
Abstract
Objectives:
To elucidate the global disease burden and care quality associated with pressure injury (PI).
Approach:
This study examined temporal trends in PI incidence over the past 32 years. Decomposition analysis attributed these trends to demographic and epidemiological shifts, and cross-national health inequities were quantified. The Quality of Care Index (QCI) was constructed using principal component analysis to assess spatiotemporal variations in global PI care quality. A log-linear age-period-cohort model was employed to forecast trends over the next 15 years.
Results:
In 2021, there were nearly 2.47 million PI cases globally, a 115.92% increase from 1.14 million in 1990. Decomposition analysis revealed that population aging and demographic growth were the primary drivers of increasing PI incidence. Lower QCI was concentrated in African countries and those with low sociodemographic index (SDI). Incidence rates increased gradually with improving SDI. Significant health inequalities existed among 204 countries and regions, with minimal changes in inequality slope indices over time. Projections indicate a gradual increase to 3.5 million PI cases globally by 2035.
Innovation:
This study developed a novel comprehensive indicator, the QCI, and for the first time, shed light on health inequalities in PI across 204 countries and territories.
Conclusion:
Over the past 32 years, the global disease burden of PI has been significant, accompanied by health inequalities across countries and regions. For nations with low SDI, there remains considerable room for improvement in the quality of care for PI, necessitating more effective strategies to address health care disparities.
Zhen Yang

Li Zhou

INTRODUCTION
Pressure injury (PI), defined as localized damage to the skin and underlying soft tissue resulting from impaired blood flow due to pressure, is typically caused by intense or prolonged pressure, shear, or friction forces. 1 Global disease burden data indicate that in 2019, the number of incident PI cases reached 850,000. 2 Among adult hospitalized patients, the prevalence of PI was 12.8%, with an incidence rate of 5.4 cases per 10,000 patient-days. 3 The most common stages of skin compromise observed were Stage I and Stage II. 3 The body regions most frequently affected were the sacrum, heels, and hips. Research demonstrates that PI adversely impacts patient outcomes, including elevated infection rates, increased mortality risks, prolonged hospital stays, compromised quality of care, and escalated overall hospitalization costs. 2,4 In the United States, annual health care expenditures associated with PI are estimated at approximately US$10 billion, highlighting PI as a substantial burden for both patients and the health care system. 5
Numerous factors suggest that the epidemiology of PI may have shifted since the onset of the coronavirus disease 2019 (COVID-19) pandemic. Critically ill COVID-19 patients are exposed to PI risk factors such as immobility, reduced perfusion, and the use of medical devices such as ventilators and masks. 6 Patients on mechanical ventilation often require head-of-bed elevation to facilitate respiration, shifting more pressure to the sacrum and potentially elevating their PI risk. 7 Additionally, prone positioning, widely employed for treating acute respiratory distress syndrome in COVID-19, has been recognized as a leading cause of PI complications. 8 –10 Furthermore, diarrhea, a common symptom in COVID-19 patients, 11,12 may contribute to an increased incidence of sacral PI. 13 Studies have confirmed that thrombosis and inflammatory responses triggered by severe acute respiratory syndrome coronavirus 2 infection can lead to cutaneous vascular thrombosis and tissue ischemia, further augmenting the risk of developing PI. 14 –16 For elderly COVID-19 patients, chronic illnesses, malnutrition, and mobility impairments compound their vulnerability to PI. 17
In the aftermath of the COVID-19 pandemic, the Global Burden of Disease (GBD) framework has refined its analysis of health determinants, conducting systematic and up-to-date assessments of the burden by cause, age, sex, location, and year to better comprehend the shifts in disease burden subsequent to the emergence and widespread transmission of COVID-19. 18 To date, only a handful of studies have investigated the current burden of PI at the national level, exploring incidence, prevalence, and disability-adjusted life years (DALYs) associated with PI. 19,20 Notably, epidemiological reports from select countries do not adequately represent the global PI burden. 21 A notable study, which examined PI incidence across 204 countries and territories from 1990 to 2019, introduced years lived with disability (YLD) and age-standardized rate (ASR) as novel metrics to describe the PI burden. However, this study relied on data from the GBD 2019 database, inherently incorporating a time lag in its findings. 2
However, previous research has overlooked the indices of care quality and transnational health disparities among patients with PI. The epidemiological landscape of PI has become increasingly complex, influenced by factors such as the COVID-19 pandemic and population aging, necessitating urgent exploration of the current PI burden and quality of care. Inequality is defined as the avoidable differences in health outcomes between different population groups. 22 The United Nations 2030 Agenda for Sustainable Development, adopted in 2015, embodies the ongoing commitment of the World Health Organization (WHO) and global development partners to addressing inequality. At its core, this agenda strives to reduce inequalities within and between countries. 23
In summary, the existing literature on the global burden of PI necessitates an update. The present study aims to delineate the trends of PI from 1990 to 2021 at the global, regional, and national levels, analyze cross-national health inequalities, and forecast changes until 2035.
INNOVATION
This study introduces the Quality of Care Index (QCI) to evaluate the spatiotemporal disparities in the quality of care for patients with PI over time and explore its potential for improvement. Additionally, the study innovatively addresses and explores health inequalities in the field of wound care, providing quantitative assessments. Furthermore, a decomposition analysis of the factors influencing the incidence of PI was conducted to explore the specific contributions of population growth, aging, and epidemiological factors to the disease burden of PI.
