
Abstract
Objective:
This study aimed to investigate patterns and risk factors associated with co-occurring pressure injuries (PrIs) using real-world clinical data.
Approach:
This retrospective cohort study analyzed electronic health records (EHRs) of adult patients with PrIs from 2015 to 2023 across five hospitals within a large U.S. health care system. An EHR-based phenotype—a set of algorithmic rules using structured clinical data—was developed and validated to identify patients with co-occurring PrIs, enabling classification of all patients in the study cohort into either single-occurring or co-occurring PrI groups. The accuracy of the co-occurring PrI phenotype was assessed through chart review. Univariate analyses and binary logistic regression were employed to identify risk factors associated with co-occurring PrIs. All findings are reported in accordance with the STROBE checklist.
Results:
Among 18,195 patients with at least one PrI record, 4,415 (24.3%) had co-occurring PrIs. The phenotype demonstrated high accuracy (accuracy = 0.96). Pattern analysis showed a direct association between the number of PrIs and severe-stage injuries. Logistic regression revealed that severe PrIs (odds ratio [OR] 3.47; 95% confidence interval [CI]: 3.23–3.74) were most strongly associated with co-occurring PrIs, followed by Black or African American race (OR: 1.45; 95% CI: 1.14–1.84) and spinal cord injury (OR: 1.32; 95% CI: 1.14–1.52).
Innovation:
This study introduces a validated EHR-based phenotype for identifying co-occurring PrIs. It reveals a direct link between co-occurring PrIs and injury severity, as well as unique risk factors associated with co-occurring PrIs.
Conclusions:
Co-occurring PrIs are prevalent and strongly associated with severe PrIs. This study also revealed distinct occurrence patterns, with injury severity increasing as the number of co-occurring PrIs rises. The findings from this study emphasize the need for targeted risk assessment and prevention efforts for co-occurring PrIs.
INTRODUCTION
Pressure injuries (PrIs) are defined by the National Pressure Injury Advisory Panel (NPIAP) as “A pressure injury is localized damage to the skin and/or underlying soft tissue, usually over a bony prominence or related to a medical or other device.” To support clinical decision-making, treatment, and prevention, the NPIAP classifies PrIs by severity into stages 1–4, deep tissue injury (DTI), unstageable injury, and mucosal membrane PrI. 1 In the United States, more than 2.5 million patients develop PrIs annually, resulting in significant pain, reduced quality of life, prolonged hospital stays, and an estimated $26.8 billion in treatment costs.2,3 Known PrI risk factors include low physical activity, incontinence, older age, lower albumin level, malnutrition, stay in intensive care unit, comorbidity, and anemia.4–6 Despite the development of prevention strategies, PrI-related mortality remains significant at 7.6%. 2 Additionally, previous studies have shown that having an initial PrI significantly increases the risk of developing additional new PrIs.7–9 While single PrIs are well-studied, co-occurring PrIs (multiple simultaneous PrIs in a patient) remain underexplored. Studies indicate that 28% to 47.2% of PrI patients experience co-occurring PrIs, yet research on their risk factors and clinical impact is limited.10–13 Understanding the patterns, risk factors, and severity associations of co-occurring PrIs is crucial for improving patient outcomes.
Veysel Karani Baris, RN, PhD
Clinical problem addressed
Despite advances in PrI risk assessment and prevention, co-occurring PrIs remain a critical yet underrecognized clinical issue. Co-occurring PrIs may be associated with higher severity outcomes and prolonged healing times, which may contribute to longer hospital stays and increased health care costs.9,10 Standard PrI risk assessment tools are often inadequate for identifying patients at risk of multiple PrIs, as they do not account for co-occurring PrI susceptibility. Furthermore, existing evidence-based prevention strategies are largely based on single-PrI models, leaving a gap in targeted interventions for patients experiencing multiple PrIs. 7
By addressing these gaps, this study provides critical insights into the risk factors, patterns, and clinical impact of co-occurring PrIs, which can guide prevention and intervention strategies. Findings from this study have the potential to enhance clinical decision-making, optimize resource allocation, and improve patient outcomes in PrI management.
The aim of this study was to examine occurrence patterns and related risk factors of patients with co-occurring PrIs using electronic health record (EHR) data from five hospitals within a large, integrated health care system.
