
Abstract
Objective:
To evaluate global, regional, and national trends in the prevalence and disability-adjusted life years (DALYs) of pressure injuries (PIs) from 1990 to 2021 and project future trends to 2035, based on data from the Global Burden of Disease (GBD) study.
Approach:
This study used GBD 2021 data to analyze PIs prevalence and DALYs by age, sex, and Sociodemographic Index (SDI) region. The Bayesian age-period-cohort model was employed for temporal trend analysis and future projections.
Results:
From 1990 to 2021, the global prevalence slightly decreased from 8.246 to 7.920 per 100,000 (estimated annual percentage change −0.023%), whereas DALYs decreased by 9.7%. High-SDI regions presented significant DALY reductions (−39.3%), whereas middle- and low-middle-SDI regions presented increased prevalence rates (20.5% and 28.9%, respectively). The prevalence was highest in the ageing population, peaking in the 95+ year age group. Projections estimate that there will be 720,660 global cases by 2035, with the greatest burden expected among older adults in developing regions.
Innovation:
This study provides a comprehensive longitudinal analysis of PIs, revealing global disparities and emphasizing demographic-specific risks, especially in ageing populations and low-SDI regions. Bayesian modeling offered robust future projections.
Conclusion:
Despite modest improvements globally, significant disparities in the prevalence of PIs persist, particularly in developing regions and among older adults. Targeted interventions, preventive strategies, and health care policies are critical for addressing these challenges and mitigating future disease burdens.
INTRODUCTION
Pressure injuries (PIs), also known as pressure ulcers, are localized injuries to the skin and underlying tissue, primarily caused by prolonged pressure or friction on the skin. 1 PIs significantly impact patients’ quality of life, increasing morbidity and mortality rates, and pose a substantial burden on caregivers and health care systems globally. 2 According to statistical data, the total cost in Australian public hospitals alone reaches as high as 9.11 billion Australian dollars, and annual health care costs exceeding $26.8 billion in United States. 3
Shuting Li, BN

Zhicheng Hu, MD, PhD

Jiayuan Zhu, MD, PhD

The incidence and prevalence of PIs vary considerably across different regions and populations and are influenced by factors such as health care quality, economic conditions, and demographic profiles. 4 This study aimed to bridge this gap by utilizing data from the Global Burden of Disease (GBD) study and other authoritative sources to evaluate trends in the prevalence and disability-adjusted life years (DALYs) associated with PIs over the past three decades. By analyzing these indicators at the global, regional, and national levels, we sought to elucidate the spatial and temporal patterns of pressure ulcer burden.
Our study indicates that the global incidence of PIs has shown a modest decline over the past three decades. However, among the elderly population and in economically underdeveloped regions, the prevalence and DALYs rate continue to exhibit an upward trend. The findings of this research will provide valuable insights for health care policymakers, practitioners, and researchers. Identifying high-risk regions and vulnerable populations can facilitate the allocation of resources more effectively and the development of targeted interventions to prevent PIs and manage their complications. Ultimately, this study contributes to reducing the global burden of PIs, improving patient outcomes, and alleviating strain on health care systems.
CLINICAL PROBLEM ADDRESSED
PIs remain a pervasive health care challenge for patients and pose a substantial burden on caregivers and health care systems worldwide. Understanding the epidemiological trends of PIs is essential for developing effective prevention and management strategies.
METHODS
Data source
This study followed the guidelines for reporting observational studies (the guidelines for reporting observational studies [STROBE], see the Supplementary Data) in epidemiology. All the data were generated from the most up-to-date version of the GBD 2021 from the Global Health Data Exchange query tool (https://vizhub.healthdata.org/gbd-results/). The detailed GBD 2021 protocol and methods have been reported previously. 5
Study population and data collection
Initially, we designated “decubitus ulcers” as our research field on the platform, given that the GBD retains “decubitus ulcers” as the nomenclature for PI. We subsequently downloaded the corresponding data segregated by age, sex, Sociodemographic Index (SDI) region, geographical area, and nation. The SDI ranges from 0 to 1, where 0 represents the minimum level of development and 1 represents the maximum level. 6 The 204 countries and regions were categorized into five groups on the basis of their SDI values: high-SDI, medium- to high-SDI, medium-SDI, medium- to low-SDI, and low-SDI regions. Our study also aligned with the GBD’s definition, considering 21 regions with similar geographic and epidemiological characteristics, as well as 204 individual nations and territories.
We extracted annual data from 1990 to 2021, encompassing the number and rates of prevalence and DALYs. DALYs are a measure used in public health to capture the total amount of healthy life lost to all causes. DALYs essentially combine years of life lost due to premature mortality and years lived with disability. In GBD 2021, estimates with uncertainty intervals (UIs) were generated for all locations every year, even in instances of sparse or missing data. 7 All reported rates were standardized and expressed per 100,000 individuals, ensuring comparability. Within the GBD framework, a specific algorithm was employed to estimate the uncertainty of a health statistic by iterating the estimation 1,000 times. These 1,000 estimates were arranged in ascending order. We selected the values corresponding to the 2.5th and 97.5th percentiles from these iterations to represent the 95% UI. 8
Statistical analysis
Temporal trends from 1990 to 2021 were quantified by the estimated annual percentage change (EAPC) to assess the burden of PIs. 9 The 95% confidence intervals (CIs) of the EAPCs were determined by linear modeling. If the upper limit of both the EAPC and its 95% CI is negative, its corresponding rate shows a decreasing trend; conversely, if the lower limit of both the EAPC and its 95% CI is positive, its corresponding rate shows an increasing trend. The future disease burden from 2022 to 2035 was predicted by using the Bayesian age-period-cohort (BAPC) model. 10 The R package “BAPC” is based on the integrated nested Laplace approximation used for predicting GBD data. 11 The data analysis was conducted using the R program (version 4.3.1) and RStudio.
