
Abstract
Significance:
This systematic review was conducted to assess the quality of clinical practice guidelines (CPGs) on prevention and management of pressure injury (PI) in patients undergoing prone position ventilation (PPV) and summarize the recommendations based on the analyses of the CPGs.
Recent Advances:
We searched the PubMed, Cochrane library, Embase databases, guideline websites, professional association, quality standards, and Wound-Related Research Journals from January 1, 2010 to August 31, 2024. Included guidelines were those with recommendations for prevention and management of PI in patients undergoing PPV published in English. Four researchers independently assessed the eligible studies and extracted the data. Appraisal of Guidelines Research & Evaluation (AGREE II) instrument and the Reporting Items for Practice Guidelines in Healthcare checklist were used to assess the quality of the CPGs.
Critical Issues:
A total of 13 CPGs were included in this review. AGREE II demonstrated that the highest mean score was based on the scope and purpose and was 73.65 ± 10.91, whereas the lowest mean score was based on the editorial independence and was 49.79 ± 19.49. The scores of inter-rater agreements for AGREE-II quality appraisal ranged from 0.86 to 0.96. Recommendations for prevention and management of PI in patients undergoing PPV were inconsistent.
Future Directions:
The included CPGs were limited due to methodological issues and exhibited discrepancies in the coverage of important topics. Therefore, existing evidence should be used to propose identifiable recommendations and strengthen the rigor and standardization of guideline development in future research.

INTRODUCTION
Prone position ventilation (PPV) refers to a technique of positioning a patient in a prone position to enhance ventilation by redistributing lung gases more evenly, optimizing the ventilation–blood flow ratio, and improving oxygenation.1,2 In a meta-analysis that included 2,129 patients, the results showed that PPV has the potential to reduce mortality among patients with severe acute respiratory distress syndrome (ARDS) when applied daily for at least 12 h. 3 A systematic review reported that 43.4% of pressure injury (PI) was associated with prone ventilation. 4 A study conducted by Lucchini et al. 5 indicated that commonly occurred in positions of PI for patients undergoing PPV were as follows: face/chin, face/cheekbones, thorax, and trochanter. Notably, critically ill patients are required to maintain a nonphysiological position for a longer duration when undergoing PPV; however, this may lead to complications such as PI, unplanned extubation, peripheral nerve damage, and gastric contents reflux. 6
PI refers to damage of the skin, subcutaneous tissue, or muscles occurring at the bony sites due to pressure, shear force, or friction. 7 PI is the most prevalent complication in PPV patients, with an incidence rate of 25.7%, which is primarily attributed to its stages I and II. 8 This prevalence rate is further corroborated by the results of ancillary study 9 of a prospective multicenter randomized controlled trial in patients with severe ARDS, which demonstrated that the incidence of PI was 56.9%. Another study 10 reported that 43.4% of PI cases were associated with PPV. PI in patients undergoing PPV increases patient pain and medical costs, as well as the risk of secondary infections. This noncompliance affects treatment of the underlying diseases, as well as the effectiveness of the PPV.11,12 In response, several PI prevention guidelines for patients undergoing PPV13,14 have been developed to assist physicians and practitioners to integrate evidenced-based clinical decisions during the PPV treatment.
Clinical practice guidelines (CPGs) serve as crucial documents for guiding all caregivers’ interventions by providing specific recommendations to guide all caregivers. 15 Low-quality CPGs can negatively affect health care professionals’ clinical decision-making, resulting in poor patient outcomes and unnecessary financial burdens. 16 Conversely, high-quality CPGs serve as valuable decision-making tools for bridging the gap between current best evidence and clinical practice.17,18
Although several PI prevention and management CPGs for patients undergoing PPV have been developed globally, the quality of these guidelines remain uncertain. Subsequently, evaluation of the quality of these guidelines, along with consolidation of related recommendations, is essential. This systematic review assessed the methodological quality of PI CPGs applied during PPV, with Appraisal of Guidelines Research & Evaluation (AGREE II) instrument and Reporting Items for Practice Guidelines in Healthcare (RIGHT) being used as the assessment metrics.
METHODS
This review was reported in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses checklist. The review protocol was registered on the international prospective register of systematic reviews (PROSPERO identification CRD42024618461).
Search strategy and selection criteria
Literature search was conducted by two reviewers from January 1, 2010 to August 31, 2024. CPGs search was conducted in the following databases: PubMed, Cochrane library, Embase databases, guideline websites [National Guidelines Clearing house, National Institute for Health and Care Excellence (NICE), Scottish Intercollegiate Guidelines Network, and Guidelines International Network], professional associations [Canadian Association of Wound Care, National Pressure Ulcer Advisory Panel, The Canadian Association for Enterostomal Therapy, Ontario Wound Care Interest Group, European Pressure Ulcer Advisory Panel (EPUAP), Wound, Ostomy and Continence Nurses Society (WOCNS), and International Wound Infection Institute], quality standards [Accreditation Canada and Agency for Healthcare Research and Quality], and Wound-Related Research Journals [Wound Care Canada, Advances in Skin and Wound Care, Journal of Wound Care, Journal of the World Council of Enterostomal Therapists, Journal of Wound, Ostomy and Continence Nursing, and Ostomy Wound Management]. Detailed construction of these search strategies is attached in Supplementary Material: Supplementary Appendix A1.
