
Abstract
The federal Supplemental Security Income (SSI) program is an important part of the safety net in the United States, paying means-tested benefits to children with disabilities, nonelderly adults with disabilities, and elderly individuals. In this article, we describe the eligibility criteria for the program, how these have changed over time, and the impact of these changes on SSI enrollment. We also show that over time, SSI has grown to serve a heterogenous population, with an array of life experiences and needs. In this context, we discuss potential reforms intended to modernize the program and increase its ability to achieve its goals. These include a proposal to raise the generosity of benefits for elderly SSI recipients, increase the incentive to work among nonelderly adult SSI recipients, and harmonize disability decision-making across medical examiners and administrative law judges.
Supplemental Security Income (SSI) is a national means-tested transfer program for aged, blind, and disabled individuals with low incomes and assets. The federal SSI program was enacted in 1972 and began paying cash benefits in 1974, replacing a patchwork of state-run entitlement programs that were created under the Social Security Act of 1935 and its subsequent amendments in 1950. The establishment of SSI was the culmination of a four-year debate over a more ambitious welfare reform proposal—the Family Assistance Plan (FAP)—that was intended to extend the federal social safety net to all low-income Americans. While Congress eventually rejected the universality of FAP, it passed SSI, a categorical welfare program based on the same negative income tax principles as FAP but targeted on a much smaller subset of low-income individuals who were not expected to work—the aged, blind, and disabled. 1
SSI is funded by the federal government and administered by the federal Social Security Administration (SSA), following federally determined income, asset, and medical eligibility criteria (for those with disabilities). Benefits are set at the federal level and rise each year with inflation (using the Bureau of Labor Statistics Consumer Price Index). States are allowed to provide supplemental funding for SSI benefits, with all but four states supplementing the federal benefit for some or all of their SSI beneficiaries. In eleven states and the District of Columbia, the federal government administers state SSI supplements (SSA 2018c). In the other thirty-five states, SSI supplements are paid directly by state governments to SSI recipients. 2
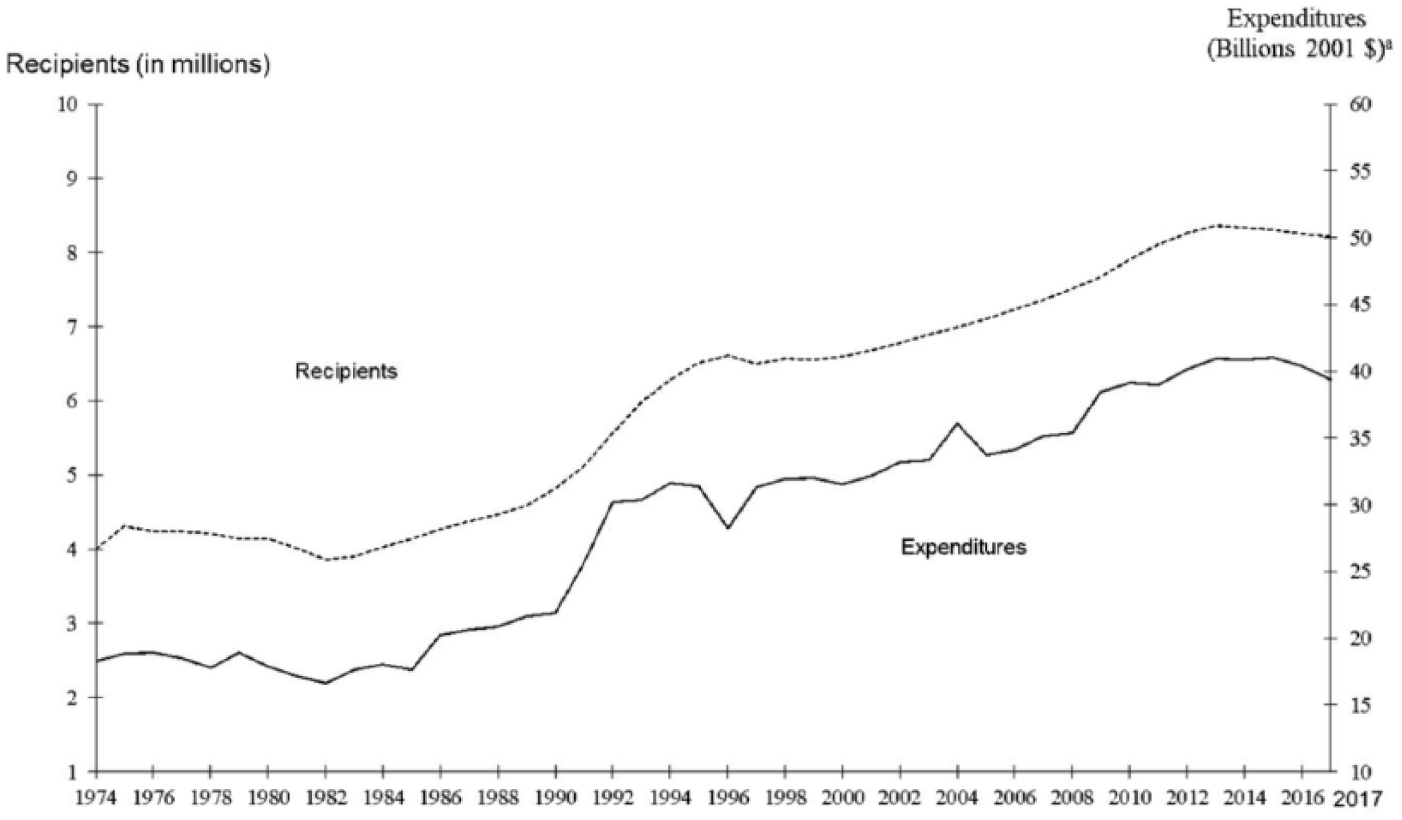
SSI began as a relatively small program providing benefits to a largely elderly population. For example, in 1974, more than 60 percent of the program’s 4.0 million beneficiaries were aged 65 and up. Since that time, SSI has grown to be one of the largest federal means-tested cash assistance programs in the United States, with a caseload that is now dominated by children and working-age adults with disabilities. 3 In December 2017, 8.2 million people—the vast majority under age 65—received federal SSI benefits. Total SSI benefits paid in 2017 exceeded $54 billion, reflecting an average annualized benefit of about $7,000. Figure 1 shows trends in program enrollment and expenditures since SSI’s inception in 1974. Total SSI expenditures are comparable to spending on the Earned Income Tax Credit (EITC) and Supplemental Nutrition Assistance Program (food stamp program) and substantially larger than the amount spent on the Temporary Assistance to Needy Families (TANF). An additional $127 billion was paid for SSI recipients’ health insurance through the Medicaid program in 2014. 4
SSI Program Growth, 1974–2017
Rapid program growth, the changing composition of SSI beneficiaries, and increasing pressure to better integrate traditional “nonworkers” into the labor market all have raised questions about the role that SSI plays in the broader U.S. social welfare system. While there have been various attempts to improve the economic outcomes of SSI recipients over time, for example, by encouraging current SSI recipients to return to work or by assisting child SSI recipients in transitioning off the program and into gainful employment in adulthood, SSI remains an absorbing state for most recipients. In other words, once individuals go on the SSI program and begin to draw benefits, relatively few will later exit the program to work.