Ethics approval
This study followed the Guidelines for Accurate and Transparent Health Estimates Reporting. The GBD 2021 study consists of aggregated, deidentified data. This study was approved as exempt by the Institutional Review Board of the First Affiliated Hospital of Sun Yat-sen University.
Role of the funding source
The funders had no role in the study design, data collection, analysis, interpretation, or writing of the article. The authors were independent of the study sponsors. All the authors had full access to all the data in the study and had final responsibility for the decision to submit for publication.
RESULTS
Global trends of PIs
From 1990 to 2021, the global prevalence rate of PIs slightly decreased (Table 1). In 1990, the prevalence was 8.246 (95% UI: 7.388–9.179) per 100,000 people, which declined to 7.920 (95% UI: 7.138–8.728) in 2021. Globally, the DALYs associated with PIs decreased from 10.741 (95% UI: 8.870–12.738) per 100,000 population in 1990 to 9.696 (95% UI: 7.409–10.884) in 2021.
Prevalence and disability-adjusted life years of pressure injuries between 1990 and 2021 at the global and regional levels
DALYs, disability-adjusted life years; EAPCs, estimated annual percentage change; SDI, Sociodemographic Index.
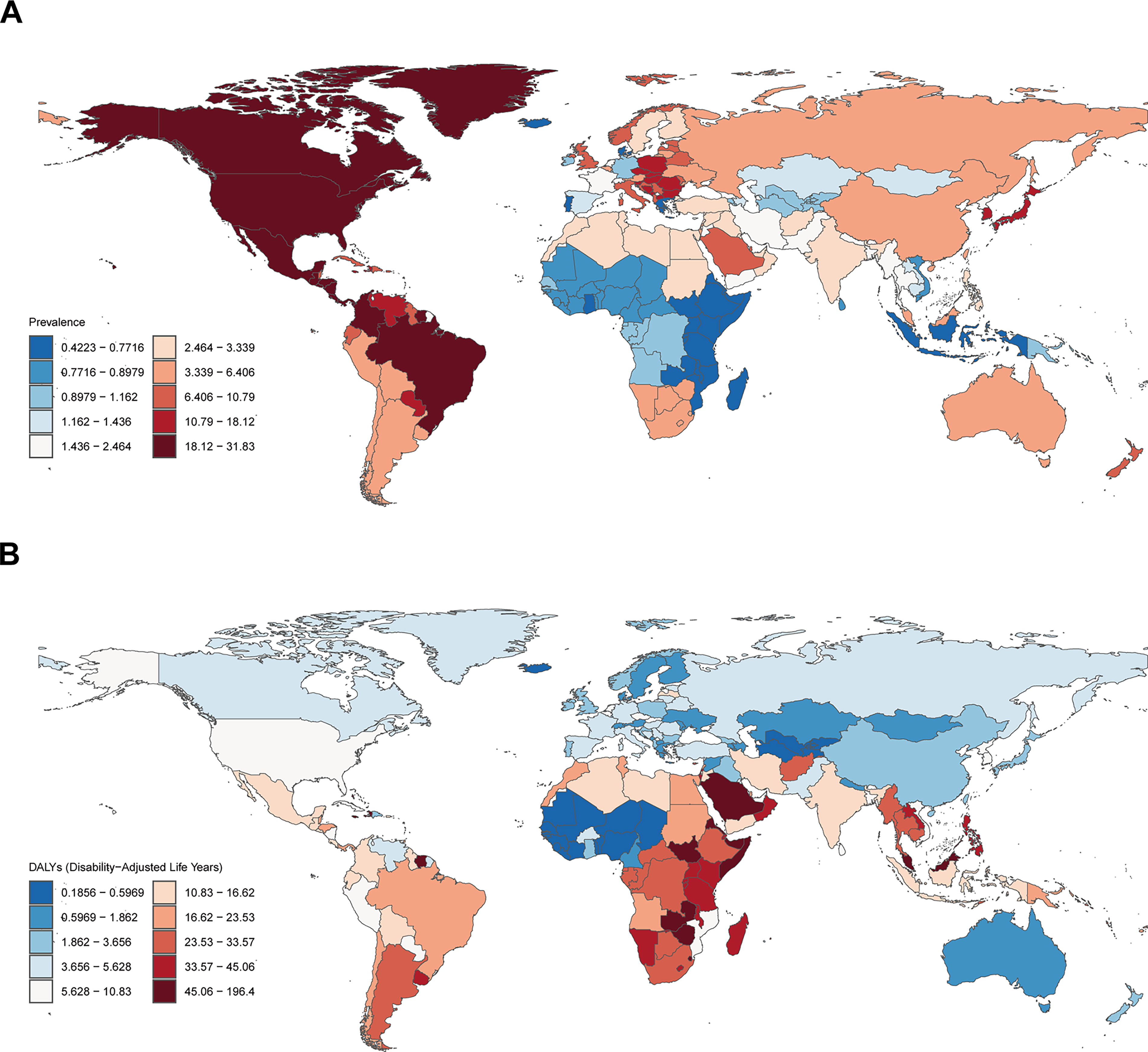
An analysis of the global distribution of PIs in 2021 is illustrated on a world map (Fig. 1). The following five countries had the highest age-standardized prevalence rates of PIs: the United States, Barbados, the Republic of Panama, the United Mexican States, and Greenland (Fig. 1A and Supplementary Table S1). Additionally, the countries with the highest age-standardized DALYs for PIs are Barbados, the Commonwealth of the Bahamas, the Commonwealth of Dominica, Grenada, and Antigua and Barbuda (Fig. 1B and Supplementary Table S2).
