
Abstract
To better focus efforts in recruiting psychoanalytic candidates, current candidates’ demographics, practice patterns, and satisfaction with psychoanalytic training were investigated. An anonymous web-based survey was distributed by e-mail to all candidates subscribing to the affiliate member e-mail list in 2009–2010. Surveys were completed by 226 of 565 affiliate members, for a return rate of 40%. The majority of respondents were women 45 to 64 years of age, married, with a doctoral degree, in private practice, with an annual household income of over $100,000. Most candidates devoted 11 to 30 hours a week to training and had no analysts or candidates in their workplace. Almost half had considered training for more than four years before matriculation, with financial issues cited most frequently as delaying entry. Over 80% of respondents were satisfied with their training. The most frequently cited reasons for dissatisfaction were a negative institute atmosphere, concerns about teaching or the curriculum, and difficulty finding cases. Candidates in training for eight years or more accounted for almost 20% of the group and were more often dissatisfied with training. This study demonstrates that the majority of current candidates are satisfied with training but suggests that recruitment may become increasingly difficult unless factors related to time, cost, case finding, graduation requirements, and institute atmosphere can be addressed.
Increasing concern has been expressed about the decline in both candidate enrollment in psychoanalytic training programs and membership in the American Psychoanalytic Association (APsaA). Over ten years, there has been a 12% decrease in APsaA candidates, from 952 in 1999–2000 to 836 in 2009–2010. In addition, there has been a 13% decline in candidate membership in APsaA, with 81% of candidates belonging to APsaA in 1999–2000, but only 68% in 2009–2010 (Debbie Steinke, personal communication, 2011). In 2010, thirty candidates abandoned their training, and over a hundred members resigned from APsaA (Warren Procci, personal communication, 2011). Recruitment and retention of candidates are serious problems. These trends are particularly disturbing, since candidates represent the future of psychoanalysis as a discipline and as a profession.
A variety of social and economic forces have contributed to the decline in interest in psychoanalytic training, including the emphasis on empirically proven treatments by mental health training programs and insurers, increasing use of psychotropic medication, and reduced third-party reimbursement for outpatient treatment. In addition, mental health trainees today may have less exposure to psychodynamic supervisors and less experience practicing psychodynamic psychotherapy, may engage less often in personal treatment, and may feel less confident in their psychodynamic skills (Habl, Mintz, and Bailey 2010; Katz and Kaplan 2010; Katz, Tuttle, and Housman 2011). Despite these factors, there is still strong interest, at least among psychiatrist trainees, in psychoanalytic concepts and psychodynamic psychotherapy, but considerations of cost and time deter many residents from applying for psychoanalytic training (Katz and Kaplan 2010). A recent study (Damsa et al. 2010) describes an effort—using exploratory seminars with psychiatric residents and discussions with psychoanalytic psychotherapists from several countries—to determine which factors prevent residents from pursuing psychoanalytic training. The authors debated the feedback from residents and therapists and arrived at several conclusions. These included concerns about the closed-mindedness, dismissive behavior, and rigid beliefs of many psychoanalysts, especially regarding the need for empirical evidence that psychoanalysis is effective, and about the lack of openness and clarity in teaching psy-choanalytic concepts in a way grounded in clinical reality. These are certainly not new or surprising observations by nonanalysts about the psychoanalytic establishment, but with the declining numbers of mental health professionals who see psychoanalytic training as instrumental to career satisfaction, it is urgent that we recognize and respond to such criticism.
While there have been many critiques of psychoanalytic education (Auchincloss and Michels 2003; Kernberg 1996, 2000, 2006, 2007, 2010; San Martino 2003; Wallerstein 2007), few studies address candidates’ perceptions of their training experience (Bosworth, Aizaga, and Cabaniss 2009; Cabaniss, Glick, and Roose 2001; Cabaniss and Roose 1997; Cabaniss et al. 2003; Ward, Gibson, and Miqueu-Baz 2010). A recent survey of candidates at the British Psychoanalytical Society (Ward, Gibson, and Miqueu-Baz 2010) demonstrates that candidates overall have a positive experience of training, with concerns expressed by a minority. When concerns were expressed, however, the negative experiences reported were recognized and keenly felt by the peer group. Although the structure of training is different in the British Society, this study demonstrates that concerns about abuse of power and subsequent compliance, submission, and fear among candidates (Casement 2004) prove largely unwarranted when candidates are surveyed directly. This study underscores both the importance of hearing directly from candidates about their training experience and the complexity of the data elicited.
In contrast to the postwar era, when candidates for psychoanalytic training abounded, the number of candidates in International Psychoanalytical Association (IPA) training programs has decreased (Widlöcher 2005). A variety of initiatives have been developed to enhance recruitment of analytic candidates in the U.S., including local and national fellowship programs, initiatives in undergraduate education, institute psychotherapy programs, and programs to enhance the skills of teachers of psychotherapy. Since there is little information on the demographics or professional backgrounds of current applicants for training and what factors influence entry into and progression through training, it is unclear what impact these programs have or whether they are well targeted. This study was designed to evaluate the demographics of current candidates, the time commitment and financial resources required of them, the factors that facilitated or deterred their entry into training, their level of satisfaction with their education, and the factors associated with failure to graduate or progress in training.
Method
An anonymous web-based survey was distributed by e-mail to all candidates subscribing to the affiliate e-mail list in 2009–2010. Participation was voluntary, and no financial incentive was offered. The survey consisted of twenty-four questions answered using a 5-point Likert scale, with many questions allowing open responses. IRB approval was obtained from the University of Kentucky Office of Research Integrity (IRB # 09-0587-X6B). In the findings, sample size may vary since some respondents left questions unanswered.
