
Abstract
Objective:
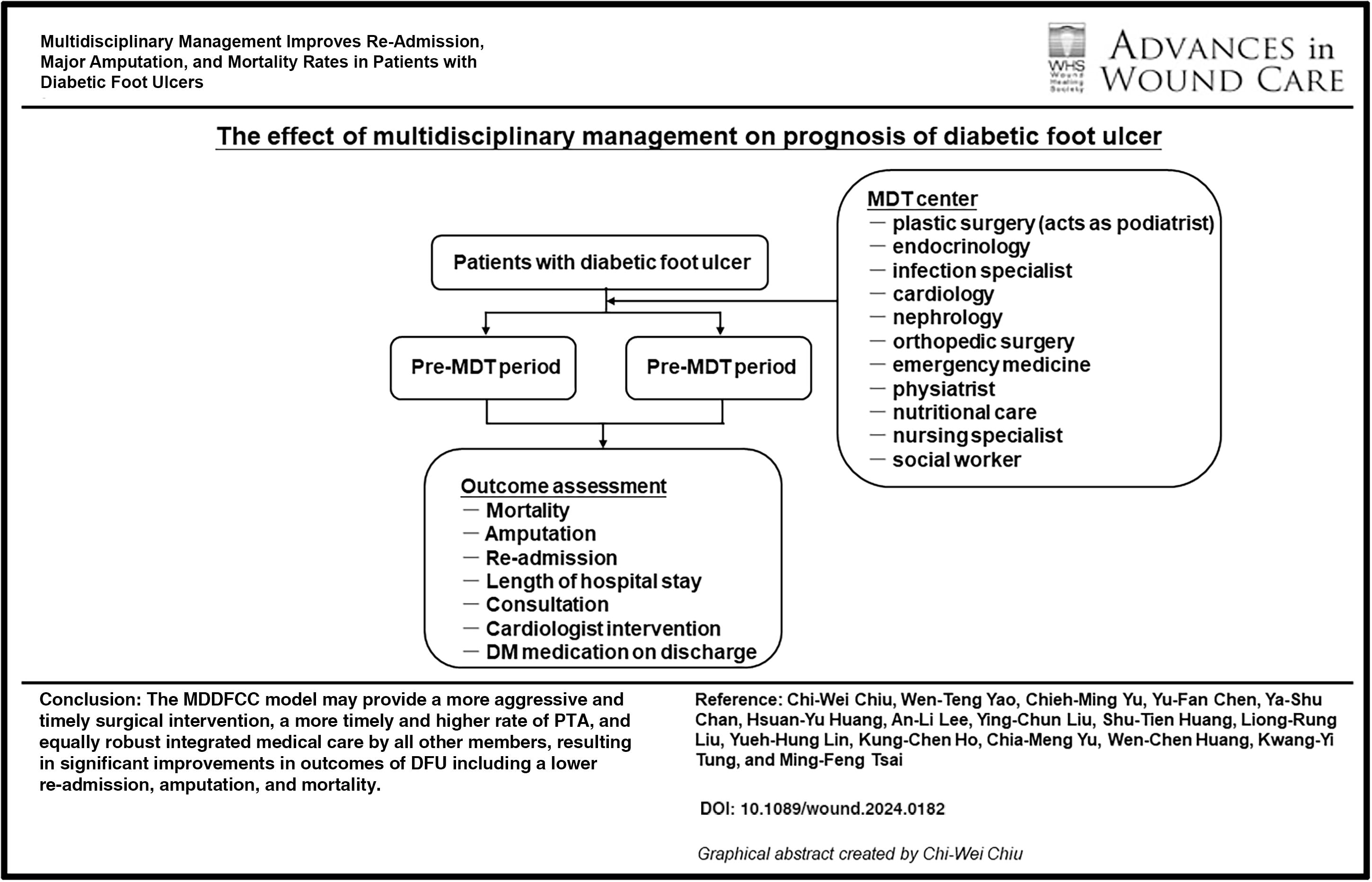
The objective of this study was to evaluate the impact of a multidisciplinary team (MDT) approach in the management of diabetic foot ulcers (DFUs).
Approach:
A multidisciplinary diabetic foot care center (MDDFCC) was opened at our institution in August 2018. Outcomes of DFU treatment, including re-admission, amputation, and mortality rates, were compared before and after opening the MDDFCC.
