
Abstract
Two research traditions have evolved to assess links between recessions and health, with seemingly divergent findings. Aggregate-level studies generally find that mortality rates decline during recessionary periods. By contrast, individual-level studies generally find that events that frequently occur during recessions, like job loss, unemployment, and material hardship, carry negative health consequences. We comprehensively review evidence from these two bodies of research, illustrate key findings, and show how the different mechanisms can operate in parallel. We also outline some of the limitations of the extant evidence, discuss studies emerging to address these limits and directions for future research, and provide brief empirical examples to illustrate some of these limits and directions using the Health and Retirement Study and the Michigan Recession and Recovery Study. Our review emphasizes the importance of considering both the aggregate- and individual-level associations when evaluating the likely short- and longer-term consequences of the Great Recession for health and health disparities.
Individual and public health are linked to financial stability and economic well-being. As such, it is reasonable to expect that the Great Recession of 2007–2009, which caused turmoil in labor, housing, and financial markets, would have an impact on health and health behaviors. Two independent bodies of research assess these associations, with seemingly divergent findings. One focuses on aggregate-level associations between business cycle indicators (e.g., unemployment rates) and rates of mortality, generally finding that mortality declines during recessionary periods. The other considers individuals who experience the kinds of events that happen more frequently during recessions, generally finding worse health among those who experience job loss, unemployment, and material hardships such as housing or food insecurity. Seldom is the evidence from these two bodies of research considered together, and doing so in this review provides a more comprehensive view of the multiple ways that the Great Recession may have affected the health of populations, social groups, and individuals.
In this article, we discuss aggregate and individual levels in turn, reviewing evidence from studies that illustrate key findings and the proposed mechanisms underlying associations between recessions and health. We do not attempt an exhaustive literature review but, rather, map key contours of several broad literatures across social and health science disciplines. We draw on evidence from a variety of societal contexts but focus mainly on the case of the United States. The United States has unique characteristics that condition the associations we discuss, such as the tight link between employment and access to health insurance coverage among working-aged adults—an important pathway potentially linking unemployment and well-being. Our review emphasizes the importance of considering the different mechanisms and consequences operating at the aggregate and individual levels. We also outline some of the limitations of the extant evidence at each level, discuss some of the studies emerging to address these limits and directions for future research, and provide a few empirical examples for illustration. Finally, we discuss the likely short- and longer-term consequences of the Great Recession for health and health disparities based on our review of extant research.
Recessions and Health: Aggregate-Level Studies
One area of research has focused centrally on the aggregate, or population-level, associations between macroeconomic conditions and mortality rates. This set of studies, conducted mainly by economists, has shown that despite sometimes having drastically negative financial consequences, economic downturns are linked to decreases in several major causes of mortality at the aggregate level. In other words, mortality is procyclically linked with the business cycle, as mortality rates rise when the economy grows and fall during economic downturns. The major exception to this somewhat counterintuitive pattern of procyclical mortality is the suicide rate, which rises in recessions.
Research from as early as the 1920s showed a procyclical association between the business cycle and mortality in the United States (Ogburn and Thomas 1922), and recent studies have confirmed reductions in all-cause mortality rates during economic downturns (Ruhm 2005a; Tapia Granados 2005), particularly in deaths from traffic accidents and other external causes, and cardiovascular and respiratory deaths. Procyclical mortality has been reported for other high- and middle-income economies, including Germany (Neumayer 2004), Japan (Tapia Granados 2008), Mexico (Gonzalez and Quast 2011), and twenty-three member states of the Organisation for Economic Co-operation and Development (OECD) over the 1960–1997 period (Gerdtham and Ruhm 2006), though a few studies have not found procyclical associations (e.g., Gerdtham and Johannesson 2005). In Figure 1, we illustrate some of the most commonly studied pathways and mechanisms hypothesized to result in these changing mortality rates. We use this figure to guide a review of the relevant literature and summarize some of the current debates and new directions in aggregate-level studies of recessions and health.
