
Abstract
Object:
The aim of this study was to compare the long-term effects of fractional carbon dioxide (CO2) laser treatment with traditional therapy on surgical scars by analyzing and comparing observational indicators.
Approach:
A randomized controlled trial was conducted on 116 patients who received scar treatment in our hospital, of which 58 patients received fractional CO2 laser treatment, and 58 patients received injection treatment. The outcome measures comprised the Vancouver Scar Scale (VSS) and the Patient and Observer Scar Assessment Scale (POSAS). The observation intervals occur at specific times. Evaluated at 6 months of follow-up, the outcome was blinded, on-site evaluation using the dermatological appearance scale (DAS) and visual analog scale (VAS).
Results:
Patients in the fractional carbon-dioxide laser (CO2FL) group rated better than those in the injection group in the POSAS, VSS, DAS, and VAS scores (p < 0.05). The therapeutic efficacy and patients’ satisfaction of the research group were superior to those in the control group.
Innovation:
Scars following surgical procedures can be treated in a variety of methods, but there is no consensus on the best method. CO2FL has exhibited safety and is more effective than traditional injection treatments for surgical scars. It is a worthwhile approach to consider in clinical treatment.
Conclusions:
This study demonstrates that CO2FL achieves more significant long-term results in surgical scars, including improved scar appearance, safety, and patient satisfaction.
INTRODUCTION
Surgical scars are a daily concern for thousands of patients worldwide. Surgical scars are scars that result from a surgical procedure. When the skin is cut during surgery, the body naturally heals itself by forming scar tissue over the incision site.1–3 While some surgical scars may be inconspicuous and small, others can be more prominent or raised. Factors such as the location of the incision, wound tension during healing, and the suture type used can all influence how the scar looks. The main types of surgical scars are hypertrophic scars, with a small percentage being keloids. Conventional interventions for surgical scars encompass topical silicone gel application, intralesional corticosteroid injection directly into scar tissue, cryotherapy, and sometimes even surgical revision. 4 However, the efficacy of these methods is not satisfactory. Therefore, it is necessary to explore methods that can improve appearance and alleviate symptoms associated with surgical scars.
Liang Chen, MD, PhD

In previous studies, Karmisholt et al. 2 reported a study that investigates the positive impact of nonablative fractional laser treatments on early wound healing stages in comparison with an untreated control group, employing randomized and controlled methods. This study provides us with a new therapeutic strategy for the treatment of scars with laser. In recent years, fractional carbon dioxide (CO2) laser (CO2FL) therapy has shown great potential in effectively treating scars. CO2FL fills the gap between conservative (silica gel, cryotherapy, and injection) and surgical treatment. Collagen remodeling is often cited as a key mechanism responsible for the improvements observed with CO2FL therapy, although this process is still under investigation. This innovative approach delivers controlled thermal energy in a fractionated manner, facilitating tissue remodeling and collagen synthesis, thereby ameliorating scar appearance and texture. 5 The CO2FL targets the water inside cells, which vaporizes and coagulates the nearby protein outside cells. The scar that undergoes treatment experiences collagen remodeling similar to that of normal skin. 6 By precisely targeting microscopic columns of tissue while sparing surrounding skin, CO2FL therapy stimulates epidermal turnover and dermal restructuring, leading to a smoother and more homogenous skin texture. Noteworthy advantages of CO2FL therapy over conventional treatments include its ability to precisely target scar tissue, minimal recovery time, and decreased chances of skin discoloration. 7 However, despite the increasing utilization of CO2FL therapy, its comparative efficacy and safety relative to traditional treatments for surgical scars remain incompletely elucidated.8,9 Therefore, this study endeavors to conduct a randomized controlled trial to compare and analyze the efficacy and safety profiles of CO2FL therapy with those of traditional treatments for surgical scars, in order to evaluate differences between CO2FL therapy and traditional injection therapy in terms of efficacy and safety.
INNOVATION
The optimal treatment for surgical scars remains undetermined despite the existence of numerous approaches. As an emerging treatment technology, there are few articles that compare fractional CO2 therapy with injection therapy, which is the most commonly used conservative treatment method for surgical scars. This study is one of the first to indicate that CO2FL therapy is more effective and satisfying compared with injection therapy. The results provide new evidence supporting this therapeutic approach, and it is worth considering for clinical treatment. It provides evidence for identifying the best treatment for surgical scars.