CPGs met the following criteria: (1) Align with the definition by the Institute of Medicine 19 ; (2) appear in the most recent publication versions; if a new version of CPG had been published, the old version was excluded; (3) contain recommendations for the assessment, prevention, education, and management of PI in intensive care unit (ICU) patients undergoing PPV; and (4) written in English language.
Data extraction
Two independent investigators extracted the required information, which included the guideline title, year of publication, organization, version, and scope. In addition, the investigators collected information regarding the recommendations for prevention and management of PI for ICU patients undergoing PPV. We screened the full texts to identify the included CPGs/consensus. Disagreements were resolved by consensus or a third reviewer.
Assessment of guideline quality
Four independent reviewers used the AGREE II and the RIGHT guidelines to evaluate the quality of the CPGs. In cases of disagreements among the reviewers, resolution was achieved through discussions. The AGREE II instrument comprises 23 items categorized into six domains (scope and purpose; stakeholder involvement; rigor of development; clarity of presentation; applicability; editorial independence). 20 The reviewers were required to respond to the 23 items, with each entry graded on a 7-point scale, with a minimum score of 1 indicating strong disagreement and a maximum score of 7 indicating strong agreement based on the AGREE II examples and instructions. Subsequently, each domain score was normalized to a percentage based on the following formula found in the AGREE II manual: (score obtained–minimum possible score)/(maximum possible score–minimum possible score) × 100%. The overall domain scores were calculated for each guideline, with domain score ≤50% defined as poor, 50% to 70% defined as satisfactory, and ≥70% defined as excellent. 21 The overall assessment was classified into three categories as follows: recommended, recommended with modifications, and not recommended. 22
The reviewers then independently appraised the reported quality of CPGs using RIGHT, which consists of 22 items, including seven fields (basic information, background, evidence, recommendations, review and assurance, funding, declaration, and management of interests, and content). 23 Based on the content of report, each item was graded “Yes” (information about the item is presented completely), “Partial” (information about the item is presented partially), and “No” (information about the item is completely missing) for each item evaluated.
Data synthesis and analysis
For the included CPGs, the AGREE II score for each domain was presented as the percentage of the maximum possible score and standardized range, with the descriptive statistics being mean and standard deviation. Reported quality of data was presented in terms of the number of RIGHT Checklist items reported as per CPG and the number of CPGs reported for a single RIGHT Checklist item. Raincloud plotting and bubble plots were developed using R software (4.4.2) and posit (Rstudio) (v2024.12.0–467).
Intraclass correlation coefficients (ICCs) were used to assess the consistency of agreement among researchers. The values of ICC range between 0 and 1, with 0 denoting untrustworthy and 1 denoting completely reliable. The degree of agreements less than 0.4 were considered as poor consistency, 0.45 to 0.75 as good consistency, and greater than 0.75 as high consistency. 24 Statistical Package for Social Science version 25.0 software was used to analyze all statistical data.