In this article, we review the evolution of the SSI program, the determinants of caseload growth, and the evidence about its impacts on the targeted populations. We conclude with potential policy reforms. The article proceeds as follows. In the next section, we review the basic eligibility criteria for the program, and how some of those criteria have evolved over time. Then we describe trends in SSI caseloads and discuss their determinants. We go on to present a brief review of the economic issues associated with the program design and discuss the evidence regarding the impact of SSI on the targeted populations. Finally, we use what we have learned from the preceding sections to present reform ideas for SSI, and we end with conclusions.
SSI Eligibility Criteria
SSI is an income support program that provides benefits to three distinct low-income populations: the aged, the blind, and the disabled. As such, SSI eligibility is a function of three program-based categorical criteria—age, disability, or blindness—as well as more general requirements associated with income and asset limits and citizenship and residency rules. The SSA is responsible for screening applicants and making awards for SSI. Table 1 summarizes the SSI eligibility requirements that are described in detail in the remainder of this section.
SSI Eligibility Requirements in 2019
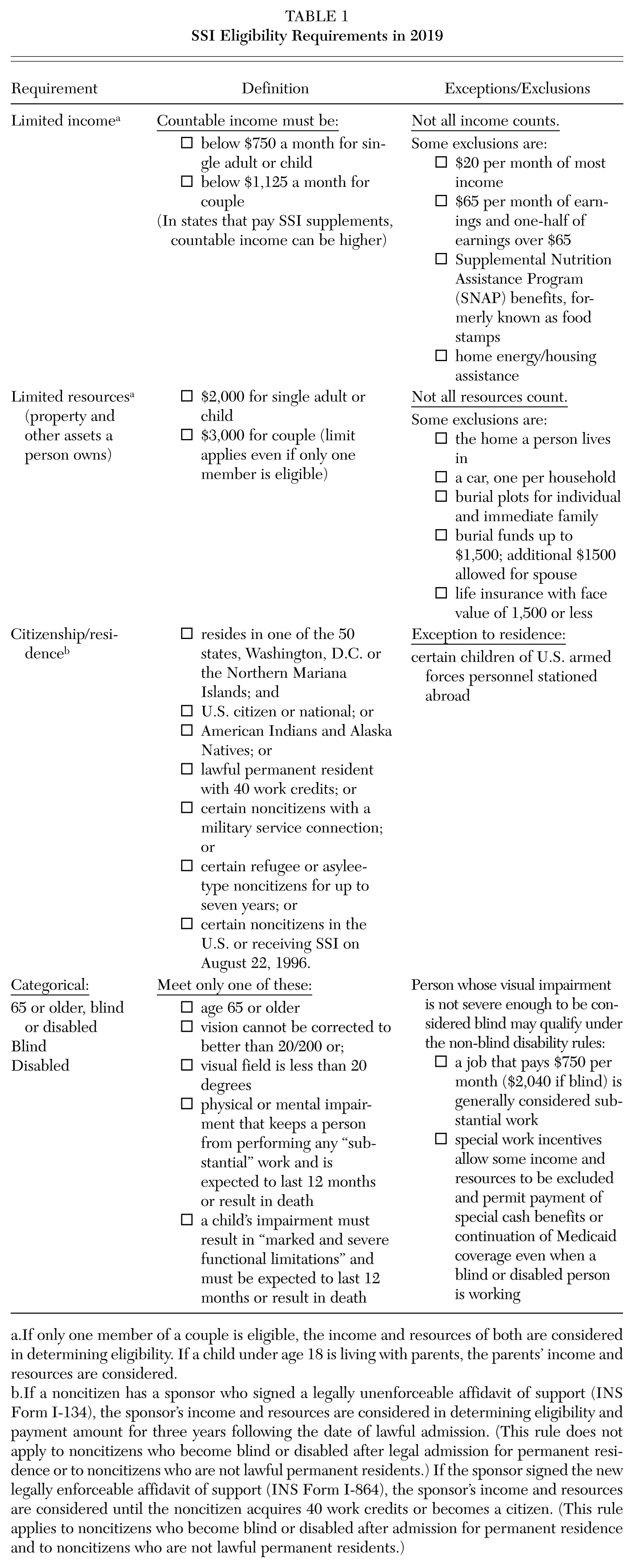
If only one member of a couple is eligible, the income and resources of both are considered in determining eligibility. If a child under age 18 is living with parents, the parents’ income and resources are considered.
If a noncitizen has a sponsor who signed a legally unenforceable affidavit of support (INS Form I-134), the sponsor’s income and resources are considered in determining eligibility and payment amount for three years following the date of lawful admission. (This rule does not apply to noncitizens who become blind or disabled after legal admission for permanent residence or to noncitizens who are not lawful permanent residents.) If the sponsor signed the new legally enforceable affidavit of support (INS Form I-864), the sponsor’s income and resources are considered until the noncitizen acquires 40 work credits or becomes a citizen. (This rule applies to noncitizens who become blind or disabled after admission for permanent residence and to noncitizens who are not lawful permanent residents.)
Because SSI is a means-tested program, all applicants must meet basic income and asset tests. Applicants over the age of 65 who meet these tests automatically qualify for SSI benefits. Individuals also may receive SSI benefits for the blind if they have 20/200 (or worse) vision with the use of a correcting lens in their better eye, or if they have tunnel vision of 20 degrees or less (SSA 2018e). The criteria for nonelderly adults and children with disabilities are stricter and are subject to more judgment among evaluators. Below, we describe the process of disability determination for both nonelderly adults and children applying for SSI disability benefits.
