
Abstract
Significance:
Management of infection is a critical aspect of wound care. It involves the application of various interventions to treat the wound and prevent the infection from spreading to other parts of the body, which may lead to serious complications, including sepsis. Local treatment of skin wound infections is the favored route of administration, reducing the risk of adverse systemic effects while providing very high therapeutic concentrations at the target site. The purpose of this article was to review clinical trials from 2013 and onward, focusing on local treatment of acute wounds and burns as well as chronic wounds as their primary outcome measurement.
Recent Advances:
Based on our literature search, 49 clinical trials were focusing on treating infected chronic wounds, and 6 trials studied infection as their primary outcome in acute wounds during the last 10 years.
Critical Issues:
Currently commercially available local treatments do not prevent the onset of invasive infection. Therefore, there is a need for more effective local therapies.
Future Directions:
Despite multiple preclinical studies introducing novel and promising strategies in terms of novel antimicrobial agents and delivery methods to prevent and treat skin wound infections locally, many have yet to be tested in a clinical setting. These preclinically tested approaches could still be valuable additions to today’s care of infected skin wounds.

SCOPE AND SIGNIFICANCE
Wounds that don’t progress normally remain open and may become chronic. 1 Wound infections are the likeliest reason to cause impaired healing. If neglected they can spread from the injury site and develop deep invasive infections that are life threatening. 2 The purpose of this article is to review recent clinical trials that have focused on treating acute and chronic wound infections locally. In addition, the review addresses the importance of good wound bed preparation to prevent infection.
TRANSLATIONAL RELEVANCE
Novel and more efficient means to manage skin wound infections locally to prevent them from progressing to systemic infections causing sepsis and multiple organ dysfunction syndrome are needed. Therefore, research is being conducted to develop and test novel treatment modalities and to improve already existing products. Besides novel antimicrobial agents, current research is focusing on new delivery methods to maximize the efficacy of the agent at the injury site. 3 –5
CLINICAL RELEVANCE
Accurate and timely management of wound infections is critical. Local treatment of skin wound infections is the favored route of administration. Local drug delivery systems can be applied directly to the injured area, and their properties to release therapeutics can be tailored. Topical treatment also reduces the risk of adverse systemic effects while providing very high therapeutic concentrations at the target site. 6,7
BACKGROUND
Skin wound infections are ubiquitous and may be caused by bacteria, fungi, or viruses. Fungi and viral wound infections are rare and have a limited impact outside of burn wounds. Bacteria are the most prevalent pathogens causing wound infections, and practically all wound infection clinical trials deal with bacterial infections. Common bacteria that cause wound infections include, Staphylococcus aureus, Pseudomonas aeruginosa, Escherichia coli, Acinetobacter baumannii and Streptococcus. 8,9
Wounds become infected when pathogens enter and colonize the wound. In fact, all wounds become colonized yet only a fraction are defined as infected. 10 To determine a colony forming unit (CFU) threshold for wound infection is cumbers, but it has been shown that bacterial counts equal to or greater than 106 CFU per milliliter in wound exudate significantly increase the risk of infection. 11 In addition, earlier clinical studies from our institute (U.S. Army Institute of Surgical Research) have shown that wounds with greater than 105 CFU per gram of wound tissue did not heal, whereas wounds with fewer than 105 CFU per gram closed successfully. 12
Ordinary symptoms of wound infection include pus, spreading redness, increased pain or swelling, and fever. 13 However, if the treatment of the local infection is overlooked, it can progress to a life-threatening systemic infection causing sepsis and multiple organ dysfunction syndrome. 14 Wound infections also prolong inflammation that results in delayed wound healing. The basic pathophysiology of wound infection involves the manipulation of the host inflammatory response. 15 In the inflammation phase of wound healing, granulocytes clear the wound by removing contaminating microorganisms. However, incomplete microbial clearance leads to prolonged inflammation that impairs healing. The presence of microbes and endotoxins in the wound increases pro-inflammatory cytokines such as interleukins (ILs) and tumor necrosis factor alpha (TNFa). Furthermore, the prolonged inflammation increases the extracellular matrix degrading matrix metalloproteases in the wound bed. 16 The inability of the host immune system to dampen the inflammatory response due to infection delays wound healing. The prolonged inflammation prevents the wounds from progressing to the proliferative phase of healing, delaying re-epithelialization and predisposing the wound to become chronic. 17,18
