
Abstract
We analyze policies that support and affect the provision and costs of child care in the United States. These policies are motivated by at least three objectives: (1) improving the cognitive and social development of young children, (2) facilitating maternal employment, and (3) alleviating poverty. We summarize this policy landscape and the evidence on the effects they have on the development of children and parents. We provide a summary of the use and costs of nonparental child care services; and we summarize existing policies and programs that subsidize child care costs, provide child care to certain groups, and regulate various aspects of the services provided in the United States. We then review the evidence on the effects that child care policies have on these objectives. We go on to discuss the existing evidence of their effects on various outcomes. Finally, we outline three reform proposals that will both facilitate work by low-income mothers and improve the quality of child care that their children receive.
The early educational experiences and care of America’s children have become major focuses of public policy over the last 40 years. This increasing focus is motivated by at least three separate issues. First, there is growing evidence that exposure of young children, especially infants and toddlers, to enriching child care has important impacts on both children’s cognitive, personal, and social development; and their readiness for successful entry into primary school (K–6). In addition, increasing evidence indicates that such exposure has impacts on individuals’ success in college, careers, and a range of other later life outcomes. Second, access to nonparental child care for young children has become a requirement for the labor force participation of women with young children. In 2017, for example, 65.3 percent of the 22.9 million children in the United States under the age of six had mothers who were in the labor force. 1 Finally, and related to the first two, it appears that access to child care and early education, especially that which is of high quality, ameliorates the short- and long-term consequences of poverty in the United States for the some 20 percent of America’s children who live in poverty, 2 as well as for their parents, especially single mothers.
In this article, we analyze the main policies that support and affect the provision and costs of child care in the United States. 3 We summarize this policy landscape and the evidence on the effects these policies have on maternal employment, child poverty, and child development. As we discuss, federal child care policy has focused primarily on facilitating maternal employment of low-income families and on alleviating poverty. But other child care policies have focused primarily on improving the quality of child care that children from disadvantaged backgrounds receive, based on increasing evidence of the developmental benefits of early childhood education. An important theme of our analysis is the tensions and trade-offs in designing and implementing public policies for child care and early education. Finally, based on existing evidence, we consider possible reforms, including expansions of the existing Head Start program and the provision of universal child care in the United States; expansions of existing child care subsidies and tax credits for child care expenses; and ways to improve information that parents, especially those in low-income families, have about the quality of child care services available to them, and how they can use this information to make their child care decisions.
In the next section, we provide a brief summary of evidence on child care use and costs in the United States, emphasizing differences across the income distribution of families. We then provide an overview of existing child care policies that directly provide child care services, ones that subsidize their costs, state programs that regulate the provision and quality of child care services, and more recent state quality rating improvement systems (QRISs) that seek to improve information on the quality of child care providers in local markets. We go on to summarize the evidence on the impacts of the direct-provision and subsidy programs, for state child care regulations, and for QRISs.
We focus on how these programs and policies affect maternal labor supply, poverty, and child development. Finally, we discuss proposals for three different sets of child care policy reforms, some of which entail expansions of existing programs and others that are modeled after those in other countries. We outline the specifics of these reforms and their likely costs and critically evaluate their likelihood for improving the well-being of low-income families and their children’s development.
Child Care Use, Its Costs, and Licensed Facilities
In this section, we briefly summarize patterns of child care use, expenditures, and the number and capacity of licensed child care facilities in the United States.
Use of child care
Here, we examine the use of different types of child care, using the 2012 National Survey of Early Care and Education (NSECE). 4 Figure 1 displays the average hours of care in different care types for each household child. Average hours are constructed for a 40-hour “regular” work week, allowing a focus on the child care most relevant for parental work schedules. For children in their first year, on average about 16 of the 40 hours are spent in various forms of child care, and not with parents. Of that 16 hours of care, about 3 hours on average are in child care centers, 4.5 hours with a regular paid individual caregiver (e.g., a nanny), 5.5 hours with a regular unpaid individual caregiver (e.g., a grandparent), and a remaining nearly 3 hours are in irregularly provided care.
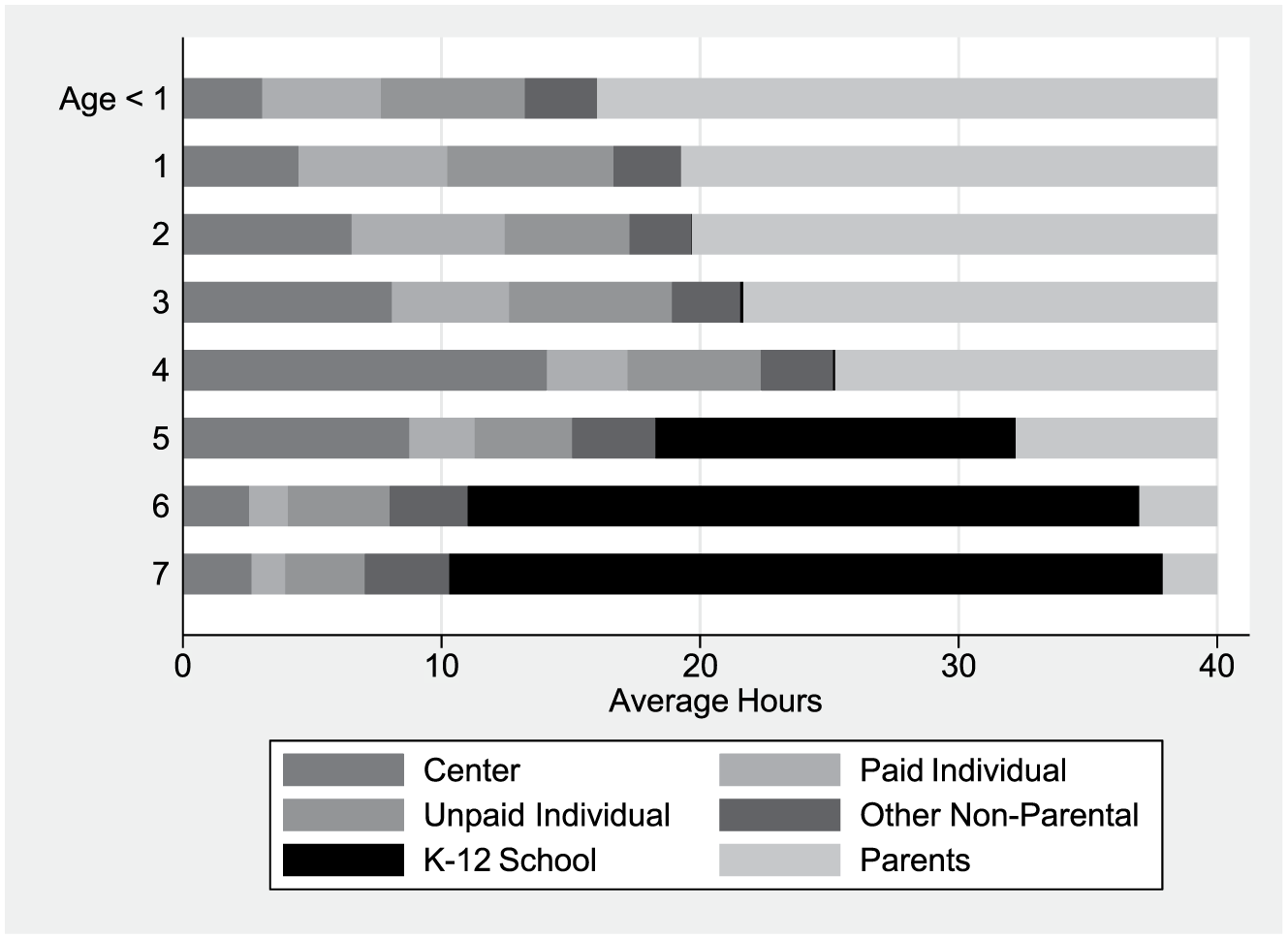
Mean Hours of Care during Regular Work Week
As children age, they spend less time in the care of their parents. At age four, nonparental child care peaks at about 25 hours on average, with on average only 15 hours of the 40 regular work week hours spent with parents. The fraction of households using regular center-based care in particular rises from less than 10 percent of households in the first year to the majority of households by age four. This increase in center-based care is due in part to the increase in pre-K usage among households. Even after K–12 school entry (ages 6–8), nonparental care still is substantial with about 10 hours of child time spent in various forms of nonparental child care, representing mainly after-school care.
