
Abstract
Category emergence has been a central question in organization theory. Yet, we still do not understand what drives category persistence and updating during emergence as new information arises. We investigate this question through a rich set of oral histories and archival materials on the emergence of the category AIDS from 1978 to 1985. We show that the initial proto-category’s features and causal theories cohered with its stigmatized moral meanings. Over time, anomalies challenging these features and theories spurred a minority of medical professionals to update the category’s causal theory. However, a silent majority resisted updating the category because the new causal theory conflicted with the proto-category’s moral meanings, challenging the clear moral boundary dividing what was perceived as worthy from what was perceived as unworthy. As a result, the majority silenced the vocal minority’s updated understandings and withheld resources from the category. This article contributes to the literature on categorization by showing that conflicts between category dimensions can stifle updating, amplify imprinting, and prolong category persistence. Particularly, the dichotomous nature of the moral dimension might hinder the updating of other dimensions, such as the causal one, despite accumulated evidence suggesting the need for updates. We show that calls for category updating backed solely by rational arguments may fail to persuade the silent majority and may falter until the moral boundary is punctured and the category is morally reappraised.
In 1981, medical professionals in the United States began to notice an extremely unusual type of bacterial pneumonia and rare skin cancer among several homosexual men. They referred to the new disease as “gay cancer” or “gay-related immunodeficiency” (GRID), and the category quickly became infused with deeply stigmatized moral meanings. Over time, a small minority of medical professionals realized that the disease could be transmitted through blood to individuals across various demographics, and they updated its label to “Acquired immunodeficiency syndrome” (AIDS). However, the updated theory that AIDS was not only a disease among homosexual men but also a serious threat to general public health faced strong resistance from a majority of medical professionals and broader audiences. A vocal minority’s demands to allocate more resources to AIDS and to introduce preventive measures met skepticism and silence. The silent majority’s persistence in their category understanding had dire organizational and social consequences, leading to the withholding of resources while the virus spread unchecked. In retrospect, this case poses a significant empirical question: why did the initial perception of AIDS as a gay disease persist despite strong evidence to the contrary? Why was it so difficult for the majority to update the category?
This case not only triggers an interesting empirical puzzle, but it also raises critical theoretical questions concerning the process of category persistence and updating during category emergence (Durand and Khaire, 2017). Categories are defined as groupings of objects or entities that are perceived as similar (Kennedy and Fiss, 2013; Anthony, Nelson, and Tripsas, 2016; Arjaliès and Durand, 2019). Category updating happens when the category schema—a system of interlocking meanings and knowledge about a category structured along different dimensions—is revised in the face of new information (Khaire and Wadhwani, 2010; Bingham and Kahl, 2013; Boghossian and David, 2021). In contrast, category persistence occurs when the category schema remains unchanged (Pontikes and Barnett, 2015; Glaser, Fiss, and Kennedy, 2016). Scholars have suggested that during emergence, audiences update the category as the category schema gradually reflects an influx of new information about the category (Khaire and Wadhwani, 2010; Jones et al., 2012; Grodal, 2018; Hannan et al., 2019). For example, Bingham and Kahl (2013) examined how audiences updated the schema of the category “computer” as new offerings were introduced: they gradually shifted from drawing analogies between computers and preexisting machines to perceiving computers as being similar to human brains. Likewise, Hsu and Grodal (2021) illustrated how audiences updated the schema of the e-cigarette category as more information arrived, increasingly perceiving it as morally reprehensible.
Yet, in the nascent stages of emergence when categories are still unstable proto-categories, imprinting from their initial conditions can make it difficult for updating to occur smoothly (Marquis and Tilcsik, 2013). The first salient information about a category may play an outsize role in shaping the category schema, and new information about the category may clash with these initially imprinted understandings (Rhee et al., 2017). Furthermore, category updating might encounter resistance from actors who benefit from the existing social structures and patterns of resource allocation (Lamont and Molnár, 2002; Lee, Hiatt, and Lounsbury, 2017; Grodal, 2018). Therefore, during category emergence, tension can exist between category persistence as a result of imprinting and the need for category updating based on new information. Despite these tensions, our understanding of what drives category persistence and updating during emergence remains limited.
Understanding the dynamics of category persistence and updating is crucial because categories impact audiences’ evaluations of individuals and organizations, influencing their decisions on rewards, penalties, and resource allocation (Lamont and Molnár, 2002; Lounsbury and Rao, 2004; Lamont, 2012). Failing to update a category in response to new information can result in human suffering and organizational costs because such failure might stifle precautionary actions and strategic initiatives (Hsu and Grodal, 2015; Lashley and Pollock, 2020). Furthermore, failing to convince broader audiences to update categories poses a challenge for proponents of categories. For instance, in order for the whole stem cell category not to falter, proponents of the category must devise strategies to convince powerful audiences to redraw their boundary of what they consider to be human and not human (Evans, 2021). Advocates of mandatory childhood vaccination may face the complex task of guiding audiences to revise their perception of what is natural and unnatural (Goldberg and Stein, 2018). In a broader sense, without understanding how categories persist or are updated in light of new information, we might not be able to combat important societal problems such as increasing political polarization, skepticism of science, and the persistence of misinformation (Vosoughi, Roy, and Aral, 2018).
To deepen our understanding of category emergence, we must unpack how the persistence or updating of a category schema occurs. Category schemas often comprise multiple dimensions (e.g., moral meanings associated with a category, causal theories explaining its functioning) that are compatible and do not invoke cognitive dissonance (Barsalou, 1983; Murphy and Medin, 1985; Gavetti, Levinthal, and Rivkin, 2005). For instance, the causal theory linked to the category “marijuana” (i.e., it can induce psychoactive effects) used to be aligned with the category’s stigmatized moral meaning. However, when new information emerged suggesting that marijuana could offer therapeutic benefits to people with certain medical conditions, the updated causal theory conflicted with this moral meaning (Lashley and Pollock, 2020; Khessina, Reis, and Verhaal, 2021).
Audiences tend to selectively adopt ideas and meanings that cohere with one another (Lo et al., 2020; Soublière, Lo, and Rhee, 2023); thus, if an updated dimension collides with other dimensions, some audiences may cling to their original understandings of the category. In the case of marijuana, such conflicts may have hindered its establishment as a legitimate medical product (Hsu, Kocak, and Kovács, 2018). Furthermore, certain category dimensions, such as the moral dimension, tend to be dichotomous because they position entities and people as polar opposites and, thus, pose challenges to category updating. Reconceptualizing an entity from one extreme (e.g., the sacred) to the other (e.g., the profane) often proves difficult. For instance, categorizing a “priest” as a “sex offender” presented challenges for certain audiences because these categories were associated with opposite moral meanings, leading to delays in revising beliefs and taking corrective actions to crimes (Gutierrez, Howard-Grenville, and Scully, 2010).
Indeed, the extant literature has emphasized that category persistence and updating are not only cognitive processes but also social and political processes that occur at the intersection of different social groups (Strauss, 1978; Becker, 1982; Quinn and Munir, 2017; Hsu and Grodal, 2021). Different social groups might vary in their category understandings, adhere to different sets of ideas that cohere with one another, and establish different boundaries for a category (Lamont and Fournier, 1992; Cornelissen and Werner, 2014; Grimes, Williams, and Zhao, 2019). Contestation arises regarding what is sacred, valuable, and acceptable versus what is profane, worthless, and taboo (Durkheim, 1912; Durkheim and Mauss, 1967). These processes are not devoid of power dynamics (Foucault, 1977; Bourdieu, 1987; Fairclough, 2013). As power is unevenly distributed across different social groups, some groups may exert greater influence in shaping category persistence and updating, while others are marginalized. Overall, during category emergence, tensions exist between category persistence and updating.
We unpack these tensions by drawing on an extensive corpus of oral histories and archival materials about the emergence of the category AIDS. Our findings reveal that when updating one category dimension requires simultaneous updates in other dimensions, category schemas may not update as new information arises. In contrast to the model of gradual updating often assumed in the literature, some category dimensions are updated discontinuously, i.e., in an abrupt and often binary manner, from one discrete state to another. The conflicts between multiple discontinuous category dimensions can hinder category updating and prolong persistence. We further extend the literature by shedding light on the conflict between the moral and causal dimensions, emphasizing the often overlooked causal dimension in the category literature. We also illuminate power dynamics between different social groups engaging with the category; when the controlling majority remains silent about the category, the voices of the minority that champion category updating can be stifled, prolonging the persistence of imprinted category schemas. Even when accumulated evidence supports a new causal theory, the silent majority may not update their category understandings until their moral boundary is punctured and the category is morally reappraised.
Category Persistence and Updating During Emergence
The first step in category emergence is the formation of proto-categories, which are “new groupings . . . that are only weakly entrenched but have the potential to become widely institutionalized” (Zhao et al., 2018: 588). Proto-categories emerge as audiences cluster anomalies (Sætre and Van de Ven, 2021), either based on similarities with one another or with a salient exemplar, and create an initial category schema (Zhao et al., 2018; Younger and Fisher, 2020). During emergence, the schema of proto-categories may persist or become updated (Durand, Granqvist, and Tyllström, 2017). Categories can be updated when new information challenges the existing category schema. However, emerging categories can also be imprinted with their initial association with an existing category (Lashley and Pollock, 2020; Hsu and Grodal, 2021). For instance, Pontikes, Negro, and Rao (2010) showed that associations with the category “communist” had a long-lasting impact on the career trajectories of Hollywood artists who were uninvolved in the category. Similarly, Glaser, Fiss, and Kennedy (2016) illustrated that the emerging online advertisement exchange category was imprinted with an analogy to financial exchanges, although this proved to be an ill-fitting schema. These studies suggest that despite the arrival of novel information, imprinted category understandings might persist (Marquis and Tilcsik, 2013; Rhee et al., 2017).
To understand what drives category persistence and updating during category emergence, we need to unpack how categories are structured (Hannan, Pólos, and Carroll, 2007). Scholars have recently emphasized that categories consist of multiple dimensions (Durand and Paolella, 2013; Kennedy and Fiss, 2013). Categories are not based solely on feature similarity to a prototype (Rosa et al., 1999; Hsu, 2006) but also on congruence with other dimensions, such as causal theories or moral meanings (Durand and Paolella, 2013; Granqvist and Ritvala, 2016; Boghossian and David, 2021). In order for a category to make sense, the different dimensions must “hang together” in a state of coherence (Murphy and Medin, 1985: 291). For instance, the schema of the category “grass-fed beef” comprises a prototypical dimension (its appearance), a causal dimension (how it is produced), and a moral dimension (its moral value), all cohering without friction (Weber, Heinze, and DeSoucey, 2008). Coherent categories tend to be more viable and function more effectively (Lo et al., 2020; Zilber, 2024).
However, maintaining category coherence can be challenging, particularly for emerging categories in which new information is constantly introduced (Kennedy and Fiss, 2013). Such categories often encounter anomalous entities that align with certain dimensions but are dissonant with others in the category schema (Hannan, Pólos, and Carroll, 2007). These anomalies can disrupt the coherence among category dimensions, yielding instability and controversies (Boltanski and Thévenot, 1999; Jones et al., 2012). For instance, Arjaliès and Durand (2019) showed that the category “socially responsible fund” faced significant challenges when anomalies emerged, such as oil-investing funds, that did not fit the category along all dimensions. While such anomalies may align with the causal dimension of socially responsible funds (meeting certain non-financial criteria), they violated the moral dimension (lacking moral acceptability). Updating the category in this context required prioritizing “the relative weighting” of the moral dimension over other dimensions (Murphy and Medin, 1985: 292; Zuckerman, 2017). In other words, category updating rarely involves revising a single dimension of the category schema alone, as this would create imbalance and dissonance. Instead, category updating often entails revising the relative weighting of the dimensions and simultaneously updating multiple dimensions.
The difficulty of category updating can be particularly accentuated during the emergence of morally laden categories (Zelizer, 1985; Haveman and Rao, 1997; Arjaliès and Durand, 2019). Moral meanings “embody humans’ highest goals and aspirations and define what is deemed appropriate” and inappropriate (Arjaliès and Durand, 2019: 887), and they tend to be dichotomous (Douglas, 1966; Barthes, 1967; Lévi-Strauss, 1974; Weber, Heinze, and DeSoucey, 2008). Moral boundaries—socially constructed divisions that demarcate what is perceived as worthy from unworthy (Lamont and Molnár, 2002; Cattani, Ferriani, and Allison, 2014)—can pose significant obstacles to category updating as audiences struggle to reconceptualize and reconcile entities placed on opposite sides of a moral boundary (Lauderdale, 1976). For instance, Lamont (1992) demonstrated how the majority of White working-class men established a moral boundary against Black working-class men, perceiving them as possessing inferior moral values and work ethics. This boundary has had significant implications, such as the disproportionate incidents of police brutality against and incarceration of Black individuals. Revising entrenched moral meanings often entails puncturing this moral boundary, i.e., equalizing entities and people on opposite sides of the boundary. These boundaries are not easily confronted and punctured, except through highly publicized events such as the murder of George Floyd (Buchanan, Bui, and Patel, 2020).
