
Abstract
This study explored a psychodynamic model for suicide risk by examining risk factors for medically serious suicide attempts, including assessments of affect flooding, negative self-schema / fragmentation, and impaired reality testing, closely approximating Maltsberger’s psycho-dynamic formulation of suicide crisis. Baseline risk factors including age, gender, psychiatric symptoms, high-risk behaviors, and the Implicit Risk for Suicide Index (IRSI) were used to detect medically serious suicide attempts monitored for up to a year after the assessment. Twenty-five psychiatric inpatients who made life-threatening suicide attempts after assessment were compared to 25 inpatients and 25 psychotherapy outpatients who made no suicide attempts during follow-up. Statistical analysis revealed that a history of at least one suicide attempt and elevated IRSI scores accounted for 60 percent of the variance in detecting medically serious suicide attempts. Elevated IRSI accurately identified suicide attempt status above and beyond past suicide attempts and other empirically validated risk factors. Results are discussed in light of psychodynamic formulations of suicide risk.
Psychotherapists undertaking the treatment of patients suffering from depression, borderline personality disorder, and co-occurring conditions face a heightened risk of suicide and suicide attempts in their clinical practice (Oldham 2006). Initial and ongoing assessment of suicide risk is thus crucial in the treatment of these patients, especially during periods of turmoil, when regression and stressful life events increase the risk. When theoretically informed assessments are conducted with an emphasis on underlying psychological vulnerabilities, clinicians can better understand and empathize with the patient, and the assessments can serve as a valuable heuristic in guiding treatment decisions.
After reviewing the empirical evidence supporting the use of a psychodynamic formulation of suicidal crises (Maltsberger 2004), we pre-sent the results of a study assessing the Implicit Risk for Suicide Index (IRSI; Fowler, Hilsenroth, and Piers 2001), a Rorschach scale closely aligned with Maltsberger’s model. Rorschach protocols and empirically validated risk factors were assessed at admission, and then tested for their unique predictive validity in identifying patients who would make a medically serious suicide attempt within a year of initial assessment.
In the influential paper “The Descent into Suicide,” Maltsberger (2004) synthesized more than forty years of suicide research to formulate a model of suicide crisis that captures the primary psychological components of many suicide attempts. His précis is austere yet complex:
I propose the following four aspects: the first, which can be compared to flooding, finds the patient awash in an overwhelming deluge of intolerable painful feeling. This is the aspect of ‘affect deluge’. Aspect 2, ‘efforts to master affective flooding’, finds the patient attempting to subjugate and contain painful feeling, succeeding sometimes, sinking sometimes, and struggling, as it were, to stay afloat. When he can do this no longer, movement into the third aspect occurs, which can be likened to drowning with the patient feeling out of control and desperate. Aspect 3 is named ‘loss of control and disintegration’. In Aspect 4, we see the patient, his ego crippled by lost reality testing, mounting grandiose schemes for self-preservation that may include self-preservation through the jettison of his body. This aspect is labeled ‘grandiose survival and body jettison’ [p. 654].
These aspects do not necessarily occur in sequence; rather, before making a suicide attempt, individuals may rapidly and chaotically shift among them. Maltsberger notes several common stressors that trigger a suicidal crisis, including real or imagined loss of a close attachment figure, narcissistic injury, and failure to live up to perfectionistic standards. While negative stressful life events occur across the life cycle, only a fraction of individuals respond by becoming suicidal, even when they are considered high risk (Yen et al. 2005); for that reason, exploring potential psychological vulnerabilities predisposing some individuals to react catastrophically is crucial in assessing suicide risk. Aspects of Maltsberger’s formulation are considered in light of recent empirical research, and the theoretical link to the IRSI is articulated.