Results:
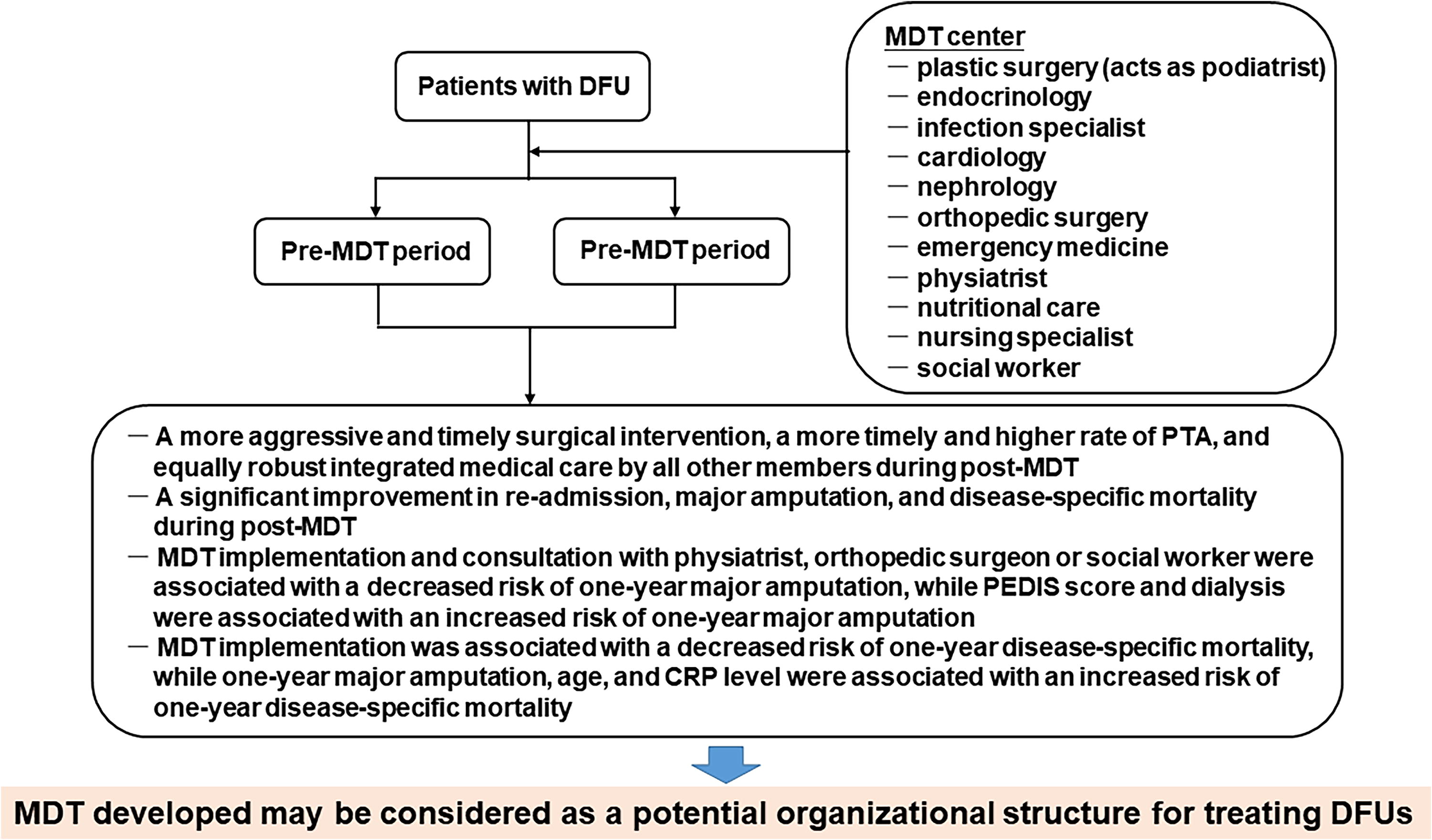
Patients seen after the MDDFCC was opened had a lower risk of 1-year re-admission (hazard ratio [HR] = 0.697, 95% confidence interval [CI]: 0.387–0.988), 1-year major amputation (HR = 0.447, 95% CI: 0.091–0.984), and 1-year disease-specific mortality (HR = 0.277, 95% CI: 0.105–0.730). PEDIS score (HR = 2.343, 95% CI: 1.264–2.971), history of dialysis (HR = 1.858, 95% CI: 1.258–4.053), and consultation with a physiatrist (HR = 0.368, 95% CI: 0.172–0.788), orthopedist (HR = 0.105, 95% CI: 0.042–0.261), or social worker (HR = 0.370, 95% CI: 0.082–0.871) were associated with 1-year major amputation. One-year major amputation (HR = 2.636, 95% CI: 1.586–4.570), age (HR = 1.094, 95% CI: 1.051–1.140), and C-reactive protein level (HR = 1.052, 95% CI: 1.008–1.098) were associated with 1-year disease-specific mortality.
Innovation:
Plastic surgeons received patients at the MDDFCC, with active participation by all contributing members. This arrangement brought advantages, including more aggressive and timely surgical intervention, a more timely and higher rate of percutaneous transluminal angioplasty, and equally robust integrated medical care by all other members.
Conclusion:
The MDDFCC approach may be a potential organizational structure with for treating DFUs, resulting in significant improvements in outcomes of DFU including a lower re-admission, amputation, and mortality.