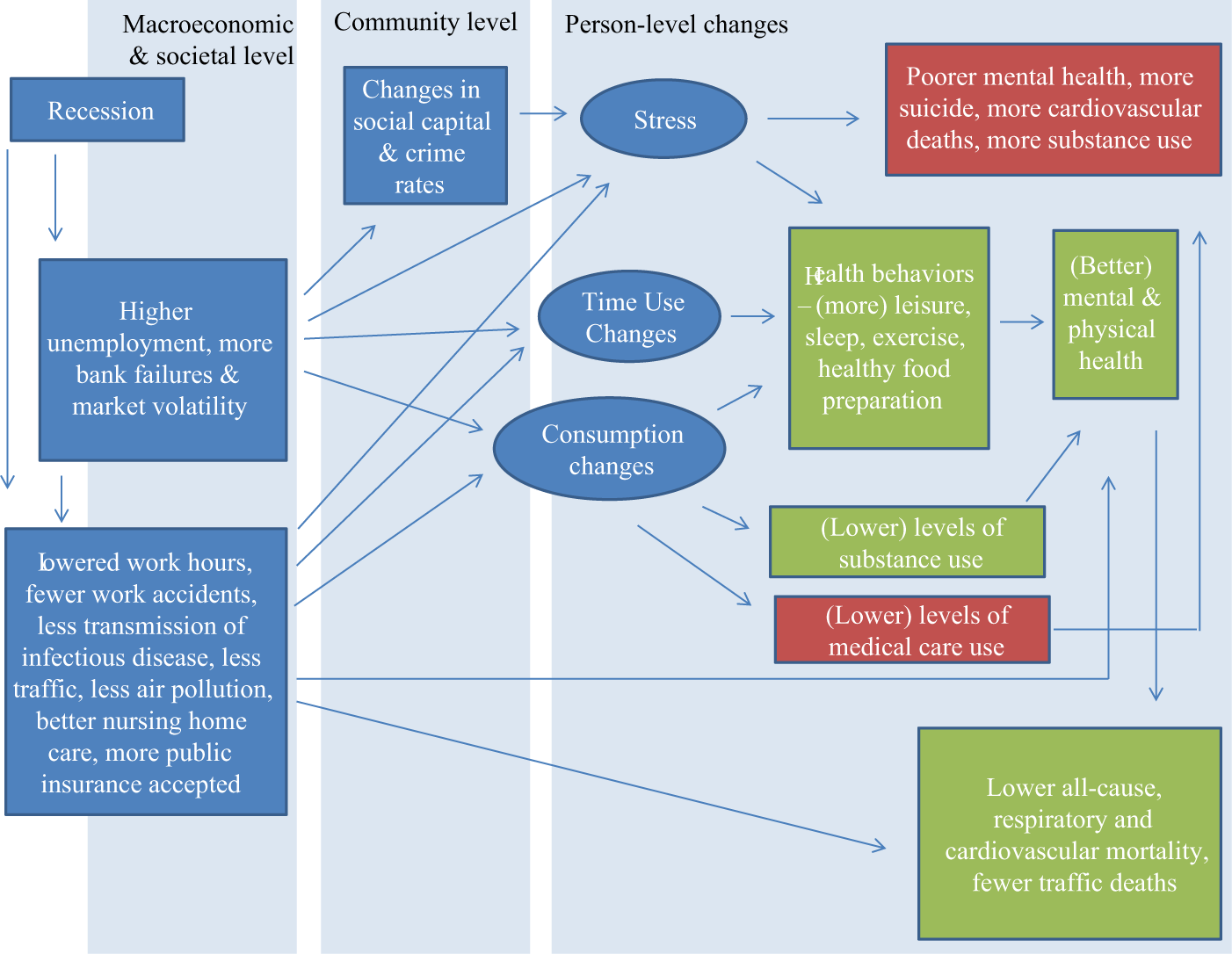
Selected Aggregate-Level Hypothesized Pathways Linking Recessions to Health
As Figure 1 suggests, recessions cause changes at the macroeconomic level that can affect health and mortality in several ways. A slower pace of production and growth in weaker economic periods can reduce workplace accidents and the proportion of inexperienced workers on the job in construction and other dangerous industries. Changes in the population’s behavior during recessions can also lessen traffic and lower air pollution and reduce infectious disease transmission, accidental deaths, and cardiovascular or respiratory deaths among those with predisposing conditions. These changes may also allow for more leisure and socializing and less stress for the population overall, particularly those who do not experience major economic hardship as a result of the recession. Some researchers have particularly emphasized the way that higher unemployment and shorter work hours change both time use and consumption behaviors. The time availability hypothesis suggests that individuals will use increases in available time for more leisure, sleep, exercise, and healthful food preparation, for example, and this hypothesis has received some support. Ruhm (2005b) found that macroeconomic growth was associated with increased obesity, reduced physical activity, and worse diets in the United States over the 1987 to 2000 period, particularly among the obese and the physically inactive. Other aggregate-level studies have also shown lower levels of exercise in better macroeconomic times (Xu 2013). Recessions could also improve health via a reduction in consumption of harmful substances, such as tobacco (Ruhm 2005b; Xu 2013). Some studies have also shown that alcohol use and alcohol-involved driving are procyclical behaviors (Ruhm 1995), helping to explain why there are fewer deaths attributed to traffic accidents in recessions.
However, the economic and employment volatility of recessions may also change spending patterns in harmful ways. For example, more recent U.S. data have shown that fruit and vegetable consumption declines when the unemployment rate rises, while fast food and snack consumption increase (Dave and Kelly 2012). Aggregate findings on alcohol consumption and abuse are mixed (Catalano et al. 2011), and a recent study found that four types of problematic alcohol consumption increased as the economy declined (Dávalos, Fang, and French 2012). Moreover, consumption of some kinds of medical and dental care decreases during recessions, including during the Great Recession (Lusardi, Schneider, and Tufano 2010; Wall, Vujicic, and Nasseh 2012), which could have negative longer-term consequences.
Some aggregate-level studies have provided an alternative explanation for procyclical mortality, focusing on changes associated with the business cycle that shape the quality of available medical care. These studies argue that the elderly contribute most of the avoided deaths in recessions, but changes in time use or employment conditions, or voluntary changes in substance use, are unlikely to explain their improved survival. Some research has focused on specific ages, causes, and locations of deaths and argues that nursing home care quality improves in recessions, when more qualified health care personnel are seeking work, potentially explaining why deaths among the institutionalized elderly decline in those periods (Stevens et al. 2011). Others have argued that recessions induce medical care providers to accept more public insurance and that other changes in the quality and availability of health care, as well as declines in air pollution that are particularly salient for the elderly, account for much of the procyclical association (Miller et al. 2009). A study of coronary heart disease deaths suggests a related mechanism, finding that seniors are less likely to receive specific cardiovascular medical procedures when the economy is growing, though the reasons underlying this decrease in access to care are not clear from existing data (Ruhm 2007). Though the majority of deaths occurs among the elderly, some studies have found procyclical effects on mortality rates of infants (Dehejia and Lleras-Muney 2004) and working-aged adults (Ruhm 2000), suggesting the importance of considering mechanisms that affect survival across the life course, whether they reflect intentional behavioral changes or spillovers of the business cycle. A recent paper suggests that corrections to misspecification of models in past studies confirm that procyclical associations are found across the life course (Ionides, Wang, and Tapia Granados, forthcoming).
