
Abstract
Objective:
Chronic wounds have a high prevalence and poor outcomes in a geriatric population. It is unknown whether higher rates of successful wound healing are associated with better long-term outcomes. We sought to determine the association of risk-adjusted healing rates in wound care clinics with postdischarge outcomes.
Approach:
This observational study compared outcomes of Medicare patients with chronic wounds who received care at clinics with the highest risk-adjusted wound healing rates (n = 91) to those with the lowest rates (n = 88) in a network of 510 specialized U.S. wound care clinics. All 12,703 patients with chronic wounds at the clinics that could be identified in Medicare data were included. The outcomes were incidences of wound recurrence, gangrene, sepsis, and amputation after discharge.
Results:
The study included 6,462 and 6,241 patients in top- and bottom-performing clinics, respectively. Being treated in a top-performing clinic was associated with a lower cumulative incidence of all four outcomes. The difference was statistically significantly lower for wound recurrence (adjusted hazard ratio [aHR] = 0.82, 95% confidence interval [CI] 0.76–0.87, p < 0.001) and gangrene (aHR = 0.62, 95% CI 0.52–0.76, p < 0.001) but not for sepsis (aHR = 0.88, 95% CI 0.76–1.001, p = 0.065) and amputation (aHR = 0.75, 95% CI 0.65–1.00, p = 0.055).
Innovation:
This study is the first to suggest that patients treated in clinics with better wound-healing outcomes also have better outcomes after discharge. This finding can inform analyses to understand differences in practice patterns that lead to better outcomes.
Conclusion:
Treatment of chronic wounds in wound care clinics with higher risk-adjusted healing rates is associated with a lower risk of wound-related adverse events during follow-up, particularly in the first year. More research is needed to understand the factors that contribute to this effect and to determine interventions to improve outcomes sustainably as well as assess the impact of changes in outcomes on resource utilization and patients’ quality of life.
Soeren Mattke, MD, DSc

INTRODUCTION
Chronic wounds, usually defined as wounds that do not heal within an expected time frame, 1 typically 4–12 weeks, are a growing but little-recognized public health challenge, predominately affecting the elderly population. 2 Their prevalence is similar to that of heart failure, affecting 6.5 million people or 2% of the population in the United States. 3 In 2019, the estimated Medicare expenditure related to managing chronic wounds and associated complications ranged between $22.5 and $67.1 billion, the majority of which was incurred in the outpatient setting. 4 Chronic wounds are a visible manifestation of poorly controlled chronic diseases, such as diabetes and peripheral artery disease. Consequently, unless the underlying conditions are improved, there is a substantial risk of relapse and complications related to open or nonhealing wounds, such as infections, that may lead to sepsis, amputations, or death. In addition, patients with chronic wounds often suffer loss of productivity, psychological distress, decreased quality of life, and reduced life expectancy. 5 Disadvantaged populations have both a higher burden 6 and worse outcomes. 2 Despite the growing prevalence and economic burden in the aging U.S. population, chronic wound care remains an area with inconsistent adherence to evidence-based recommendations and variable quality of care. 7
Specialized wound care clinics have emerged as a care model to improve practice standards and thereby patient outcomes. 8,9 However, evidence for the better performance of such clinics under real-world conditions remains limited, and adherence to guideline recommendations in such clinics is inconsistent 10 –14
Thus, it would be important to determine whether clinics with higher adherence to evidence-based care achieve better long-term outcomes. A commonly used approach to compare outcomes across institutions is to estimate the rate at which medical events are projected to occur given an institution’s case mix and relate that to the actual observed rate, often called the observed to expected (O/E) ratio. These types of metrics are used for benchmarking purposes, for instance, the Agency for Healthcare Research and Quality has developed similar metrics using inpatient administrative data to determine whether a hospital had more or fewer adverse events than expected. 15 Conceptually, the O/E ratio reflects a risk-adjusted event rate but is more intuitive to understand, with O/E ratios above 1.0 for positive events indicating better-than-expected performance.
Historically, the gold standard to understand wound care performance has been the intent-to-treat wound healing rate. 16 However, due to variances across clinics in patient mix, the current authors had previously developed healing rate O/E ratios to better understand and standardize wound clinic performance. 17 A previously developed model that predicts the probability of a chronic wound healing within 12 weeks of treatment onset 18 was used to derive the expected healing rates, which were compared with the actual healing rates to calculate the O/E ratios for 532 wound care clinics in the United States.