This dichotomous nature of moral boundaries can pose a problem for category updating because updating some dimensions, such as the causal one, often clashes with moral-based categorization and requires overriding moral boundaries (DiMaggio, 1997; Negro et al., 2021; Naumovska and Zajac, 2022). For instance, the evidence-based understanding of mental health conditions required a shift in moral meanings associated with these conditions, but some people still struggle to equate seeking counseling with visiting a doctor, particularly in certain cultures that persistently stigmatize mental health issues (Nagar, 2022). Likewise, updating a causal theory often occurs discontinuously as theories tend to persist in the face of contradictory anomalies until an alternative theory emerges (Kuhn, 1962; Lakatos, 1970; Latour and Woolgar, 1986; Latour, 1987). Thus, when a discontinuous update in one dimension requires simultaneously revising other dimensions, the process of updating the entire category schema may come to a halt. For instance, adopting an updated causal theory of climate change requires revising the moral meanings associated with ingrained cultural practices such as beef consumption. The difficulty of this updating may explain the persistence of schemas such as climate change denialism (Norgaard, 2011; Schüssler, Rüling, and Wittneben, 2014).
Further complicating category persistence and updating is that these dynamics unfold across heterogenous social groups that are often unequally embedded in existing power relations (Lamont and Molnár, 2002; Grodal and Kahl, 2017; Quinn and Munir, 2017). While prior research has focused primarily on overt contestation among these groups (Jones et al., 2012; Cattani, Ferriani, and Allison, 2014; Grodal, 2018), some studies in organization theory have highlighted the role of silence and inaction in engendering persistence (Tripsas, 2009; Stainback, Tomaskovic-Devey, and Skaggs, 2010; Anteby, 2016). As explicated by Foucault (1978: 27), “we must try to determine the different ways of not saying such things, how those who can and those who cannot speak of them are distributed, which type of discourse is authorized . . . [as such silence is] an integral part of the strategies that underlie and permeate discourses.” While silence does not leave a paper trail and thus is challenging to examine, scholarship has recognized silencing as an effective discursive strategy, particularly with morally controversial issues (Briscoe and Murphy, 2012; Carlos and Lewis, 2018). When the majority resists updating a category, silencing minority voices can be a discursive strategy to protect existing power relations and patterns of resource allocation (Mora, 2014; Clemente and Roulet, 2015; Anteby, 2016). However, the specific mechanisms through which power dynamics influence category persistence and updating have not been fully explored. In this study, we explore what drives category persistence and updating during category emergence, and in doing so, we elucidate the often invisible underbelly of category persistence propelled by silence.
Methods
To shed light on the mechanisms that shape category persistence and updating, we sought to identify a context in which the process of categorization was both complex and multifaceted (Garfinkel, 1967; Eisenhardt, 1989; Yin, 1989). The medical category AIDS during the early years of the epidemic in the U.S. from 1978 to 1985 fulfilled both these criteria. Currently, medical authorities, such as the Centers for Disease Control (CDC), define AIDS as “the most severe phase of HIV (Human Immunodeficiency Virus) infection” (CDC, 2023). HIV attacks the immune system, specifically CD4 cells, or T-cells, making the body vulnerable to various types of viral, bacterial, and fungal infections over time. While advances in medical treatment now allow many HIV-infected individuals to remain asymptomatic without progressing to AIDS, this was not the case before the mid-1990s. Prior to the availability of effective therapies, people infected with HIV invariably progressed to the final stage, AIDS, and eventually died. Medical professionals initially observed and categorized the end-stage symptoms without knowing they were caused by a new virus.
Contemporary research indicates that the AIDS epidemic originated in isolated rural areas of central Africa and later spread to urban populations in the mid-twentieth century due to rapid urbanization in the region. As central Africa became more integrated into the global economy, the virus slowly infiltrated other parts of the world during the 1960s and 1970s. In the late 1970s, U.S. medical professionals began encountering patients with diverse and inexplicable symptoms such as skin cancer, pneumonia, weight loss, and dementia. These symptoms affected various demographic groups, including homosexual men, Haitian immigrants, infants, and hemophiliacs. The complexity made it extremely difficult for medical professionals to initially identify a pattern and to gradually update the proto-category. Additionally, the epidemic’s causal complexity was further complicated by the deep, divisive moral meanings infused into the category. Thus, the extreme complexity and multiple categorical dimensions of the case provide an ideal setting for building theories of category persistence and updating (Eisenhardt, 1989).
Data Collection
We conducted an in-depth theory-building study (Langley, 1999) using five corpora of archival data: oral histories, medical articles, media data, congressional reports, and secondary sources that attest the history of the early AIDS epidemic. Analyzing multiple data sources allowed us to triangulate among data to minimize potential retrospective biases in oral histories and to validate our findings. Table 1 provides an overview of the data.
Overview of Archival Data*
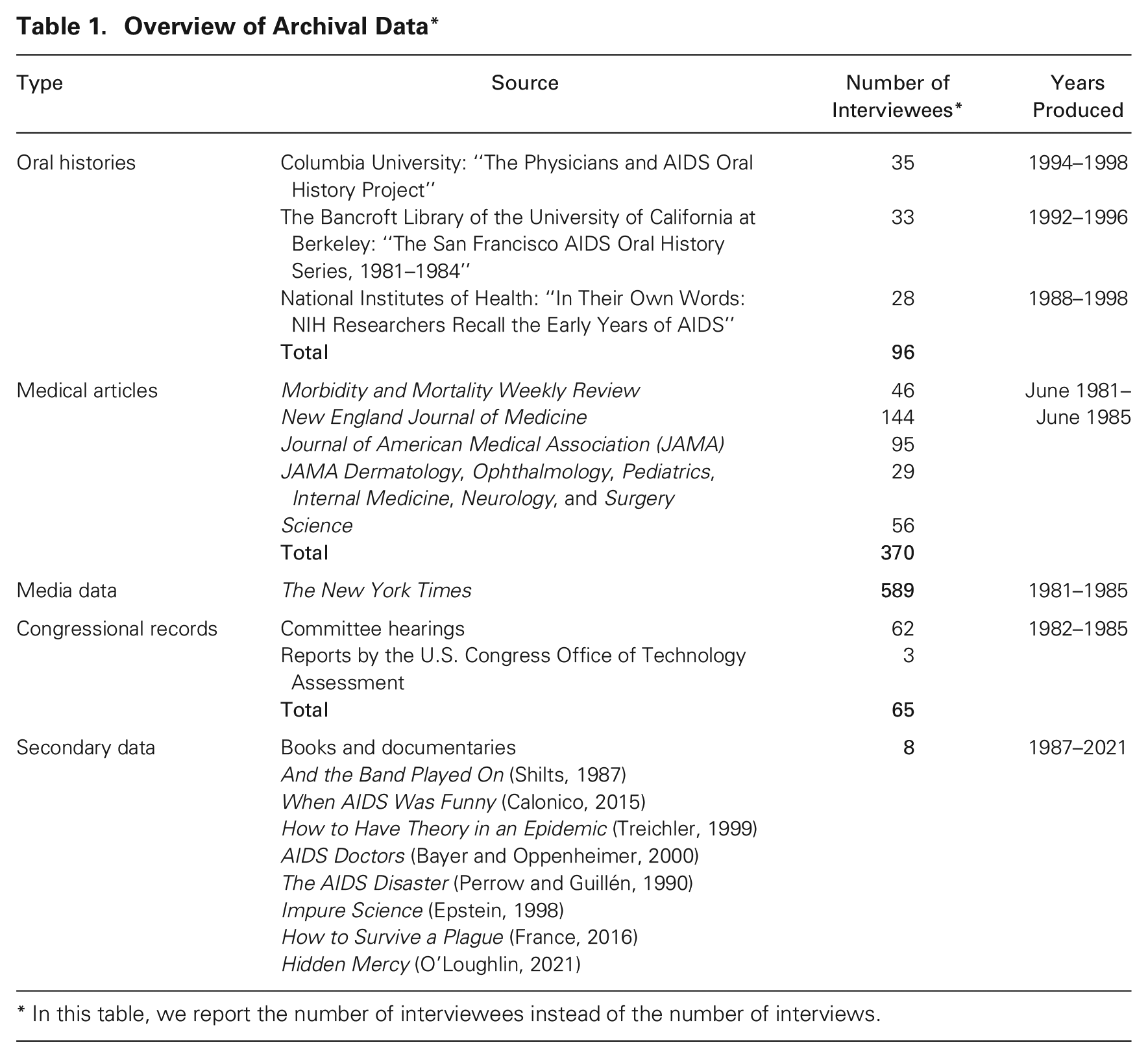
In this table, we report the number of interviewees instead of the number of interviews.
Oral histories
Our primary data source was 103 oral histories provided by 96 medical professionals who participated in the early AIDS epidemic. We used oral histories collected by historians and sociologists at three institutions: Columbia University, the University of California San Francisco, and the National Institutes of Health (NIH) Historical Office. These oral histories provide rich accounts of how medical professionals thought about, understood, and categorized the disease—cognitive processes that are often invisible from official records, statistics, and publications. Table 1 includes an overview of these oral history collections.
Medical articles
To mitigate potential retrospective biases in the oral histories and gain further insight into the process of categorizing the disease, we collected and analyzed academic articles published between 1981 and 1985 in four major medical and scientific journals: Morbidity and Mortality Weekly Review, The New England Journal of Medicine, The Journal of the American Medical Association, and Science. 1 Due to the difficulty of identifying AIDS-related articles published before the label AIDS was created in 1982, we manually examined the titles and abstracts of all articles published in the four journals between 1981 and 1983. We identified 370 AIDS-related articles published across these journals.
Media data
To gain insight into how broader audiences discussed knowledge and theories produced by medical professionals, we collected an additional 589 articles written about AIDS published in The New York Times between 1981 and 1985. Using knowledge gained from the oral histories and medical articles, we searched using the keywords “Kaposi,”“Pneumocystis,”“immunodeficien*,”“immuno-deficien*,”“immune deficien*,”“gay cancer/pneumonia/disease/syndrome,” and “homosexual” to identify articles written about the epidemic before the term AIDS became official.
Congressional hearings
To understand the federal response to the epidemic, we collected congressional records, using the same keywords as those used for the media data. In total, we collected 62 congressional hearings. We also collected reports that included funding information produced by the Office of Technical Assessment, a now-defunct congressional arm that was responsible for providing unbiased analyses of complex scientific and technical issues.
Secondary sources
To deepen our understanding of the context, we extensively read secondary sources and watched documentaries and video recordings. We used intertextual references (Kahl and Grodal, 2016) to compile our list of these sources. We mitigated potential biases in non-academic accounts by triangulating them with our primary data sources of medical articles, media data, and congressional reports. Table 1 lists our main secondary sources.
Data Analysis
We analyzed the data by drawing on abductive methods to develop a process theory (Langley, 1999; Grodal, Anteby, and Holm, 2020). Figure 1 provides an overview of our data analysis process.
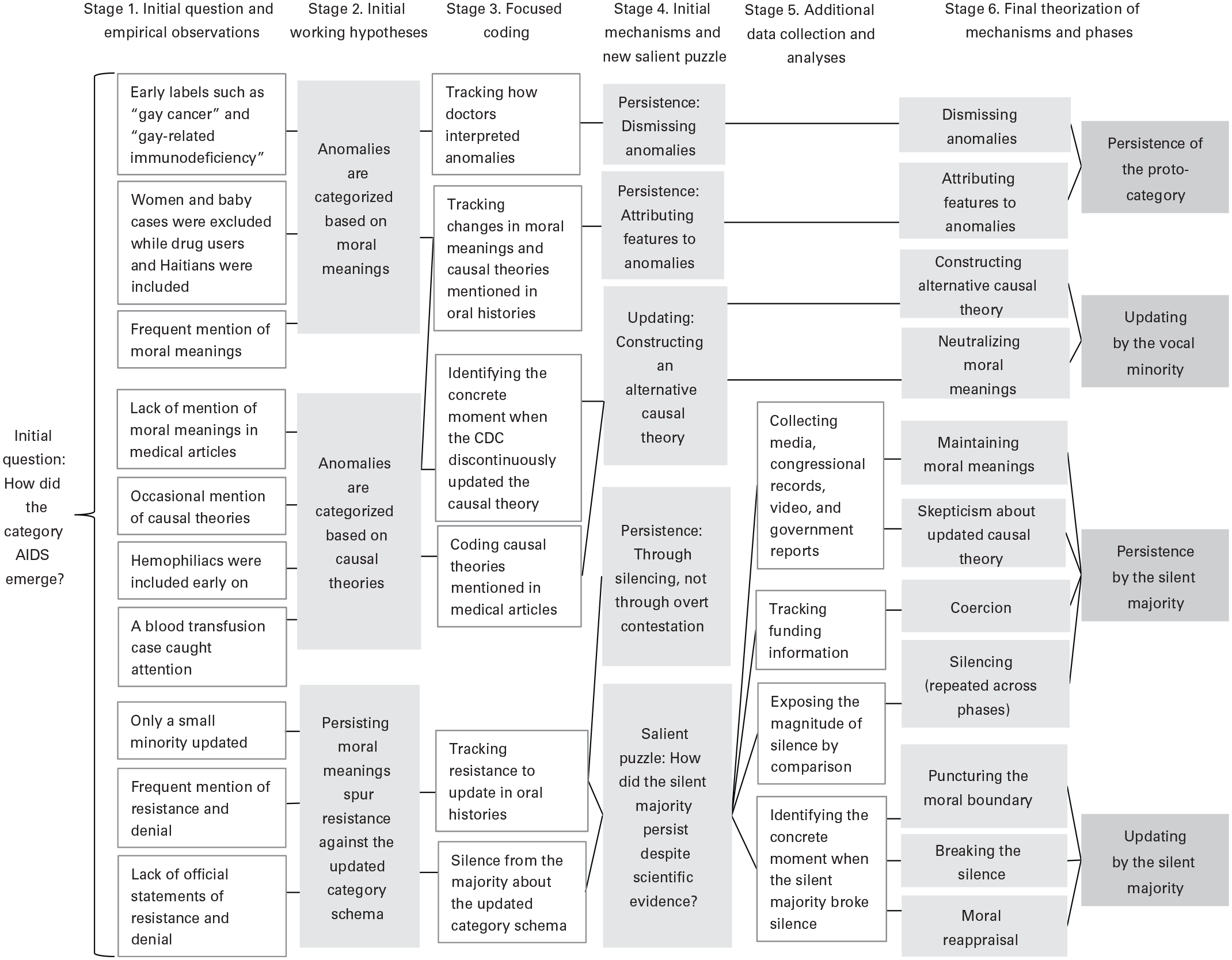
Process of Data Analysis
Stage 1: Initial question and empirical observations
We began our data analysis with the initial grand tour question (Spradley, 1979) of how medical professionals in the United States constructed the category AIDS during the initial stages of the epidemic. First, we created a chronological timeline of key events and began coding our oral histories with particular emphasis on the demographics of patients encountered by doctors (e.g., “gay man,”“drug user,”“woman,”“hemophiliac,” etc.) and on whether doctors included or excluded these patients from the emerging category. Since the early epidemic lacked an official label, we also tracked the evolving labels used over time, drawing from both our oral histories and archival data (e.g. “gay cancer,”“gay-related immunodeficiency”). We were quickly intrigued by the initial categorization of the emerging epidemic as a “gay disease” and how medical professionals categorized patients whom they viewed as anomalies—that is, those who did not fit their initial understandings of the emerging category.