Aspect 1
Affect deluge may strike well-adjusted individuals during periods of crisis, but for those with limited capacity to modulate emotions, it may be the single greatest vulnerability to suicide and suicide attempts. When individuals cannot escape intense emotional pain, the risk of suicide is alarmingly high. According to Maltsberger (1992), “the driving force behind almost every suicide, clinically speaking, is mental pain” (p. 37). Shneidman (1993) came to a similar conclusion: “As I near the end of my career in suicidology, I think I can now say what has been on my mind in as few as five words: Suicide is caused by psychache. Psychache refers to the hurt, anguish, soreness, aching, psychological pain in the psyche, the mind. It is intrinsically psychological—the pain of excessively felt shame, or guilt, or humiliation, or loneliness, or fear, or angst, or dread of growing old or of dying badly, or whatever” (p. 147).
Empirical evidence linking affect deluge and suicide risk is quickly mounting. Based on psychological autopsy findings that patients experienced a dramatic intensification of intolerable affects before suicide (Hendin et al. 2004), the Affective States Questionnaire was developed to assess extreme states of affective arousal (ASQ; Hendin, Maltsberger, and Szanto 2007). The ASQ was tested prospectively for its ability to predict suicidal behavior at a Veterans Health Administration Medical Center, yielding acceptable levels of true positive prediction of suicide-related behavior and true negative prediction within three months of assessment (Hendin et al. 2010). Direct self-report measures of psychache have found that the experience of overwhelming emotional pain was related to suicide-related behaviors (Flamenbaum and Holden 2007). Further, patients with recent or past suicide attempts expressed significantly higher levels of psychological pain and a higher intensity and frequency of current suicidal ideation than patients without a history of suicidal acts (Olié et al. 2010).
The link between affective overstimulation and suicide risk has also been explored using the color-shading blend responses on the Rorschach. Appelbaum (Appelbaum and Colson 1968; Appelbaum and Holtzman 1962) observed that the combined use of shading and color in order to create an image in a Rorschach inkblot reflects an immersion in affective experiences, with little capacity to dampen the level of affective arousal. While the content of color-shading blends (e.g., “A sunset over a lake—the colors blur together creating a hazy view”) can appear innocuous to the untrained observer, they have emerged as a potent predictor of completed suicide (Appelbaum and Colson 1968; Appelbaum and Holtzman 1962; Exner 1993; Exner and Wylie 1977) and serious suicide attempts (Affra 1982; Fowler et al. 2001; Silberg and Armstrong 1992). In the first study to assess suicidal behaviors with the IRSI, the color-shading blend was the strongest single variable in predicting medically serious suicide attempts (Fowler, Hilsenroth, and Piers 2001).
Aspect 2
Efforts to master affective flooding can be conceptualized as the total range of defensive functioning that prevents loss of control and disintegration. While it is feasible to examine defenses in Rorschach responses, it is not possible to identify instances of effective dampening of affective arousal without direct measurement of physiological markers during administration of the Rorschach. We set aside the thorny issue of operationalizing Aspect 2, choosing instead to focus on the breakdown products of the failure to contain affect summarized in Aspect 3.
Aspect 3
Loss of control and disintegration occurs when efforts to contain affective deluge fail, resulting in faltering ego functions and the experience of falling apart or losing one’s mind. While many ego functions deteriorate in the context of intense negative affect, Maltsberger (2004) emphasizes the disorganizing impact of affective flooding on the structure of the self-representation and the heightened risk of suicide that ensues: “When the self-representation disarticulates and the portion of it that represents the body takes on the characteristics of an object representation, the way is open for attacking the body as though it were something or someone else, not the self” (p. 660).
Observations by psychoanalysts support the assertion that many patients in the midst of a suicidal crisis experience fragmentation of self-representations, and that split-off aspects of the self become the object of attack (Asch 1980; Fenichel 1945; Freud 1917; Havens 1965; Maltsberger and Buie 1980). For such individuals the suffering takes on a painful inner experience of being at war with split-off and alien aspects of the self: “the weak and helpless patient feels himself to be under the constant contemptuous scrutiny of an alien yet inner presence. . . . At times this presence may become sufficiently contemptuous of the self so as to demand an execution, and the spent self may hopelessly acquiesce” (Maltsberger and Buie 1980, p. 64).
