
Abstract
Objective:
To evaluate the clinical efficacy of combining an offloading device with a contralateral shoe lift to compensate for induced limb-length discrepancies in participants with plantar diabetes-related foot ulcers.
Approach:
Between March 2021 and December 2023, 42 consecutive patients with active plantar diabetic foot ulcers (DFUs) were randomly assigned (1:1) to the treatment group (limb-length discrepancy compensation with a shoe lift in the therapeutic footwear of the contralateral limb) or a control group that did not receive limb-length discrepancy compensation. Primary outcomes included the 20-week wound-healing rate and wound area reduction. Secondary outcomes included minor amputation, new ulcers in the contralateral limb, perceived comfort, and hip pain.
Results:
On an intention-to-treat basis, 15 participants in the control and 19 in the treatment group showed ulcer healing (p = 0.0023). In those with >80% adherence to the offloading device, multivariate analysis showed that the shoe lifts improved ulcer healing time. The use of a shoe lift reduced the number of minor amputations and the occurrence of new ulcers in the contralateral limb (p = 0.035; p = 0.033 respectively). Hip pain and perceived comfort improved with the use of shoe lifts (p < 0.001).
Innovation:
It validates the use of shoe lifts for patients with DFUs, as it is the first largest study of its kind to establish a clear reference standard to guide clinician decision-making.
Conclusion:
The use of shoe lifts reduced healing time in participants with diabetes and active plantar foot ulcers. Shoe lifts reduce late complications, including new ulcers in the contralateral limb and minor amputations.
INTRODUCTION
Diabetes-related foot ulcers affect approximately 18.6 million people worldwide 1 and are associated with decreased physical function, affecting the quality of life and increasing health care utilization. 2,3 Without appropriate care, foot ulcers can lead to infection, hospitalization, and amputation. 4 Approximately 20% of people with diabetic foot ulcers (DFUs) will undergo an amputation, irrespective of the level. 5
DFUs develop as a result of loss of protective sensation, in addition to foot deformity and biomechanical abnormalities, 6 and in the case of weight bearing, it can cause hemorrhage beneath a callus presenting as damage that extends below the epidermis and dermis, becoming a full-thickness DFU. 2 Once a foot ulcer in a person with diabetes appears, offloading is the most important intervention for effective healing. 7 The International Working Group on the Diabetic Foot (IWGDF) recommends the use of different offloading devices, footwear, surgery, and other interventions to heal DFUs. 8 Adherence is a main factor associated with clinical success and wound healing. 9 In contrast, self-reported neuropathic postural instability has been found to be the main factor associated with poor adherence. 10 Induced limb-length discrepancy affects not only adherence, but a previous study also found that the peak pressure of the total foot on the short limb increased with a footwear-induced limb-length discrepancy of 20 mm or more. 11 They also found that the peak pressure was especially high under the second through fifth metatarsal heads and that the maximum vertical force was increased beneath the third through fifth metatarsal heads. 11
CLINICAL PROBLEM ADDRESSED
The 2023 IWGDF update recommends that in a person with a DFU for whom a knee-high or ankle-high offloading device is used, the use of a shoe lift on the contralateral limb should be considered to improve comfort and balance while walking in the device. 8 Contralateral limb-length discrepancy compensation improves patient adherence to offloading devices owing to enhanced comfort during use. 12
However, to the best of our knowledge, there is no evidence relating an increase in healing rates to improved adherence in patients using contralateral limb-length discrepancy compensation. Therefore, the present study aimed to evaluate the clinical efficacy of combining an offloading device with a contralateral shoe lift to compensate for limb-length discrepancy in patients with plantar DFU.
MATERIALS AND METHODS
Trial design
A monocenter randomized controlled parallel (1:1) clinical trial included 42 consecutive patients with diabetes and active DFU. This study was approved by the Hospital Clínico San Carlos Ethics Committee in Madrid, Spain, in July 2019 (approval number: 19/337–E). Before inclusion in the study, all participants provided written informed consent according to the principles of the Declaration of Helsinki. 13 This study was registered at ClinicalTrials. gov (registration no.: NCT04117269).
Participants
Patients who met the following selection criteria were enrolled consecutively from our specialized outpatient diabetic foot unit.