The age-standardized prevalence
Trends by SDI region
The global trends in PIs across different SDI regions from 1990 to 2021 revealed distinct patterns (Table 1). High-SDI regions experienced a slight decrease in prevalence, from 14.938 (95% UI: 13.365–16.679) in 1990 to 14.406 (95% UI: 13.038–15.831) in 2021, representing a percentage change of −3.560% (95% UI: −6.031% to −0.822%) and an EAPC of −0.181% (95% CI: −0.231% to −0.131%). DALYs in these regions significantly decreased by −39.285% (95% UI: −43.510% to −34.545%), with an EAPC of −1.892% (95% CI: −2.060% to −1.724%). High-middle-SDI regions showed a modest increase in prevalence, from 5.465 (95% UI: 4.875–6.124) to 5.642 (95% UI: 5.089–6.245), translating to a percentage change of 3.237% (95% UI: −0.335% to 7.087%) and an EAPC of 0.285% (95% CI: 0.144–0.426%). However, DALYs increased significantly, by 58.486% (95% UI: 33.236–78.337%), with an EAPC of 1.588% (95% CI: 1.173–2.004%). The middle-SDI regions experienced a notable increase in prevalence, from 5.670 (95% UI: 5.120–6.268) to 6.829 (95% UI: 6.163–7.524), a percentage change of 20.453% (95% UI: 17.420–24.087%) and an EAPC of 0.847% (95% CI: 0.701–0.993%). DALYs in these regions decreased slightly by −3.469% (95% UI: −19.173% to 14.600%), with an EAPC of −0.225% (95% CI: −0.338% to −0.113%). The low-middle-SDI regions presented a significant increase in prevalence, from 3.166 (95% UI: 2.821–3.510) to 4.082 (95% UI: 3.690–4.514), a percentage change of 28.918% (95% UI: 26.454–31.620%) and an EAPC of 1.157% (95% CI: 0.975–1.339%). DALYs remained relatively stable, with a slight decrease of −0.898% (95% UI: −27.372% to 29.822%) and an EAPC of −0.458% (95% CI: −1.021% to 0.109%). The low-SDI regions presented a modest increase in prevalence, from 1.492 (95% UI: 1.299–1.691) to 1.585 (95% UI: 1.384–1.793), representing a percentage change of 6.225% (95% UI: 4.355–8.092%) and an EAPC of 0.442% (95% CI: 0.288–0.596%). DALYs decreased by −15.873% (95% UI: −34.837% to 12.200%), with an EAPC of −0.884% (95% CI: −1.122% to −0.647%).
From 1990 to the early 2000s, prevalence rates across all SDI groups exhibited slight fluctuations without a clear trend. However, from the mid-2000s onward, divergent patterns became apparent (Fig. 2A). Globally, the prevalence of PIs has gradually declined from 8.25% in 1990 to 7.99% in 2021. This trend, however, was not uniform across the SDI groups. Despite initially having the lowest prevalence rates, low-SDI regions experienced a steady increase from 1.49% in 1990 to 1.59% in 2021. Conversely, high-SDI regions, which started with the highest prevalence (14.94% in 1990), experienced a decrease to 14.41% by 2021. The middle-SDI regions showed a contrasting trend, with the prevalence increasing from 3.17% in 1991 to 3.30% in 2021 (Supplementary Table S3). The age-standardized DALY rates for PIs also reflected these complex patterns (Fig. 2B). Globally, we observed a modest decrease from 10.74 (95% UI: 8.87–12.74) per 100,000 people in 1990 to 9.70 (95% UI: 7.41–10.88) in 2021, representing a 9.7% reduction. This decline, however, was not linear, with a more rapid decrease observed from 2000 to 2010, followed by a slight increase in recent years. Substantial disparities in DALY rates persisted between SDI regions throughout the study period. Paradoxically, while low-SDI regions had the lowest prevalence, they consistently presented the highest burden, with DALY rates ranging from 19.55 (95% UI: 11.90–30.98) in 1990 to 16.45 (95% UI: 10.55–22.02) in 2021. In contrast, high-SDI regions, despite having the highest prevalence, presented the lowest DALY rates, which decreased from 10.96 (95% UI: 10.05–11.98) in 1990 to 6.66 (95% UI: 5.87–7.53) in 2021 (Supplementary Table S4).

Trends in pressure injuries across SDI groups in the GBD study from 1990 to 2021.
Regional trends of PIs
The results revealed varying trends in the prevalence of PIs across regions (Table 1). Notably, the prevalence rate in Andean Latin America decreased from 7.695 (95% CI: 6.947–8.613) in 1990 to 6.724 (95% CI: 6.025–7.464) in 2021, representing a decline of 12.614% (EAPC: −0.567). In contrast, Tropical Latin America experienced a significant increase in prevalence, increasing from 10.576 (95% CI: 9.590–11.530) to 19.331 (95% CI: 17.404–21.200), an 82.775% increase (EAPC: 2.648). With respect to DALYs, the Caribbean and Central Latin American regions presented notable reductions. The Caribbean DALYs decreased from 36.668 (95% CI: 31.976–43.394) to 29.723 (95% CI: 24.257–36.762), a reduction of 18.940% (EAPC: −0.834), whereas Central Latin America experienced an even more substantial drop from 28.019 (95% CI: 26.545–29.630) to 12.152 (95% CI: 10.235–14.633), a 56.631% decline (EAPC: −2.591). Conversely, regions such as East Asia and Eastern Europe presented mixed trends. East Asia exhibited a moderate increase in prevalence from 4.671 (95% CI: 4.168–5.217) to 5.761 (95% CI: 5.212–6.366), with a 23.320% increase (EAPC: 1.028). Eastern Europe, meanwhile, experienced a significant increase in DALYs, underscoring regional disparities.
A strong positive correlation was observed between the SDI and prevalence rates (r = 0.6077, p < 0.001), indicating that regions with higher SDIs tend to have higher prevalence rates of PIs (Fig. 3A). Conversely, a moderate negative correlation was found between the SDI and age-standardized DALY rates (r = −0.4001, p < 0.001). Notably, the strength of the SDI–DALY relationship varied across regions, with high-income areas generally demonstrating stronger negative correlations. In contrast, some low- and middle-income regions presented weaker or even positive correlations (Fig. 3B).