CLINICAL PROBLEM ADDRESSED
The introduction of fractional photothermolysis (FP) laser technology aimed to overcome the limitations associated with traditional laser technologies, and it was first launched in the United States and the United Kingdom in 2003. The U.S. FDA (Food and Drug Administration) approved its use for pigmented lesions, treatment of melasma, skin resurfacing, and various scars. The effectiveness of CO2FL treatment for surgical scars remains uncertain and lacks consensus among experts. This study aimed to compare the effectiveness and satisfaction of CO2FL with traditional injection treatments for surgical scars, in order to identify the best treatment for surgical scars.
MATERIALS AND METHODS
Study design
A randomized controlled trial was conducted to compare the clinical appearance of surgical scars after CO2FL exposures or injections. The patients who came for treatment were randomly divided into two groups, A and B. The patients are assigned numbers from 1 to 116 based on a computer randomization program (Excel, Microsoft, Washington, USA). Stratifying the randomization process based on scar type and location before assigning patients to treatment groups would help ensure that these factors are evenly distributed between the research (CO2FL) and control (injection) groups. Hypertrophic and atrophic scars, and high-tension and low-tension areas, stratified randomization ensures that each treatment group has a balanced number of participants. The patients will then receive the corresponding treatment according to their assigned group (the details can be found in Supplementary Data). Both the patients and the researchers remained unaware of group assignment during the entire treatment process. Treatment procedures, including local anesthesia and post-treatment care, were provided by independent personnel to avoid any bias from the research team. An on-site clinical evaluation of scars has been conducted at the following times: immediately before treatment and 2nd, 4th, 6th, 8th, 10th, and 12th week after initial therapy. Furthermore, a blinded clinical photo evaluation of scars was performed 6 months after the treatment. This is the end point of the study, and the treatment effects are evaluated based on the skin assessment systems of the Patient and Observer Scar Assessment Scale (POSAS), Vancouver Scar Scale (VSS), dermatological appearance scale (DAS), and visual analog scale (VAS) scores. Allocation concealment was achieved using a centralized randomization system or sealed envelope method by an independent researcher, ensuring that the study staff enrolling participants could not predict group assignment. The treatment allocation information was concealed in closed envelopes or via an online system until after data collection. In cases where missing data occur, multiple imputations will be used to estimate the missing values. Approval for the study was obtained from our hospital’s ethics committee and was conducted in accordance with the Declaration of Helsinki. The study was registered at researchregistry.com (UIN:10474). Written informed consent was obtained from all patients enrolled in the study. Electronic laboratory notebook was not used.
Patients
One hundred and sixteen patients (56 females, 60 males, ages 18–58 years, mean age 38.9 years) who underwent scars repair at our hospital’s Department of Dermatology, Department of Hepatobiliary Surgery, Department of Thoracic Surgery, and Department of Orthopedics between March 2020 and December 2023 were included in this analysis. The participants were divided into two groups, with each group consisting of 58 individuals. Group A (control group) received treatment with triamcinolone acetonide via intralesional injection, while group B (research group) underwent CO2FL therapy specifically targeting the area of the scar. The two groups’ scars treated in this study encompassed various types of surgical incision scars, located on different anatomical locations including the face, neck, arms, thorax, abdomen, and legs. All patients had surgical scars that persisted for more than a year, and there were no keloids, infections, or inflammatory skin conditions. Moreover, it is essential for participants to be capable of adhering to the prescribed treatment plan and fulfilling all post-treatment obligations.
Treatment methods
The treatment area was thoroughly cleansed before the treatment using a mild skin cleanser. In group A (injection), triamcinolone is administered via dermal injection beneath the scars. A 26-G needle is utilized to inject 1 mL lidocaine and 1 mL triamcinolone acetonide (10 mg/mL, XIANJU, Taizhou, China). The mixture is injected at a rate of 0.1 mL per centimeter. The therapy was immediately followed by the application of silicone gel (KELO-COTE, North Carolina, USA) topically. Injections are repeated biweekly for a maximum of six administrations. In group B (CO2FL), lidocaine was used to locally anesthetize the skin 30 min before treatment. The scars were treated with fractional ablative CO2 laser (SPLB, JYLASER, Chongqing, China), an ablative fractionated CO2 laser (10,600 nm) at settings of 20 W, stack 4 and 500 μm pitch for 1,000–1,500 μs. The laser therapy was immediately followed by the application of silicone gel (KELO-COTE, North Carolina, USA) topically. After the operation, they were given ice for 2 h to reduce the degree of heat damage. The combination of laser therapy and topical application of silicone gel was repeated every fortnight for a total of six sessions. The study using the CO2 fractionated laser device as a treatment has not been approved by the FDA, but specific devices or lasers employing this technology have been approved either through the pre-market approval process or via the 510(k) pathway.