Inclusion criteria were having confirmed type 1 or 2 diabetes mellitus, aged >18 years, presenting with a plantar neuropathic DFU classified as Texas IA or IIA, glycemic control confirmed by a hemoglobin A1c of ≤10% (85.8 mmol/mol) in the previous 3 months, and having a wound area (WA) surface size of 1–30 cm2 at the time of inclusion. The exclusion criteria were critical limb ischemia as defined by the Trans-Atlantic Inter-Society Consensus II guidelines, 14 presence of active DFU in the contralateral limb, presence of major amputation (below or above the knee) in the contralateral limb of examination, presence of soft tissue infection, untreated diabetic foot osteomyelitis, or the need for walking aids. Lesser toe-related DFUs were excluded from the study due to the different indication of the offloading device. Diabetic peripheral neuropathy was diagnosed as an inability to sense the pressure of a 10-g Semmes-Weinstein monofilament at three plantar foot sites and/or a vibration perception threshold > 25 V as assessed using a biotensiometer (Me.Te.Da. s.r.l., Via Silvio Pellico, 4, 63,074 San Benedetto del Tronto, Italy). 15
Peripheral artery disease was confirmed by vascular assessment of the affected foot based on distal pedal pulse palpation, ankle–brachial index, toe–brachial index, and transcutaneous oxygen pressure. Critical limb ischemia was defined as an ankle–brachial index of ≤0.4 and an ankle systolic blood pressure of <50 mm Hg or a toe systolic blood pressure of <30 mm Hg. 16
Interventions
Participants were randomly assigned to the control or treatment groups. After randomization, all participants were followed for 20 weeks or until wound healing. Both groups received the same standard of care throughout the trial. The participants visited the outpatient clinic twice weekly where the DFU was cleaned with sterile physiologic saline and debrided, if needed. All wounds were dressed with neutral dressings, depending on the exudate level.
In addition, all participants were offloaded according to the IWGDF offloading guidelines. 8 A removable knee-high offloading device is the second choice for the offloading treatment (Stabil-D, Podartis s.r.l Unipersonale—Crocceta del Montello [TV], Italy).
The WA surface and photographs were assessed during each monthly study visit, until wound healing or until the end of the study.
Planimetric wound size measurements were performed by tracing the perimeter on an acetate grid with a fine-nibbed pen using Visitrak (Smith & Nephew, UK), and digital photographs were taken.
Induced limb-length discrepancy compensation
Patients allocated to the treatment group were prescribed a shoe lift on their usual therapeutic footwear on the contralateral limb. Limb-length discrepancy is a relatively common problem found in as many as 40% to 70% of the population, patients with foot ulcerations often require offloading devices with an elevated sole construction, which usually induce unintended limb-length discrepancy. 11
Limb-length discrepancy compensation was measured depending on the patient’s offloading device and assuming that some patients could suffer from previous limb-length discrepancy, using the following protocol. 17
The participants were placed barefoot in a standing position on the gait platform for the limb-length discrepancy assessment. From a posterior view, the inferior knee fold (femorotibial joint) was marked and measured with a caliper to confirm that there is no fold asymmetry. Then, the participant put their offloading device on the ulcerated limb and their usual therapeutic footwear and orthoses, if they wear it, on the contralateral limb. All the patients included in the research wore a multilayer custom-made orthosis (40 shore degrees base of ethyl vinyl acetate). It did not affect the limb-length discrepancy measurement as all the patients were evaluated for induced limb-length discrepancy with their usual therapeutic footwear and the custom-made insole.
Next, the contralateral limb was balanced by incrementally adding standard boards (0.5 cm) until the knee folds were symmetrical, and the millimeters required for the shoe lift of the contralateral limb were calculated. Shoe lifts were constructed in all cases by the same prosthetist using high-density ethylene-vinyl-acetate with a rocker outsole design. The modification was applied to usual indoor and outdoor therapeutic footwear.
Once the modification was performed, the participant was provided with the modified therapeutic footwear, and the investigator verified the correct height compensation. Every participant wore a therapeutic footwear for preventive purposes.
Outcome measures
The primary outcome measure was the 20-week healing rate defined as “intact skin at a previous foot ulcer site, meaning “complete epithelialization without any drainage.” 18 In addition, the WA percent reduction was calculated as [(A0 − A1)/A0] × 100. Where A0 is the initial would area and A1 is the WA after treatment (each visit).
