
Abstract
Objective:
The meta-analysis was performed to evaluate the effectiveness of telemedicine interventions on patients with diabetic foot ulcers (DFU).
Approach:
The authors conducted a comprehensive search across eight databases. The aim was to identify randomized controlled trials examining the effectiveness of telemedicine for patients with DFU. Methodological qualities of included studies were assessed using Cochrane Handbook for Systematic Reviews of Intervention. Subsequently, a meta-analysis was conducted using RevMan 5.3 to synthesize the findings.
Results:
Ten studies involving 1,678 patients with DFU were included in the meta-analysis. In comparison to the face-to-face intervention group, telemedicine interventions significantly reduced the amputation rate (risk ratio = 0.64, 95% confidence interval [CI] = 0.44–0.92, p = 0.02), decreased costs (mean difference [MD] = −4158.51, 95% CI = −7304.69 to −1012.34, p = 0.01), better controlled fasting blood glucose (MD = −0.89, 95% CI = −1.43 to −0.36, p = 0.001), and achieved superior glycated hemoglobin control (MD = −0.71, 95% CI = −1.01 to −0.41, p < 0.00001). No significant differences were observed between the telemedicine group and the face-to-face group in terms of healing rate, mortality, and healing time.
Innovations:
Our study suggests that telemedicine is a viable strategy for managing DFU.
Conclusions:
The meta-analysis indicates that telemedicine interventions have a positive effect on DFU. Nevertheless, more well-designed and high-quality studies are needed to reach a conclusion with greater confidence.

INTRODUCTION
Diabetes mellitus is a global health issue, with an estimated prevalence of over 536 million adults worldwide in 2021, projected to increase to 12.2% by 2045. 1 In 2021, it is estimated that China has about 141 million patients with diabetes aged between 20 and 79 years, making it the country with the highest number of cases to date. 2 Among these individuals, approximately 25% of patients with diabetes are expected to develop diabetic foot ulcers (DFU). 3
DFU is considered to be one of the most expensive and devastating complications of diabetes mellitus. 4 A meta-analysis revealed a remarkably high overall mortality rate for DFU, with a mortality rate approaching 50% within 5 years. 5 The amputation rate attributed to DFU is as high as 27.3%. 6 The findings indicated that DFU was significantly associated with an elevated risk of all-cause mortality (risk ratio 2.45, 95% confidence interval [CI] 1.85–2.85). 7 DFU contributes to increased hospital expenditures, diminished productivity, unemployment, social isolation, and depression, significantly impacting the quality of life. 8
With the continuous upgrade of health care systems and the development of information technology, telemedicine technology has emerged. This technology assists health care professionals in monitoring, educating, and managing patients with DFU, providing safe and effective foot care. It is particularly beneficial for patients who face mobility challenges or reside in remote villages or communities far from medical centers. The application of telemedicine technology helps reduce patient travel to hospitals and waiting times for examinations, thereby easing the physical and financial burdens on patients and relieving strain on health care resources. 9 Telemedicine technology is considered a promising and potential approach to caring for patients with DFU. 10 Through remote monitoring, it effectively reduces the clinical burden without increasing overall treatment costs. 11 A systematic review found that the telemedicine group exhibited similar healing rates, healing times, and mortality rates compared to the face-to-face group. In addition, there was a trend toward lower costs in the telemedicine group. 12 Patients with DFU perceive telemedicine as valuable for self-monitoring. However, the actual effect of telemedicine may vary because of various facilitating factors and barriers. 13
Despite the numerous advantages demonstrated by telemedicine technology, its role in the management of diabetes-related foot disease remains controversial. 14 Rasmussen et al. revealed a higher mortality rate in the telemedicine group compared to the standard outpatient monitoring group. 15 To comprehensively assess the effects of telemedicine interventions on patients with DFU, we conducted a meta-analysis by incorporating a greater number of eligible studies, including Chinese literature. Beyond evaluating the impact on wound healing, we also investigated the effects on diabetes-related indicators. Such assessments contribute to providing more robust evidence for guiding clinical practices and further optimizing care and management strategies for patients with DFU.