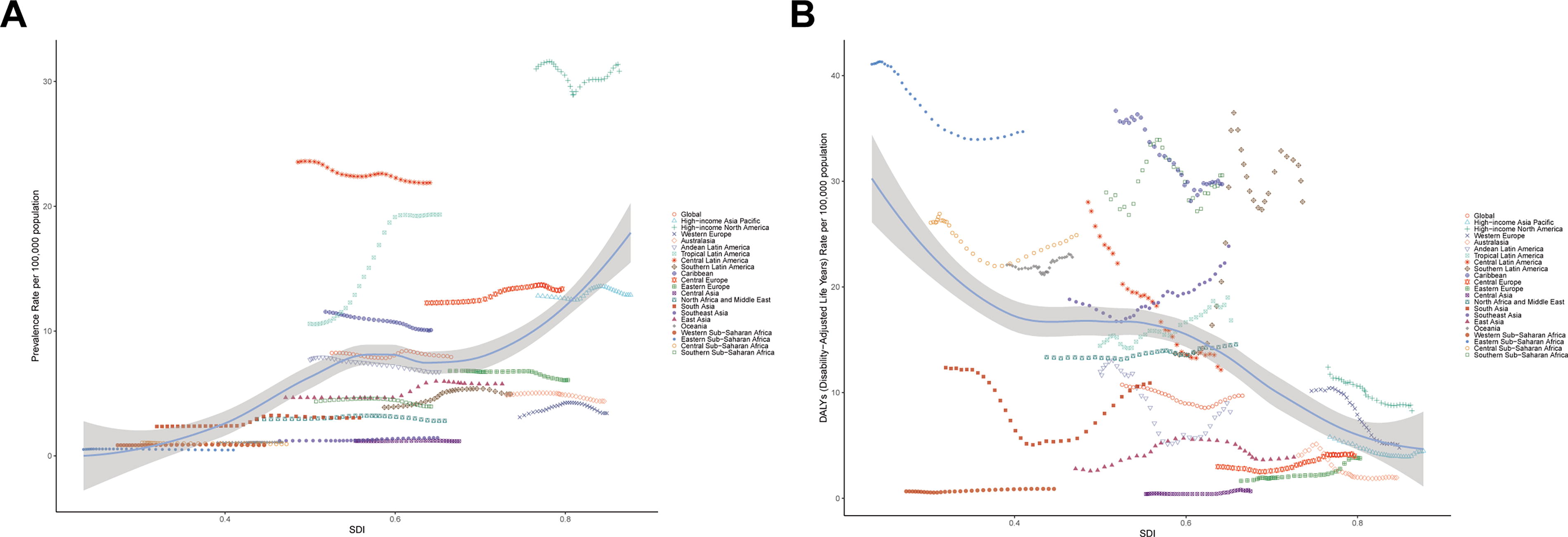
Association trends of pressure injuries and SDI for 21 regions in the GBD study.
Age- and sex-specific prevalence and DALYs of PIs
The prevalence clearly increased with age for both sexes, ranging from 0.15 (95% UI: 0.09–0.24) per 100,000 individuals in the youngest age group (<5 years) to 456.77 (95% UI: 347.47–597.46) and 497.95 (95% UI: 386.34–632.72) per 100,000 individuals for males and females, respectively, in the oldest age group (95+ years). Interesting sex-specific patterns emerged across the lifespan: males consistently presented slightly higher prevalence rates in early life (0–19 years), and this disparity became more pronounced in young and middle adulthood (20–59 years). However, the trend reversed in older adults (60+ years), with females showing higher prevalence rates, particularly in very old age groups. The data revealed a nonlinear increase in prevalence with age, with risk accelerating rapidly after age 60 for both sexes (Fig. 4A).
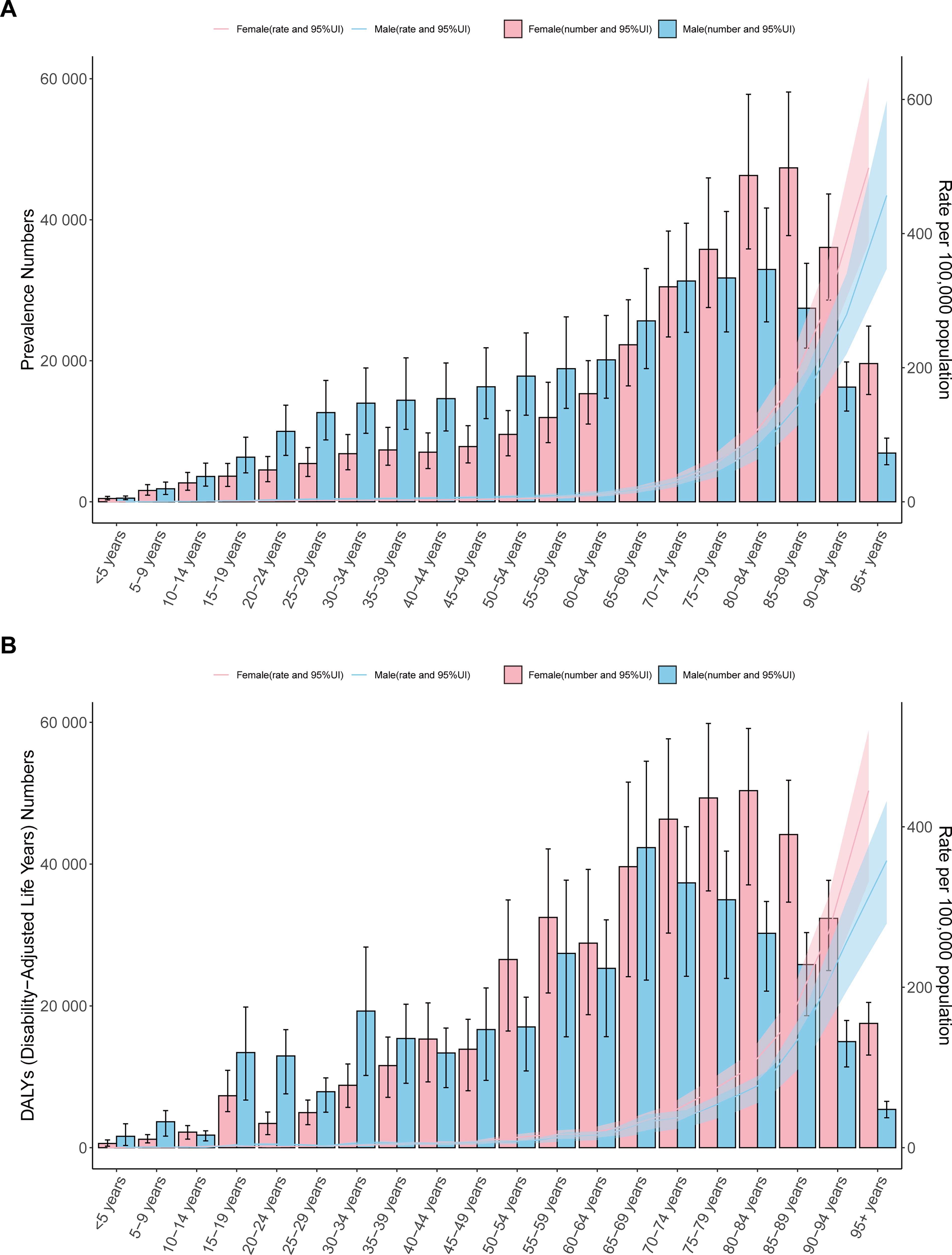
The trends of pressure injuries in the different age and gender groups in global 2021.