Ming-Feng Tsai, MD

INTRODUCTION
The prevalence of diabetes is increasing worldwide, 1 and diabetic foot ulcer (DFU) is a common and important complication. 2 Up to 25% of people with diabetes will develop a DFU in their lifetime, and about 85% of lower limb amputations are preceded by a DFU. 3 A DFU is difficult to treat because of various diabetes-related complications, including venous insufficiency, peripheral arterial disease (PAD), elevated and prolonged foot pressure, and peripheral neuropathy. 4 These comorbidities, coupled with secondary infections due to impaired ulcer healing, increase the risk of major lower extremity amputation, defined as an above-ankle amputation. 5 Notably, the 5-year mortality rate exceeds 70% in patients who require a lower extremity amputation due to a DFU. 6 A DFU has a major long-term impact on morbidity, mortality, physical distress, and quality of life because of impaired mobility. 7 In addition, a DFU imposes a financial challenge to health care systems globally. In the United States, the per-person incremental annual health care costs for persons with DFUs receiving Medicare were $11,710. 8 In Taiwan, the per-person annual health care costs are $4,702 in 1 year. 9
As diabetes is a multi-organ systemic disease, all comorbidities that affect wound healing should be managed by a multidisciplinary team (MDT) to optimize outcomes of patients with a DFU. Optimal management of patients with DFUs includes clinical awareness, adequate blood glucose control, periodic foot inspection, custom therapeutic footwear, pressure offloading to the foot, proper diagnosis, timely local wound care, and swift interventions for osteomyelitis and ischemia.3,10 DFUs should be perceived as a major warning for morbidity and mortality, and as such they require close monitoring, medical follow-up, and integrated foot care. 11 Integrated foot care is a pathway of management with rapid and appropriate access to an MDT for coordinated care between hospital and community services. 12 Recent studies have demonstrated that an MDT approach may reduce the rate of major lower extremity amputations in patients with a DFU.13,14 Notably, an MDT approach can decrease the risk of amputation in patients with a DFU by 50–85%.5,6
While the benefits of an MDT approach for treating DFUs are well-documented and included in most major guidelines, several studies have noted high heterogeneity with respect to the composition of MDTs and interventions.15–17 The structure and delivery of care by MDTs vary across settings and countries,18,19 and are often dependent on local culture and customs, available resources, government policies, and geography. Health care disciplines that may be included in an MDT include general medicine, endocrinology, infectious disease, vascular surgery, podiatry, plastic surgery, orthopedic surgery, nursing, nutrition management, orthotics and prosthetics, physiotherapy, and psychology. The impact of each discipline in the MDT depends in large part on the stage of the DFU; however, podiatry has a central role throughout. 20 As part of an MDT approach, it has been suggested that podiatrists serve as gatekeepers for the prevention and management of DFUs and complications. 21
In August 2018, an MDT center for the management of DFUs was opened at our institution (multidisciplinary diabetic foot care center [MDDFCC]). The center includes experts from the fields of plastic surgery (acted as podiatrist), endocrinology, infectious disease, cardiology, nephrology, orthopedic surgery, emergency medicine, psychiatry, nutritional care, and nurse specialists and social workers. The center is headed by the plastic surgery department. Wound debridement, vascular intervention, education, blood glucose control, advanced dressing changes, pressure offloading, surgery, and other advanced therapies are available at the clinic, and services are provided in a structured and integrated approach, with constant review of the process. As such, understanding and evaluating the effect of the MDT approach is essential. Thus, the objective of this study is to evaluate the impact of the MDT for the care of DFUs. The primary outcomes evaluated were the 1-year re-admission rate, 1-year major amputation rate, and 1-year disease-specific mortality rate. Risk factors for these outcomes were also examined.
Innovation
Within the framework of an MDT approach, it has been proposed that podiatrists assume the role of gatekeepers in the prevention and management of DFUs and their associated complications. This is the first study to highlight that a plastic surgeon (acts as podiatrist) is in charge of the MDDFCC, and patient care is provided by many medical specialties. Treatment of DFUs is delivered through a structured and integrated approach, with constant review of the process. The results support that this MDT approach provides more aggressive and timely surgical intervention, a higher rate of prompt percutaneous transluminal angioplasty (PTA) and post-discharge anti-diabetes medications, and robust integrated medical care from all other members. The MDT developed may thus be considered as a potential organizational structure for treating DFUs.
Clinical Problem Addressed
A DFU is a common and important complication of diabetes, and the 5-year mortality rate for patients who require a lower extremity amputation because of a DFU surpasses 70%. DFUs significantly affect long-term morbidity, mortality, and physical well-being, as well as overall quality of life due to reduced mobility. Furthermore, DFUs present a substantial economic burden on health care systems worldwide. Recent studies have demonstrated that an MDT approach may reduce the risk of a major lower extremity amputation in patients with a DFU by 50–85%. While the benefits of an MDT approach for treating DFUs are well-documented and included in most major guidelines, several studies have noted high heterogeneity with respect to the composition of MDTs and interventions.
METHODS
Study design and participants
This retrospective study was conducted at Mackay Memorial Hospital, a tertiary care and teaching hospital in Taipei, Taiwan. Patients with a DFU who were admitted and received surgery between August 2015 and July 2022 were included in the study. Patients who were lost to follow-up and those with incomplete treatments were excluded. Data were extracted from the hospital information system for analysis, and patients were divided into two groups: patients admitted and treated between August 2015 and July 2018, before establishment of the MDDFCC, and patients admitted and treated between August 2018 and July 2022, after establishing the MDDFCC (Fig. 1). Approval for the study was obtained from the ethics committee of our hospital (No. 24MMHIS236e). The need for informed consent was waived as this study was a retrospective review of medical records, and all patient data were de-identified.
Summary graphic illustration.
