
Abstract
Significance:
Sterility and reduction of the bioburden are crucial for healing in chronic wounds such as diabetic foot ulcers. Although there are methods for measuring bioburdens, such as semiquantitative analysis of swab/biopsy samples, microbiological sampling, and molecular diagnostics, these tools are less accessible owing to costs or not being as quick as other methods. These methods are also dependent on clinical assessment by the clinician, and high bacterial burden may appear asymptomatic.
Recent Advances:
Autofluorescence (AF) imaging is a novel technology for identifying and quantifying chronic inhibitory bacterial load in chronic wounds. Eighty-seven percent of bacteria that frequent chronic wounds have fluorophores that fluoresce under violet light as red or cyan, depending on the type of fluorophore. Therefore, AF image-guided treatment is becoming increasingly effective for physicians to implement wound dressing changes and debridement because bacterial burdens are difficult to locate clinically.
Critical Issue:
Products such as the commercially available MolecuLight i:X and MolecuLight DX function as handheld cameras for physicians to use as a reference but require additional work to ensure that the photograph will be taken with adequate lighting.
Future Directions:
Designs for Vision Inc. introduced a device called REVEAL, an AF imaging form factor that allows the device to be worn on top of a pair of glasses, which the physician would wear intraoperatively. The benefits of this form factor include not requiring certain lighting conditions and not having to interpret the results using a handheld camera, allowing the device to be used during active surgical debridement.
Johnson V. John, PhD

David G. Armstrong, DPM, MD, PhD

SCOPE AND SIGNIFICANCE
This review focuses on the existing commercially available technologies used for autofluorescence (AF) imaging with regard to chronic wound treatment. The concepts, technological details, and clinical protocols of current handheld imaging devices are summarized. The limitations and benefits of handheld devices are discussed, with a summary of published clinical trials involving wound treatment centered on AF imaging. This review also explores the potential benefits of a new form factor in AF imaging, particularly its impact in guiding surgical debridement.
TRANSLATIONAL RELEVANCE
This article seeks to provide a new perspective on the current AF imaging devices. Assessing infection in chronic wounds was initially reliant on timely and costly laboratory work, but with the introduction of AF imaging, clinicians could guide the treatment of chronic wounds in near real time. With the overwhelmingly positive wound outcomes caused by AF imaging, incorporating it into surgical operations is the next step in improving chronic wound treatment. This transition from handheld to worn devices will facilitate the widespread use of AF imaging in debridement.