CLINICAL PROBLEM ADDRESSED
DFU exhibits a high incidence, disability, and mortality rate. Owing to patients’ limited mobility and delayed wound healing, there is an increased physiological, psychological, and economic burden. Some studies suggest that telemedicine interventions may serve as effective measures for patients with DFU. Therefore, through a systematic analysis of the effectiveness of telemedicine interventions in the management of DFU, we aim to provide evidence-based insights and explore its potential as a sustainable solution for improving patient outcomes, reducing complications, and enhancing overall care.
MATERIALS AND METHODS
This study represents a systematic review and meta-analysis of randomized controlled trials (RCTs). The researchers strictly followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist for the comprehensive reporting of systematic reviews that incorporate meta-analysis. The utilization of the PRISMA checklist ensures a standardized and transparent presentation of the findings in this review. The protocol of this systematic review and meta-analysis was published on PROSPERO (CRD42024505926).
Literature search strategy
The authors conducted a literature search of relevant RCTs in English databases (i.e., PubMed, Web of Science, the Cochrane Library, and EMBASE) and Chinese databases (i.e., China Biology Medicine, China National Knowledge Infrastructure, WanFang, and VIP databases) from database establishment until January 2024. The search strategy used the following terms: “diabetic foot” or “diabetic feet” or “diabetic foot ulcer” or “DF” or “DFU,” and “telemedicine” or “mhealth” or “eHealth” or “telehealth” or “telemonitoring” or “software” or “mobile health” or “mobile application” or “APP,” and “Randomized Controlled” or “Clinical Trial”.
In addition to the systematically identified studies, we conducted a manual search of references from both the identified studies and previous systematic reviews to uncover relevant articles that may not have surfaced in the initial database search. Articles found during this manual search underwent the same retrieval and screening process as the other studies. The authors were contacted when necessary to obtain any additional information. Our search criteria were confined to trials involving human participants, and we focused on studies with full texts published in either English or Chinese.
Study inclusion and exclusion criteria
The inclusion criteria for this study were as follows: (1) patients diagnosed with DFU; (2) study design: RCTs; (3) interventions: the intervention group received any form of telemedicine interventions (e.g., mobile applications, internet, web-based systems, teleconsultation, and telemonitoring), whereas the control group received standard care (e.g., face-to-face wound care management in a clinic/hospital or at home); and (4) articles published in English or Chinese. The exclusion criteria were as follows: (1) repeated publication of literature; (2) inability to obtain the original text; (3) lack of response from authors or inability to access the dataset, leading to exclusion as a category without detailed data; (4) difficulties in data extraction or incomplete data in the literature; and (5) studies not involving patients with DFU in comparisons between telemedicine interventions and face-to-face interventions.
Data abstraction and quality assessment
Two reviewers independently utilized a predesigned manual form to extract data, encompassing the following information: study characteristics (author names, publication year, and country), participants (sample size), intervention features (intervention methods and study duration), and outcomes. To ensure accuracy, the extracted data underwent validation by a third reviewer. Any discrepancies or differences in data extraction were discussed and resolved through consensus among the three reviewers.
Two researchers independently evaluated the risk of bias in the included studies using the risk of bias assessment tool recommended in Cochrane Handbook 5.1.0. 16
In instances of disagreement, a thorough discussion was conducted to achieve a consensus or a final decision was reached by a third researcher. Adhering to the handbook’s guidelines, the risk of bias assessment considered various aspects, including random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias), and other biases. The researchers rendered judgments of low, high, or unclear risk of bias for each included study.
Statistical analyses
All statistical analyses were performed using the Review Manager Software (RevMan5.3; Microsoft, Redmond, WA). Continuous data were amalgamated using the mean difference (MD) and a 95% CI, whereas dichotomous outcomes were scrutinized through the calculation of relative risk (RR) with a 95% CI. The heterogeneity among the results of included studies was assessed using the I 2 statistic, and this statistic was combined with a χ 2-test to determine the degree of heterogeneity. To assess heterogeneity among the various studies, if there is no significant heterogeneity (p > 0.1, I 2 < 50%), a fixed-effects model is used for analysis. In cases where heterogeneity is present (p < 0.1, I 2 > 50%), but clinical judgment suggests the need for consolidation of results with consistency across groups, a random-effects model is used for analysis, and subgroup analyses are conducted to identify the sources of heterogeneity. In addition, potential publication bias was assessed when >10 studies were available using a funnel plot.