One of the key considerations for a policy reform that would subsidize child care or otherwise change its availability or desirability is the potential take-up or demand for child care. This demand could come from households that are not using nonparental arrangements to care for their children or ones that have their children in some form of nonparental care. To provide some evidence on this potential demand, Figure 2 displays the mean weekly hours of nonparental child care, where nonparental hours is the sum of all hours spent in various forms of formal and informal childcare, but not with parents. Across all ages, the highest-income households (those with annual incomes greater than $75,000) use more nonparental care hours, and for the youngest children (in the first year), the highest-income households use twice as much nonparental care as the lowest income households.
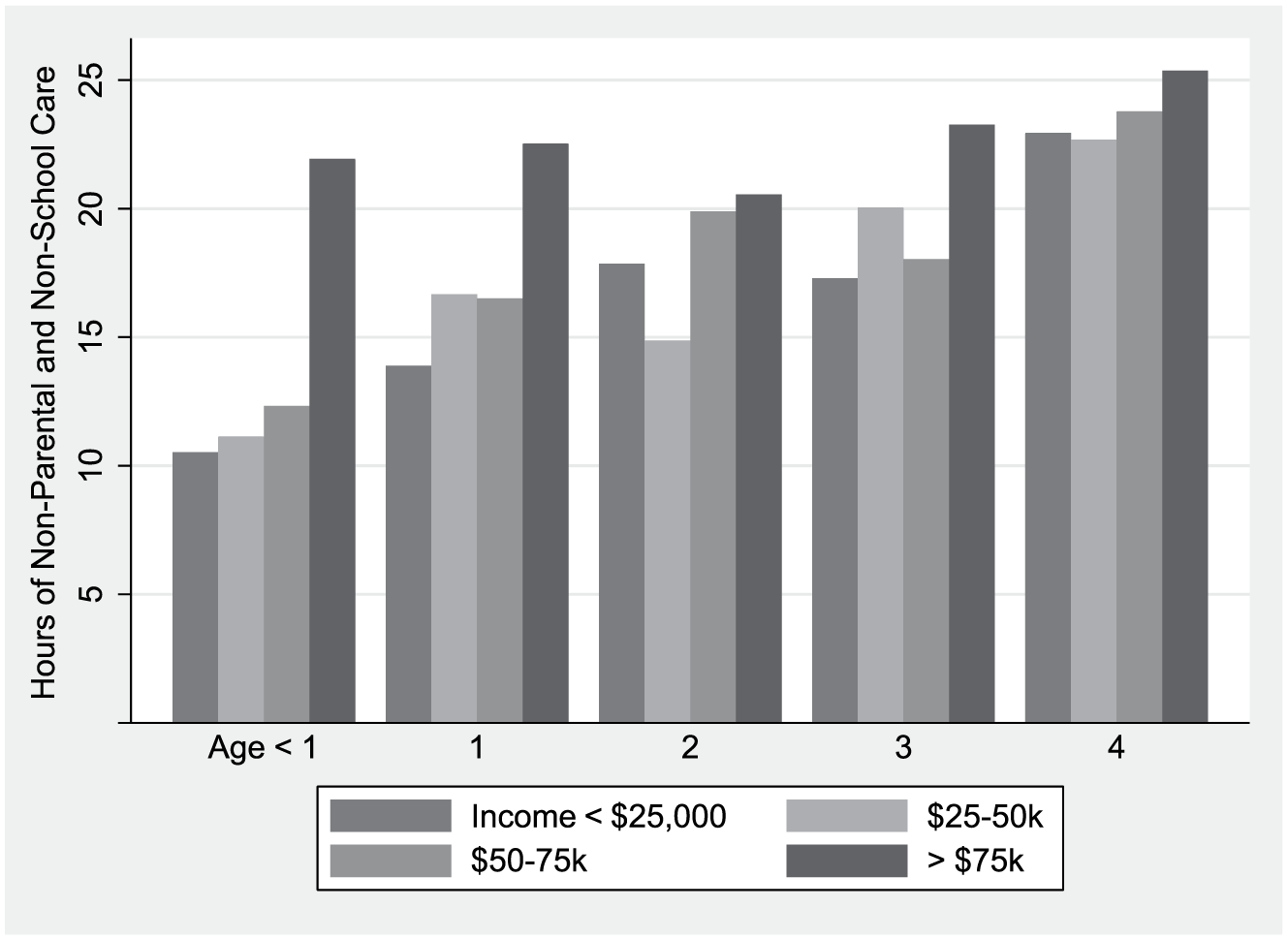
Mean Weekly Hours of Nonparental Care by Family Income
Household expenditures
We next turn to examining recent patterns in household expenditures on child care. We examine household “out-of-pocket” expenditures on child care, net any subsidies they receive. 5 Figure 3 reports expenditures as a percentage of household income only for those households that report positive expenditures. These figures illustrate the regressivity of costs facing families. Focusing first on child care for the youngest children (aged 0–2), for the lowest-income households that are paying something out of pocket for child care, the median percentage of income paid on child care is about 30 percent of household income. For the high-income households, this figure is much lower, about 7 percent. As the children age, the percentage paid by the lowest-income households falls to about 20 percent, still several times higher than the high-income households. 6
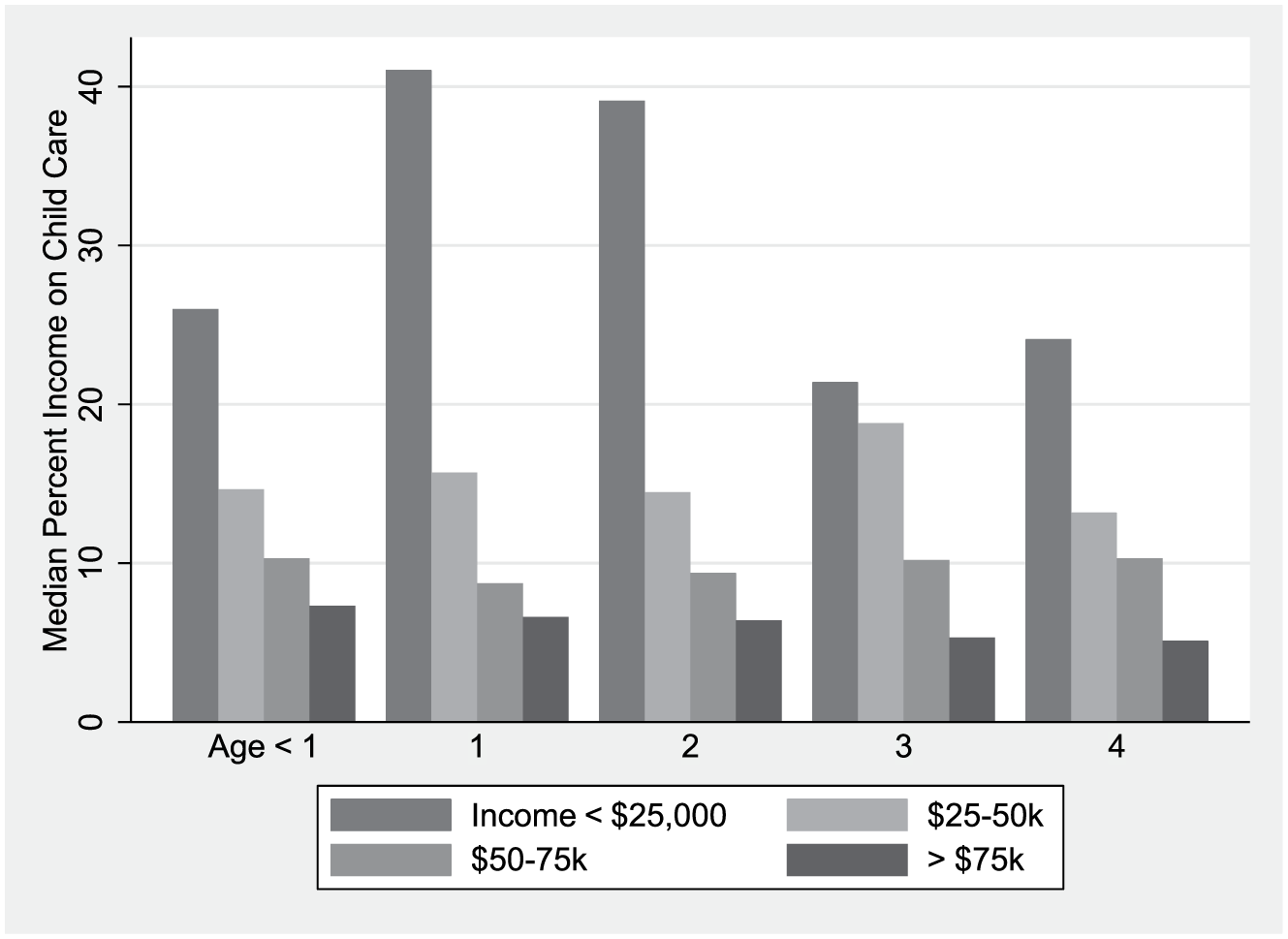
Median Percentage of Household Income Spent on Child Care (if positive expenditure)
Number and Capacity of Licensed Child Care Facilities
Figure 4 displays trends in the number and total capacity of licensed child care facilities by type in the United States over the period 2005 to 2014. The figure shows trends in three types of child care facilities: (1) child care centers, that is, child care services provided in a nonresidential setting that involve multiple staff (directors, teachers, assistants, etc.) with multiple children; (2) family child care homes, that is, a single individual providing child care to children in their own home; and (3) group child care homes, that is, child care provided to children in a provider’s home but where there is more than one individual providing the care. Over this period, the number of licensed child care facilities has actually declined, due to declines in the number of family child care homes (–30.6 percent) and group child care homes (–11.4 percent), even though the number of child care centers increased slightly (4.5 percent). At the same time, the capacity of child care facilities has increased by 15 percent, largely because the average licensed child care center became 26 percent larger over this period. This increased capacity of licensed child care centers is likely to benefit the development of young children, given the evidence that we discuss below that licensed child care centers tend to provide more developmentally enriching environments than informal modes of child care. It is important to note, however, that even with this growth in capacity, as of 2014, the existing capacity in licensed child care centers only would have accommodated 33 percent of the children in the United States under the age of 6.