Sometimes, the bacteria in the wound can form biofilms, which help them adhere to the wound surface and make eradication difficult. Biofilms that are formed by multiple pathogens are one of the most important underlying contributors to the difficult-to-heal or chronic wounds. A biofilm is an extracellular polymeric substance that allows exponentially increased antimicrobial resistance compared to planktonic microbes—or those in their free-living state. 19,20 Biofilms confer bacteria protection from host defense mechanisms as well as antimicrobials and help facilitate the uptake of nutrients and the removal of metabolic products. It allows gene transfer and gene expression regulation that would otherwise not take place without a biofilm. Furthermore, a polymicrobial environment within a biofilm contributes to a synergy that can promote a non-virulent bacterial species to become virulent and cause further damage to the wound or the host. 19,21,22
According to the Center for Disease Control and Prevention and National Health Institute, about 65% to 80% of bacterial infectious diseases are caused by biofilm-producing bacteria, and several studies in the military have demonstrated chronic wounds to be affected by biofilms in 60% to 80% of cases. 20,23 Biofilms have a profound impact on the survival of the bacteria within them and the development and persistence of difficult-to-treat chronic wounds. They can act as a diffusion barrier against foreign molecules (e.g., host defense mechanisms, antimicrobials), promote nutritional limitation, and optimize general stress mechanisms that confer physiological changes within the bacterial colonies that offer protection from environmental stresses, facilitate quorum sensing to synchronize gene expression, and maintain an optimal environment for bacterial proliferation—all of which contribute to recalcitrant wound healing. The production of destructive enzymes and toxins by the bacteria alongside a hyperinflammatory state (locally and in some cases systemically) creates an imbalance in host defense systems that ultimately favors bacterial physiological processes. 19
Recognizing the presence of a biofilm is of paramount importance when treating a nonhealing or difficult-to-treat wound. Unfortunately, however, there currently aren’t standardized, widespread, economical, and easy-to-use methods for detecting biofilm presence within a wound bed. The physical exam findings that many use to assume biofilm presence—other than a persistent, nonhealing wound—are rather nonspecific: a slimy/sticky, shiny layer atop the wound bed that can rapidly redevelop after removal. 19 Culture swabs may be falsely negative for classical biofilm-producing bacteria (Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, among others), and there is no readily available biomarker test that is routinely performed that can accurately diagnose presence of a biofilm. 22,24 There does exist genetic testing of biofilm biomarkers (surface proteins involved in biofilm formation) such as extracellular polymeric substances (EPS) and cellulose, but this is not implemented into standard practice. 24 –26 There are other methods and imaging technologies that are available or being studied that can aid with biofilm testing such as crystal violet assays and transepidermal water loss detection devices, but again this is not standard practice. 22 In a research setting, or specific clinical settings, scanning electron microscopy has been widely acknowledged to diagnose biofilms but again, this is not routinely used in the clinical setting. 20 Due to the lack of a standardized, widely available diagnostic approach, many clinicians will simply assume a biofilm is present if they face a difficult-to-treat, persistent, or worsening wound.
Treatment of a biofilm consists of varying approaches that have largely been studied in case series and retrospective studies. The presence of multiple well-performed prospective, randomized controlled trials is lacking for the many different treatments that exist. As outlined by Sen et al (2021) in their modified representation of levels of evidence in the context of antibiofilm strategies, they did not find any Level 1 (at least 3 good randomized controlled trials (RCT)) or any Level 2 (1 well designed RCT or multisite study) studies; the majority were categorized as Level 3 (few clinical studies). 20 Their review evaluated published studies examining traditional and nontraditional strategies including debridement, ultrasound debridement, maggot therapy, nonthermal plasma, photodynamic therapy, nanomaterials, silver-based treatments, iodine-based treatments, hypochlorous acid, manuka honey, quorum sensing inhibitors, electroceuticals, phage therapy, probiotics, antimicrobial peptides (AMPs), dispersal agents, and various biofilm life-cycle inhibitors. 19,20,22 Despite the many avenues that exist within the anti-biofilm armamentarium, debridement appears to remain a consistent and reliable approach for the treatment and eradication of a biofilm and its associated bacteria. Removal of necrotic or nonviable tissue to a region of healthy, beefy granulation tissue to allow for a new, fresh wound bed that can benefit from effective topical antimicrobials and cleansing solutions may afford a previously difficult-to-treat wound the opportunity for improved healing. In fact, this method is a mainstay in wound bed preparation. 27
Often wound infections are treated with systemic antibiotics, and sometimes surgical intervention is needed to clean the wound from the infected tissue. Local delivery of antimicrobials to treat and prevent wound infections is an attractive approach since it maximizes the effect at the target site minimizing systemic toxicity. Multiple antimicrobial agents and antisepsis strategies have been used to prevent and treat wound infection. 4,28,29 The purpose of this review article is to focus on novel local treatments in the management of infected traumatic wounds, burns, and chronic wounds.