Empirical studies highlight the risk factors of depression, hopelessness, and self-directed hostility; yet rarely do these studies consider fragmentation of the self as an exacerbating factor. Rorschach studies demonstrate a strong association between excessive preoccupation with morbid imagery and later suicidal behavior (Affra 1982; Exner and Wylie 1977; Exner 1993; Fowler et al. 2001; Silberg and Armstrong 1992). While the Rorschach morbid response has long been associated with depressive and hostile affects (Exner 1993; Schafer 1954), scant attention is given to the fragmentation and disintegration of representations embedded in morbid responses. It is our contention that these responses (e.g., “A man’s face . . . the skin is flaking off and there is blood coming out of the mouth”) capture depressive or hostile ideation, as well as the disintegration of self-representations. In the initial IRSI study, patients who later engaged in medically serious suicide attempts produced significantly more morbid images in their Rorschach protocols than did nonsuicidal patients (Fowler, Hilsenroth, and Piers 2001).
Aspect 4
Grandiose survival and body jettison reflects desperate efforts to escape the overwhelming affects exacerbated by the disturbing experience of disintegrating self-representations. As the gulf widens between fragmenting self-representations, fantasies frequently emerge of jettisoning the weak and hated aspects of the self while the fantasized good aspects survive. Grandiose and illogical fantasies of destroying hated parts of the self are noted in clinical research, especially among more seriously disturbed suicidal patients (Goldblatt and Maltsberger 2010; Hendin 1991, 1992; Maltsberger and Buie 1980). Other analysts emphasize fantasies of transcending the limitations of human existence by surviving suicide and being fused with an idealized, all-powerful other (Asch 1980). In both scenarios, the suicidal individual engages in highly illogical grandiose fantasies.
The link between impaired reality testing and suicide has been explored with transparency and cross-section responses on the Rorschach. Roth and Blatt (1974) interpreted transparencies appearing in dream imagery and Rorschach responses as representing failures to maintain adequate ego boundaries, failures that increase the risk for suicidal behavior. Blatt and Ritzler (1974) confirmed this when they found a significantly higher number of transparency and cross-section responses in the Rorschach protocols of patients who committed suicide. Transparency responses (e.g., “Two women wearing black tuxedos. I can see their hearts pumping and blood coursing through their bodies”) are indicative of poor reality testing, marked by an uncritical acceptance of perception beyond the confines of normal human sight. Such responses may parallel the suicidal patient’s fantasy of survival following suicide (Goldblatt and Maltsberger 2010). Fowler, Hilsenroth, and Piers (2001) added to this evidence base, showing that patients who later engaged in medically serious suicide attempts produced significantly more transparency and cross-section responses in their Rorschach protocols than did nonsuicidal patients. In addition, they reported a case vignette highlighting a suicidal patient’s grandiose fantasies of transcending death to be reunited with her deceased father. This female patient (who months earlier had produced three Rorschach transparency responses) assumed that after she reunited with her father, she would simply come to her next psychotherapy appointment with her (very much alive) therapist. While far from definitive evidence, the case illustration bolstered the argument that transparency and cross-section responses may well represent boundary disturbance marked by grandiose transcendent fantasies.
The Current Study
The original study assessing risk factors of affect deluge, self-hatred and fragmentation, and grandiose fantasies correctly identified 87 percent of inpatients who made a medically serious suicide attempt within sixty days after administration of the Rorschach (Fowler, Hilsenroth, and Piers 2001). The authors were skeptical of replicating these findings given the high degree of accurate identification; furthermore, questions lingered regarding whether the variables assessed by the IRSI were state-dependent and would therefore not be predictive of suicidal risk beyond sixty days. A replication study was undertaken to extend the time frame to a full year after administration of the Rorschach, and the study design was enhanced to assess the unique contributions of a broad array of well-established risk factors. Based on an extensive review of risk factors, and in light of the fact that suicide assessment requires an integration of multiple sources of data (APA 2004; Nock et al. 2008), the following risk factors were included in the analyses: (1) demographic features such as age and gender (Goldsmith et al. 2002); (2) psychiatric diagnoses including major depressive disorders, bipolar spectrum disorders, anxiety disorders, substance abuse, psychotic spectrum disorders, and borderline personality disorders (Neves, Malloy-Diniz, and Correa 2009; Soloff and Fabio 2008; Yen et al. 2003); (3) high-risk behaviors including recent suicide attempts, suicidal ideation, nonsuicidal self-injury, deterioration in functioning, and recent hospitalization (Beautrais 2004; Leon et al. 1990; Oquendo et al. 2004); and (4) total IRSI score reflecting the degree of affect flooding, negative self-schema / fragmentation, and impaired reality testing characterized by grandiose and illogical percepts (Fowler, Hilsenroth, and Piers 2001).