The secondary outcomes evaluated included minor amputation, defined as “any resection through or distal to the ankle,” and a new ulcer in the contralateral limb. The participants were provided with two accelerometer devices (Uniaxial accelerometer—Tractivity, Kineteks Corporations) to monitor adherence and physical activity. One accelerometer was placed inside the bandage, and the other inside the offloading device using nonremovable straps. Therapeutic adherence was calculated based on the number of steps registered by the offloading device accelerometer/number of steps registered by the bandage pedometer. Based on this proportion, the subgroups were before statistical analysis using a cutoff of 80% adherence, which was indicated by previous studies as being appropriate for creating similar-sized participant groups with high and low adherence. 19
In addition, physical activity was assessed based on the number of steps registered by the bandage accelerometer during the 20-week trial period. Average daily step count and offloading device adherence were calculated from these measurements. Offloading device adherence was defined as the percentage of cumulative steps over 7 days of recording that the offloading device was worn.
The comfort of the prescribed offloading device, interventions, and hip pain assessment were evaluated in both groups using a visual analog scale score, after the 20-week follow-up period. It consists of a straight horizontal line from 0 to 10 where 0 means “no pain” and 10 means “worst pain imaginable” for pain assessment and “not comfortable at all” and “the most comfortable imaginable” for comfort assessment, respectively. 20
Sample size calculation
The target sample size was calculated using Epidat® v.4.2 for Mac OS based on previously reported 20-week healing rates of neuropathic DFU in participants treated with offloading devices similar to those used in the present study. 21
We assumed a 20% difference in wound healing between Group 1 (treatment group) with a healing rate of 0.9 (19) and Group 2 (control group) with a healing rate of 0.7. 22
Based on a desired power of 90%, an α level of 0.05 with a confidence interval of 95%, and assuming a dropout rate of broadly 10%, at least 21 participants must be included per group in the study and 42 randomly assigned participants are required.
Randomization
Before study recruitment, the study investigator (M.L.M.) randomly assigned the participants to two groups (1:1) using a computer-generated simple randomization list. Group 1 (treatment group) received limb-length discrepancy compensation (shoe lift) in the therapeutic footwear of the contralateral limb, whereas group 2 (control group) did not receive limb-length discrepancy compensation. Due to the nature of the trial, participant blinding was not feasible. The investigators who analyzed primary and secondary outcomes (M.G.M.; R.J.M.B.) were blinded to the randomization sequence and the participant treatment.
Statistical methods
In an intention-to-treat analysis, univariate analysis of risk factors associated with ulcer location was performed using the chi-square test for categorical variables and Student’s t test for quantitative variables using SPSS version 29.0 (SPSS, Chicago, IL, USA). The strength of difference in the effect size was calculated using the Phi coefficient for the chi-square test and the r coefficient for the nonparametric test, considering the values >0.01, >0.30, and >0.50 as small, medium, and large effects, respectively. Cohen’s d was calculated as the effect size for parametric and considered the values >0.2, >0.5, and >0.8 as small, moderate, and large effects, respectively. 23 Relative risk reduction (RRR) = treatment group risk—control group risk/control group risk and the number needed to treat (NNT) = 1/treatment group risk—control group risk were used to estimate the size of the effect. Differences in survival between the subgroups (>80% adherence to the offloading treatment) were evaluated using the log-rank test and expressed using Kaplan–Meier curves. Continuous and categorical variables with p < 0.10 in the univariate analysis were selected as covariates to develop a multiple logistic regression model for determining covariates associated with ulcer recurrence-free survival time, it was expressed using hazard ratios with a forward stepwise selection method.
RESULTS
Between March 2021 and December 2023, we enrolled 42 participants in the study who were randomly assigned to the following two groups: the control group (n = 21 participants) and the shoe lift group (n = 21 participants) (Fig. 1). All participants included in the study were prescribed with a knee-high offloading device (n = 42) Table 1.

Trial profile.
All participants included in the study were followed up for 20 weeks to assess wound healing. Participants who did not achieve wound healing within 20 weeks were followed up for 12 months to assess late complications, such as delayed wound healing, new lesions in the contralateral limb, and minor amputation. In addition, control group participants resulted in a lower adherence level compared with the intervention group (p = 0.004) (Table 2).
Patients’ baseline characteristics and diabetes complications (N = 42)
SD, standard deviation; CI, confidence interval; VAS, visual analog scale; TcpO2, transcutaneous oxygen pressure; MTH, metatarsal head; TMA, transmetatarsal amputation.