Establishment of the MDDFCC
Prior to establishing the MDDFCC, there was no clear or well-defined protocol for the treatment of DFUs. Patients were managed only by their attending physician, and consultations with other medical specialties or allied health professionals were at the discretion of the physician. During this period, physicians were trained in diabetic foot surgery, and diabetic foot nurse specialists were trained to provide diabetic foot care under medical supervision.
The core composition of the MDDFCC included a plastic surgeon (acted as podiatrist) who received patients, two metabolic endocrinologists, two infection specialists, two cardiologists, one orthopedist surgeon, one physiatrist, two nutritionists, four diabetic foot nurse specialists, and one social worker (Fig. 2). A weekly special clinic for diabetic foot was also established, and exclusively dealt with patients suffering from diabetic foot wound. New patients were first seen by a plastic surgeon and admitted to the hospital if deemed necessary. After admission, patients were seen by other members of the MDDFCC, and assessed to determine if the patient required surgical wound management (e.g., revascularization, surgical debridement, skin grafting, amputation, negative pressure wound therapy, hyperbaric oxygen), optimization of glucose control, and management of other factors such as cardiac and renal function, nutritional management, patient education (diet, exercise, medication, wound care), and specialized footwear. All patients were seen by a social worker to help provide financial or social assistance if required. After all evaluations were completed, each case was discussed by the MDT to integrate the evaluations of each team member and develop a patient-specific management plan (Fig. 3). The MDDFCC accepted referrals from all hospital and community clinicians.
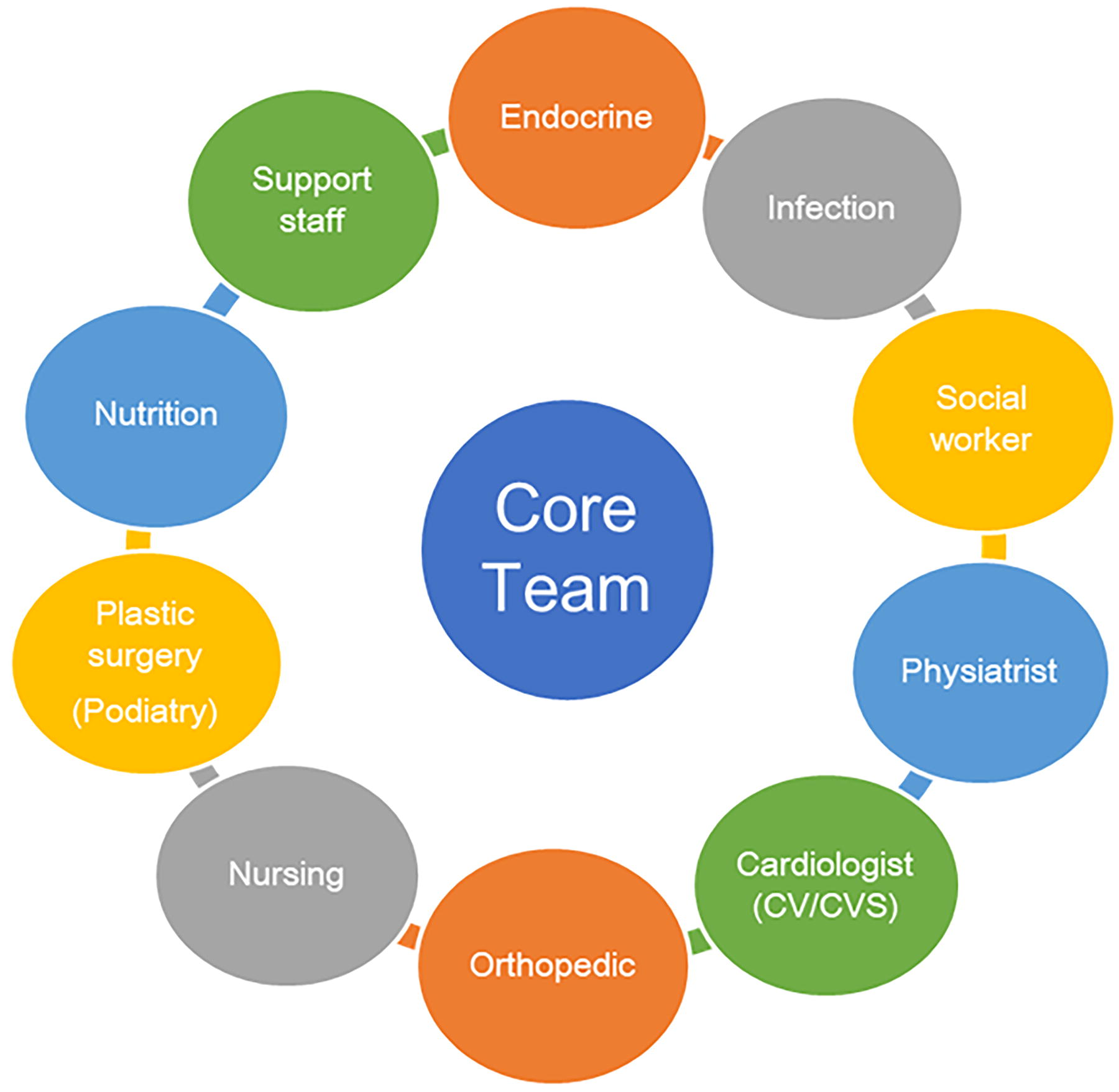
Composition of the core structure of the multidisciplinary diabetic foot care center (MDDFCC).