Evaluations after therapy
The assessment criteria for the primary outcome measures in scars involve standardized measures such as the POSAS and VSS, assessed at the 12th week after the initial therapy. The co-primary outcome measures in scars involve standardized measures such as the VAS and DAS 6 months after the last treatment. The POSAS observer evaluated separate scar elements using the following items: pliability, thickness, vascularity, surface area, pigmentation, and relief. The patient evaluated the separate scar elements using the following items: pain, itch, pliability, relief, thickness, and self-assessment. The assessment of each element is conducted on a scale ranging from 1 to 10, where 1 represents “normal skin” and 10 indicates the “worst imaginable scar” compared with normal skin around it. The total score of the POSAS is determined by summing up the values of the first six items, which range from 6 to 60 points. The VSS elements include the following items: pliability, pigmentation, height and vascularity from 0 to 5. The 0 score indicates normal skin, while the maximum score represents the worst outcome. The scar condition in both groups was evaluated at different observation time points utilizing the VSS and POSAS. The observation intervals occurred during the 2nd, 4th, 6th, 8th, 10th, and 12th week after the initial therapy. Two dermatologists (X.M.Q. and L.C.) evaluated the scars and assigned scores using the VSS. Subsequently, both the dermatologists and the patients independently assessed the scars and provided scores utilizing the POSAS. Finally, all scores were recorded and analyzed according to the assigned groups by designated personnel. In addition, 6 months after the last treatment of each patient, relevant photos were captured according to standardized protocols. The photos were put into envelopes and numbered. The sequence was concealed using closed, consecutively numbered, nontransparent envelopes prepared by an independent third party to ensure random allocation concealment. After all the patients’ photos had been placed into envelopes, two dermatologists (X.M.Q. and L.C.) evaluated the clinical photos randomly based on standardized assessment. The standardized assessment included a VAS and a DAS. The VAS scale ranges from 0 to 10 cm (0 represents normal skin, while 10 indicates maximal scarring), and the DAS ranges from 1 to 10 (1 represents normal skin, while 10 indicates very different from normal skin). Close monitoring is conducted to detect any adverse reactions.
Statistical methods
Sample size calculations indicated that the study could detect a clinically significant difference of two points in the POSAS score, with a significance level of 0.05 and 90% power. The calculation determined that at least 104 patients (52 per group) are required. To account for potential dropout, the sample size was increased by 15%, resulting in a total of 116 patients (58 per group). This sample size ensures sufficient power to detect meaningful differences between the two treatments. The aim of this study was to compare the long-term effects of CO2FL treatment with traditional therapy on surgical scars by analyzing and comparing observational indicators. The null hypothesis is that there is no significant difference in scar recovery after treatment measured by scoring between the two groups of patients, while the alternative hypothesis is that the patients in the experimental group have lower scores after treatment than those in the control group, meaning that the experimental group has better therapeutic effects than the control group. The descriptive statistics of the data were indicated as mean, standard deviation, frequency, ratio, median, maximum, and minimum. The Shapiro–Wilk test was used to examine the normality assumption for numerical variables: those following a normal distribution were reported as (
Satisfaction questionnaire
As a secondary outcome measure, a satisfaction questionnaire was sent to all 58 patients in the laser group 6 months after the last treatment, and they were asked the following questions: On a scale of 1–10 (with 10 being the best), are the beneficial results of laser treatment still maintained? How satisfied were you with the treatment? Would you recommend this treatment to other patients with scars? Did you have any side effects from the treatment? Patients were welcome to enter any additional comments in a text box.