The clearest exception to the procyclical association between business cycles and mortality is the suicide rate, which has been shown to rise in recessions, including in the Great Depression (Tapia Granados and Diez Roux 2009), and in recent years in the United States (Nandi et al. 2012; Tapia Granados 2005), England (Barr et al. 2012), and Japan (Tapia Granados 2008). Researchers theorize that high unemployment rates and financial market volatility can generate perceived or actual economic insecurity for individuals, increasing stress that can predict poorer mental health and higher suicide mortality. Other specific causes of mortality linked to stress may also be affected; one study found that cardiovascular deaths rise when there are more bank failures (Stuckler, Meissner, and King 2008), but there has been only limited evidence for countercyclical mortality from causes other than suicide. Recessionary changes at the community level may also increase individual stress and could harm health, though there has been less research examining these pathways. Nonetheless, studies have shown that recessions over past decades in the United States have been associated with an uptick in burglary and robbery (Bushway, Cook, and Phillips 2012), and attention to influences of recessions on social capital and other community resources and conditions may be warranted.
Limitations of aggregate-level evidence and future directions
For those interested in forecasting the health consequences of the Great Recession, aggregate-level studies cannot meet every need. First, there has been a heavy focus on mortality, a reliable outcome measure that can be obtained from high-quality public records. However, the full impact of recessions on health may be underestimated if changes in health that do not result in death are not considered. Poor mental and physical health results in high costs for society in terms of productivity and health care utilization, for example, even if it does not result in suicide or acute cardiovascular mortality. Despite the difficulty obtaining population-level morbidity data, a few studies have assessed the association between economic changes and aggregate patterns of physical and mental health and have found results generally consistent with the mechanisms proposed by mortality studies. For example, health problems from back ailments to ischemic heart disease increased with economic growth in the 1970s U.S., especially for those of prime working age, employed individuals under 65, and men, though nonpsychotic mental disorders became less common (Ruhm 2003). A recent study used aggregate Internet search query surveillance to show that queries about psychological distress rose with an increase in the rate of mortgage delinquencies and foreclosure or rates of unemployment in the Great Recession (Ayers et al. 2012).
A second issue is the temporal period over which health consequences of recessions should be measured. Mortality consequences have generally been measured for the year or few years contemporaneous to the recessionary period. Changes in behaviors proposed as mechanisms can have acute effects, such as in the case of an avoided alcohol-induced traffic accident or death of a seriously ill elderly person, but they may take considerable time to result in health decline and death for other individuals if the underlying mechanism is stress, leading to more incremental changes in behavior and well-being. The issue of lagged effects has been debated, but is particularly relevant as more aggregate-level studies of morbidity, rather than only mortality, are conducted.
Third, with the exception of studies of the Great Depression (Stuckler et al. 2012; Tapia Granados and Diez Roux 2009), most aggregate-level studies are based on recessions less severe than the Great Recession. Moreover, there is some suggestion that the impact of macroeconomic change on mortality rates may be weaker in recent years in the United States (McInerney and Mellor 2012). One explanation for a weakening procyclical association suggests that cancer has accounted for a growing share of deaths over the past decades as the population ages, and many types of cancer are unrelated to the business cycle (Tapia Granados 2008). If the procyclical association between recessions and mortality changed over time because of changes in population composition or in the distribution of causes of death, if it varies with the severity of the recession or the policy response to it, or if findings about mortality do not perfectly extend to questions of morbidity, additional research may be necessary to understand the broad array of population health consequences of the Great Recession.
Recessions and Health: Individual-Level Studies
A separate body of research has focused on individual-level health and health-relevant behavioral consequences of recessions. Most studies examine the links between the kinds of events that increase during recessions, such as job losses, unemployment, and the material hardships that result from financial strain, and health outcomes of individuals who experience them. A much smaller set of studies assesses health change in individuals before and after macroeconomic downturns, among those who do and do not experience obvious recessionary shocks to employment, housing, or finances. Selection pressures on experiences such as unemployment may differ during good and bad macroeconomic periods, so the kinds of individuals experiencing recession-type shocks may differ in recessions. In particular, there may be fewer “for cause” job losses during recessions, particularly when entire firms are shuttered. Moreover, the experience and consequences of job losses, housing insecurity, or material hardship could vary depending on the macroeconomic climate because the stigma of these recession-type events may be lower if hardship levels are high across the population, though the strain on buffering networks and resources may also be greater.
Given these caveats about the available individual-level evidence, past studies often find that recession-type events are associated with poorer health for the individuals who experience them. Individual-level studies also assess a wider range of health consequences; a few examine mortality risk, but more examine mental and physical health outcomes that could be affected in the short or longer term, and health behaviors that could lead to health change over time. The most convincing individual-level studies use detailed longitudinal data to control for the stable characteristics of individuals that would differentiate their health regardless of whether the economy was in a downturn. In Figure 2, we illustrate pathways, recession-type events, mechanisms, and behavioral changes hypothesized to result in negative changes in health in individual-level studies.