Stage 2: Initial working hypotheses
In light of these initial observations, we generated a set of working hypotheses about the categorization dynamics (see Figure 1). For instance, the frequent omission of female and pediatric patients by medical professionals, coupled with the frequent mentions of moral meanings infused into the category in our oral histories data (e.g., “The public was not very supportive of this disease or this segment of the population. . . . People were saying that this was God’s way of saying gays should not be doing this,” Dr. Quinn, oral history), led us to posit the working hypothesis that “anomalies are categorized based on moral meanings.” In contrast, our observation that a small number of medical professionals included hemophiliacs in the category early on, coupled with references to causal theories in our medical archival data, spurred us to generate the working hypothesis that “anomalies are categorized based on causal theories.” Considering numerous accounts of resistance to updating in the oral histories, we also posited that “persisting moral meanings spur resistance against the updated category schema.” At this point, we revisited the literature on categorization and realized that examining categorization processes based on moral meanings and causal theories held significant potential to extend the existing literature (Durand and Paolella, 2013).
Stage 3: Focused coding
The initial working hypotheses guided our focused coding process to track core constructs. We tracked changes in the category’s moral meanings and causal theories, with particular attention to how medical professionals persisted in or updated their prior understandings in the face of anomalies. For instance, we pondered why drug users barely challenged either the moral meanings or the causal theories of the emerging category (e.g., “People were saying [about drug users] ‘maybe these are really gay men that are selling themselves to get drugs,’” Dr. Curran, oral history), while babies with similar symptoms disrupted both the moral meanings and causal theories (e.g., “no one wanted to believe that . . . this sort of filthy disease could occur in children,” Dr. Oleske, oral history). Specifically, through triangulation between oral histories and medical articles, we pinpointed the concrete moment when the CDC discontinuously updated their causal theory (see Phase 3 in our Findings section). During this stage, we came to realize that different social groups engaged in category persistence and updating at different points in time.
Stage 4: Initial mechanisms and a new salient puzzle
The focused coding led us to develop several initial mechanisms of category persistence and updating (see Figure 1). For example, we developed the code “dismissing” (e.g., “I remember there was a woman who clearly had AIDS. There were no women reported. [Her case] sat on the shelf for about two years,” Dr. Grossman, oral history) as an important mechanism that spurred persistence. We also coded for “constructing an alternative causal theory” (e.g., “In this week’s MMWR [Morbidity and Mortality Weekly Review], there will be an article describing three AIDS patients with hemophilia, and we think this makes it look very much like it is a virus that is transmitted in the blood,” Dr. Curran, oral history), which linked this code to category updating. Among others, the code “silencing” (e.g., “The stories just weren’t coming out on the gay syndrome. . . . Editors were killing pieces. They didn’t want stories about gays,”Shilts, 1987: 99) emerged as an important mechanism of persistence. At this point, we iterated back to the categorization literature and realized that it has often characterized category contestation as overt and explicit discursive conflicts (Jones et al., 2012; Grodal, 2018), which made the silence occurring in our setting theoretically more salient.
We then began coding to identify when and by whom the category was updated or persisted. We observed that a small, core group of medical professionals revised the causal theory of the category relatively early in the process and began advocating for others to update the category as well. We labeled this core group the vocal minority. In contrast, a larger number of peripheral actors displayed resistance to updating the category, forming what we termed the silent majority (Cattani, Ferriani, and Allison, 2014; Hsu and Grodal, 2021). This perspective brought forth a new salient puzzle: despite the abundant evidence supporting the updated causal theory of AIDS, why and how did the silent majority persist in their initial understanding of the category?
Stage 5: Additional data collection and analyses
Our archival data at this stage were skewed toward the categorization process within the vocal minority who had left extensive paper trails. In contrast, exposing persistence and silence within the silent majority was empirically challenging because these actions tend to not leave a paper trail. To address this methodological issue (Grodal, Anteby, and Holm, 2021), we collected extensive additional data, such as media articles, congressional reports, and various secondary sources, including journalistic investigations and video recordings. We also identified government reports to track federal funding allocated to AIDS during our study period (U.S. Congress, 1985; see Table 1 for an overview of the data).
We devised three analytic strategies to shine light on silencing and persistence: (1) comparative analysis: we highlighted the degree of silence by contrasting media coverage of the AIDS epidemic with that of another epidemic, Legionnaires’ disease, whose scale and fatality rate were comparable to those of AIDS in the latter’s early days; (2) temporal analysis: we tracked temporal trends in media attention, using New York Times articles to see how the extent of silence surrounding AIDS changed over time (see Phase 5 of the Findings section for details); (3) observations of micro-interactions: we analyzed video recordings of federal and state government officials to examine the prevalence of silence in contexts where the topic of AIDS should have been relevant. Using these rich data, we conducted coding for the micro-interactions that occurred after questions about AIDS were raised, focusing on whether these questions were adequately addressed or disregarded.
Stage 6: Final theorization of mechanisms and phases
By incorporating the initial mechanisms that we identified in Stage 4 and new insights gained from the additional data collection and analyses in Stage 5, we finalized the temporal map of events and formulated the final mechanisms that drive category persistence and updating. Figure 2 shows the temporal map of events. We then sequenced the mechanisms into a theoretical model that illuminates the process of proto-category formation, category persistence, and category updating. Table 1A in the Online Appendix provides an overview of the mechanisms identified along the temporal phases.
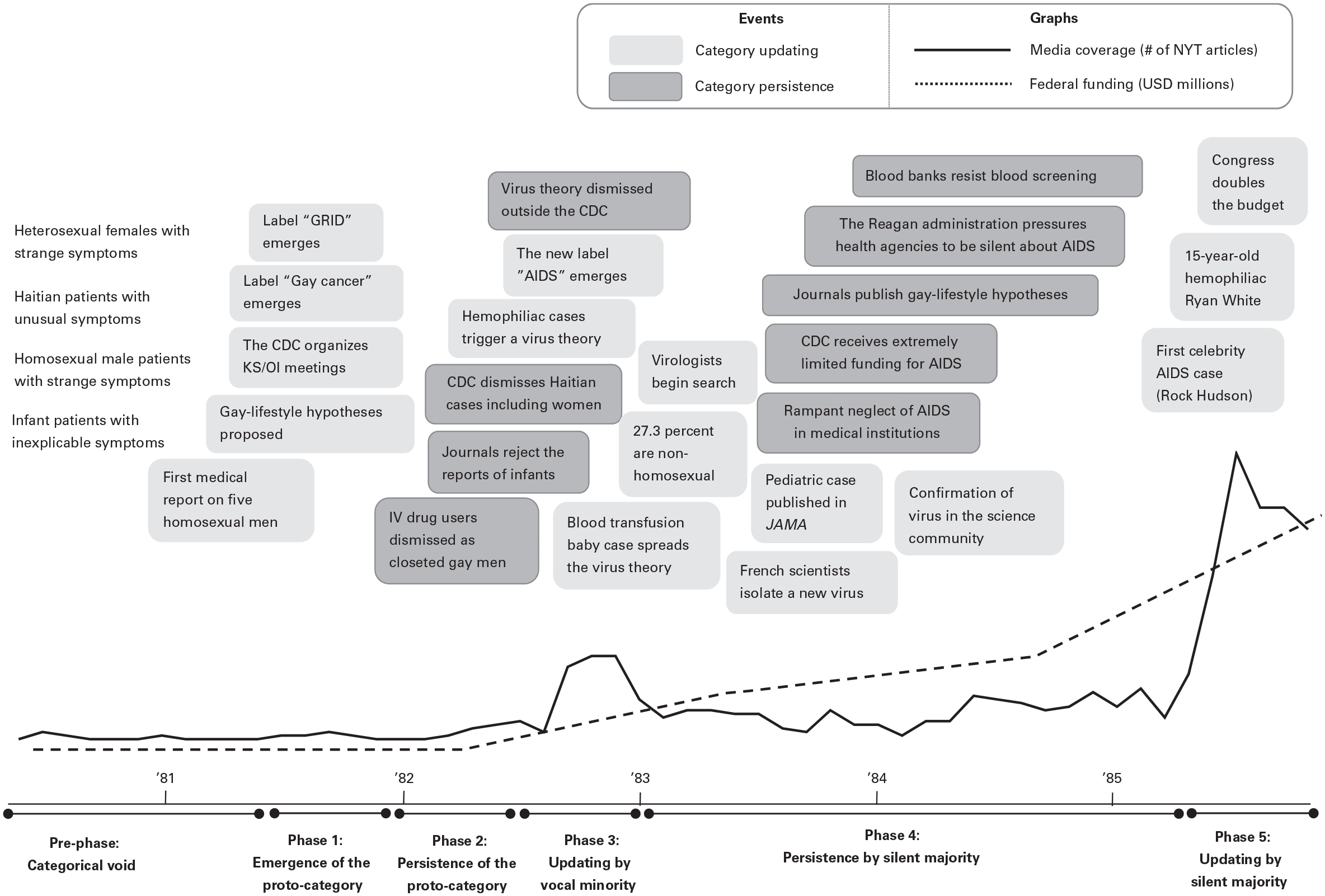
Temporal Map of Events
Drawing from the insights gained through these analyses, we structured each phase of our Findings section as follows: we begin by describing anomalies that challenged the existing category schema, outline the mechanisms driving persistence and updating within different social groups, and then present the consequences of persistence and updating for resource allocation.
Findings
Our study of the early AIDS epidemic in the U.S. aimed to identify the mechanisms driving category persistence and updating during category emergence. Table 2 provides an abstract overview of the conditions driving category persistence and updating, derived from our findings. We show that a category, particularly one laden with strong moral meanings, is updated only when both of these conditions are met: a new causal theory offers an alternative explanation for the category’s functioning, and the puncturing of a moral boundary redefines the category’s moral meanings. We elucidate how the absence of either a new causal theory or puncturing of a moral boundary results in category persistence. In particular, we focus on category persistence within the silent majority despite accumulated evidence. In our case, only when the moral boundary was punctured did the silent majority also begin to accept the new causal theory and update their category understanding. Below, we elaborate on the mechanisms through which categories persist or are updated in light of new information and their consequences for resource allocation.
Overview of the Conditions Driving Category Persistence and Updating

Pre-Phase: Categorical Void—1978 to May 1981
Shelving anomalies
From around 1978 to early 1981, medical professionals began to encounter heterogeneous groups of patients suffering from anomalous symptoms that did not fit existing medical categories. For example, Dr. Rubinstein recalled, “I fell upon the first patient with AIDS in 1978 . . . The baby had a lot of bacterial infections, huge lymph nodes, and a very high serum gamma globulin level, which was very unusual for a six-week-old baby.” Likewise, Dr. Calabrese recalled his amazement when he first saw a patient with inexplicable symptoms: “I still remember the first case of a young man who came to Cleveland and was literally covered with Kaposi’s [purple skin lesions]. . . . He had no less than 11 opportunistic infections. The whole picture of this, just strange, unusual, kind of other-worldly; I was struck by the gravity of the whole thing.”
Initially, medical professionals did not recognize any patterns among the individual cases. The symptoms included skin cancer, pneumonia, wasting, dementia, and swollen lymph nodes, while the patient demographics spanned infants, women from impoverished communities, young men in big cities, and undocumented immigrants. For example, Dr. Quinn saw a female patient with Pneumocystis pneumonia at the National Institutes of Health in January 1981. Although he and his colleagues were intrigued by the patient, Dr. Quinn stated that they “did not pursue the case further,” saying, “who knows what she [the patient] had.” Such cases were “lost to follow-up, nothing was left [to pursue].” These cases were regarded as isolated and inexplicable, from which a pattern could not be drawn. Medical professionals thus shelved these anomalies in the back of their minds without realizing the need to create a new category.