Results
Response Rate, Demographics, and Setting
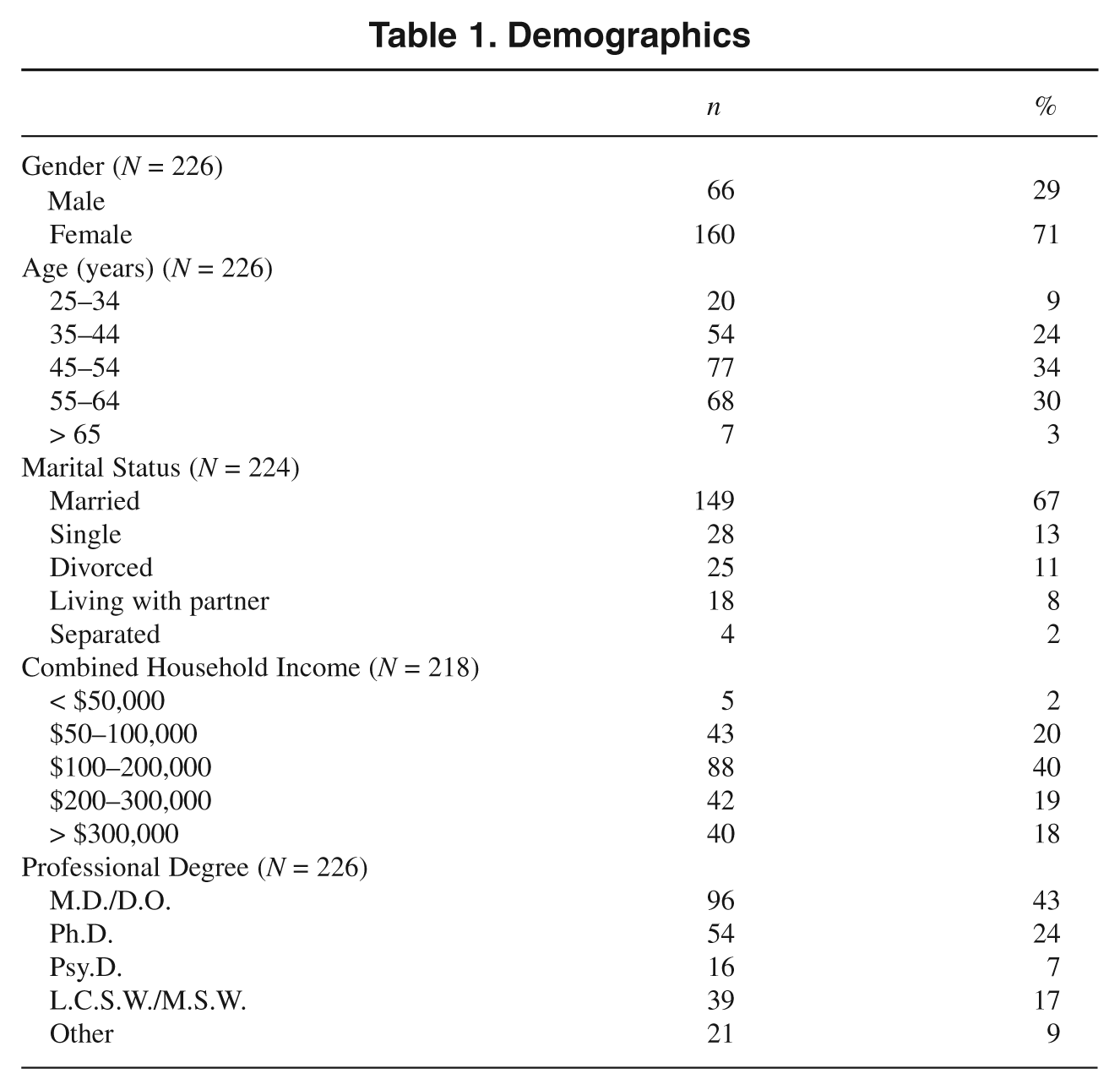
Surveys were completed by 226 of 565 affiliate members, for a response rate of 40%. Demographic data are presented in Table 1. Of the respondents, the majority were women (71%) between the ages of 45 and 64 years (64%). Over two-thirds were married (67%), with an annual household income of $100,000 or more (77%). Over one-third (37%) had annual household incomes of more than $200,000. Only five candidates (2%) earned less than $50,000 annually. The largest group of respondents were M.D.s or D.O.s (43%), followed by Ph.D.s (24%) and social workers (17%). Twenty-one respondents (9%) had other degrees including doctorates (e.g., Ed.D.s and J.D.s), masters degrees (e.g., in marital and family therapy or counseling psychology), or combined degrees (e.g., an M.D. and a Ph.D.).
Demographics
Geographic and practice information is summarized in Table 2. The majority of respondents came from the Northeast (44%), followed by the Midwest (23%), the West (13%), the Northwest (9%), the South (8%) and the Southwest (5%). The majority of candidates saw analytic patients in private or home offices (79%, 7%). Of note, eight candidates (4%) saw analytic patients by telephone or videoconferencing. Of the 206 respondents to this question, 28 (14%) gave write-in responses, with 25 (12%) stating they did not yet have an analytic case.
Practice setting

The majority of candidates had no analytic colleagues in their work setting, with 145 of 206 (70%) having no analyst colleagues and 163 (79%) having no candidate colleagues. Forty-three of 206 candidates (21%) had one to three analyst colleagues and 34 of 206 (17%) had one to three candidate colleagues in their work setting. When these percentages were combined, over 90% of candidates had three or fewer analyst or candidate colleagues in their work setting, with most having none.
Time
Temporal data collected included length of time candidates considered training before applying, time spent commuting, time devoted weekly to training activities, and the length of time respondents had been in training.
Time before starting psychoanalytic training
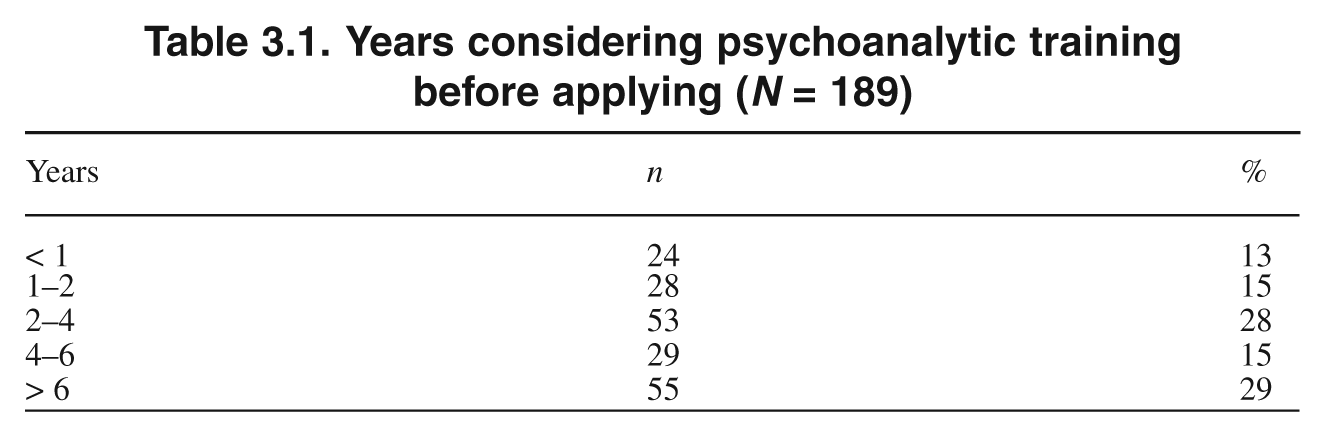
Candidates were asked how long they had considered psychoanalytic training before applying and what factors might have enabled them to enter training sooner (Tables 3.1 and 3.2). Few candidates made quick decisions to enter training, with 29% considering it for more than six years, 15% for four to six years, and 28% for two to four years (Table 3.1). Thus, almost half (44%) considered psychoanalytic training for four or more years before applying and almost three-fourths (72%) for more than two.