RESULTS
Search process
A preliminary literature search through the dataset revealed 1,080 articles, with an additional 1 article from other sources. After removing 92 duplicate articles using EndNote X9 reference management software, 989 articles were retained. Upon reviewing titles and abstracts, 938 articles were excluded as they did not meet the inclusion criteria, leaving 51 articles. Following a thorough examination of the full texts based on inclusion and exclusion criteria, a total of 13 articles were qualitatively synthesized, and 3 articles were subsequently excluded. 17,21,24 Ultimately, 10 studies were included in the meta-analysis (Fig. 1). 11,15,18 –20,22,23,25 –27
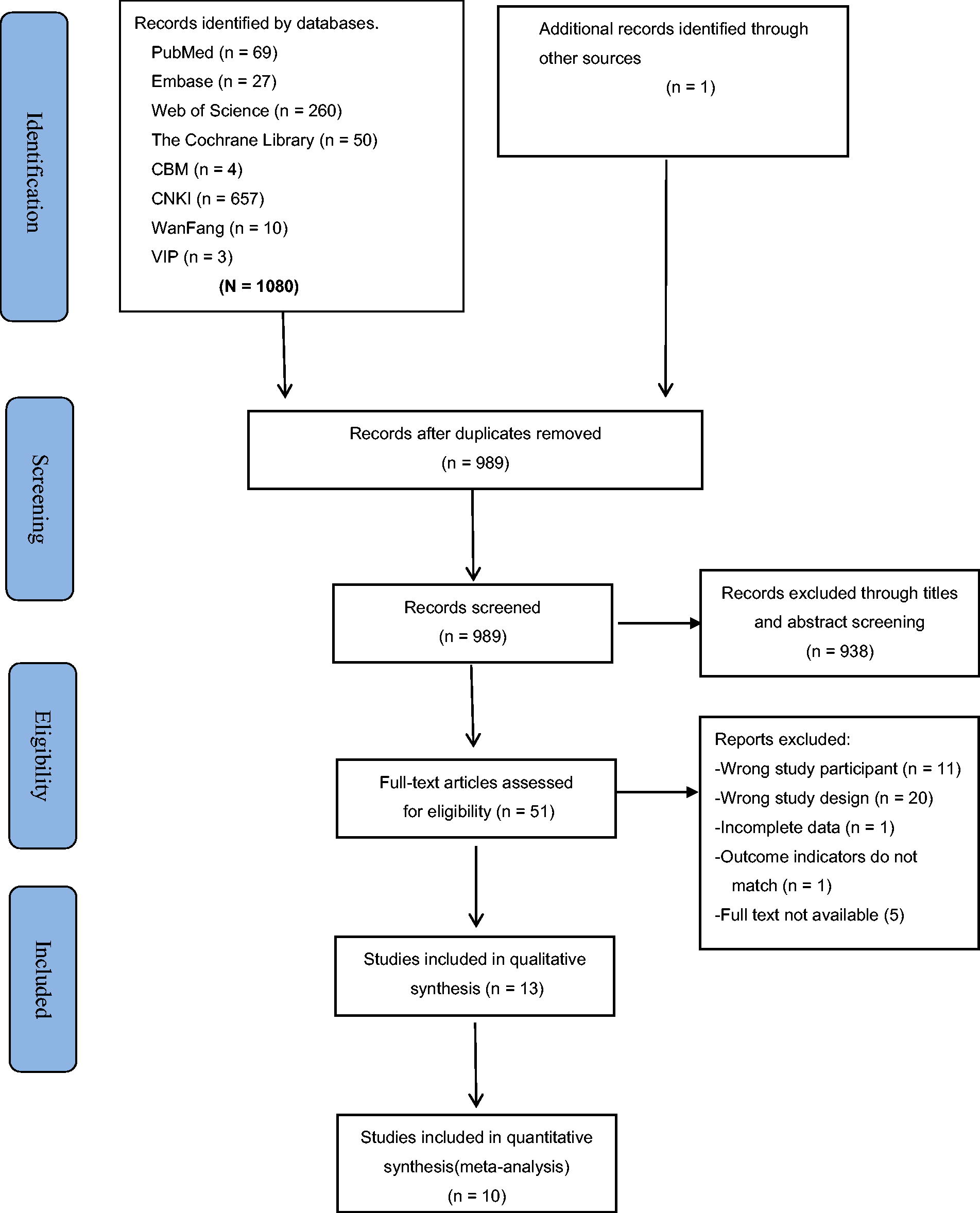
Flow chart of the study selection process.