Clinical problem addressed
Given the COVID-19 pandemic and global aging, this study necessitates new measurements of the current disease burden for PI patients. It enhances the attention of frontline clinicians to the quality of wound care. The study also quantifies health inequalities across different countries and regions by predicting trends in cases and age-standardized incidence rates over the next 15 years. This research offers valuable insights into the global burden of PI, quality of care, and health disparities.
MATERIALS AND METHODS
Data sources
The data for this study were derived from the publicly accessible GBD 2021 database. A comprehensive analysis of PI data spanning 1990–2021 across 204 countries and territories was conducted using the GBD 2021 repository. The original data source is available at: https://www.healthdata.org/research-analysis/gbd. The specific codebooks used for PI estimation in the GBD study are accessible via: https://ghdx.healthdata.org/gbd-2021/code/nonfatal-13. Notably, no electronic laboratory notebook was utilized for data collection in this investigation.
This study examined temporal trends in the disease burden of PI over the past three decades, decomposing variations according to demographic factors (population aging and epidemiological shifts) to quantify cross-national health inequities. Projections of global incident cases and ASR over the next 15-year period were also generated. Following systematic organization and analysis of data from 21 GBD regions, stratified analyses were performed by region, sex, and the sociodemographic index (SDI). Key metrics extracted included PI case counts, ASR, the Quality of Care Index (QCI), and gender disparity ratios (GDRs).
Measures of Disease Burden
Data extracted from the GBD study were used to calculate incidence, prevalence, and mortality rates of PI using descriptive statistics, with 95% uncertainty intervals (UIs) derived from 1,000 posterior draws. The data were stratified and analyzed according to aging, population growth, and epidemiological shifts to quantify the proportional contributions of these factors to PI incidence trends over the past 32 years. ASR, with 95% confidence intervals (CIs), was computed using a log-linear regression model ([eβ − 1] ×100) to characterize long-term trends in PI disease burden. Additionally, the current state of care quality across age groups was evaluated by analyzing the QCI within 21 GBD super-regions and 5 SDI-stratified tiers. This analysis aimed to elucidate age-related disparities in care quality (Supplementary Data S1—Table 1).
