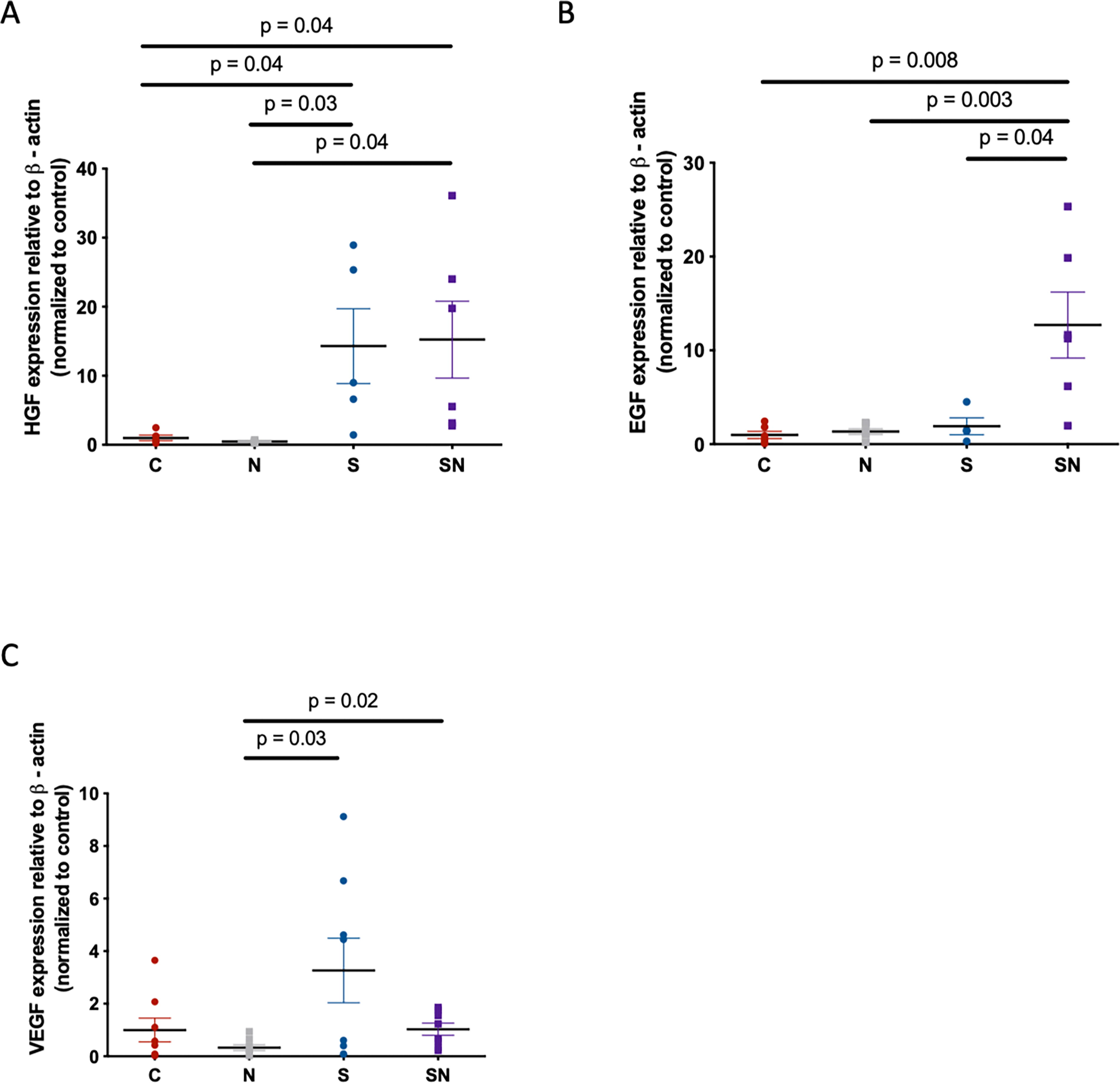
Growth factor expression levels at the wound beds at 10 POD. The relative HGF mRNA expression levels in the wound bed specimen were significantly higher in the SN group (15.24 ± 13.6) compared with both the control (1.00 ± 0.9, p = 0.04) and N (0.47 ± 0.18, p = 0.04) groups
DISCUSSION
Cell therapies have been an important method for treating refractory wounds in recent years. Clinical outcomes of keratinocyte-, fibroblast- and SVF-based cytotherapies have similarly shown to reduce the healing time and increase complete healing in diabetic foot ulcers, 11 –17,39 demonstrating considerable therapeutic value of each of the types of the treatment, and SVF as a viable fibroblast/ADSC substitute (and perhaps more). A key difference, however, is that, unlike keratinocytes and fibroblasts which rely on direct functions of the transplanted cells, SVF cells are thought to exert their wound healing effects mainly through promoting the activities of fibroblasts and changing those of other cells found in the wound site. 7,22 It then follows that the efficacy of the SVF-based treatment greatly depends on the spatial and temporal interactions of cells at the wound site. Low cell retention post-transplantation at the wound site therefore presents one of the greatest obstacles to SVF-based therapy, and improving this aspect holds promise for attaining superior therapeutic outcomes. Indeed, recent studies have shown that adversity of low cell retention after transplantation due to both migration and apoptosis of the transplanted cells and low retention rate of cells was associated with poorer therapeutic outcomes in cell therapies. 8,9,23,24
SVF cells are typically derived from fat tissue digestion. Digestion can either be enzymatic, the most common isolation method, or nonenzymatic. Enzymatic digestion involves the use of collagenase, dispase, or trypsin, while nonenzymatic digestion, also called mechanical digestion, includes centrifugation, filtration, and microfragmentation. 40,41 It is worthwhile discussing the effects of using SVF cells and AD-MSCs on regeneration on wound healing, which have been extensively studied. SVF therapy was shown to successfully help burn patients during their rehabilitation, improving wound and scar healing. 41 Combining SVF cells and AD-MSCs with growth factors like F-GRF and PRP in a nano-fat material/scaffold has also shown improvement in wound healing and reduction of scar areas. 41 Interestingly, SVF therapy has been a research focus in breast reconstruction. Gentile et al. found an increased 3D volume of the breast 12 weeks post reconstruction and an improved restoration of its contour in patients who received fat grafting enhanced with SVF cells compared with patients who only received acellular fat grafting. 42 Apart from being used in regenerative surgery, adipose stem cells could have a prooncogenic effect as has been shown in experimental cancer models. This could partially be due to their biological mechanism of differentiation involving the activity of receptor tyrosine kinases (RTKs), which apart from being crucial for the regulation of cellular homeostasis, also mediate cancer progression. 43 Owing to their high secretory activity and preferential targeting of tumor cells, ASCs can potentially be a means of anticancer drug delivery. 44,45 In talking about wound healing, researchers should therefore keep in mind its risks for tumor progression and delve into the oncological safety of ASCs. 44