Study characteristics
The 10 RCTs included in the meta-analysis were conducted between 2004 and 2023. A total of 1,678 participants were involved, with 798 patients in the telemedicine group and 880 patients in the face-to-face group. Four studies were conducted in China, two in Denmark, two in Norway, one in France, and one in the United States. The intervention durations varied from three clinic visits to one year. The detailed demographic data of the 10 studies are summarized in Table 1.
Characteristics of the included studies
APP, mobile application; F, face-to-face; FPG, fasting plasma glucose; HbA1c, glycated hemoglobin; NA, not available or not applicable; RCT, randomized control trial; T, telemedicine. (1) Healing rate (2) Amputation rate (3) Mortality (4) Costs (5) Healing time (6) FPG (7) HbA1c (8) Self-management behavior (9) Days spent in hospital (10) Self-reported health (11) Well-being (12) Quality of life (13) Problem areas in diabetes (14) Self-efficacy.
Risk of bias in the included studies
The authors utilized the Cochrane Risk of Bias tool to assess the risk of bias for each study (Fig. 2). All studies were described as randomized, with only two studies not specifying the use of a random sequence generation method (i.e., generated by a computer program or random number table). Approximately 30.8% (4 out of 13) of the studies disclosed allocation concealment, and none met the criteria for blinding participants, personnel, and outcome assessment. Except for 1 study that did not disclose dropout or loss to follow-up, 26 the remaining 12 studies all reported such information. All studies explicitly outlined expected outcomes to mitigate reporting bias. Baseline characteristics, including gender, age, and duration of diabetes, were compared between the experimental and control groups in all studies, demonstrating comparability at baseline. Three studies were excluded from the analysis because of analysis bias and data selection. 17,21,24

Results of quality assessment.
Outcome analysis
Healing rate
Four RCTs 11,15,20,26 reported wound healing rate, and there was little heterogeneity observed among the studies (I 2 = 5%, p = 0.37). A fixed-effects model was used to analyze the pooled RR, yielding a result of 1.02 (95% CI = 0.94–1.12, p = 0.59). The findings indicate that the application of telemedicine interventions in patients with DFU demonstrates no significant difference in wound healing compared to face-to-face interventions. Figure 3 illustrates a forest plot comparing wound healing rates between telemedicine interventions and face-to-face interventions.
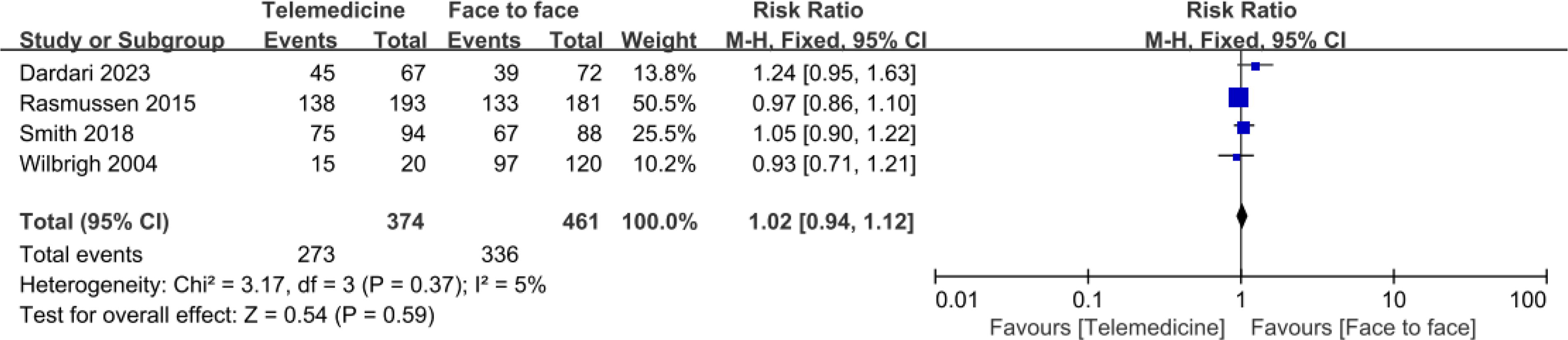
Forest plot for healing rate in studies with telemedicine group versus face-to-face group.