Phase 1: Emergence of a Proto-Category—May to December, 1981
Generating the category schema by grouping salient anomalies
The initial categorization process was triggered when, around May 1981, a small group of medical professionals began to spot a pattern among a few anomalies that existing medical categories did not explain. In early 1981, dermatologists in San Francisco and New York City realized that they were observing the occurrence of Kaposi’s sarcoma, an extremely rare skin cancer that causes purplish lesions, in multiple homosexual men. Dr. Conant recalled, The [Kaposi’s sarcoma] patients were, from the moment they were diagnosed, very visible. . . . The first of April of 1981, I learned through Jim Groundwater, who was a dermatologist here in town [San Francisco], that Alvin Friedman-Kien was seeing cases in New York. . . . So I called him, and he told me that, yes, they were seeing Kaposi’s sarcoma, and that it was very interesting.
Simultaneously, a group of physicians in Los Angeles spotted the occurrence of Pneumocystis pneumonia in five homosexual men and submitted a case report to the CDC. This bacterial infection was extremely rare, and it killed young, previously healthy patients at a rapid pace. In June 1981, the CDC released a case report in its main periodical, Morbidity and Mortality Weekly Review, which became the first report of the epidemic (Gottlieb et al., 1981).
As Kaposi’s sarcoma and Pneumocystis pneumonia co-occurred in multiple patients, the CDC quickly organized a small task force on this new potential epidemic. This trigger event spurred medical professionals to group the salient anomalies and create a proto-category.
Generating the category schema through infusing moral meanings
Quickly, a schema pertaining to the proto-category arose, emphasizing one salient feature: the patients’ homosexuality. The earliest labels for the proto-category contained the term “gay,” such as gay cancer, gay pneumonia, gay syndrome, and later, gay-related immunodeficiency (GRID). For instance, Dr. Ammann admitted, “I’m embarrassed by it now, but if you go through my research notes and reprints, the early ones have ‘gay syndrome’ written across them.” Dr. Conant recounted, The disease wasn’t called AIDS in the beginning. It was called the gay cancer, and then a few months later became known as GRID, gay-related immune deficiency syndrome. . . . gay cancer, it was a uniformly fatal disease, and it was the wrath of God being visited on these men, . . . being punished for this behavior.
In 1981, homosexuality was still a divisive and provocative topic that evoked strong moralizing emotions such as disgust among the general public (Herek, 2004). Homosexuality had been removed from the American Psychiatric Association’s official list of mental disorders only in 1973, and 29 states in the United States still had so-called sodomy laws outlawing sexual acts between persons of the same sex. In general, homosexuality was largely considered a morally deviant form of sexuality (Eskridge, 2008; Tilcsik, Anteby, and Knight, 2015) and remained an undiscussable topic (Adut, 2005; Tebble, 2011). The proto-category AIDS was, thus, infused with stigmatized moral meanings that placed it outside the moral boundary of what was deemed worthy and discussable (Douglas, 1966).
Generating the category schema through constructing a causal theory
Only a very small group of doctors and public health officials paid attention to the emerging proto-category and tried to identify a cause for the disease. Most early hypotheses revolved around the salient feature of homosexuality. For example, Dr. Dritz and her team thought, Maybe some chemicals in the gay community are suppressing the immune system. So we began to look at the environment. All the gays—generalizing, of course—had plants in their house. What do you use on your plants? Plant food, plant chemicals, bug sprays . . . What do you use to get a high? We sent two of my men into the Jaguar Bookstore and the Ambush, and they bought “poppers” under the counter.
In the earliest phase, as Dr. Levine said, “most investigators believed that the cause was something restricted to the gay population and it probably was a drug or a toxicant,” not a viral or infectious agent. An editorial published in The New England Journal of Medicine stated, These salient features have emerged: The patients are typically young homosexual men, most of whom live in large cities and many of whom use drugs . . . Why this group? . . . So-called “recreational” drugs are one possibility. (Durack, 1981)
In other words, medical professionals constructed causal theories referencing gay men’s lifestyle to explain the rise of the proto-category.
Persistence of the category schema through silencing
By August 1981, less than three months after the first report, a total of 107 cases and about 50 deaths from the mysterious disease had already been reported (Associated Press, 1981). However, this new epidemic received extremely limited media attention, compared to other past epidemics of similar size and fatality rate. For example, when Legionnaires’ disease befell 182 American veterans and killed 29 of them in 1976, it immediately garnered nationwide attention, with The New York Times running five front-page articles within a week from the onset. In contrast, the same newspaper ran only three short back-page articles about the “homosexual epidemic” throughout 1981, “setting the tone for non-coverage nationally” (Shilts, 1987: 99). Table 3 shows the stark difference in media attention between Legionnaire’s disease and AIDS over a similar time span. The media’s silence meant that most medical professionals and broader audiences were either unaware of the epidemic or viewed it, as Dr. Ziegler noted, “not worth going after.” Only a very small minority of medical professionals paid attention to the proto-category.
Comparison of The New York Times Coverage of Legionnaire’s Disease and AIDS Within the First Four Months of Outbreak
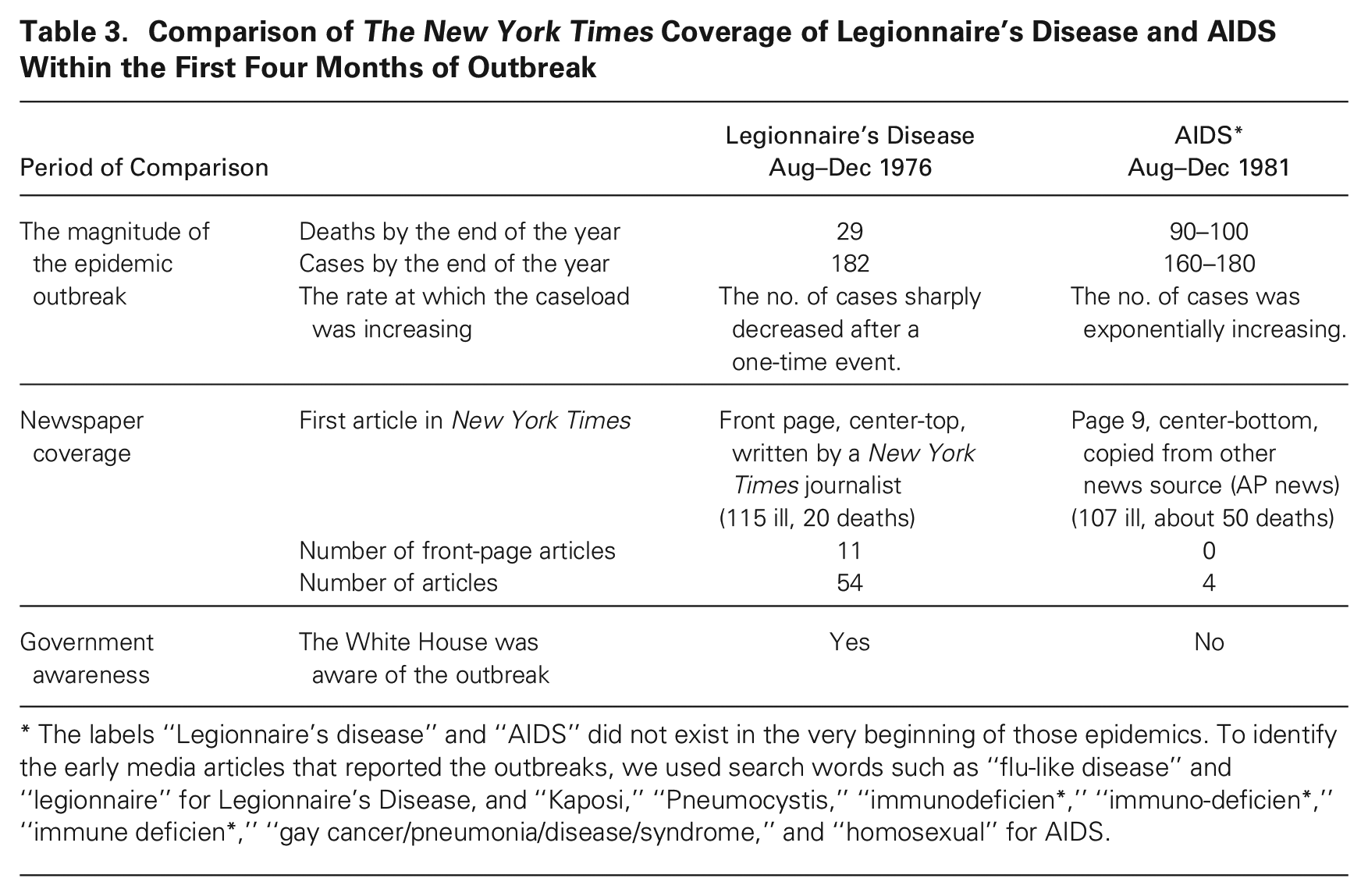
The labels “Legionnaire’s disease” and “AIDS” did not exist in the very beginning of those epidemics. To identify the early media articles that reported the outbreaks, we used search words such as “flu-like disease” and “legionnaire” for Legionnaire’s Disease, and “Kaposi,”“Pneumocystis,”“immunodeficien*,”“immuno-deficien*,”“immune deficien*,”“gay cancer/pneumonia/disease/syndrome,” and “homosexual” for AIDS.
The state of the category schema
The initial state of the category schema involved prototypical features (abhorrent and fatal symptoms such as Kaposi’s sarcoma and Pneumocystis pneumonia), stigmatized moral meanings (a disease among homosexual men), and causal theory (a disease caused by gay lifestyle), creating coherence surrounding the category. Silencing emerged as a dominant reaction toward the proto-category from the majority of audiences, including most medical professionals.
Consequences for resource allocation
This powerful moral marginalization resulted in a dearth of resources allocated to dealing with the proto-category. A congressional report shows that no federal funding was allocated to the epidemic during this period (U.S. Congress, 1985). Figure 3 shows the trends in federal funding for AIDS and in media coverage during our period of study from 1981 through 1985.
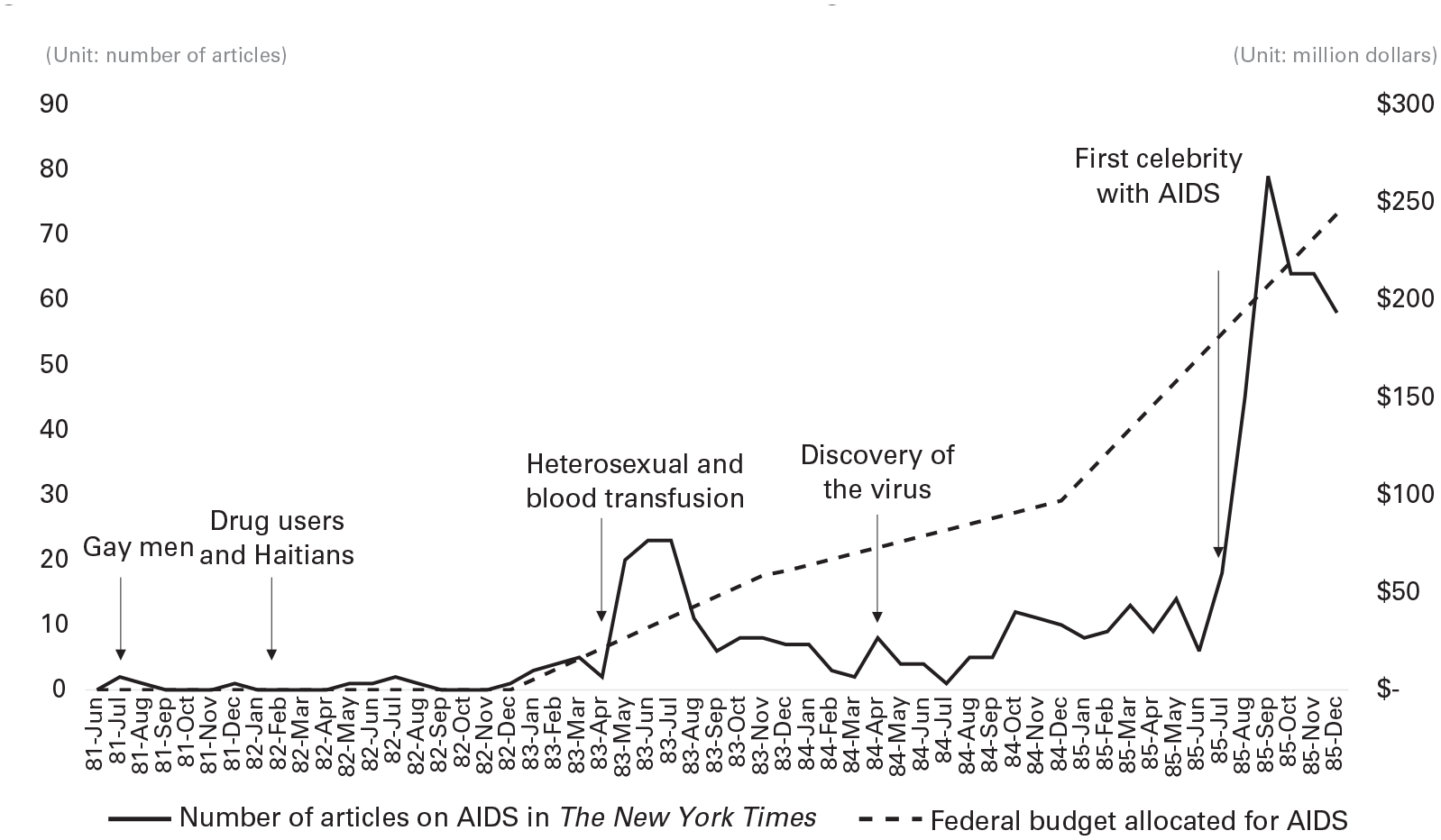
Trends in Media Attention and Federal Budget for AIDS
The CDC was the only federal agency that paid attention, along with a few individual doctors who were in direct contact with patients. Back then, however, the CDC was a low-status, resource-deprived institution geographically isolated in Atlanta. According to Dr. Dritz, CDC’s job was . . . if there’s a case of malaria in Louisiana, you go out there and clean it up. That’s why they’re down in Atlanta in the first place, because that was the place where malaria and the other deep South diseases were focused. CDC wanted to move to the Washington area, but they weren’t permitted to.