The SDI, a composite metric integrating total fertility rate among women aged <25 years, mean years of education, and lag-distributed income per capita, was used to classify countries into five quintiles: high, high-middle, middle, low-middle, and low SDI. 24 The SDI facilitates cross-regional and temporal comparisons of societal development, with higher SDI values indicating superior socioeconomic conditions. 25,26
Statistical analysis
Estimation of the QCI
This study extracted and computed four ratio metrics for PI patients: mortality-to-incidence ratio, prevalence-to-incidence ratio, DALYs-to-prevalence ratio, and years of life lost-to-YLDs. These four ratios were integrated via principal component analysis to construct the QCI. Separate QCI values were calculated globally, across 5 SDI quintiles, and within 21 GBD regions, stratified by overall QCI and gender-specific QCI. The QCI is scored on a 0–100 scale, with higher scores indicating superior care quality.
Additionally, the GDR was computed as the ratio of female-to-male QCI values (GDR = QCI female/QCImale) to quantify gender-based disparities in PI care. A GDR of 1 denotes absolute gender parity, values <1 indicate better male care quality, and values >1 reflect superior female care quality. Relative changes in age-standardized QCI (AS-QCI) from 1990 to 2021 were calculated using the formula: Relative change (%) = [(AS-QCI2021−AS-QCI1990)/AS-QCI1990] ×100%. This analysis evaluated spatiotemporal disparities in global PI care quality over the 32-year period (Figs. 1 and 2; Supplementary Data S1—Table 2).
Decomposition analysis
The raw case data were stratified by age, population dynamics, and epidemiological shifts to quantify the contributions of population growth, aging, and epidemiological changes to PI incidence trends across 21 GBD regions and 5 SDI quintiles over the 32-year period. This analysis also explored the differential impacts of these factors on PI incidence by gender within each region (Fig. 3).
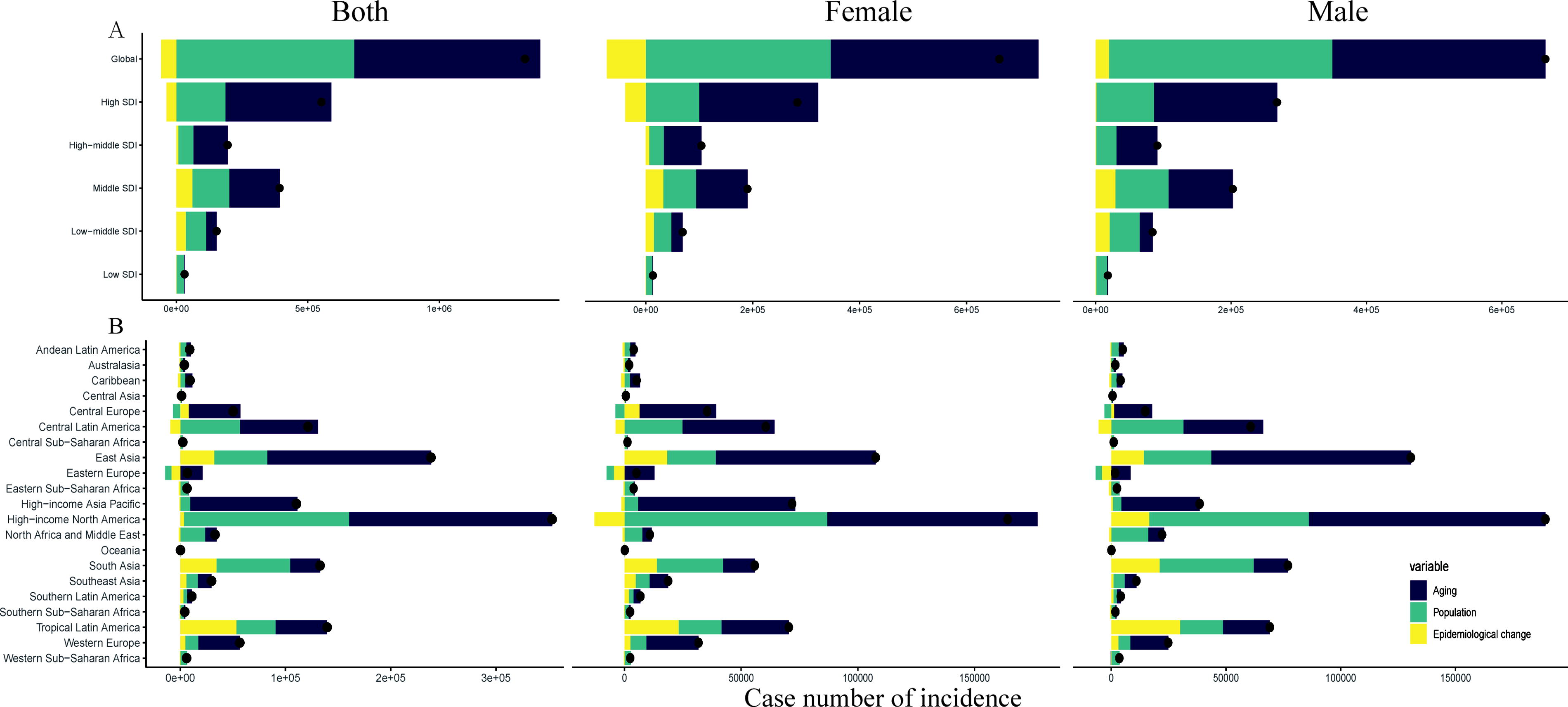
Changes in incidence of PI according to population-level determinants including aging, population growth, and epidemiological change from 1990 to 2021 at the global level and by SDI quintiles
Cross-national inequality analysis