RESULTS
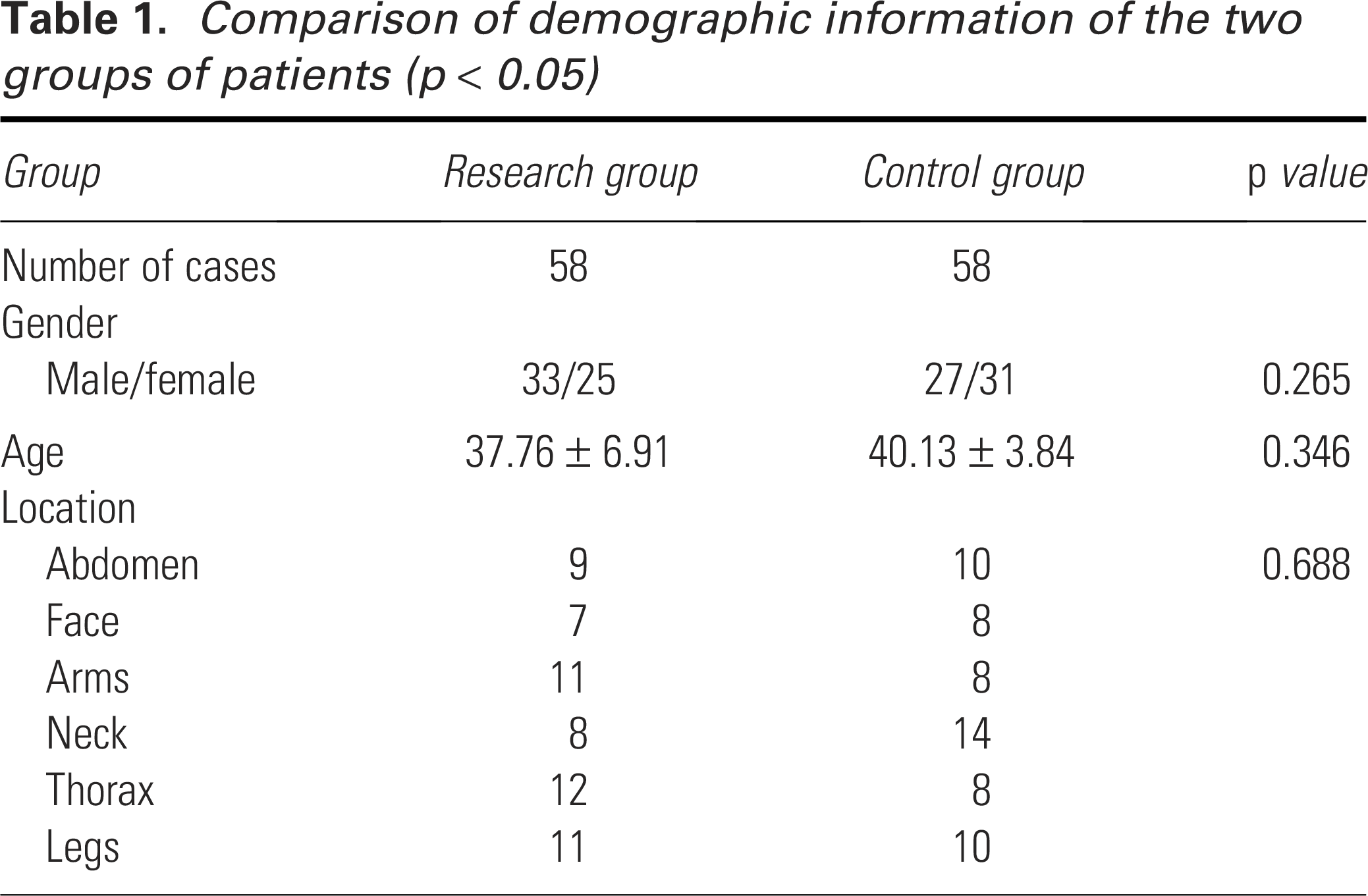
The research findings indicated that there were no notable variations in the demographic attributes observed among the two groups of patients (p < 0. 05). The specific details can be found in Table 1. Furthermore, the patient exhibited scars distributed across multiple anatomical regions, as depicted in Fig. 1. Scars are classified according to their anatomical location, including the face, neck, arms, thorax, abdomen, and legs, with approximately equal numbers of scars in each anatomical location. This can minimize bias and improve the accuracy of treatment effect estimates, ensuring that results are generalizable across different subgroups within the study population. There are no missing data in this study.

The diagram illustrates the correlation between grouping and scar location. The number of scars in each area was approximately equal.
Comparison of demographic information of the two groups of patients (p < 0.05)
Clinical response
At the conclusion of the study, significant improvements were observed in terms of scar flexibility or height, vascularity, and pigmentation for both groups. All the patients completed the trial. None of the patients reported any worsening of their surgical scars following treatment. After the injection therapy, spot bleeding and pain in the operated area were reported by 15 (26%) patients in the injection group. These side effects usually disappear within 3 days. Only 6 (10%) patients experienced mild to moderate discomfort during and after CO2FL treatment, along with mild to moderate redness and swelling that resolved within 3–7 days. These were the only side effects reported in the CO2FL group. Although some patients noted a longer duration of redness with CO2FL, this did not pose a significant issue. Three months after the final of six laser treatments, as assessed by both dermatologists and patients using the POSAS and VSS assessment, skin texture, atrophy, pigmentation, and overall appearance had improved in all scars based on patients and physician scoring. Supplementary Figs. S1 and S2 display clinical photographs showcasing certain results. In terms of the POSAS and VSS scores, there was a significant decrease in scores for patients in the CO2FL group compared with those in the injection group after the initial treatment. The 12th week POSAS scores indicate: CO2FL-treated median 21, IQR 16–27 versus control median 30, IQR 26–32; p < 0.05. In the meantime, the VSS scores indicate: CO2FL-treated median 2, IQR 1–3 versus control median 4, IQR 2–5; p < 0.05. Relevant infections were not detected in either study group after the treatment was administered. Group B (CO2FL group) demonstrated a relatively lower inclination toward the occurrence of long-term adverse effects in comparison with the observed prevalence rate within group A (injection group). Furthermore, in terms of the comparison between the two groups at each observation time point, it was observed that patients in the research group (CO2FL group) who underwent CO2FL treatment had notably lower scores after their first treatment compared with those in the control group (injection group) who received injections (p < 0.05; Tables 2 and 3).