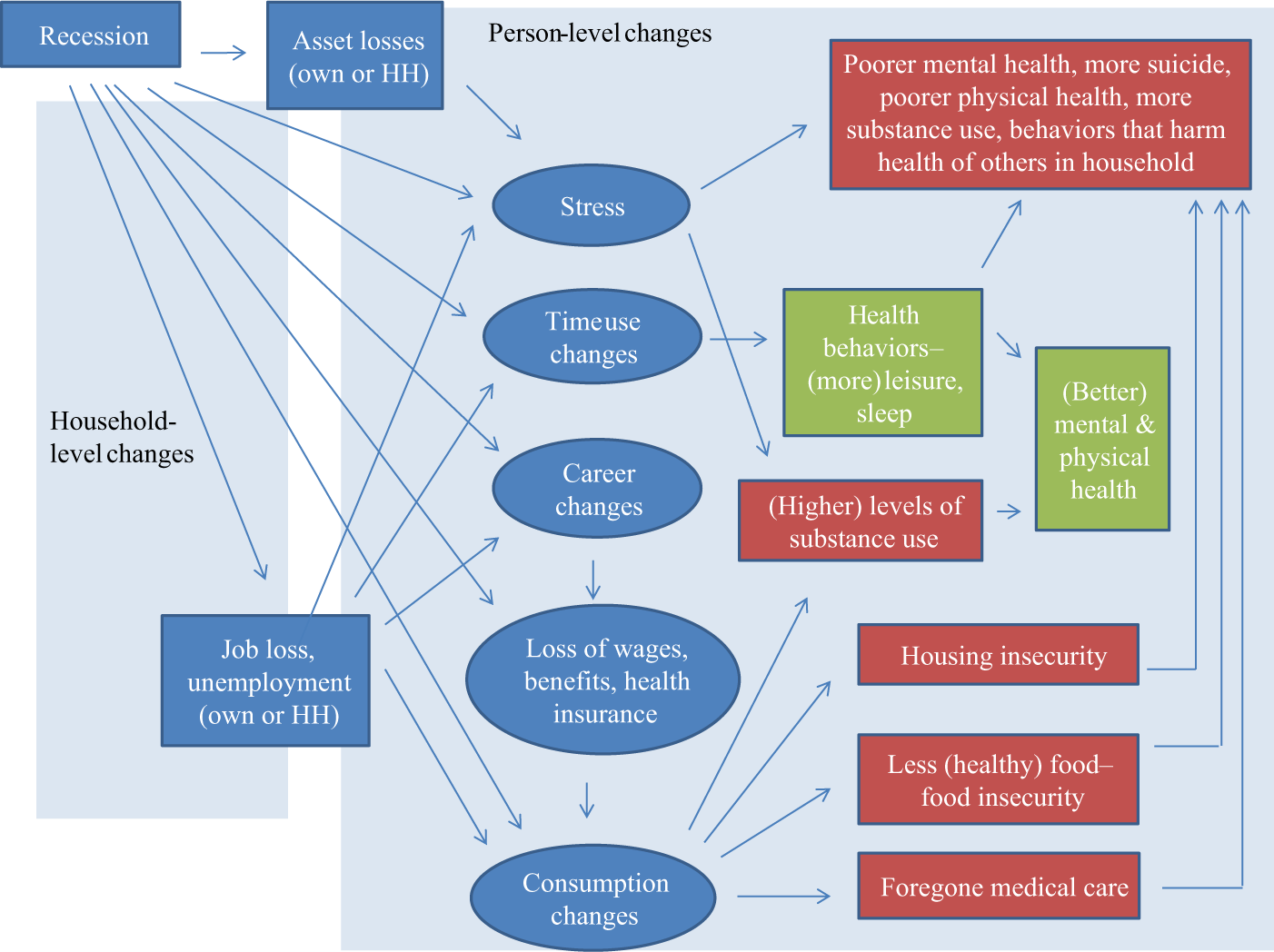
Selected Individual- and Household-Level Hypothesized Pathways Linking Recessions to Health
One of the most central indicators of recessions is a high unemployment rate. A long tradition of research has shown that working-aged people who do not work for pay or are unemployed are less healthy than those in the paid labor force, based on their risk of mortality, self-rated health, and mental health (P. Krueger and Burgard 2011; Rogers, Hummer, and Nam 2000; Ross and Mirowsky 1995). Studies have also shown that U.S. workers who lost jobs through no fault of their own had higher mortality risks in the short and longer term (Sullivan and von Wachter 2009), and were more likely to rate their overall health as fair or poor or to develop new health conditions (Strully 2009).
Researchers propose that negative health consequences of job loss or unemployment are driven by some of the same mechanisms evoked by aggregate-level researchers, such as stress and changes in time use and consumption. Their research tends to find that these mechanisms culminate in worsened health for individuals who experience these events directly. A key mechanism linking exposure to recessionary-type events to poorer health is an increase in stress, which can lead to mental health decrements in the short term and behavioral and physiological changes that become harmful when they persist (Catalano et al. 2011). For example, stressful experiences could increase harmful coping behaviors. One study found that middle-aged Norwegians displaced from their jobs showed worsened cardiovascular health, due almost entirely to increases in smoking (Black, Devereau, and Slavanes 2012). Additionally, considerable research has focused on the links between unemployment or job loss and alcohol use; results are mixed but sometimes show more harmful alcohol use (Catalano et al. 2011).
Another major pathway from job loss or unemployment to health is through changes in material resources that affect consumption. Earnings are the major source of financial resources necessary to purchase health-enhancing goods and services for most workers and their families. Studies have linked unemployment to economic strain that can impact mental health and catalyze an array of secondary stressors (Price, Choi, and Vinokur 2002). In the United States, other essential material resources are also directly tied to employers, including pensions, health insurance coverage, and eligibility for unemployment insurance. Loss of a job can negatively impact current income but also future earnings and benefits accumulation, shaping long-term material well-being and, potentially, health. Moreover, experiencing a recession at a particular life stage could endanger health due to career changes and disruption of existing plans for retirement and economic security. A longitudinal study of older Americans showed that for those who experience a recession in their late 50s, any short-term positive benefits were more than offset by longer-term health deterioration, which resulted in poorer survival prospects (Coile, Levine, and McKnight 2012). The same study did not find health decline for those who were 62 or older, a group eligible for social security benefits, that would mitigate negative impacts on employment and economic stability, health insurance coverage, or ability to retire.
These material losses associated with employment disruptions can change consumption patterns in multiple ways relevant for health. A potentially positive change is lower disposable income for purchasing health-harming goods such as tobacco or fast food. However, most of the spending changes portend poorer health in the short or longer run, particularly if they are sustained. Financial problems stemming from employment disruptions could lead to housing instability—involuntary moves, such as for evictions or foreclosures, or the need to move to less expensive housing—that have been linked in some research to poorer health (Alley et al. 2011; Burgard, Seefeldt, and Zelner 2012; McLaughlin et al. 2012). Financial strain could also increase the likelihood of food insecurity, a risk factor for negative health consequences in the longer term (Alley et al. 2009). Loss of health insurance coverage or financial problems could lead individuals to forgo needed medical care or to skip or split their medication for cost reasons, with potentially harmful consequences for their longer-term health and total health care costs (Catalano 2009). Individuals who experience multiple material hardships of this kind are likely to have the poorest health (Alley et al. 2009), but studies of such cascades of consequences are rare in the context of the Great Recession.