Method
Sampling and Group Classification
The initial inpatient sample consisted of all adult patients (N = 304) consecutively admitted to an inpatient residential treatment center between November 2001 and May 2007. The outpatient sample consisted of the first 25 adult outpatients assigned to one of several treatment groups in a process-outcome study (Hilsenroth et al. 2003). Subjects gave informed consent, and the study was granted IRB approval. At admission, board-certified and licensed psychologists or psychiatrists assigned DSM-IV diagnoses employing the method of longitudinal expert evalu-ation using all data (LEAD; Pilkonis et al. 1991). Baseline risk factor assessments included demographic variables, psychiatric diagnoses including Axis V Global Assessment of Functioning Scores, recent history of self-destructive behavior, presenting psychiatric symptoms including substance use, hypomanic presentation, symptoms of anxiety, dysphoria, dissociation, and interpersonal relationship impairment.
For the inpatient sample, digital medical records were collected during the index hospitalization. Daily nursing-shift notes contained detailed descriptions of self-destructive activity, physical trauma incurred as a result of self-destructive acts, medical procedures performed, and information regarding emergency medical transfers. The data were collected from admission to up to a year for inpatients, and constituted the outcome data for rating instances of medically serious suicide attempts. For the outpatient sample, research staff systematically collected periodic evaluations of behavioral functioning from the patients and their therapists.
Behavioral records were classified as either nonsuicidal (NS) or medically serious suicide attempt (MSSA) using the Lethality of Suicide Attempt Rating Scale–II (LSARS-II; Berman, Shepherd, and Silverman 2003), a well-validated scale that differentiates medically serious suicide attempts from suicidal gestures and nonsuicidal self-injury. Classification as nonsuicidal required that a patient’s records be free of any self-destructive/suicidal behavior during the index treatment. A medically serious suicide attempt was defined as a suicide attempt requiring medical hospital admission and meeting one of the following treatment criteria: (1) treatment in specialized medical units; (2) surgery under general anesthesia (excluding superficial cuts); (3) extensive medical treatment, including telemetry, antidotes for drug overdoses, or repeated tests or investigations. In addition, patients who attempted suicide by methods with a high risk of fatality, specifically, hanging or gunshot, but did not meet the preceding treatment criteria were also included in the group who made serious suicide attempts (Beautrais 2003).
Ratings of suicidal behavior were made blind to the study design and to identifying information, ensuring that ratings were free of bias from suicide risk factors. Independently coded ratings of 304 inpatients demonstrated excellent reliability for coding the LSARS-II (ICC2,1 = .82). Once reliability estimates were established, all disagreements in rating were discussed until consensus was reached among the four raters. LSARS-II ratings identified 25 inpatients with a medically serious suicide attempt during the index hospitalization. Twenty-five inpatients with no suicidal activity during the first year of hospitalization were randomly selected from the initial pool to serve as a comparison group, and 25 adult outpatients with no suicidal activity during a six-month period served as an outpatient control group.
The Rorschach Inkblot Method
The Rorschach inkblot method is an implicit performance-based measure that samples perceptual/verbal responses to ten chromatic and achromatic visual stimuli under highly standardized administration and scoring rules (Meyer and Kurtz 2006). By activating cognitive problem-solving strategies to contend with complex ambiguous stimuli and minimal instructional set, the method elicits data from the domains of information processing including quality of reality testing, affect management, and self-representation/self-schema. Administration and scoring followed standard procedures and guidelines (Exner 1993).