Our results showed that the nanosheet can hold cells in a single-cell layer and improve their even distribution when applied on a solid surface. Furthermore, the nanosheet was able to significantly increase the overall retention of cells at the wound site 10 days following transplantation on the wounds in vivo. Together, these results demonstrate that the nanosheet can function well as a cellular scaffold to enhance the localization and/or survival of transplanted cells without the need for prior seeding. The wound closure was significantly fastened by the application of SVF cells or SVF cells in combination with the nanosheet, but not by the nanosheet alone. Importantly, placement of the nanosheet significantly enhanced the improvement in the wound closure rate by SVF cells, indicating that it was able to augment the regenerative effects of those transplanted cells. Next, we examined which aspects of wound healing might be regulated by SVF cells, the nanosheet or their combination. SVF cells alone or in combination with nanosheet were able to improve all the parameters of the wound healing evaluated, namely, reepithelialization, cell proliferation, vascularization, and collagen deposition. These results were consistent with the previous study that demonstrated that SVF cells, as well as ADSCs, contributed to the angiogenic processes and collagen deposition when transplanted on a refractory wound in vivo. 22 Collagen deposition, however, was uniquely augmented in the group treated with the SVF cells in combination with the nanosheet in comparison to the other groups. This may outline the core mechanism by which the nanosheet supplements the transplanted cells in fastening wound closure: Collagen deposition reflects fibroblast activities that are known to be dampened in diabetic wounds and enhanced by SVF cells. 7,40 The improvement in the localization/retention of the transplanted SVF cells by the nanosheet may have a particular benefit on their effects in restoring the activities of the diabetic fibroblast cells at the wound beds. Indeed, placement of the nanosheet with SVF cells significantly improved the expression of EGF, a key factor responsible for stimulating fibroblast migration and collagen synthesis, indicating its likely role in bringing about the observed acceleration in wound closure. The nanosheet may have allowed for longer exposure of the wound beds to increased levels of EGF, which may in turn have resulted in augmentation of the fibroblast activity/migration. Taken together, our results indicate that the SVF cells are able to promote the overall wound healing in refractory skin wound by inducing collagen production and angiogenic processes, consistent with the findings from the previous studies. 7,22 The nanosheet particularly augments the effect of SVF cells on collagen synthesis through EGF, most likely by enhancing the activities/number of dermal fibroblasts at the wound beds, and significantly improves the overall wound healing rate without prior cell seeding. Compared with the existing methods, the method proposed in this study may offer a better clinical potential due to the mitigation of cell culture and associated legislative and practical challenges, made possible by the unique property of the nanosheet and improved therapeutic outcomes.