Comparison of patient and POSAS scores between the two groups at time points (p < 0.05)
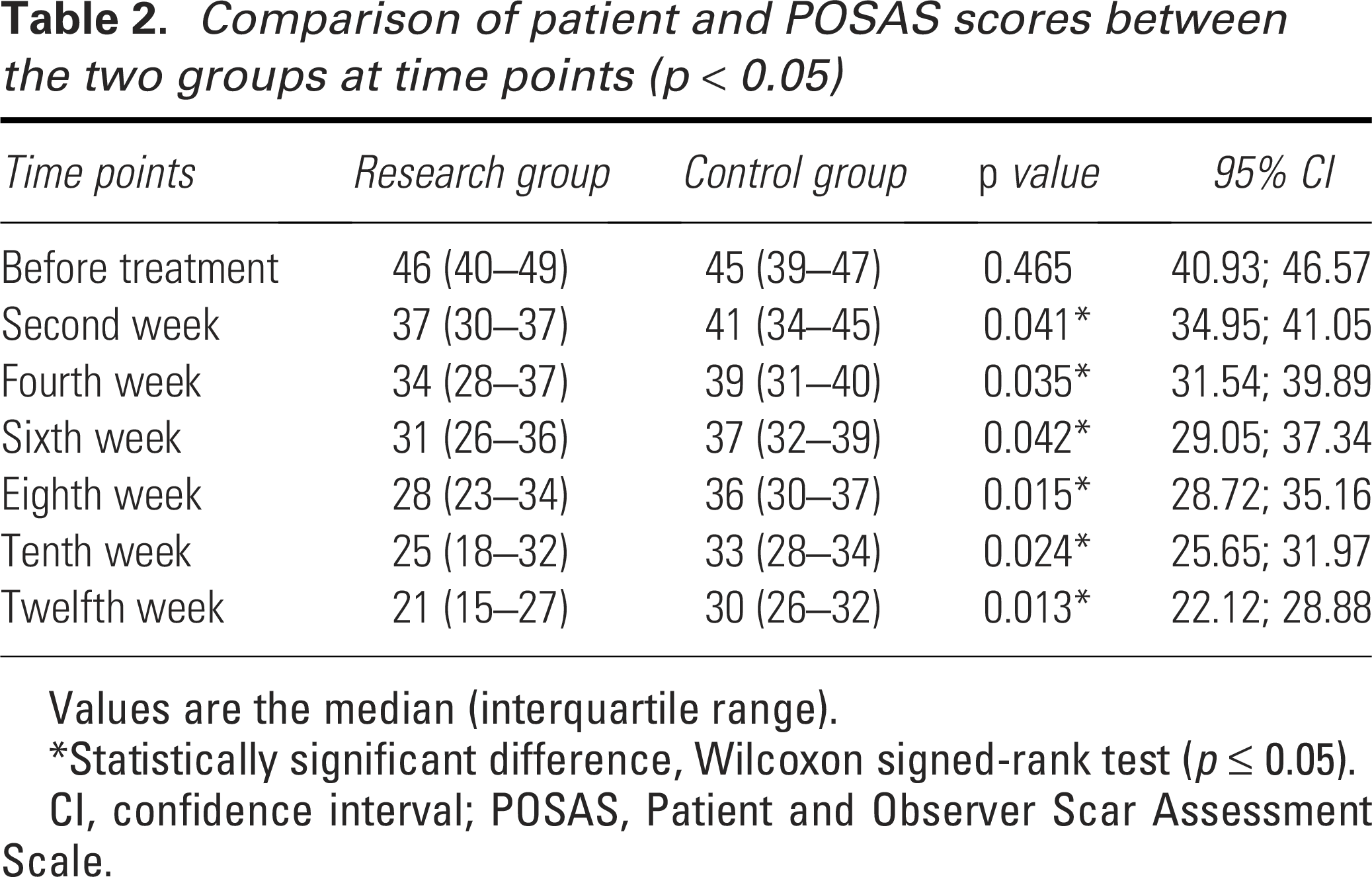
Values are the median (interquartile range).