Employment disruption could improve an individual’s health in some ways. As many aggregate-level studies have suggested, people spending less time in paid work have more time for health-enhancing activities, including sleep, exercise, or food preparation, or spending more time with those in their social networks. Evidence suggests that unemployed individuals spend more time in cooking, childcare, and housework, as well as in leisure and sleep (Aguiar, Hurst, and Karabarbonis 2011; A. Krueger and Mueller 2012). However, one study showed that the unemployed are sadder despite their greater leisure time and that their sadness declines on reemployment (A. Krueger and Mueller 2012).
Though the consequences of employment disruption are a central pathway by which recessions can negatively impact individuals’ health, others are also possible. Even in the absence of job loss, for example, older Americans who experienced sudden and substantial wealth losses in the Great Recession were more likely to report depressive symptoms and antidepressant medication use, net of their prerecession characteristics (McInerney, Mellor, and Nicholas 2012). Even the threat of employment or financial insecurity during recessions could have negative health consequences. For example, workers who think they may lose their jobs in the near future, but have not yet been displaced, have worse mental and physical health (Sverke, Hellgren, and Näswall 2002). These findings hold even when adjustment is made for actual job losses or unemployment (Burgard, Brand, and House 2009). Workers undergoing firm restructuring or layoffs, even if not yet displaced, have also shown poorer biomedical indicators such as increases in blood pressure (Ferrie et al. 2002) and worse general health attributable at least partly to perceived job insecurity (Geuskens et al. 2012). Perceived economic vulnerability among individuals nearing retirement also may have been affected by the massive financial volatility of the Great Recession. A longitudinal study of older Australian adults showed that depressive symptoms and anxiety increased in the wake of the Great Recession, more so for those directly financially impacted, but even for those who were not (Sargent-Cox, Butterworth, and Anstey 2011).
While the largest negative impacts of recessions appear to accrue for those who experience job or asset losses, many changes resulting from a recession will affect all individuals, and these broader effects may mimic those hypothesized to underlie the salutary health effects at the aggregate level. Time use could shift to allow more leisure and sleep (Asgeirsdottir et al. 2012; Aguiar, Hurst, and Karabarbonis 2011) and potentially other health-enhancing behaviors. Additionally, a study of the Great Recession showed that Icelanders reduced their health-harming consumption of tobacco, alcohol, daily sweets, weekly fast food, and tanning, likely due to price increases for these activities (Agsgeirsdottir et al. 2012). However, generalized price increases may also have negative consequences for health, as these individuals also reduced consumption of fruits and vegetables. Moreover, a general reduction in working hours or changes in the behavior of employers during recessions could reduce the benefits of all workers, even those who keep their jobs. For example, health insurance coverage for working-aged U.S. men declined in the recent recession, even among those who remained employed (Cawley, Moriya, and Simon 2011).
Individual-level studies sometimes also consider exposures and transfers that occur within households and social networks as a result of one or more members experiencing recession-type events. Job loss or asset losses in the household can affect other members’ health, via the stress that financial hardship puts on relationships (Conger et al. 1990), or because all members’ access to health-enhancing goods is reduced when household income drops. Members of a household or social network may also make financial or time transfers to help those experiencing negative recessionary events. Parents may house or financially support an adult child facing an unexpected unemployment spell, or a spouse may need to increase work hours and assist financially so that her or his partner can pay down debt accumulated due to the loss of health insurance coverage, for example. In these cases, a job loss or loss of benefits to someone in an individual’s network could generate stress and endanger that individual’s own health if it changes her or his own spending on health-relevant resources. Time transfers could also affect the well-being of the providers as much as the recipients; an individual spending more time in paid work because of another household member’s job loss, for example, may have less time to care for his or her own health.
Limitations of individual-level evidence and future directions
The extant individual-level evidence generally provides support for an association between recessions and poorer health, primarily for those who experience employment disruptions or asset losses, but there is room for further research. We focus on some key limitations here and provide empirical examples to illustrate. Generally, prior studies have focused on job loss or unemployment as the primary exposures but have not traced the pathways through mechanisms of stress, time use changes, and consumption changes. Most prior studies have not considered the more proximate material hardships that could link individuals’ decisions in the face of recessionary events to eventual declines in health. A better understanding of the short- and longer-term chains of events that link recessionary experiences to changes in individuals’ health would strengthen inferences about these connections and guide interventions to mitigate negative consequences.
The need to trace individuals’ responses to recessionary events
Individual-level research on recessions and health could be more attentive to the ways that individuals respond to recessionary shocks with changes in their time use or consumption of health-related goods and services. How do they reduce their spending, for example, and is there a broad change in consumption behavior or are only those who experience recessionary events changing their behavior? Or are those who experience financial strain regardless of the business cycle accounting for the bulk of consumption changes in recessions—does chronic poverty explain any associations we might find?