MATERIALS AND METHODS
Data source and initial cohort development
For this retrospective cohort study, patients with PrIs were identified from a centralized clinical data warehouse with five independent Harvard-affiliated hospitals within the Mass General Brigham Healthcare System.
Each patient was assigned an individual ID, and a separate hospitalization ID was generated for each admission. PrI details—including stage, location, and date—were extracted from structured nursing documentation flowsheets, which include a dedicated “pressure injury” section focused on daily skin assessments and clinical observations. When a PrI is identified, nurses document the date, time, stage, location, and whether it was present upon admission.
The initial cohort included 19,853 patients aged 18 or older with at least one recorded PrI documented between 2015 and 2023.
Developing the co-occurring PrI phenotype
The study population was divided into two PrI groups based on definitions defined by our expert team: the single-occurring PrI group and the co-occurring PrIs group.
To identify patients with co-occurring PrIs using EHR data, a multivariable phenotyping algorithm was created using patient IDs, hospitalization IDs, the dates of occurrence, and date of resolution of PrIs. Some patients may have several hospital admissions, and each admission was handled separately. The steps used to develop the Co-occurring PrI Phenotype Algorithm are included below: Group each patient’s PrI records using a unique patient ID. Filter out patients with only one PrI record (assign single-occurring PrI group). For patients with more than one PrI record, group their records by unique hospitalization ID. Filter hospitalizations that have fewer than two PrI records (assign single-occurring PrI group). Identify hospitalizations where there is more than one PrI record on the same date using injury occurrence and resolution time. Identify hospitalizations where co-occurring PrIs are in the same anatomical location and have the same orientation (e.g., two PrIs on the right buttock)—(exclude these hospitalizations).
To ensure that each PrI in co-occurring cases was truly distinct, we applied strict inclusion criteria during phenotype development. Cases with multiple PrIs documented at the same anatomical location and orientation (e.g., two injuries on the right buttock) were excluded to avoid misclassification or overcounting. This approach ensured that each co-occurring injury represented a unique, clinically distinguishable event rather than a subdivision or duplicate documentation of a single injury. This distinction was further confirmed through manual chart review by two independent nurse experts.
An example of the algorithm is included as Supplementary Fig. S1 in the Supplementary Data.
Validation of co-occurring PrI phenotype against the gold standard
The charts of 200 randomly selected patients (100 with co-occurring PrIs and 100 with single PrIs) were manually reviewed to validate the co-occurring PrI phenotype. We calculated the required sample size using the method described by Liu et al. (2021), which is specifically designed for validating EHR phenotyping algorithms based on predefined sensitivity and specificity targets. 14 Assuming expected sensitivity and specificity values of ≥95% and a 5% margin of error, the minimum required sample size was determined to be 73 cases per group. To exceed this threshold and strengthen the robustness of our validation, we reviewed a total of 200 cases—comprising 100 co-occurring and 100 single-occurring PrI cases. Two trained nurse experts from the study team independently reviewed patients’ EHRs. The goal of the chart review was to determine, based on all available documentation, whether the patient experienced a single PrI or multiple distinct PrIs that were simultaneously present during hospitalization. They examined structured nursing flowsheets, skin assessment documentation, and PrI-related entries to determine whether each patient truly had single or co-occurring PrIs during their hospitalization. The manual chart review classifications were accepted as the gold standard and compared with the classifications identified using the phenotype. Phenotype performance was evaluated using sensitivity, specificity, negative predictive value (NPV), positive predictive value (PPV), precision, accuracy, and F1-score, which is the harmonic mean of precision and recall and provides a balanced measure of test performance.
The data extraction, algorithm application, and chart review process are summarized in Fig. 1.