In a subsequent study, the authors compared measures of care continuity and clinical quality for the top- and bottom-performing clinics in terms of their O/E ratio quintiles. 17 The top-performing clinics had numerically higher patient volume and achieved significantly better care continuity as determined based on the percentage of patients who saw their wound care provider at least once per week, the percentage of patients with additional nurse visits, and the visit cancellation rate. They also debrided wounds more frequently, which is known to promote wound healing. 19,20 In addition, we compared clinic-level utilization rates of indication-specific treatment modalities: use of compression therapy for venous lower leg ulcers, hyperbaric oxygen therapy and total contact casting for diabetic foot ulcers, and artificial skin substitutes for lower leg wounds that do not show signs of healing after 30 days of treatment. The top-performing clinics had higher rates for all of those measures, although only the difference in the use of total contact casting was statistically significant.
Having shown the association of O/E ratios with measures of care continuity and clinical quality, the next question is whether such improved processes and higher rates of wound healing are also associated with better posttreatment outcomes for patients. The current study analyzes whether patients under care in high-performing clinics based on their O/E ratio have lower rates of wound recurrence, amputation, gangrene, and sepsis after discharge from the clinics than patients treated in lower-performing clinics by linking O/E ratio data to Medicare administrative data.
INNOVATION
Collecting long-term outcomes data on chronic wound patients who are treated in specialized clinics remains a challenge under real-world conditions, as patients typically return to community-based care after discharge. We used an innovative Big Data approach to combine data from wound care clinics’ electronic health records, which contain detailed clinical information, with Medicare administrative data, which allow for long-term follow-up. This approach allows us to demonstrate that better wound healing outcomes are associated with better long-term results.
CLINICAL PROBLEM ADDRESSED
Chronic wounds that do not heal within 4–12 weeks are a growing but little-recognized public health challenge. 2 Despite the growing prevalence and economic burden in the aging U.S. population, chronic wound care remains an area with inconsistent adherence to evidence-based recommendations and variable quality of care. 7 Health services research, often using large-scale secondary data, is evolved as a discipline to measure and compare quality of care and to use those results to improve practice 21 but remains uncommonly used in wound care.
Our study demonstrates that it is feasible to merge data from wound care clinics with Medicare administrative data in order to understand treatment patterns and their relationship to patient outcomes. Combined with our earlier work, which showed an association of care continuity and adherence to evidence-based practices with healing rates, 17 the study also finds an association of healing rates with long-term outcomes. The findings underscore the need to ensure consistent and high quality of wound care as well as to use the rich data generated by it to continuously improve practice.
METHODS
Data sources
We obtained the data for all individuals in traditional Medicare and Medicare Advantage Plans who received care for a chronic wound in an outpatient setting, identified based on International Classification of Diseases (ICD)-10 diagnosis codes in claims and encounter data between 2016 and 2020. The data included the enrollment files and the full longitudinal information on inpatient, outpatient, physician office, skilled nursing facility, and hospice claims and encounters for a total of 5,710,907 unique patients with a diagnosis of chronic wounds. As the data are used for billing and reimbursement purposes and audited to ensure program integrity, they are fully adjudicated without missing data.
Data were accessed through the Centers for Medicare and Medicaid Services Virtual Research Data Center, and the study protocol and data protection procedures were approved by the USC Institutional Review Board (UP-22-00290) under expedited review and with a waiver for informed consent and Health Insurance Portability and Accountability Act authorization. Data were processed and analyzed with SAS Enterprise Guide 7.15 (SAS Institute Inc.) and StataSE 16 (StataCorp). An electronic laboratory notebook was not used.
The year 2017 was chosen to identify high- and low-performing clinics in order to have a follow-up period unperturbed by the COVID-19 pandemic. We constructed the 2017 O/E ratios for 532 wound care clinics and obtained the list of National Provider Identifier (NPI) and CMS Certification Number (CCN) for these clinics and the clinicians practicing in them. A total of 510 clinics that had both a listed NPI and a listed CCN were retained for the analysis.
Data linkage and episode construction
The objective of the data linkage procedure was to identify outpatient wound care episodes that started in 2017 in any of the clinics for which we had the O/E ratios. First, we identified all patients who had an outpatient or physician office visit with a primary diagnosis of a chronic wound based on ICD-10 codes (Supplementary Appendix). Only those patients with a principal or nonprincipal chronic wound diagnosis both at one of the included clinics (identified by organization NPI or CCN) and by one of the included clinic’s clinicians (identified by clinician NPI) were retained.
The start date of a treatment episode was defined as the first clinic visit with no prior visits for a look-back period of 45 days. Visits to other providers during this look-back period were permitted, as the clinics typically serve as referral centers for complex wounds. We did not include, however, episodes in which the patient had any overlapping inpatient or skilled nursing facility utilization, which signals that the patient was referred from an institutional setting, i.e., potentially a hospital-acquired event. Also not included were episodes in which the initial clinic visit was not followed by another visit within 28 days, indicating the patient was seen at the clinic for consultation only.