The IRSI scores were extracted from Rorschach protocols. All identifying information was eliminated to ensure that raters of the protocols were blind to the patient’s demographic, diagnostic, behavioral, and suicide attempt status. Twenty protocols were randomly selected and scored independently by four raters to ascertain interrater reliability. All components of the IRSI demonstrated excellent reliability: affect deluge characterized by color-shading blends (ICC2,1 = .77), fragmented self-schema characterized by a morbid preoccupation with death and damage (ICC2,1 = .97), grandiose scheming and cognitive disturbance in reality testing characterized by cross-sections and transparency responses (ICC2,1 = .77), and total IRSI score (ICC2,1 = .84). After reliability estimates were calculated, all disagreements were discussed until consensus was reached.
Results
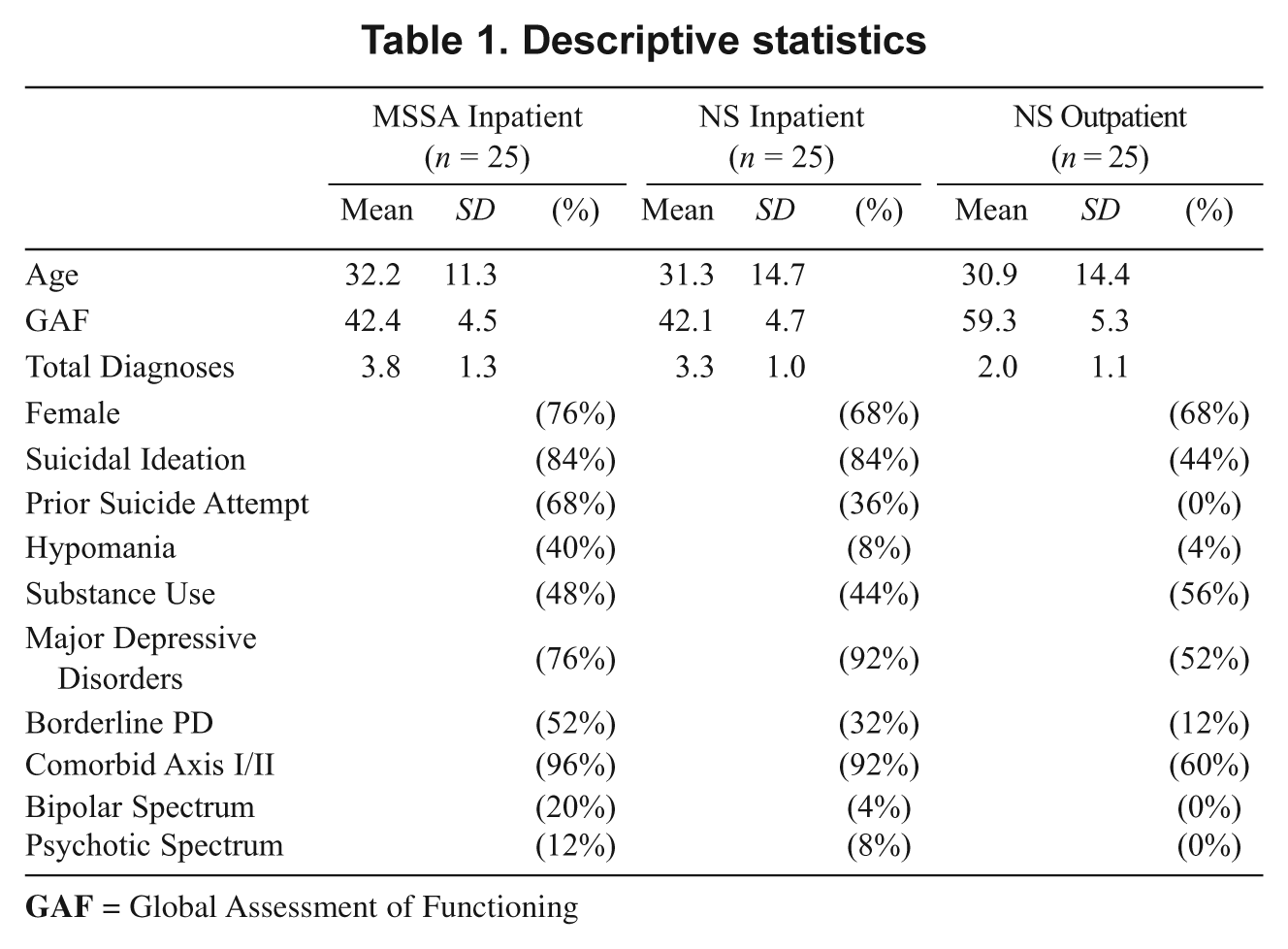
Descriptive statistics (Table 1) reflect high levels of psychopathology with many risk factors for suicide, particularly in the two inpatient groups. As anticipated, the outpatient sample had fewer overt behavioral risk factors, with the exception of recent substance use (56%), relatively high rates of major depressive disorders (52%), comorbid Axis I and Axis II disorders (60%), and suicidal ideation (44%), suggestive of elevated risk for suicide-related behaviors.