Disability determination for nonelderly adults
Nonelderly adults apply for SSI benefits through one of the approximately twelve hundred SSA field offices in the United States. 5 SSA employees determine whether each applicant meets nonmedical requirements, including that he or she has sufficiently low income and assets. If monthly earnings exceed SSA’s definition of substantial gainful activity (SGA), the applicant is deemed categorically ineligible. 6
Applications that meet these financial criteria are then forwarded on to a state agency, where the disability determination process is typically carried out by a two-person team (Duggan, Kearney, and Rennane 2016). The first person is a state disability examiner, who assembles both medical and nonmedical evidence and requests a consultative exam when the medical evidence is not sufficient to make a disability determination. The examiner also prepares (or assists in preparation for more complicated cases) an assessment of the applicant’s residual functional capacity. The second person on the team is a medical consultant who reviews the available medical evidence provided by the applicant and acquired through one or more additional consultative exams. The examiner prepares the paperwork for the final determination, which is subsequently signed by the medical consultant.
To qualify for SSI benefits, a nonelderly adult applicant must provide evidence of a medically determined physical or mental disability that limits her or his ability to engage in substantial gainful activity. Furthermore, the applicant must demonstrate that this condition will persist for at least 12 months or will result in death. If the condition passes a severity threshold and is on SSA’s list of medical impairments, then the applicant has passed the disability determination. If the impairment is not on this list, then SSA considers whether the applicant can perform labor market tasks that she or he previously performed. If this is possible, then the applicant is found ineligible. If the applicant is unable to do past work, then the disability examiner considers whether there are other occupations in the economy that she or he could perform. In this case, the examining team considers not only the applicant’s medical condition but also her or his age, education, and work experience. 7
The medical eligibility criteria used by the SSI program do not vary across states and are the same as those used by the Social Security Disability Insurance (SSDI) program. Previous research has shown that there is variation across geographic areas in award rates, as one would expect if the applicant pools varied across states (Gruber and Kubik 1997). Furthermore, the disability determination is made by individual examiners and will inevitably involve some subjective judgments. Indeed, recent research (Maestas, Mullen, and Strand 2013) has shown that there is substantial variation across examiners in disability award rates even after controlling for the characteristics of applicants.
Applicants who are rejected on this “first round” may appeal the decision, which is considered by a second team of examiners. More than half of individuals rejected at the first round do file an appeal. Applicants denied on this second round then have the option to appeal to an administrative law judge (ALJ), and approximately 80 percent of those rejected at stage two do this. The assignment to ALJs is “essentially random” (Daub et al. 2006) and is determined based on the field office where the application was initially made (French and Song 2014). At this stage, the applicant is often joined by a lawyer or some other representative when appearing before the ALJ. One striking feature of these hearings is that only one side is represented—the SSA does not have representation to explain the reason for the initial decisions. Recent research has shown significant variation in award rates at this stage as well (French and Song 2014). Applicants denied at this second appeal can try again by appealing to the Social Security Appeals Council and then one more time to their district court.
During the past 10 years, accounting for decisions at all stages of the process including appeals, between 45 and 50 percent of nonelderly adult SSI applicants with a medical decision have been awarded benefits (SSA 2018a). 8 The average time from the initial application to the first decision is four months, while those appealing to the ALJ level or higher typically wait more than two years for the decision (Office of the Inspector General [OIG] 2008).
Disability determination for children
Screening children for SSI eligibility is in some respects even more complex than adult disability screening. Under the original legislation, Congress wrote that a child should be considered disabled if “he suffers from any medically determinable physical or mental impairment of comparable severity” to a disabling impairment in an adult (SSA 1997). In practice, children originally qualified for SSI if they had “a medically determinable physical or mental impairment which results in marked and severe functional limitations, and which can be expected to result in death, or which has lasted or can be expected to last for a continuous period of not less than 12 months.” Between 1974 and 1989, the child disability determination process did not include a functional assessment or take into account the equivalent of adult vocational factors.
This changed in 1990 when the Supreme Court decided the case of Sullivan v. Zebley (493 U.S. 521 [1990]). The Court ruled that to meet the standard of equal treatment, a functional limitation component parallel to that of adults must be included in the initial disability determination process for children. In response, in 1990, SSA added two new bases for finding children eligible for benefits: (1) functional equivalence, which was set at the medical listing level of the disability determination process; and (2) an individual functional assessment (IFA), which was designed to be parallel with the functional and vocational assessment provided for adults. By allowing applicants who did not meet the medical listing to be found disabled if their impairments were severe enough to limit their ability to engage in age-appropriate activities, such as attending school, the IFA relaxed the eligibility criteria for children to be eligible for SSI benefits (U.S. General Accounting Office [GAO] 1994, 1995).
During the several years after this 1990 Supreme Court decision, SSA’s use of the IFA, along with the new criteria that emphasized functioning when determining mental disabilities, led to a large expansion in the number of children determined to be categorically eligible for SSI. Many of these children had less severe disabilities than did those children awarded SSI benefits in the 1970s and 1980s. In the years prior to the Supreme Court decision, the number of children receiving SSI benefits was growing by about 3 percent per year and stood at 264,000 in 1989. In the seven years following the decision, the number of children on SSI rose to 955,000, an increase of 260 percent from 1989 to 1996. During this same period, the share of children receiving SSI benefits more than tripled from 0.4 percent to 1.4 percent (Duggan and Kearney 2007).
Perhaps partly because of this rapid growth in SSI enrollment, Congress changed the SSI eligibility rules for children as part of its well-known 1996 welfare reform legislation. The new regulations no longer used an individual functional assessment but retained the spirit of the functional limitation notion. To be found categorically eligible, a child had to demonstrate “a medically determinable physical or mental impairment or combination of impairments that causes marked and severe functional limitations, and that can be expected to cause death or that has lasted or can be expected to last for a continuous period of not less than 12 months” (SSA 2008). As a result of this change, nearly 100,000 children were terminated from the program in 1997, and the share of children receiving SSI remained steady at 1.2 percent from late 1997 through 2000. The new regulations also required children who reached the age of 18 to be evaluated again to determine whether they would continue to receive SSI benefits as adults.