Further studies are required to establish whether the observed increase in collagen disposition with the nanosheet is due to enhanced activities of the fibroblasts or/and increase in the migration. It is also unclear as to why the nanosheet affects the effect of SVF cells on collagen synthesis more than the other aspect of the wound healing evaluated. It is possible that this is simply a reflection of the mechanism by which SVF cells promote wound closure—and its dependence on the fibroblast activities/migration being the most significant. Another possibility is that it provided a better environment for the dermal fibroblast cells once they were activated by their interactions with the SVF cells. This brings us onto another question: If the nanosheet was able to augment the activity of the fibroblasts partially through supporting their activity directly, does it have the ability to augment the regenerative activities of transplanted fibroblasts, especially those that have been cryopreserved? Answering this question may allow better exploitation of the regenerative potentials of commercially available allogenic fibroblasts in wound therapies. Finally, although the present study demonstrated that the nanosheet functions well as a cellular scaffold in general, it remains uncertain as to whether other cell types can further benefit from the placement of the nanosheet. Another exciting avenue that could be explored is the use of nanosheet as an acellular scaffold for direct delivery of growth factors. For example, the results of the present study indicate that supplementation of EGF may be able to replicate some of the regenerative effects of SVF cells in promoting wound healing, and the biocompatible nanosheet may be a suitable vehicle.
CONCLUSION
The present study demonstrated that the nanosheet functions well as a unique cellular scaffold which can improve the cellular retention without prior seeding, making its use ideal for cytotherapies with uncultured cells such as SVF cells. Nanosheet allows effective harnessing of the regenerative potential of transplanted, uncultured SVF cells through increasing the exposure of the wound to EGF and improves collagen deposition and overall wound healing.
KEY FINDINGS
The nanosheet can hold cells in a single-cell layer and improves their even distribution when applied on a solid surface.
The nanosheet can increase the overall cell retention following transplantation on the wounds.
The nanosheet augments the effect of SVF cells on collagen synthesis through EGF and improves overall wound healing.
ACKNOWLEDGEMENT AND FUNDING SOURCES
Funding was received from Wound Healing Society Innovation Grant (to I.S.).
AUTHOR CONFIRMATION
Y.E. analyzed the results, wrote the bulk of the article, contributed to the experiments, and produced figures. S.A. conceptualized the initial experiment and conducted the experiment; C.G. contributed to the article writing; M.W. conducted experiments; A.K. contributed to the article writing; M.T. conducted the preliminary experiments; J.M. and L.W. analyzed the data; T.F. constructed the initial experimental design; K.N. oversaw the overall experiment; and I.S. conceptualized the experiment, edited the article, and oversaw the entire project.
Footnotes
AUTHOR DISCLOSURE AND GHOSTWRITING
I.S. reports a relationship with InPrint Bio, LLC that includes equity or stocks. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the article apart from those disclosed. The authors have no ghostwriters to disclose.
ABOUT THE AUTHORS