To examine the emerging epidemic, the CDC had only a few young doctors and a very small amount of resources from their internal budget.
Phase 2: Persistence of the Proto-Category—December 1981 to July 1982
Anomalies challenging the category schema
In December 1981, medical professionals began to spot a new set of anomalies, such as intravenous drug users, Haitian immigrants, heterosexual women, and infants, that were difficult to explain by the existing category schema. While these anomalies aligned with the schema of the proto-category along the prototypical dimension (symptoms), they misaligned with the category schema along the dimensions of moral meanings and causal theories. During this phase, most medical professionals maintained the category schema’s existing moral and causal dimensions, without updating, through three mechanisms: attributing features, dismissing anomalies, and silencing.
Persistence of the category schema through attributing features to anomalies
When encountering anomalies, medical professionals often tried to fit them into the existing causal theory of GRID. For example, when physicians reported GRID-like symptoms in male heterosexual drug users (Masur et al., 1981), many assumed that these drug users were either gay or had engaged in gay sex. Dr. Curran, who was the head of the CDC task force, explained: [Masur et al. (1981)] reported drug users . . . People were saying, “Maybe these are really gay men that are selling themselves to get drugs.” . . . It was hard to demonstrate that it was occurring in other groups [besides gay men] initially.
The inclusion of male heterosexual drug users in the category did not require major revisions to both the moral meanings and causal theory of the category. Drug users were an equally if not more marginalized group, making it easier to attribute characteristics to them. The category schema persisted by most medical professionals attributing features to the anomalies to fit the existing dimensions.
Persistence of the category schema through dismissing anomalies
When it was difficult to attribute features to anomalies to fit the category schema, such as when medical professionals encountered GRID-like symptoms in women and children, these professionals simply dismissed the anomalies altogether. For example, Dr. Piot recounted, Yes, we were seeing women. . . . But we hadn’t completely internalized the thinking that this was the same thing we were seeing [in gay men] because there seemed to be such a dogma that this was a gay disease . . . they called it GRID.
Dr. Rubinstein, a pediatrician, recalled, “No one else began even to think about pediatric AIDS. 2 In 1981, we caused a lot of turmoil whenever we even hinted that such a syndrome may exist. In a meeting [of the American Academy of Pediatrics] . . . when I raised my hand and spoke about children, everyone pooh-poohed it.” Overall, dismissing anomalies was a powerful mechanism through which the initial category schema persisted.
Persistence of the category schema through silencing
A strong moral boundary continued to separate AIDS patients from the general public. In early 1982, there were over 120 reported deaths, including heterosexual drug users, women, and children. Nevertheless, the media was still silent, and editors rejected articles written about the subject (Nelkin, 1991). Slowly, the small minority of medical professionals and concerned individuals began to think that the stigmatized moral meanings were behind the public’s puzzling silence. Representative Waxman, from California, held the first hearing on the disease in Los Angeles, in which he said, I want to be especially blunt about the political aspects of Kaposi’s Sarcoma. This horrible disease afflicts members of one of the nation’s most stigmatized and discriminated-against minorities. . . . There is no doubt in my mind if the same disease had appeared among Americans of Norwegian descent or among tennis players rather than among gay males, the responses of the government and the medical community would have been different. (“Kaposi’s Sarcoma and Related Opportunistic Infections,” 1982)
Despite these early voices, the majority of the public and medical professionals remained unaware of and silent about the epidemic.
The state of the category schema
At this stage, anomalies appeared that aligned with the prototypical features but were dissonant with the proto-category’s moral meanings and causal theory. Despite this contradiction, attributing, dismissing, and silencing were used to maintain the initial coherent category schema among both medical professionals and the general public.
Consequences for resource allocation
A congressional report shows that no federal funding was allocated to the epidemic during this period (U.S. Congress, 1985).
Phase 3: Category Updating by the Vocal Minority—July 1982 to January 1983
A turning point in the emergence of the category AIDS occurred during the latter part of 1982. Triggered by anomalies, a small minority of medical professionals updated the category schema by constructing a new causal theory. In addition, by neutralizing the moral meanings, they were able to develop a new coherent category schema. However, the majority persisted in their initial understanding of the category by resorting to silencing.
Anomalies challenging the category schema
In mid-1982, CDC investigators received a report about two heterosexual hemophiliac patients who showed GRID-like symptoms. Hemophilia is a hereditary disorder in which blood does not clot, meaning that the patients rely on blood products to survive.
Vocal minority: Updating of the category schema through constructing a new causal theory
The general public may not readily associate hemophiliacs and gay men, but the infectious disease specialists at the CDC knew there was a common link between the two: hepatitis B. Within this core group of doctors, the news of the two hemophiliacs almost immediately evoked an alternative causal theory for the proto-category: that the disease, akin to hepatitis B, might be caused by a virus that spreads through sex and blood. Dr. Curran recounted, Dr. Bruce Evatt, the head of CDC’s hematology group, announced at a task force meeting, “There is an old man with hemophilia from Florida who had Pneumocystis and who died.” I said, “What?” We were all thinking blood—it was going to be in the blood supply if it were caused by a virus like hepatitis B. . . . But not everybody wanted to believe this.
The virus hypothesis immediately emerged as the most promising causal theory among the small group of CDC doctors, catalyzing a sudden seismic shift in their understanding of the category. In particular, they recognized that this had implications for dismantling the moral boundary between the category and the mainstream population: anyone could contract the disease, similar to hepatitis B. This meant that the disease could potentially evolve into a widespread public health crisis affecting broader populations.
The small number of doctors who updated the category’s causal theory began feeling a greater urgency to raise their voices about the epidemic. Slowly, a vocal minority began to form, which, beyond the CDC, included a few primary care doctors, patient groups, and public figures. This vocal minority also began to criticize the widely circulated label GRID, which eventually faded out. Around September 1982, the CDC adopted the more neutral label AIDS, which then became the category’s official label. The creation of the label AIDS was an important step in solidifying the updated category schema among the vocal minority. The proto-category GRID fell out of use, giving way to the more institutionalized category AIDS.
Vocal minority: Updating of the category schema through neutralizing moral meanings
The updating of the category’s causal theory was facilitated by the vocal minority’s ability to neutralize the stigmatized moral meanings associated with AIDS. For instance, many members of the CDC task force on AIDS had prior experience dealing with infectious and sexually transmitted diseases among marginalized communities, which fostered non-judgmental attitudes among these members. For those without such prior experiences, they neutralized the preconceived moral meanings through direct engagement with patients. For example, Dr. Sherer described his experience: In the very beginning the most important thing you could do was to just be there, and not be freaking out that a person has or is suspected of having HIV, or that they’re gay, or that they’re transsexual, and that they work at nights in a club, and so they’re on estrogens, and all this other stuff. I mean just to be in a non-judgmental setting.
In other words, when an alternative theory emerged, the doctors who had already been neutralizing the moral meanings of the epidemic were able to swiftly update the causal theory.
Silent majority: Persistence of the category schema through silencing
This drastic shift in the category schema among the vocal minority had little impact on the moral meanings associated with the category in the minds of the silent majority. The media’s silence continued, and much of the general public remained unaware of AIDS despite the fact that it had killed about 200 people and infected many more. The silence around the growing AIDS epidemic was also prominent among government officials and policymakers. For example, in October 1982, a journalist asked the first question about AIDS in a White House press briefing (Calonico, 2015). Deputy Press Secretary Larry Speakes answered the question in the following dialogue:
Larry, does the President have any reaction to the announcement by the Center for Disease Control in Atlanta that A-I-D-S is now an epidemic in over 600 cases?
A-I-D-S? No, I haven’t heard of that.
Over a third of them have died . . . It’s known as a “gay plague.”
[Laughter]
[Raising his voice] No, it is, it’s a pretty serious thing. One in every three people that get this has died. I wonder if the President was aware of this?
I don’t have it . . . do you?
[Laughter]
The White House looks on this as a great joke? . . . Does the President, does anybody in the White House know about this epidemic, Larry?
I don’t think so, I don’t think there’s been any . . .
This exchange exemplifies how the category schema persisted through silencing. The strong moral meanings spurred most people within the silent majority to dismiss the epidemic.
As of late 1982, the caseload of AIDS patients was exponentially increasing, encompassing patients from diverse demographic groups. The updated virus-centered causal theory implied that the nation’s blood supply was at risk. In July 1982, the CDC organized a meeting with blood bankers, the FDA, the NIH, and gay communities to raise concerns about blood safety. However, this attempt was met with deep skepticism and silence from most of the invited stakeholders. Dr. Francis recalled that the blood banking industry and other government officials thought that “the CDC [was] fabricating a disease for a budget increase.” The meeting fizzled out, without success.
The state of the category schema
Two divergent yet internally coherent versions of the category schema emerged in a vocal minority and a silent majority. The vocal minority updated the schema by putting more weight on the updated virus-centered causal theory while neutralizing moral meanings and accepting diverse patients and symptoms, whereas the silent majority maintained the initial stigmatized moral meanings and the profound moral boundary between AIDS patients and mainstream society. The vocal minority’s voices were still extremely feeble.
Consequences for resource allocation
Federal funding requested or allocated to the epidemic in this period remained nonexistent (U.S. Congress, 1985). In the entire fiscal year 1982, the CDC had no budget specifically earmarked for AIDS, having to reallocate funds from its other activities to investigate the disease. This caused a serious constraint in its ability to fight the epidemic. For example, in 1983 Dr. Francis, at the CDC, wrote, The inadequate funding to date has seriously restricted our work and has presumably deepened the invasion of this disease into the American population. . . . We are again understaffed and underfunded. . . . In this vast and wealthy country, there must be a way to get $10–20 million immediately for this disease.” (Quoted in Shilts, 1987: 232)
The silent majority’s category persistence obstructed diffusion of the updated understanding of the disease and severely hampered the allocation of resources.
Phase 4: Persistence of the Category Schema Among the Silent Majority—January 1983 to July 1985
In this phase, the updated category schema spread as the vocal minority expanded and increasingly spoke louder about the need for action in light of the accumulating causal evidence supporting the updated schema. Yet, the silent majority persisted in clinging to their category schema through maintaining moral meanings, skepticism about the updated causal theory, and silencing.
Anomalies challenging the category schema
In December 1982, San Francisco’s public health authority identified an infant who had developed AIDS-like symptoms and died at the age of 20 months after receiving blood transfusions (Schmeck, 1982). The investigators traced all individuals linked to the baby’s blood transfusion and found one donor who turned out to have AIDS. The unequivocal link and the fact that the patient was a baby—who was assigned moral meanings of purity and to whom no one could attribute the causal theory of “gay lifestyle” or “drug use”—made the case a salient anomaly.
Vocal minority: Spread of the updated category schema
The case of the baby prompted more members of the scientific community to accept the updated causal theory of the category centered on a blood-transmitted virus (Check, 1983). In May 1983, two articles reporting AIDS in children were published in JAMA (Oleske et al., 1983; Rubinstein et al., 1983). Dr. Ammann stated, “when pediatric AIDS and AIDS in women came up, suddenly you could see how the basic scientists, the ‘mouse’ doctors, started listening.” In May 1983, a team of French scientists at the Pasteur Institute even isolated a new type of retrovirus from one AIDS patient, which would be later known as HIV (Barré-Sinoussi et al., 1983).
3
Although at the time it was disputed whether the virus they had isolated was, indeed, the disease’s causative agent (CDC, 1983), supporting evidence was accumulating (Check, 1983). Dr. Conant recalled, So a point came somewhere in the spring of ’83 where, in my mind, the overwhelming majority [of the scientific community], if not 100 percent, would have said, “Yes, this is a blood-borne communicable disease.”
Thus, the updated causal theory of the category began to spread beyond the initial vocal minority. Moreover, the vocal minority recognized that the prototypical symptoms of AIDS, like Kaposi’s sarcoma, might represent only a fraction of the affected population. They realized that milder symptoms commonly seen in many gay men, such as swollen lymph nodes, weight loss, and fever, could also be related to AIDS (Ioachim, Lerner, and Tapper, 1983).
Vocal minority: Calls for change
In early 1983, it was reported that 27.3 percent of the first 1,000 AIDS patients were not homosexual men (Jaffe, Bregman, and Selik, 1983) and that the number of patients in all demographic groups was increasing at an alarming rate.