The DALY rates clearly increased with age for both sexes, ranging from 0.47 (95% UI: 0.09–0.99) per 100,000 for males and 0.19 (95% UI: 0.07–0.34) per 100,000 for females in the youngest age group (<5 years) to 357.76 (95% UI: 279.50–431.99) per 100,000 for males and 445.08 (95% UI: 331.64–520.28) per 100,000 for females in the oldest age group (95+ years). Interesting sex-specific patterns emerged across the lifespan: the burden was generally low for both sexes in early life (0–14 years), males consistently presented higher DALY rates in adolescence and young adulthood (15–34 years), the sex difference became less pronounced in middle adulthood (35–59 years), with females showing higher rates in some age groups, and females consistently presented higher DALY rates in older adulthood (60+ years). The data revealed a nonlinear increase in DALY rates with age, with the burden accelerating rapidly after age 60 for both sexes. The highest absolute number of DALYs for males was observed in the 65–69 years age group, whereas for females, it peaked in the 80–84 years age group (Fig. 4B).
Trends and projections in the prevalence of PIs
The prevalence of PIs steadily increased from 1990 to 2021 (Fig. 5A). In 1990, the estimated number of cases was 445,729 (95% UI: 443,576–447,882). By 2021, this figure had risen to 632,888 (95% UI: 630,696–635,080), a 42% increase over the 31-year period. Projections indicate a continued rise in prevalence in the short term, with the number of cases expected to reach 669,961 (95% UI: 645,044–694,877) by 2025, representing an additional 5.9% increase from 2021. The upward trend is anticipated to persist in the medium term, with a projected number of cases of 699,502 (95% UI: 660,531–738,474) by 2030, which is a 10.5% increase from 2021. In the long term, the model forecasts a continued rise in prevalence, albeit at a slightly slower rate. By 2035, the projected number of cases is expected to reach 720,660 (95% UI: 668,620–772,700), a 13.9% increase from 2021. The average annual growth rate in prevalence is projected to decrease slightly over time. From 2021 to 2025, the average annual growth rate is estimated at 1.44%. This rate is expected to drop to 0.86% for the 2026–2030 period and further to 0.60% for the 2031–2035 period (Supplementary Table S5).
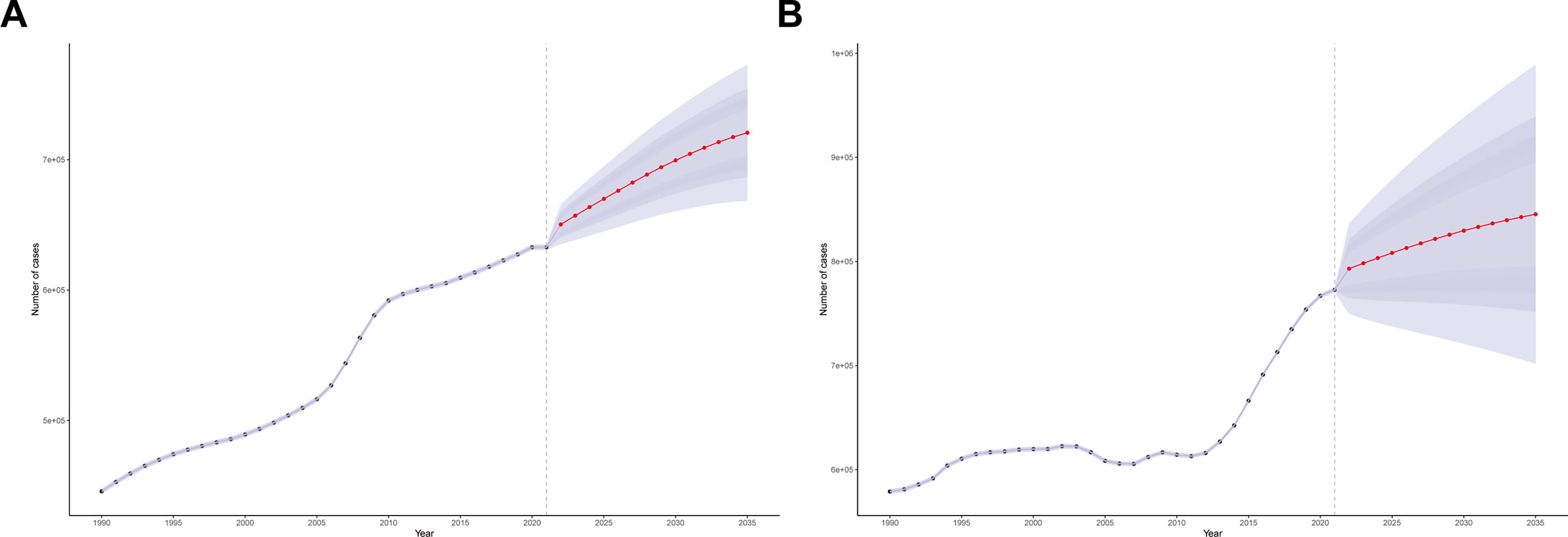
The predictions of global trends from 2022 to 2030.