CLINICAL RELEVANCE
The introduction of a new form factor to AF-guided debridement will improve the efficiency of surgical debridement by allowing the clinician to actively visualize the bacterial burden during the operation. Future clinical trials involving the device could address the effectiveness of such a form factor, as well as the results of the chronic wound following the treatment. It is unknown whether the outcomes of using a head-mounted tool match the utility of the handheld device.
INTRODUCTION
Generally, infections caused by different opportunistic pathogens lead to amputation from chronic wounds, such as diabetic foot ulcers (DFUs). Biofilms are found in 68–100% of DFUs 1 and are the main causes of infections that lead to amputation. This makes it vital to take actions to prevent biofilm growth in a chronic wound. Early detection and appropriate treatment of DFU infection can reduce the risk of amputation by up to 72%. 2 Signs of infection in DFUs may be asymptomatic owing to neuropathy and a slowed immune response 3 ; therefore, the International Working Group on the Diabetic Foot criteria are currently poor predictors of the presence and location of bacterial loads in wounds, regardless of the number of colony-forming units per gram (CFU/g). 3 –5 In a recent study by Armstrong et al., 95% of DFUs had enough bacterial load to inhibit wound healing and application of therapies, known as chronic inhibitory bacterial load. 3,6
Microbiological methods for quantifying the bioburden in a wound include semiquantitative surface swabs and quantitative biopsies, 7,8 which can guide the surgical debridement of a wound. Swabbing the wound using the Levine technique is the most common method because of its decreased pain and cost compared with biopsies. 7 –9 However, these methods are inaccessible as point-of-care wound diagnostics, as reported days after the wound is sampled. 7,8 Owing to the sample collection protocol, the microbiological data only represent the bacteria from the center of the wound. 4 In Armstrong’s study, 84% of DFUs had bacterial loads on the periphery of the wound bed, which caused a callused ring surrounding the wound center. 3
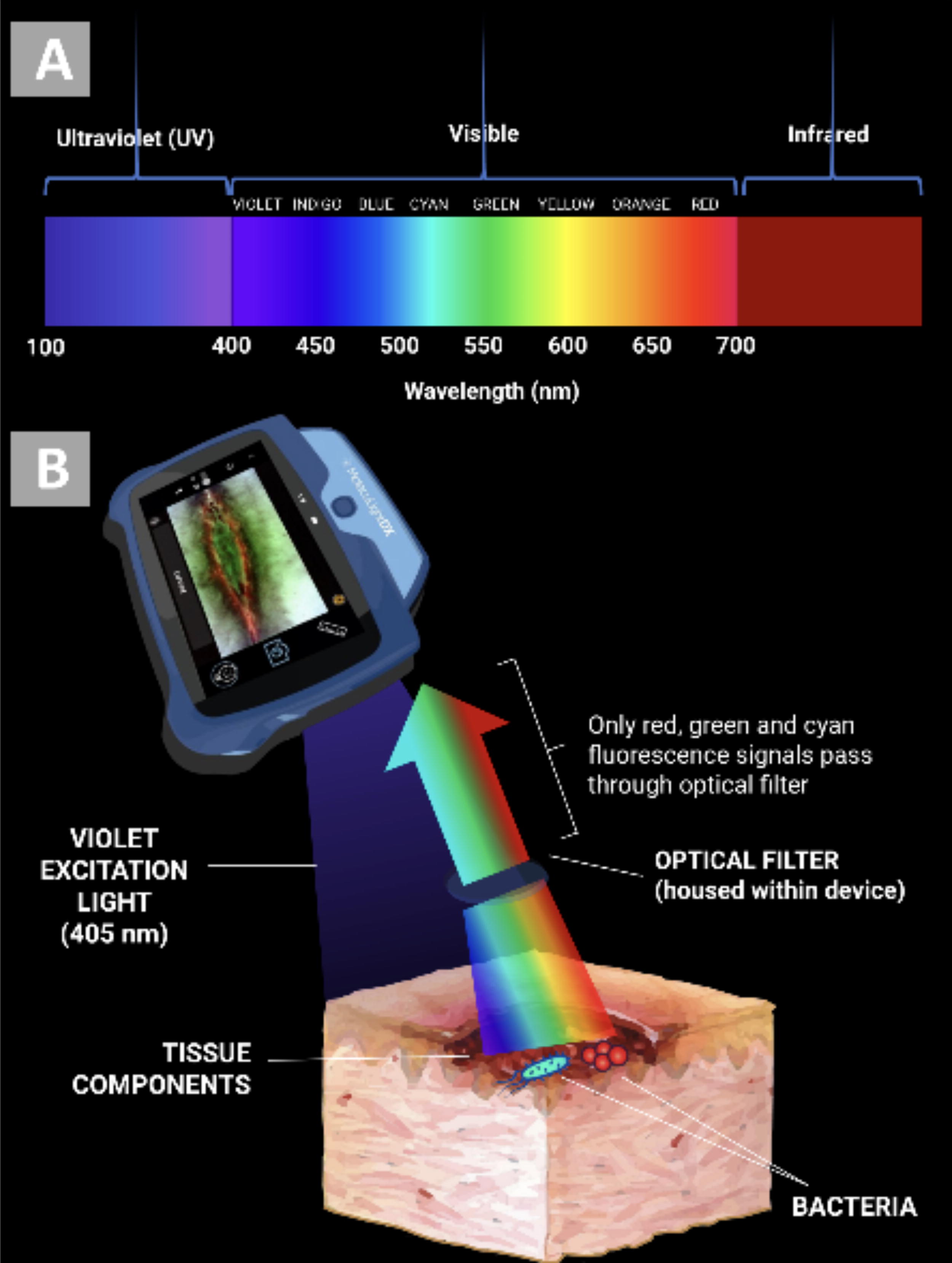
AF imaging is a technique that helps visualize areas in the wound with a high bioburden, allowing physicians to easily debride or change the dressing of infected areas. Bacterial burdens cannot be seen with the naked eye, but when bacteria in a wound exceed 104 CFU/g, the fluorophores emitted by the bacteria can be detected by the imaging device (Fig. 1).