Years considering psychoanalytic training before applying (N = 189)
Factors preventing earlier entry into psychoanalytic training (N = 134)
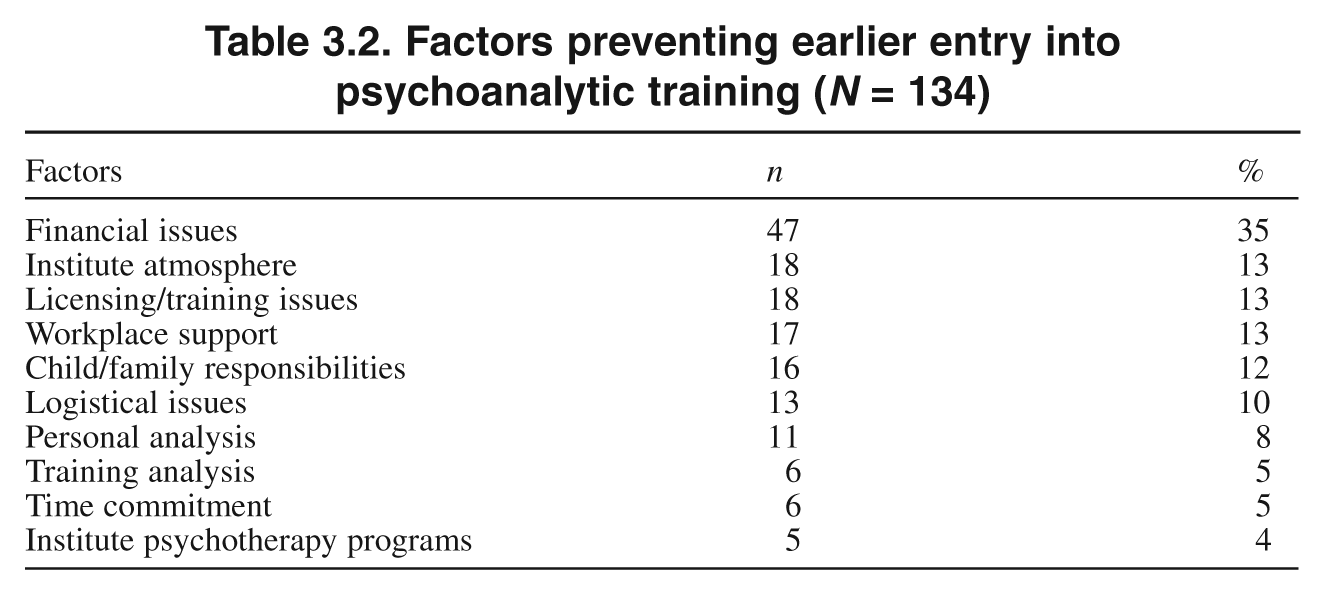
One hundred fifty-two of 226 candidates (67%) responded to an open-ended question regarding what might have enabled them to start training sooner. Eighteen of the respondents (12%) stated there was nothing that would have enabled them to start sooner (e.g., they started training when they were ready or at an appropriate time in their career). For the remaining 134 respondents (88%), narrative comments were analyzed regarding factors that prevented them from starting training sooner (Table 3.2). Some candidates mentioned more than one factor in their narrative responses, thus accounting for more than 134 responses. The most important factors cited included (1) financial issues (e.g., need for a better financial situation and higher income, scholarship support, and/or lower supervisory and training analysis fees): 47/134 (35%); (2) institute atmosphere (e.g., unwelcoming environment, a perception of “elitism,” wishes for more guidance, outreach, flexibility, and information, bias toward lesbian, gay, or nonmedical candidates): 18/134 (13%); (3) licensing or training issues (e.g., need for proper credentials, resolution of waiver issues, accepting social workers as candidates): 18/134 (13%); (4) workplace support (e.g., encouragement from employer, accommodations in schedule, assistance with practice-building, support for analytic training instead of a psychotherapy program): 17/134 (12%); (5) child-rearing or family responsibilities: 16/134 (12%); (6) logistical issues (e.g., establishing a practice, proximity to an institute, waiting for an institute class to start): 13/134 (10%); (7) issues regarding the personal analysis (e.g., starting sooner, meeting the frequency requirement, making more progress before applying): 11/134 (8%); (8) concerns regarding the training analyst requirement (e.g., need to change analysts before beginning training, the wish for more flexibility with the TA requirement, the need to wait for an analyst to become a TA): 6/134 respondents (5%); and (9) concerns about the impact of institute psychotherapy programs (e.g., delaying entry into psychoanalytic training): 5/134 (3%).
Commuting
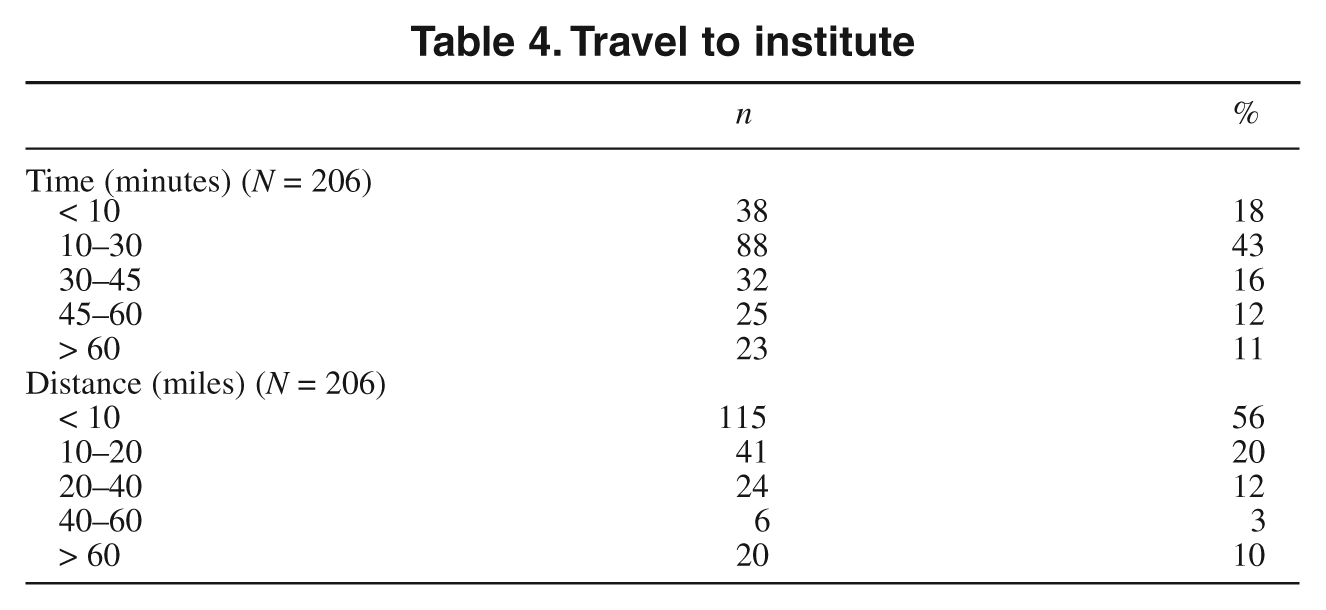
Most candidates had a reasonable commute to their analytic institute (Table 4). The majority of candidates had a commute of less than thirty minutes (61%) or less than ten miles (56%), although a small percentage (11%) had a commute of greater than sixty minutes or traveled more than sixty miles (10%). In written responses, those with longer commutes reported traveling distances of eighty-five to three hundred miles, commutes of up to three hours each way, and travel by taxi, public transportation, or air. One candidate’s commute involved a border crossing.