4
Concerned about the presence of a virus in the blood supply, some CDC members literally started to “yell and scream to institute core testing [blood screening]” in their meetings with other medical institutions, according to Dr. Conant and other witnesses. A few congressmen began to call out the pervasive silence and speak up for more funding. For example, Rep. Biaggi (1983), from New York, stated that “while [AIDS] has been associated with a limited segment of the population, it is now affecting people who may acquire it from blood transfusions. It’s affecting men and women.” Rep. AuCoin (1983), from Oregon, further argued, Although new evidence shows [AIDS] is striking other segments of the population in growing numbers . . . there is an ignorance about AIDS which is being fueled by a larger social prejudice against the gay community. . . . The prejudice has silenced informed public discussion of the disease and prejudices prevented the formulation of a coordinated response by health professionals in the federal government.
In May 1983, two years after the beginning of the epidemic, the Secretary of Health and Human Services announced for the first time that “AIDS had become the No. 1 priority of the United States Public Health Service” (Pear, 1983). Overall, with the spread of the category’s updated causal theory, the voices of the vocal minority grew louder and more influential.
Silent majority: Persistence of the category schema through maintaining moral meanings
Despite the growing recognition that AIDS was a blood-borne disease, the majority continued to preserve the moral boundary between AIDS patients and mainstream society. For instance, Jerry Falwell (1985), a famous conservative reverend, commented that “AIDS [is] the homosexual disease despite attempts by the press to call it something else.” Dr. Francis succinctly summarized this: “Now the whole issue of ‘them and us’ stood out . . . they could do a ‘them’ thing very easily. ‘It is all junkies and queers. What do we care?’”
Even more troubling was the fact that a majority of medical professionals still adhered to the moral boundary between AIDS patients and the general public: one-third of doctors responded to a survey by opining that they would not provide care for AIDS patients (Gerbert et al., 1991). Drs. Volberding and Conant noted that AIDS patients received “very spotty care” and that medical institutions “were not very eager to be involved [with AIDS].” Dr. Sonnabend stated, It was mistaken to think of scientists as being dispassionate, in the sense that I was well aware that many of my fellow scientists . . . were sex-phobic, homophobic . . . They were just human beings who were squeamish about sex . . . particularly squeamish about homosexual sex. Some were antipathetic, you know, hostile. But they were human beings . . . not to be trusted with, huh, being particularly concerned about the plight of gay men or drug addicts or Black people. I don’t know why they were just as bigoted as anybody else.
The moral meanings proved to be a profoundly dichotomous and polarizing dimension of the category schema, as exemplified by Dr. Schram’s remarks: So many of the other [medical professionals] don’t give a d*** and are judgmental and antagonistic and disgraceful human beings when it comes to dealing with this epidemic. On the other hand, there have been some—and no small number any more—that have been superb. But there haven’t been a lot in between. It’s mostly real good or real bad.
Thus, a majority of medical professionals and broader audiences maintained the category’s imprinted moral meanings.
Silent majority: Persistence of the category schema through skepticism about the updated causal theory
The category schema also persisted as the silent majority remained skeptical of the virus-centered causal theory and its implication that anyone could contract AIDS. Articles attributing AIDS to “sperm, other microbes [of venereal diseases], drug abuse, and profound promiscuity” were still published in top medical journals (Sonnabend, Witkin, and Purtilo, 1983: 2371). In November 1983, six months after the isolation of a new virus by French scientists, some medical professionals still denied AIDS in women and children. Dr. Ammann said, There was a tremendous resistance on everybody’s part to expand the disease beyond a very restrictive definition. . . . When we presented our cases of pediatric AIDS . . . in November 1983, my previous mentor, Bob Good, got up and said that he didn’t think that we were seeing AIDS in children . . . There was over-resistance. People just didn’t want AIDS to affect infants.
This skepticism intensified when economic vested interests were at stake. Blood banks, including nonprofit organizations such as the American Red Cross, intensely resisted the virus-centered causal theory. Dr. Volberding recalled, “There was a meeting in March of 1983 at NYU where [Joseph] Joe Bove, who was the director of the blood bank at Yale, said he wasn’t convinced that HIV could be transmitted in the blood.” According to Dr. Moss, The blood banks f***ed it up disastrously. They didn’t get it; they didn’t react. . . . also it’s money. They don’t want to have to throw all the blood away or whatever . . . Very big powers were now involved, not just us little assistant professors.
In June 1983, the U.S. Secretary of Health and Human Services Margaret Heckler announced to the public, “I want to assure the American people that the blood supply is 100 percent safe.” Overall, reinforced by vested interests, the silent majority persisted in their category schema through skepticism of the updated causal theory, which cohered with their upheld moral boundaries.
Silent majority: Persistence of the category schema through silencing
In April 1984, three years into the epidemic, four articles published in Science demonstrated the presence of a new virus in individuals with AIDS, showcasing its mechanisms of transmission and its effects on the immune system (Gallo et al., 1984). 5 The scientific community in the United States widely recognized these articles as a confirmation of the virus causal theory. However, although this discovery was hailed as a remarkable scientific achievement, it had little impact on the level of media attention to AIDS and federal funding allocated to the epidemic (see Figure 3).
Within the media, the general public, policymakers, and the federal and state governments, the direness of AIDS and the suffering of its victims were downplayed and silenced. In New York, Governor Mario Cuomo vetoed a $5 million state-budget allocation for AIDS. In a hearing in 1983, the state health commissioner, David Axelrod, was quoted as saying, “Hypertension [is] a more important state health issue [than AIDS] in New York State” (Shilts, 1987: 340; Perrow and Guillén, 1990: 83). In December 1984, eight months after the virus theory was confirmed and the nationwide caseload approached 10,000, White House Press Secretary Larry Speakes answered a question about AIDS in a briefing by dismissively saying, “I haven’t heard him [the President] express concern, but I must confess I haven’t asked him,” as the audience laughed in the background (Calonico, 2015). According to Dr. Kotler, There was no sense of that [urgency] at all . . . I was—I can’t say dumbstruck, but it was almost surreal because the reality on the wards did not fit at all the words and concepts that were given by anybody who was supervising anything, from the hospital to the city to the state to the federal government.
According to Dr. Francis, federal efforts were “leaderless and resources [were] lacking.” The federal government did not organize any coordinated action to address the spread of the disease.
Silent majority: Persistence of the category schema through coercion
A U.S. Congressional memorandum reported that at the top level of the administration, silence and inaction had often been subtly coerced (U.S. Congress, 1985). The heads of health agencies such as the CDC and NIH were coerced into toeing the line and remaining silent about the AIDS crisis, and budget requests were often cut even before reaching the president. Dr. Conant, who served as an expert witness in many congressional hearings on AIDS, summarized his experience with the government’s inaction: Ronald Reagan and those nice people were not going to listen to me or anybody else. No matter what strategy you use—you could be reasonable, you could be hysterical, you could be confrontational, you could be diplomatic—you could do anything you wanted to do. It was not that they didn’t understand. They did not want to hear it. It’s that simple. They did not want to hear it.
It is noteworthy that this combination of skepticism, silencing, and coercion persisted long after the first proposal of the updated category schema, the virus hypothesis. For instance, even though members of the vocal minority had been advocating for blood screening using hepatitis B test results as a surrogate marker, both blood banks and the federal government failed to take action to implement such measures over a prolonged period between 1982 and 1985.
The state of the category schema
The silent majority’s adherence to imprinted moral meanings hindered updates to their category schema, as accepting a new causal theory would create dissonance with the persisting moral meanings. Although the vocal minority expanded as evidence accumulated that supported their updated theory, the silent majority still maintained the initial moral meanings and suppressed concerned voices through skepticism, silencing, and coercion.
Consequences for resource allocation
A Congressional report shows that no federal funding was requested and allocated for the year 1983 (U.S. Congress, 1985). The first budget appropriation for AIDS by Congress did not occur until 1984 (see Figure 3), and the majority of this budget allocation was earmarked for scientific research, whereas “the service needs of AIDS patients, and public education and prevention have not been considered funding priorities” (U.S. Congress, 1985). The executive branch often denied the need for funding these measures. Dr. Conant wrote a New York Times op-ed in 1985, deploring the inaction: The Secretary of Health and Human Services . . . [said that the] Administration has declared AIDS its No. 1 health priority and that her department is fighting an all-out war on this new disease. . . . We had hoped to hear from Secretary Heckler where her armies are deployed, what her funds are for supplies and armaments, what her targets and strategies are. None of these matters were addressed. Furthermore, we would like to be reassured that the Commander in Chief, President Reagan, is even aware that the Public Health Service has declared this war.
In the midst of this persistence and inaction, AIDS caseloads shot up from 1,000 in 1983 to 12,000 in 1985 (United Press International, 1985). Note that this number represented gross underreporting because only the patients who were in their final stage of the infection and had definitive AIDS symptoms were counted. According to a later CDC report, more than 5,000 blood transfusion recipients and over 70 percent of the hemophiliac population were infected with HIV between 1981 and 1985 due to the lack of preventive measures (CDC, 1987). These numbers do not include an estimate of the human lives that might have been saved by developing effective education programs for gay communities and needle exchange programs for drug users. In the absence of treatment options, at this point in history the mortality rate of the disease was near 100 percent.
Phase 5: The Silent Majority Updates the Category Schema—July 1985 and Onward
Anomalies puncturing the moral boundary
The grim news that AIDS caseloads had passed 10,000 had little impact on the level of media attention and funding. However, in July 1985, a second turning point in the emergence of the AIDS category, which would break the nationwide silence about the disease, arrived from an unexpected source. An American actor named Rock Hudson, one of the most popular movie stars of his time, was found to have been secretly treated at a Paris hospital, ostensibly for liver cancer. After collapsing in a hotel lobby, the actor admitted to the media that he had been diagnosed with AIDS. He became “the best-known American to acknowledge publicly that he has AIDS” (Altman, 1985).
Silent majority: Updating the category schema by breaking the silence
The public announcement of Hudson’s AIDS status punctured the silent majority’s moral boundary between “us and them.” Although Hudson’s disclosure fueled the perception that he was a closeted homosexual, his public image as an all-American, Republican Hollywood heartthrob still placed him on the opposite side of the moral boundary from that of other AIDS patients (Griffin, 2019). His announcement immediately received massive media attention, and he began to personify a medical condition that had been deeply marginalized and silenced. When his chartered jet from Paris landed at Los Angeles International Airport, “hundreds of newspeople and television cameras” gathered to see the country’s first celebrity AIDS patient, which broke the nationwide silence that had, until then, characterized the public’s reaction to the epidemic (Shilts, 1987).
Silent majority: Updating the category schema by morally reappraising the category
That summer and fall, media coverage of the AIDS epidemic skyrocketed (see Figure 3), creating a “glut of publicity” (Rice, 1985). Suddenly, both empathy and hysteria about AIDS swept across the country.
Hudson’s announcement coincided with a new school year, and the public’s attention quickly shifted to children with AIDS (Brier, 2006). Some parent groups vehemently opposed children with AIDS attending school, which, ironically, further punctured the moral boundary between the majority and AIDS patients (Rohter, 1985). Notably, a 15-year-old hemophiliac patient with AIDS named Ryan White (and his family) began a legal battle with his school in Indiana because widespread panic had prevented him from attending his classes (White and Cunningham, 1991). The battle catapulted White into the national spotlight, making him a poster child of AIDS in the national media. As children—a societal group imbued with moral meanings of purity, in opposition to the stigmatized moral meanings of AIDS—became the public face of the epidemic, the moral meanings associated with the disease began to shift. For example, Dr. Selwyn recalled, “reading through a medical chart . . . [we] use the term ‘unfortunate,’ you’d read, ‘this unfortunate 34-year-old woman,’ or ‘unfortunate 65-year-old blood transfusion recipient’ . . . the notion of innocent victims meaning non-gay men, non-drug users.” The moral boundary between the majority and AIDS patients became porous as the images portraying victims as individuals with human faces flooded in.
During this time, a Hollywood fundraising event was held for AIDS victims, “a cause that was far from popular a few months ago,” according to a New York Times article depicting the event (Harmetz, 1985). Famous socialites and celebrities suddenly “begged for an end to the stigma attached to people who have AIDS” and claimed that “it was time to make AIDS everyone’s business.” In this charity event, President Reagan—the head of the government who had remained silent about the crisis—stated through a telegram that “[the] Administration had made halting the spread of AIDS a top priority.” This, once again, signified the puncture of the moral boundary between the mainstream and the epidemic.
The state of the category schema
The puncturing of the moral boundary prompted the silent majority to update their moral meanings, leading to the boundary’s neutralization. Breaking silence enabled them to adopt the updated coherent category that reflected diluted stigma, diverse symptoms and patients, the virus-centered causal theory, and its public health implications. The public began to reappraise the category as a tragedy of human suffering and a dire public health issue.
Consequences for resource allocation
As the category’s moral meanings were updated, resources for AIDS poured in. Dr. Friedland described the dynamics succinctly: If you look historically at the sort of blips in increase in funding, heterosexual transmission, “Oh, my God, we can get it!” Right? Boom, big increase in funding. Children, “Oh, the poor innocent victims!” Boom, big increase in funding.
Just one month after the news that Rock Hudson had been diagnosed with AIDS and the ensuing upsurge of public discourse concerning the crisis, the House Appropriations subcommittee voted “to double the budget for research on AIDS, and to increase funds for education and public health programs” (The New York Times, 1985). As shown in Figure 3, the largest increase in funding for AIDS happened between 1985 and 1986, coinciding with the sharp rise in media attention. Furthermore, in 1990, shortly after Ryan White’s death, Congress passed legislation named after him, the “Ryan White CARE Act,” which remains the largest federally funded program for AIDS patients passed to date.