Possible bacterial changes after debridement, as evidenced by fluorescence imaging. 1. Imaging reveals elimination of bacterial load fluorescence (FL) signals. (a) Standard (ST) image of an ankle ulcer. (b) Corresponding FL image showing areas containing high bacterial loads (red) in the periwound. (c) ST image postdebridement of ankle wound. (d) Corresponding FL image showing complete removal of the red FL signals after postdebridement. 2. Imaging reveals reduction in bacterial load FL signals. (a) ST image of a plantar DFU. (b) Corresponding FL image showing high bacterial loads (red FL) in the wound and periwound. (c) ST image after debridement of the plantar diabetic foot ulcer. (d) Corresponding FL image showing the residual red FL at the center of the wound. This indicates the need for further debridement and the use of antimicrobials. 3. Imaging postdebridement reveals deeper FL signals. (a) ST image of a diabetic foot second right toe ulcer. (b) Corresponding FL image predebridement. (c) Postdebridement FL image, removal of superficial layers of tissue reveals deeper bacterial involvement. This indicates the need for further treatment (e.g., mechanical removal and/or antimicrobials). All images are taken with the MolecuLight DX device. Images used with permission from MolecuLight, Inc. Color images are available online.
With the introduction of AF imaging, traditional methods for determining bacterial load that are time-consuming can be exchanged for a qualitative view of bacterial localization on the wound. This is potentially useful for debridement, where visualization of the bioburden would benefit the clinician before and during the operation.
METHODOLOGY
A literature review was conducted to determine how AF imaging influenced and benefited debridement and other methods of chronic wound treatment. The PubMed, Google Scholar, Ovid, and Embase databases were used. Keywords used for the search included autofluorescence imaging, MolecuLight, debridement, MolecuLight, chronic wounds, and diabetic foot ulcers. A total of 25 articles regarding AF-guided chronic wound treatment, debridement, and MolecuLight and REVEAL were considered. No studies involving MolecuLight were excluded; however, six studies were excluded, as they pertained to REVEAL being used in operations not centered on DFU care or debridement.
VISUALIZATION OF BACTERIA BY AF IMAGING