RESULTS
Study selection
A total of 5,708 records were retrieved from the online databases, whereas 4 records were retrieved from other sources. After screening for duplicates, we excluded 3,093 records based on their titles, abstracts, and full text. An additional 2,606 records were excluded for the following reasons: 2,597 did not meet the guideline definition according to the Institute of Medicine, and 11 did not contain recommendations on prevention and management of PI-related PPV. Subsequently, 13 CPGs were eligible for review. The detailed search results of the CPGs are presented in Fig. 1.14,25–36
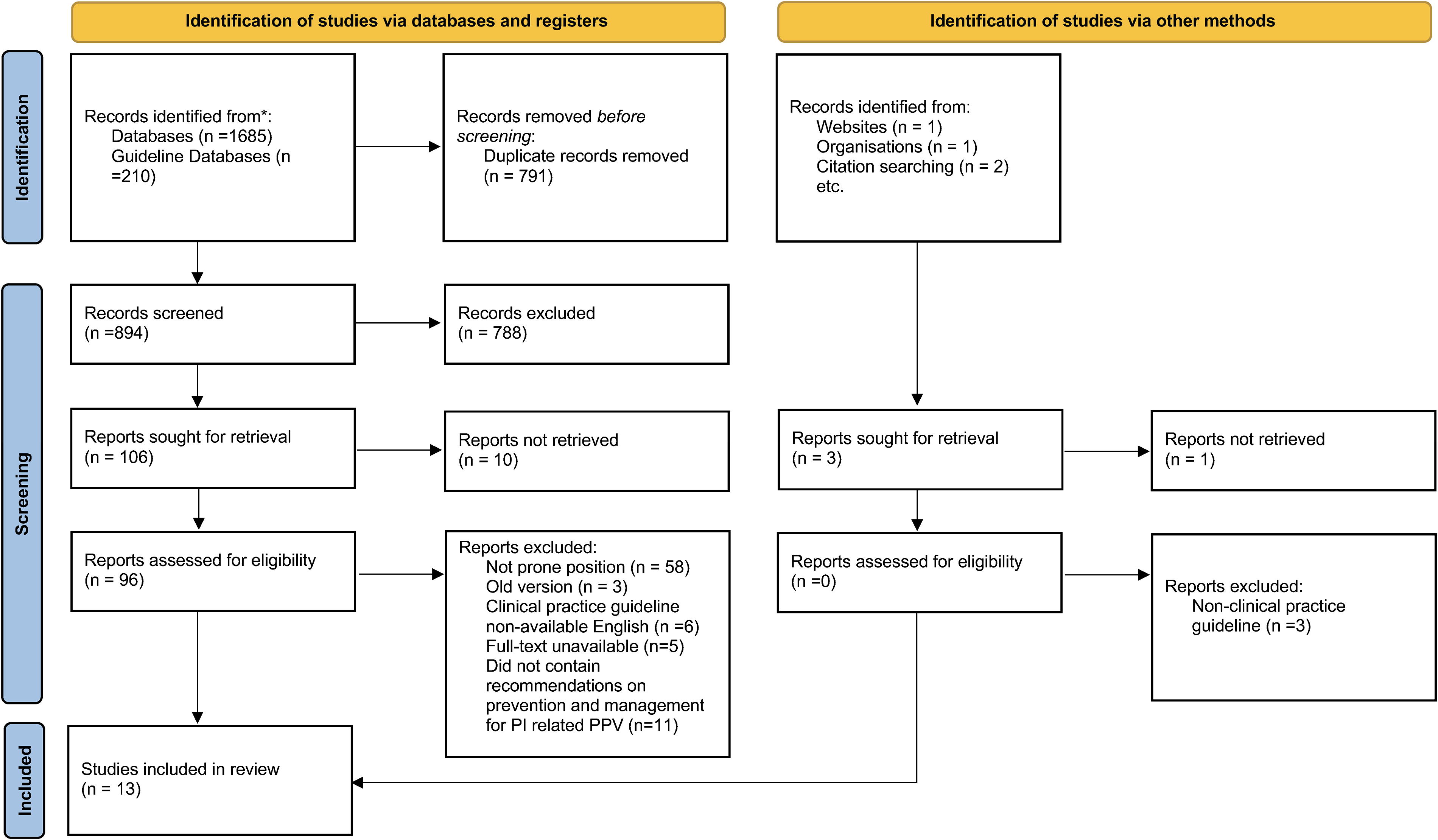
Flowchart of selection process for CPGs. CPGs, clinical practice guidelines.
Characteristics of included CPGs
Seven CPGs14,25–27,30,34,35 were focused on PI or pressure ulcer treatment, whereas the rest focused on the treatment of ARDS and included recommendations for the prevention and management of PI in patients undergoing PPV. Notably, seven CPGs14,25,26,28,30,33,35 were from different pressure ulcer/wound societies, four CPGs27,29,34,36 were developed by the professional CPG development organizations, and two CPGs31,32 were from medical or health centers. In addition, these CPGs were published between 2010 and 2022, with 10 guidelines14,25–27,29,31–33,35,36 being the original versions and three guidelines28,30,34 being updated versions (Table 1).
Characteristics of included clinical practice guidelines
Grading systems and methods for guideline development
Among the included 13 CPGs, 614,26–28,31,32 used the grading system to assess the level of evidence, recommendation grade, and recommendation classification. Notably, three CPGs used the27,31,32 GRADE system. The level of evidence was determined by the study design, with most grading systems evaluating the strength of recommendations based on the quality of the supporting evidence (Table 2).
Grading systems and methods for guideline development a
The grading system was developed according to the Ottawa Panel for alphabetical grading system and to the Cochrane Collaboration for international nominal grading system.
The level of evidence is based on the type of study.
Not reported sources of recommended ratings were reported.
Grade of recommendation depending on the quality of evidence; Class I = There is evidence and/or agreement of expert opinion that a procedure or treatment is beneficial and effective with greater benefit than harm Is indicated and recommended; should be done; Class II = There is limited evidence and/or agreement of expert opinion that a procedure or treatment can be beneficial and effective with greater benefit than harm may be indicated; is reasonable to perform; may be considered; Class III = Evidence and/or agreement of expert opinion about a procedure or treatment is less well established or uncertain and has conflicting evidence or divergence of opinion about the benefit and effectiveness, or there are risks/side effects that may limit benefit may be reasonable; may be considered in select instances; Class IV = There is evidence and/or agreement of expert opinion that a procedure or treatment is not beneficial or effective, and/ or can be harmful in some cases where risks/side effects outweigh the benefit is not indicated or recommended; should not be performed.