Epilogue: Persistence of the moral meanings
The puncturing of the moral meanings of AIDS “irrevocably” updated the silent majority’s perception of the category AIDS (Shilts, 1987: 480; Brodie et al., 2004). AIDS slowly became a regular item in Congress’s budget and agenda (Summers and Kates, 2004). Nonetheless, until quite recently, AIDS remained a stigmatized medical condition, not just for patients but also for medical professionals who provided care for them (Snyder, Omoto, and Crain, 1999). As AIDS became a pandemic in the Global South during the 1990s, the silence and misinformation that had plagued the public reaction to AIDS in the U.S. would also devastate the public health of developing countries (Konotey-Ahulu, 1987).
Theoretical Model: A Process Model of Category Persistence and Updating
Figure 4 provides an overview of the theoretical model generated from our study. Below, we discuss each phase of our model and demonstrate how the elements within each phase generalize to the emergence of other categories studied in the literature.
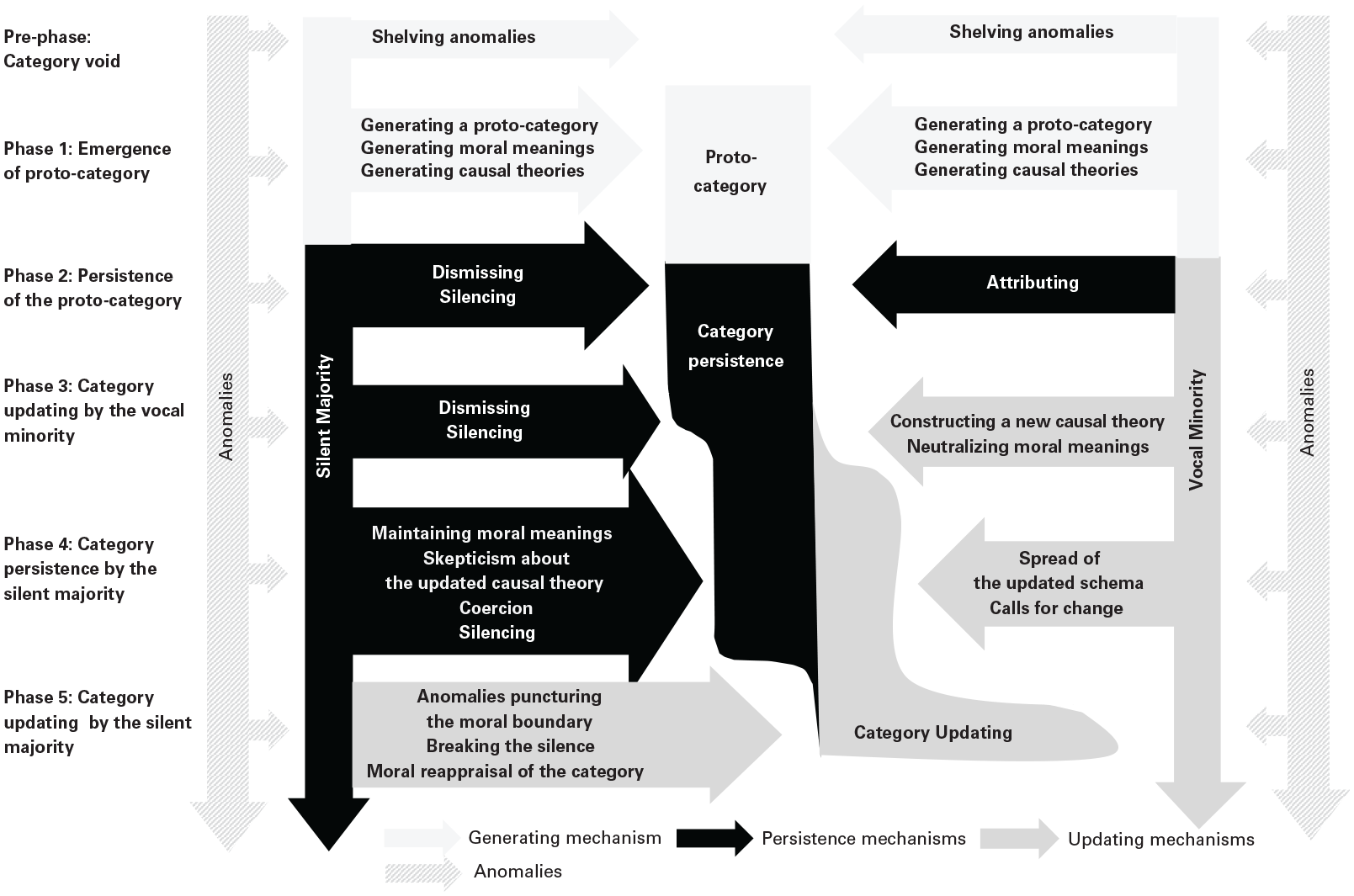
Process Model of Achieving Category Coherence
We identified a pre-phase and five phases during which a category is updated or persists. During the pre-phase, audiences encounter anomalies that cannot be explained by the existing categories, but without seeing a pattern they simply shelve the anomalies and do not create a new category. This mechanism applies to other contexts, such as the modern Indian art category, in which anomalous art pieces were shelved and undervalued for an extended period without being reclassified into a new category (Khaire and Wadhwani, 2010).
During the first phase, emergence of a proto-category, a small group that later becomes the vocal minority identifies a pattern among salient anomalies that are perceived to be similar. While this initial proto-category is infused with moral meanings, the vocal minority generates a rough causal theory to explain the category’s existence. During this phase, the three dimensions of the initial category schema—prototypical features, moral meanings, and causal theories—cohere with one another. The initial category schema persists through silencing as the majority remains silent about the category, limiting resource allocation to the category. This process is comparable to the emergence of the grass-fed beef category, in which producers constructed a coherent category by infusing it with strong moral meanings aligned with a causal theory of how grass-fed beef was produced (Weber, Heinze, and DeSoucey, 2008).
The second phase, persistence of the proto-category, is ignited when anomalies challenge the category schema. During this phase, audiences persist in their initial coherent understanding of the proto-category through three mechanisms that, together, allow audiences to dismiss the anomalies: attributing features to anomalies, dismissing anomalies, and silencing. This extends to other contexts in which actors uphold an ill-fitting category schema. For instance, participants in the nascent online advertisement exchange category perceived it as similar to financial exchanges, despite evidence suggesting otherwise. These participants persisted in their initial understandings by stretching and bending features (Glaser, Fiss, and Kennedy, 2016). In another case, anomalous practices such as financial derivatives conflicted with the moral dimension of the Islamic banking category, i.e., a financial model that avoids charging interest rates and thereby adheres to Sharia law, but these anomalies were dismissed by a “silencing of the normative attributes of the product” (Arjaliès and Durand, 2019: 900) to uphold the initial category schema (Syakhroza, Paolella, and Munir, 2019).
The third phase, category updating by the vocal minority, is triggered when the vocal minority generates an alternative causal theory that can explain anomalies challenging the category schema. This spurs the vocal minority to update their category schema by revising not just their causal theory but also the moral meanings in order to construct an updated coherent category. We identify similar mechanisms in other settings. For example, Lee, Hiatt, and Lounsbury (2017) showed that the organic food category was transformed as emphasis shifted from the category being associated with holistic moral principles toward the use of specific inputs and production methods. This shift in emphasis toward the causal dimension of the category schema coincided with a gradual neutralization of moral meanings.
During the fourth phase, category persistence by the silent majority, more people join the vocal minority as the updated causal theory spreads, and they begin calling for change to persuade broader audiences to also update their category schema. But the silent majority maintains the imprinted moral meanings, with which the updated causal theory does not cohere. The silent majority persists in their imprinted category schema by covertly casting skepticism on the updated causal theory, silencing the vocal minority, and relying on coercion. As the silent majority holds the dominant position in the power structure, this hampers resource allocation to the category. This phase applies to many contexts. For example, in the stem cell category, despite potential scientific breakthroughs associated with stem cells, the majority persists in adhering to the moral meaning that embryos are sacred and thus exempted from human manipulation, and remains skeptical of the updated understanding of stem cells (Evans, 2021). Likewise, the tobacco industry’s use of doubt and misinformation effectively silenced the vocal minority advocating for a causal relationship between smoking and lung cancer. As a result, for a prolonged period a large part of the American population resisted updating their understandings of the risks associated with smoking (Brandt, 2007; Hsu and Grodal, 2015). Clashes between the moral and causal dimensions of category schemas and the silencing of causal theories have also become increasingly evident in contemporary phenomena such as climate change denialism and the proliferation of misinformation (Norgaard, 2011; Schüssler, Rüling, and Wittneben, 2014).
The last phase, category updating by the silent majority, commences when anomalies that challenge the moral meanings of the category appear. This breaks the silence by puncturing the moral boundary between the stigmatized members of the category and the majority, which catalyzes public conversations among the silent majority and eventually helps them to reappraise the category. The puncturing of the moral boundary facilitates updating the category schema such that an alternative coherent schema forms regarding the updated prototypical features, moral meanings, and causal theories. After the majority updates the category schema, they reappraise its value and eventually channel resources toward the emerging category. In other contexts, similar mechanisms can be observed. For example, people using hearing aids have long faced moral stigma due to the device’s association with aging, fragility, and even low intelligence, creating a moral boundary that isolates and silences individuals with hearing loss (Krabbe and Grodal, 2023). Despite marketing efforts, hearing aids’ market penetration rate had long hovered around only 20 percent (Abrams and Kihm, 2015). However, on “September 7, 1983, White House Spokesman Larry Speakes announced that President Ronald Reagan was wearing hearing aids. It was the fitting heard round the world. A barrage of public press coverage concerning hearing healthcare and hearing aids ensued” (Strom, 2013: 1). President Reagan’s announcement helped to puncture the moral boundary isolating people with hearing loss, paving the way for a dramatic 29.8 percent growth in the U.S. hearing aid market (Kirkwood, 2003). The phases in our model collectively offer a theoretical framework that can be generalized to help scholars understand the mechanisms driving category persistence and updating.
Discussion
Our findings contribute to theories of category emergence by unpacking the dynamics of category persistence and updating and by investigating the role of imprinting, silence, and power in category persistence. We discuss each of these contributions below.
The Dynamics of Category Persistence and Updating
We contribute to the categorization literature by identifying how and why category schemas persist or are updated as new information arises during category emergence (Kennedy and Fiss, 2013; Durand and Boulongne, 2017). The category literature has assumed that category schemas are gradually updated as information about the novel category accumulates (Khaire and Wadhwani, 2010; Bingham and Kahl, 2013; Hsu and Grodal, 2021). In contrast, the literature on imprinting presumes that the initial schemas imprinted into a category make category updating difficult in the face of new information (Marquis and Tilcsik, 2013; Rhee et al., 2017). This study bridges these conflicting assumptions by simultaneously investigating the processes that drive both persistence and updating. We show that conflicts among different category dimensions can stifle updating, thereby prolonging category persistence. That is, despite the accumulation of dissonant information, category schemas can still persist (Pontikes and Barnett, 2015; Glaser, Fiss, and Kennedy, 2016) if audiences cling to existing moral understandings while disregarding accumulated evidence and urgent calls for category updating.
We can explain this puzzling phenomenon by pointing to category coherence (Murphy and Medin, 1985; Soublière, Lo, and Rhee, 2023): updating occurs only when audiences construct a coherent category across multiple category dimensions. By emphasizing the multidimensionality of categorization processes (Granqvist and Ritvala, 2016; Boulongne and Durand, 2021), we add nuance to the existing literature on category coherence (Murphy and Medin, 1985; Soublière, Lo, and Rhee, 2023), which often equates category coherence with the degree of internal category heterogeneity (Lo et al., 2020; Soublière, Lo, and Rhee, 2023). Building on Durand and Paolella’s (2013: 1112) insight that “for a given audience, cognitive compatibility across categories [dimensions] may vary,” we suggest that category coherence can also represent the degree of alignment between different category dimensions. In doing so, we expand on the existing literature by highlighting the important roles, for achieving category coherence, of dismissing and attributing certain features to align or misalign with existing category dimensions (Glaser, Fiss, and Kennedy, 2016; Arjaliès and Durand, 2019).
We also extend existing scholarship by showing that an oppositional category structure can be detrimental to category emergence and updating (Hsu and Grodal, 2021). Scholars have pointed to the generative role of oppositional categories in stimulating category emergence (Rao, Monin, and Durand, 2005; Sine and Lee, 2009; Lee, Hiatt, and Lounsbury, 2017). For instance, Weber and colleagues (2008) showed how the category “grass-fed beef” was infused with moral meanings that were oppositional to traditional beef and how this opposition benefited the category’s emergence. In contrast to these studies, we show that the oppositional category structure can stifle emergence and hinder updating (Durkheim, 1912; Douglas, 1966; Barley, 1983; Anteby, 2010; Vergne, 2012).