When illuminated at 405 nm (Fig. 2A) from violet-blue light-emitting diodes (LEDs), porphyrins produced by 87.5% of chronic wound pathogens 10 and pyoverdines from Pseudomonas aeruginosa would cause the wound to fluoresce red or cyan, respectively 1 (Fig. 2B). Fluorophores within the wound would excite up to a depth of 1.5 mm. 11 Under 405 nm violet light, tissues fluoresce because of red blood cells or extracellular matrix proteins such as collagen, elastin, and fibrin. The intensity and shade of the light allow it to be distinguished from bacterial fluorescence (FL), as collagen-rich tissues such as tendon or bone and high-fibrin slough tissue glow bright green to white, skin appearing less intense green (dependent on skin color, as darker skin tones absorb more violet light due to melanin), flaky skin as green with white edges, and blood appearing as a dark maroon color (Fig. 3).
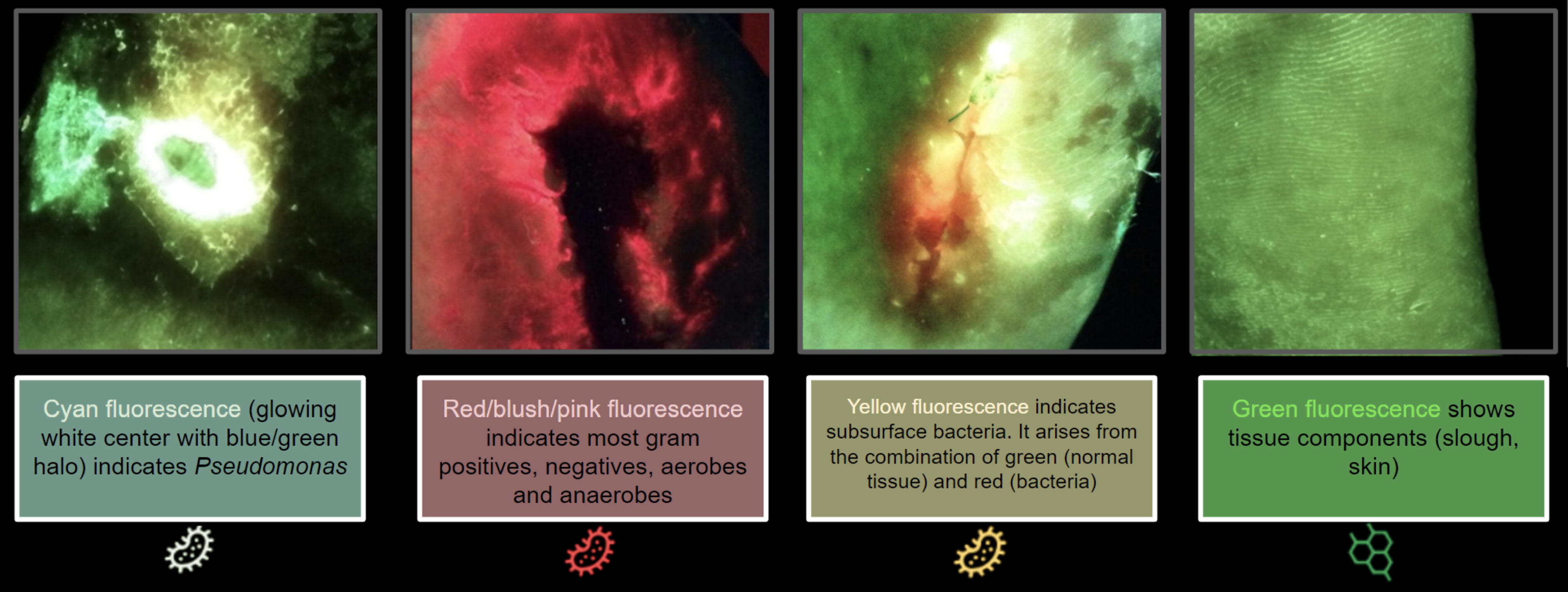
A scale of the colors produced by autofluorescence imaging. Bacteria can appear as red or cyan, whereas living tissue is generally green owing to the presence of collagen. Images used with permission from MolecuLight, Inc. Color images are available online.
IMAGING TECHNOLOGIES FOR DEBRIDEMENT
MolecuLight i:X and DX by MolecuLight Inc. are commercially available medical imaging devices that are currently used in clinical settings to locate bioburden and to assist clinicians in its elimination. MolecuLight i:X operates using a touch screen device configured with 405 nm LEDs (Fig. 4) and specialized optical filters to show only informative (red, green, and cyan) FL signals from tissue and bacteria. 2,7 The positive predictive value for red and cyan FL signals in detecting bacteria in chronic wounds is very high at 93–100%. 12 A range finder is included in the device, which confirms the appropriate distance for imaging (8–12 cm from the wound). MolecuLight i:X requires that the room be darkened, and ambient light sensors indicate when the room is appropriately dark enough for imaging to occur. If the ambient light threshold was too high for the device, drapes that arrived with the device were used. 11 MolecuLight i:X is also capable of digital planimetry for wound measurement, which would be used in ambient light.

(
In addition to its FL imaging capability, the MolecuLight DX is able to accurately measure the dimensions of chronic wounds, only without the need for calibration stickers. Wound area is auto-tracked by the MolecuLight DX and graphed over time to previous imaging sessions, which is an exceedingly valuable feature to view the evolution of the wound. 13 The DX model of the device also has more options for wound measurement settings (e.g., a variety of options for measuring length and width) and a larger screen and coregisters standard and FL images to display them side-by-side. The MolecuLight i:X and/or DX devices have regulatory clearance across North America (Food and Drug Administration and Health Canada) and Europe (Conformite Europeenne marking) and are registered throughout Asia, the Middle East, Latin America, and Australia/New Zealand.