Travel to institute
Time devoted each week to training
Candidates were asked how much time they devoted each week, outside of commuting, to analytic training activities (e.g., personal analysis, supervision, classes, etc.). It appears that candidates spend a significant amount of time in these activities (Figure 1). The majority (52%) spend between 11 and 20 hours a week and the next largest group (20%) 21 to 30 hours a week. Analytic training requires a significant time commitment, with 80% of the group spending over 11 hours a week on training.
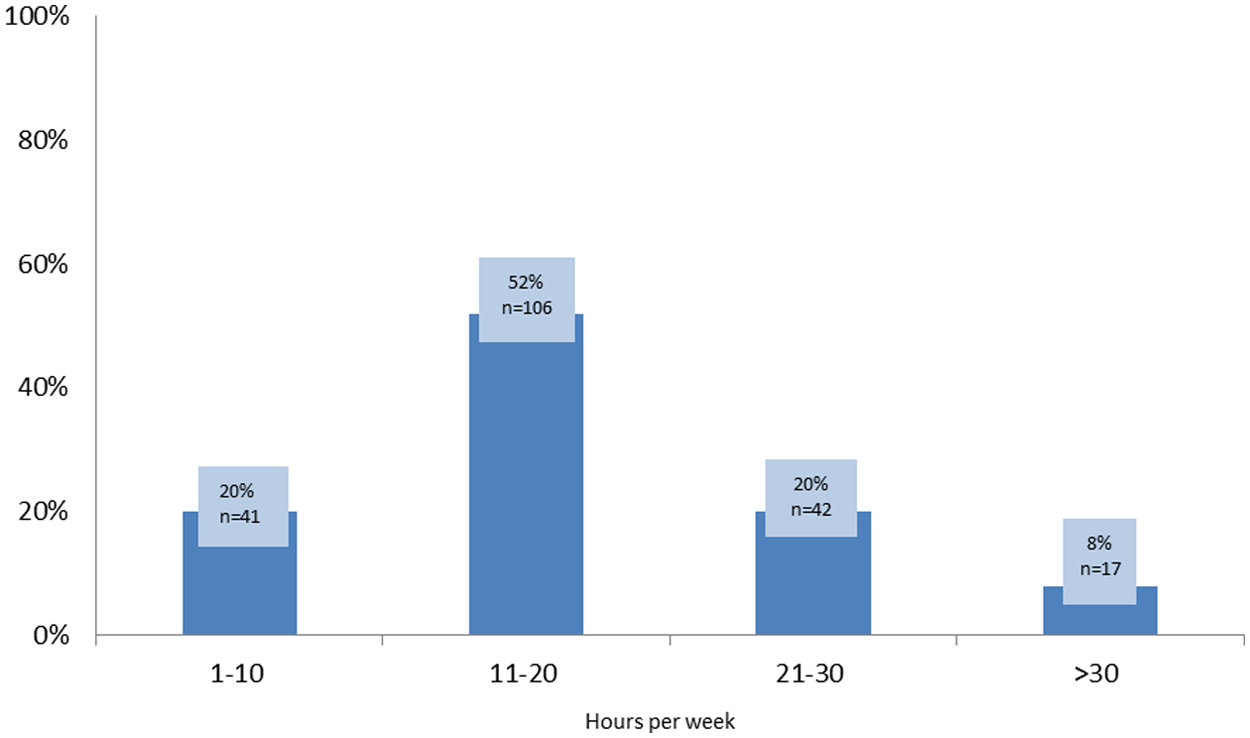
Hours per week on psychoanalytic training (N = 206)
Duration of training
With regard to years in training, this sample displayed a bell-shaped curve (Figure 2), with the median time in training being three to five years. Approximately two-thirds of the candidates surveyed (62%) had been in training for five years or less, and approximately one-third (38%) for more than five. Forty-two of the 226 respondents (19%) had been in training eight or more years. Of this group, 30 (13%) had been in training for eight to twelve years, and 12 (5%) for more than twelve years.
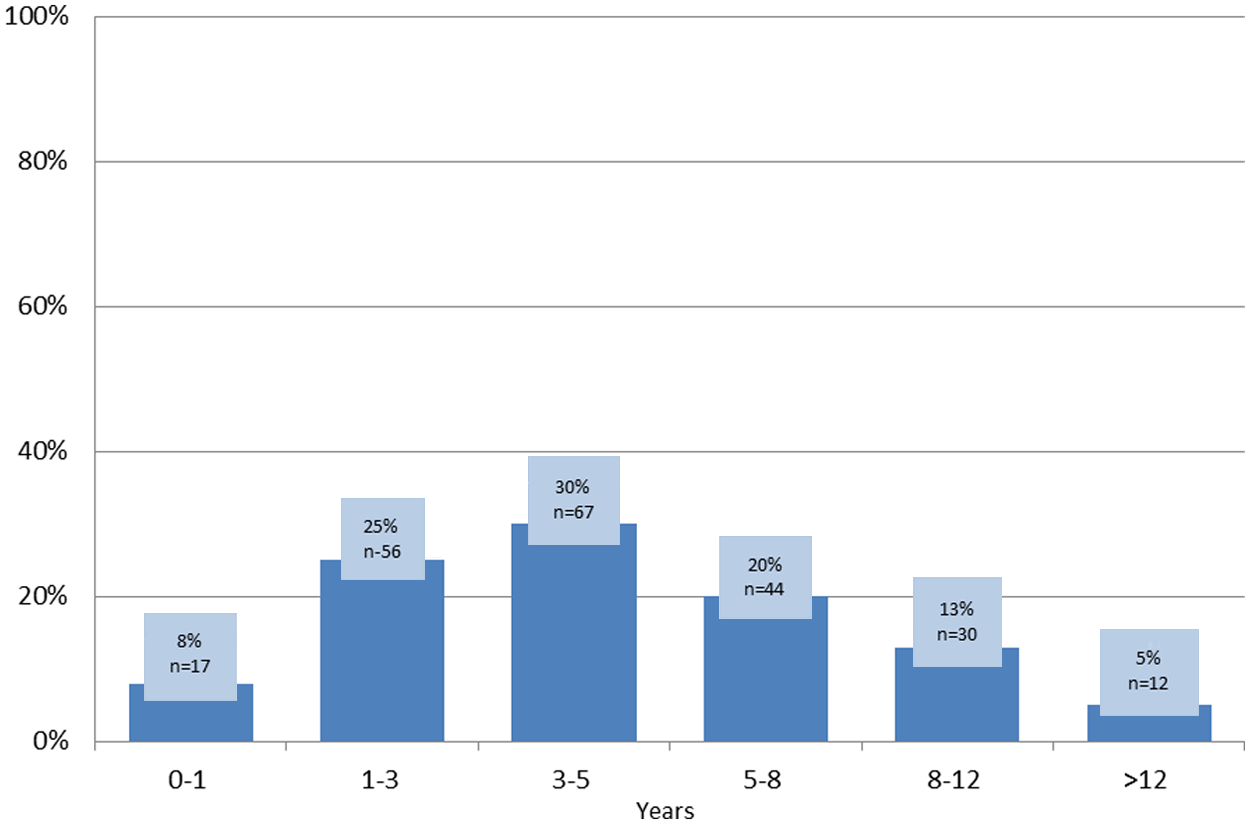
Years in Training (N = 226)
The group in training more than eight years (the “long duration” group) was compared with the group in training less than eight years (the “short duration” group). Pearson chi-square tests were used to assess statistical significance between the long and short duration groups in a variety of areas. Significant findings are included in Tables 5.1–5.4. Table 5.1 shows that those in the long duration group were significantly older (p < .0001), with only 2% under 45 years of age, compared to 40% of the short duration group. Table 5.2 shows that the long duration group were more dissatisfied with training than the short duration group (p < .0001). Tables 5.3 and 5.4 show that the long duration group had significantly more negative personal interactions at their institutes (p = .0143) and expressed significantly more concerns regarding graduation requirements (p = .0062) than the short duration group.