Health inequality refers to measurable disparities in health outcomes between population subgroups defined by sociodemographic, economic, or geographic characteristics. 27 Measuring and monitoring health inequalities are critical for achieving health equity. While disaggregated data are commonly used to assess health disparities across subgroups, aggregated metrics of health inequality play a pivotal role in surveillance. The health inequality concentration index was computed by fitting the observed cumulative relative distribution of the population, stratified by SDI and disease prevalence rankings, to a Lorenz concentration curve and numerically integrating the area under the curve (Fig. 4).
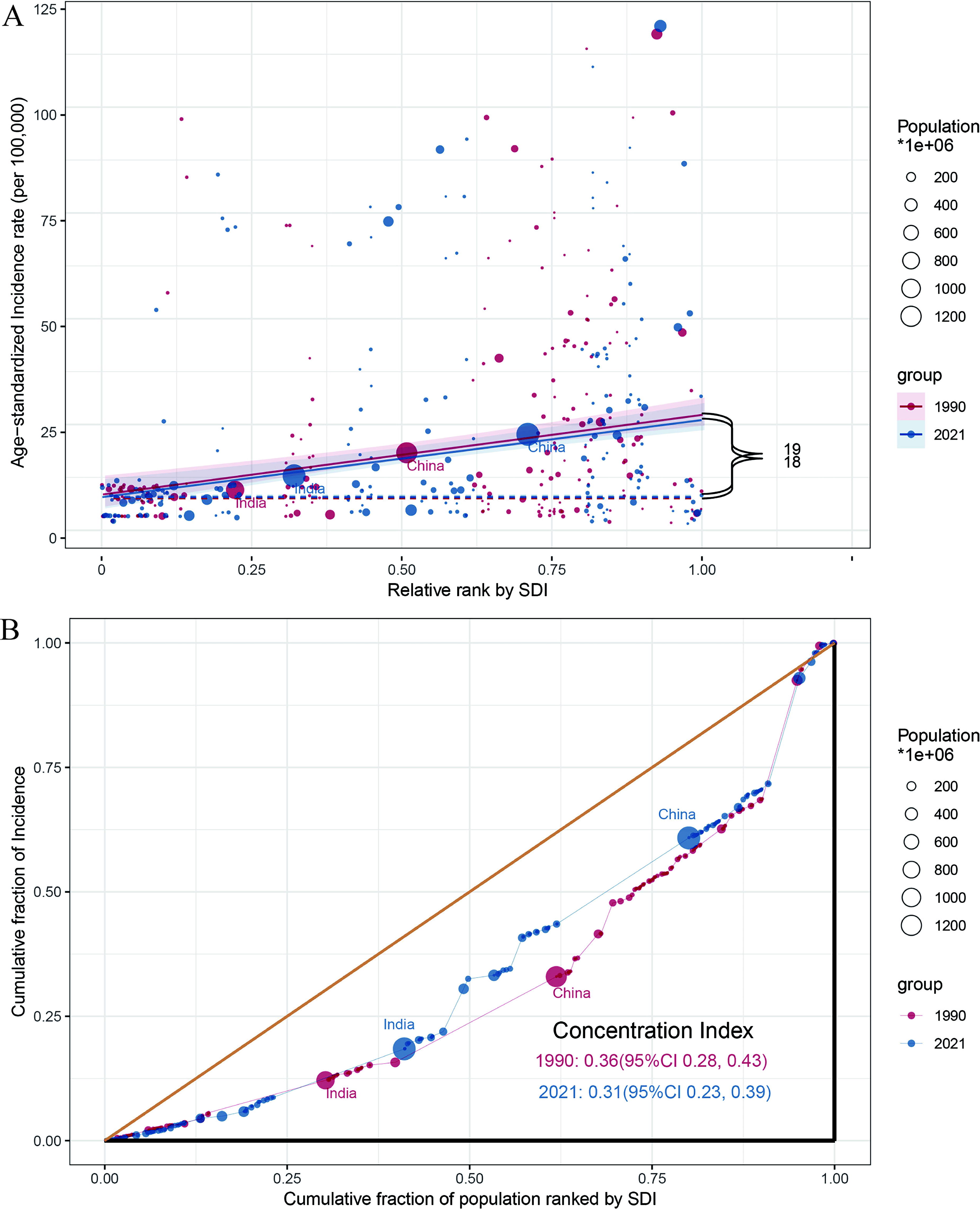
Health inequality regression curves
Predictive analysis
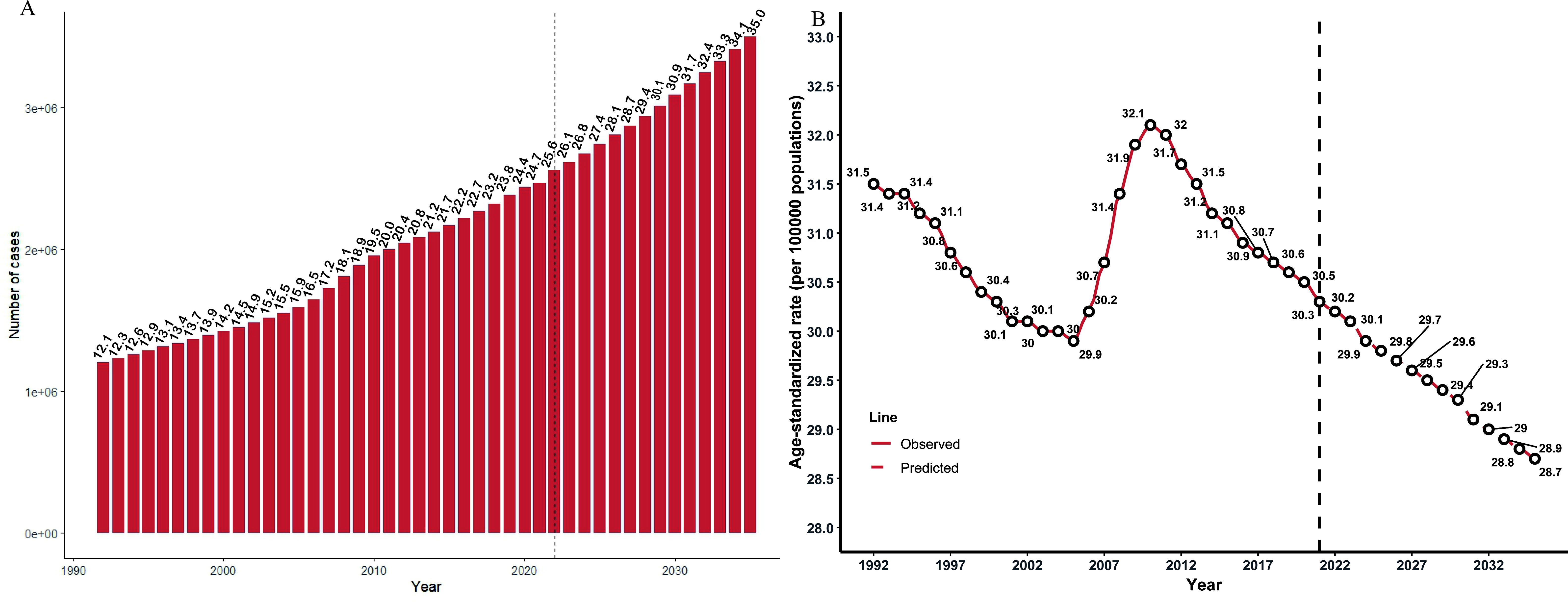
To project the number of new cases and incidence rates of PI from 2021 to 2035, this study employed a log-linear age-period-cohort model, which effectively controls for exponential growth trends and constrains linear trend projections. The model specification, estimation methods, and parameter estimates are detailed in the analysis. The model was implemented using the NORDTRED package in R software. Predicted disease incidence rates for 2035, derived from available data, were averaged and weighted and then applied to the corresponding United Nations population projections for that year to extrapolate case counts and ASR to 2035. Population forecasts and world standard population data were sourced from the Institute for Health Metrics and Evaluation population projections and GBD 2021, respectively 28 (Fig. 5).
Limitations of statistical methods
The findings of this study are entirely derived from data provided by the GBD database. Although the initial data processing methods accounted for known inconsistencies in the source data to the greatest extent possible, measurement errors and reporting inaccuracies persisted in the raw data collected. Moreover, the acquired data may be biased due to undiagnosed or misdiagnosed cases of PI. This study could not infer country-specific drivers of disease burden or disparities in uneven development using macro-level data alone. Given the limited confounding factors disclosed in GBD 2021 for stratification and adjustment, the results cannot exclude the potential influence of unreported confounders on the QCI. Additionally, this analysis did not account for other confounding factors that may affect QCI outcomes, such as variations in incidence rates across ethnic groups or regional heterogeneities.