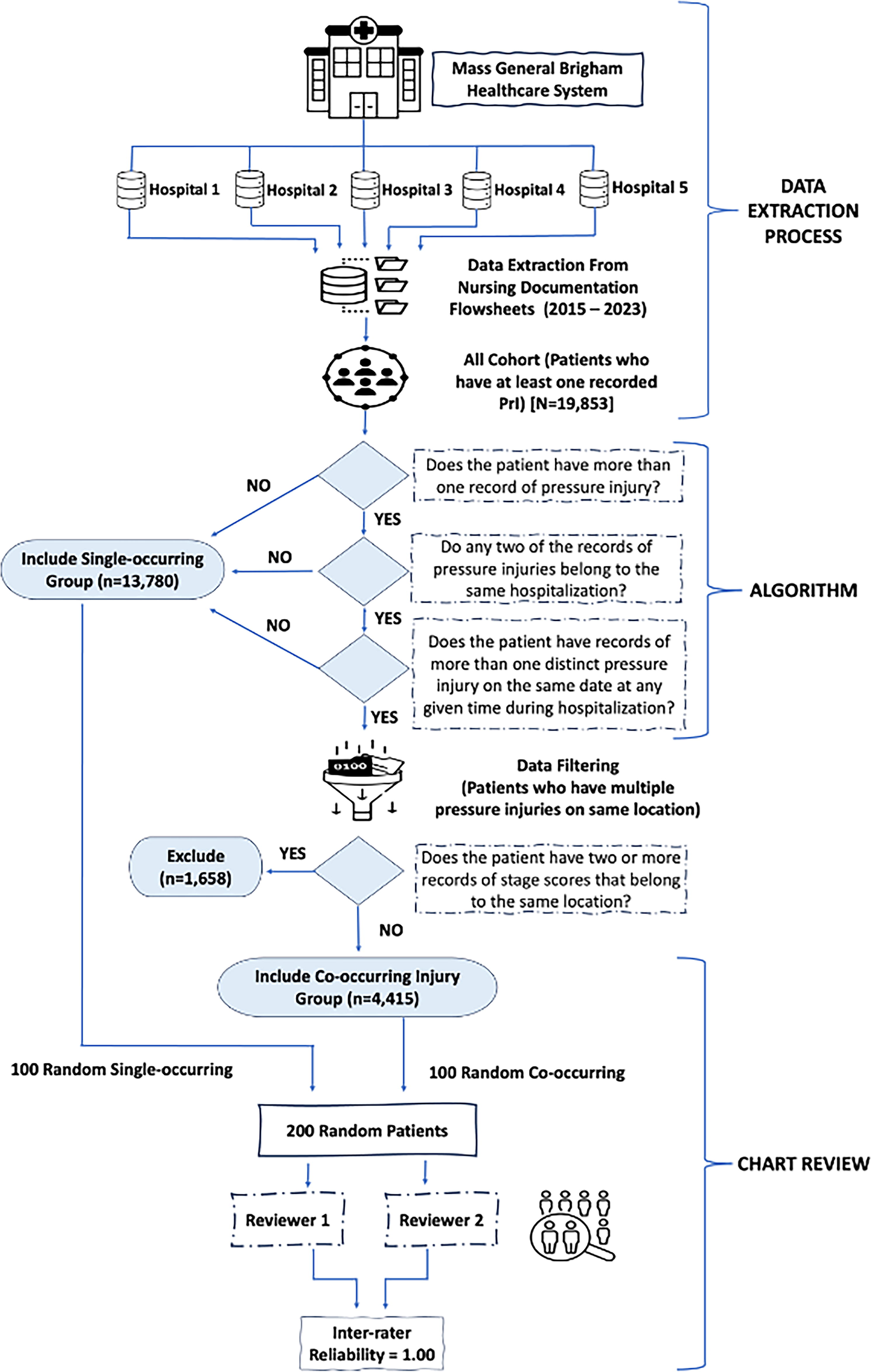
Data extraction, algorithm, and validation process. A simplified overview of the workflow used to develop and validate the algorithm. Clinical and administrative data were extracted and processed to identify relevant pressure injury cases. Key variables were input into the algorithm, which stratified cases based on the number of pressure injuries. Validation was performed through statistical comparisons and clinical chart review to ensure accuracy and reliability.
Outcome and risk factor assessment
The primary outcome was the occurrence of at least one co-occurring PrI. PrIs were classified using NPIAP guidelines 1 and included stages 1–4, deep tissue, and unstageable injuries. Following clinical expert recommendations, patients with multiple PrIs at the same anatomical location (e.g., two PrIs on the right buttock) were excluded to avoid confounding, as these injuries could be interrelated and often managed as a single PrI. Patients with mucosal PrIs were excluded, as these occur on mucous membranes and cannot be staged using standard classification due to the tissue type involved.