*Statistically significant difference, Wilcoxon signed-rank test (p ≤ 0.05).
CI, confidence interval; POSAS, Patient and Observer Scar Assessment Scale.
Comparison of patient and VSS scores between the two groups at time points (p < 0.05)
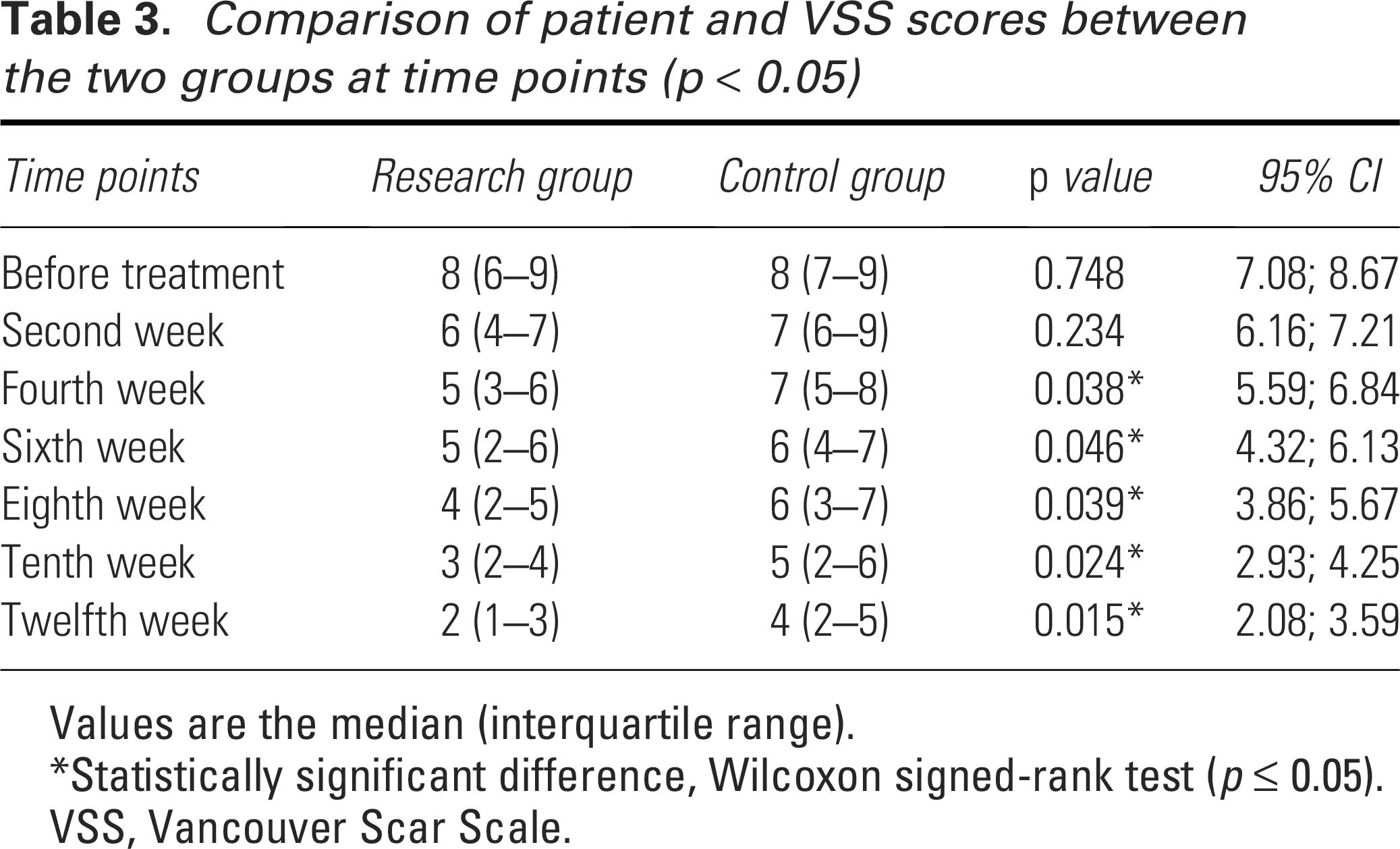
Values are the median (interquartile range).
*Statistically significant difference, Wilcoxon signed-rank test (p ≤ 0.05).
VSS, Vancouver Scar Scale.