Age vs. duration of psychoanalytic training (N = 226)

p< .0001
Satisfaction vs. duration of psychoanalytic training (N = 89)

p< .0001
Negative personal interactions at institute vs. duration of training (N = 188)

p = .0143
Concern about graduation requirements (N = 187)
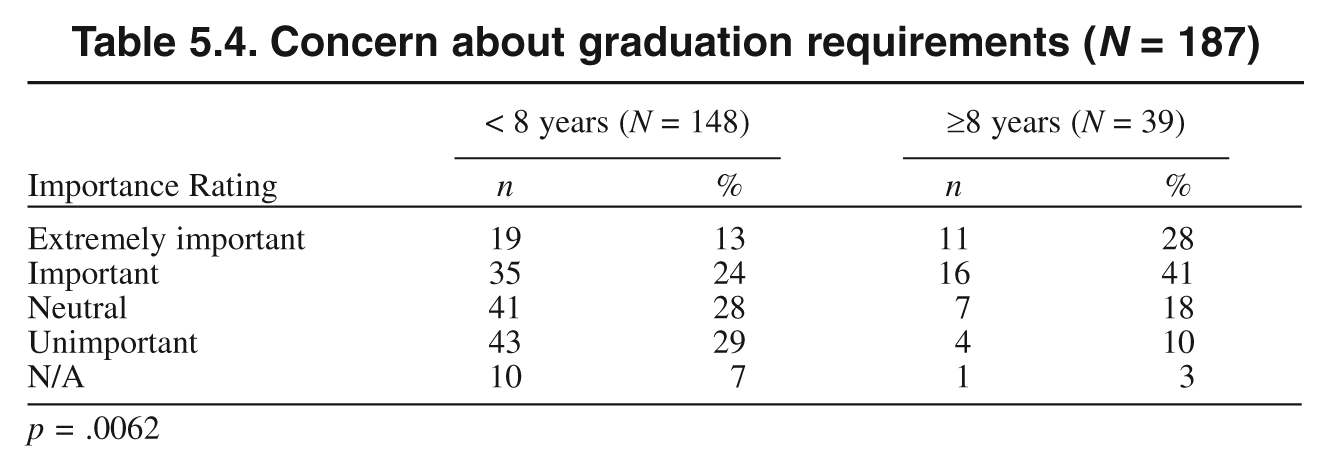
p = .0062
Satisfaction
The majority of candidates were very satisfied (41%) or moderately satisfied (41%) with their training (Figure 3). While 82% of candidates expressed satisfaction, 4% were neutral, 11% were moderately dissatisfied, and 2% were very dissatisfied. Thus, 13% of the entire group were dissatisfied to some degree with their training experience. This question inspired 43 of 189 respondents (23%) to write comments, with 14 of these (33%) including comments regarding positive aspects of training. Examples of positive comments include the following:
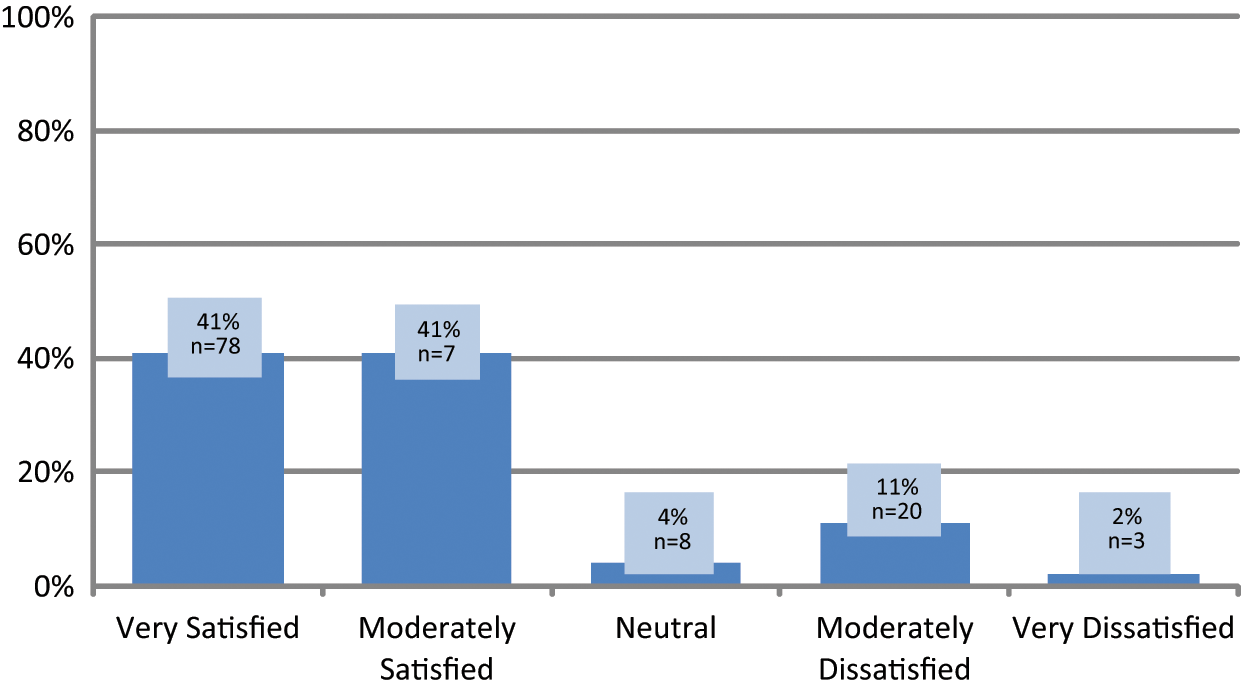
Satisfaction with psychoanalytic training (N = 187)
“The best thing I ever did for myself in my life.” “Outstanding clinical experience with my psychoanalytic patients, great supervision, great classes, great colleagues.” “Very satisfied with TA, supervisor, advisor, research mentor and most of the teachers.” “Love my analyst and like my classes.” “Courses are wonderful and the institute has been very enthusiastic and supportive of candidates.”