Our analysis also revealed significant age-specific trends and projections in the prevalence of PIs from 1990 to 2035 (Fig. 6A). The prevalence trends varied across different age groups, with the most notable increases observed in older populations. For example, in the 95+ year age group, the number of cases increased from 5,546 (95% UI: 5,298–5,794) in 1990 to 26,378 (95% UI: 25,445–27,310) in 2021, representing a staggering 375% increase. In contrast, younger age groups experienced more modest changes. The <5 years age group slightly decreased from 1,202 (95% UI: 0–249,356) in 1990 to 988 (95% UI: 0–262,387) in 2021, reflecting a 17.8% reduction. The 5–9 years age group remained relatively stable, with a slight decrease from 3,474 (95% UI: 0–203,842) in 1990 to 3,428 (95% UI: 0–244,758) in 2021, indicating a 1.3% decrease. Looking forward, projections for 2022–2035 predict continued increases across all age groups, with the most dramatic increases expected in the oldest populations. The 85–89 years age group is anticipated to experience a 101% increase, reaching 150,774 (95% UI: 88,850–212,698) by 2035. Even younger age groups, although projected to experience less pronounced increases, will still experience changes, with the <5 years age group expected to decrease slightly to 812 (95% UI: 0–992,958) by 2035, a 17.8% reduction, whereas the 5–9 years age group is projected to decline by 19.3%, reaching 2,766 (95% UI: 0–689,642) cases (Supplementary Table S6).
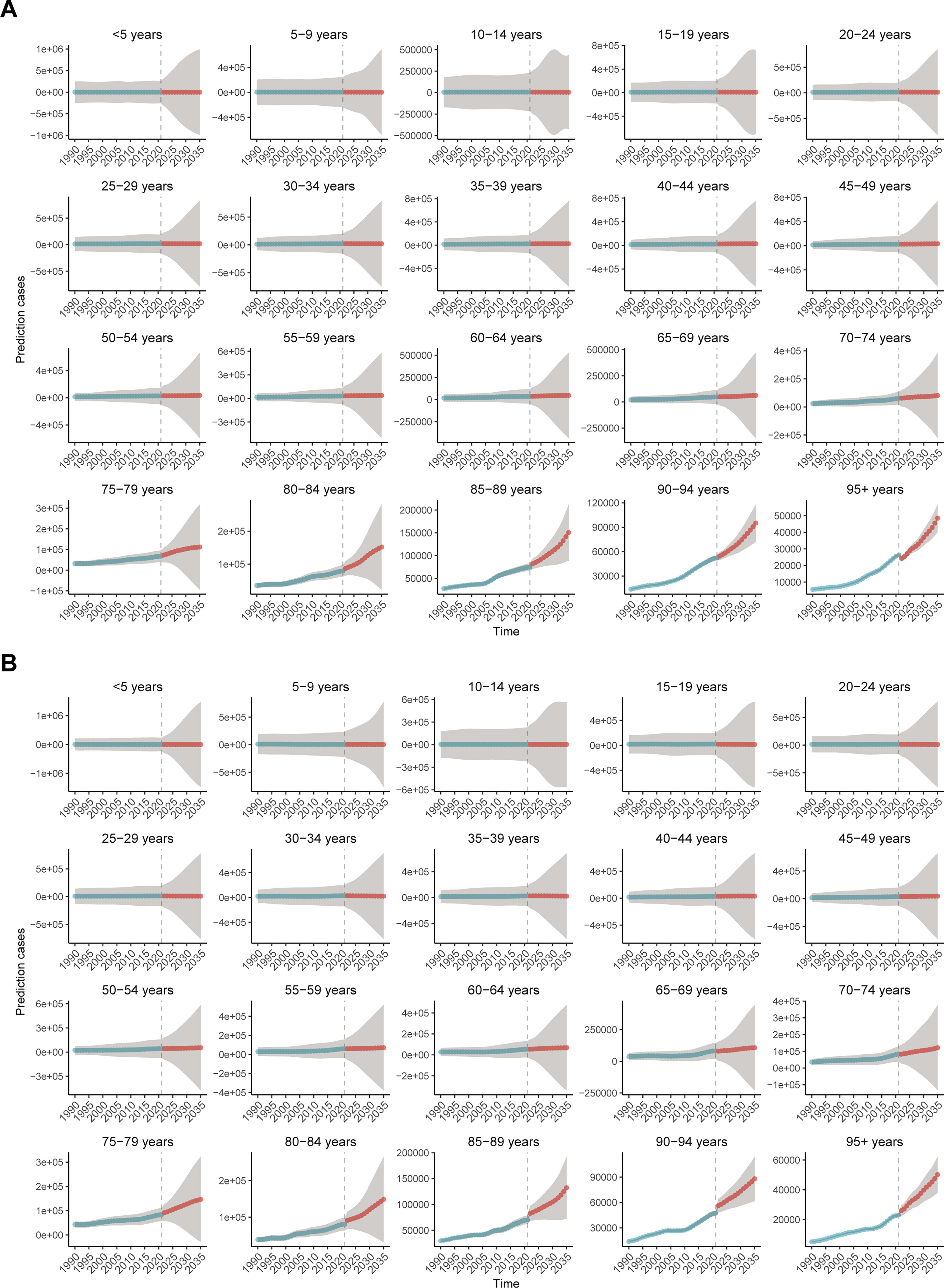
The predictions of global trends in different age groups.