DISCUSSION
Though surgical debridement is often considered a definitive treatment for an infected wound, it may not always be the optimal approach for a particular wound or patient. Local treatment of infected wounds remains of paramount importance in addition to debridement, especially in those who may not be appropriate for surgery. 13 Topical treatments for infected wounds remain vast; interestingly, despite introductions of new products and dressings, older products such as chlorhexidine, iodine-based solutions, honey, silver sulfadiazine, and topical antibiotics (e.g., bacitracin, mafenide acetate) continue to be used. 5
In this section, we will first discuss about the importance of good wound bed preparation to prevent infection. Subsequently, we have reviewed clinical trials from the last ten years with the main focus on treating wound infections locally. The literature search was performed using all available databases and google, using keywords wound infection, local treatment, topical treatment, clinical trial. Only peer reviewed published studies with wound infection as their primary outcome measurement were included. Studies that did directly measure infection or were published in another language but English were excluded. The trials are divided into clinical studies on infected acute wounds and infected chronic wounds. Some clinical trials are using therapeutics that are not yet commercially available. The studies have been summarized in Tables 1 and 2.
Summary of the infected chronic wound clinical trials focusing on local antimicrobial treatments
In total 49 studies are described from 2013 to 2024.
EGF, Epidermal growth factor; bFGF, basic fibroblast growth factor; Peceleganan, PL-5; SOC, Standard of care.
Summary of the infected acute wound clinical focusing on local antimicrobial treatments
In total 6 studies are described from 2012 to 2024.
AEs, Adverse Events; ALA-PDT, Aminolevulinic acid – Photodynamic Therapy; DFU, Diabetic foot ulcers; N/R, Not recorded; PMMA, Poly (methyl methylacrylate); SOC, Standard of care.
Wound bed preparation
Appropriate wound bed preparation is critical to the success of healing a wound. Whether it be an acute wound in an otherwise healthy patient who does not need significant intervention or a chronic wound in a patient with predisposing comorbidities leading to a decreased likelihood of healing, a systematic, protocolized approach that focuses on wound assessment, patient assessment, treatment, and re-assessment creates the foundation of wound care. Taking such an approach facilitates optimal wound healing both endogenously and using other therapeutic measures. 85
While many hospitals and programs have developed their own structured approach to wound care, there have been several protocolized approaches that have been well published. One such method is the “Wound Bed Preparation” approach that was first published in 2000 and has since undergone several updates, most recently in 2021. This approach breaks down wound care and wound bed preparation into 10 separate statements, each containing several components that are necessary to address in order to optimize the chance of a wound healing. These statements center around (1) treating the underlying cause and ensuring adequate blood supply; (2) patient centered concerns; (3) determination of the ability or likelihood to heal; (4) local wound care consisting of wound documentation, wound cleansing and reassessment; (5) debridement and pain control; (6) control and treatment of infection and inflammation; (7) moisture management; (8) evaluation of rate of healing; (9) edge effect; and (10) organizational support. Each update since its initial publication has offered more nuanced strategies that may be more widely available or easier to learn than previous recommendations (e.g., use of a handheld doppler for distal vasculature for a quick clinical assessment of arterial supply) alongside a more patient-centered approach to fully understand all components that contribute to a difficult wound. 86
Another systematic approach that has been well published and implemented in various health systems is the TIMERS framework recently revised in 2019: tissue management, inflammation and infection, moisture balance, edge/epithelial advancement, regeneration and repair, and social factors. 87 Similarly to the “Wound Bed Preparation” algorithm, this system prioritizes wound characterization, patient assessment, and local wound care involving tissue management, inflammation, infection, and moisture control. Of significant in both approaches is the emphasis on re-assessment, which allows for the clinician to modify treatment strategies if healing has stalled. In either model, individualization of every wound is best to ensure steps are not missed or inadvertently disregarded in the overall treatment. Hard-to-heal wounds are unlikely to respond in a clinically significant way until patient comorbidities (e.g., peripheral vascular disease), wound features (e.g., biofilm), and other risk factors are appropriately diagnosed and addressed first. 88
Approaching a difficult-to-heal wound requires a holistic approach with appropriate and timely diagnosis, assessment, treatment, re-evaluation, and frequent follow-up. While there are many products on the market that can be used in wound care, having an understanding of what should comprise a basic wound toolkit is critical. 89 Antiseptic and saline solutions, cleansing solutions, dressings, negative pressure therapy options, local antimicrobials, and debridement options comprise the foundation for adequately addressing a wound. Knowing which specific products within each component (e.g., hydrogel dressings, hydrocolloids, silver dressings, hypochlorous acid) should be applied to the wound being evaluated will depend on the specific characteristics and scenario in which the wound presents. 90
Acute wounds and burns
Mismanagement of acute wounds may result in infection leading to poor healing outcomes and prolonged hospital stays. Especially, significant traumatic and thermal injuries induce a state of immunosuppression that predisposes patients to infections. Furthermore, the longer the injury stays untreated the greater the risk of infection. 91 Here, clinical trials focusing on managing wound infections in traumatic wounds including burns have been reviewed (Table 2). The search criteria used was (acute wound) OR (burn) OR (traumatic wound) AND (infection OR infected) OR (biofilm) OR (wound preparation) AND (local therapy) OR (topical therapy) OR (debridement) OR (novel therapeutics) AND (clinical trial) OR (clinical study) on PubMed® and Google Scholar™. Studies involving negative pressure wound therapy (NPWT) were excluded from the review, since its involvement complicates the evaluation of the efficacy of the therapeutics. In addition, studies were excluded if they were in a language other than English, were nonhuman animal studies, were single-patient case studies, only involved ophthalmical, oral, or intra-abdominal injuries, or if the studies did not specifically address infection or biofilm in some way. The literature search demonstrated that there are only few studies on acute wounds that have infections as their primary end point since most of the acute wound clinical trials focus on healing outcomes instead. Figure 1A shows how the studies have divided into different treatment modalities, and Figure 2 contains representative images of infected acute wounds.