Potential risk factors for co-occurring PrIs were identified through a comprehensive literature review and validated by clinical experts.10–12 These included: Having severe stage PrI Age Length of stay (LOS) Gender Race Comorbidity score (Charlson Comorbidity Index [CCI]
15
) Spinal injury Hypotension Cancer Cardiovascular disease Diabetes ICU stay Laboratory markers (albumin, Blood Urea Nitrogen (BUN), chloride, creatinine, hemoglobin) Braden subscale scores (sensory perception, activity, mobility, friction and shear, nutrition, moisture) Body mass index (BMI) Ventilation use Vasopressor use
Early stage PrIs (Stages 1–2) and severe-stage PrIs (Stages 3–4, unstageable, deep tissue injuries) were grouped based on expert consensus and prior research.16,17
Data were extracted from EHRs, including demographic and clinical variables. Age and BMI were continuous variables, while gender and race were categorical. LOS was calculated from admission and discharge dates. The CCI was derived from International Classification of Diseases (ICD) codes. 15 ICU stays, ventilation, and medication use were determined from flowsheets, medication administration records, and Rx.NORM codes. Braden subscale scores were included to avoid multicollinearity with the total score. For all diagnoses, laboratory results, ventilation status, and medications, the study team aimed to use records from the period prior to the PrI assessment date to ensure that these variables reflected the patient’s status before injury identification. However, due to variations in documentation and care trajectories, this was not possible for all patients. In cases where PrIs were documented at the time of hospital admission, data recorded on the same day as the PrI assessment were used.
Data analysis
Group comparisons
Mean, standard deviation, numbers, and percentages were used for descriptive statistics. Normally distributed numeric variables were compared using the independent t-test, while non-normally distributed variables were analyzed with the Mann–Whitney U test. The association between categorical variables was assessed using the chi-square test. A p-value less than 0.05 was the statistically significant threshold.
Identifying risk factors associated with co-occurring PrIs
A binomial logistic regression analysis was performed to identify risk factors associated with co-occurring PrIs among patients with at least one PrI. The binary dependent variable was the presence of co-occurring PrIs. Independent variables included in the model were selected based on prior research and expert recommendations. Given that previous studies 16 have reported a U-shaped relationship between BMI and PrI occurrence, a scatter plot of residuals was examined against BMI to confirm this pattern. Based on this analysis, both linear and quadratic BMI terms were included in the logistic regression model.
The results were expressed as odds ratios (ORs) with corresponding 95% confidence intervals (CIs) and p-values. Model performance was evaluated using the C-statistic, while multicollinearity among independent variables was assessed by calculating variance inflation factors (VIFs). Electronic laboratory notebook was not used.
RESULTS
Validation of co-occurring PrI phenotype against the gold standard
Based on the comparison between the results of the chart review and the co-occurring PrI phenotype, the sensitivity was calculated as 0.969, specificity as 0.960, NPV as 0.970, PPV as 0.960, accuracy as 0.965, F1-score as 0.964, and precision as 0.960 (Supplementary Table S1 in Supplementary Data).
The chart review identified only one phenotype misclassification. Detailed examination of the patient’s records uncovered a reporting error, as all entries referred to the same PrI event.
Characteristics of PrIs study cohort
Our study cohort included 19,853 patients. After excluding 1,658 patients with multiple PrIs at the same anatomical location or mucosal PrIs, 25,124 PrIs across 18,195 patients were analyzed. Among these, 13,780 had single PrIs, and 4,415 had co-occurring PrIs. The characteristics of PrIs are summarized in Table 1. The top five PrI locations were consistent across groups but differed in rank order. For single PrIs, the coccyx was most common (50.4%), followed by the buttocks (29.2%), sacrum (10.4%), heel (7.1%), and back (2.9%). Among co-occurring PrIs, the coccyx remained most frequent (21.5%) but with reduced prevalence, followed by the buttocks (20.4%), heel (14.7%), sacrum (5.9%), and back (4.6%), with other locations comprising nearly 34%.
Characteristics of pressure injuries
DTI, deep tissue injury.
The distribution of PrI stages also varied between groups. In single-occurring PrIs, Stage 2 was most common (41.5%), followed by Stage 1 (26.7%) and DTI (12.8%). In co-occurring PrIs, Stage 2 remained most frequent (33.7%), but unstageable injuries (21.6%) and DTI (20.2%) were more prevalent.