The end of the episode was defined as the last clinic visit that was not followed by another visit within 28 days to account for lower visit frequency toward the nearing of wound closure. Lastly, we restricted the analyses to episodes for which the patient had near-continuous Medicare enrollment for 12 months prior to the start date to establish baseline comorbidities and a minimum of 18 months after the end date or date of death (sourced from CMS Medicare enrollment files) to ascertain our outcomes. While a patient could have had more than one episode, only the first episode was included. A total of 464 clinics had at least one qualifying episode and were retained for the analysis. These 464 clinics were ranked by O/E ratio and assigned to quintiles, with the top quintile (n = 91) representing the highest-performing clinics and the bottom quintile (n = 88) representing the lowest performers for the analytic sample of 179 clinics.
Wound care outcomes
We identified four potential adverse outcomes after treatment conclusion: wound recurrence, surgical amputation, gangrene, and sepsis. Identification started the day after the end date of the treatment episode until death or the end of data coverage. Wound recurrence was defined as receipt of inpatient or outpatient care with at least one diagnosis of a chronic wound. Amputations were identified based on current procedural terminology and ICD-10 procedure codes for surgical procedures, and gangrene and sepsis were identified based on ICD-10 diagnosis codes. All code lists are documented in the Supplementary Appendix.
Risk adjustment variables
Variables used for risk adjustment included age (<65, 65–69, 70–74, 75–79, 80–84, and 85+ years of age), sex, race/ethnicity (White, Black, Hispanic, and other/missing), and presence of chronic conditions. Presence of chronic conditions was determined using ICD-10 diagnosis codes from the Chronic Condition Warehouse using the 12 months of data prior to the episode start date and included conditions that could interfere with the care plan (Alzheimer’s disease or non-Alzheimer’s dementia, depression, bipolar, or other depressive mood disorders) and cardiovascular conditions and risk factors (chronic kidney disease, chronic obstructive pulmonary disease [as a proxy for smoking], diabetes, heart failure and nonischemic heart disease, hyperlipidemia, hypertension, obesity, and peripheral vascular disease). We also adjusted for wound etiology (diabetic, arterial, venous, and pressure) and the duration of the treatment episode as a proxy for wound severity.
Analytic approach
Descriptive analysis
Sample composition in terms of demographics and burden of chronic disease, as well as adverse event and mortality rates, was compared between the top and bottom quintile clinics using two-tailed t-tests for independent samples. We also included the standard mean differences for variables with nonzero standard deviations.
Statistical modeling
The analysis compares the time to the first of each of the four above-listed adverse outcomes at the patient level between the top- and bottom-performing clinics, based on the top and bottom O/E ratio quintiles, accounting for the clustering of patients within clinics and patient-level risk factors.
A challenge in estimating a time-to-event model in a population of patients with chronic wounds is the high mortality rate of these severely ill individuals with over 10% in the first year after discharge and almost 50% over the full observation period of our study. Differences in mortality between the two groups could result in systematic differences in patients experiencing our outcomes because of differential censoring. To account for this potential competing risk of death, we used a generalization of the standard Cox proportional hazards model introduced by Fine and Gray 22 instead of the standard model. This model allows for direct estimation of the probability of the event of interest occurring by a certain time while accounting for the competing events (the cumulative incidence function). For a textbook treatment of the competing risks regression, see Collett. 23
Reporting of results followed the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. 24
RESULTS
Descriptive analysis
In Table 1, we compare summary statistics of patient characteristics as well as patient-level event and mortality rates, separately for high- and low-performing clinics with a two-sample t-test of mean differences between the groups. The bottom-quintile clinics have a significantly larger percentage of Black and Hispanic patients and a lower percentage of White patients. In these clinics, patients have a significantly higher prevalence of pre-existing dementia and stroke. In contrast, top-performing clinics have a significantly larger number of patients with obesity, pulmonary disease, and depression.
Summary statistics of patient-level variables for top- and bottom-quintile clinics
Std, standard deviation; SMD, standardized mean difference.
While mortality and sepsis incidence after discharge are similar for both groups, the top-performing clinics have a significantly lower incidence of wound recurrence, gangrene, and amputations.
Event-free survival time analysis
Figures 1–4 show the estimated cumulative incidence of adverse long-term outcomes after discharge from treatment, separately for high- and low-performing clinics and accounting for the competing risk of mortality. In addition, in Supplementary Appendix Tables A1–A4, the full results of estimating the competing risks regression for each adverse outcome are reported. We controlled for the patient’s race/ethnicity, age, chronic conditions, and the quartile of the length of the wound care episode. The variable of interest is the variable indicating whether the patient received care from a top- or bottom-quintile clinic.