For categorical variables: chi-square test, as the Phi coefficient, where an effect size of 0.01 representing a small effect, 0.30 medium effect, and 0.50 large effect.
For normally distributed variables: for independent samples, Student’s t-test; effect size as Cohen’s d: representing effect size values >0.2 as small effect, >0.5 as moderate effect, and >0.8 as large effect; d is positive if the mean difference is in the predicted direction.
p < 0.05, significant association.
Outcome measures by study groups (N = 42)
SD, standard deviation; CI, confidence interval; IQR, interquartile range; VAS, visual analog scale; WA, wound area; WAR, wound area reduction.
For categorical variables: chi-square test, as the Phi coefficient, where an effect size of 0.01 representing a small effect, 0.30 medium effect, and 0.50 large effect.
For normally distributed variables: for independent samples, Student’s t-test; effect size as Cohen’s d: representing effect size values >0.2 as small effect, >0.5 as moderate effect; and >0.8 as large effect; d is positive if the mean difference is in the predicted direction.
p < 0.05, significant association.
All participants (n = 42) completed the planned study visit twice a week for the 20-week follow-up period. Ulcers healed in 15 participants (71.4%) in the control group and 19 participants (90.5%) in the treatment group. The median healing time for the treatment group was 12 weeks, interquartile ranges (IQRs 8–16), and 20 weeks (IQR 16–20) for the control group. The main and secondary outcome measures for the study groups are presented in Table 2. We observed that the treatment group showed less hip pain (4.2 ± 2.5 vs. 0.9 ± 1.2; p < 0.001) and perceived comfort (3.6 ± 1.6 vs. 5.5 ± 1.3; p < 0.001) via the use of a shoe lift than the control group.
A total of four patients in the control group (19%) suffered a minor amputation event compared with no minor amputation in the treatment group (p = 0.035) (Table 2). Causes for minor amputation were worsening of DFU requiring treatment of secondary diabetic foot osteomyelitis in all the cases.
Intent-to-treat analyses were performed in all the participants included in the study (n = 42) (Supplementary Table S1). We observed that 34 participants (80.95%) resulted in high adherence to offloading device. Seventeen participants resulted in high adherence (>80%) in the control group, while in the experimental group 19 participants resulted in a high level of adherence (>80%). After excluding nonadherent (<80% of adherence to offloading device) participants (n = 6), adherent participants were evaluated using univariate analyses per protocol (Supplementary Table S2). The results derived from outcome measures divided by healing and nonhealing participants (Supplementary Table S2) were similar to those obtained in the outcome measure analyses divided by study groups (Table 2). Mainly, after excluding nonadherent participants, we observed that belonging to the experimental group was a protective factor for healing (13 healers in control group vs. 19 healers in the experimental group, p = 0.019).
The RRR for DFU healing via the use of shoe lift compared with the control group was 26%, and the NNT was 5.3.
Participants prescribed a shoe lift showed a reduction in healing time (12-week IQR [8–16]) compared with the control group participants (20-week IQR [16–20]). Figure 2 shows the association between randomization groups and the time-to-heal survival time (log-rank p = 0.004) in participants with high adherence to offloading devices (n = 36).