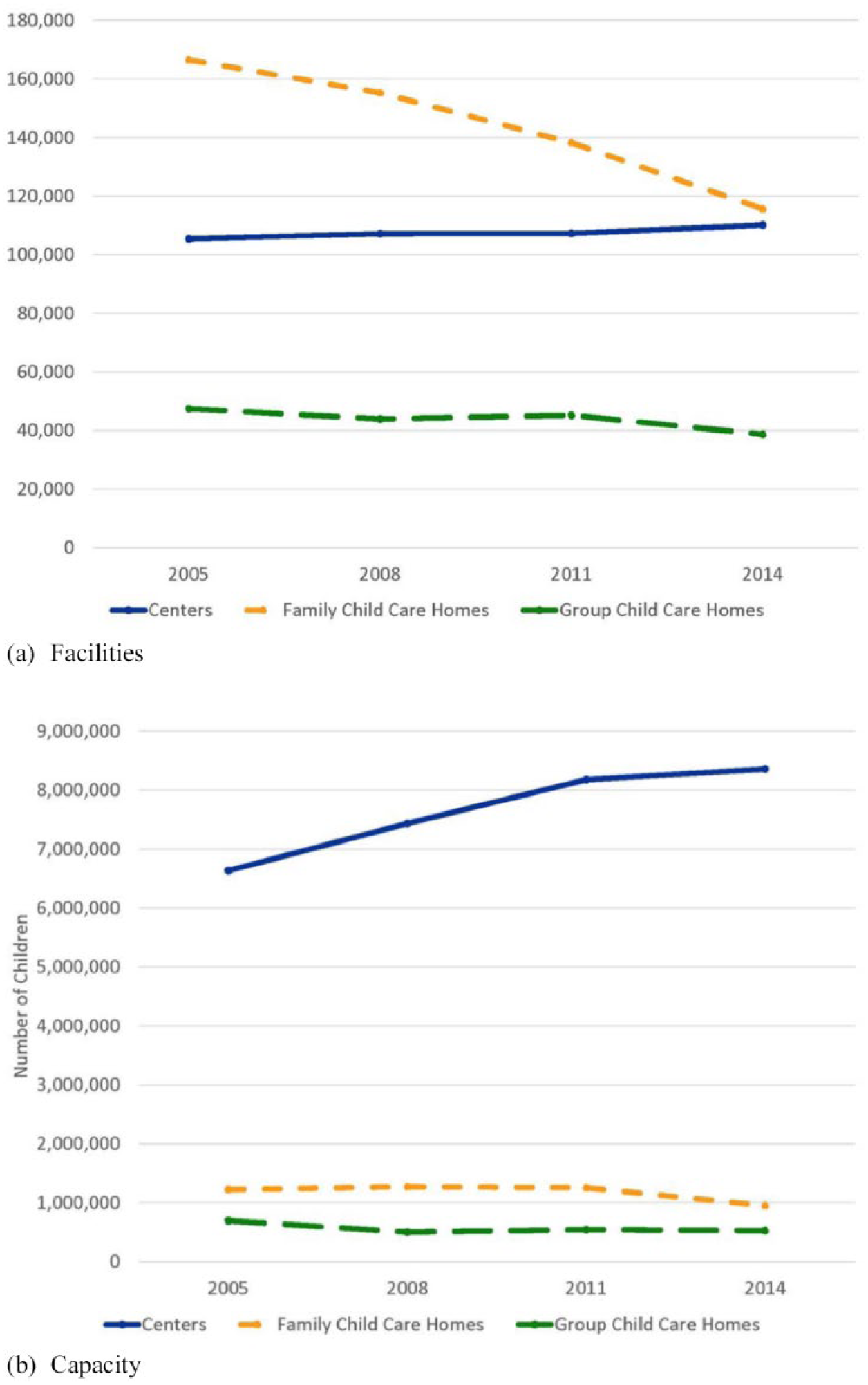
Number and Capacity of Licensed Child Care Facilities in the United States, by Type, 2005–2014
Child Care Policies, Regulations, and Information Provision
In this section, we discuss the major U.S. policies related to child care, with a focus on those that subsidize child care, assist directly in its provision, and regulate the services and settings of its providers. 7
Child Care Development Fund
The Child Care Development Fund (CCDF) authorized under the Child Care Development Block Grant (CCDBG) Act provides grants to states to subsidize the child care expenses of low-income working parents with young children. In fiscal year (FY) 2018, the federal appropriation was $5.23 billion, with a state match of $2.92 billion, bringing the combined funding under the CCDF program to $8.1 billion. CCDF subsidies are provided in the form of vouchers to eligible families, which can then be used to defray the cost of child care at private providers. In FY2017, approximately 1.32 million children and 796,000 families received child care assistance under the CCDF, with 74 percent of those families having incomes less than 150 percent of the federal poverty level (Administration for Children and Families 2019). States have discretion over setting the eligibility requirements, including thresholds for family income and the maximum age of children covered by these subsidies, 8 and which work- and education-related activities (e.g., work, job search, training, and education) qualify for these subsidies (Stevens, Blatt, and Minton 2017). States also have discretion over setting requirements and policies that apply to child care providers that qualify for CCDF subsidies, including reimbursement rates for CCDF subsidized care and licensing regulations.
The 2014 reauthorization of the CCDBG Act included two key components to reorient the provision of child care assistance to low-income populations. The first set aside CCDF funds to improve the quality of child care services available to eligible children, and the second helped states to fund child care quality rating and information systems to help low-income families be more informed and, thus, better consumers of child care services. We discuss the latter component below.