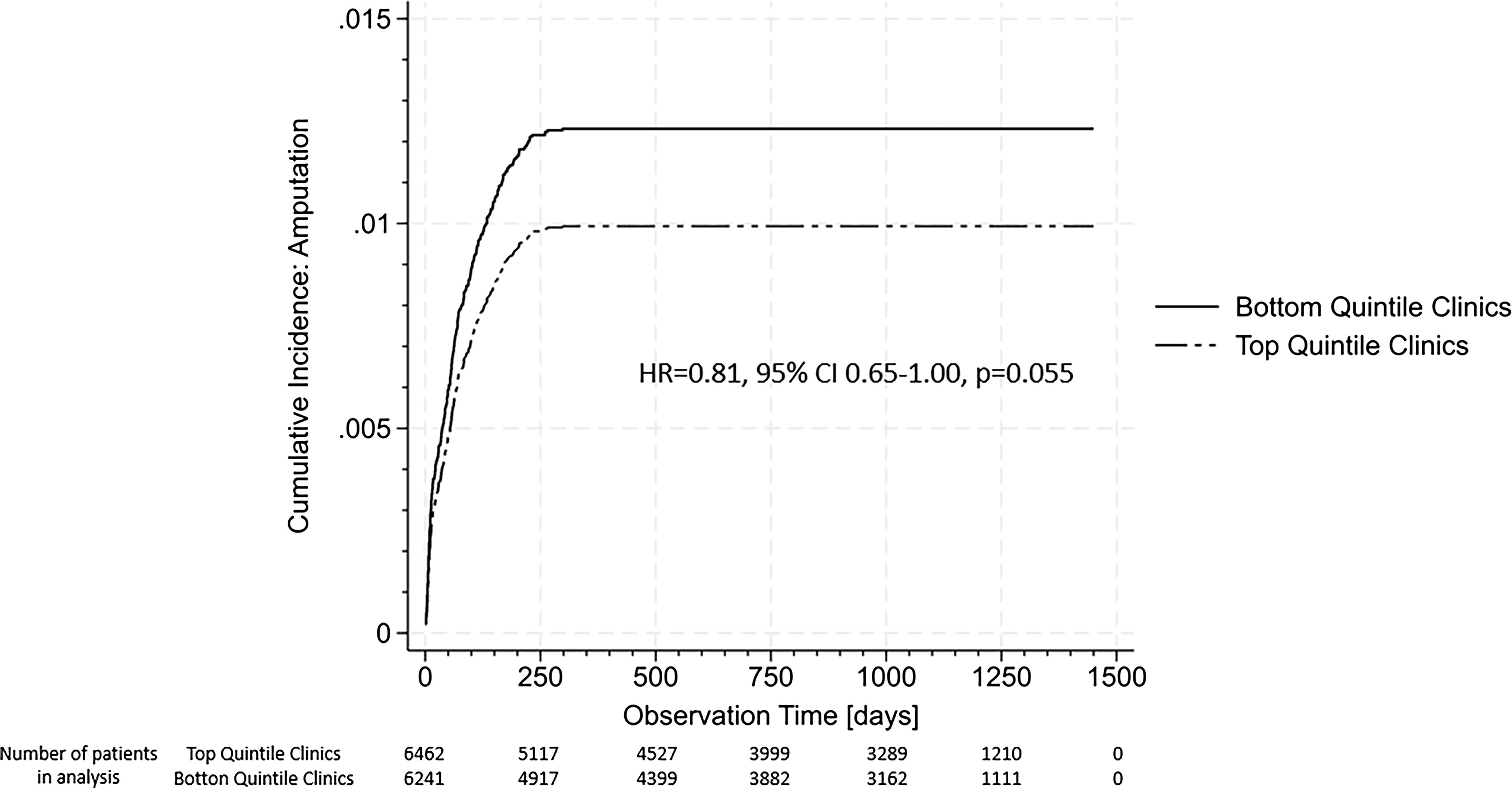
The estimated cumulative incidence of amputation for top- and bottom-quintile clinics for a statistically average patient. Note: HR denotes hazard ratio, CI denotes confidence intervals. If the CI includes the 1.0, the time to the event is not significantly different between the two groups.