A trend of increasing PrI severity was observed with higher numbers of co-occurring injuries (Fig. 2). Among single-PrI cases, 68.1% of injuries were early stage (Stages 1 and 2), and 31.9% were severe-stage (Stages 3, 4, DTI, and unstageable). In patients with seven or more PrIs, severe-stage injuries rose to 72.6%, with early stage injuries dropping to 27.4% (Table 1).
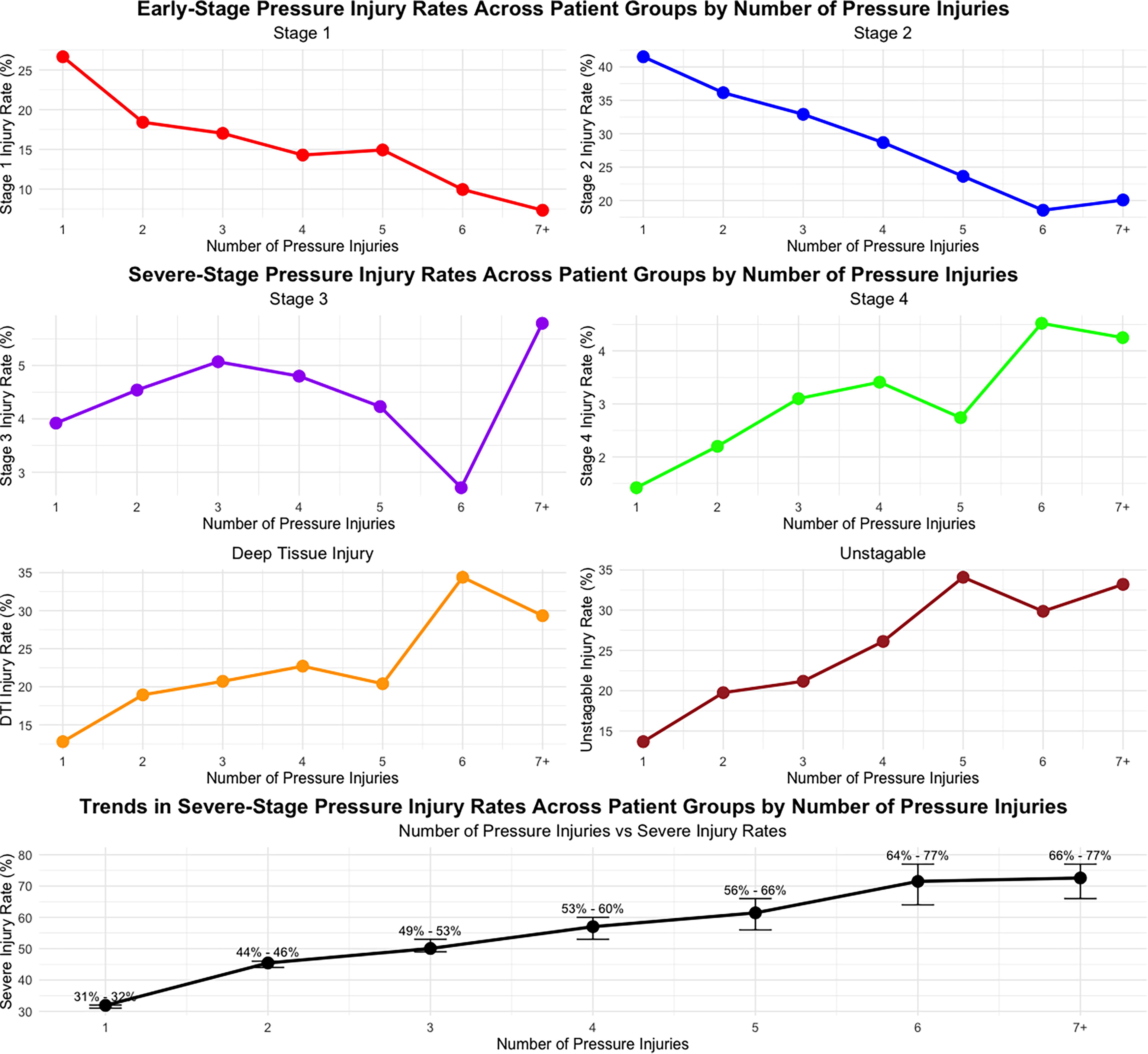
Stage levels based on number of pressure injuries. A line graph illustrating the relationship between the number of pressure injuries and the corresponding severity rate. Each data point represents the average severity rate stratified by the number of pressure injuries. The trend suggests a positive association, with higher injury counts corresponding to increased severity rates. This highlights the potential utility of injury count as a proxy for severity stratification.