The pie charts depict how the performed clinical trials have divided into different local treatment modalities.
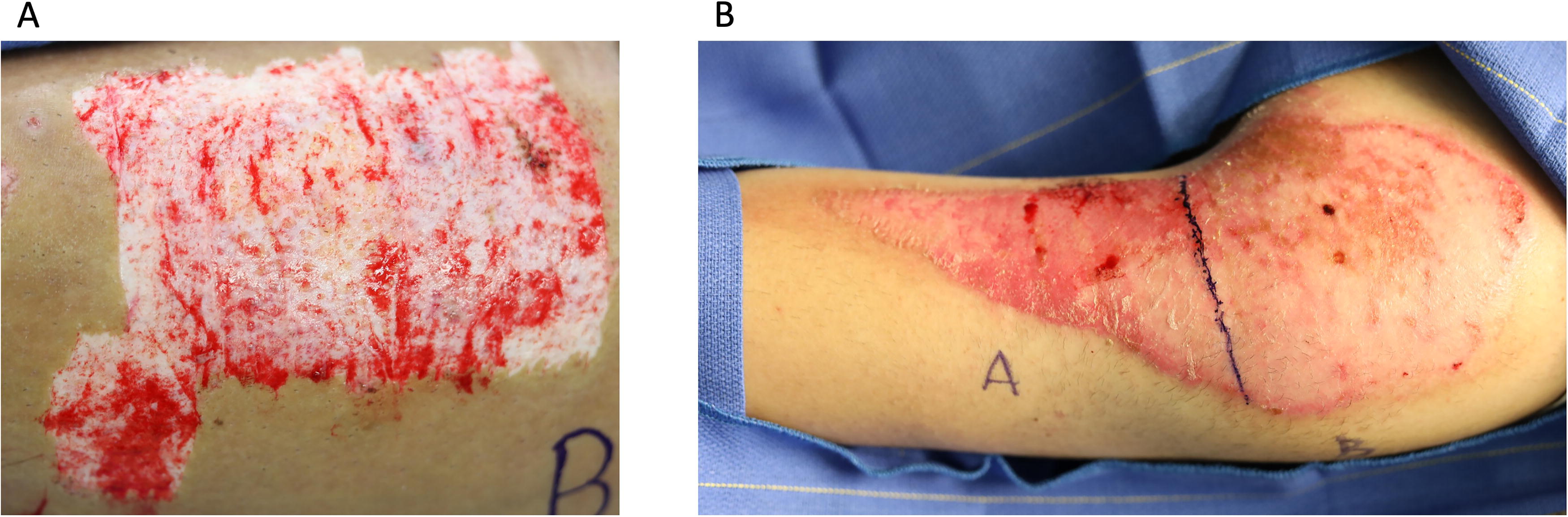
Representative images of infected acute wounds.