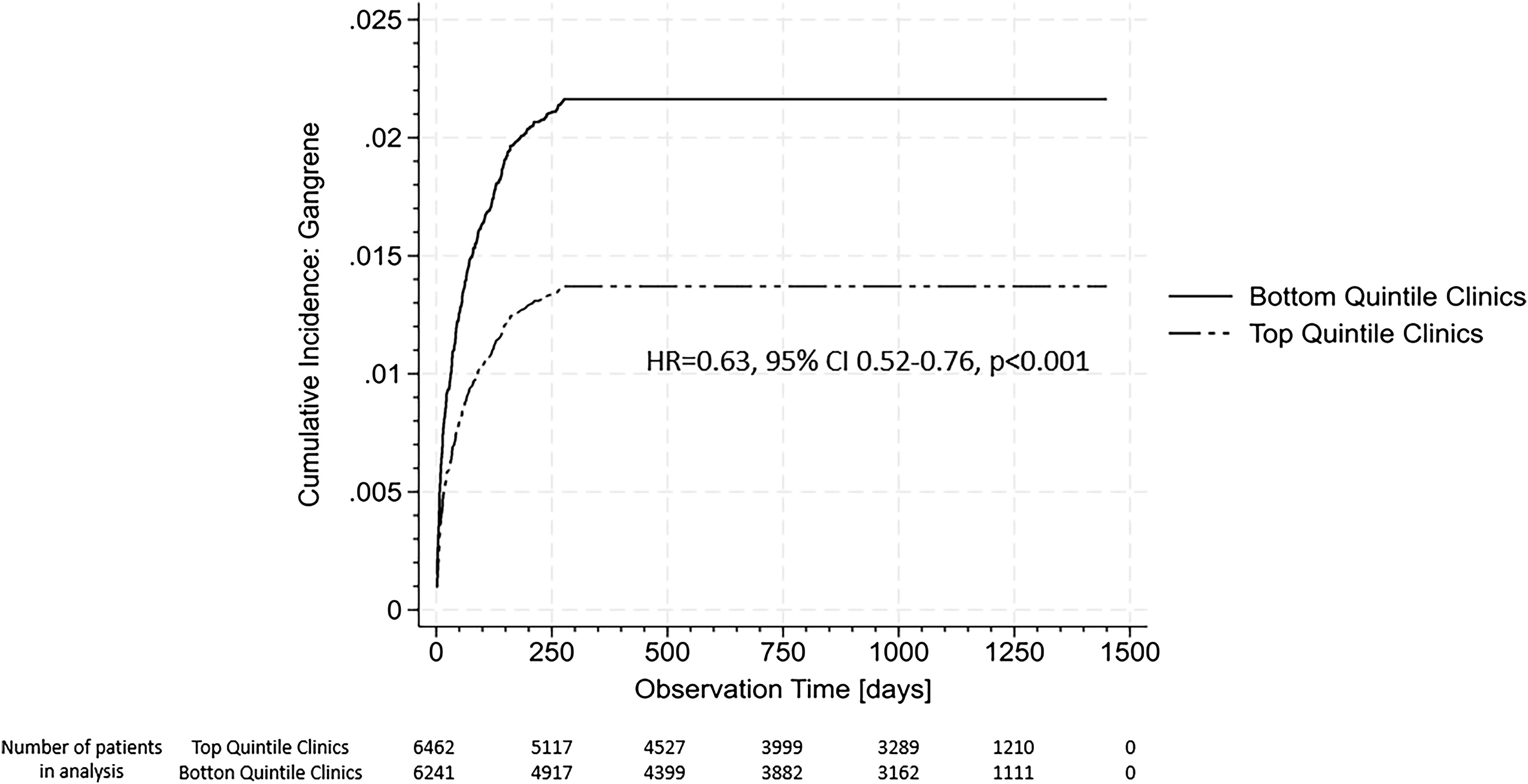
The estimated cumulative incidence of gangrene for top and bottom-quintile clinics for a statistically average patient. Note: HR denotes hazard ratio, CI denotes confidence intervals. If the CI includes the 1.0, the time to the event is not significantly different between the two groups.