RESULTS
Trend analysis
The global incidence of PI in 2021 stood at 2,468,317.5 cases (95% UI 2,255,077.3–2,720,436.7), marking a substantial increase of 115.92% from 1,142,594.8 cases (95% UI 1,030,311.6–1,276,015.9) reported in 1990. Furthermore, the global ASR of PI demonstrated a slight decline, from 31.5 (95% UI 28.4–35.2) in 1990 to 30.3 (95% UI 27.7–33.3) in 2021. Notably, while the ASR among males was marginally higher across the years, the absolute number of PI cases among females surpassed that of males. Substantial variations in ASR were observed across different SDI regions. Specifically, high SDI regions exhibited the highest ASR, with 56.2 (95% UI 50.8–63.1) in 1990 and 54.1 (95% UI 49.4–59.6) in 2021. Conversely, low SDI regions recorded the lowest ASR, increasing slightly from 7.8 (95% UI 6.9–8.9) in 1990 to 8.0 (95% UI 7.1–9.0) in 2021. Regionally, High-income North America consistently reported the highest ASR, with 115.7 (95% UI 103.6–130.1) in 1990 and 115.5 (95% UI 105.1–126.7) in 2021. In contrast, Western Sub-Saharan Africa had the lowest ASR, at 3.4 (95% UI 2.9–3.9) in 1990 and 3.5 (95% UI 3.0–4.0) in 2021 (Supplementary Data S1—Table 1). Across a 32-year period and an analysis of ASR in 204 countries, 100 countries showed a decrease in their ASR, while 104 countries exhibited an upward trend.
QCI trend analysis
The global QCI for PI remained largely stable, with the index of 97.3 in 1990 and 97.4 in 2021. High SDI regions consistently recorded the highest QCI, with values of 98.4 in 1990 and 99.0 in 2021. In 2021, among the 21 GBD regions, High-income Asia Pacific recorded the highest QCI (QCI = 99.6). Lower QCI was concentrated in Africa, Southeast Asia, Oceania, and countries within low SDI regions. Notably, Eastern Sub-Saharan Africa had the lowest QCI, with values of 21.8 in 1990 and 25.1 in 2021 (Fig. 1; Supplementary Data S1—Table 2). From 1990 to 2021, most regions observed a slight upward trend in QCI, with Eastern Sub-Saharan Africa demonstrating the most notable improvement, increasing by 15.1% from 21.8 to 25.1. Analysis of QCI across 204 countries revealed that 89 countries experienced an increase in QCI since 1990, with Ethiopia recording the largest gain (19.55% increase). Conversely, 115 countries saw a decline, with Mauritius experiencing the most significant drop (17.54% decrease; Supplementary Data S2).
This study characterized regional QCI trends and age-stratified patterns across time. Analysis of QCI values for PI patients by age group in 21 regions for 1990 and 2021 revealed that in low SDI regions, the QCI improved among PI patients aged 0–79 years, while a declining trend was observed for those aged >80 years. Notably, lower QCI values were concentrated in the 0–5, 30–34, and >45 age groups. In Eastern Sub-Saharan Africa, Central Sub-Saharan Africa, and Oceania, patients aged 40–94 years exhibited significantly lower QCI values compared with other age groups (Fig. 2A, B).
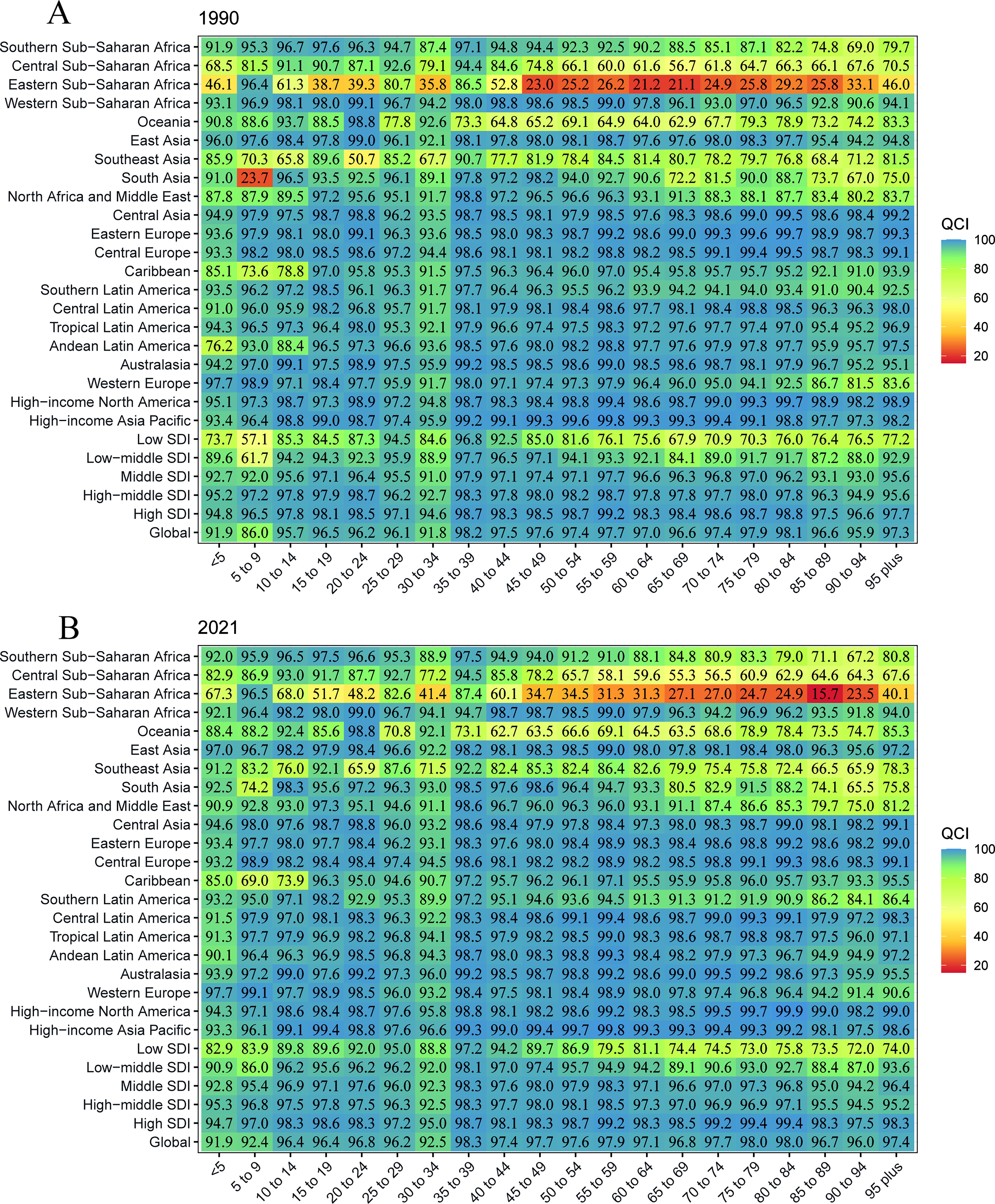
Impact of age on the Quality of Care Index for patients with PI, globally and across five SDI quintiles, 1990–2021. PI, pressure injury; SDI, sociodemographic index.
Trend analysis of gender differences