Descriptive statistics
To assess the influence of individual risk factors in the prediction of medically serious suicide attempts, we used stepwise hierarchical logistic regression analysis. This statistical procedure estimates the relative contribution of individual risk factors in predicting a given outcome, in this case suicide attempt status. A priori risk factors were entered in separate steps in the following sequence: Step 1: demographic variables (age, gender); Step 2: DSM-IV diagnostic variables (GAF, major depressive disorders, BPD, any Axis II disorder, bipolar spectrum, psychotic spectrum, comorbid Axis I & II, multiple Axis I, multiple Axis II); Step 3: high-risk behaviors and symptoms (prior suicide attempt, suicidal ideation, substance use, dissociation, anxiety, hypomania, relationship impairment); and Step 4: the IRSI. Conducting the data analysis in this sequence ensures that risk factors entering the model in later steps provide unique prediction above and beyond the risk factors entered in earlier steps (creating an estimate of the incremental validity of each risk factor). The selection of variables for each step followed a clinically pragmatic model in which traditional psychiatric intake data that are easily obtained (e.g., age, gender) enter in the early steps, and the most complex and time-intensive assessments (the IRSI) are entered last. If the standard assessment approach produces equal or better prediction than the time-intensive IRSI, then there is no practical benefit to adding the IRSI assessment.
Results (Table 2) indicate a final regression model with a 2-variable solution accounting for approximately 60 percent of the estimated variance. None of the demographic or DSM-IV diagnostic variables or the initial GAF score enters the model. Of the seven behavioral risk factors, past suicide attempt was the only variable that predicted suicide attempt status. In the final step, the IRSI entered the model, adding approximately 18 percent of the variance to the prediction of medically serious suicide attempt, thus demonstrating incremental validity over and above past suicide attempt.
Hierarchical logistic regression of MSSA status as a function of all risk factors

Because the IRSI provided incremental prediction above well-established risk factors, post hoc analyses of variance (ANOVAs) were computed to assess the individual components of the IRSI (Table 3). The MSSA group produced a significantly higher number of color-shading blend responses reflecting affect deluge (F(1,73) = 22.2, p = .0001; Cohen’s d = 1.2), morbid responses, reflecting fragmented self-representation (F(1,73) = 14.7, p = .03; Cohen’s d = .95), and transparency and cross-section responses reflecting cognitive disturbance in reality testing marked by grandiose scheming (F(1,73) = 24.3, p = .0001; Cohen’s d = 1.2). Contrasting the clinical groups on IRSI total score (the sum of all components) revealed that MSSA patients produced significantly higher scores than NS patients (F(1,73) = 36.7, p = .0001; Cohen’s d = 1.5). In all analyses, large effect sizes were observed, indicating the robustness of the individual components in differentiating the suicidal from the non-suicidal group.