Standardized assessment
In the standardized assessment comparing the control group (injection group) and the research group (CO2FL group), patients in the CO2FL group rated better than those in the injection group in the DSA and VSA scores. The DSA scores indicate: CO2FL-treated median 3, IQR 2–6 versus control median 4, IQR 3–6; p < 0.05. Concurrently, the VAS scores indicate: CO2FL-treated median 4, IQR 3–6 versus control median 5, IQR 3–8; p < 0.05 (Supplementary Table S1). Inter-rater reliability for POSAS and VSS evaluations was excellent, with Cohen’s kappa values of 0.82 for POSAS and 0.79 for VSS, indicating strong agreement between the two dermatologists. All assessment methods demonstrated concordance in the patients’ responses.
Satisfaction survey
As shown in Table 4, most patients were satisfied (n = 58, 57%) or very satisfied with the results (n = 29, 25%). However, outcomes were maintained in 60 patients (51%), with complete or partial repigmentation occurring in 32 (28%) and 24 (21%) patients. Furthermore, most patients (81%) would be willing to undergo CO2FL treatment again in the event of scar recurrence and 91% of patients would recommend CO2FL treatment to other patients, respectively. The drawback is that the time of the procedure was an inconvenience for some patients (comments from text box). Most patients were pleased with the improvement in scar appearance, noting smoother texture and reduced visibility. However, some patients expressed concerns about the number of treatment sessions required, finding it somewhat inconvenient despite the positive results. In addition, few patients reported mild side effects such as redness and swelling, but these were generally brief and did not significantly affect overall satisfaction.
Results of patient satisfaction survey

DISCUSSION
The formation of surgical scars is an inherent element of the body’s natural healing process following surgery. 3 When the skin is incised during a surgical procedure, collagen production is initiated by the body to facilitate wound repair, leading to the development of scar tissue at the site of incision.10,11 Superficial wounds that do not extend to the reticular dermis typically do not trigger abnormal wound healing characterized by prolonged localized inflammation, along with an abundance of newly formed blood vessels, fibroblasts, inflammatory cells, and collagen deposition.7,12 FP is a novel laser technology that generates numerous tiny areas of thermal damage in the epidermis and dermis, surrounded by unaffected tissue.13,14 This technique minimizes injury and promotes rapid healing of the skin. 15 While the exact mechanism behind FP for treating surgical scars remains unclear, it is believed that these localized areas of thermal damage may trigger a series of events leading to collagen normalization. 16 Prior to the introduction of fractionated technology, ablative laser devices (such as CO2 and Er:yttrium aluminum garnet) were commonly utilized for treating surgical scars. However, these devices often resulted in undesirable effects including prolonged swelling, crusting, redness, and increased pigmentation. Moreover, there were potential long-term risks associated with permanent changes in skin coloration and scarring as well as other irregularities in texture. 17
Unlike traditional lasers, fractional lasers avoid excessive heating of the skin, reducing the risk of nonspecific thermal damage that could worsen scarring. Prior studies have established that FP has the potential to induce the migration of normal melanocytes from adjacent tissue into the newly resurfaced area, thereby facilitating the repigmentation of hypopigmented scars.6,18 Research indicates that a significant number of patients undergo various forms of treatment prior to laser therapy, and patients seem to prefer other forms of treatment to remove scars before opting for laser therapy. The high cost of laser treatment and the requirement for multiple treatments may be factors that influence this orientation.19,20 Even so, the efficacy, noninvasiveness, and patient recommendations have led to an increasing number of individuals to choose laser therapy.
The aim of this study was to compare the long-term effects of CO2FL treatment with traditional injection therapy on scar healing by analyzing and comparing observational indicators. The results indicated that patients who underwent CO2FL treatment achieved significantly superior outcomes in terms of scar appearance evaluation compared with those in the traditional injection group. This implies that CO2FL effectively enhances the aesthetic aspects of scars by addressing concerns related to color, height, width, and texture. In addition, receiving CO2FL treatment resulted in more significant improvement, as indicated by the global evaluation conducted by physicians and subjective scoring reported by patients, compared with the group treated with injections. Our findings indicate that the clinical appearance of surgical scars can be enhanced by both injection and CO2FL, but the therapeutic effect of CO2FL is more significant. These results align with previous studies on the treatment of hypertrophic scar using CO2FL.21,22 While the clinical photos may not clearly demonstrate it, patients with surgical scars in joint areas experienced significant improvement in scar flexibility, alleviating both functional limitations and aesthetic concerns. It was shown in the follow-up after the treatment that CO2FL had a better patient satisfaction rate. Most patients found the CO2FL to be more effective and would recommend this procedure to other patients. This study is one of the first to indicate that CO2FL therapy is more effective and satisfying compared with injection therapy. The use of a well-defined comparison group and established clinical assessment tools provides a strong foundation for conclusions. The study design is robust, especially in the area of satisfaction surveys, this innovative design enables us to assess the effect more comprehensively. It contributes valuable findings to the wound care and dermatology field, specifically for scar management.