Child and dependent care tax credit and exclusion of child care expenses benefits
There are two tax benefits that offset families’ work-related child care expenses. 9 The first and largest, the Child and Dependent Care Tax Credit (CDCTC), provides a credit worth between 20 percent and 35 percent of a family’s work-related child care expenses for children under age 18. Eligible care expenses are limited to $3,000 per child ($6,000 for two or more dependents), and credits vary by a family’s adjusted gross income (AGI). 10 A key feature of this credit is that it is nonrefundable, so it can only offset income taxes that the filer owes. Thus, low-income families with no or low incomes get no or little benefit from the CDCTC. In addition to the federal credit, twenty-four states currently have a version of the CDCTC, and ten of these states have credits that are partially or fully refundable. 11
Tax filers can also make use of dependent care flexible spending accounts (FSAs), provided through their employer and similar to FSAs used for health care expenses, that allow employees to set aside a portion of their pretax income to pay for child care expenses. Employees with children also may have access to subsidized workplace-provided child care as a nontaxable fringe benefit. Both of these provisions tend to benefit full-time, higher-income workers and are not available to individuals who do not work. 12 As shown in Figure 5, 6.2 million families (tax filers) claimed the CDCTC for a total of $3.4 billion in tax year 2016, while 1.4 percent benefited from child care FSAs for a $1.14 billion tax benefit, for a combined tax benefit of $5.3 billion to 6.8 million families. As can be seen in this figure, these tax-related benefits are primarily used by and benefit high-income families.
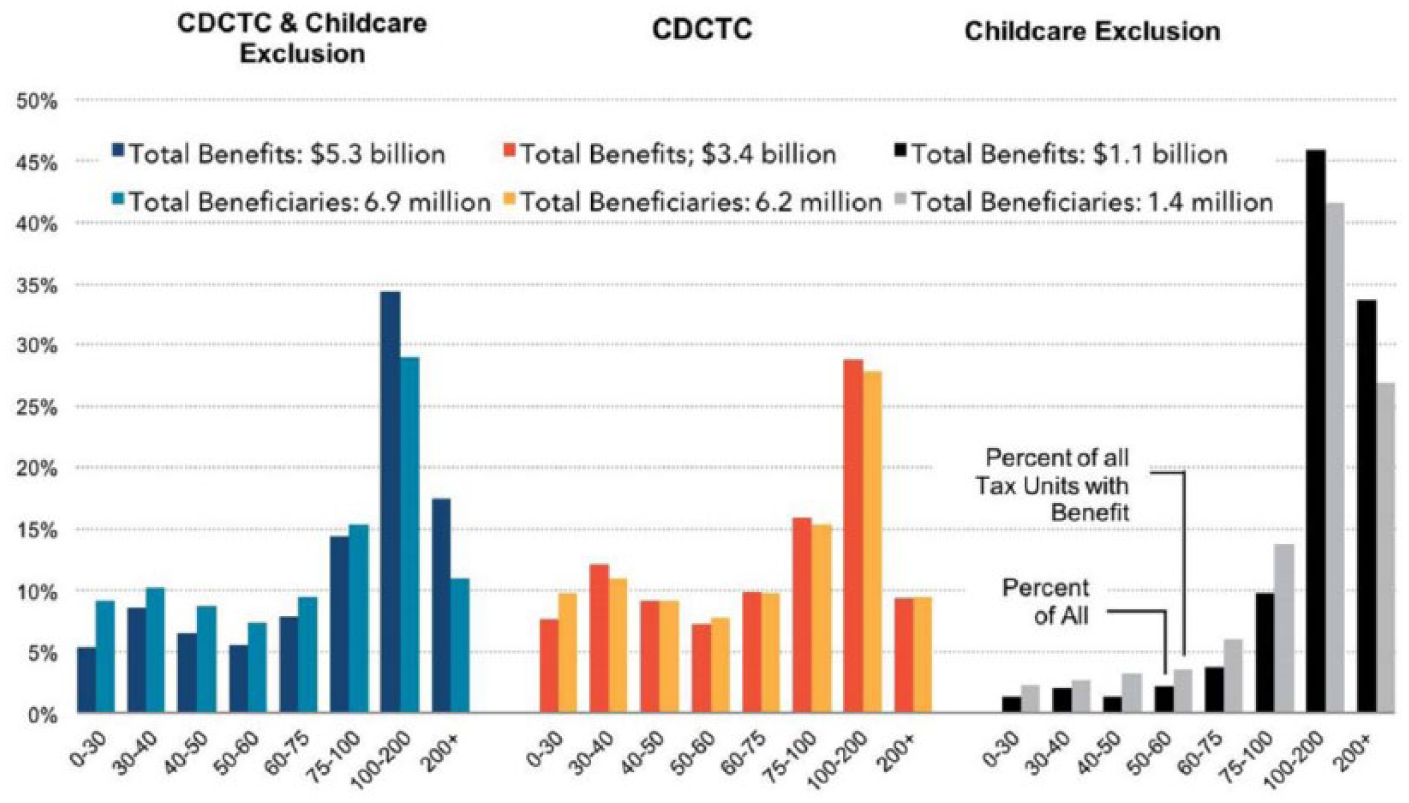
Families Benefiting and Amount of Benefit from the CDCTC and the Tax Exclusion of Child Care Benefits by Adjustable Gross Income, Tax Year 2016
Head Start and Early Head Start programs
Head Start is a federal program providing direct funding for child care centers to provide free care to eligible children, primarily from low-income households. In 2017, Head Start served about 1 million children, at an outlay of about $9 billion in federal government funding. Head Start primarily serves three- and four-year-old children, but about 20 percent of the children were younger than three and enrolled in the Early Head Start program (Administration for Children and Families 2017). In addition to child care, Head Start also provides an array of services to enrolled children and their families, including health services for children.
State regulation of child care providers
In the United States, regulation of child care providers is almost exclusively the domain of states. However, states do not regulate the quality of child care services directly; rather, they impose standards on the various aspects of these services. Existing state regulations of child care facilities and providers can be loosely organized into those regulating (1) labor intensiveness of care; (2) training and qualifications required of providers and their staff; (3) the health and safety of child care settings and staff obligations; and (4) strategies for verifying compliance, that is, inspections. 13 These dimensions of child care services are what developmental psychologists refer to as “structural quality” (Yoshikawa et al. 2013).
With respect to regulating the labor intensiveness of care, all states impose minimum child/staff ratios for center-based facilities, and the majority of states impose maximum group size restrictions. These regulations differ by the age of children. State regulations for the training and education of child care staff include minimum educational and experience requirements and periodic on-going training that differ by staff position (directors vs. teachers vs. aides). While both of these types of regulations vary across states, on average their stringency has not changed much over the past 20 years. Some previous research has indicated that regulations of the labor intensiveness of care and the educational qualifications of providers are associated with objective measures of child care quality (e.g., the cognitive, emotional, and social development of young children), 14 other research questions these findings (Blau 2000, 2003b). More recently, states have been developing regulations to address the health and safety of child care providers, including safety features of facilities and requiring criminal background checks of child care staff, which have resulted from heightened concerns about staff with histories of child abuse. Finally, most states conduct periodic inspections of child care facilities, especially child care centers, and some states conduct unannounced inspections.
Child care resource and referral (CCR&R) services and QRISs
The CCDBG Act, with CCDF grants, also seeks to improve the quality of child care and the information consumers have by helping to fund state and local CCR&R agencies and, more recently, states’ QRISs. State CCR&R networks provide assistance to child care providers and parents in developing and locating high-quality child care programs at the local level. These agencies provide business development assistance to child care providers and have developed databases on child care programs that meet certain standards that parents can use to identify child care programs in their local markets. Since 1980, the federal government has mandated that states maintain such databases as a condition for receiving funding under the CCDF and provide guidelines, technical assistance, and grants for their operation and development. At the same time, these databases do not collect or distribute detailed information about the quality of individual providers.
As part of the 2014 reauthorization of the CCDBG Act, the federal government has “incentivized” states to develop QRISs that do provide information to parents and others about the developmental, safety, and health dimensions of child care facilities and providers. In particular, the 2014 reauthorization envisioned systems in which ratings of the quality of child care providers that would stimulate increased availability and use of high-quality child care. 15 Figure 6 displays the “logic model” envisioned for these systems. As noted in Cannon et al. (2017), this logic views QRISs as market-oriented systems in which information provided via ratings of programs improves parents’ ability to judge the quality of alternative child care providers and to use this information in making their choices. Better-informed parents are presumed to be more likely to choose higher-rated and higher-quality care. As a result, lower-rated providers are motivated to improve the quality of their programs. State-level systems then help providers, both existing and new entrants, to develop “business plans” to improve their curricula, facilities, workforces, and management practices to achieve higher ratings and better compete in the child care marketplace (see also Zellman and Perlman 2008).