Ionic therapies
While silver sulfadiazine and other silver based topical treatments have remained the standard of care (SOC) treatment for many wound and burn infections, ionic therapy has evolved to include silver impregnated dressings, hydrofiber, and hydrogel dressings that incorporate ionic properties and sustained ion (e.g., silver) release to treat infection. 30,90,92 Aquacel-Ag, for example, is a hydrofiber dressing that retains moisture for a better wound healing environment while allowing continual release of silver into the wound bed. 93 Hydrogel based dressings absorb water, are permeable to oxygen and nutrients, dissolve slowly, and also allow for a continual release of medication into the wound. Hydrogels have the added benefit of being prepared in various fashions to create targeted antimicrobial dressings. 94 Eisenbeiß et al. (2012) compared an Octenidine hydrogel with a standard hydrogel in the treatment of burns and found that microbial wound colonization was significantly lower in the antimicrobial hydrogel group. Additionally, the treatment group did not have statistically significant wound healing impairment when compared to the control group. 95 There are numerous products that incorporate this technology, and many studies and meta-analyses have been performed to evaluate their efficacy compared to standard therapies. 31
Antimicrobial peptides
Antimicrobial peptides (AMPs) are a fundamental part of the innate immune response system and are responsible for eliminating pathological microorganisms within the host. They help promote production of antigen presenting cells and phagocytosis of these microorganisms and otherwise play a critical role in host defense and inflammatory signaling modulation. 32 AMPs are widely found in nature and can be isolated and engineered to combat wound infections; however, despite this, translation of topical AMP formulations into the clinical world remains poor. 96 In review of the literature, there appears to be a single, recent, multicenter, open-label randomized, controlled clinical trial using topical AMPs. Wei et al. (2023) compared the use of various concentrations (1%, 2%, and 5%) of an AMP topical spray (Peceleganan, PL-5) to standard topical 1% silver sulfadiazine in patients with skin wound infections. PL-5 is a chemically synthesized α-helical AMP containing 26 amino acid residues. In preclinical studies, it has shown a stronger and broader spectrum of antibacterial activities against both Gram-positive and Gram-negative bacteria in comparison to conventional antibiotics. Patients underwent daily dressing changes with interval wound swab collections for 7 days. Subjectively, it was noted that some of the wounds dressed with PL-5 demonstrated a decrease in exudate, purulence, erythema, inflammation, and edema; however, there was no statistically significant difference between any of the groups in regards to overall clinical efficacy (to include pathogen clearance, recurrence, and superinfection). 33 A separate 2022 meta-analysis of 5 Western studies and 11 non-Western studies evaluated Polymyxin-B ointment, another topical AMP to SOC for burn wounds. Few studies within the meta-analysis assessed bacterial count, but the pooled results demonstrated improved bacterial elimination with a risk ratio of 3.93 (95% CI: 2.28–6.79, p < 0.001), and 2 studies demonstrated a faster time to a clean wound bed by of 6 days (p = 0.0012). 97
The successful translation into clinical research and practice has been unfortunately impacted by ineffectiveness, AMP cytotoxicity (e.g., nephro- and neurotoxicity with polymyxins) and financial disadvantage. 32 As such, no new AMP has been FDA-approved for clinical use as an antimicrobial since Daptomycin in 2003, which does not come in topical form. 34 Despite this, the realm of AMP research still sounds promising as these peptides can be endowed with powerful antibacterial, antiviral, and antifungal properties that may provide improved antimicrobial coverage during a time of increased antibiotic resistance.
Electroceutical treatment
Wireless electroceutical dressings (WEDs) are a relatively recent development in wound care that has been demonstrated to prevent and disrupt biofilm infection. 98 These dressings work by ions—usually silver and zinc—to induce superoxide anion radical formation via an electrical field that disrupts bacterial growth. They are disposable, easily transportable, and do not require an external power supply. Furthermore, electroceutical dressings should not succumb to bacterial resistance. 35 Procellera, for example, is a woven fabric bandage with microelectrodes and microdeposits of silver and zinc ions that generate superoxides to facilitate destruction of pathogens. In a prospective, randomized, controlled single center trial, WED was compared to SOC therapies for burn wounds and evaluated for biofilm and bacteriological analysis. At the time of dressing removal, there was a statistically significant decrease in biofilm score in 48% of the patients in the WED group compared to only 28% of the patients in the SOC group. No significant differences were observed in terms of overall wound healing and quality of healing, meaning that the WED-treated wounds performed just as well as the SOC in this regard. 98 A separate prospective randomized controlled clinical study using Procellera against SOC for blister treatment in Rangers was unable to conduct a statistical analysis for wound bioburden at the conclusion of the study, but did not demonstrate inferiority in wound healing compared to SOC. 99 Despite the current overall lack of clinical trials in support of WED therapy, further research needs to be performed to take advantage of a potentially affordable, logistically easy, and low risk treatment option for wound infections.