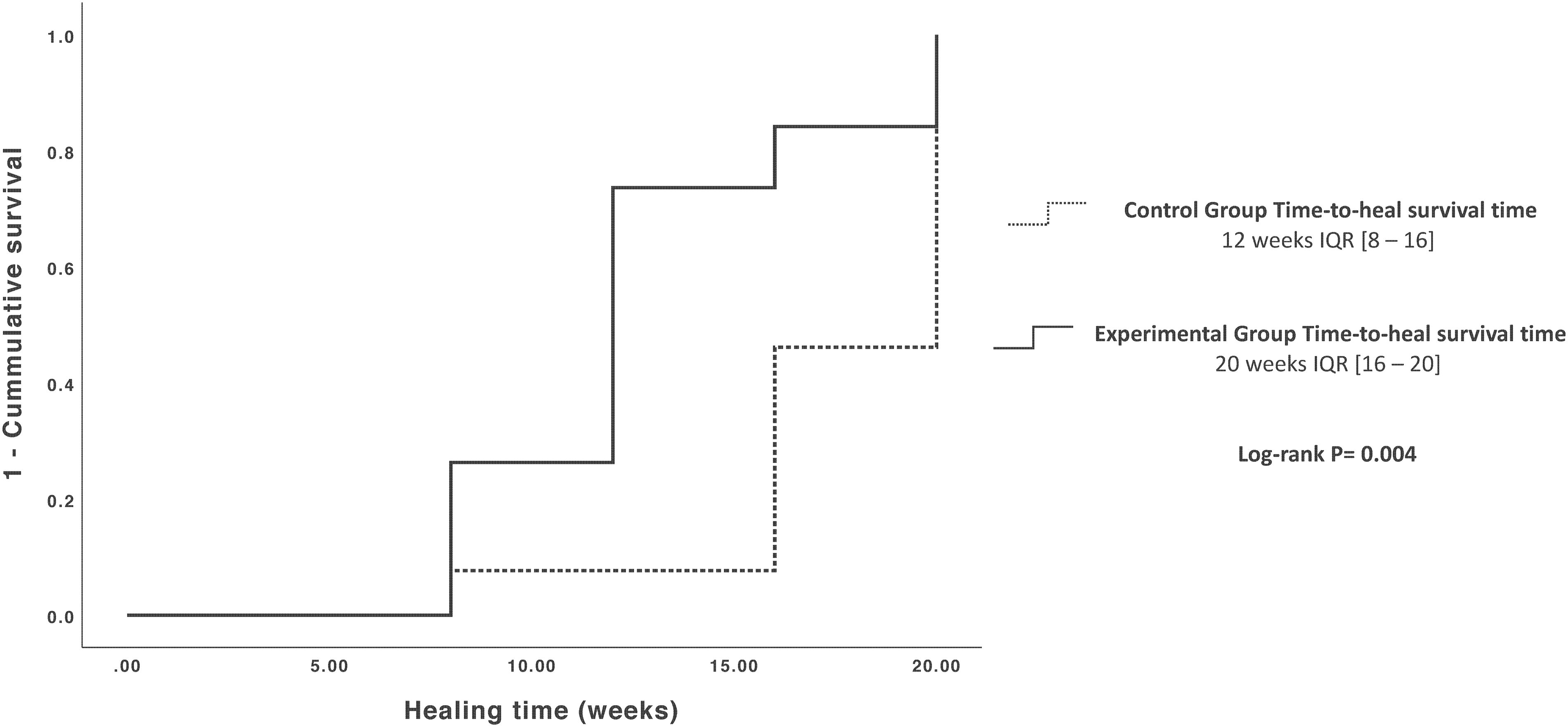
Time to heal for both study groups (per-protocol analysis participants).
Variables with p < 0.1 in the univariate analysis (type of diabetes, cardiovascular disease, body mass index, contralateral height discrepancy, minor amputation, and allocation) were included in the logistic regression model. The use of a shoe lift was the only variable associated with ulcer healing time in the multivariate model; the use of a shoe lift was found to be a protective factor related to DFU healing in diabetic participants with polyneuropathy and an active DFU (p = 0.044; 95% confidence interval 1.022–4.411; hazard ratio 2.12).
DISCUSSION
To the best of our knowledge, this is the first report to demonstrate an association between the compensation of a contralateral lower limb discrepancy with a shoe lift in participants with plantar DFUs using an offloading device and wound healing time. In this randomized clinical trial, participants who were prescribed with shoe lifts showed a 46% higher prevalence of DFU healing than those in the control group. In addition, the results demonstrate that the treatment group showed less hip pain and perceived comfort via the use of a shoe lift than the control group. The results of the current trial can be compared with those of Crews et al., 12 who found that shoe lifts reduced stance phase times in participants at risk of DFU; it is important to highlight that reducing the stance phase time reduces the peak plantar pressure in the forefoot, 24,25 and for that reason, shoe lifts result in higher healing rates. Following the same trend, Perttunen et al. 26 analyzed plantar pressures in nondiabetic participants with limb-length discrepancies and found that the loading of the long limb was greater, and the foot loading patterns shifted more to the forefoot in the long limb to compensate for walking disturbances caused by limb-length discrepancies. Reducing limb-length discrepancy with a shoe lift reduces plantar pressure in the long limb, reducing the time to heal. In addition, our participants experienced no minor amputations during the follow-up period, which could be a protective factor against patient morbidity due to the use of a shoe lift.