Amputation rate
Four RCTs 11,15,19,20 were included to evaluate the amputation rate. The fixed-effects model was applied because no heterogeneity was indicated in the analysis (I 2 = 0%, p = 0.60). A difference in the reduction of amputation rates was observed when comparing the telemedicine group to the face-to-face group (RR = 0.64, 95% CI = 0.44–0.92, p = 0.02) (Fig. 4).
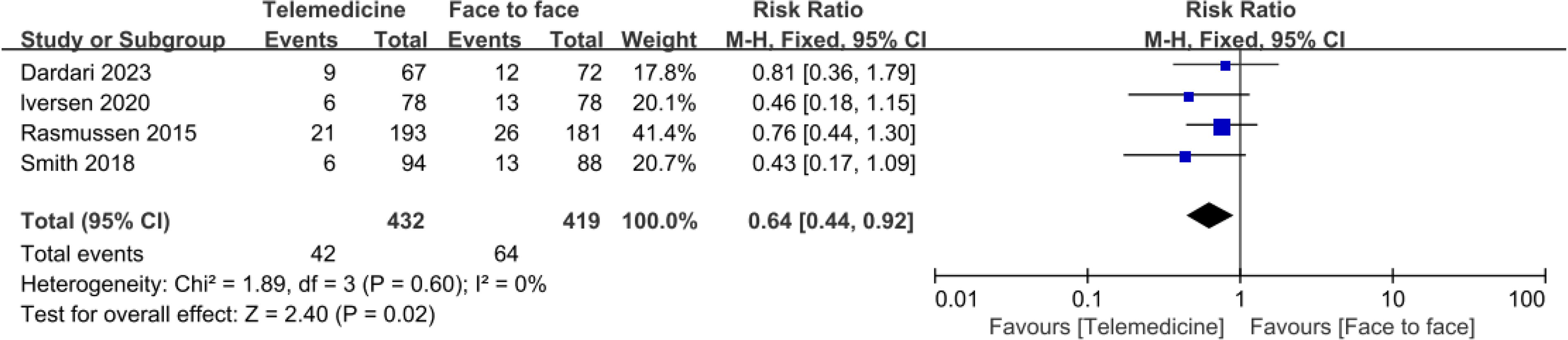
Forest plot for amputation rate in studies with telemedicine group versus face-to-face group.
Mortality
Three RCTs 11,15,20 were included to evaluate the mortality. The fixed-effects model was applied because no heterogeneity was indicated in the analysis (I 2 = 41%, p = 0.18). When comparing the telemedicine group with the face-to-face group, no significant difference was observed in reducing mortality (RR = 1.53, 95% CI = 0.78–3.02, p = 0.22) (Fig. 5).

Forest plot for mortality in studies with telemedicine group versus face-to-face group.
Costs
Two RCTs 11,18 were included. A fixed-effects model was applied, revealing no heterogeneity in the analysis (I 2 = 0%, p = 0.98). When comparing the telemedicine group with the face-to-face group, there was a significant difference in the one-year cost for patients with DFU (MD = −4158.51, 95% CI = −7304.69 to −1012.34, p = 0.01) (Fig. 6).

Forest plot for cost in studies with telemedicine group versus face-to-face group.
Healing time
Three RCTs 19,20,26 were included to evaluate healing time. The fixed-effects model was applied because no heterogeneity was indicated in the analysis (I 2 = 0%, p = 0.74). No significant difference in healing time was observed when comparing the telemedicine group with the face-to-face group (MD = −3.28, 95% CI = −15.78 − 9.22, p = 0.61) (Fig. 7).

Forest plot for healing time in studies with telemedicine group versus face-to-face group.