The current determination process for children to receive SSI benefits is significantly less restrictive than it was before the Sullivan v. Zebley Supreme Court decision (493 U.S. 521 [1990]) but somewhat more restrictive than it was during the early 1990s (Berkowitz and DeWitt 2013; Wittenburg 2011; Wiseman 2010). SSI enrollment among children has risen substantially among children since 2000, with 1.6 percent of children receiving SSI benefits in 2017. 9
The changes in child disability determination since the early 1990s has meant that a child’s disability status is frequently determined by a subjective determination about performance in school, relative to age-appropriate peers. This has led to concerns that the program eligibility criteria may lead to an increase in diagnosing children with learning or behavioral disabilities, potentially leading to inappropriate medical treatment (Wen 2010; Wittenberg 2011). Recent research, while far from definitive, is consistent with this hypothesis. Leckman-Westin et al. (2018) found that children receiving SSI benefits due to a mental disorder were twice as likely as other children to be treated with higher-than-recommended dosage amounts of antipsychotic medications. 10
SSI Program Caseloads
To make meaningful suggestions for improving SSI it is important to understand the characteristics of program beneficiaries. In this section, we describe the evolution of SSI caseloads, paying particular attention to participation among the three targeted populations. We also consider variation in program usage across states and for nonelderly adults and children with disabilities—the diagnoses that ultimately qualified them for the program.
As noted previously, SSI enrollment has grown substantially since the program’s inception. Figure 2 shows that the composition of the program has also changed. The number of elderly recipients has remained relatively constant at approximately 2.1 million during the entire life of the program. In contrast, the number of children and nonelderly adults has more than tripled, from 1.9 million in 1983 to 6.0 million by 2017. 11 As a result, elderly (aged 65 and up) beneficiaries currently account for less than 30 percent of all SSI recipients, compared to 60 percent in 1974.
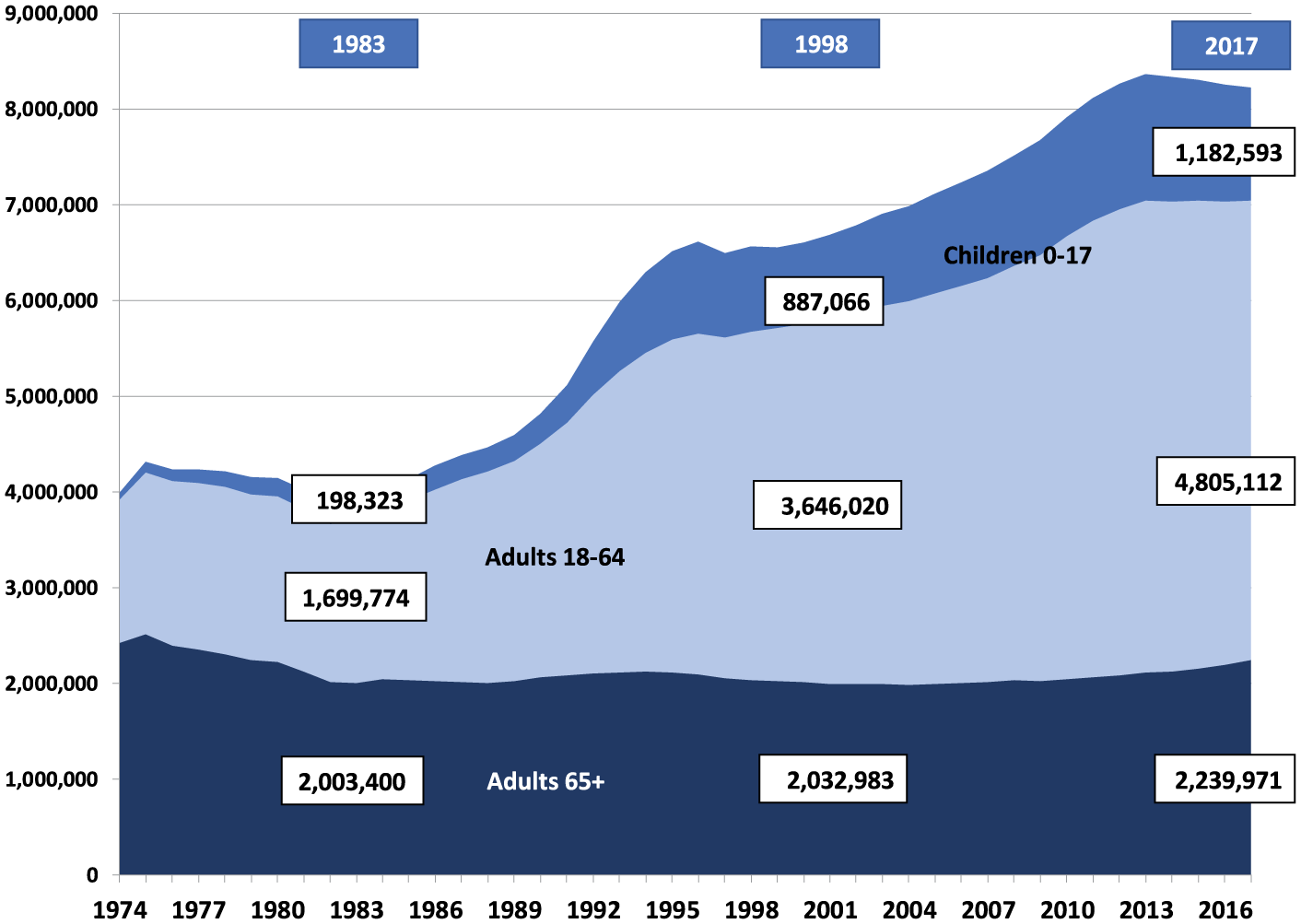
SSI Caseload Trends, 1974–2017
As a result of these trends, the fraction of elderly individuals receiving SSI benefits has steadily fallen over time, from 7.0 percent in the early 1980s to just 4.4 percent in 2017. In contrast, the fraction of nonelderly adults receiving SSI has risen substantially (from 1.5 to 2.4 percent over the same period) and by even more among children (from 0.4 to 1.6 percent).