Nahas MR et al. 11 observed that peak pressures in the short limb were higher; following this trend, we observed that participants in the treatment group showed fewer ulcer occurrences (9.5%) in the nonulcerated limb than those control group participants (23.8%). The fact that peak pressures in the short and long limb increase within the use of offloading devices can be explained with higher occurrence even with the worsening of foot ulcers; the use of a shoe lift in the short limb may balance foot pressures and prevent further complications such us minor amputations and occurrence of new ulcers.
Limb-length discrepancy has been demonstrated to increase oxygen consumption and muscular fatigue 27 ; we found that participants in the treatment group demonstrated higher values of perceived comfort, which can be explained by the fact that participants with a shoe lift can walk further with less metabolic consumption.
In our study, all participants were prescribed a knee-high offloading device and the healing rate did not differ based on the offloading treatment method; in addition, the adherence to wearing the offloading device in all participants (n = 42) was high (>80%), and we observed that shoe lifts improved the adherence to wearing the offloading device (93%) versus control group (87%), this played a large role in the good prognosis of participants prescribed with a shoe lift. Last, the presence of different anatomical locations of DFUs should be analyzed in depth; midfoot and rearfoot ulcers are known to be more severe compared with forefoot ulcers, thus researchers should analyze this fact in depth in further studies.
The present study has some related limitations; first, the randomized clinical trial was not blinded due to the nature of the shoe lift. Second, the sample size was reduced in number, due to the difficulty in recruiting patients and the difficulty in finding the requirement in the characteristic needed.
In conclusion, the use of a shoe lift in combination with a high knee-offloading device resulted in a higher healing rate at 20 weeks. The use of a shoe lift increased patient comfort, reduced hip pain, and increased the rate of ulcer occurrence in the contralateral limb. Clinicians should consider prescribing shoe lifts in combination with an offloading device to improve clinical outcomes.
INNOVATION
The study has several important strengths, including being the first randomized clinical trial to evaluate the healing rate and clinical outcomes after prescribing a shoe lift to participants with plantar diabetic foot ulcer. The International Working Group on the Diabetic Foot recommends considering a shoe lift on the contralateral limb to improve the person’s comfort and balance while walking in the offloading device, which is based on very low evidence. Our research is the basis for always prescribing a shoe lift; it should be evaluated as a high level of evidence research. 28 In addition, our research was based on an objective limb-length discrepancy measurement, and the shoe lift was custom-made based on the measured limb-length difference for each participant. Previous research used a standard shoe lift that could influence clinical outcomes. Our research was based on the best standard of practice, following international recommendations, 15 using a removable knee-high offloading device.
KEY FINDINGS
Approximately 20% of people with diabetic foot ulcers will undergo an amputation.
Do shoe lifts to compensate for limb-length discrepancy result in increased adherence and healing rates?
The use of a shoe lift reduced the number of minor amputations and the occurrence of new ulcers in the contralateral limb, while improving hip pain and perceived comfort.
Clinicians should consider prescribing shoe lifts in combination with an offloading device to improve clinical outcomes.
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
The authors gratefully acknowledge the support of the staff and patients of the Diabetic Foot Unit of the Complutense University of Madrid. This research received no external funding.
ClinicalTrials. gov registration no.: NCT04117269. External Shoe Lift to Improve Healing and Adherence in Patients with Diabetic Foot Ulcers.
AUTHOR DISCLOSURE AND GHOSTWRITING
Conceptualization: M.G.M., M.L.-M., and J.L.L.M. Methodology: M.G.M., M.L.M., R.J.M.B., I.S.C.-A., and J.L.L.M. Software: M.L.M. and A.T.G. Validation: M.G.M., M.L.M., and J.L.L.M. Formal analysis: R.J.M.B. and M.L.M. Investigation: M.G.M., M.L.M., I.S.C., A.T.G., and J.L.L.M. Resources: M.L.M. and J.L.L.M. Data curation: M.G.M. and M.L.M. Writing—original draft preparation: M.G.M., M.L.-M., and R.J.M.B. Writing—review and editing: M.G.M., M.L.M., R.J.M.B., I.S.C., A.T.G., and J.L.L.M. Visualization: J.L.L.M. Supervision: M.L.-M. and J.L.L.M. Project administration: J.L.L.-M. All authors have read and agreed to the published version of the article. The authors declare the absence of ghostwriters in the current research.
ABOUT THE AUTHORS
SUPPLEMENTARY MATERIAL
Supplementary Table S1
Supplementary Table S2
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.