Globally, the overall global GDR has remained essentially unchanged over the past 32 years, with a GDR of 1.00 in both 1990 and 2021. By 2021, Oceania is the region with the highest GDR, at 1.15, and Southeast Asia is the region with the lowest GDR, at 0.94. Eastern sub-Saharan Africa, with a GDR of 1.53 in 1990, has the highest gender gap between men and women in the 21 GBD regions, whereas in 2021 the region’s GDR falls to 1.03, a decrease of 32.68%, and is in second place along with the Western sub-Saharan Africa region. In the low SDI region, the GDR has progressed from 0.98 in 1990 to 0.94 in 2021, indicating an increase in the gender gap in male orientation. Although there has been a slight reduction in the gender gap in female tendencies in Oceania over the past 32 years, the GDR for the region in 2021 is 1.15, which is the highest gender gap of all the regions (Supplementary Data S1—Table 2).
Decomposition analysis
Analysis of population-level determinants (aging, demographic growth, and epidemiological shifts) on PI incidence revealed that, globally, demographic growth and aging contributed 51.00% and 53.35%, respectively, to the rise in PI prevalence between 1990 and 2021. Irrespective of gender, population aging and growth emerged as the primary factors driving the rise in PI incidence. The impact of population growth was most pronounced in high SDI and high-middle SDI regions, contributing 33.78% and 35.76% to the observed trends, respectively. Aging’s contribution to the overall incidence was particularly evident in high SDI (73.06%), high-middle SDI (66.67%), middle SDI (48.83%), and low-middle SDI (25.96%) regions, with a lesser impact in low SDI regions (7.35%). Thus, the incidence of PI in high and high-middle SDI regions was primarily attributable to population growth and aging (Fig. 3A). In the examination of PI incidence cases across the 21 GBD regions, aging made substantial contributions to the overall incidence in Central Europe (98.07%), Central Latin America (61.11%), East Asia (65.29%), High-income Asia Pacific (92.22%), and High-income North America (54.60%). Demographic factors were most influential in Central Latin America (46.69%), High-income North America (36.76%), and South Asia (52.68%; Fig. 3B; Supplementary Data S3).
Analysis of transnational inequality
Study findings indicate that inequities in PI disease burden were significantly associated with the SDI, with minimal temporal variation in the slope index of inequality. When stratified by SDI quintiles, notable increases in ASR and cumulative incidence were evident across countries. Higher incidence rates were disproportionately concentrated in nations with higher SDI levels (Fig. 4A). Specifically, in 1990, the slope index of inequality was 19, indicating that the country with the highest SDI had 19 more cases per 100,000 population than the country with the lowest SDI. By 2021, this disparity had slightly narrowed to 18 cases per 100,000. Similarly, the concentration index declined from 0.36 in 1990 to 0.31 in 2021 (Fig. 4B).
Forecasting development trends
Between 1990 and 2021, the global burden of PI increased by over 1.32 million cases. Forecasts for the global PI disease burden from 2022 to 2035 indicate a projected rise in incident cases. Our predictive analysis reveals that, despite a further decrease in the global ASR by 2035 compared with 2021 estimates (Fig. 5B), the absolute number of incident cases will continue to escalate, surpassing 3.5 million by 2035 (Fig. 5A). Furthermore, the forecast of QCI across 204 countries and territories reveals a continued enhancement of the QCI in high-income developed nations, whereas lower QCI predominantly persists in African countries.