Phage dressings
Bacteriophages are species-specific viruses that infect and replicate within bacterial cells. While phages may be responsible for encoding pathogenic toxins and horizontal gene transfer between bacteria, their ability to infect and multiply within a bacterium and cause its destruction has raised interest in its use as an antimicrobial agent. 100 In 2010, the PhagoBurn randomized controlled trial set to investigate the efficacy and tolerability of a bacteriophage cocktail against burn wounds infected with Pseudomonas aeruginosa when compared to SOC, silver sulfadiazine. Unfortunately, this trial was stopped short due to the insufficient efficacy of the phage dressing as displayed by a significant delay in achieving the primary end point—sustained reduction in bacterial burden. Patients with the SOC silver sulfadiazine dressing achieved this endpoint in 4 days, whereas the treatment group took 12 day to achieve the same effect. 101 It is worth noting, however, that due to unexpected effects of manufacturing on the density of the phages within the dressing, the actual phage concentration was found to be 103 lower than intended and could potentially have negatively impacted the dressing’s efficacy. While clinical research in the world of phage therapy for wound and burn infections remains quite limited, further investigation is warranted.
Chronic wounds
There is a paucity of studies directly measuring infection status/bacterial burden in chronic wounds. Most studies focus on the healing outcomes of various interventions. However, we have chosen to limit the scope of this section to those studies that directly address the status of microbial burden in these hard-to-heal wounds. The search criteria used were (chronic wound) OR (ulcer) OR (hard-to-heal wound) AND (infection OR infected) AND (local therapy) OR (topical therapy) AND (clinical trial) OR (clinical study) on PubMed® and Google Scholar™. Like in the Acute Wounds and Burns section, the studies in a language other than English, animal studies, single-patient case studies, corneal ulcers (e.g., keratitis), apthous ulcers, sexually transmitted infections, osteomyelitis, leprosy, NPWT studies, and the studies that did not directly address infection in some way were excluded. Thus, we found 49 clinical trials that matched these criteria (Table 2). Figure 1B shows how the studies have divided into different treatment modalities, and Figure 3 contains representative images of infected chronic wounds.

Representative images of infected chronic wounds.
Impregnated dressings
Various therapy-impregnated dressings have been tested to improve outcomes in chronic wounds. Octenidine is commonly used as an antiseptic effective against gram-negative and gram-positive microbes. 36 It has been incorporated into an absorbent dressing that showed a similar reduction in bacterial burden to a silver dressing, showing promise to reduce clinical costs. 37 However, a foam dressing containing povidone-iodine (PI) did not perform better than a placebo dressing in a study of 71 patients. 38 Recent studies of silver-impregnated dressings showed within-patient reductions in bacterial burden. 39 –43 Manuka honey dressings have been shown to perform similarly to silver dressings and improve healing outcomes. 44 –46 In a prospective, randomized controlled trial of 79 patients, a chitosan fiber-based dressing showed significantly improved healing outcomes in nonhealing chronic wounds compared to the SOC. 47 Finally, Stryja et al. (2023) demonstrated that a dressing impregnated with octenidine with hylaluron lowered infection similar to a silver dressing but had significantly greater reduction in wound size. 48 Dialkylcarbamoyl chloride (DACC) coated dressings’ fibers are covered with a hydrophobic derivative of fatty acids that physically binds several kinds of bacteria which are removed when the dressing is changed. Two trials investigated the ability of DACC dressings to improve infection outcomes. Malone et al. (2023) showed that biofilms adhered to the DACC dressings in a proof-of-concept study. 49 In a 40 patient, randomized controlled trial, DACC dressings significantly lowered bacterial burdens in infected leg ulcers when compared to a silver dressing. 50
Local irrigation
Wound care and cleansing are the critical parts of chronic wound management. In the last decade, five clinical trials have compared the effectiveness of treatments to irrigation with sterile saline. In a prospective cohort study of 260 patients, various wound irrigants and antiseptic solutions reduced bacterial burdens, leading the authors to recommend their use in chronic wounds. 51 Polyhexamethyle biguanide (PHMB) binds to bacterial plasma membranes, increasing its permeability, losing low-molecular-weight solutes, and finally rupturing the membrane and killing the microbe. 52 Two randomized controlled trials, however, showed that PHMB did not significantly reduce bacterial burden in venous leg ulcers and hard-to-heal cardiac surgical wounds. 52,53 However, sodium hypochlorite was shown to reduce bacterial burden and promote healing in a small trial of 16 patients. 54 A double-blinded trial with 54 patients investigated the efficacy of a novel antibiofilm cleanser and gel to reduce bacterial load in the treatment of hard-to-heal wounds. The solution contains surfactant and ethylenediaminetetraacetic acid (EDTA) to disrupt the biofilm and PHMB to kill the bacteria. It was used to cleanse wounds following debridement, followed by application of an antimicrobial hydrogel. The study showed that the treatment lowered bacterial burden compared to placebo in a prospective, randomized controlled trial. 55