Of the thirty comments (70% of the 43 write-ins) that touched on negative aspects of training, eleven (26%) cited a negative institute atmosphere, including “lack of true support or concern by local officers of the education committee,” “rigid rules,” disruptive experiences such as boundary violations or analysts with dementia, unclear criteria for progression and graduation, late notice of the need for additional cases, “political battles about the TA issue,” “lack of ability to progress,” and theoretical battles among institute faculty. Concerns about the curriculum or teaching were expressed in ten comments (23%), citing “lack of curriculum organization,” “too much reading,” “little assistance in metabolizing all the disparate works assigned,” “too many classes,” “some classes that are patronizing and repetitive,” “poor quality of instruction,” “too much ego psychology,” “course work that is too simplified and not theoretical,” and “the wish for more diversity of models taught on a clinical and theoretical level.” Difficulty finding cases was expressed in nine comments (21%), with concern expressed about requirements for the number and frequency of control cases (e.g., the need for both genders, number of cases needed to graduate, three vs. four times weekly), financial and insurance issues interfering with the ability to start control cases, the problem of finding appropriate cases, and the need for more help from institutes and low-fee clinics in publicizing treatment or referring patients. Of the remaining comments, six (14%) expressed concerns about strained relationships or the perception of a lack of concern by faculty, and four (9%) expressed concerns about issues related to the training analysis (e.g., an analyst who developed dementia, the personal and institute impact of a TA who abruptly terminated an analysis, political battles over TA issues, lack of benefit from the personal analysis). Examples of negative comments include the following:
“Certain individuals among institute faculty have been dogmatic and hostile to ideas diverging from their own, thus squelching independent ideas.” “Too expensive for young professionals.” “The field is a mess, and the institutes are in turmoil. It is hard to get cases, at least for me, as patients have not heard of analysis and I have to develop them slowly. Lots quit therapy when I bring up frequency or analysis—others quit analysis for one or the other reason. It has been tough.” “The quality of instruction is poor. Most classes consist of my classmates and I discussing what we’ve read. Only two of our teachers so far have contributed in the way of organization of material and didactics.” “So much disruptive stuff at my institute, I could write a book: training analyst booting a patient, unclear criteria for graduation, late notice I needed one more case, training analyst who abruptly ended analysis for ‘personal countertransference’ reasons, below-the-surface battle between Kleinians and others. Good grief.” “It’s hard finding control cases and the fact that insurers do not pay for analysis makes it difficult now and makes anticipating a future practice somewhat dim.” “There were constant unexplained hoops to go through which ultimately made it frustrating. Too little communication between the institute and the candidates. This was noted during a site visit with the recommendation to get the candidates more involved at every level.” “I was subject to a boundary violation and my training was very disrupted. It still is to a large degree although I am trying to finish—many problems.” “Obtaining three control cases for four-times-a-week analysis is unrealistic yet required. This delays graduation and makes training more difficult than it should be.”
Study Limitations
This study has several limitations. The survey had a 40% return rate. Online surveys have a 30% average response rate, and e-mail surveys a 40% average response rate (Instructional Assessment Resources 2010), making this survey’s response rate average. Since the survey was distributed through the affiliate members’ e-mail list, those who responded were, by definition, candidate members of APsaA. Data regarding nonrespondents or candidates not members of APsaA are therefore unavailable. Since most respondents were from the Northeast (44%) or Midwest (23%), it is possible that our findings are skewed by geographic factors. Our sample might overrepresent those motivated to complete the survey by frustrations they have experienced with training. It is equally possible that the sample overrepresents those more satisfied with and more engaged in training, since all in the group are APsaA members and responded to a survey request on the affiliate members’ e-mail list.
Questions that elicited written responses were difficult to quantify and were reported after coding the topics into recognizable groups. Candidates often reported on more than one topic in their narrative responses, which accounts for some questions having a larger number of responses than there were candidates answering the question. In addition, because questions that asked for a write-in response were not mandatory, candidates had to have the motivation to write in a comment. There was no multiple choice question asked about number of cases seen or difficulty finding cases. Since these figured frequently in the write-in responses, it would have been helpful had the survey elicited this information directly.
As there has been no previous national survey of candidates, there is no group to which our sample can be compared, which makes it hard to comment on trends (e.g., Are current candidates more or less satisfied than earlier groups? How do the demographics of current candidates compare with those of earlier cohorts?). Because there is no comparison group, the survey is difficult to analyze for statistical significance.
Discussion
As we have noted, this study is the first national survey of psychoanalytic candidates. This paper reports on demographics, practice patterns, and satisfaction with training. Part II of this study will report on motivations, obstacles, and ideas on increasing interest in psychoanalytic training. The findings from this study that are particularly relevant can be sorted roughly into four groups.
The majority of current candidates are women (71%), middle-aged or older (67%), with a doctoral degree (74%) and a household income greater than $100,000 (77%), and are in private practice (79%). The majority of candidates (more than 90%) practice in relative isolation, with few candidates or analysts in their workplace.
More than two-thirds of candidates (72%) contemplate psychoanalytic training for two or more years, and more than one-third (44%) for four or more years, before applying. Financial reasons are most frequently cited as the factor preventing earlier application. Training activities occupy a significant amount of time each week (11–30 hours) for the majority of candidates (72%).
The majority of candidates (82%) are satisfied with psychoanalytic training, with half of these (42%) being very satisfied and half (42%) being moderately satisfied. Of the 13% who are either moderately (11%) or very (2%) dissatisfied, the most frequently cited reasons for dissatisfaction were a negative institute atmosphere, concerns about teaching or the curriculum, and difficulty finding cases.
Candidates in training for eight years or more (the “long duration” group) accounted for almost 20% of the candidate group surveyed. They were older, more dissatisfied with training, had more negative interactions at their institutes, and expressed more concerns about graduation requirements than did candidates in the “short duration” group (p < .05).
This study shows that, once engaged, candidates are satisfied or very satisfied with their training. This confirms the results of another recent study showing that candidates overall are satisfied with their training (Ward, Gibson, and Miqueu-Baz 2010). This is reassuring in that, once enrolled in training, candidates find that the experience meets or exceeds their expectations. However, the factors identified in this study, particularly regarding cost and time, impact in a variety of ways on this group of candidates and will likely have a significant impact on the recruitment of candidates in the future. Current candidates have waited until later in life to undertake training and appear to need a high income to support their training. Since the majority of candidates today are middle-aged or older, the years they have to practice and the time and energy they have available to teach and mentor future generations are limited. The cost of training also likely limits potential candidates to those who are in private practice, make a sizable income, and whose household income includes that of a working spouse or partner. This may account in part for the preponderance of married candidates. That 77% of candidates have a household income exceeding $100,000 annually, with 37% earning twice that or more, makes it clear that psychoanalytic training is out of reach financially for those in residency or graduate school or with significant debt or expenses. Middle-aged candidates are more likely to have older or grown children and a more stable income, thus freeing up more time and financial resources for training.
The impact of cost and time may have unforeseen effects on the diversity of current candidates with respect to age, socioeconomic background, marital status, and work setting. For example, it would be much harder for a single candidate with young children working in a community mental health clinic or in the academic world to free up the time needed for training and to afford the cost. Candidates in private practice have the most control and flexibility with their schedules and may make higher incomes than those in salaried positions. In addition, the vast majority of candidates (90%) live within a reasonable commute of their analytic institute. Because of the time demands involved, analytic training for those living in areas distant from institutes would likely be quite challenging. These restrictions imposed by cost and time may have unanticipated consequences such as reducing the number of academics or researchers who enter training, limiting candidates to those without significant professional debt (which excludes most residents and graduate students) and favoring candidates with significant financial resources or a spouse, partner, or other family member who can carry the financial burden. These issues may have the unintended consequence, as well, of restricting candidates from racial, ethnic, sexual, or socioeconomic minorities or from cities distant from analytic institutes.