Trends and projections in DALYs due to PIs
Historical trends from 1990 to 2021 showed a steady increase, with DALY numbers rising from 578,956 (95% UI: 576,532–581,381) in 1990 to 772,786 (95% UI: 770,368–775,203) in 2021 (Fig. 5B). This represents a 33.5% increase over 31 years, with an average annual growth rate of ∼0.94%. Key milestones during this period included DALYs surpassing 600,000 in 1995, reaching 610,504 (95% UI: 608,073–612,935), followed by a temporary decline in 2005 to 608,470 (95% UI: 606,151–610,788), and then exceeding 650,000 in 2015, where it reached 666,271 (95% UI: 663,969–668,574) (Supplementary Table S5). This suggests potential stabilization of the burden of PIs, although the absolute number of DALYs continues to rise.
Our analysis also revealed a consistent and substantial increase in the global burden of PIs from 1990 to 2035, as measured by DALYs (Fig. 6B). The estimated global DALY numbers rose dramatically from 578,956 (95% UI: −576,532 to 581,380) in 1990 to 845,365 (95% UI: −701,860 to 988,869) in 2035, representing a nearly 46-fold increase over this 45-year period. Age-specific trends showed distinct patterns, with younger age groups (<50 years) demonstrating lower DALY numbers and slower rates of increase, middle-aged groups (50–69 years) showing moderate DALY numbers with faster rates of increase, and older age groups (70+ years) exhibiting the highest DALY numbers and the fastest rates of increase. Temporally, we observed three distinct phases: a period of relatively slow increase from 1990 to 2000, accelerated growth from 2000 to 2020, and a projected rapid increase from 2020 to 2035 (Supplementary Table S6).
DISCUSSION
Our findings revealed a modest global decline in PIs prevalence. This marginal improvement over three decades underscores the persistent challenge that PIs pose to global health systems. This trend aligns with other studies reporting stagnation in pressure ulcer prevalence across various populations and health care settings.4,12 The stagnation in prevalence rates raises questions about the efficacy of current prevention and treatment approaches.
Socioeconomic, geographic, and demographic disparities
The relatively stable prevalence rates may reflect changing demographics and health care landscapes. As populations age and medical advancements prolong their lives, the pool of high-risk individuals for PIs has expanded. 4 This demographic shift may offset gains made in prevention and treatment. The complex interplay between ageing populations and pressure ulcer risk is well-documented, with comorbidities such as diabetes mellitus, cardiovascular diseases, and chronic kidney disease, playing a significant role in ulcer development among older adults. 4 Although the elderly population constitutes the predominant demographic for PI development, epidemiological data confirm a clinically prevalence rate among nonelderly cohorts. 13 The development of PIs in nonelderly populations may predominantly stem from obesity or malnutrition, mobility impairment (prolonged bed rest, post-orthopedic surgical immobilization), and diabetes mellitus with suboptimal glycemic control. 13 These comorbidities or complications typically elevate the risk of PIs and exacerbate their progression through mechanisms such as impaired blood circulation, increased mechanical stress, and inflammatory responses, among others. Furthermore, distinct risk factors exist across different age groups. In the elderly population, the vulnerability of skin is markedly exacerbated by age-related physiological changes, such as collagen depletion, epidermal atrophy, and microvascular dysfunction, and diminished mobility and reduced adherence collectively render older adults the demographic most severely impacted by PIs. 14 In contrast, among younger individuals, psychiatric disorders (e.g., depression) contribute to neglect of self-care practices, compounded by the escalating prevalence of mental health conditions observed in recent epidemiological trends. 15 Despite advancements in prevention strategies, including comprehensive programs and improved nursing knowledge, the challenge of pressure ulcer prevention remains significant.16,17
The global decline in pressure ulcer DALYs from 10.741 to 9.696 per 100,000 population between 1990 and 2021 shows modest progress but must be interpreted within broader health trends and demographic shifts. 18 Analysis across SDI regions reveals critical disparities. High-SDI regions show improvements due to evidence-based prevention, advanced technologies, enhanced staff education, and quality initiatives. 19 Low-middle- and middle-SDI regions face increasing prevalence rates and fluctuating DALYs, which are attributed to limited resources, insufficient training, a lack of standardized protocols, and rapid urbanization. 20 Low-SDI regions face unique challenges, including limited health care access, low awareness, scarcity of specialized products, and competing health priorities. 21 Addressing these disparities requires a multifaceted approach tailored to specific regional needs, including capacity building, culturally appropriate education, low-cost interventions, and the integration of pressure ulcer prevention into broader health initiatives. 22
The age- and sex-specific prevalence rates of PIs are disproportionate for older adults, particularly women. The sharp increase in prevalence after age 60 underscores the urgency for targeted prevention strategies. 4 The higher prevalence rates in older women than in men highlight the role of biological differences and sociocultural factors. 23 The incidence of PIs can reach 28% in individuals over 65 years of age and up to 40% in intensive care patients. 24 This age-related increase in risk is attributed to factors such as decreased skin elasticity, poor nutrition, and the cumulative effects of chronic diseases. 25 Therefore, health care professionals should adopt a multifaceted approach to prevent and manage PIs, including regular risk assessments, personalized skin care, nutritional support, and the use of advanced pressure redistribution devices. 26 These findings emphasize the need for more targeted research to fully understand the specific roles of age and sex in pressure ulcer development. Only through a deep understanding of these factors can we design truly effective, targeted prevention and treatment strategies to improve health outcomes for patients of all ages and genders. 12
Regional analyses revealed significant disparities in pressure ulcer prevalence trends across different areas. These contrasting trends underscore the complex interplay of socioeconomic factors, health care policies, and cultural attitudes in shaping pressure ulcer rates. Areas with better health care access, education, and preventive measures have shown improved outcomes. 27 Cultural attitudes toward elderly care influence pressure ulcer risk. In regions with prevalent family-based care, rates tend to be lower, but these practices can also lead to underreporting. 4 Undoubtedly, socioeconomic factors play crucial roles, with a strong inverse correlation between a nation’s gross domestic product (GDP) and pressure ulcer prevalence. 19 The improvement of health care infrastructure significantly enhances the clinical environment for patients. Economically advanced regions typically possess state-of-the-art medical equipment and highly specialized health care teams, whereas underresourced areas frequently face challenges such as material scarcity and critical shortages of health care professionals. Health care policies significantly impact pressure ulcer rates. Future policy interventions must prioritize measures including international aid, cross-border medical collaboration, capacity building for frontline health care workers, telemedicine initiatives, and cost containment strategies to address above systemic disparities. Regions implementing comprehensive prevention protocols have seen notable reductions in prevalence. 28 These findings emphasize the need for tailored, region-specific strategies that consider local health care structures, cultural norms, and economic realities. 29 In conclusion, regional variations in pressure ulcer prevalence highlight the complex nature of this health care challenge. Localized studies and culturally appropriate interventions are crucial for reducing the global burden of PIs.