AAWC, Association for the Advancement of Wound Care; EPUAP/NPIAP/PPPIA, European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel, and Pan Pacific Pressure Injury Alliance; NICE, National Institute for Health and Care Excellence; AICM, German Society of Anaesthesiology and Intensive Care Medicine; CCHS, Christiana Care Health Service; TVS2022, Tissue Viability Society (2022); POM, Peri-Operative Medicine; AIC, Department of Anesthesiology and Intensive Care; ICU&ICS, intensive care unit and intensive care society; RNAO, Registered Nurses’ Association of Ontario; TVS 2016, Tissue Viability Society (2016); CAN, Chinese Nursing Association; WOCNS, Wound, Ostomy and Continence Nurses Society; TFC, Task Force Consensus; GPS, Good Practice Statement.
Analysis and grading of the methodological and reporting quality of CPGs
The AGREE II quality scores of domains ranged from 0.33 to 0.88, see Figure 2. Among the included CPGs, the domain with the highest mean score was the scope and purpose with 73.65 ± 10.91, followed by clarity of presentation domain with a mean score of 72.36 ± 15.85. The lowest score was the editorial independence domain with a mean score of 49.79 ± 19.49. Based on the CPGs overall mean score, four CPGs25,28,29,34 were identified as “excellent” and thereby classified as recommended for clinical practice. Seven CPGs26,27,30–33,36 were identified as “satisfactory” and, subsequently, classified as recommended with modifications. In addition, two CPGs14,35 were identified as “poor” and were classified as not recommended (Table 3).
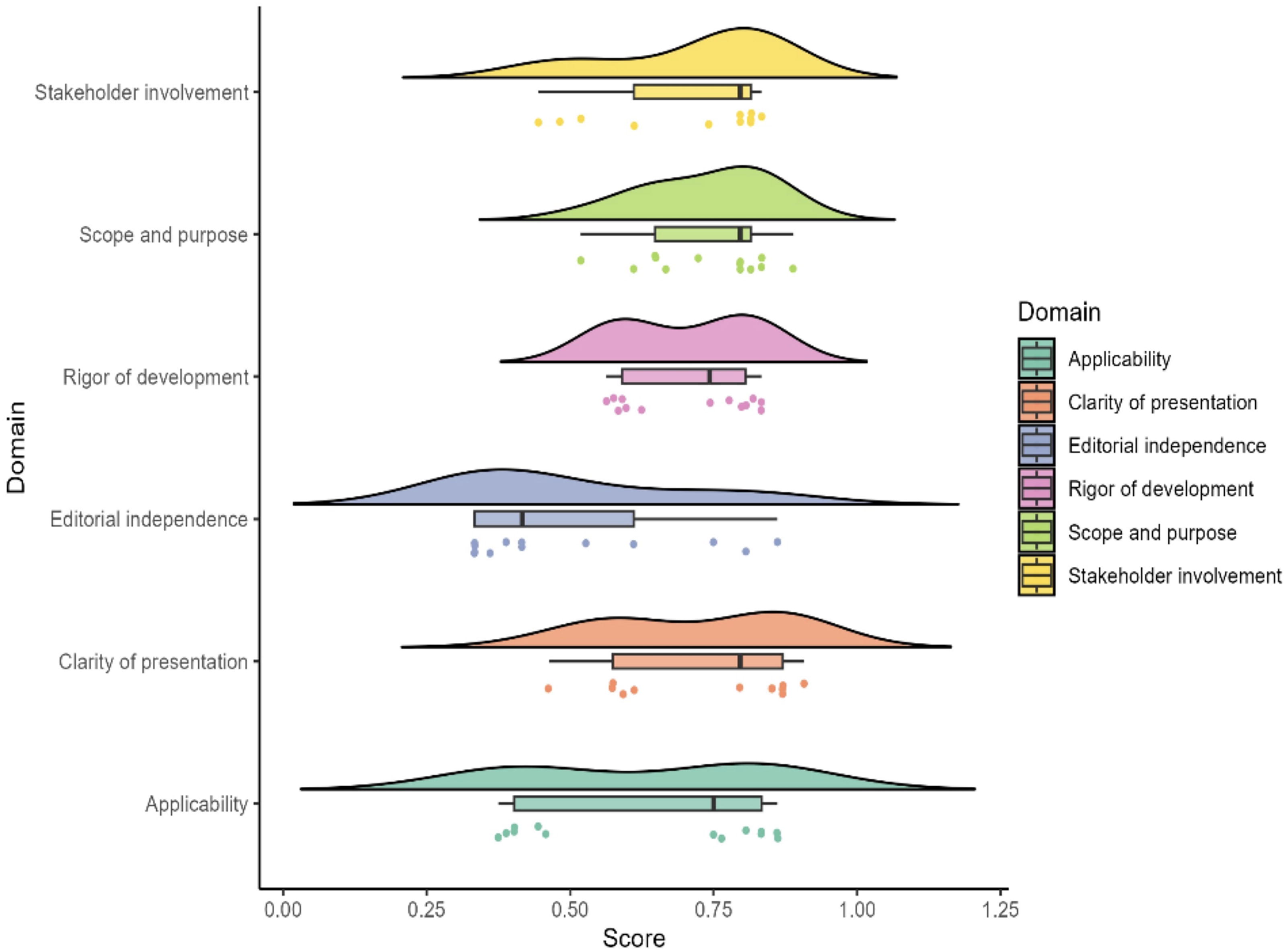
AGREE II assessment by domain of 13 guidelines. The raincloud plot with mean score ±95% CI comprehensively depicts the distribution of the AGREE II score of the guidelines in each domain. Each dot exhibits the standard value combined assessment of four researchers concerning each guideline. AGREE II, Appraisal of Guidelines Research & Evaluation.