Photodynamic therapy (PDT)
Microbial and fungal infections can be susceptible to reactive oxygen species. 56 However, delivery of these chemicals in vivo can be difficult. One method of delivery is to apply precursor chemicals in hydrogels to the wound after inundating the wound and penetrating the biofilm, and activate them with visible light, often red light at 620 ηm. 57,58 A trial involving 32 patients showed that PDT significantly decreased bacterial burden in infected foot ulcers and improved healing outcomes. 58 A pair of studies indicated that photo-activated δ-Aminolevulinic acid significantly reduced microbial levals and improved healing outcomes in chronic ulcers. 57 Mannucci et al. (2014) in a prospective randomized controlled trial of 62 patients, tested 3 doses of a cationic zinc phthalocyanine derivative, activated by red light and showed that the 2 most concentrated doses significantly reduced microbial load in diabetic foot ulcers. 59
Resorbable materials
Several studies have investigated the effect of resorbable materials on chronic wounds (Fig. 1C, Table 2). Chloramine hydrogel and pirfenidone hydrogel did not perform better than SOC in diabetic ulcers. 60,61 Three studies evaluated ALCS in treating chronic wounds, but none showed statistically significant improvement compared to SOC or placebo controls. 62 –64 A biofilm disrupting hydrogel has been developed that combines a pH buffer system of an acid and its conjugate base with the surfactant benzakonium chloride. The components disrupt biofilms’ EPS and lyse the cells. 102 Two randomized, controlled trials showed that this biofilm targeting gel significantly reduced wound size in recalcitrant wounds. 65,66
Topical application of therapy
Eighteen studies investigated the effects of direct application of topical therapies to chronic wounds (Fig. 1B, Table 2). In a randomized, controlled trial of 90 patients, mupirocin combined with sulfacrylate in an ointment saw similar decreases in infection to mupirocin ointment, but the combination treatment showed significantly greater wound healing in chronic skin ulcers. 67 Cadexomer consists of small polysaccharide beads that, when combined with 0.9% iodine, have been shown to reduce microbial burden. In a trial of 18 patients, it was shown that treating thrice weekly with cadexomer iodine (CI) for 2 weeks or 6 weeks resulted in similar bacterial levels. 68 Raju et al. showed that there was no difference in CI powder or ointment on bacterial levels; rather, any form of CI significantly reduced infection compared to SOC alone. 69 Buzzi et al. showed that hydroglycolic extract from marigolds (Callendula officnalis) improved bioburden and wound odor in Diabetic foot ulcers (DFUs). 70 Similarly, in another study by Henshaw et al (2014), it was shown that beehive propolis reduced bioburden in DFUs, although not significantly. 71 Silver sulfadiazine combined with cerium nitrate significantly lowered infection rates in patients with ischemic necrosis of the leg and foot. 72 Otaviano et al. evaluated the effect of Topical Oxygen Jet Therapy (TOJT) on infected, chronic surgical wounds. TOJT involves applying gaseous oxygen directly to the wound, and in a randomized, controlled trial of 73 patients, TOJT was comparable to the SOC alone, in terms of bacterial burden. 73 Seven clinical trials investigated how Cold Atmospheric Plasma (CAP) would affect hard-to-heal wounds (Table 2). CAP is an ionized gas (plasma) that generates reactive oxygen and nitrogen species, along with some visible, ultraviolet, and infrared radiation. These qualities render it capable of disrupting and destroying microbes. 74 Two trials showed that CAP was equally effective as the SOC. 75,76 A pilot study showed that CAP was less effective than SOC. 77 However, five studies showed that CAP lowered bacterial burden and improved healing outcomes in ulcers. 78 –80 The Platform Wound Device (PWD) that is a treatment platform that protects wounds and allows for precise topical delivery of drugs such as analgesics and antibiotics. 4 In a prospective, RCT of 45 patients, the PWD was utilized to deliver gentamicin cream to treat different ulcers. The treatment decreased both inflammation and bacterial growth but no significant differences to the SoC were observed. 81 Pravibismane (MicroBion Corp.) is a novel small molecule drug that disrupts microbial bioenergetics by reduing adenosine triphosphate concentrations in biofilm and planktonic bacteria. In a phase 1b, randomized controlled trial of infected DFUs, pravibismane was shown to be safe, and it lowered reinfections and reduced ulcer size, though those results were not significant in this early phase study. 82 One clinical trial tested the efficacy of AMPs on infected chronic wounds. LL-37, the active form of the cathelicidin AMP, was loaded into a cream and applied to infected DFUs in a prospective RCT of 25 patients. The cream enhanced healing in mildly infected DFUs, but it did not significantly decrease aerobic bacteria colonization of wounds on near-term follow-up visits. 83 Poly (methyl methylacrylate) (PMMA) is primarily used in orthopedics as an anchoring material in arthroplasties and osteoplasties, filling free spaces and providing structural support. 103 PMMA is a solid, rigid material formed by combining a polymer powder and a monomer liquid. Antibiotics have been loaded into the powder form to combat infections since the 1970s. 104 In a retrospective review, infected DFUs were debrided and treated with PMMA loaded with vancomycin and gentamicin or covered with gauze. Patients treated with antibiotic-loaded PMMA showed significantly lowered healing duration and frequency of follow-up debridement. 84