The SDI paradox: Prevalence versus DALY trends
Analysis revealed a complex relationship between the SDI and pressure ulcer outcomes: a strong positive correlation between the SDI and prevalence rates coupled with a moderate negative correlation with DALY rates. This paradox suggests that while higher income and development levels are associated with an increased prevalence of PIs, they also correlate with better management of these conditions, resulting in lower DALY rates. The positive correlation between SDI and prevalence rates may be attributed to factors including ageing populations and advanced health care systems in high-SDI countries, leading to increased detection and reporting. 27 Conversely, the negative correlation between the SDI and DALY rates suggests that health care systems in more developed regions are better equipped to manage PIs effectively. 3 However, this paradox raises questions about the focus of health care systems in high-SDI regions. These data suggest that these systems may be more oriented toward the treatment rather than the prevention of PIs. 30 To address this paradox, health care systems in high-SDI regions should consider rebalancing their approach to pressure ulcer management, including strengthening preventive strategies, enhancing education and training, aligning incentives, and promoting research. 31 In conclusion, the observed relationships between the SDI, prevalence rates, and DALY rates for PIs present both challenges and opportunities for global health policy. This paradox underscores the need for a balanced approach that emphasizes both prevention and treatment, tailored to the specific needs and resources of different regions.
Future projections and strategic imperatives
Projections indicate a concerning increase in PIs prevalence, particularly among the oldest age groups, aligning with global demographic shifts toward an ageing population. By 2035, a significant escalation is predicted, especially in the 95+ age group, attributed to increased longevity, rising chronic conditions, and shifts toward institutional care. 4 To address this challenge, a comprehensive approach is essential. This encompasses implementing standardized, evidence-based prevention protocols; driving technological innovation through smart textiles and AI-powered risk assessment tools; developing personalized care plans; investing in specialized training for health care professionals; enacting sustainable health care policies that prioritize elderly care; increasing research funding; and raising public awareness about pressure ulcer risks and prevention.3,32,33 This projected increase presents both a significant challenge and an opportunity to revolutionize elderly care and chronic wound management.
The findings of this study underscore the pressing need for global, regional, and national strategies aimed at reducing the burden of PIs. Targeted interventions, particularly in high-risk populations, and the integration of pressure ulcer prevention into standard care protocols are essential. Collaborative efforts among health care providers, policymakers, and researchers are vital to address the multifaceted challenges presented by PIs. By doing so, we can improve patient outcomes, reduce health care costs, and increase the overall quality of life for individuals at risk of developing these debilitating injuries.
Limitations
This study has several limitations. First, similar to other GBD studies, this research relies heavily on the accuracy of the original data. Owing to the limitations in data registration and collection across different countries and regions, and potential selection bias, there are instances of data loss, which may lead to an underestimation of the true disease burden of PIs. Second, the BAPC model implemented in this study carries inherent parametric rigidity due to its fixed-interval operationalization of age strata and temporal cycles, which may introduce ecological bias when approximating continuous demographic distributions. Future studies will consider employing eXtreme Gradient Boosting (XGBoost) to validate the robustness of the BAPC model, while capturing nonlinear relationships and dynamic population characteristics through this machine learning framework. Finally, while this study has analyzed PI risk factors through socioeconomic, demographic (gender/age), and health care lenses, certain limitations remain that warrant further investigation to fully elucidate these complex relationships.
KEY FINDINGS
From 1990 to 2021, the global prevalence slightly decreased (8.246–7.920 per 100,000), and DALYs decreased by 9.7%. In high-SDI regions, DALYs decreased by 39.3%, whereas the prevalence increased in middle-(20.5%) and low-middle-SDI regions (28.9%). Prevalence and DALYs peaked in the 95+ year age group, with women over 60 being more affected than men. By 2035, the prevalence of PIs will increase to 720,660 cases globally, impacting ageing populations and low-resource regions.
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
The GBD 2021 study was supported by the Bill and Melinda Gates Foundation. This work was supported in part by the
AUTHORS' CONTRIBUTIONS
H.Y.: Conceptualization, writing-original draft. Y.Z.: Methodology, writing-original draft. H.W.: Formal Analysis, writing-original draft. Y.C.: Data Curation, visualization. X.L.: Visualization, resources. P.W.: Visualization, supervision. J.Z.: Funding Acquisition, writing-review and editing. Z.H.: Funding Acquisition, writing-review and editing. S.L.: Writing-review and editing. All authors have read and approved the manuscript.
AUTHOR DISCLOSURE AND GHOSTWRITING
No ghostwriters were used for this article. The authors have no competing interests to declare.
ABOUT THE AUTHORS
SUPPLEMENTARY MATERIAL
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Data