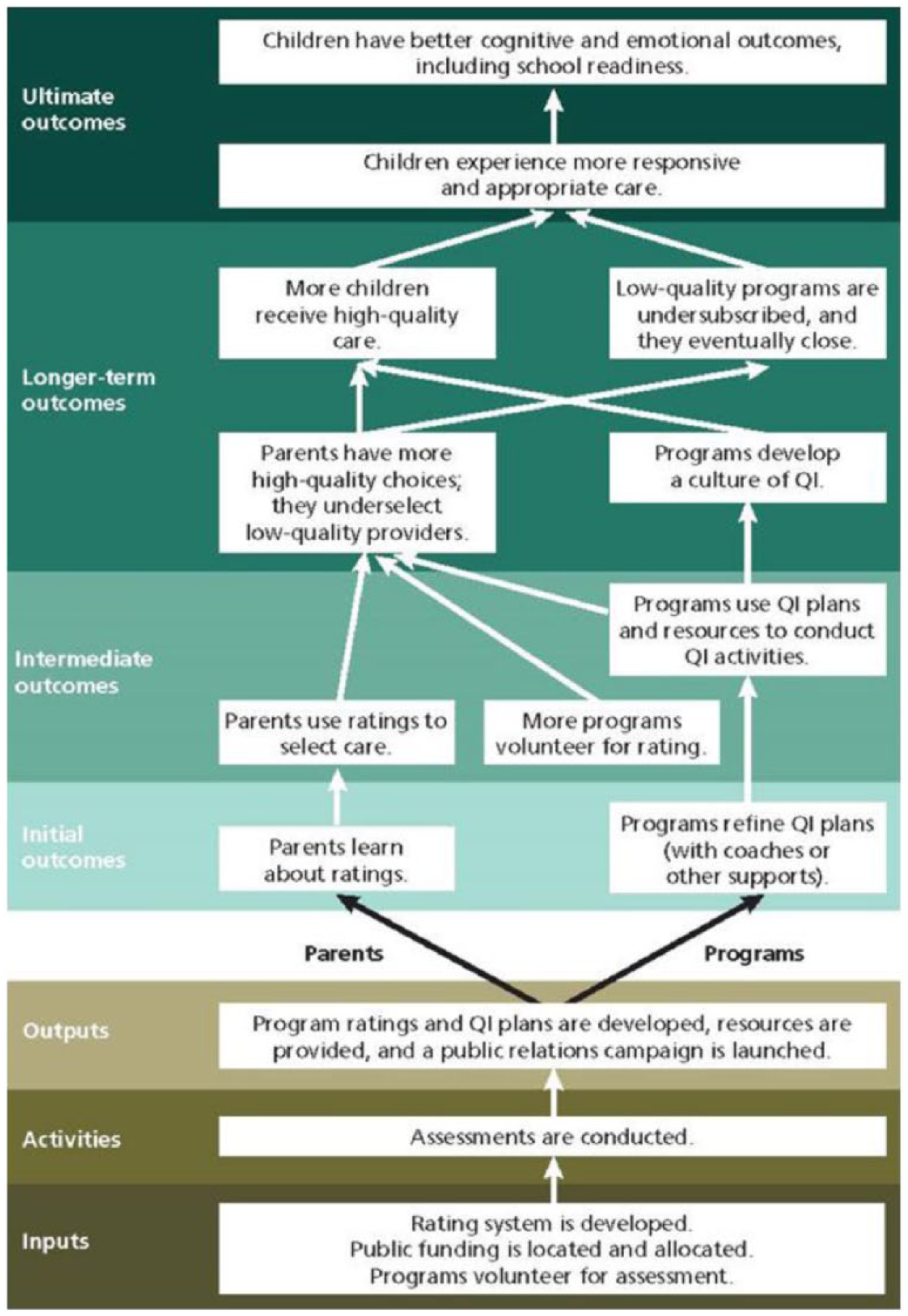
The QRIS Logic Model
Evidence on the Effects of Child Care Subsidies
Child care subsidies can take several forms: in-kind subsidies of an offer of a tuition subsidized spot at a government funded child care center like Head Start or vouchers that households could use to subsidize the costs of using nongovernment providers of their choice. In addition, child care is subsidized via tax credits that tax-paying households can use to defray their child care expenses.
An important consideration in assessing the impacts of programs that provide or subsidize child care services is that they may not be used (or taken up) by all households eligible for them. Some households may prefer their current child care arrangements, even when the subsidy is substantial, or prefer parental care over any nonparental form of care. Still other households may prefer their current child care center and not want, for example, to travel farther for their children to attend a government funded care center. How take-up is affected by the particular program structure is an important consideration for evaluating the impacts of different policies.
Another important consideration is that an offer of subsidized care, although it may facilitate parental employment and improve household finances, will not necessarily benefit children and their development. If the take-up of the care causes the household to substitute away from higher-quality forms of care toward lower-quality care, then the care subsidy may harm children’s development. A leading example of this possibility is a government program offering free but low-quality care, which causes some households to substitute away from higher-quality care. This possibility highlights the salience of the quality of the care being subsidized, and the particular restrictions and regulations associated with the policy.
Small-scale demonstration programs
A number of small-scale demonstration programs—most prominent among them Perry Preschool Project (began 1962), Carolina Abcedarian Project (1972), and the Infant Health and Development Program (IHDP) (1985)—have provided evidence of the short- and long-term effects of offering free center-based care, largely to disadvantaged populations. Each of these programs has been extensively evaluated using the random assignment of the treatment offer to provide credible estimates of the effects of these programs. Elango, García, and Heckman (2016) provide a recent review of evidence on their effects on child development and conclude that they had positive effects on short-run IQ and beneficial effects on various longer-term outcomes, including educational attainment, employment, health, and criminal activity. The IHDP program stands out among these programs in that it did not restrict program eligibility based on family income, and provided evidence that the offer of free center-based care to children ages one to three primarily benefited lower- and middle-income families, who substituted away from maternal care toward the center-based program care (Duncan and Sojourner 2013; Chaparro and Sojourner 2015).
Head Start
A number of previous studies have evaluated the effect of Head Start. Some use nonexperimental methods (comparison of participants to nonparticipant siblings and discontinuities in program rules); others, like the Head Start Impact Study (HSIS), are based on random assignment designs (Currie and Thomas 1995; Ludwig and Miller 2007; Deming 2009; Bitler, Hoynes, and Domina 2014; Carneiro and Ginja 2014; Feller et al. 2016; Walters and Kline 2016; Morris et al. 2018). Like the small-scale demonstration programs, these studies find that Head Start improved short-run test scores and had a number of beneficial long-run effects on educational attainment, earnings, health, and crime. Some of the most recent analyses using the HSIS experiment have emphasized the importance of care substitution in understanding the heterogeneity in the effects of the program (Feller et al. 2016; Walters and Kline 2016; Morris et al. 2018). These recent studies have concluded that the impacts of Head Start were substantially larger for children who would have otherwise received parental or informal nonparental care and were small or nonexistent for children who would have otherwise been cared for through other center-based care. Positive effects of Early Head Start, serving younger children, have also been found (Love et al. 2002). The evidence of the effects of Head Start on parents is more mixed. Using experimental variation in the HSIS, Sabol and Chase-Lansdale (2015) find an effect on parental educational attainment but not their labor supply. A more recent unpublished paper using state-level changes in Head Start eligibility finds that Head Start increased mother’s labor supply, particularly among black women (Russo 2017).