Although no data are available on the gender breakdown of earlier generations of candidates, there is a predominance of women candidates in this study that parallels the rise of women in mental health careers in general (American Psychiatric Association 2010; Center for Health Workforce Studies & National Association of Social Work Center for Workforce Studies 2006; Cynkar 2007; Jain and Ballamudi 2004; Pion et al. 1996). Recently there has been discussion in the popular media of the “feminization” of mental health care, leading to a decline in the number of male psychotherapy patients, which in turn may impact on the economics and possibly the prestige of the profession (Carey 2011). This has implications for role-modeling and recruitment, particularly of male candidates. There are no comparison data regarding gender breakdown to place against our findings, but a 2010 IPA survey reveals that its membership is 55% female and 45% male, with an average age of 62 to 65 years. It appears that the younger generation of candidates is more predominantly female than earlier cohorts, which may facilitate the continued entry of women into training. The average age of IPA members also speaks to the advanced age of current candidates and the trend for analytic training to be undertaken in the middle or later stages of one’s career.
In addition to a gender shift among candidates, a shift in professional background is evident. Limited data are available for past generations of candidates, but in 1993 a full 93% of candidates held a doctoral degree (75% M.D.s, 18% Ph.D.s) (Debbie Steinke, personal communication, 2011), as compared to the 77% in our study who hold such degrees (43% M.D.s, 24% Ph.D.s). While it may be hard to compare with any exactitude the percentage of candidates holding doctorates in 1993 and now, since our study includes Psy.D.s and those with combined doctoral degrees, it is noteworthy that 17% of current candidates are social workers. This speaks to the increasing diversity of candidates and to greater openness to trainees from a variety of backgrounds. It is also noteworthy that, possibly contrary to popular perception, the majority of candidates still do have doctoral degrees, though compared to the situation in the past there are now fewer M.D.s and more Ph.D.s. This has implications for local and national efforts to make and maintain contact with trainees in psychiatry and psychology programs and to stimulate their interest in psychoanalytic training.
The decline in M.D. candidates is of concern and is likely related to a variety of factors, including the impact of managed care, the increasing use of medication, a change in the role and identity of psychiatrists, the expanding use of mental health professionals from other disciplines to treat patients (Gabbard and Kay 2001), and the decline in psychotherapy provided by psychiatrists (Mojtabai and Olfson 2008). The current generation of leaders at APsaA institutes trained during the 1970s and 1980s, when traditional psychoanalytic practice was mainstream; unless actively working with students in various mental health fields, they may not recognize the extent to which today’s trainees lack exposure to psychoanalytic principles and technique. Moreover, fewer mental health trainees themselves undertake individual psychotherapy or psychoanalysis, lessening their exposure to psychoanalysts and the benefits of psychotherapy (Haak and Kaye 2009; Habl, Mintz, and Bailey 2010). This means that outreach must start at a much more basic level.
Concerns have been expressed about the state of psychodynamic psychotherapy training in residency programs (Drell 2007; Mellman 2006), but it appears that residents are still interested in practicing psychotherapy. A recent study of over two hundred residents from fifteen U.S. residency programs showed that 82% viewed becoming a psychotherapist as integral to their psychiatric identity, and that 54% planned to provide formal psychotherapy to patients after graduation (Lanouette et al. 2011). Another study, of seventy-five residents from five programs, showed that the majority of residents value psychoanalytic concepts and plan to incorporate psychodynamic psychotherapy into their careers but have little faith in the level of their skills or the adequacy of their training (Katz and Kaplan 2010). It appears that residents have interest in further training in both psychodynamic psychotherapy and psychoanalysis and are a group that can be engaged if barriers involving cost and time can be reduced, research evidence for psychodynamic treatments can be presented, and close, respectful relationships with analyst supervisors or mentors can be built (Damsa 2010; Katz and Kaplan 2010; Katz, Tuttle, and Housman 2011).
Since analytic training most frequently takes place in the postgraduate period, and usually long after formal training has finished, there may not be a cohort of other trainees with whom to share psychoanalytic interests. This study demonstrates that current candidates are relatively isolated, with 79% having no other candidates in their workplace and 70% having no analysts there. Over 90% have three or fewer analysts or other candidates in their workplace. This may be due in large measure to the fact that the majority of candidates today are in private practice, but it also speaks to the relative isolation of candidates more generally. Those not in private practice often must overcome the prejudice or misunderstanding of workplace colleagues in order to pursue training. Thus, positive interaction with analysts becomes even more important for candidates today. Likewise, negative interactions or experiences may take on increased significance, result in paranoia or distrust, and affect the candidate peer group if not addressed (Ward, Gibson, and Miqueu-Baz 2010).
The time demands of analytic training are significant and, in combination with financial factors, likely contribute to the long period it typically takes to decide to apply for training. Almost half the candidates in this study (44%) considered analytic training for four or more years before applying. Candidates had a lot to say about this issue, with 67% of the sample electing to write in a comment. Financial issues were the most frequent reason given for the delay in starting training, but issues such as institute atmosphere, licensing/training issues, workplace support, and child/family responsibilities were also important. Together these factors seem to have a cumulative effect.
Comments about institute atmosphere were particularly heartfelt, with remarks about feeling unwelcome, biases against lesbian, gay, or nonmedical candidates, perceptions of rigidity and elitism, a lack of flexibility regarding the cost of the training analysis and supervision, and a lack of honest information about the difficulties of training. This would seem a relatively easy area to fix, leading to a greater sense of collegiality and making the prospect of training more attractive. Of note, APsaA standards for certification and training analyst status and their impact on personal analysis were cited as obstacles by only a small minority of respondents. We suspect this illustrates the mismatch between the concerns of APsaA institute leadership and the needs of potential candidates. In addition, institute psychotherapy programs do not appear to siphon off potential analytic candidates or to prevent those who are interested from pursuing analytic training. If anything, these programs are an important means of generating interest in psychoanalytic training.
Several decades ago, when there were fewer APsaA institutes, candidates regularly traveled to get training, but at that time most candidates were men without primary responsibility for child care, and there was a much more robust market for psychoanalytic treatment. Today traveling to get training is a different matter for candidates facing an uncertain demand for psychoanalytic treatment once they graduate and for women with child care responsibilities. Most candidates in this study had a reasonable commute to their analytic institute, but a minority spent more than forty-five minutes commuting (23%) or traveled more than forty miles to their institute (13%). Some candidates regularly spent several hours driving to their institute or had to fly. One even had to cross an international border. These efforts speak to the commitment of many candidates to pursue training despite significant obstacles and to the importance of videoconferencing, telephone or shuttle analysis, and strong administrative oversight in planning schedules. They also suggest the potential for recruiting candidates outside the immediate area of the institute.