Standardized scores of guidelines by Appraisal of Guidelines Research and Evaluation instrument
Domain score classification: Red (#FF0000) = “poor”; Green (#32CD32) = “excellent”; Yellow (#FFFF00) = “satisfactory.”
Scope and purpose: The overall objective(s) of the guideline is(are) specifically described; the clinical question(s) covered by the guideline is(are) specifically described; and the patients to whom the guideline is meant to apply are specifically described.
Stakeholder involvement: The guideline development group includes individuals from all the relevant professional groups; the patients’ views and preferences have been sought; target users of the guideline are clearly defined; and the guideline has been piloted among end users.
Rigor of development: Systematic methods were used to search for evidence; the criteria for selecting the evidence are clearly described; the methods for formulating the recommendations are clearly described; the health benefits, side effects, and risks have been considered in formulating the recommendations; there is an explicit link between the recommendations and the supporting evidence; the guideline has been externally reviewed by experts before its publication; and a procedure for updating the guideline is provided.
Clarity of presentation: The recommendations are specific and unambiguous; the different options for management of the condition are clearly presented; and key recommendations are easily identifiable.
Applicability: The guideline is supported with tools for application. The guideline is editorially independent from the funding body; conflicts of interest of guideline development members have been recorded; the potential cost implications of applying the recommendations have been considered; and the guideline presents key review criteria for monitoring and/or audit purposes.
Editorial independence: The guideline is editorially independent from the funding body; and conflicts of interest of guideline development members have been recorded.
AAWC, Association for the Advancement of Wound Care; EPUAP/NPIAP/PPPIA, European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel, and Pan Pacific Pressure Injury Alliance; NICE, National Institute for Health and Care Excellence; AICM, German Society of Anaesthesiology and Intensive Care Medicine; CCHS, Christiana Care Health Service; TVS2022, Tissue Viability Society (2022); POM, Peri-Operative Medicine; AIC, Department of Anesthesiology and Intensive Care; ICU&ICS, intensive care unit and intensive care society; RNAO, Registered Nurses’ Association of Ontario; TVS 2016, Tissue Viability Society (2016); CAN, Chinese Nursing Association; WOCNS, Wound, Ostomy and Continence Nurses Society; R, recommendation; RM, recommendation with modifications; NR, not recommended; SD, standard deviation.
The RIGHT checklist comprises 22 items divided into 7 domains with a total of 35 items. Tissue Viability Society (2022) (TVS2022) CPGs 30 demonstrated the highest number of reported items, 29, using RIGHT checklist, followed by Registered Nurses’ Association of Ontario (RNAO) CPGs, which exhibited 26 items. Among the seven domains of RIGHT checklist, field one (basic information) demonstrated the highest reporting rate (65.38%) and field six (funding, declaration, and management of interest) exhibited the lowest reporting rate (34.62%) (Supplementary Appendix A2).
The ICC analysis demonstrated very good agreement among the four reviewers, with the inter-rater agreement scores based on AGREE-II quality appraisal as follows: “Scope and purpose” (median 89%, range: 60–96%), “Stakeholder involvement” (median 93%, range: 91–95%), “Rigor of development” (median 96%, range: 98–100%, Supplementary Appendix A2), “Clarity of presentation” (median 92%, range: 54–96%), “Applicability” (median 88%, range: 81–99%), and “Editorial independence” (median 86%, range: 75–97%) (Table 4).
Inter-rater agreement for Appraisal of Guidelines Research and Evaluation quality appraisal
ICC, intraclass correlation coefficient.