For the elderly, the decline in SSI enrollment relates to increased coverage under the Social Security (Old Age, Survivors, and Disability Insurance, or OASDI) program. Part of SSI’s original goal was to supplement OASDI benefits for low-income individuals and households or to provide a minimum benefit for those individuals and households not eligible for Social Security benefits. As enrollment in OASDI has risen, the need for the SSI elderly program has declined. OASDI benefits are indexed to average wage growth in the economy. As OASDI benefit amounts have increased, the gap between the SSI supplement amount and OASDI has closed thereby reducing the need for the SSI supplement.
For nonelderly adults and children with disabilities, growth in the number of recipients reflects material changes, as we discussed, that relaxed the medical eligibility criteria and made it easier to qualify for SSI benefits relative to earlier periods.
As the next three figures reveal, the fraction of people enrolled in SSI varies substantially across states, ranging from a low of 1 percent in North Dakota to a high of more than 5 percent in West Virginia. 12 Some of this is accounted for by differences across states in income levels and in health, for which we do not attempt to adjust in the figures that follow.
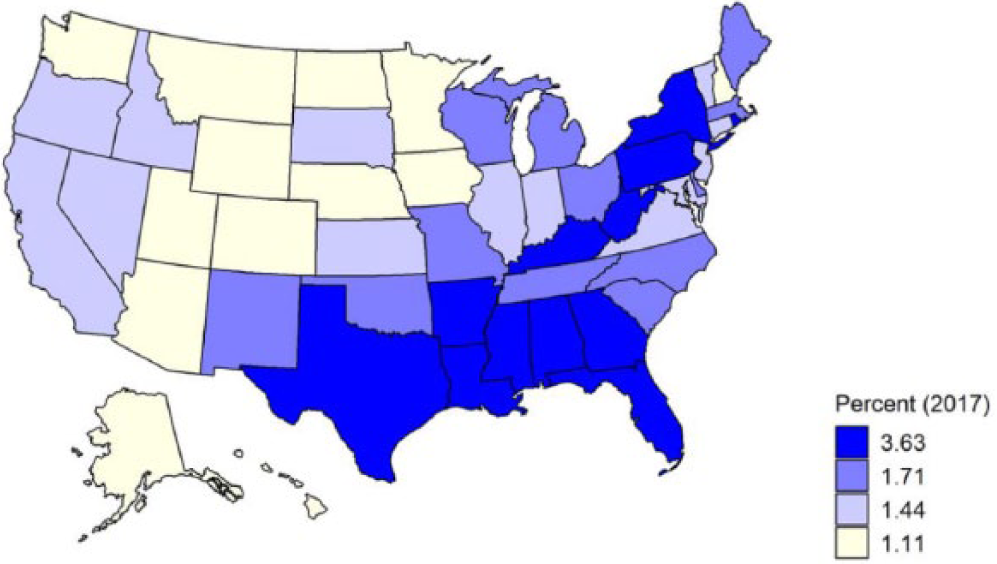
Figures 3 through 5 group states into quartiles of the targeted group’s SSI participation rate distribution. Figure 3 shows that among the nonelderly adult SSI population, states with the highest rates of SSI enrollment tend to be in the South, while many of those with relatively low enrollment are in the West. Participation in the child SSI program also exhibits substantial geographic variation, as displayed in Figure 4. While most of the states with high adult SSI participation also have high child participation, there are some differences. For example, while Texas is in the top quartile of child SSI participation, it is below the median for nonelderly adult SSI participation. The elderly caseload—mapped in Figure 5—has a similar range and geographic pattern with the exception of two outliers: California and New York. In these two states, the elderly SSI caseload was approximately 13 and 9 percent of the total elderly population, respectively, which are the two highest state-specific enrollment rates. This likely reflects the more generous supplementation of SSI benefits in these states so that Social Security benefits are less likely to fully phase out the SSI benefits.
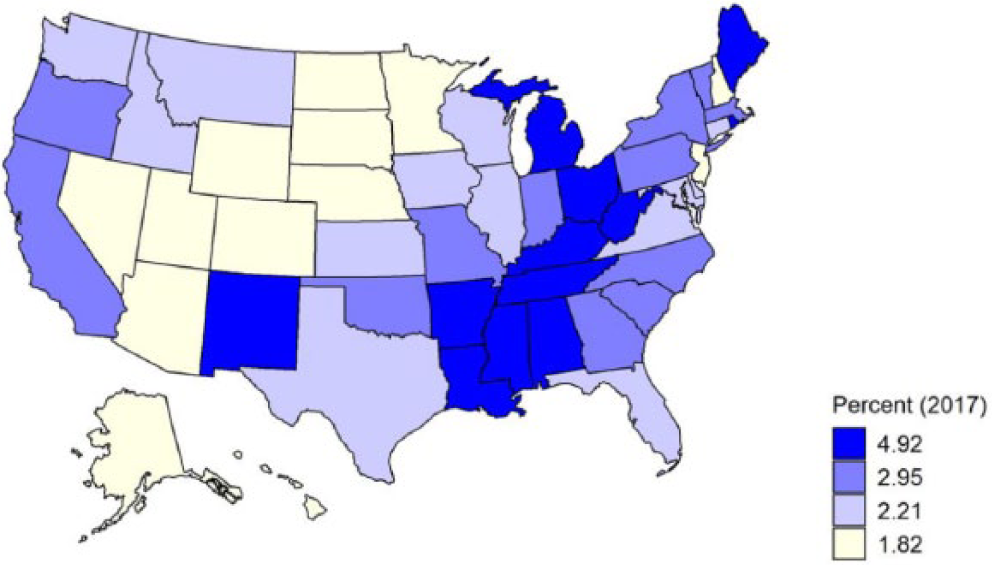
Nonelderly Adult SSI Population as Percentage of State Adult Population, 2017
Child SSI Population as Percentage of State Child Population, 2017
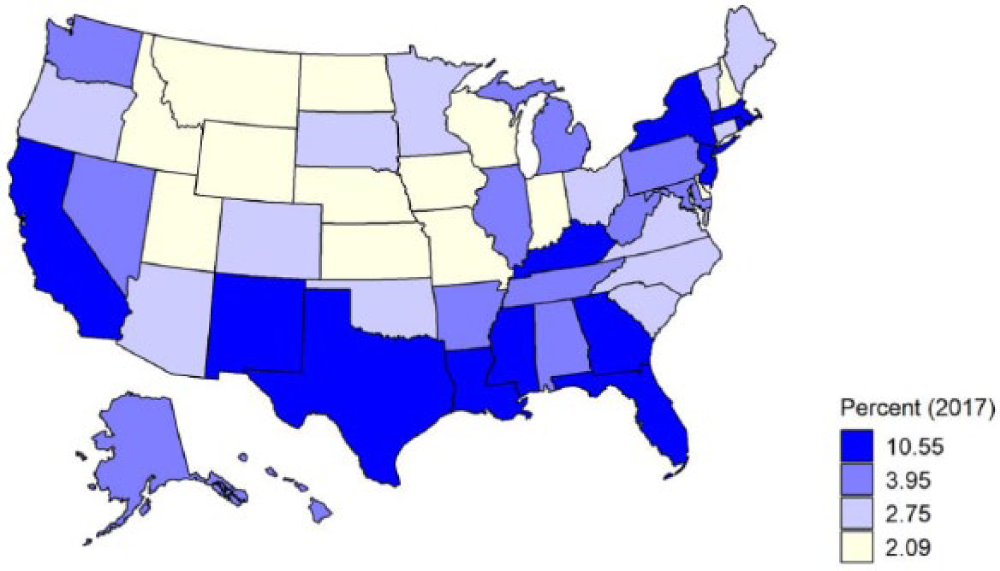
Elderly SSI Population as Percentage of Elderly Adult Population, 2017
Another important aspect of the SSI program for the nonelderly adult and child populations is the composition of qualifying diagnoses. As shown in Figure 6, this varies considerably across the age distribution. The figure plots the percentage of recipients who qualify for the program based on a physical impairment. The data reveal a u-shaped pattern in qualifying diagnoses. A majority of the youngest and oldest beneficiaries become eligible primarily on the basis of a physical disability—nearly 70 percent of children under age 5 and 65 percent of adults age 60 to 64. In contrast, less than 30 percent of recipients between the ages of 5 and 39 had a physical disability as their primary diagnosis. Mental and intellectual disabilities accounted for 57 percent of the total nonelderly adult SSI caseload in 2017. Most of these diagnoses are for conditions other than intellectual disabilities. These include mood disorders along with schizophrenic and other psychotic disorders.

Percentage of 2017 SSI Disability Caseload Diagnosed with a Physical Disability
The trends in SSI caseloads, variation in participation across states, and heterogeneity of diagnosis by age underscore the complexity of the SSI program. Below, we discuss how this complexity produces economic incentives at odds with stated program goals because the program is still administered with a one-size-fits-all approach that was created 45 years ago.
Economic Issues and Research Evidence