Characteristics of the single-occurring and co-occurring PrI patient groups
Among the total 18,195 patients analyzed, 13,780 (75.7%) had single-occurring PrIs, and 4,415 (24.3%) had co-occurring PrIs. The cohort’s mean age was 71.85 (15.41) years, with 54.5% male and 83.5% White.
Table 2 presents a comparison of PrI characteristics between the single-occurring and co-occurring PrI groups. Statistically significant differences between the PrI groups were identified for several variables, including age, LOS, BMI, Braden total score, and all Braden subscales (sensory perception, moisture, activity, mobility, nutrition, friction and shear), albumin, BUN, hemoglobin, creatinine, gender, race, injury severity, spinal cord injury, cardiovascular disease and cancer diagnosis, staying at ICU, ventilation use, vasopressor use, and discharge status.
Comparison of characteristics between single and co-occurring pressure injury groups
Values in bold indicate statistical significance.
Independent simple t-test.
Mann–Whitney U test.
Chi-square test.
BMI, body mass index; CCI, Charlson Comorbidity Index; SD, standard deviation.
mr = Mean rank
Risk factors associated with co-occurring PrIs
Logistic regression analysis identified several factors that significantly increased the risk of co-occurring PrIs in patients with PrIs (Table 3). These factors included increasing age (95% CI: 1.0001–1.005), longer LOS (95% CI: 1.010–1.014), male gender (95% CI: 1.010–1.174), having severe PrI (95% CI: 3.230–3.740), Black or African American race (95% CI: 1.137–1.844), higher CCI Index Score (95% CI: 1.001–1.033), having spinal cord injury (95% CI: 1.141–1.520), not having cancer diagnosis (95% CI: 0.713–0.878), lower albumin levels (95% CI: 0.830–0.928), higher BUN (95% CI: 1.002–1.006), lower chloride levels (95% CI: 0.995–0.996), and lower scores on the Braden subscales for sensory perception (95% CI: 0.883–0.987), activity (95% CI: 0.785–0.879), friction and shear (95% CI: 0.691–0.791), and moisture (95% CI: 0.866–0.975).
Multivariate logistic regression analysis of risk factors for co-occurring pressure injuries
Values in bold indicate statistical significance.
References: race = other, gender = female, severity = early stage.
β, logistic regression coefficient (log-odds); SE β, standard error of the coefficient; Wald chi-square test (χ2), test statistic used to assess the significance of each coefficient.
CI, confidence interval; LOS, length of stay; OR, odds ratio.
I (BMI2): Quadratic term of BMI (BMI squared).
VIFs of all variables were less than 2 in the regression model, except for BMI’s linear and quadratic terms. The area under the curve was 0.73.
Additionally, logistic regression analysis showed that the linear term of BMI had a significant negative association with the likelihood of having co-occurring PrIs (95% CI: 0.946–0.981), while the quadratic term of BMI had a significant positive effect on having co-occurring PrIs (95% CI: 1.0002–1.0007). This result indicates a U-shaped relationship between BMI and the likelihood of having co-occurring PrIs among patients with PrI. The analysis further showed that a BMI of 35–40 minimized the probability of having co-occurring PrIs (Supplementary Fig. S2 in Supplementary Data).
DISCUSSION
PrIs have significant implications for patients and health care systems, leading to substantial suffering, reduced quality of life, increased mortality, and higher health care costs. Co-occurring PrIs may exacerbate these outcomes, potentially following distinct occurrence patterns and risk factors compared with single-occurring PrIs.11,12 Prior small-scale studies have found that certain established risk factors for initial PrIs are not significant predictors for co-occurring PrIs.10–13 This highlights the critical need to assess the risk of co-occurring PrIs in patients with existing injuries. Reflecting this, the joint clinical practice guidelines from the European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel (NPIAP), and Pan Pacific Pressure Injury Alliance recommend considering “the potential impact of an existing pressure injury of any Category/Stage on the development of additional pressure injuries.” 4 In this study, we examined the occurrence patterns of co-occurring PrIs, their relationship with PrI severity, and the risk factors associated with their development.