DISCUSSION
This study identified that the rapid increase in PI incidence is predominantly concentrated in relatively developed countries within high SDI, high-middle SDI, and middle SDI regions. In 2021, the United States and China ranked first and second globally in PI case counts, with 706,150 and 397,312 cases, respectively. A positive correlation was observed between the QCI and SDI, with high-SDI countries exhibiting significantly higher QCI values compared with low-SDI counterparts. This discrepancy may be attributed to the accelerated advancement of health care infrastructure in high-SDI regions, driving progress in disease mechanism research, diagnostic innovations, and advanced treatment modalities. 29 In China, expanded health care access correlates with increased life expectancy among older adults, 30 a factor contributing to reduced mortality rates—a key component of QCI calculation. Conversely, in resource-constrained settings, limited availability of treatment and care standards exacerbates regional disparities. Although global age-standardized QCI values have improved since 1990, countries in Africa (Zambia, Zimbabwe) and low-SDI regions continue to lag, underscoring substantial room for improvement. Widening income gaps undermine equitable health and social development, perpetuating disparities. 31 Socioeconomic inequities may result in inadequate diagnostic/treatment capacity or unaffordable care costs, hindering optimal care delivery. Reducing income disparities could enhance population health and well-being. WHO data reveal that African countries allocate only 48% of the international average to public health care expenditure. 32 PI burden exacerbates morbidity and mortality, particularly among elderly and long-term hospitalized patients, imposing additional financial strain on health care systems due to escalating treatment costs. In low-income countries, this funding pressure impedes investments in human resources, specialized PI management equipment, and professional health care teams, ultimately stagnating nursing quality improvements in underdeveloped regions.
Despite a moderate increase in the age-standardized QCI over the past 32 years, the global incidence of PI has surged dramatically, with a growth rate of 115.92%. Our analysis underscores aging and population growth as the primary drivers of this shift. External factors contributing to PI development include climate, environment, and violent conflicts, 33 while internal factors are intimately tied to the active or passive loss of mobility among patients, compounded by comorbidities such as advanced age, impaired tissue perfusion, and altered nutritional status. 34 A systematic review encompassing multiple studies identified age ≥65 years and diabetes as two decisive factors elevating PI incidence. 35 Currently, the primary preventive measure for PI involves repositioning patients every 2–3 h; however, research reveals that this interval often widens during routine care practices and shift changes, thereby contributing to PI development. 36 Furthermore, studies on COVID-19 patients have demonstrated widespread occurrence of PI, particularly among critically ill individuals, with a higher predisposition in those comorbid with diabetes, coronary artery disease, hypertension, chronic kidney disease, depression, and long-term use of nonsteroidal anti-inflammatory drugs. 37 The escalating incidence of PI globally imposes a formidable burden on health care systems. The increase in PI cases attributed to COVID-19 primarily stems from two mechanisms: PI induced by pressure from personal protective equipment (masks, goggles, and face shields) during infection prevention protocols and PI associated with prolonged prone positioning during intensive care, likely exacerbated by reduced repositioning frequency due to shortages in medical resources and nursing staff during the pandemic. Effectively preventing PI remains a paramount concern. A cross-sectional study reported that healthy diets and increased physical activity can significantly reduce PI incidence among patients. 14 The 2023 update to the World Health Surgical Safety Checklist guidelines advocates for enhanced risk assessment and pressure redistribution strategies to mitigate PI incidence by optimizing pressure redistribution, minimizing shear forces, and regulating microenvironmental conditions among high-risk patients. 38 To address PI escalation during pandemics, the use of prophylactic adjuncts—such as multilayered silicone foam dressings—is recommended to prevent sacral and coccygeal PI in patients with persistent severe diarrhea or fragile skin. The United Kingdom’s National Wound Care Strategy Program issued COVID-19-specific PI management guidelines emphasizing interdisciplinary collaboration to facilitate effective PI prevention and healing. 39 Additionally, elucidating the mechanistic interplay between wound healing and inflammatory mediators may inform novel preventive strategies for refractory wounds, thereby improving outcomes in high-risk PI populations. 40
The study found that in Africa, Oceania, and Southeast Asia, the disease burden of PI was concentrated among patients aged 45–94 years, with the QCI for PI exhibiting an overall decline with increasing age. Notably, a marked decline in the quality of care is evident among elderly patients aged 60 years and above. A notable study reported an incidence rate of 8.5% (95% CI 4.4–13.5%) for nursing home-acquired PI among the elderly, encompassing a total of 79,998 elderly residents, with over 6,700 cases of PI recorded. 41 This underscores the substantial room for improvement in the quality of care for elderly PI patients in these regions, significantly impacting the overall QCI. The skin integrity alterations, comorbidities, incontinence, malnutrition, and diminished self-repair capabilities that accompany the aging process in elderly patients not only elevate their risk of developing PI 42 but also compromise the quality of care once PI occurs. This underscores the global imperative to formulate targeted policies and nursing strategies for these high-risk age groups to mitigate their disease burden. For many diagnosed patients, the significance of PI treatment strategies and their prognoses may not be immediately apparent, as patients often prioritize more immediately distressing health concerns. Consequently, there is a heightened necessity for preventive initiatives that enhance public awareness of PI incidence, risk factors, consequences, and treatment modalities.
CONCLUSIONS
The aforementioned findings underscore the substantial global burden of PI over the past 32 years, highlighting health inequalities across countries and regions. Notably, for nations with low SDI, there remains considerable room for improvement in the quality of care for PI. The implementation of targeted and effective strategies for prevention and management, along with a focus on narrowing health care disparities, is paramount.