Summary of prevention and management of PI in patients undergoing PPV recommendations
A summary of the recommendations is presented in Table 5 and Fig. 3. In addition, descriptive statistics analysis of all CPG recommendations is presented in Supplementary Appendix A2. Six CPGs14,25–27,30,34 recommended that greater attention should be given to risk factors and risk assessment for prevention and management of PIs. Skin and tissue factors should be addressed in a timely manner as recommended by four CPGs.25–27,36 These skin and tissue factors comprise anatomical location, size, and exudate type. Association for the Advancement of Wound Care (AAWC) 25 and EPUAP/National Pressure Injury Advisory Panel (NPIAP)/Pan Pacific Pressure Injury Alliance (PPPIA) guidelines 26 recommended implementation of a skin care regimen to prevent PI. The CPGs published by TVS2022, ICU &Intensive Care Society, Tissue Viability Society (2016) (TVS2016), and WOCNS14,30,33,35 advocated for the safe use of medical devices in clinical practice. CPGs from AAWC, EPUAP/NPIAP/PPPIA, NICE, and WOCNS14,25–27 proposed that wound dressing should be examined regularly for appropriateness and be modified as necessary to optimize wound healing. Recommendation from AAWC guidelines 25 indicated that excess moisture at the affected sites must be removed and managed with care. CPGs developed by AAWC, 25 EPUAP/NPIAP/PPPIA, 26 NICE, 27 and WOCNS 14 recommended monitoring and assessing the wound on a regular basis and at every dressing change to determine whether the type of dressing is appropriate or should be modified. Three CPGs recommended selecting support surface that meets an individual’s need for pressure redistribution, taking into account the identified risk factors.14,26,36 The CPGs published by EPUAP/NPIAP/PPPIA 26 and German Society of Anaesthesiology and Intensive Care Medicine(AICM) 28 proposed that greater attention should be accorded to medical device-related pressure injury (MDRPI), as well as regular monitoring of the tension of medical device fixtures, to ensure optimal performance and related complications. Six CPGs28,29,31,33,35,36 recommended that patients must be securely positioned when applying the PPV technique, with appropriate restart of the mattress pump whenever necessary. Guidelines published by AAWC and RNAO recommended use of a consistent, valid, and reliable tool tailored to an individual’s cognitive ability for assessing PI pain during examinations, with ongoing pain monitoring at subsequent visits.25,34 According to AICM guidelines, 28 an adapted analgosedation (Richmond Agitation Sedation Scale [RASS-Score] ≤−2) is necessary for the rotational maneuver to prevent coughing, compaction, or regurgitation; after positioning the maneuver, the analgosedation is reduced. CPGs published by AAWC, 25 EPUAP/NPIAP/PPPIA, 26 NICE, 27 Chinese Nursing Association (CAN), 36 and WOCNS 14 recommended that a comprehensive nutrition assessment must be conducted for all adults at risk of PI, with significant emphasis on those identified to be at risk of malnutrition. CPGs published by Christiana care health service (CCHS) 29 and RNAO 34 proposed the development and implementation of a comprehensive and sustainable interprofessional PI education program for medical staffs.

Different contents covering prevention and management of PI for patients with PPV recommendations and quality assessment of guidelines and consensus based on AGREE II. The size of the circle represents the number of recommendations; as the number increases, the circles become larger. PI, pressure injury; PPV, prone position ventilation; AGREE II, Appraisal of Guidelines Research & Evaluation.
Recommendations for prevention and management of pressure injury in patients with prone position ventilation a
Red (#FF0000), no grade provided; Green (#32CD32), strong recommendation; Blue (#87CEFA), moderate recommendation; Yellow (#FFFF00), low recommendation; Orange (#FFA500), expert or statement.
Details on prevention and management recommendations of pressure injury in critically ill patients undergoing prone position ventilation are provided in Supplementary Appendix A1.
AAWC, Association for the Advancement of Wound Care; EPUAP/NPIAP/PPPIA, European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel, and Pan Pacific Pressure Injury Alliance; NICE, National Institute for Health and Care Excellence; AICM, German Society of Anaesthesiology and Intensive Care Medicine; CCHS, Christiana Care Health Service; TVS2022, Tissue Viability Society (2022); POM, Peri-Operative Medicine; AIC, Department of Anesthesiology and Intensive Care; ICU&ICS, intensive care unit and intensive care society; RNAO, Registered Nurses’ Association of Ontario; TVS 2016, Tissue Viability Society (2016); CAN, Chinese Nursing Association; WOCNS, Wound, Ostomy and Continence Nurses society; AGREE II, Appraisal of Guidelines Research and Evaluation.
DISCUSSION
A total of 13 CPGs were identified in this review of CPGs on prevention and management of PIs for patients undergoing PPV. The quality of the included CPGs was varied as determined by the CPGs evaluation criteria applied. The quality of CPGs published by AAWC, AICM, CCHS, and RNAO was relatively high.
This study conducted a systematic review of the CPGs to identify challenges in the prevention and management of PIs in undergoing PPV. However, discrepancies were noted in the recommendations from several important organizations, highlighting conflicts in the guidelines regarding certain aspects of PI prevention and management. Discrepancies exist in several areas, including: (1) The current guidelines fail to identify the optimal choice for healing wounds; (2) dressing selection; (3) ventilation time for prone position; and (4) RASS-Score.