Pre-K and kindergarten in the United States
Prior evidence on the effects of child care policies comes from the U.S. experience with the expansion of public school kindergarten (typically children aged 5–6), beginning in the 1960s, and the more recent expansion of pre-K programs (typically aged 4–5). 16 Some evidence indicates that the introduction of public kindergarten in the 1960s and 1970s increased maternal employment, particularly among single mothers (Cascio 2009; Gelbach 2002). But evidence from recent pre-K introduction indicates there are small, if any, effects on maternal employment, possibly due to the availability of other child care subsidies (Fitzpatrick 2010). In a recent paper, Cascio (2017a) studies the recent expansion of pre-K in the United States, from only four states with public funding in the early 1980s to forty states by 2011, and finds substantial positive effects of attending universal pre-K on reading and mathematics scores of four-year-old children from low-income households, but smaller to no effects for high-income households. 17
Child care subsidies
There is a fairly extensive literature on the effects of subsidizing child care costs on maternal employment summarized in Blau (2003a); Ziliak, Hokayem, and Hardy (2008); and Morrissey (2017). Past studies differ by the source of variation in child care prices and subsidies used, the demographic groups considered, and the statistical strategies used to identify their effects on maternal employment. Typically, studies present their findings in terms of elasticities, that is, the percentage change in an outcome (e.g., employment) due to a 1 percent change in the net hourly cost of child care. Studies reviewed by Blau (2003a) show elasticities with respect to maternal employment ranging from 0.06 to –0.34; those reviewed by Ziliak, Hokayem, and Hardy have slightly larger (in absolute value) elasticities; those by Morrissey have slightly smaller ones, while both of their ranges are less than 0. 18 Finally, Enchautegui et al. (2016) estimate employment elasticities of 0.05 for women with children ages 0 to 12 and 0.07 for women with children ages 0 to 3, using aggregate state-level employment data and changes in state CCDF subsidy rates. Taken together, these findings indicate that reductions in child care costs will result in fairly modest increases in maternal employment. Furthermore, by comparison, Ziliak, Hokayem, and Hardy note that subsidizing child care costs tends to produce larger maternal employment increases than does increasing the minimum wage but smaller ones than does increasing the EITC.
A series of papers (Herbst and Tekin 2010, 2016; Hawkinson et al. 2013; Johnson, Ryan, and Brooks-Gunn 2012) study the relationship between child outcomes and parents’ report of receiving a subsidy for their child’s care in the year before kindergarten, where most of the studies are based on temporal and across-state variation in CCDF-funded vouchers. These studies find that subsidy receipt reduces math and reading scores measured at kindergarten entry and increases reports of behavioral problems, among other measured deleterious effects. 19 But they also find that the adverse effects are mainly for children with mothers with high human capital, suggesting that the care subsidies, which are in general not restricted by quality, are inducing some households to switch from higher-quality maternal care to lower-quality paid care.
Evidence from outside the United States
A rich variety of child care policies in other countries provide potentially important evidence for evaluating policy reform in the United States. A number of recent studies have examined experiences with mainly universal child care programs, across a number of different countries and areas: Argentina (Berlinski and Galiani 2007), Israel (Schlosser 2010), Italy (Brilli, Del Boca, and Pronzato 2016; Biroli et al. 2018), Sweden (Lundin, Mörk, and Öckert 2008), England (Brewer et al. 2016), Spain (Felfe, Nollenberger, and Rodriguez-Planas 2015), Germany (Bauernschuster and Schlotter 2015), Norway (Havnes and Mogstad 2011a, 2011b, 2015; Andresen and Havnes 2018), and Québec (Baker, Gruber, and Milligan 2008, 2015). A few findings stand out.
First, the effect of universal child care programs depends on the existing usage of child care and the ages of children covered. In the Norwegian case for example, a universal child care program started in the 1970s covering children aged three to six is estimated to have had modest positive effects on maternal labor supply because the program mainly caused a substitution between different types of nonparental care, from unsubsidized care to subsidized care (Havnes and Mogstad 2011b). In contrast, a later Norwegian universal program started in 2002, covering children aged two and up, had a larger positive effect on maternal labor supply (Andresen and Havnes 2018).
Second, the issue of the quality of care offered in the universal program comes to the fore in understanding the results of a Québec universal child care program. Starting in the 1990s, the Canadian province of Québec provided universal care to children of all ages, with an out-of-pocket cost capped at CAN$5 per day. Using differences between Québec and other Canadian provinces, Baker, Gruber, and Milligan (2008, 2015) find that this program had substantial deleterious effects on child outcomes, such as anxiety, aggressiveness, motor and social skills, and health. However, it appears that the types of care subsidized under this program were of lower quality than the programs considered in the United States. 20 In addition, the take-up of the Québec program was twice as large for educated mothers (some college or more) than for less educated mothers (high school or less), likely because the low-income households already had access to some subsidized care at the time that the program began. Therefore, it is possible that the Québec program caused many households to switch from higher- to lower-quality care. Baker, Gruber, and Milligan (2015) conclude that in the case of the Québec program, “Our findings for young children clearly contrast with those of the Perry, Abecedarian, and Head Start studies. These latter programs both provide higher quality care and are targeted at less advantaged children” (p. 30).
Evidence on the Effects of Child Care Regulations and QRISs
The theoretical literature most relevant to assessing the effects of child care regulations is that of imposing minimum quality standards or licensing in a competitive product market (Leland 1979; Shapiro 1986; Klein and Leffler 1981). Assuming products/services vary in quality that is costly to produce and that consumers care about quality, but are uncertain ex ante about quality, imposing binding minimum quality standards would increase average product/service quality and increase consumers’ willingness to pay for it, due to assurance of higher quality. But consumers will face higher prices for the higher-quality product/service, which will discourage their purchase. The net effect of these opposing forces on consumers—greater quality assurance versus higher cost of quality—is ambiguous. At the same time, they imply that the overall supply of child care services is likely to decline, although the available supply should be of higher quality.
But, as noted in the literature on the effects of child care regulation (Blau 2003b; Blau and Currie 2006; Blau 2007; Hotz and Xiao 2011), this simple theory does not adequately characterize key features of the child care market. First, the quality of child care services is not directly regulated; rather, states tend to regulate the quality of “inputs” used in the production of these services, such as the educational qualifications of staff or the number of staff per child in a center. Thus, there is the potential for input-substitution when some inputs are regulated and others are not. Second, in the presence of alternative modes of child care, imposing higher minimum quality standards on one mode can induce mode-substitution, for example, parents substitute from child care centers to unregulated (or less regulated) providers in response to more stringent regulations. Finally, child care services involve multiple dimensions beyond their developmental quality. This complicates the capacity for regulation to improve quality, since regulating this aspect of services will increase their cost but also may induce parents to substitute toward providers that are high in other dimensions, for example, are closer to their work or have more convenient hours, which will mitigate some of the regulation’s impact on quality.
Effects of state regulations
We begin with the findings on the effects of child care regulations on use of regulated care and the substitution to nonregulated (or less regulated) modes of care. The evidence is mixed. Most studies (Chipty and Witte 1997; Gormley 1991; Lowenberg and Tinnin 1992; Currie and Hotz 2004) find that more stringent child/staff requirements for child care centers and other regulations reduce the incidence and hours of such care used by parents (Hotz and Kilburn 1997; Hofferth and Chaplin 1998). But other studies (Ribar 1992; Chipty 1995; Blau 2003b) either find no impacts or imprecisely estimated negative effects of more stringent regulations on use and hours of center-based care.
The evidence of more stringent regulations on how much parents spend on child care also is mixed. Hotz and Kilburn (1997) and Hofferth and Chaplin (1998) find that tougher regulations are associated with higher family expenditures per hour of child care among families paying for care. Chipty (1995) finds that stricter group size regulations increase family expenditures per hour on child care but stricter child/staff ratios reduce it. 21
Several studies have examined the effects of more stringent child care regulations on maternal employment. Most studies (Ribar 1992; Blau 1993; Hotz and Kilburn 1997) find either small negative or insignificant positive effects of more stringent regulations on maternal labor supply. More recently, Han and Waldfogel (2001) find that more stringent regulations lead single mothers to be less likely to be employed but increase the employment rates of married mothers. They argue this finding is consistent with married mothers, who are wealthier than single ones, being more sensitive to the improved quality arising from more stringent regulations, while the employment of single (and poorer) mothers is more affected by the higher costs that regulation produces.