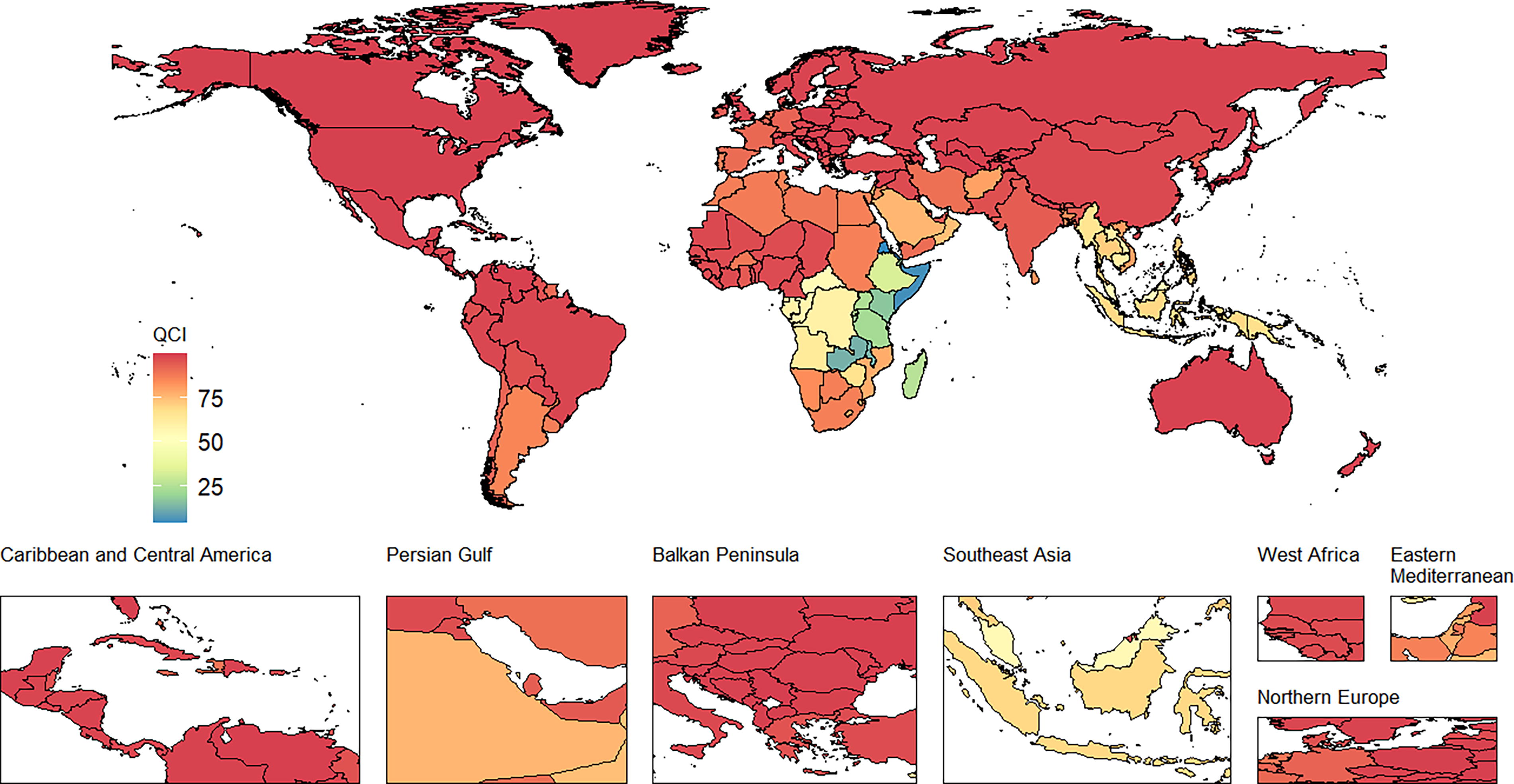
The QCI of PI in 2021. QCI, Quality of Care Index; PI, pressure injury.
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
The authors thank the Department of Science and Technology of Jiangxi Province, China, for funding this research (grant number: 20192BBGL70016
AUTHORS’ CONTRIBUTIONS
Z.-Q.X.: Conceptualization, methodology, software, validation, writing—original draft, visualization, investigation, and formal analysis; X.-M.T.: Conceptualization, methodology, software, validation, formal analysis, data curation, visualization, investigation, and writing—review and editing; Z.-Q.W.: Supervision, project administration, data curation, and writing—review and editing; Y.-Y.D.: Formal analysis, investigation, and writing—review and editing; L.-X.Y.: Formal analysis, investigation, and writing—original draft; C.X.: Formal analysis, writing—original draft, and investigation; H.-X.Y.: Conceptualization, visualization, and formal analysis; M.Z.: Conceptualization, methodology, software, validation, and data curation; W.-Y.X.: Conceptualization, writing—review and editing, and project administration; S.-H.C.: Writing—original draft, visualization, and formal analysis; C.-Z.H.: Writing—original draft, visualization, and funding acquisition; R.L.: Writing—review and editing, data curation, methodology, and software; L.Z.: Writing—review and editing, validation, supervision, project administration, and investigation; Z.Y.: Conceptualization, writing—review and editing, supervision, project administration, resources, validation, and investigation.
AUTHOR DISCLOSURE AND GHOSTWRITING
The authors have no conflict of interest to declare. The authors of this article hereby confirm that the entire content has been authored solely by members of THEIR research team. No external individuals or entities were engaged in ghostwriting or contributing to the article in a manner that would not be attributed to them. The research findings and conclusions presented within this article solely represent the views and interpretations of THE research group and have not been influenced by any external organizations. The authors affirm the integrity of their work and stand by its authenticity.
ABOUT THE AUTHORS
SUPPLEMENTARY MATERIAL
Supplementary Data
Abbreviations And Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.