Fasting plasma glucose
Four RCTs 22,23,25,27 were included, and high heterogeneity was observed among the research (p = 0.01, I 2 = 72%). Therefore, a random-effects model was used for the meta-analysis. The results indicated that patients in the telemedicine group had fasting plasma glucose (FPG) monitoring levels of 0.89 lower than those in the face-to-face group, with better control, and the difference was statistically significant (MD = −0.89, 95% CI = −1.43 to −0.36, p = 0.001) (Fig. 8).

Forest plot for FPG in studies with telemedicine group versus face-to-face group. FPG, fasting blood glucose.
Glycated hemoglobin
Incorporating three studies, 23,25,27 no heterogeneity was observed among the research (p = 0.78, I 2 = 0%). The fixed-effects model was used for the meta-analysis. The results indicated that patients in the telemedicine group had glycated hemoglobin (HbA1c) levels of 0.71 lower than those in the face-to-face group, with better control, and the difference was statistically significant (MD = −0.71, 95% CI = −1.01 to −0.41, p < 0.00001) (Fig. 9).

Forest plot for HbA1c in studies with telemedicine group versus face-to-face group. HbA1c, glycated hemoglobin.
DISCUSSION
The purpose of this meta-analysis is to evaluate the impact of telemedicine interventions on patients with DFU. Our meta-analysis includes 10 studies, and the results indicate that telemedicine interventions for patients with DFU can reduce amputation rates, decrease costs, and better control FPG and HbA1c when compared with face-to-face interventions. There is no significant difference in healing rates, mortality rates, and healing time between telemedicine interventions and face-to-face interventions, indicating that telemedicine interventions are not inferior. Overall, this meta-analysis reveals a positive trend in the beneficial effects of telemedicine interventions on DFU.
Telemedicine intervention proves to be an effective approach to managing DFU, facilitating the rational allocation of health care resources, and reducing health care costs. Its application can extend to rural areas or regions with limited health care service coverage, providing community hospitals with technical guidance from specialized professionals to maintain high standards of wound care. Research indicates that the costs associated with telemedicine intervention are lower than standard levels, a trend more pronounced in rural and remote areas. 18 This study’s synthesis reaffirms this perspective. A study in the United Kingdom revealed that diabetes foot care constitutes a significant portion of health care expenditures, exceeding the total costs of breast cancer, prostate cancer, and lung cancer. Most expenses arise from long-term severe ulcers. 28 Therefore, the widespread adoption of telemedicine intervention will alleviate the pressure on health care systems.
HbA1c stands out as the prime indicator for evaluating average blood sugar regulation. 29 Research indicates that maintaining HbA1c levels between 7% and 8% in patients with DFU is conducive to ulcer healing without escalating mortality rates. 30 Elevated HbA1c levels (≥8%) and fasting blood sugar levels (≥7mmol/L) correlate with heightened risks of lower limb amputation in DFU cases. 31 Studies, including Dissanayake et al., underscore the pivotal role of glucose control in mitigating amputation risks and expediting wound healing among patients with DFU. 32 Notably, inadequate blood sugar monitoring in patients with DFU has been reported by Chin YF et al. 33 Leveraging telemedicine offers a promising solution, facilitating real-time reminders, imparting disease awareness through telemedicine health education, and bolstering patient compliance and self-care consistency. In the study by Qin Xuemei et al., 27 continuous care interventions for patients with DFU were conducted via the WeChat platform. A multidisciplinary management team was established, and disease knowledge content was sent to patients through text, video, and images or animations in WeChat groups, strengthening interaction between medical professionals and patients or peers. After 6 months, patients with DFU showed a significant decrease in blood glucose levels. There were noticeable improvements in self-management behaviors and self-efficacy. This meta-analysis demonstrates that telemedicine interventions have a more favorable impact on the control of FPG and HbA1c levels in patients with DFU. Given the importance of blood sugar control, it is hoped that more health care managers will take measures to enhance blood sugar control of patients with DFU. Telemedicine is considered a good choice to achieve this goal.