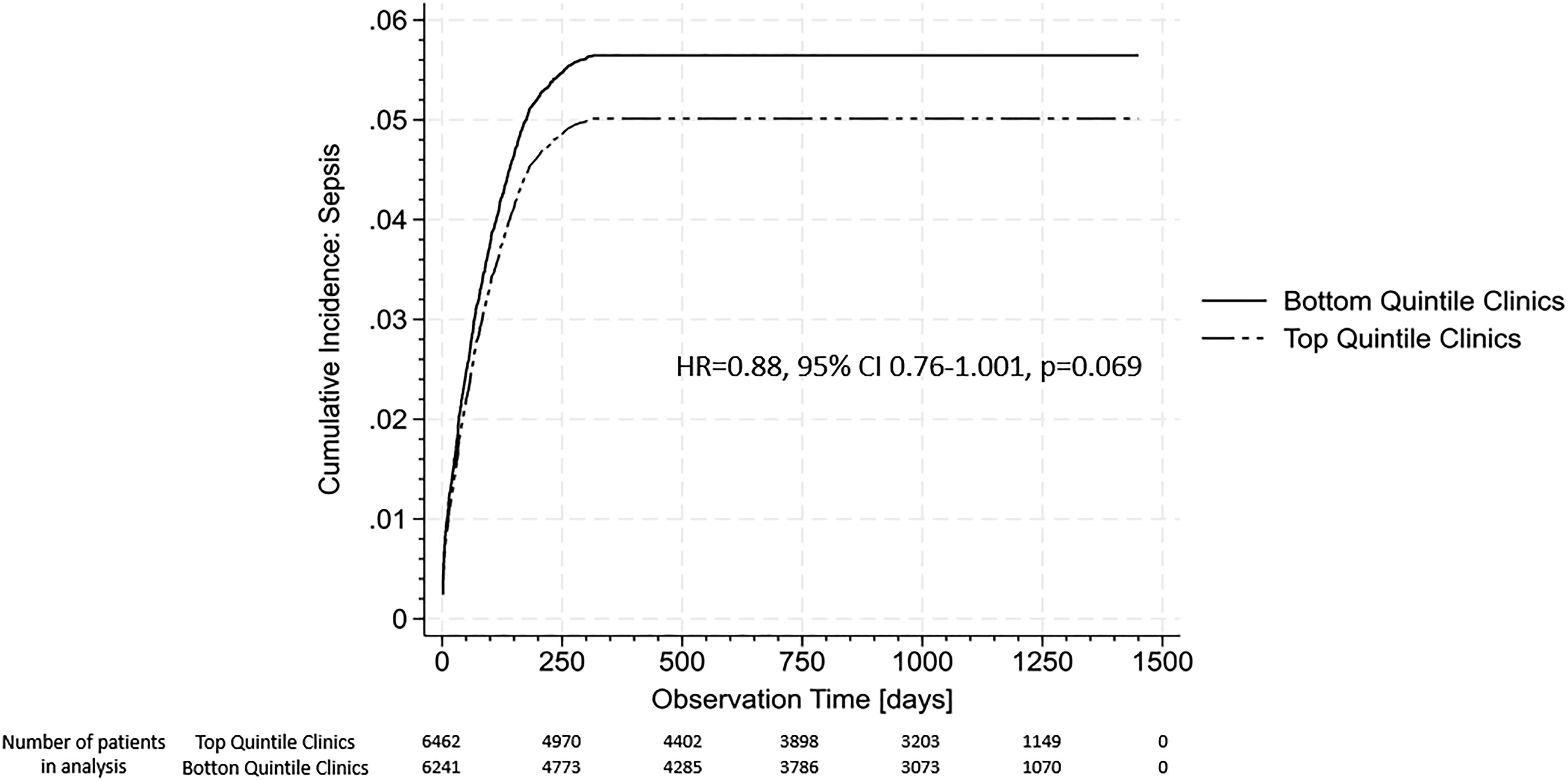
The estimated cumulative incidence of sepsis for top- and bottom-quintile clinics for a statistically average patient. Note: HR denotes hazard ratio, CI denotes confidence intervals. If the CI includes the 1.0, the time to event is not significantly different between the two groups.