SUMMARY
Effective wound bed preparation is essential to prevent infection, and management of infection is vital to prevent serious complications, promote wound healing, and improve long-term healing outcomes. Antimicrobial resistance and the presence of multidrug-resistant organisms complicate treatment as only limited options are currently available for effective therapy. 22,105 Biofilm formation is another major challenge, and their eradication is very difficult due to decreased antibiotic susceptibility. 106
In this article, published clinical trials since 2013 focusing on local treatment of wound infection were reviewed (Tables 1 and 2). The trials were divided into traumatic and chronic wound infections. Significantly more clinical trials over past 10 years have focused on the treatment of infection in chronic wounds (49) than in acute wounds (6). The literature search also indicated that local treatments for infected wounds remain vast, and most of the clinical trials utilize different antimicrobial agents combined with a biomaterial (Fig. 1). Commonly used agents include different antibiotics, silver, chlorhexidine, and iodine-based solutions. 105 The more recent treatments with antimicrobial agents involve the use of bacteriophages and antimicrobial peptides. These various agents can be embedded in wound dressings and scaffolds or formulated in hydrogels, creams, and ointments. 100,107 Most of the trials compared novel treatment modalities to current standard of care (SoC) treatments and in general the main finding was that they were not significantly better than the current SoC treatments.
As noted in this review, there is a dearth of full clinical studies of local therapies to reduce infection in wounds. On the contrary, there are myriad of basic science and preclinical studies investigating potential treatments to mitigate this issue. 108,109 This is a pressing problem throughout biomedical research; there is a significant gap between the lab bench and the patient’s bedside. 110 In drug development, 90% of potential therapeutics fail to reach patients, and those that do take an average of 10–15 years to be fully approved. 111 Research funding for wound care has been a consistent challenge; although 0.9% of health costs in the United States were related to chronic wounds, only 0.1% of National Health Institute funded research projects focused on cutaneous wounds. 112 Lyme disease research accounted for more research funding than chronic cutaneous wounds in 2016 despite having a tenfold higher burden on the U.S. healthcare system. 113 Additionally, despite the significant market for wound care, perhaps surpassing $30B by 2030, the cost/benefit ratio can be unattractive for healthcare systems and capital investment. 108,112 Navigating the regulatory environment alongside developing new treatments is another major stumbling block. For example, regulators may require the team developing a novel wound dressing to characterize both the therapeutic drug as well as changes to the structure of the said dressing, adding significant costs. 109 These potential pitfalls, combined with the incredible complexity of wounds, make developing new products an inherently expensive and time-consuming process. Single molecule cancer treatments cost billions to develop and have an only 5% success rate. 114 It is no surprise that venture capital and pharmaceutical companies are reticent to invest. 109,114 Without buy-in from these “power players,” it is unlikely that governmental organizations will shift funding toward wound care research in any meaningful way. Further, our animal models of wound healing face limitations when attempting to bring new therapies to patients. Chronic wounds are especially difficult to model in lab animals. 108 These matters should be taken into consideration when initiating projects. An ongoing challenge is the integration a vast, multidisciplinary team of basic scientists, translational scientists, Good Laboratory Practice (GLP) and Good Manufacturing Practice experts, clinicians, statisticians, public health professionals, capital investors, legal experts, clinical trial professionals, and politicians. Coordinating and achieving buy-in from this diverse group to successfully launch a new therapy may be the biggest ongoing hurdle. 108,110 Successful project coordination and management is critical to unclogging the bench-to-bedside pipeline. 110 Future studies must harness the power of high-throughput screening to harness a multi-omic technologies to screen biomarkers, drug sensitivity/toxicity, integrate advanced noninvasive imaging, and make clinical predictions. 108,110
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
No funding was received to support this work. Kristin Anselmo, RN, Victoria Diaz, RN and Rodney Chan, MD are thanked for providing images for Figures 2 and ![]() .
.
AUTHOR DISCLOSURE AND GHOSTWRITING
The views expressed in this article are those of the author(s) and do not reflect the official policy or position of the U.S. Army Medical Department, Department of the Army, DOD, or the U.S. Government. The authors declare no conflict of interests. No ghostwriters were involved in the writing of this article.
ABOUT THE AUTHORS