A computable phenotype was developed and validated to identify co-occurring PrIs using routinely collected EHR variables. When compared with the gold standard, this phenotype demonstrated high performance. 18 Specifically, a manual review of 200 cases (100 co-occurring and 100 single-occurring PrIs) showed strong agreement. Our method overcomes the limitations of ICD code-based approaches, which are susceptible to entry errors and coding inaccuracies.19,20 The high PPV and NPV further underscore its precision. This validated phenotype offers a standardized and reproducible approach for identifying patients with co-occurring PrIs across diverse health care settings.
The rate of co-occurring PrIs in our study was lower than in previous reports,10–13,21 likely due to differences in study populations. Earlier studies focused on specific, limited populations at high risk for PrIs, whereas our analysis used a multihospital dataset with a diverse patient population from all inpatient units. This broader inclusion enhances the generalizability of our findings.
PrI severity varied significantly between single and co-occurring injury groups. Patients with co-occurring PrIs had more severe injuries compared with those with single-occurring PrIs, and the proportion of severe-stage injuries increased with the number of co-occurring PrIs. Two potential explanations may account for this trend: (1) Co-occurring PrIs may increase the complexity of treatment and care, making it more challenging for health care professionals to manage them effectively and in a timely manner. PrIs in multiple locations limit repositioning options and require individualized care for each injury, which may worsen overall outcomes and lead to more severe injuries; and (2) in patients with an existing severe PrI, health care providers may focus on treating the existing injury, which may unintentionally lead to less attention being given to preventive measures for new injuries. This could result in a higher likelihood of co-occurring PrIs in patients with an existing severe injury.
In their meta-analysis, Song et al. (2019) reported that PrIs increase mortality risk among older adults. 22 Although our study included patients of all ages, mortality was higher in those with co-occurring PrIs compared with single-occurring PrIs. This finding reinforces the notion that while a single-occurring PrI can increase mortality risk, co-occurring PrIs may further elevate this risk. While the association between PrIs and increased mortality is well established, the precise mechanisms remain unclear. PrIs may serve as markers of severe underlying illness, contributing to complications that increase the risk of death. 22 Co-occurring PrIs may amplify this risk by exacerbating these complications.
Our logistic multivariate model provided new insights into the risk factors for co-occurring PrIs. While univariate analysis linked low hemoglobin levels and vasopressin to co-occurring PrIs, the multivariate analysis did not confirm these associations, suggesting that these factors may increase risk primarily in specific patient groups, such as those who are mechanically ventilated. 12 Surprisingly, despite being major risk factors for PrIs, mobility and nutrition showed no association with co-occurring PrIs, possibly reflecting limitations in the Braden scale’s sensitivity to these domains.10–13 In contrast, moist skin, a known PrI risk, 9 was associated with co-occurring PrIs in our study, whereas other research suggests a link with dry skin, potentially due to dehydration in surgical patients. 10 Our analysis also revealed new associations that have not been previously reported. These factors include age, male gender, Black or African American race, CCI, spinal cord injury, and specific lab markers (BUN, chloride, creatinine). Additionally, significant associations were found with the Braden subscales for sensory perception and activity. Finally, our study found a U-shaped relationship between BMI and co-occurring PrIs, where both low and high BMI values were associated with higher risk of co-occurring PrIs. This pattern aligns with previous research on general PrIs15,23 and may assist clinicians in improving BMI-based prevention strategies for co-occurring PrIs. These findings underscore the importance of broadening co-occurring PrI assessments beyond traditional metrics.
Limitations
Our study has several limitations. First, the phenotype was developed within a specific hospital system where PrIs are documented individually, which may differ from practices in other institutions, requiring adjustments for variability. However, the documentation requirements are based on the NPIAP guidelines, so they should be generalizable to systems that have also structured clinical documentation based on this national standard. Second, reliance on occurrence and resolution dates from nursing flowsheets may introduce bias due to potential data entry errors. Third, clinical notes were not included, which might offer additional insights into co-occurring PrIs. Incorporating these notes in future studies could enhance phenotyping accuracy.