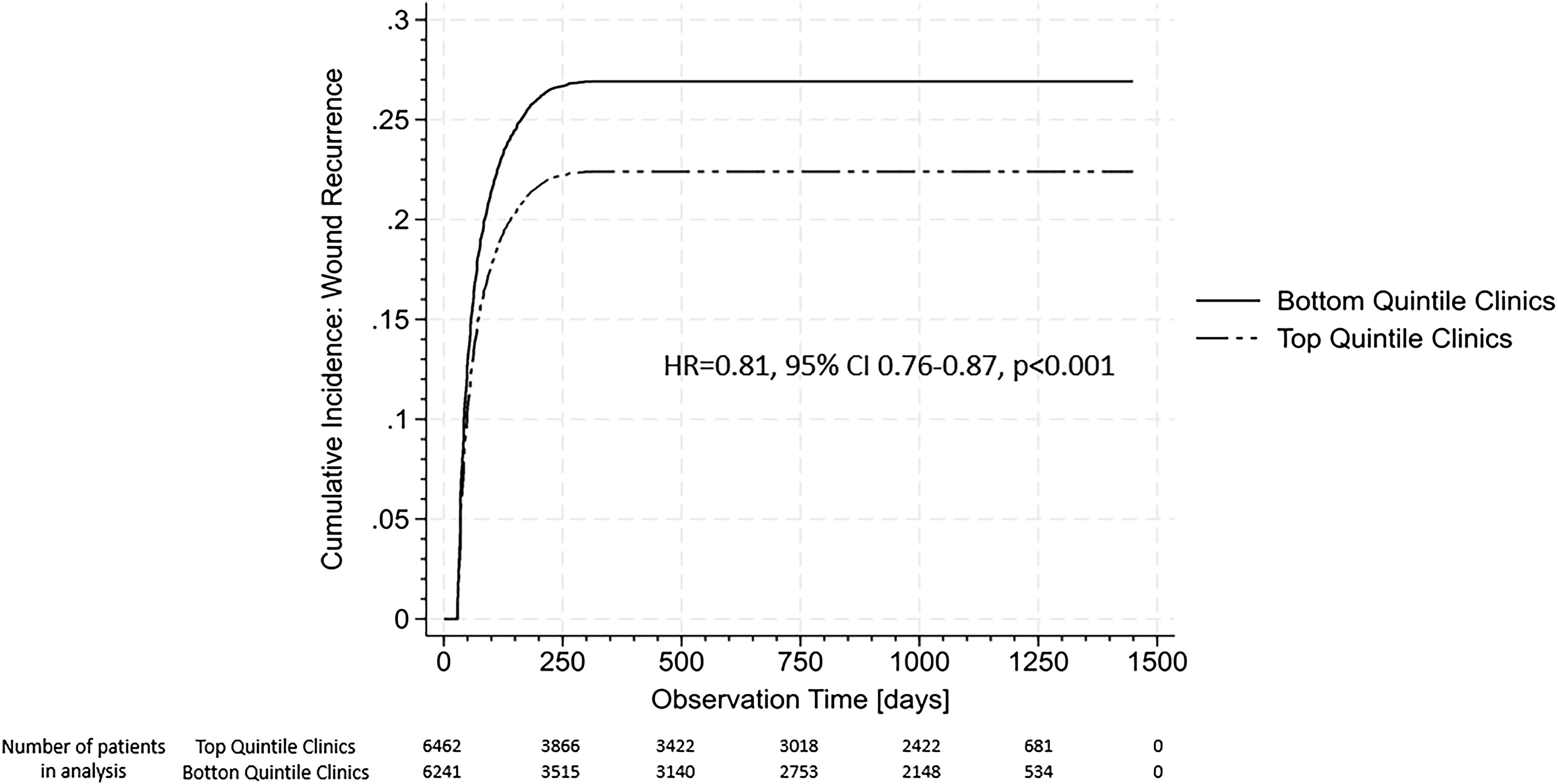
The estimated cumulative incidence of wound recurrence for top- and bottom-quintile clinics for a statistically average patient. Note: HR denotes hazard ratio, CI denotes confidence intervals. If the CI includes the 1.0, the time to event is not significantly different between the two groups.
The cumulative incidence function graphs share two common features for all four adverse outcomes. First, the cumulative incidence of all four is numerically lower in the top-performing clinics, and, second, the difference occurs largely in the first year after discharge from treatment. However, the difference is only statistically different for wound recurrence (adjusted hazard ratio [aHR] = 0.82, 95% confidence interval [CI] 0.76–0.87, p < 0.001) and gangrene (aHR = 0.62, 95% CI 0.52–0.76, p < 0.001) but not for sepsis (aHR = 0.88, 95% CI 0.76–1.001, p = 0.065) and amputation (aHR = 0.75, 95% CI 0.65–1.00, p = 0.055).
In Table 2, we report the expected number of adverse outcomes for a homogeneous population of 1,000 statistically average patients after treatment in a high- or low-performing clinic separately.
Estimated average number of adverse events in the first year after treatment, per 1,000 statistically average patients. Standard errors in parentheses
DISCUSSION
In this cross-sectional and observational analysis, we show that outcomes after discharge from outpatient care for chronic wounds are better for patients, who received care in clinics with the highest O/E ratios, which reflect risk-adjusted healing rates, compared with those with the lowest O/E ratio. In other words, better success in healing a chronic wound is associated with fewer wound-associated complications, particularly in the first year after discharge, suggesting a lasting effect on patients’ health. While an observational study cannot establish causality, our findings contribute to the evidence that high-quality wound care has positive effects on patients even after discharge. This result underscores the need for stricter and less variable adherence to evidence-based standards of care and care continuity, as an earlier study 17 had shown that those factors are also associated with higher risk-adjusted healing rates.