This study focuses on introducing the clinical experience of CO2FL in the treatment of surgical scars. However, it should be noted that there is variability in the initial morphology, anatomy, age, and etiology sites of scars. The selection of subjects, who have surgical scars, may vary from case to case and will not be consistent in depth, area, or location, which could affect the outcomes. To further validate these findings, controlled side-to-side comparative studies with larger sample sizes and longer follow-up periods are necessary. This study used standardized statistical methods to ensure the data’s reliability to the greatest extent possible. However, the demographics section is not sufficiently comprehensive, and patients’ self-scoring may be influenced by personal factors, leading to potential bias in the results. No correction for multiple comparisons was performed, as the primary outcome was the difference in POSAS scores between the two groups. As a result, p values should be interpreted with caution due to the potential for type 1 error. Because type 1 error is not controlled for in our analysis, a few of the statistically significant results may not actually be statistically significant. Furthermore, the mean follow-up time of 9.8 months is quite short for scar assessment, as scar tissue continues to remodel for at least a year after wounding. Insufficient observation time may introduce bias to the results, as some patients’ scars may undergo changes for about 1 year. Therefore, extending the observation period in future studies is necessary to capture long-term outcomes more comprehensively and accurately. The study did not account for scar age, which is a factor influencing the response to treatment, as older scars may have less potential for remodeling compared with newer scars. In addition, unmeasured confounders such as skin type, healing capacity, or underlying health conditions may have impacted the results, suggesting that future studies should include these variables to improve precision.23,24 While this study focused on surgical scars, its findings may have limited generalizability to other scar types, such as keloids and acne scars, due to differences in their pathophysiology and treatment response. Surgical scars generally heal through a controlled process that allows treatments such as CO2FL therapy to improve scar appearance effectively. However, keloids, which involve excessive collagen deposition and tissue overgrowth, are unlikely to respond similarly to laser treatment alone and may require alternative therapies such as corticosteroid injections or surgery. 25 Acne scars, which are often atrophic in nature, may benefit from laser treatment, but the results could vary depending on the type and severity of the scar. Future studies should explore the efficacy of CO2FL therapy across a broader spectrum of scar types and patient populations to determine its applicability to nonsurgical scars.26,27 Lastly, the subjective assessment of the patient may introduce potential biases, and future studies should aim to validate the effectiveness of this approach by utilizing a larger sample size, standardized measures in conjunction with patient-reported outcomes, exploring alternative topical medications, and different laser parameters to establish an optimal surgical scar treatment protocol. In conclusion, the utilization of CO2FL treatment proves to be both safe and effective when treating surgical scars. Although multiple sessions may be necessary to achieve optimal outcomes, noticeable enhancements are evident following just one round of treatment. This is a worthwhile approach to consider in clinical treatment.
KEY FINDINGS
Significant improvements were observed in terms of scar flexibility or height, vascularity, and pigmentation for both fractional CO2 laser and injection, but the outcomes of laser treatment are more pronounced.
Most patients (82%) are more satisfied with the laser treatment method, and most of them (91%) are willing to recommend it to others.
This study is one of the first to indicate that fractional CO2 laser therapy is more effective and satisfying compared with injection therapy for surgical scars. It provides significant meaning in identifying the best treatment for surgical scars.
AUTHORS’ CONTRIBUTIONS
L.C. and X.M.Q.: Study conception and design. L.C., Q.Y.W., X.M.Q., P.C., H.X., and L.Q.W.: Data collection. L.C., P.C., H.X., and Q.Y.W.: Analysis and interpretation of results. L.C., X.M.Q., H.X., P.C., L.Q.W., and Q.Y.W.: Draft article preparation. L.C., H.X., Q.Y.W., P.C., L.Q.W., and X.M.Q.: Reviewed the results and approved the final version of the article.
Footnotes
ACKNOWLEDGMENT AND FUNDING SOURCES
The authors thank Dr. Qiu Yu Wang for the language revision of this commentary. None declared. There are no financial disclosures, commercial associations, or any other conditions posing a conflict of interest to report for any of the above authors.
AUTHOR DISCLOSURE AND GHOSTWRITING
No competing financial interests exist. There are no ghostwriters involved in the writing of this paper.