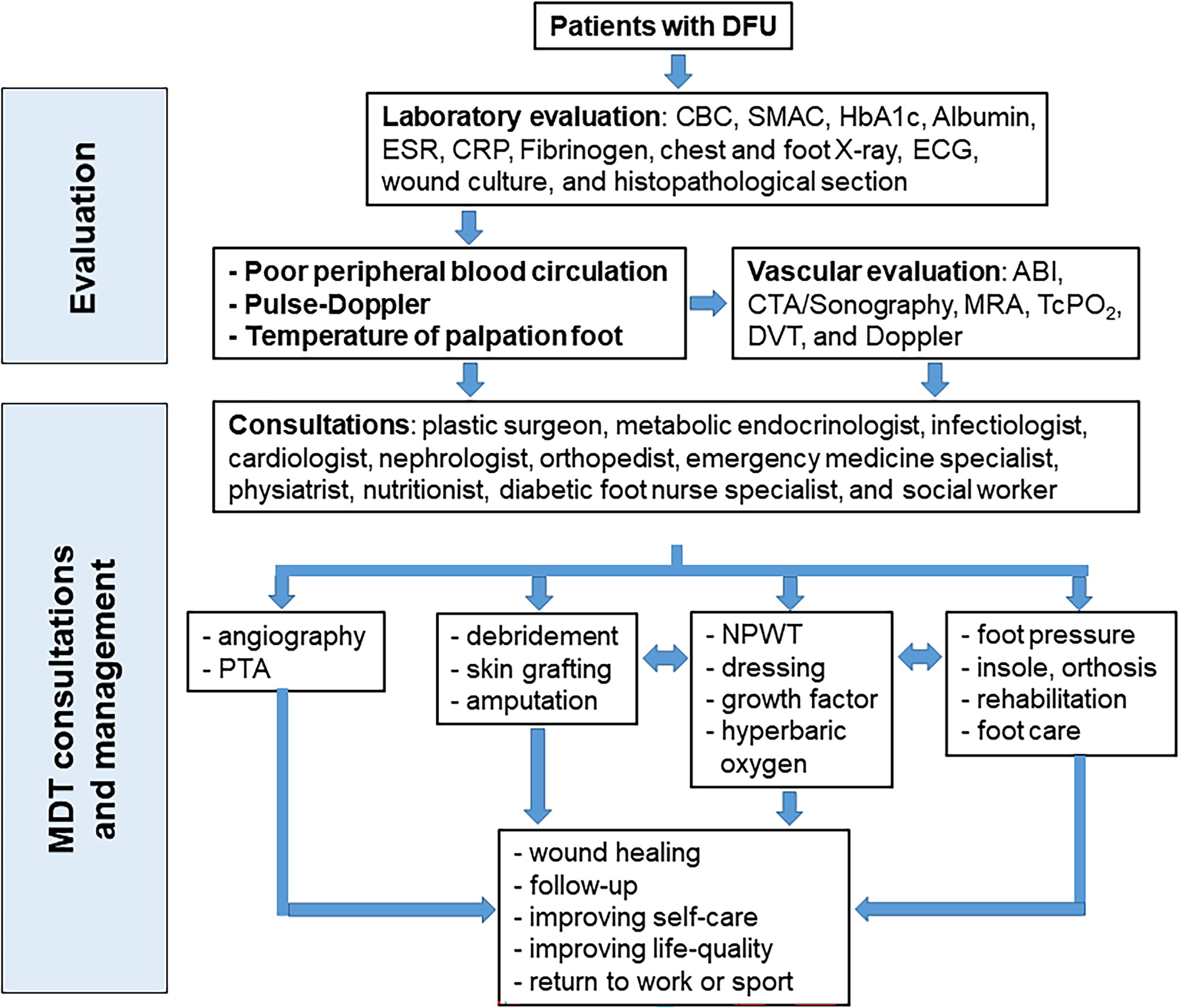
Workflow of the multidisciplinary diabetic foot care center (MDDFCC) for managing diabetic foot ulcers (DFUs). ABI, ankle-brachial index; CBC, complete blood count; CRP, C-reactive protein; CTA, computed tomography angiography; DVT, deep vein thrombosis; EKG, electrocardiography; ESR, erythrocyte sedimentation rate; HbA1c, hemoglobin A1c; NPWT, negative pressure wound therapy; PTA, percutaneous transluminal angioplasty; SMAC, sequential multiple analysis; TcPO2, transcutaneous oxygen measurement.
Data collection and evaluation
Patient outcomes were compared between patients seen before and after the establishment of the MDDFCC. The primary outcomes were mortality, major/minor amputation, length of hospital stay, and re-admission. Major amputations were defined as amputations above the ankle. Minor amputations were defined as amputations below the ankle. Each patient was followed up for a minimum of 1 year after initial discharge.
The secondary outcomes included time to PTA, medications prescribed for diabetes at discharge, white blood cell (WBC) count, C-reactive protein (CRP), and hemoglobin A1c (HbA1c). Other data collected from the medical records to evaluate risk factors for the primary outcomes included patient age and sex, Wagner classification, the perfusion, extent, depth, infection, and sensation (PEDIS) classification system score, hypertension, dialysis, PAD, history of diabetic foot, smoking, and alcohol consumption.