To explain the discontinuity of category schema dimensions, we connect the theory of category emergence with the literature on scientific evolution (Kuhn, 1962; Lakatos, 1970; Latour and Woolgar, 1986; Latour, 1987). Kuhn (1962) described how a scientific theory persists despite the discovery of anomalies that ought to falsify the theory, and he claimed that updating the theory happens only when an alternative theory emerges that can explain the anomalies. We show that this discontinuous process not only occurs in the context of changes in scientific paradigm but might also occur multiple times during category emergence, albeit at a more granular level. We further demonstrate that the process of updating scientific theories might be governed by the need to establish category coherence across the moral as well as causal dimensions. Thus, while the existing literature has argued that scientists might experience a strain between morality and science (Evans, 2021), we further assert that such conflicts can even originate at the category schema level such that updating the category’s causal dimension might conflict with updating its moral dimension.
In particular, our study highlights the difficulties of updating causal understandings when a category’s moral dimension carries significant weight (Howard-Grenville et al., 2017; Arjaliès and Durand, 2019; Lashley and Pollock, 2020). Such categories can create polarizing moral boundaries (Lamont and Molnár, 2002) that are guarded and preserved through active policing (Hampel and Tracey, 2017; Grodal, 2018; Siltaoja et al., 2020; Lockwood, Glynn, and Giorgi, 2023). Audiences might resist updating a morally laden category when new causal understandings require a moral boundary to be redrawn, which thereby equalizes the audiences on either side of the boundary. We contribute to the literature by showing that a moral boundary can be punctured when a salient event spurs audiences to reposition individuals and entities previously placed outside of the moral boundary to within it, thereby reducing the perceived divide between opposing sides. Understanding how moral boundaries are punctured is crucial for addressing inequality and social injustice. For example, the killing of George Floyd helped to puncture the moral boundary established between Black Americans and the White majority, drawing an outpouring of resources and attention to racial inequality (Onwuachi-Willig, 2021).
Our findings related to puncturing a moral boundary expand our understanding of how scientific discoveries and causal theories can be communicated to the general public (Burns, O’Connor, and Stocklmayer, 2003). Currently, many Americans hold a sense of distrust toward professionals and the government and have erected a moral boundary that separates these elite groups from the majority (Hahl, Kim, and Zuckerman Sivan, 2018). The elites often seek to shape public opinions on grand challenge issues such as climate change (Norgaard, 2011; Schüssler, Rüling, and Wittneben, 2014). Yet, they often communicate in scientific terms, which may not be effective in persuading the majority (Grodal and O’Mahony, 2017). When a silent majority clings to a strong moral boundary, advocating for category updating solely through rational arguments and causal explanations is likely to fail, as we have observed in the recent proliferation of misinformation (Vosoughi, Roy, and Aral, 2018) and denialism (Thornton, 2004). Instead, the vocal minority might have to first focus on puncturing the moral boundary before attempting to update the category along the causal dimension.
Category Persistence: Imprinting, Silence, and Power
While much of the categorization literature has attended to category updating (Rosa et al., 1999; Lee, Hiatt, and Lounsbury, 2017), our article focuses specifically on the mechanisms driving category persistence. First, by showing how moral meanings can be imprinted on a category and how these understandings might persist (Tilcsik, 2014; Rhee et al., 2017), we answer calls to develop a more nuanced theory of imprinting, through our investigation of “tensions between imprint decay, persistence, and amplification” (Marquis and Tilcsik, 2013: 197). We suggest that sensitive periods—that is, times of transition—can be an opportunity for both imprint decay and amplification. In our study, sensitive periods occurred when new anomalies arose that challenged the emerging category schema. In some cases, these anomalies spurred imprint amplification because the anomalies were aligned with the imprinted category dimension. In other cases, the anomalies generated imprint decay because they were dissonant with the imprinted category dimension, which over time undermined the strength of the imprinted category dimension.
In refining the dynamics of category imprinting, we also offer a more nuanced perspective on Rhee and colleagues’ (2017) conceptualization of “proof” and a professional community’s authority in defining a category. In contrast to their study’s prediction that professional authority stabilizes categories and amplifies imprinting, our findings reveal that the general public may readily dismiss this authority. It is crucial to emphasize that the public may not engage in overt challenges or arguments but, rather, may disempower professional authority through silencing and dismissal. This underscores the need to differentiate a category’s authority from that authority’s power to impose understanding of the category on the majority (Neisser, 1987; Boulongne, Cudennec, and Durand, 2019). When a category’s authority and power are decoupled and controlled by different social groups, one group may have the authority to define the category, but the spread of their understanding of the category to the powerful majority might face delays or not prevail at all. This insight challenges the literature’s previous assumption that limited access to information prompts lay audiences to rely on experts (Beckert and Musselin, 2013). Our study suggests that if a moral boundary constraining a category is robust enough, the public might not heed information conveyed by experts.
Furthermore, much of the existing literature has studied category persistence as resulting from active contestation between different stakeholders (Khaire and Wadhwani, 2010; Jones et al., 2012; Grodal, 2018). Hoffman (1999), for example, illustrated that the contestation over “corporate environmentalism” spurred the creation of a category around the issue. Overt contestation has garnered scholarly attention because it leaves a traceable paper trail (Grodal and Kahl, 2017). However, a growing literature suggests that contestation can also unfold through silence (Bird, 1996; Morrison and Milliken, 2000; Anteby, 2016; Carlos and Lewis, 2018; Arjaliès and Durand, 2019). We expand this literature by showing how silencing can affect category persistence and updating. For example, tobacco producers successfully prevented the majority from updating the smoking category by employing silence and casting doubt on the causal link between smoking and lung cancer (Hsu and Grodal, 2015).
By explicating how silence hinders category updating, we extend the burgeoning literature on silence (Clemente and Roulet, 2015; Arjaliès and Durand, 2019). Recent such literature has predominantly focused on how transgressions of a moral boundary are silenced (Anteby, 2008). For instance, violations committed by individuals or entities within a moral boundary (i.e., perceived as morally virtuous)—such as Catholic priests (Gutierrez, Howard-Grenville, and Scully, 2010), socially responsible funds (Arjaliès and Durand, 2019), and Islamic banking (Syakhroza, Paolella, and Munir, 2019)—are often veiled in a self-reinforcing spiral of silence (Clemente and Roulet, 2015). Changes occur when salient events or entrepreneurial efforts force discussions about these transgressions. Most studies have examined the process of reinstating a moral boundary after these trigger events break the silence. This reinstating process often involves moving the violation or perpetrator, such as the Catholic priests who molested children, from the inside (i.e., morally good) to the outside (i.e., morally bad) of the moral boundary (Gutierrez, Howard-Grenville, and Scully, 2010; Arjaliès and Durand, 2019). For example, through a study of the scandal regarding Oscar Wilde, Adut (2005) showed that Victorian society tolerated homosexual behaviors among elites as long as they remained unspoken. But when Wilde’s lawsuit against the Marquess of Queensbury forced public discussions of his homosexual relationships, it led to his exclusion from the inside of the moral boundary.
Our research extends the literature by showing an opposite process through which the breaking of silence erodes a moral boundary, thereby equalizing the entities on both sides of the boundary. When we silence the experiences and existence of specific individuals and entities (e.g., homosexual, transgender, or Black individuals), we mute discussions of their unequal treatment, which is, at times, subject to reevaluation. The puncturing of a moral boundary occurs when entities that were placed outside this moral boundary are repositioned within, thereby redrawing the boundary (Lashley and Pollock, 2020). The act of explicitly articulating moral boundaries can help to puncture rather than reinforce them, particularly when individuals placed outside the boundary are humanized and recognized as victims of this division. Our study extends Clemente and Roulet’s (2015) work by suggesting that the spiral of silence affects not only actors’ practices within a field but also the category schema they hold and the dynamics of category persistence and updating.
We also contribute to the literature on the relationship between categories and power by moving away from considering categories as passive cognitive devices. In doing so, we answer calls to incorporate power and politics more explicitly into categorization theory (Grodal and Kahl, 2017; Quinn and Munir, 2017). We extend the literature through our examination of the role that powerful professionals play in the categorization process. The existing literature has pointed to professionals as originators of category legitimation in fields as diverse as life insurance (Zelizer, 1994; Chan, 2009) and green chemistry (Howard-Grenville et al., 2017). According to the existing literature, we should predict that professionals would uphold professional norms; for example, physicians ought to uphold the Hippocratic oath to serve all clients equally despite their social standing, and participate actively in legitimizing their clients (Abbott, 1981, 1988). However, we observed that many professionals used silence and avoidance to hinder the legitimacy of the category. Such observations suggest that in order to develop a more nuanced understanding of the role that professionals play in category emergence, we must understand how professionals’ embeddedness within broader societal norms (Dunn and Jones, 2010; Thornton, Ocasio, and Lounsbury, 2012) can create conflicts between their professional norms and moral values. This can happen, for example, when professionals are part of both professional and religious groups that have conflicting category understandings (Thornton, 2004).
Boundary Conditions and Future Research
While we provide a framework of mechanisms that drive category persistence and updating, there are boundary conditions to the generalizability of our findings. First, we studied a category that from its inception was imprinted with strong moral meanings. While our findings can generalize beyond morally laden categories (Weber, Heinze, and DeSoucey, 2008; Anteby, 2010; Arjaliès and Durand, 2019; Lashley and Pollock, 2020; Hsu and Grodal, 2021), our mechanisms apply particularly to contexts in which category dimensions, such as the moral or causal dimension, are discontinuously updated. In contrast, updating along a continuous dimension, such as the prototype dimension, might yield a pattern of more-gradual updating (Rao, Monin, and Durand, 2005) but still might yield periods of persistence interspersed with updating. To fully understand this process, we need more-granular future studies that uncover the micro-dynamics of category persistence and updating.
Another boundary condition of our study is that we examined a category that was not strategically introduced into a market but, instead, emerged organically. In categories that are strategically created, stakeholders might work to either facilitate category updating or prolong category persistence to serve their self-interests (Kennedy, 2008; Weber, Heinze, and DeSoucey, 2008; Navis and Glynn, 2010). However, these strategic actions can spur conflicts and challenges in maintaining coherence among multiple dimensions of a category schema. Strategic actions to update or maintain a category in audiences’ minds may face the same challenges along a discontinuous dimension such as moral meanings or causal theories. For instance, prior studies have often viewed moral opposition as an effective strategy for category creation and new market emergence (Weber, Heinze, and DeSoucey, 2008), but this reliance on categorical dichotomy and oppositional positioning may backfire (Hsu and Grodal, 2021). For example, when advocates for categories such as renewable energy (Sine and Lee, 2009), electric cars (Suarez et al., 2018), and plant-based meat (Ehlers, 2022) aim to expand their markets beyond their initial customer base, how would they convince the majority of the public to adopt their products if those customers fundamentally disagree with the underlying causal theory that the climate is changing and our civilization is in danger? Therefore, future research might examine how strategic actors promote category persistence and updating along discontinuous and often dichotomous dimensions, such as the moral and causal dimensions, in market settings.
Lastly, in our case, the causal model was eventually updated, and scientifically informed understandings of the category prevailed. But other categories might evolve differently. Because we studied a fatal disease in which the relationship between cause (having the virus) and effect (succumbing to illness) was simple (Hastie, 1984), it was difficult to avoid updating the causal model in the long run. In other categories whose relationship between cause and effect is more complex, updating might take longer or never happen at all. Our study calls for future research to investigate the rising contention between causal theories and moral meanings that increasingly plagues many democracies around the world. The dissonance between science-backed causal theories and the moral meanings held by a majority of the populace is leading to the creation of misinformation (Vosoughi, Roy, and Aral, 2018), anti-intellectualism (Bonikowski and DiMaggio, 2016; Hahl, Kim, and Zuckerman Sivan, 2018), climate change denialism (Norgaard, 2011), and the politicization of organizations (Gupta, Briscoe, and Hambrick, 2017). Our research calls on future studies to investigate the cognitive underpinnings of these broader social phenomena that affect both organizations and the public at large.
Supplemental Material
sj-pdf-1-asq-10.1177_00018392241240319 – Supplemental material for Junkies, Queers, and Babies: Persistence and Updating of the Category AIDS Through Silencing and Puncturing of the Moral Boundary
Supplemental material, sj-pdf-1-asq-10.1177_00018392241240319 for Junkies, Queers, and Babies: Persistence and Updating of the Category AIDS Through Silencing and Puncturing of the Moral Boundary by Mia Chang-Zunino and Stine Grodal in Administrative Science Quarterly
Footnotes
Acknowledgements
We thank our editor András Tilcsik and three anonymous reviewers for their constructive feedback and suggestions. We would also like to thank the following scholars for their helpful comments on prior versions of this manuscript: Michel Anteby, Mary Ann Glynn, Nina Granqvist, Elizabeth Hood, Anders Krabbe, Michael Lounsbury, Giacomo Negro, William Ocasio, Siobhan O’Mahony, Micah Rajunov, and Diego Zunino. This study was supported in part by Questrom School of Business.
Supplementary Material
1
We collected articles from The Journal of the American Medical Association (JAMA) and specialty publications such as JAMA Dermatology, JAMA Ophthalmology, JAMA Pediatrics, JAMA Internal Medicine, JAMA Neurology, and JAMA Surgery.
2
The interviewee used the label “AIDS” anachronistically; the label did not yet exist at this time.
3
This achievement would earn Luc Montagnier and Françoise Barré-Sinoussi the 2008 Nobel Prize.
4
The actual percentage was higher given that the report systematically excluded child patients from the statistics, and female and other types of non-homosexual patients were frequently omitted from diagnosis.
5
This virus would later be verified as identical to the one detected by the Pasteur Institute.
Authors’ Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.