The theory implies that more stringent regulations would reduce the available supply of child care but increase the quality of care of providers that remain in business. Early studies based on survey data of households (Gormley 1991; Chipty 1995; Lowenberg and Tinnin 1992) or, for example, of child care providers (Chipty and Witte 1997), found that stricter regulations reduce the number of slots in regulated facilities and result in higher turnover of providers. More recently, Hotz and Xiao (2011), using panel data on the universe of all child care centers, 22 also find that more stringent regulations reduce the number of child care centers or group child care homes in local markets. 23 They find that this crowd out of center care facilities is greater in local markets with higher concentrations of low-income parents.
Blau finds mixed evidence on the effects of more stringent regulations on the quality of child care services available to parents (Blau 1997, 2000, 2007), with results being sensitive to the statistical methods used to control for other state-level differences that may be correlated with state regulations. In contrast, Hotz and Xiao (2011), using panel data on child care providers and a more robust estimation strategy, find that more stringent regulations increase the fraction of centers that are of sufficient quality to be accredited by an external and independent accrediting agency, although these increases accrue disproportionately to higher-income markets. Finally, we note that Currie and Hotz (2004) find that more stringent regulations improve the safety of child care centers, reducing the incidence of accidents in child care centers requiring medical attention.
In summary, the evidence suggests that more stringent regulations provide mixed benefits. While such regulations do appear to reduce the exposure of children to providers with unacceptably low levels of quality, they also tend to induce substitutions on various margins that, on average, tend to benefit children and parents from more advantaged backgrounds. As such, regulating child care services appears to be, at best, a rather blunt policy instrument for improving the quality of child care, especially for disadvantaged children.
Effects of state QRISs
In a recent study, Herbst (2018) examined the effects of the presence of QRISs in states on child care choices, maternal employment, and the supply and compensation of child care workers. Using the variation in when states rolled out their QRIS over time to identify these effects, Herbst finds that the presence of a state QRIS increases the probability of parents using nonparental forms of child care, although he finds that high-income families are more likely to use formal modes of care (child care centers), while low-income households are more likely to use informal modes of care, that is, family child care homes. He also finds that the presence of a state QRIS increases weeks worked and hours of work of mothers, but these effects are only for high-skilled mothers. Finally, Herbst finds that the presence of state QRISs increases the qualifications of child care workers.
In another recent study, Bassok, Dee, and Latham (2019) more directly examine the effectiveness of QRISs in stimulating the improvement of quality of child care providers. Recall the QRIS logic model discussed above. It presumed that QRISs would incentivize lower-rated child care providers to improve the quality of their services in response to parental use of higher-rated providers. Using data for North Carolina, Bassok, Dee, and Latham (2019) find that lower-quality providers do experience declines in enrollment after the implementation of that state’s QRIS and that these declines were larger in markets with greater concentrations of other providers.
While the findings of Herbst (2018) and especially Bassok, Dee, and Latham (2019) are promising for the potential of the QRIS logic model to improve the quality of child care services, more evidence is needed on the impacts of these systems on the supply and demand (by parents) of higher-quality child care services before one can draw reliable conclusions.
Finally, we note the cautionary nature of the findings of Quick et al. (2016) in their assessment of California’s QRIS. As they note, California’s ratings of providers did not include measures of “process quality,” such as measures of child interactions with teachers and other children and the overall classroom environment. Research has found that such measures are more predictive of cognitive and behavioral outcomes than measures of structural quality (Sabol et al. 2013). Furthermore, Quick et al. find that parents were either unaware of the relevance of such developmentally based measures for child care or tended to place greater value on other dimensions of their providers, such as proximity to workplaces and convenience of hours. The latter findings suggest the need to educate parents on the benefits of developmentally enriched child care services and on how to use information in QRISs to identify facilities that provide them.
Options for Reforming Child Care Policies
Our discussion of reforms focuses on three kinds of policy interventions: (1) direct provision of child care services by government, (2) expanding and better targeting child care subsidies and tax credits, and (3) improving the information that parents have about the quality of child care provider services. For each, we evaluate specific policy reforms, assessing their promise and their potential drawbacks for addressing the major policy objectives discussed above: (1) increasing maternal employment among low-income families, (2) reducing the exposure of the young children in these families to poverty, and (3) improving the development of these children.
We do not include possible reforms to existing state regulations of child care providers. While reforms are possible in this domain, the existing evidence summarized above indicates that without coupling them with some combination of the reforms we do consider, increasing the stringency of regulations is not likely to significantly produce developmentally relevant improvements in quality and is likely to exacerbate low-income families’ access to affordable child care.
Policy reform 1: Direct provision: Expanding Head Start or universal child care
We first consider policy reforms in which there is an active government role in providing child care, either through a targeted expansion of Head Start to all children in poverty or through an expansion to a universal program offered to all children, as in many other countries. With respect to targeted policies, our review of the existing evidence, both for the United States and elsewhere, indicates that low-income and disadvantaged families tend to benefit the most, both in terms of increasing maternal employment and child development. Thus, on economic efficiency grounds, targeting child care policies for such families clearly makes sense.
To calculate the cost of expanding Head Start to all 3.8 million children living in poverty in 2018, 24 we start with computing the per hour cost of the current Head Start program, which is not directly available from government statistics. We estimate that the hourly cost of Head Start is about $5.92 per hour. 25 This is an expensive per hour rate, higher than the median price paid per hour by high-income households on the private market. 26 The high cost likely reflects the relative high quality of Head Start care and the range of health and other services Head Start provides to their participating children and families. The cost of covering all children under age five living in poverty with a full-time (40 hours) and all year (52 weeks) offer of child care would then be $47.12 billion, 27 or a cost per child per year of $12,313. This is the total cost assuming that every child participates. Subtracting the funding Head Start already receives and funding from other state and federal programs that this program would replace, and taking into account that take-up would not be full, the new funding required could be between $10.5 to $25 billion, implying the expanded program would need between two and four times the current budget. 28
If all 20 million children under the age of five in the United States were to be provided access to and took up a universally available program of child care at the cost of Head Start, the total cost would be approximately $246 billion. The new funding required would likely be between $100 and $175 billion, given that take-up would likely be less than 100 percent and netting out the cost of existing governmental programs (primarily Head Start, CCDF, and CDTC) that would no longer be needed. Even with these adjustments, this would be an expensive program. Furthermore, existing evidence suggests that many households, particularly higher-income ones, would not experience any increases in maternal employment nor improvements in child outcomes, as this program would simply substitute subsidized care for high-quality parental or nonparental care that high-income households already provide for their children. On the other hand, universal policies do have a number of potential advantages, even if they are not as efficient as targeted ones. For one, the administrative burden of checking eligibility is eliminated. In addition, universal programs would eliminate any incentives for households to reduce or stop working to qualify for means-tested assistance. Universal programs also may reduce the stigma of program participation, extending care to households who might otherwise be reluctant to enroll.
Policy reform 2: Subsidizing child care costs
An alternative to the direct provision of child care services is to subsidize these services through vouchers under CCDF-funded programs and the tax treatment of child care expenses through the CDCTC. The evidence reviewed above indicates that providing CCDF-funded vouchers to low-income families increases maternal employment, while the existing CDCTC also increases the labor supply of mothers in households with sufficient tax liabilities to be eligible for the credit. Recently, Ziliak (2014), Children’s Defense Fund (2015), Hamm and Martin (2015), and Cascio (2017b) have proposed to expand the coverage for CCDF-funded subsidies or make the CDCTC refundable and better target its coverage to increase maternal employment of low-income families and thereby reduce poverty. We focus on proposals to reform these two subsidy programs evaluated in the National Academies of Sciences, Engineering and Medicine (2019)—hereafter the “Poverty Report”—to reduce childhood poverty in the United States. We briefly describe each.