Statistical analysis
Continuous variables were represented as median and range, and comparisons between groups were performed with the Mann-Whitney U test. Categorical variables were expressed as number (percentage) and assessed by Fisher’s exact test following Bonferroni correction for comparisons between groups. Multivariate logistic regression analysis was performed to examine associations between patient characteristics and post-treatment outcomes. SPSS version 25.0 software (IBM Corp., New York, USA) was used for all statistical analyses. A value of p < 0.05 was considered to indicate a statistically significant difference.
RESULTS
Patient characteristics
The characteristics of patients seen before establishment of the MDDFCC (n = 154) and after establishment of the MDDFCC (n = 224) are shown in Table 1. The distributions of age and sex, PEDIS score, Wagner classification, history of diabetic foot, hypertension, dialysis, smoking, alcohol use, WBC count, and CRP level were not significantly different between the two groups (all, p > 0.05). However, patients seen after the establishment of the MDDFCC had a higher frequency of PAD, and higher HbA1c and CRP levels (all, p < 0.05).
Patient demographic and clinical characteristics
Data are presented as median (range) or count (percentage).
p < 0.05.
CRP, C-reactive protein; DM, diabetes mellitus; HbA1c, hemoglobin A1c; HTN, hypertension; MDDFCC, multidisciplinary diabetic foot care center; PAD, peripheral artery disease; PEDIS score, perfusion, extent, depth, infection, and sensation classification system score; WBC, white blood cell.
Outcomes
Compared with the pre-MDDFCC group, the post-MDDFCC group had a lower 1-year disease-specific mortality rate, a lower major amputation rate within 1-year of follow-up, a lower re-admission rate within 3 and 3–6 months after discharge, a lower number of re-admissions within 1 year after discharge, a shorter time to angiography or PTA intervention and a higher angiography or PTA intervention rate, a higher rate of consultations with an infection specialist, nutritionist, psychiatrist, or social worker, a higher rate of anti-diabetic medication use (oral or insulin), and a lower rate of consultations with orthopedists (all, p < 0.05, Table 2). However, the immediate mortality and 1-year all-cause mortality rates, immediate major amputation rate and 1-year minor amputation rates, length of hospital stay, and rate of consultations with cardiologists or metabolic endocrinologists were not significantly different between the two groups (all, p > 0.05, Table 2).
Comparison of treatment outcomes between the two groups
Data are presented as median (range) or count (percentage).
p < 0.05.
PTA, percutaneous transluminal angioplasty.
Risk factors for re-admission within 1-year after initial discharge
Univariate Cox regression analysis showed that factors associated with re-admission within 1 year included MDDFCC implementation, sex, dialysis, consultation with a cardiologist, and PTA intervention (all, p < 0.05, Supplementary Table S1). Multivariate Cox regression analysis showed that only MDDFCC implementation (hazard ratio [HR] = 0.697, 95% confidence interval [CI]: 0.387–0.988, p = 0.041, Supplementary Table S1) was negatively associated with 1-year re-admission. Notably, sex, diabetes, consultation with cardiologists, and PTA were not significantly associated with 1-year re-admission (all, p > 0.05, Supplementary Table S1).
Risk factors for major amputation within 1-year after initial discharge
Univariate Cox regression analysis showed that factors associated with major amputation within 1 year after initial discharge were MDDFCC implementation, PEDIS score, history of PAD, hypertension, dialysis, CRP level, and consultations with cardiologist, physiatrist, orthopedic surgeon, or social worker (all, p < 0.05, Table 3). Multivariate Cox regression analysis showed that MDDFCC implementation (HR = 0.447, 95% CI: 0.091–0.984, p = 0.036) and consultation with physiatrist (HR = 0.368, 95% CI: 0.172–0.788, p = 0.010), orthopedic surgeon (HR = 0.105, 95% CI: 0.042–0.261, p < 0.001), or social worker (HR = 0.370, 95% CI: 0.082–0.871, p = 0.026) were negatively associated with major amputation within 1 year, while PEDIS score (HR = 2.343, 95% CI: 1.264–2.971, p = 0.002) and dialysis (HR = 1.858, 95% CI: 1.258–4.053, p = 0.019) were positively associated with amputation within 1 year (Table 3). However, PAD, hypertension, CRP level, and consultation with cardiologist were not significantly associated with amputation within 1 year (all, p > 0.05, Table 3).
Cox regression analysis of factors associated with 1-year major amputation
p < 0.05.
CI, confidence interval; HR, hazard ratio.
Risk factors for 1-year disease-specific mortality
Univariate Cox regression analysis showed that factors associated with 1-year disease-specific mortality were MDDFCC implementation, major amputation within 1 year, age, PEDIS score, PAD, CRP level, consultation with an orthopedist surgeon, and anti-diabetic medication on discharge (all, p < 0.05, Table 4). Multivariate Cox regression analysis showed that MDDFCC implementation (HR = 0.277, 95% CI: 0.105–0.730, p = 0.009) was negatively associated with 1-year disease-specific mortality, while major amputation within 1 year (HR = 2.636, 95% CI: 1.586–4.570, p = 0.027), age (HR = 1.094, 95% CI: 1.051–1.140, p < 0.001), and CRP level (HR = 1.052, 95% CI: 1.008–1.098, p = 0.022) were positively associated with 1-year disease-specific mortality (Table 4). However, PEDIS score, PAD, anti-diabetes medication on discharge, and consultation with an orthopedic surgeon were not significantly associated with 1-year disease-specific mortality (all, p > 0.05, Table 4).