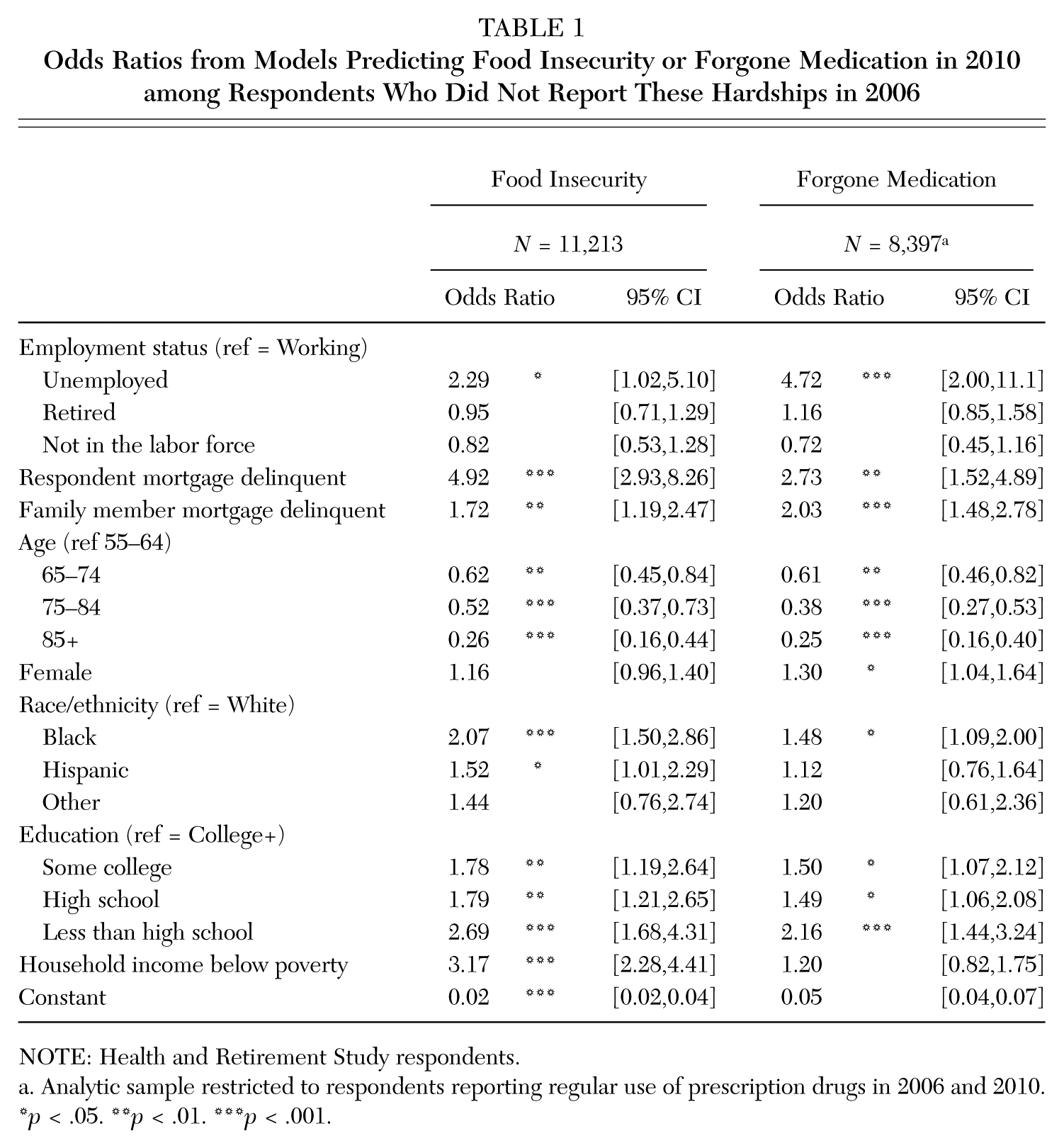
To illustrate how we might assess the impact of recessionary events on spending decisions, we examined food insecurity and foregoing medication among older adults, assessing changes from the pre– to the post–Great Recession period and examining how unemployment or mortgage delinquency may have affected these outcomes. We used a large sample from the Health and Retirement Study (HRS), an ongoing, nationally representative sample of U.S. adults over age 50 initiated in 1992. Details about the sample and methods for this and all analyses can be found in the appendix. These analyses assessed whether unemployment in 2008 or mortgage problems between 2008 and 2010 predicted food insecurity or forgone medication in 2010. We assessed both the respondent’s own mortgage delinquency and any mortgage delinquency of a family member to assess how even events in an individual’s close personal network could affect his or her consumption behaviors. We also eliminated from consideration those who reported recent food insecurity (for the first regression model) or forgoing medication recently (for the second model) in 2006, to address the possibility that these behaviors in 2010 were driven by individuals who had a long-standing material hardship on these dimensions. Assessments of forgone medications were limited to individuals reporting regular use of prescription drugs in 2006 and 2010.
Table 1 presents odds ratios and 95 percent confidence intervals for logistic regression models. We find that unemployment and own or a family member’s mortgage delinquency are independently associated with significantly higher odds of these material hardships, and that the associations are robust to adjustment for poverty status and other measures of social advantage. Among otherwise average individuals, our models predict that about 21 percent of those behind on their own mortgage would experience new food insecurity, compared to only 3 percent of those who were not behind on their mortgage. Similarly, predicted new food insecurity is 7 percent among those with family members experiencing mortgage delinquency, compared to 3 percent among those without these mortgage problems in their family. While causal inference is always threatened in observational studies by unmeasured individual characteristics and other problems, these results illustrate the value of panel data that can help to trace within-person changes and the paths from recessions, to employment and housing shocks, to behavioral changes that could have health consequences.
Odds Ratios from Models Predicting Food Insecurity or Forgone Medication in 2010 among Respondents Who Did Not Report These Hardships in 2006
NOTE: Health and Retirement Study respondents.
Analytic sample restricted to respondents reporting regular use of prescription drugs in 2006 and 2010.
p < .05. **p < .01. ***p < .001.