Assessment of risk factors
Risk assessment for prevention and management of PIs in patients undergoing PPV included environmental, medical, and psychosocial factors, body mass index, skin, friction, and shear potential. In addition, individuals with limited mobility and activity as well as or other factors that lead to a high potential for PI development should be considered for evaluation since friction and shear increase the risk of PI. A study conducted by Tschannen et al. 37 demonstrated that risk assessment can be used to determine risk potential, leading to proper implementation of PI prevention interventions. Braden scale, as well as Norton and Waterlow scales, is recommended for use to assess the risk of PI development. However, a meta-analysis 38 asserted that the Braden Scale can only be used on limited patients, for example, it is only suitable for patients with a mean age <60 years, those hospitalized, and those of Caucasian origin. In terms of ethnicity, the Braden Scale demonstrated higher diagnostic accuracy in the Caucasian population than in Asian population. 38 The reason for this may be related to cultural difference; the Braden Scale, which was developed in the United States, might be more suitable to Caucasian population. However, previous study 39 has indicated that the Braden Scale has also been adapted for use among Black individuals. Consequently, further studies should be explored to determine the risk of using the PI Braden Scale for patients over 60 years of age and ethnicity. In addition, the study by Sato et al. 40 examined patients with coronavirus disease who were placed in the prone position in ICUs, utilizing the Braden Scale to assess risk factors for PI development. As the Braden Scale has demonstrated validity in predicting hospital-acquired PIs, their research statistically enhanced its predictive capability by incorporating assessments of sensory perception, activity level, mobility, nutrition status, and friction/shear to identify high-risk patients. Their findings indicated that the Braden Scale maintains equal applicability for coronavirus disease patients in the prone position.
Preventive skin care and moist management
The preventive skin care regimens include keeping the skin clean and properly hydrated, cleaning the skin promptly after incontinence, avoiding alkaline soaps and cleansers, and using isolation products to protect the skin from moisture. An evidence-based study conducted by Zhang et al. 41 indicated that preventive skin care regimen did not significantly improve the incidence of facial PI in patients undergoing PPV. Such a regimen significantly reduced the extent of facial PI, thereby effectively improving the quality of clinical care and outcomes for patients undergoing PPV. 41 Moisture management is also an important part of the preventive skin care regimen. The study 42 recommended placing cotton pads or absorbent pads under the patient’s head to absorb saliva or nasal secretions caused by the PPV, as well as using a mild emollient to maintain the skin’s moisture homeostasis. Patients undergoing PPV experience increased oral and nasal secretions. Notably, the inability to clear these secretions in a timely manner increases the risk of PI. 43 To address this issue, an edema measuring device can be used as an adjunct to routine clinical skin assessment.
Safe use of devices
Studies 44 have reported that MDRPI is a skin pathology with a high prevalence and incidence, 10% and 20%, respectively. Consequently, there has been focus on MDRPI prevention strategies. Severely ill patients inevitably contact a variety of medical devices during examination and treatment; therefore, measures should be taken to mitigate the harm caused by medical devices to patients and reduce the occurrence of PIs. A systematic review 43 reported that safe use of devices can be beneficial for MDRPI prevention. The result of study conducted by Smart et al. 45 also reported that the application of silicone-based dressings beneath N95 respirators represents a safe and effective intervention for preventing facial skin injuries while maintaining optimal mask seal performance. However, patients undergoing PPV are usually in a comatose state and are unable to self-assess safe use of devices. Therefore, medical staff should timely, accurately, and dynamically assess the skin status of patients to reduce the incidence of PI.46,47
Dressings
Dressing plays an important role on prevention of PI for patients undergoing PPV. This study’s findings 48 suggest that dressings can reduce the occurrence of PIs in critically ill patients. Four CPGs14,25–27advocated for preventive use of dressings to avoid direct contact between medical devices and the patient’s skin. Numerous types of dressings were designed to address various needs, such as hydrogel dressings to hydrate dry ulcers, foam dressing to absorb wound exudate, collagen dressings to improve wound healing rate and symptoms of inflammation, and platelet-derived growth and platelet-rich plasma factor to promote healing in category/stage III and IV PIs. However, the current evidence fails to identify the optimal choice for healing wounds. A meta-analysis by Zhang et al. 49 reported that foam and hydrocolloid dressings required the least healing time, and moist dressings were associated with fewer dressing changes. Geng et al. 50 concurred in their meta-analysis, also reporting that moist dressings are more effective than traditional dressings in the treatment of PIs. Therefore, it is advisable to select the most appropriate dressings consistent with abilities of caregivers, principles of PI care, patient needs, and PI status as determined through clinical assessment, including the diameter, shape, and depth of the PI.
Support surfaces
Support surfaces effectively manage friction, pressure, and localized microenvironments, which prevents localized contouring and continuous decompression, which are key measurements for the prevention of PI. CPGs published by WOCNS 14 recommended the use of appropriate support surfaces to redistribute pressure in adults and bariatric patients in care settings where the length of hospitalization greater than or equal to 24 h prevent PI occurrence. Previous studies51,52 explored the roles of various types of support surfaces and reported as follows: reactive air surfaces reduce the risk of PI and promote complete healing of ulcers; alternating pressure air surfaces are cost-effective in preventing PI; and reactive gel surfaces are more effective in reducing PI occurrence for patients in the operating room or undergoing extended hospitalization. Therefore, an appropriate support surface should be selected based on the conditions of the patient and the performance of the support surface. Li et al. 53 advocated the use of a polyurethane gel cushion for head decompression in patients. However, horseshoe-shaped pillows and donut-shaped supports are contraindicated in cases of PPV patients, as they may elevate the risk of cervical spine injury and exacerbate localized facial pressure. 54 At the same time, the best evidence summary 55 on prevention of PI for critical patients recommended that support surfaces should be tested before use to ensure that they meet industry standards and have enough room for the patient to adjust their body comfortably.