The first proposal would expand child care subsidies under the CCDF to cover families with earnings less than 150 percent of the federal poverty threshold, while keeping state subsidy rates (and, thus, state copayment rates) at current levels. (Recall that states are currently given discretion in determining the income eligibility of CCDF-funded child care subsidies, and most states do not cover families up to the 150 percent poverty threshold.) Allowing for employment responses of families newly eligible for a child care subsidy, the report estimated that this proposal would reduce the child care expenses of working single mothers with children under 12 by 16.6 percent and by 0.6 percent for married mothers, and would increase the employment of single mothers by 237,000 (3.3 percent of this group’s prereform employment) and 15,000 (0.11 percent) for low-income married mothers. This expansion of CCDF subsidies would increase annual net labor earnings of low-income families by $4.2 billion. However, this policy reform would have only a modest impact on child poverty, reducing the current childhood poverty rate of 13 percent by 0.6 percent. This very modest reduction in child poverty is due, in part, to the fact that the subsidy is only a partial one, with newly employed parents having to pick up any remaining costs of child care. Finally, this expansion of CCDF-funded subsidies would increase annual net costs to government by $6.9 billion.
The Poverty Report also examined making the CDCTC fully refundable and better targeting it to benefit low-income families. Their proposed reform would (1) increase the maximum credit for one child from $3,000 to $4,000, keeping the maximum credit for two or more children at $6,000; and (2) increase the credit rate to 100 percent of qualifying child care expenses for AGI under $25,000 among families with children under age five, and then reduce the credit by 10 percentage points for each $5,000 of additional income, eliminating the credit for AGIs above $70,000. 29 (Recall that the existing credit only credited 35 percent of qualifying expenses for AGI below $15,000; reduced the credit to 20 percent for AGI at or above $43,000; and, because the CDCTC is currently nonrefundable, only offset families’ positive federal income tax liabilities.)
Again allowing for employment responses, the Poverty Report estimated that this reform would reduce the child care expenses of low-income single mothers by 42.6 percent and increase maternal employment by 8.5 percent. Although it also would reduce the child care expenses of low-income two-parent households by 16.6 percent, maternal employment for this group would actually decrease by 128,000 or 1 percent of this group’s prereform employment level. This reduction in employment is due to the fact that some lower-income intact families would no longer be eligible for the CDCTC, given its phase-out for AGIs above $70,000. Nonetheless, labor earnings of all low-income families would increase by $9.3 billion, producing a modest reduction in child poverty of 1.2 percentage points. The net cost to government of this reform would be $5.1 billion, which is substantially less than the increase in labor earnings it is projected to generate. In short, making the CDCTC refundable, more progressive, and better targeted to low-income families would significantly reduce the child care cost burden facing low-income families in the United States, facilitate maternal employment, and increase these families’ capacity to provide for themselves and their children.
Although making the CDCTC refundable and better targeted would raise maternal employment and labor earnings among low-income families, it need not improve the quality of the care received by the children in these families. This depends on whether parents use the subsidies to purchase higher-quality care. Recognizing that parents may not choose to invest in higher-quality care, several of the proposals for reforming the CDCTC also would change current qualifying child care expense provisions of the credit. For example, Ziliak (2014) has proposed to have a larger credit for parents who use licensed, center-based care, and a recent proposal by Hamm and Martin (2015) would require that CDCTCs only support expenses for child care facilities with high ratings in state QRISs.
Requiring or incentivizing low-income parents to purchase higher-quality care by such changes in the qualifying child care expenses for CDCTCs has some potential drawbacks. The Ziliak (2014) and Hamm and Martin (2015) proposals would require the IRS to verify the licensing or ratings status of child care providers from local administrative records, imposing additional administrative burdens on the IRS. These costs will be high in the short run, given that not all states have QRISs and most of them are relatively new. Also, as noted above, licensing requirements for centers or QRIS ratings may not yet be good measures of developmentally relevant quality. Finally, the findings of Hotz and Xiao (2011) that stringent regulations restrict the availability of high-quality child care in poor neighborhoods are likely to make it more difficult for low-income working families to qualify for CDCTCs that are limited to licensed or highly rated providers. For all these reasons, changing the current definition of qualifying child care expenses for CDCTCs seems premature at best. However, in the next section, we discuss ways to foster parents’ greater use of high-quality care by improving the information they have about the quality of care and the ways they use it.
Policy reform 3: Improving quality through better information
Finally, we consider the issue of improving the quality of child care used by low-income families beyond the direct provision of high-quality care discussed under reform 1. Recall one of the theoretical justifications for imposing minimum standards was to mitigate the presumed informational deficits parents have with respect to the quality of potential child care providers. An alternative way to address these deficits is to provide parents with credible information about the provider quality so that parents become more informed consumers. This is the logic model for QRISs (see Figure 6).
However, QRISs are at an early stage of development and face several challenges. First, as already noted, QRIS ratings are primarily based on measures of “structural” factors (e.g., child/staff ratios, staff education, group size) rather than measures of process quality, and only the latter have been found to be predictive of children’s cognitive, emotional, and social development. That said, process quality measures have not been used to construct QRIS ratings of providers, in large part because they require professionals to visit and directly observe the interactions and environment of the child care facility. Second, there is a lack of consensus of what process measures to include in ratings. Third, currently, provider participation in state and local QRISs is voluntary and includes only a fraction of providers. Finally, the Quick et al. (2016) findings, and those by Cryer and Burchinal (1997) and Mocan (2007), show that parents’ knowledge of and preferences for these developmentally based dimensions of child care services limit their likely impact on parents’ child care decisions even if they were included in provider ratings.
Given these challenges, we do not recommend that our proposed reform of the child care tax credit (reform 2) require that low-income working families can only claim expenses from highly ranked child care providers. At least not initially. But we do see real merit in the QRIS logic model for improving the quality of child care that low-income children experience, even if programs, like Head Start or other publicly provided child care, are expanded (reform 1). Therefore, as the third element of our proposed reforms, we recommend that the federal government, presumably under the CCDBG Act, expand and sustain its support for the development of state and local QRISs but, in addition, include additional funding for research in two areas.
The first area for research is to develop and validate measures of process quality that can be implemented at the provider level in a cost-effective manner. This will require adaptation and subsequent revalidation of existing process quality measures 30 and exploration of alternative strategies for their reducing their costs of collection so that assessments can be conducted of existing and new child care providers regardless of their size or ownership structure.
The second area is to evaluate ways of increasing parents’ awareness and understanding of the importance of early child development and, more importantly, about the relative effectiveness of different features of child care settings for facilitating such development, so that parents can make more informed child care choices and better monitor the providers they do choose. On the latter, recent studies, from Dechausay and Anzelone (2016) for example, which evaluated alternative strategies adapted from the behavioral sciences to help educate parents eligible for CCDF subsidies, should be expanded, and states should be encouraged to undertake formal evaluations of these strategies to improve the knowledge base of best practices in this area.
We are not able to provide estimates of the funding needed to support these lines of research. But we encourage the federal government to develop a sustained research program for each, incentivize states to undertake such studies, and require that credible methods be used to evaluate them.
Conclusion
Decades of research have provided strong evidence that programs, like Head Start, that provide high-quality child care to low-income households have positive effects on child development and long-term outcomes. Research also suggests that expansions of the existing child care vouchers (CCDF) and making the existing child care tax credits (CDCTC) refundable and better targeted to low-income families would significantly reduce the cost of child care for low-income families and facilitate maternal employment. However, expansions of these voucher and tax credit programs alone may have only small positive effects, and perhaps even negative ones, on child development if increasing the generosity of these programs causes households to switch away from higher-quality forms of care toward subsidized lower-quality ones. We therefore recommend the pairing of subsidy expansions with programs that increase the take-up of higher-quality forms of child care. Rather than directly increase regulatory stringency in a few domains, an alternative approach that seems promising is to expand and sustain support for the development of state and local QRISs to provide better information to parents on the quality of child care options and to better educate parents on its importance.
Footnotes
Note:
We thank Jim Ziliak and Robert Moffitt for comments on earlier drafts, Janet Currie and Melissa Kearney for their comments, and especially Aaron Sojourner for his extensive comments on an earlier draft of the article.
Notes
V. Joseph Hotz is the Arts & Sciences Professor of Economics at Duke University and a faculty research associate of the National Bureau of Economic Research. He is an applied microeconomist who conducts research on education, the family, and social policy; and on the development of applied econometric methods.
Matthew Wiswall is the Juli Plant Grainger Professor of Economics at the University of Wisconsin–Madison and a faculty research associate at the National Bureau of Economic Research. He is an applied microeconomist who conducts research on child development, education, and applied econometric methods.