Cox regression analysis of factors associated with 1-year disease-specific mortality
p < 0.05.
DISCUSSION
In patients with diabetes, DFUs significantly contribute to mortality and morbidity, often necessitating repeated hospitalizations that impose substantial burdens on both patients and health care systems. The primary objectives of DFU treatment are to promote wound healing and prevent complications such as infection, the need for amputation, and reduced quality of life. Health care providers specializing in wound care encounter many hurdles when treating patients with DFUs due to the complex nature of diabetes. Various factors need to be evaluated and considered when treating these patients, such as blood glucose level, blood pressure, lipid profile, and renal function. These factors cannot be adequately addressed within a conventional care model that involves only one medical discipline. Consequently, a multidisciplinary approach is the cornerstone of effective management, with early intervention playing a pivotal role in mitigating the risks of severe infections and amputations. To address these issues, an MDDFCC was established at our health care institution, and the results of this study indicate that an MDT approach improved the outcomes of patients with DFUs.
A comparison of the demographic and clinical characteristics of patients seen before and after the establishment of the MDDFCC showed no significant differences in most areas, including disease severity and medical history. However, patients seen after establishment of the MDDFCC had a higher frequency of PAD and higher HbA1c levels. The increased frequency of PAD may be attributed to improved history-taking and medical awareness, while the higher HbA1c levels could result from selection bias following the implementation of the MDDFCC.
There were no differences in the length of hospital stay, immediate mortality, and major amputation rates during hospitalization between the two groups. However, after opening the MDDFCC, there was a significant decrease in the 1-year disease-specific mortality, major amputation, and hospital re-admission rates. This is consistent with other reports, as the impact of an MDDFCC is likely to become more apparent over a longer period, effectively improving long-term prognosis.22,23 Immediate mortality and morbidity are more likely reflective of the acute severity of a patient’s condition upon initial admission, and this was similar between the two groups, potentially explaining the absence of significant disparities in these immediate outcomes. It is important to note that some studies have not differentiated between short- and long-term mortality and morbidity outcomes, which could possibly influence their reported conclusions.
Notably, the rate of minor amputations did not decrease after the MDDFCC was opened, a phenomenon also observed in similar studies. In a recent study by Thewjitcharoen et al., 24 the minor amputation rate increased from 19% to 22% in patients with a DFU following MDT management. It is speculated that patients who would have originally required major amputations received timely and effective treatment through early minor amputations. The reduction in time to PTA and surgical debridement further supports that the establishment of the MDDFCC allowed patients to receive comprehensive assessments and invasive treatments (e.g., surgical debridement, PTA) more promptly, leading to better outcomes. Moreover, the consultation rates for infection specialists, nutritionists, and physiatrists, as well as the increased proportion of patients undergoing PTA and those discharged with anti-diabetes medication, indicate that the MDT was able to provide more comprehensive and holistic medical care. These effects were reflected in the reduced rates of major amputations and mortality within 1 year.
To the best of our knowledge, there has been no prior investigation examining the relation between an MDT approach and the re-admission rate of patients with a DFU. Re-admission frequency should be considered when assessing the impact of an MDT approach because while re-admissions may be clinically justified, they incur significant costs. Patients face physiological challenges, including pain and impaired mobility, which adversely affect their quality of life. Additionally, they experience emotional distress characterized by increased anxiety and depression, as well as economic hardships due to lost productivity during hospital stays, leading to diminished workforce participation and financial burdens. Previous literature indicates that the majority of DFU management expenses are linked to hospital admissions and wound severity; notably, wounds requiring any level of amputation result in substantially higher costs compared with those that heal primarily.25–27 This observation suggests that an MDDFCC could potentially decrease the overall financial burden of patients and health care systems for DFU management by reducing the 1-year rates of major amputation (HR = 0.447) and re-admission (HR = 0.697).
A comparison of overall costs for DFU management before and after the MDDFCC implementation was not within the scope of this study. However, research has shown that a multidisciplinary clinic providing foot care, education, offloading footwear, and custom orthoses led to an 82% reduction in foot-related inpatient admissions and a 76% reduction of inpatient charges. 28 Other studies examining this topic have also employed economic modeling to demonstrate that similar programs can be cost-effective if they achieve target reductions in amputations.29,30
Studies have reported evidence both supporting and questioning the effectiveness of an MDT approach on DFU outcomes. While three review studies have suggested that there is insufficient evidence to support the effectiveness of complex interventions and educational initiatives in reducing the risk of lower extremity amputations due to a DFU,31–33 more recent research has demonstrated positive effects of an MDT approach in decreasing major lower extremity amputation rates.14,15 The results of the present study are consistent with the conclusions of the most recent studies, indicating that an MDT approach can effectively improve DFU outcomes. The International Working Group on the Diabetic Foot has also emphasized the importance of integrated foot care within MDTs for preventing DFUs among high-risk patients. 34 However, they have also acknowledged significant heterogeneity in the literature regarding team composition, types of interventions, and study designs.16,35 Other reports have focused on the collective effectiveness of an MDT as a whole, rather than attributing the impact to individual team members.14,15,36–38 These studies have evaluated outcomes such as major amputation rates and mortality rates, emphasizing similarities in team compositions to assess overall success. Overall, these studies highlight the considerable diversity among different MDTs and research methods, underscoring the challenges in comparing results across studies, especially when teams vary in skills and organizational structures.