THE USAGE OF THE IMAGING TOOLS
To use MolecuLight i:X and DX for imaging, the room must initially be darkened to as much as possible, with drapes used if the room cannot be further darkened. Wounds were imaged at a 90° angle 6 and from 8 to 12 cm (Fig. 5). After the images were captured on the camera, the fluorescent signals would be displayed on a digital touch screen and interpreted by the user. Images and videos can also be browsed in the image library and uploaded to the electronic patient records. 14
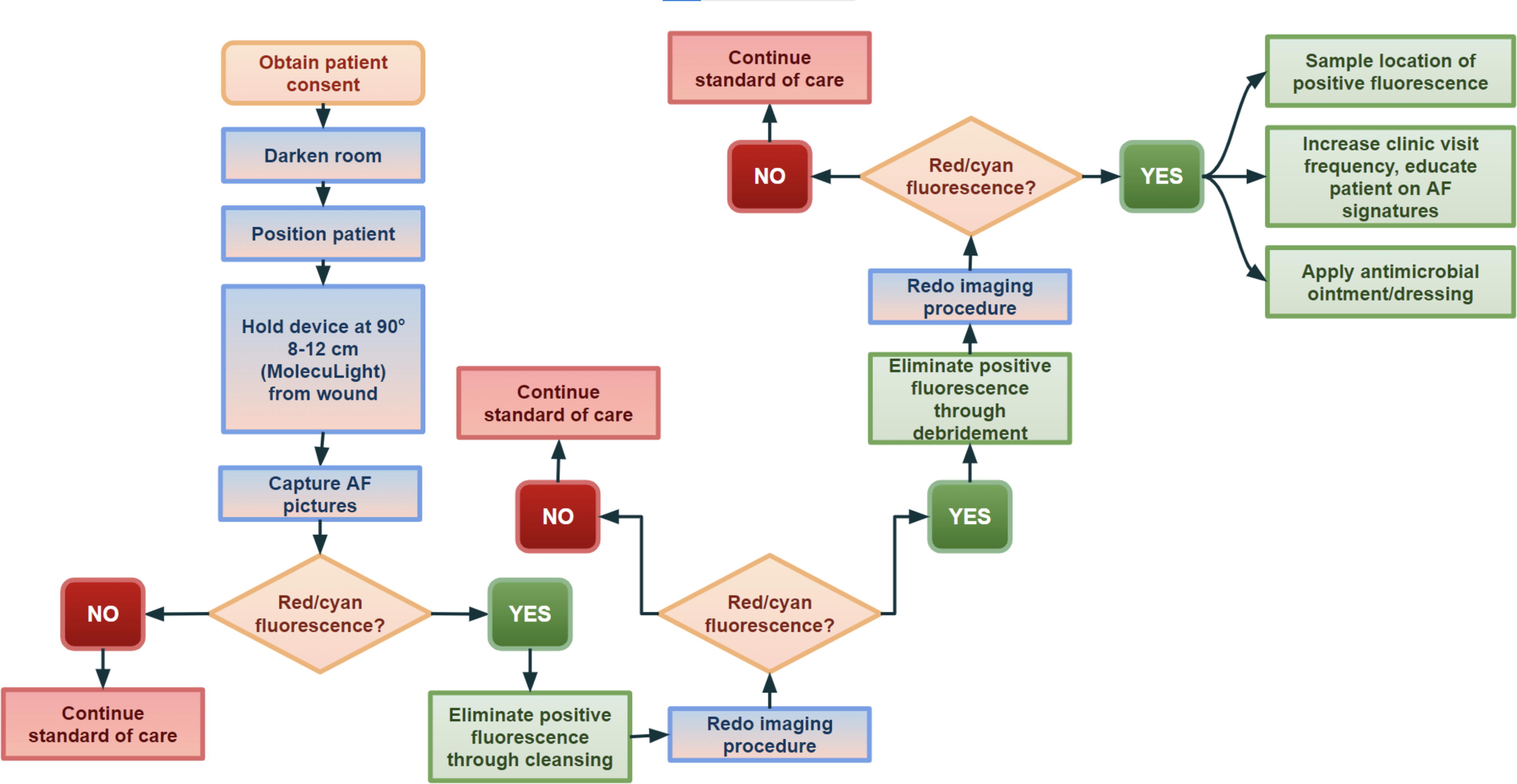
Proposed AF-guided imaging protocol, as referenced from MolecuLight i:X case studies and guidelines for fluorescence imaging by Oropallo et al. 15
SIGNIFICANCE OF IMAGING FOR BIOBURDEN REMOVAL
Detection of bioburdens using AF imaging has increased ninefold, 3 as they can detect asymptomatic infections 3,8 and can be used to guide debridement 3,8 –11,15 for chronic and burn wounds. 6 P. aeruginosa fluoresces cyan and can be used to easily detect Pseudomonas infection in a chronic wound when clinical signs are not present. 16 Many clinical studies have confirmed that FL signals can detect moderate-to-heavy loads. In previous studies, the imaging results were confirmed through microbiological testing.