The study shows that analytic training requires a significant time commitment, with 52% devoting 11 to 20 hours a week to training and 20% devoting 21 to 30. Only 20% devoted fewer than ten. The time demands of training seem to be related not to stage of training but rather to the combination of personal analysis, cases, supervision, and classes. This study also lends support to the notion that mental health professionals who are starting practices cannot afford to devote so much time to nonremunerative activities, especially in the face of large student loans to be repaid and/or a young family to support. This clearly contributes to the typical delay in training until middle age or even later and to the long period spent contemplating the decision to undertake training. The fact that analytic institutes continue to recruit candidates despite the significant cost and time demands seems to attest to the power of the psychoanalytic experience and the commitment of candidates to their training.
Time also impacts on the satisfaction of candidates who cannot graduate within a reasonable period. Candidates in training eight or more years were significantly older (98% of this group were 45 to 64 years of age, compared to 57% of the group in training for less than eight years) and were more dissatisfied with their training experience. It is hard to sort through the many factors that might be at play in these situations, but this study raises questions about whether negative interactions with institute faculty are the cause or the result of the failure of these candidates to graduate. It may also be possible that these candidates lack the requisite skills or commitment to complete analytic training, and that their institutes delayed or avoided telling them that things were not going well. Such situations raise questions about the effect that having almost 20% of candidates in training for excessive periods of time has on the morale of other candidates and on the administrative and academic functioning of the institute. That this group of candidates are more dissatisfied must raise concerns about the impact this has on candidates who are newer to training and on the recruitment of candidates. For instance, potential candidates may be leery of undertaking training if they know that a significant percentage of trainees cannot graduate within a reasonable time period, especially if they themselves are older at the time they contemplate training.
A number of write-in comments on the survey called for clearer and more realistic graduation requirements, help with overcoming obstacles to completing training (e.g., finding cases), and improved feedback regarding problems. Since most candidates now begin training in middle to later adulthood, the field cannot survive if almost 20% of trainees fail to graduate within a reasonable period. This situation may call for a reappraisal of training requirements and earlier and more systematized ways of giving feedback to candidates who are not meeting the requirements. The use of learning objectives or a clear framework to assess competence may assist in clarifying and objectifying progression and graduation and reducing confusion and mistrust among candidates (Cabaniss 2008; Tuckett 2005).
Future Directions and Conclusions
The findings of this study are encouraging in that, once engaged in training, the majority of candidates are moderately or very satisfied with the experience. Candidates in this survey appeared to feel free to speak their minds on a variety of issues. Despite the concerns voiced in this survey, especially in the write-in comments, the educational experience of candidates is generally positive, an important finding that should be heartening in the face of widespread criticism and controversy about psychoanalytic education. Psychoanalytic training continues to be enriching, intellectually stimulating, and worthy of the sacrifices and passionate commitment of candidates. However, there are also sobering realities that must be confronted. The age of candidates today, the income required to support training, the apparent decline in M.D. candidates, the relative isolation of candidates in their practices, the long period spent deciding on training, and the financial and time commitments required all contribute to the decreasing number of candidates. These factors are compounded by an accumulation of other factors such as negative institute atmosphere, family obligations, lack of workplace support, logistical issues, and an awareness that many candidates do not graduate within a reasonable period. The combination of all these factors may give prospective candidates pause.
Despite candidates’ overall satisfaction with training, this study suggests that the current model of psychoanalytic education may not be able to sustain itself. The realities of current mental health practice, the advanced age of candidates, the time demands of analytic training, and the economics of young professionals who might be future trainees seem to impact synergistically on the survival of the field. Recent data on the loss of both candidate and general members of APsaA support this grim outlook. We believe the findings in this survey call for a reappraisal of the current structure of analytic training. We agree with Kernberg (2006, 2007) that psychoanalytic training needs to be revitalized and that radical changes should be considered in its reorganization.
We suggest that in order to recruit candidates earlier in their careers, and to make training accessible to a wider pool of prospective trainees, efforts be made to modify the structure of training, particularly regarding time and cost. The enormous commitment of time and money required for analytic training as currently structured may not be feasible or may frighten potential trainees without the gradual accumulation of experience, both personally, in psychotherapy or psychoanalysis, and professionally, with cases of their own. We believe that reducing the cost of training by providing sliding scale fees for personal analysis and supervision and by developing some flexibility regarding the intensive time requirements of training is necessary to reverse the current decline in candidate recruitment. These changes may come with sacrifices on the part of senior analysts and changes in the administrative structure of institutes. Yet making psychoanalytic training more relevant to current mental health practice will enhance its attraction for prospective trainees. Candidates in this study express frustration and demoralization when they are unable to find or develop analytic cases, a problem that contributes to difficulty graduating. To deal with this problem, educational innovations have been established in some institutes to help candidates ready themselves for intensive analytic work (Rothstein 2010). Since a significant number of candidates do not have active psychoanalytic practices after graduation (Cherry et al. 2004), we believe that psychoanalysis should broaden the scope of its training to make it relevant to the large group of trainees who perceive that their formal graduate or postgraduate training has not provided them the psychotherapeutic skills they need, who want to work more intensively with patients, and who are interested in a psychoanalytic framework for a variety of clinical, educational, and research pursuits.
Psychoanalytic institutes need to actively work at creating more collegial, inviting environments. Facilitating collaborations with university departments, developing psychoanalytic centers, and encouraging research and scholarship can reduce authoritarian attitudes, isolation, distrust, and fear and legitimize and reenergize psychoanalytic training (Kernberg 2011; Wallerstein 2007). The benefits and difficulties of placing psychoanalytic institutes within university settings have been outlined by several authors (Kernberg 2011; Glick 2007; Levy 2009; Michels 2007; Paul 2007; Wallerstein 2007). The advantages include trainees’ familiarity with and acceptance of the university setting, the possibility of gradual immersion in training, engagement with a community of scholars, the promotion of research and scientific inquiry, and, importantly, financial assistance to trainees unable or unwilling to make the sacrifices entailed by traditional analytic training (Levy 2009). There are many challenges to pursuing this model, however, including the willingness of universities to accept psychoanalytic institutes, long-term competitive struggles, funding issues, and requirements for research and publication (Kernberg 2011). While analytic institutes may or may not join universities, candidates in this study remark on the need for an improvement in classroom teaching and for more positive interactions with teachers in seminars. This may involve a reconsideration of authority and power in the classroom, making educational goals explicit, developing new ways of encouraging discussion, and becoming aware of subtle interactions that interfere with participation (Power 2001; Skorczewski 2004). Finally, candidates express the wish that graduation requirements be made clear from the beginning and that feedback regarding their progress (and any assistance they might need) be provided regularly. A combination of efforts on some or all of these fronts may make psychoanalytic training more attractive to potential trainees. While some of these issues are controversial, and there are concerns about altering the time-honored experience of psychoanalytic training, we believe, given the crisis in recruitment, that all avenues of enhancing enrollment in psychoanalytic training programs should be explored.
Footnotes
Acknowledgements
The authors thank M. Carmela Perez for assistance in distribution of the survey and Karen Flanary for editorial assistance.
Results of the survey were presented at the Poster Session of the American Psychoanalytic Association, New York, January 2011.