Such findings are important to improve care for a high-risk, yet under-researched patient group. Around a quarter of patients in our sample experienced a wound recurrence during follow-up, comparable to data reported by Bundo et al. 25 for diabetic foot ulcers with a recurrence rate of 29.2% during 12 months. Armstrong et al. 26 estimated an even higher rate of 40% in the first year based on a review of 19 articles on incidence rates for ulcer recurrence. Other adverse outcomes are also common. A review by McDermott et al. 27 reported a lifetime amputation risk of 20% for patients with diabetic foot ulcers.
These poor outcomes are a consequence of the high burden of chronic disease in patients with chronic wounds. In our sample, around one-fifth suffered from dementia, approximately three-quarters from diabetes, nearly half from congestive heart failure, and 7 out of 10 patients had peripheral vascular disease. The estimated annual mortality rate was 12–13%, which is similar to the mortality rates reported by others. Saluja et al. 28 conducted a meta-analysis of 11 studies on the association between diabetic foot ulcers and all-cause mortality and estimated a crude annual mortality rate of 23.1 per 1,000 population. In addition, a study of patients with diabetic foot ulcers, who were treated in primary care centers in Catalonia, Spain, reported that 9.7% of patients died over a 12-month follow-up period.
We note that the absolute difference in event rates between high- and low-performing centers is not large in this observational study with a 4.5 percentage point difference for wound recurrence and less than one percentage point for the other three outcomes. However, even in interventional studies that specifically target a certain wound etiology, published effect sizes tend to be small. For example, in trials of customized footwear to prevent the recurrence of diabetic foot ulcers, Bus et al. 29 and Rizzo et al. 30 reported 5.4% and 5.9% absolute risk reduction. Chen et al. 31 achieved a 6% point reduction, and Frykberg et al. 32 achieved an 8.1% point reduction in amputation rate in diabetic foot ulcer patients with the use of hyperbaric oxygen therapy and a human fibroblast-derived dermal substitute, respectively. The difficulty in reducing wound recurrence and complications points to the need for better postgraduate wound care training through fellowship and recognized board certification. 33
LIMITATIONS
The results should be interpreted in the context of the study’s limitations. First, an observational study cannot generate proof of causality, and further longitudinal research is needed to confirm the findings. Second, we used administrative data rather than medical records to ascertain outcomes, which may have introduced errors. Third, patients were attributed to high- and low-performing clinics based on an algorithm that may have generated false positive and false negative cases, as might have our assumption-driven definition of a care episode. We would argue, however, that those sources of error are not likely to influence the association between clinics and outcomes. Fourth, the O/E ratios were derived from the clinics’ entire patient population and thus included patients not present in the Medicare data. Since we treat the O/E ratio as a clinic-level rather than a patient-level quality indicator, this discrepancy should not affect our results. Fifth, our findings may not generalize to populations other than Medicare beneficiaries. Lastly, our risk adjustment for demographic characteristics, diagnosed comorbidities, and treatment duration may not have fully accounted for differential risks between the two groups, as important potential confounders, such as detailed wound characteristics, management of underlying conditions, and socioeconomic status, are not captured in Medicare administrative data. However, these variables are unavailable for patients in both clinic groups. Unless they are correlated with the O/E ratios, their absence would only have introduced random error rather than bias.
CONCLUSION
The results from this observational study suggest that receiving care in wound care clinics with higher risk-adjusted healing rates is associated with a lower risk of wound-related adverse events during follow-up, particularly in the first year. More research is needed to understand the factors that contribute to this effect and to determine interventions to improve outcomes sustainably as well as assess the impact of changes in outcomes on cost of care, resource utilization, and patients’ quality of life.
Footnotes
ACKNOWLEDGMENTS AND FUNDING STATEMENT
The study was funded by a grant from
AUTHORS’ CONTRIBUTIONS
G.F., S.M., and W.E.: Concept and design; M.S., J.K., and W.E.: Acquisition of subjects and/or data; G.F., S.M., A.B., M.S., and W.E.: Analysis and interpretation of data; and all authors: Preparation of article.
AUTHOR DISCLOSURE AND GHOSTWRITING
Dr. Mattke serves on the board of directors of Senscio Systems, Inc., and the scientific advisory board of Alzpath and Boston Millennia Partners. He has received consulting and speaker fees from Biogen, C2N, Eisai, Eli Lilly, Novartis, Novo Nordisk, and Roche/Genentech. Dr. Sheridan is an employee and Dr. Ennis a consultant for
ABOUT THE AUTHORS
SUPPLEMENTARY MATERIAL
Supplementary Appendix
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.