SSI differs in several important ways from other means-tested transfer programs in the United States. First and perhaps most importantly, nonelderly individuals must have a demonstrated disability that impedes labor market activity and/or educational performance to qualify. Second, SSI benefits are generous relative to other programs, such as TANF and food stamps. Third, the vast majority of SSI benefits are paid for with federal dollars. Because of this, relatively poor states are significantly subsidized by states with higher incomes. And finally, SSI payments are not intended to be temporary, which implies that any program-induced distortions in behavior can be long-lasting (Burkhauser and Daly 2011; Duggan, Kearney, and Rennane 2016).
These program features introduce an important set of issues that have been highlighted by previous work. First, medical eligibility screening is a form of “tagging,” in which the government imposes requirements that target funds to groups with especially high needs (Akerlof 1978). This tag allows the government to redistribute more resources on a per-recipient basis than would be possible if all individuals were potentially eligible for the benefit. It can also, however, introduce an incentive for individuals to overstate the severity of their medical condition(s) in an effort to qualify for benefits. Second, the SSI program introduces the standard trade-off between income protection and distortions to the labor supply and savings decisions of those receiving benefits. More specifically, individuals may work or save less when applying for SSI or to retain SSI benefits once receiving. Third, because the SSI program is funded by the federal government, there can be an incentive for state and local governments to shift current or potential future beneficiaries of their programs (e.g., TANF) to SSI (Kubik 2003).
Despite the relatively large size of the means-tested SSI program in terms of both enrollment and expenditures, there has been relatively little research examining its effects on outcomes such as savings and labor supply. Previous research using administrative data has found that the SSI program does reduce the labor supply of near-elderly individuals (Neumark and Powers 2005). Relatedly, more recent work (Deshpande 2016b) finds that in families with a child who becomes ineligible for SSI, parents fully offset the loss in income with additional earnings. In contrast, recent research suggests that the effects on labor supply on young adults who become ineligible for the program at age 18 after a medical eligibility screen are relatively small (Deshpande 2016a), with those losing SSI eligibility earning just one dollar for every three dollars in lost benefits as young adults. The variation in findings in these and a few other studies underscores the heterogeneity of the groups being served and the complexity of the SSI program to be a single service provider to three very different groups (children, nonelderly adults, and the elderly).
There has been even less research on the effects of potential reforms to the SSI program. One interesting recent study by the U.S. Government Accountability Office (GAO 2017) found that a number of the provisions designed to encourage labor supply among SSI recipients and their families are not well-understood. For example, children and young adults under the age of 22 on SSI and enrolled in school can—through the student earned income exclusion (SEIE)—preserve more of their SSI benefits and retain their Medicaid eligibility even if they have substantial earnings. However, virtually no SSI recipients make use of this benefit that could lead to greater work incentives and economic well-being. This is especially troubling since many of these individuals will lose their SSI eligibility when they are reevaluated for the adult program and could benefit from greater work attachment now and in the future. More efforts by SSA to inform SSI recipients about these incentive provisions could have beneficial effects for recipients.
Related research (Hemmeter, Kauff, and Wittenberg 2009) has found that SSI recipient children who reach age 18 while in the program are typically not prepared for life without SSI (if they lose eligibility). This is especially true for child SSI recipients with mental disorders other than intellectual disabilities (formerly known as mental retardation), who are at much higher risk than other SSI recipients of losing benefits at or soon after age 18. Taken together, this research suggests that targeted interventions in the years leading up to and immediately following age 18 for those SSI recipients who have work capacity could have a high payoff for them for many years in the future. The bang-for-the-buck of reforms at these younger ages seems likely to be much higher than for the near-elderly adults identified by Neumark and Powers (2005) as being affected by SSI disincentives.