Infection and biofilms
New research highlights the critical impact of PI microbiota on the persistence of chronic wounds and slowed recovery. 56 The major infectious complications that may arise from PI include cellulitis, abscesses, osteomyelitis, and bacteremia. 57 Bacteremia is an uncommon complication of PI, which is mainly caused by Staphylococcus aureus, Proteus spp., and Bacteroides spp. 58 This is because the pressure ulcer may contribute to multidrug-resistant microorganisms, especially methicillin-resistant S. aureus, which are at risk for bacteremia. 59 Although bacteremia associated with pressure ulcers is a rare complication, it can lead to severe morbidity. A prospective observational cohort study 58 of patients with bacteremia associated with pressure ulcers reported that the overall mortality was 41.1%. A tissue biopsy or Levine quantitative swab technique can be used to determine the bacterial bioburden.
Nutrition assessment and treatment
Nutrition management of patients with PPV could prevent PI, promote the healing at the ulcer site, and reduce microbial infections. 60 The results of nutritional screening can be used to modify the nutritional intake, and a program that meets 60 − 80% of nutrient intake is recommended in the early stages. Energy and nutrient intake need to be gradually increased following remission of the disease. 14 Current evidence and clinical guideline61,62 underscore the growing significance of early enteral nutrition (EN) in mechanically ventilated patients maintained in the prone position. Emerging findings 63 indicate that structured nutritional protocols—such as postpyloric feeding, strict head-of-bed elevation, vigilant monitoring of gastric residuals, and titration of feeding rates—may enhance EN tolerance in this population. Furthermore, critical care nursing staff must remain cognizant of the elevated risk of gastroesophageal reflux and aspiration in prone-positioned patients. 64 Consequently, specialized training is imperative to ensure proper head positioning, continuous feeding assessment, and early recognition of EN-related complications.
Management of prone position and pain
The CPG published by AICM 28 and CAN 36 suggested before the prone position ventilation, nasal cavities, and airway secretions should be adequately cleared, and the patient should be ventilated with pure oxygen on a ventilator for 2 min to stabilize the patient’s hemodynamics and balance the volume status.
Currently, there are no standard guidelines regarding the optimal duration of prone ventilation. The study 65 used repeated prone ventilation for 6–8 h a day or prolonged prone ventilation for 17–20 h a day. The longer the duration of patients with PPV, the higher the incidence of PI. 5 Therefore, the patients should be turned slightly (20°−30°) intermittently for at least 2 h during the prone ventilation, especially those who are ventilated in the PPV for prolonged periods of time.
Besides, attention should also be given to the sedation of patients with prone position ventilation. AICM CPG 28 recommended that adapted analgosedation is necessary for prone patients, RASS score ≤−2 to avoid coughing, compaction, or reflux. However, expert consensus 66 of nursing care of patients with PPV suggested maintaining a RASS score of −3 to −4. Further research is needed to investigate sedation scores in patients with PPV. Pain management is essential to prevent agitation, which can increase skin friction and shear and, consequently, elevate the risk of PI. 66 A study conducted by Zhang et al. 41 reported that the incidence of PI in patients with PPV was 16.7%, which may be associated with poor analgesic sedation, patient agitation, and increased skin friction.
Team and education programs
Health care professionals often have limited knowledge, skills, and practices related to the assessment and management of PI in patients with PPV. Implementing training programs can enhance their understanding of PPV-related PI prevention, leading to improved identification and management and, ultimately, reducing the incidence of these injuries. The CPGs25,26,34 recommended development of an organized, structured, and comprehensive health care worker training program and implement it among health care workers, patients, families, and all nurses to prevent and treat PI. In addition, CPG developed by WOCNS 14 suggested that the content of the training program should include developed and risk factors for PI and ways to reduce the risk, as well as strategies to prevent PI, promote healing, and prevent ulcer recurrence. Therefore, to implement the training program, educational training should be based on real-life scenarios for health professional and clinical practice exercises for specific PPV and followed up regularly to ensure the effectiveness of the training in terms of the relevant knowledge, attitude, and practices. 67
CONCLUSION
This systematic review synthesizes and evaluates existing guidelines for preventing and managing PIs in critically ill patients undergoing PPV. The findings provide clear clinical recommendations as follows: adhering to CPG guidelines can improve PI prevention and management, whereas evidence mapping can enhance knowledge translation and reduce research waste. The overall quality of the included CPGs for the prevention and management of PI among patients undergoing PPV was moderate, and there were inconsistencies in some recommendations. However, this study has some limitations. Some guidelines did not explicitly rate the evidence or specify the strength of their recommendations. In addition, the evidence coding system used in these guidelines made it challenging to identify the specific components of the evidence supporting each recommendation and to conduct further research. In the future, well-powered randomized controlled trials should be conducted to improve the evidence bases.
Footnotes
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
No funding was received for this article.
ABOUT THE AUTHORS
SUPPLEMENTARY MATERIAL
Supplementary Appendix
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.