More consideration of material hardship experiences as mediators
In prior individual-level studies, there has been relatively little attention to the ways recession-type events lead to material hardships that may have proximal links to poor health outcomes. For example, unemployment could lead to financial problems and strain, causing spending changes for those without the resources to weather income losses. Spending changes could manifest as housing instability, food insecurity, or forgone medical care, but few studies have examined how these material hardships may help us to understand subsequent health decrements (but see Alley et al. 2011). We used the Michigan Recession and Recovery Study (MRRS), a representative sample of 19- to 64-year-old residents of the metropolitan Detroit area, to explore some of these associations. We examined four types of material hardship that had occurred in the past 12 months as potential links between experiences of the Great Recession and short- and medium-term health outcomes. These included financial problems (i.e., behind on utility bills, used a payday lender, etc.), housing instability (i.e., behind on rent or mortgage, doubled up to share expenses, etc.), food insecurity, and forgoing needed medical or dental care for cost reasons. We assessed whether these material hardships, measured at baseline in late 2009, were associated with poorer health in 2011, using criteria for major or minor depressive symptoms and reporting poor or fair self-rated health.
We assessed the associations between material hardships and subsequent health in three steps: (1) with adjustment for baseline age, gender, and race; (2) with these adjustments and after eliminating respondents with the given health condition at baseline, to reduce the possibility that prior health predicted material hardship or later health; and (3) with adjustments, after eliminating those with the focal condition at baseline and after eliminating those who were not employed in every month between January and November of 2007, the period immediately prior to the official start of the Great Recession. Step three helps to address the possibility that an individual’s employment problems and material hardship preceded the recession.
Table 2 shows the odds ratios and 95 percent confidence intervals associated with the four types of material hardship from models predicting each health outcome. Each material hardship was assessed in separate logistic regression models. Step one results suggest strong associations between these material hardships and both health outcomes, even after adjusting for age, gender, and race differences in risk at baseline. Step two results show that in many cases, those who had experienced material hardship in the year before baseline were already experiencing poorer health at baseline. Many of the associations with health at follow up were no longer significant after we removed respondents who reported the focal health outcome at baseline. This is a conservative step, since their baseline health could have reflected short-term impacts of recent material hardship. However, associations between recent housing instability and food insecurity at baseline and health at follow up were still statistically significant, providing stronger evidence than is available in cross-sectional studies. Step three results suggest that some of these associations remain strong and significant even when we eliminate individuals from consideration if they had any unemployment in the year prior to the Great Recession, leaving a relatively select group of individuals who may or may not have gone on to experience employment or income shocks. Among otherwise similar respondents who were not depressed at baseline and had not experienced any unemployment in the year before the recession, our models predict that about 11 percent of those experiencing housing instability would report fair or poor self-rated health, compared to only about 2 percent of those who did not. Similarly, predicted new depression is 13 percent among those with food insecurity at baseline, compared to 4 percent among those without food insecurity. The findings from these two empirical illustrations show how considering spending changes and material hardships that arise in recessions can improve understanding of the proximal pathways through which recessions impact individuals’ health, which might be targets of intervention, and what kinds of individuals are at risk.
Odds Ratios from Models Predicting Depressive Symptoms or Self-Rated Health in 2011, Considering Different Material Hardships and Levels of Adjustment
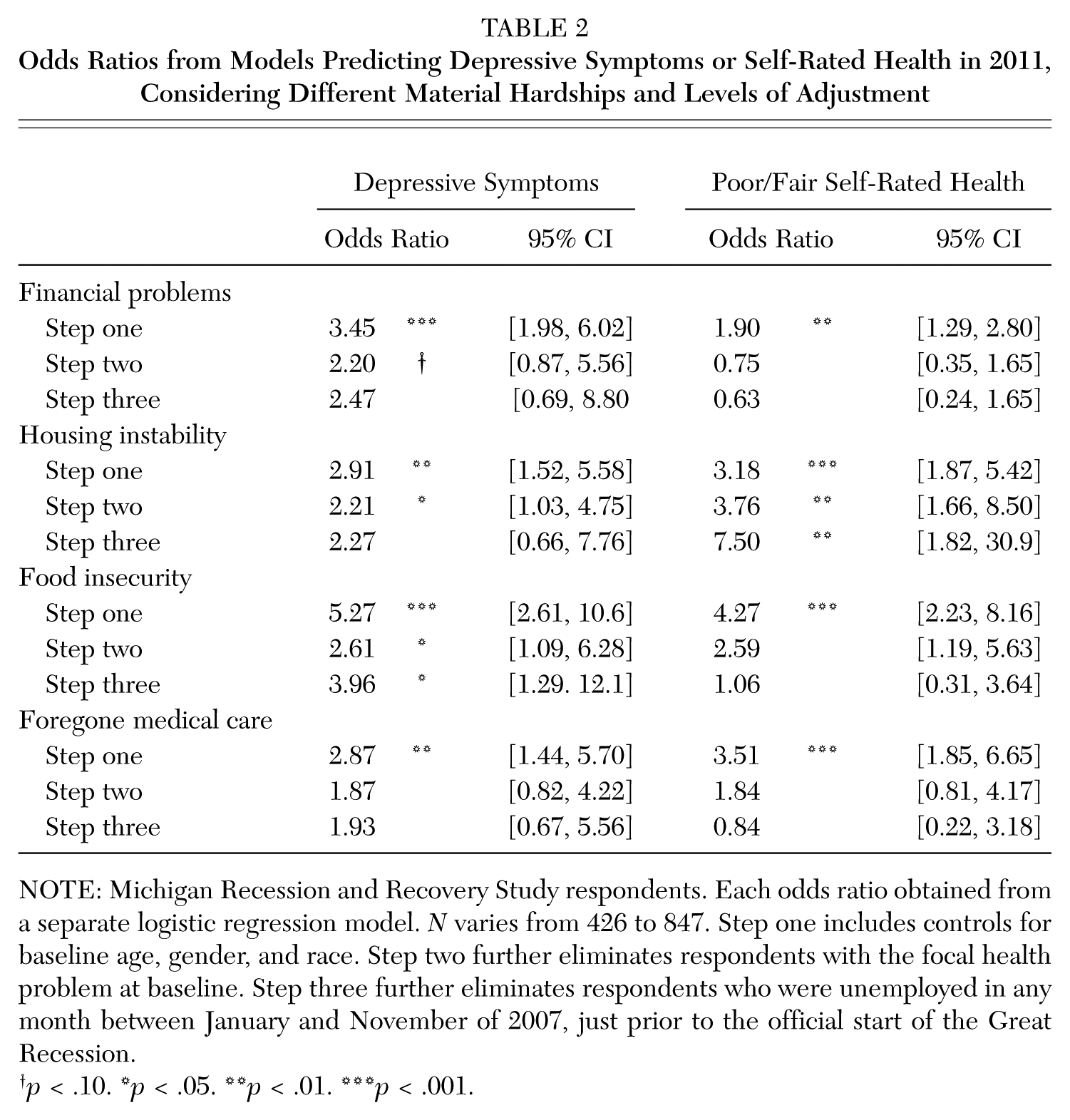
NOTE: Michigan Recession and Recovery Study respondents. Each odds ratio obtained from a separate logistic regression model. N varies from 426 to 847. Step one includes controls for baseline age, gender, and race. Step two further eliminates respondents with the focal health problem at baseline. Step three further eliminates respondents who were unemployed in any month between January and November of 2007, just prior to the official start of the Great Recession.