Reforms to the SSI program’s medical eligibility criteria, changes in the level of benefits, and changes in the phase-out rates could also strengthen the program. It is not obvious that the same monthly benefit should be paid to low-income elderly as to families with children who have a disability. Some straightforward first steps for the medical eligibility criteria would involve more efficiently targeting continuing disability reviews while also reducing the variation across disability examiners and ALJs in their decision-making about awards.
Many of these changes would involve complicated trade-offs, in some cases reducing the various distortions inherent in any means-tested program while possibly also lowering the insurance value of benefits or vice versa. It is noteworthy that state supplements to monthly SSI benefits have been falling in real terms over time, suggesting that few states consider the benefits to be far below where they optimally should be. It also seems likely that the recent reduction in enrollment is partially driven by tighter medical eligibility standards that are being employed by ALJs. These changes may have partly resulted from numerous accounts in the press of ALJs who appealed their SSDI application rejections. For example, a Wall Street Journal article from May 2011 pointed out that one judge awarded 1,280 of the 1,284 appeals that came before him and that there were many other judges with similarly high award rates. 13
More research is needed to estimate the effect of past and likely future changes in program generosity—both in the level of monthly benefits and in the stringency of the disability screen—on the health 14 and economic well-being of current and potential future recipients. Much more could be learned from pilot studies that can target interventions at specific populations to increase self-sufficiency for those with work capacity and economic well-being in the long run.
Potential Reforms
As we discussed, the SSI program currently serves three very different populations.
Elderly SSI recipients
The simplest of the three is the group of recipients above the age of 65, most of whom qualify purely due to low income rather than because of a medical condition. We see little reason to reform the basic structure of the program for this group since both the labor supply and savings incentive effects are likely small and because the share receiving benefits from this program has been steadily falling over time.
That said, it is noteworthy that the share of elderly Americans in poverty is twice as large as the share on SSI (9 percent versus 4.5 % see Figure 5). Indeed, if SSI benefits are the only source of income for an elderly individual, the ratio of his or her income to the poverty line would be just 73 percent. A modest increase in SSI benefits above the (2017) maximum of $735 per month would likely lead to significant reductions in poverty among the elderly. Alternatively, states could be encouraged to supplement the federal benefit for elderly recipients, moving them above the poverty line. In contrast to federal SSI benefits, state supplements to SSI benefits have, in inflation-adjusted terms, generally been falling over time. For example, in the State of California (which has a relatively generous SSI supplement), the state supplement for a nonelderly adult fell from $171 in 2011 to $161 in 2019. In inflation-adjusted terms, this represents a drop of 18 percent.
Related to this, with an asset test of just $3,000, many elderly individuals may have incomes far below the poverty line but assets above this threshold. This threshold has not changed since 1989. During that 1989 to 2018 time period, the consumer price index (CPI) has more than doubled (from 124.0 to 250.5). Inflation adjusting this threshold on an annual basis along with other thresholds (e.g., the amount of income that a person can earn before SSI benefits start to fall) would synchronize these program features with program benefits.
Nonelderly adult SSI recipients
For nonelderly adults, the case for revising some key features of the program seems even stronger. At present, the program provides all-or-nothing benefits that substantially lower a recipient’s incentives to work (or save). This occurs for two reasons. First, once earnings reach a certain level, SSI benefits fall by one dollar for every two dollars in earnings. Second, if an individual shows substantial work capacity, it is more likely that benefits will be terminated. Allowing SSI recipients to keep more of their earnings, both through a higher earnings disregard (the amount one can earn before taxes kick in) and a lower phase-out rate, could increase work effort for this group. Given the low exit rate from the program, the budgetary costs of this are likely to be minimal, since SSI receipt is largely an absorbing state.
Related to this, one concern that SSI recipients may have had for the first 40 years of the programs was that, if they were to return to work, they would lose health insurance through the Medicaid program (Yelowitz 2000). 15 But as of 2014, individuals with incomes below 133 percent of the poverty line were made eligible for Medicaid as a result of the Affordable Care Act. However, not all states elected to expand their Medicaid program. Currently, there are thirty-seven states (including D.C.) that have expanded their Medicaid programs and fourteen states that have not. This creates variation across states in the effective SSI incentive effects. One way to reduce these inequities would be to provide a grace period for SSI recipients in these fourteen states to retain their Medicaid health insurance coverage if they were to return to work. 16
SSI benefits are all-or-nothing—either an individual is deemed fully disabled or not disabled at all. One possible reform that accounted for the considerable heterogeneity across individuals in the severity of their disability would be to introduce partial disability benefits for those on the margin of qualifying. A similar system is used for the Veteran’s Association’s Disability Compensation program, through which disabled veterans can receive benefits reflecting disability of 10 percent all the way up to 100 percent (Autor et al. 2016). The effects of any such change on SSI expenditures, employment, and economic well-being among SSI applicants and their families would of course depend on the details. For example, the costs of the program would almost certainly increase if partial disability benefits were awarded primarily to individuals who, under the current system, would be rejected.
An additional desirable reform to the SSI program would be to provide more benefits at the “front end” so that SSI applicants who have some work capacity can avoid significant skill atrophy. For many individuals, the SSI application process takes a long time. This is especially true for applicants whose health is on the margin for qualifying, since they may not be disabled enough to be awarded benefits on the first round and so may then enter a lengthy appeals process. Indeed, more than half of rejected applicants in the 18 to 64 age range appeal the decision, and this process typically takes more than a year to complete. This group likely includes many with substantial work capacity that can be nurtured with an appropriate mix of rehabilitation (physical and/or mental) services.
Reforms to the SSI application process could also improve program efficiency and equity. It is noteworthy that more than half of applicants rejected at the first stage appeal this decision. Of those appealing this initial decision, nearly three in four are ultimately awarded benefits at the reconsideration, ALJ, or later stage. Because of this, nearly 40 percent of SSI awards to nonelderly individuals are made on appeal. Taken together, this suggests that the criteria used at later stages of the process differs from the criteria used on the front end. Synchronizing those criteria (perhaps making the criteria more lenient on the first stage) could reduce the uncertainty and wait time in the process while giving rejected applicants more confidence that the first-stage decision was the correct one. It is especially unfortunate if a person spends multiple years out of the workforce hoping to qualify for SSI and the application is ultimately denied.