In a pivotal 350-patient MolecuLight validation trial, bioburden above 104 CFU/g (clinically significant) was identified by the MolecuLight i:X device 82% of the time in the wound bed and/or periphery (p < 0.001), among a variety of chronic wound types. 16 This increased the detection of clinically significant bioburdens by fourfold (p < 0.001), as well as modified treatment plans for 69% of wounds, influenced wound bed preparation for 85% of wounds, and improved patient care by up to 90%. 16
In a 2-year retrospective analysis by Dr. Nadine Price, 17 the use of AF imaging presents economic benefits as well, as less antibiotic and antiseptic dressings were used despite a bigger number of wounds screened for (Table 1). AF imaging increased the number of wounds seen by 27% despite the expenditure of annual antimicrobial dressing decreased by 33%. In addition, using AF imaging in the study caused a 49% decrease in the prescription of antimicrobial dressings, a 33% decrease in antibiotic prescriptions, and a 23% increase in wound healing rates within 12 weeks, which is predicted to be caused by an earlier bioburden detection and intervention. 14 In retrospective, it was seen that the proportion of wounds healed by 12 weeks increased when AF imaging was added to the care. 14 A pilot randomized control study reported by Dr. Sarah et al. would also reveal that positive AF imaging led to more intervention, causing wound debridement to increase in 40.9% of cases. In contrast to 22% of patients healing within 12 weeks in the control trial, 45% of patients in the AF trial would heal within 12 weeks. 11
A table of clinical trials involving autofluorescence-guided treatment
AF, autofluorescence; DFU, diabetic foot ulcer; NPWT, negative pressure wound therapy.
LIMITATIONS OF AF-GUIDED DEBRIDEMENT
MolecuLight devices must be used in a dark room for AF imaging because light contamination can cause false positives or misinterpret FL. 16 If the room itself cannot be adequately darkened, a drape comes with a product that can be used quickly and effectively. The ambient light sensors in MolecuLight i:X and DX also let the operator know if correct light settings are reached. In addition, images must be interpreted on a color-calibrated screen, which may only be available through the imaging device as computer monitors may vary in quality. 16 FL imaging can only detect bioburdens to a depth of ∼1–1.5 mm 16 ; however, this will not be a challenge when using AF to guide debridement (Fig. 6). MolecuLight devices require specific lighting conditions to operate, which may present limitations if the devices are to be used in real time during a debridement operation.

CONCLUSIONS AND FUTURE DIRECTIONS
With MolecuLight significantly improving the treatment and outcome of chronic wounds, a new form factor used to guide debridement could further benefit the intervention against infection. Wearable AF imaging devices have been introduced as commercially available to clinicians, which proposes a new approach to the established practice of AF-guided debridement. New form factors such as wearables could address the limitations of current AF imaging form factors and provide new applications in which AF imaging could be used in the context of debridement.
In 2020, REVEAL by Designs for Vision was introduced as a device that could be used for diagnostic treatment and guidance for oral hygiene, cavity prevention, and detection of infections. 20 REVEAL is a wearable AF imaging device with glasses and magnification loupes filtered for AF use 20,21 (Fig. 7). Owing to the optical filters attached to the glasses, REVEAL does not require specific lighting conditions that MolecuLight devices need to function. A TriBeam HDiTM Headlight contains 3 LEDs that can be switched between a wide lens and two excitation settings. In addition, a wireless Bluetooth pedal can control the lighting settings for the headlights. 21

REVEAL device includes central headlight and purpose-built eyewear. Reproduced from Designs for Vision, Inc. 20
The glasses can be modified to fit the surgeon’s prescription if necessary and have a custom magnification fit to ensure that the device will not fall off or move during an operation. 21 In addition, REVEAL can be used with a 16-gigabyte camera calibrated for AF imaging, which allows for the FL from the procedure to be recorded and shown in 1,080-pixel resolution. 21 This increased mobility allows for AF imaging to be actively used during surgical debridement rather than having to interpret it on a handheld camera before the operation.
The REVEAL system cost ranges from $7,500 to $8,500. 22 As REVEAL is intended for the clinician conducting the debridement to wear it, user training can be primarily dedicated to physicians.
There are no data comparing this form factor to its handheld counterpart. Furthermore, we are unaware whether this will perform equivalently in bright light. We look forward to further data that may help confirm or refute the utility of this tool.
TAKE-HOME MESSAGES
The implementation of AF-guided clinical decisions has drastically improved chronic wound outcomes.
Other form factors for AF imaging can expand upon wound care, given the current limitations of handheld devices.
Worn AF imaging devices could be immensely helpful for demanding wound care procedures such as surgical debridement.
More clinical trials should be done to address potential complications associated with worn devices.
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
This work was partially supported by grants from the
AUTHOR DISCLOSURE AND GHOSTWRITING
There are no competing financial interests held by the authors. All the content within the review is written by the authors listed. No ghostwriters were used to write this article.
ABOUT THE AUTHORS