p < .10. *p < .05. **p < .01. ***p < .001.
Implications of the Great Recession for Health and Health Disparities
What are the potential consequences of the Great Recession for health?
The countervailing findings of health-enhancing consequences at the aggregate level versus harmful consequences of recessionary events at the individual level combine to create the overall health effects of recessions. Based on evidence from prior recessions, the number of individuals whose health is harmed by recessions is likely to be exceeded by the larger group who reap benefits, even if those positive benefits are weaker for any given individual than the health costs of, say, a long-term spell of unemployment (Riva et al. 2011; Tapia Granados 2005). The total health consequences of the Great Recession are still to be uncovered, as we await detailed cause of death data and longitudinal data collections into the coming years. However, patterns of aggregate- and individual-level effects observed during previous recessions are likely to be similar in the wake of the Great Recession. That is, we expect some reduction in overall mortality, as suggested by early findings based on mortality data through 2009 (Tapia Granados 2012) but potentially substantial costs to health and well-being for those who were affected personally by employment, income, and wealth shocks, perhaps worse than costs of recent, weaker economic downturns.
What are the implications for health disparities?
Recessions could increase or decrease existing social disparities in health, depending on the relative balance of aggregate positive effects and individual-level negative effects and contingent on the concentration of recessionary shocks among the socially disadvantaged. The Great Recession could widen existing disparities between the economically advantaged and disadvantaged, given the length and depth of the recession and slow recovery, which could lead to more cascades of hardships for those finding it difficult to smooth their spending. Moreover, less advantaged groups probably benefit less from the positive consequences of the recession; they are already less likely to be working long hours than more educated individuals, and thus the slackening of the economy probably does not afford them substantial extra time for health-enhancing behaviors or the resources to engage in them, for example.
Past studies have suggested that socioeconomic status is an important modifier of the aggregate-level association between recessions and mortality, with the less advantaged accruing fewer of the benefits of procyclical mortality (Edwards 2008; Stuckler et al. 2012). Some have argued that mortality may be procyclical in the aggregate, particularly for the socially advantaged, but possibly countercyclical for the socially disadvantaged (Edwards 2008). Some aspects of the Great Recession were particularly harmful for more advantaged groups, though, such as shocks to financial assets not commonly held by the disadvantaged (McInerney, Mellor, and Nicholas 2012).
The Great Recession also may have heterogeneous influences by age, gender, and country or region of residence (Riva et al. 2011). Age-specific associations between recessions and health that have been discussed more in aggregate-level studies probably extend to the individual level as well, whether because of differential distributions of some recessionary shocks or different implications of these for health. For example, many older Americans have paid off their mortgages and are not vulnerable to foreclosure (unless by way of family members’ struggles), but they may face difficulty affording all needed medical care before they become age-eligible for Medicare. Working-aged individuals, on the other hand, are more vulnerable to employment volatility and its consequences. Aggregate-level studies that consider gender disparities in the link between recessions and health also suggest that men fare worse in terms of both mortality (Edwards 2008; Ruhm 2000) and mental health (Katikireddi, Niedzwiedz, and Popham 2012).
Some research suggests that the policy environment has implications for the general associations between recessions and health, and for the magnitude of heath disparities. Prior evidence suggests that health effects of recessions are likely to be larger in the United States than in other advanced economies for some outcomes, including infant mortality (Gerdtham and Ruhm 2006; Neumayer 2004), because Americans are less healthy than residents of other wealthy countries, and stronger welfare state policies in those nations tend to buffer against major swings in individuals’ hardship or behaviors. For example, older U.S. workers who lose their jobs have poorer cardiovascular outcomes (Gallo et al. 2006), while such associations are not found in Northern European workers who have access to better social and financial services following job loss (Catalano et al. 2011). This suggests that policy reforms in the United States, such as the 2010 Affordable Care Act or extensions to programs designed to reduce food insecurity, might help to mitigate some of the negative individual-level and inequality consequences of the Great Recession.
Footnotes
Appendix: Data and Methods
Sarah A. Burgard is an associate professor of sociology and epidemiology and research associate professor at the Population Studies Center at the University of Michigan. She studies how stratification by race/ethnicity, gender, and socioeconomic position affect population health. She is currently conducting data collections and projects that examine links between the Great Recession and population health.
Jennifer A. Ailshire is a postdoctoral fellow in the USC/UCLA Center for Biodemography and Population Health at the University of Southern California (supported by NIH/NIA Grant K99 AG039528). Her research focuses on neighborhood context, social relationships, and health and well-being over the life course.
Lucie Kalousova is a doctoral student in the departments of Sociology and Health Management and Policy at the University of Michigan. Her research focuses on social stratification and mobility, health disparities, and comparative social policy.