A final possible proposal that is related to the previous one is that these early interventions should be tailored to the unique circumstances of each applicant. For example, it may be the case that physical therapy can help some SSI applicants to address musculoskeletal problems such as severe back pain. Alternatively, periodic visits with mental health professionals may allow many with mental disorders to better manage obstacles to realizing their potential in the workforce.
Perhaps the group that is most well positioned to spearhead these efforts is the SSI recipient’s health insurer. In recent years, many state Medicaid programs have shifted their SSI populations from fee-for-service Medicaid into managed care plans (Kaiser Family Foundation 2019). 17 These private insurers often have detailed information about the individual’s medical history and treatment effectiveness. However, they have little financial incentive to help an SSI recipient return to the workforce, since their payments do not increase if their beneficiaries’ earnings rise. The insurer actually has the opposite financial incentive, since if a person returns to work, she or he may become ineligible for Medicaid. Revising Medicaid managed care plans’ incentives so that they are rewarded as their recipients increase their work effort could lead to better outcomes both for current (or potential future) SSI recipients and for taxpayers. 18 A substantial body of previous research has shown that there are substantial health benefits to working and so the benefits to the recipient would often not be purely financial (Fitzpatrick and Moore 2017).
Child SSI recipients
We propose a somewhat different set of reforms for children who are receiving SSI benefits (Figure 4). One very innovative recent proposal by Wittenburg (2011) suggested tying the payment of a child’s SSI benefits to his or her attendance in school. This ensures that family members and local school systems will continue to invest in the human capital of their child. A potential concern is that overstretched schools would not have the services necessary to foster learning for SSI children. As such, we suggest broadening the requirement to include school or a similar investment-oriented activity, the key idea being to tie benefits for SSI children to investments in their human capital that maximize their chances of working as adults.
As with adults, we propose creating stronger financial incentives for private insures that administer Medicaid managed care plans to children. If private insures provide treatments focused on outcomes, more children will reach their full potential. For child SSI recipients, the quality of mental health care will clearly be very important, since more than 70 percent of child SSI recipients have a mental disorder as their primary qualifying condition.
The disincentive to save that the program creates is a related issue that may be especially important for families with children on SSI. Many families with a disabled child may want to save money for his or her education in the future, especially if they do not have to pay for private school during K–12 years. But given SSI’s means test, a parent who saves a nontrivial amount each year may cause the child to lose SSI benefits. This discourages saving for higher education or, for example, a private high school. Relaxing the asset requirement for qualified savings, for example, educational expenses, would allow families receiving SSI to plan for and invest in their child’s future without fear of losing benefits.
One final set of reforms that would apply for both children and adults in the SSI program would be to improve the efficiency of program administration. One area that warrants particular attention is the application process. Recent research has uncovered substantial variation across both disability examiners and ALJs in their decisions about benefit awards. This implies that—for a large fraction of SSI applicants—their application outcome depends somewhat on the “luck of the draw.” While SSA is aware of this issue and has made some progress in addressing it, further efforts to leverage the benefits of “big data” to harmonize decision-making would substantially improve the program.
Conclusion
SSI is a program that serves more than 8 million of the nation’s most disadvantaged individuals. It plays a key role in alleviating poverty among millions of individuals with disabilities while giving families additional resources that can cushion the financial and emotional costs of having a family member with a disability.
After rising steadily for decades through 2013, SSI enrollment has actually fallen among the nonelderly over the last few years. For example, the number of children receiving benefits fell from 1.32 million in 2013 to 1.15 million by 2018. 19 Similarly, the number of nonelderly adults on the program declined from 4.93 million in 2013 to 4.71 million in 2018. Whether this reflects the effects of tighter medical eligibility criteria for the program, improving health in the population, or the effects of a strong economy are important questions for future research.
But whatever the drivers of this change may be, reform of the SSI program could lead to substantial improvements in efficiency and increased benefits for program recipients. For the elderly, we propose an increase in the generosity of SSI benefits and a less stringent asset test. This would ensure that those who qualify for benefits are able to live above the poverty line and for those in poverty that they are not excluded from cash support due to asset valuations above the $3,000 limit. For nonelderly adults with disabilities, we propose changes that will increase their incentive to work while on SSI. Related to this, we encourage increases in the asset test for children on SSI so that their families can save for future educational expenses. For both adults and children with disabilities, we advocate greater efforts to harmonize disability decision-making among medical examiners and ALJs. And finally, given the substantial increase in Medicaid managed care enrollment among SSI recipients with disabilities, reforms to increase Medicaid managed care plans’ incentives to help both groups realize their potential could have a very high payoff.
When SSI was enacted in 1972, the U.S. economy and social norms were different. At that time, those not expected to work included individuals aged 65 and older, the blind, and people with disabilities. These categories were always difficult to establish and assess, particularly with regard to disability, but these challenges have grown worse over time as social expectations over who should work and who should be entitled to income transfers have changed.
In addition, the role of SSI in the broader social safety net has evolved. The normal retirement age for Social Security benefits is increasing, welfare reforms have placed limits on the number of years single mothers with children may receive benefits in lieu of working, and poverty rates among children remain high. These circumstances suggest that income maintenance programs such as SSI will play an increasingly important role in the U.S. social safety net. All these factors will impact the politically determined boundaries of the only remaining federal cash-based means-tested entitlement program without time limits available to both adults and children.
Footnotes
Note:
The views expressed here are the authors’ and not necessarily those of others at the Federal Reserve Bank of San Francisco or in the Federal Reserve System. The article draws heavily from prior work including Burkhauser and Daly (2002, 2011); Daly and Burkhauser 2003; and Duggan, Kearney, and Rennane (2016). We thank our prior coauthors for many useful discussions on these issues, along with Robert Moffitt, James Ziliak, and many conference participants for their helpful feedback.
Notes
Mary C. Daly is the president and chief executive officer of the Federal Reserve Bank of San Francisco. Her research focuses on labor market dynamics and the aggregate and distributional impacts of monetary and fiscal policy.
Mark Duggan is the Trione Director of the Stanford Institute for Economic Policy Research and The Wayne and Jodi Cooperman Professor of Economics at Stanford. His research focuses on the health care sector and the effects of government expenditure programs such as Medicare, Medicaid, and Social Security.