The results of this study hold significant implications for future research in telemedicine interventions. The follow-up duration across the included studies varied from three outpatient visit cycles to 12 months. Given the chronic nature of DFU, a more extended follow-up period should be considered for outcome evaluation. Diabetes foot guidelines emphasize the necessity for close interdisciplinary collaboration and the implementation of Multidisciplinary Team treatment models. 34 Teleconsultations based on mobile health care present more challenges compared to hospital-based treatments, with obstacles in technology and knowledge application. It is recommended to enhance effective communication among health care professionals, establish guidelines for telemedicine practice, and develop a multidisciplinary and multimodal telemedicine system.
Telemedicine serves roles in consultation, diagnosis, monitoring, and mentoring, with various implementation methods available. 35 This technology assists health care professionals in monitoring, educating, and managing patients with DFU, providing safe and effective foot care. Direct remote communication between patients and health care professionals may offer more immediate and real-time observations and guidance, facilitating a quicker response to the patient’s condition. In contrast, remote communication through community nurses may provide patients with more comprehensive care, as these nurses may have already conducted on-site assessments, offering a more thorough understanding of the patient’s background. The question of whether telemedicine is more advantageous between patients and experts or through community nurses merits further investigation. Consequently, it is recommended to conduct additional research to ascertain the optimal approach in this regard.
In this study, there were no differences observed in healing rate, mortality, and healing time between patients with DFU receiving telemedicine intervention and those receiving face-to-face intervention, consistent with the findings of Yammine et al. 12 However, owing to the limited data available for analysis, further research is needed before definitive conclusions can be drawn.
Several possible limitations of this study should be recognized. First, despite all 10 studies included in this systematic review being RCTs, the overall quality of the included studies was not high, which may have affected the results of the meta-analysis. This includes a lack of blinding among participants to the intervention measures, which may be inherent to the nature of such interventions. Second, for meta-analyses with fewer than 10 studies, funnel plot analysis was not conducted, potentially leaving room for publication bias. Third, there are significant variances in participant numbers and wound severity across the different studies, particularly in the interventions implemented in telemedicine versus face-to-face settings (such as video consultations, image transmission, and health education). These disparities may lead to heterogeneity and impact the reliability of the results.
In conclusion, DFU represent one of the most destructive complications of diabetes, exerting significant impacts on individuals’ physical, psychological, and familial aspects. Telemedicine interventions, facilitated through various remote monitoring technologies, apps, and social media, can enhance effective information exchange between patients and health care professionals. This approach has demonstrated the potential to reduce amputation rates, decrease costs, and better control FPG and HbA1c. These findings suggest that telemedicine interventions are worthy of promotion. However, owing to the limited number and quality of included studies, evidence regarding the effectiveness of telemedicine for patients with DFU remains insufficient, despite demonstrating its noninferiority. Clinical experts require meticulously designed, large-scale multicenter studies to explore the broader impact of telemedicine interventions on patients with DFU, including effects on quality of life, infection control, hospitalization rates, and other relevant aspects.
KEY FINDINGS
Telemedicine may be an effective intervention for patients with DFU.
Compared with face-to-face intervention, telemedicine interventions reduce amputation rates, decrease costs, and better control FPG and HbA1c.
INNOVATION
Telemedicine interventions enable health care professionals to monitor conditions of patients with DFU in real time. Through telemedicine diagnostic tools, the severity of the wound can be assessed, and personalized treatment plans can be developed. This promotes timely communication between patients and the health care team, providing patients with information and training on self-management of DFU, ultimately improving clinical outcomes. Our study indicates that telemedicine interventions reduce amputation rates, decrease costs, and better control FPG and HbA1c. It is a feasible strategy for managing DFU.
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
The study was funded by the Health Science and Technology Project of the Pudong New Area Health Commission (Grant/Award Number: PW2023A-09), the Academic Leaders Training Program of Pudong Health Bureau of Shanghai (Grant/Award Number: PWRd2022-16), Tongji University “Third Year Action Plan for Discipline Construction of School of Nursing” (Grant/Award Number: JS2210328), and Leading Talents in the Three Year Action Plan for Discipline Construction of the School of Nursing (Preparatory) at Tongji University School of Medicine (Grant/Award Number: JS2210204).
AUTHOR DISCLOSURE AND GHOSTWRITING
No competing financial interests exist. The content of this article was expressly written by the authors listed. No ghostwriters were used to write this article.
ABOUT THE AUTHORS