Additionally, although our dataset included key physiological and laboratory indicators (e.g., albumin, BUN, creatinine), it lacked information on several clinically relevant factors, such as preadmission care, antibiotic use, wound swab results, sepsis, pressure-relieving surface use, and anthropometric measures like skinfold thickness. We were also unable to capture time from immobility onset to PrI occurrence, or contextual care details such as caretaker support and care setting, due to limitations in structured EHR fields.
While our study included patients hospitalized during the COVID-19 pandemic, the EHR data did not allow us to assess how COVID-19 infection, associated immobility, or changes in care practices (e.g., isolation protocols, proning) may have influenced the risk of co-occurring PrIs. Future research should explore these pandemic-related factors in greater detail. Finally, although the inclusion of a broad inpatient population enhances generalizability, variability in age and primary etiology may have influenced outcomes; future research should consider stratified analyses to address this heterogeneity.
KEY FINDINGS
The validated EHR-based phenotype for identifying co-occurring PrIs demonstrated high accuracy (96%), with 0.969 sensitivity, 0.960 specificity, 0.964 F1-score, and 0.960 precision, confirming its reliability for large-scale analysis. While the coccyx remained the most common PrI site in both single and co-occurring PrI groups, co-occurring PrIs exhibited a broader distribution across multiple anatomical locations. This is the first study investigating co-occurring PrI patterns. A clear trend was observed where patients with multiple PrIs were more likely to develop severe-stage injuries. In contrast to single PrIs, where 68.1% were early-stage injuries, patients with seven or more PrIs had a 72.6% prevalence of severe-stage PrIs. Logistic regression analysis identified severe PrI (OR: 3.47), Black or African American race (OR: 1.45), and spinal cord injury (OR: 1.32) as key risk factors for co-occurring PrIs. Additionally, a U-shaped relationship between BMI and co-occurring PrI risk was discovered, with the lowest probability occurring at a BMI of 35–40.
INNOVATION
Co-occurring PrIs can develop as a progression of an initial PrI or due to independent risk factors. While existing literature has identified risk factors for single PrIs, comprehensive analysis of co-occurring PrIs using large-scale EHR data has not been conducted. Prior research on co-occurring PrIs has been limited to small sample sizes and specific patient groups,10,11 leaving a critical gap in understanding their clinical patterns and risk associations.
This study introduces and validates an EHR-based phenotype to systematically identify co-occurring PrIs across a large, multihospital dataset. This novel methodology allows for quantification of co-occurring PrIs at scale, identification of unique risk factors, and assessment of their association with injury severity.
CONCLUSION
This study offers novel evidence and insights into the occurrence patterns and associated risk factors of co-occurring PrIs. One of the key innovations of the research is the development of a validated, computable EHR-based phenotype for identifying co-occurring PrIs. This phenotype represents a valuable tool for both researchers and health care providers in the PrI field.
Using developed phenotypes, this study found that patients with co-occurring injuries were more likely to experience severe injuries, which tend to be overlooked in current clinical practice. Future research should explore the potential causal relationship between co-occurring PrIs and severe PrIs, specifically examining whether the severity of an initial injury could increase the likelihood of additional injuries. More effective preventative strategies are also needed to reduce the burden of co-occurring PrIs in hospitalized patients. These strategies should go beyond current single-PrI prevention protocols and incorporate dynamic risk reassessments throughout hospitalization, especially after the development of an initial PrI, intensified repositioning schedules, real-time skin monitoring technologies, and increased interdisciplinary collaboration may be particularly beneficial for patients with existing injuries. Preventative strategies for co-occurring PrIs may also require a shift toward individualized care plans that account for cumulative risk, anatomical constraints, and limitations in mobility imposed by existing PrIs.
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
This study was funded by
AUTHORS’ CONTRIBUTION
The authors made the following contributions to the study: study conception and design—P.C.D., V.K.B., and W.S.; data analysis—V.K.B., W.S., M-J.K., L.L., and G.L.; provision of clinical and technical expertise—P.C.D., L.S.G., T.M., S.C., D.L.C., D.F., W.G-F., L.H., B.M., J.M., L.D.M., and P.W.; study supervision—P.C.D. All authors participated in article development and are accountable for the integrity of this work.
AUTHOR DISCLOSURE AND GHOST WRITING
The authors have no conflicts of interest to declare.
ABOUT THE AUTHORS
SUPPLEMENTARY MATERIAL
Supplementary Data