In a systematic review on the effectiveness of MDTs in reducing major amputations for patients with DFUs, four essential team-related elements were identified 14 : (1) teams are composed of members from medical and surgical disciplines; (2) larger teams benefiting from a “captain” with a nuclear and ancillary team structure; (3) clear referral pathways; and (4) care algorithms that provide timely and comprehensive care. The MDDFCC at our institution was established with these guidelines in mind and anchored by plastic surgeons with active participation from all contributing members. This arrangement provides advantages including more aggressive and timely surgical intervention, a higher rate of prompt PTA (often resulting from earlier surgical debridement), and robust integrated medical care from all other members.
Compared with previous studies, this study used a more comprehensive database of each patient with DFU, encompassing re-admission rates, disease-specific mortality, follow-up within 1 year, PTA, discharge medication, and more, which better highlights the advantages and therapeutic benefits of MDT management. Nevertheless, this study may not fully capture the benefits of an MDT approach. For instance, many vulnerable patients treated at the MDDFCC benefited from improved tracking, follow-up, and assistance. The integrated outpatient service provides convenience, special assistive devices, and offloading shoes, which helped many patients regain functionality. Additionally, patient self-care abilities improved through enhanced education, and the establishment of a database and regular meetings allowed the MDDFCC team to continue refining their approach. The significant increase in rates of social worker consultations reflects just a glimpse of the benefits the MDT approach has provided, which could include financial assistance, hospital visit coordination, and home visits.
Several limitations of this study must be acknowledged. First, the data were retrospective and derived from a single center. There were some notable differences between the pre-MDDFCC and post-MDDFCC groups, which may introduce potential selection bias. Second, it is possible that variations in wound treatment and outcome are attributable to differences in the type and severity of DFUs. However, PEDIS score, Wagner classification, angiography, PTA intervention, and discharge medications were included in the regression analysis to mitigate this concern. Third, the sample size is relatively small. Larger studies with multi-center and comprehensive databases and long-term follow-up are needed to confirm the results of this study.
CONCLUSION
The MDT approach has increasingly become the standard for treating DFUs. This study demonstrated that an MDT approach is effective in reducing re-admission, major amputation, and disease-specific mortality rates. The benefits of an MDT approach include more holistic treatment, improved quality of care, shorter time to intervention, enhanced awareness and education, coordinated rehabilitation, and effective long-term follow-up. Further data and studies are needed to validate and expand upon these results.
KEY FINDINGS
The MDT was anchored by plastic surgeons, thus providing more aggressive and timely surgical intervention, a more timely and higher rate of PTA, and integrated medical care by all other members.
Managing DFUs with an MDT model improves patient outcomes by significantly reducing re-admission, major amputation, and disease-specific mortality rates.
MDDFCC implementation and consultation with a physiatrist, orthopedic surgeon, or social worker were associated with a decreased risk of 1-year major amputation, while PEDIS score and dialysis were associated with an increased risk of 1-year major amputation.
MDDFCC implementation was associated with a decreased risk of 1-year disease-specific mortality, while 1-year major amputation, age, and CRP level were associated with an increased risk of 1-year disease-specific mortality.
MDDFCC implementation was associated with a decreased risk of 1-year re-admission.
Footnotes
AUTHORS’ CONTRIBUTIONS
C.-W.C., Y.-S.C., and M.-F.T. had made substantial contributions to the conception and study design. C.-W.C., W.-T.Y., Chieh-Ming Y., Y.-F.C., Y.-S.C., H.-Y.H., A.-L.L., Y.-C.L., S.-T.H., L.-R.L., Y.-H.L., K.-C.H., Chia-Meng Y., W.-C.H., K.-Y.T., and M.-F.T. collected the data. C.-W.C., W.-T.Y., Chieh-Ming Y., Y.-F.C., Y.-S.C., H.-Y.H., A.-L.L., Y.-C.L., S.-T.H., L.-R.L., Y.-H.L., K.-C.H., Chia-Meng Y., and M.-F.T. analyzed the data. C.-W.C. and M.-F.T. prepared the article. C.-W.C., W.-T.Y., Chieh-Ming Y., Y.-F.C., Y.-S.C., H.-Y.H., A.-L.L., Y.-C.L., S.-T.H., L.-R.L., Y.-H.L., K.-C.H., Chia-Meng Y., W.-C.H., K.-Y.T., and M.-F.T. made critical revision of the article. All authors read and approved the final version for submission.
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
No funding was received for this article.
ABOUT THE AUTHORS
SUPPLEMENTARY MATERIAL
Supplementary Table S1