Post hoc analysis of variance across groups
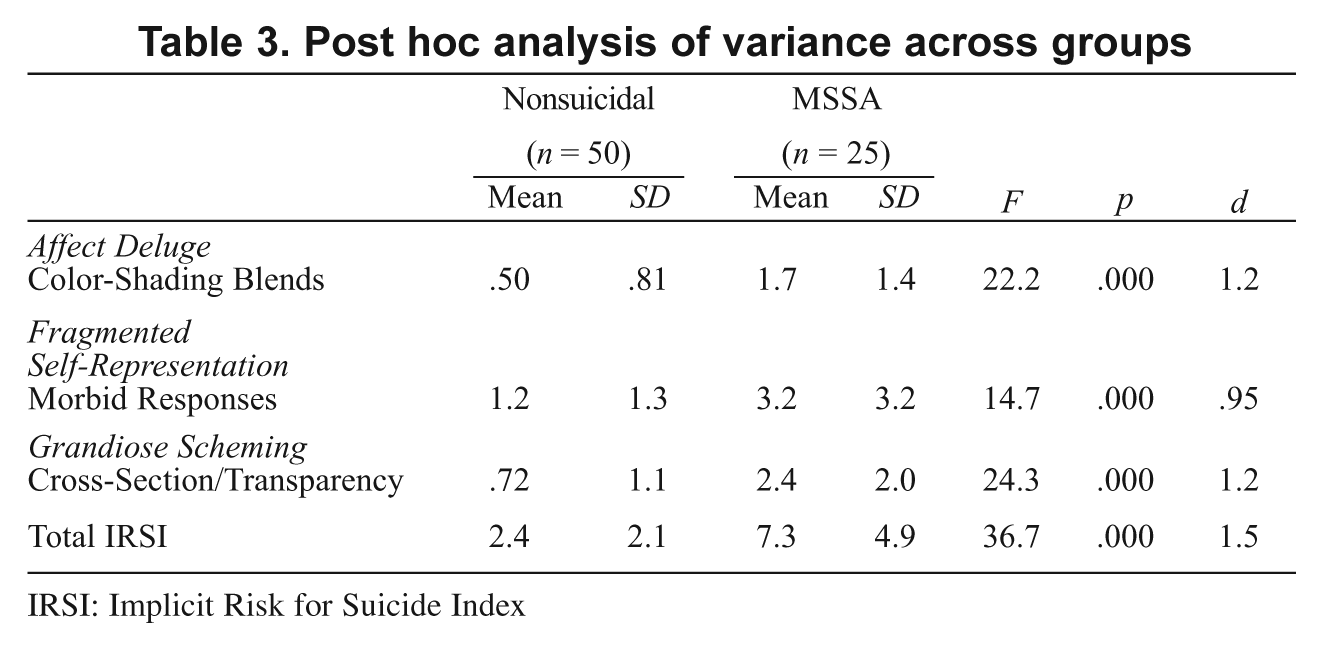
IRSI: Implicit Risk for Suicide Index
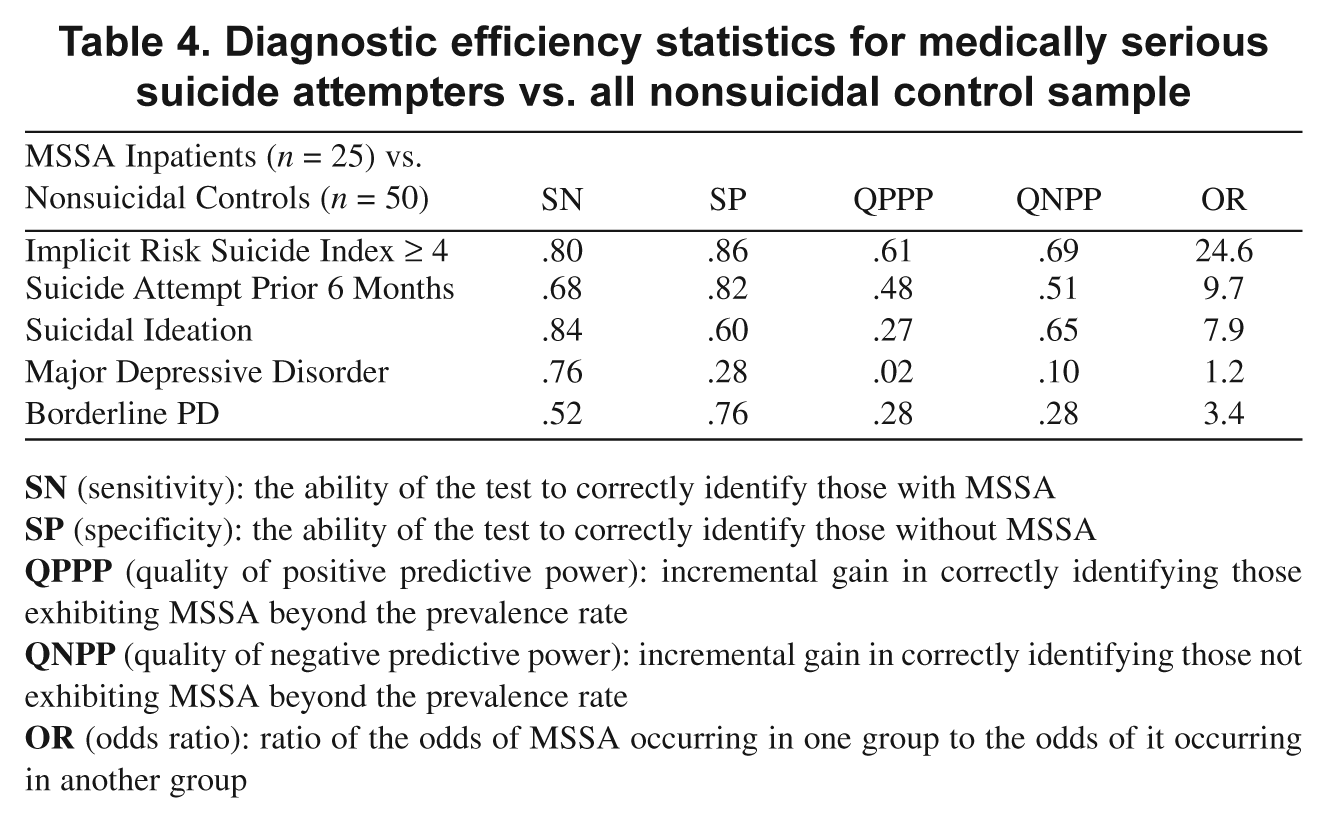
The practical utility of any diagnostic test is its ability to detect or predict an individual’s likelihood of having or acquiring the condition in question (Streiner 2003). Based on previously established cut-scores for the IRSI (Fowler, Hilsenroth, and Piers 2001), diagnostic efficiency statistics were calculated to accurately identify individual medically serious suicide attempt status from IRSI cut-scores equal to or greater than four (4). Presence or absence of past suicide attempts, suicidal ideation, major depressive disorders, and borderline personality disorders was also explored. Five statistics were calculated: (1) sensitivity (true positive rate): the ability of the index to correctly identify individuals exhibiting MSSA; (2) specificity (true negative rate): the ability of the index to correctly identify individuals as not having the trait; (3) quality of positive predictive power: the percentage of incremental gain in correctly identifying individuals exhibiting MSSA above and beyond the prevalence rate for MSSA; (4) quality of negative predictive power: the percentage of incremental gain in correctly identifying individuals not exhibiting the trait above and beyond the prevalence rate for MSSA; (5) odds ratio: ratio of the odds of MSSA occurring in one group to the odds of it occurring in another.
Results contrasting inpatients in the MSSA group with the combined inpatient and outpatient nonsuicidal sample (Table 4) indicate that an IRSI total score of four or greater led to 80% true positive prediction (sensitivity), 86% true negative prediction (specificity), 61% improvement in prediction above the prevalence rate in the accuracy of identifying MSSA (quality of positive predictive power), and 69% improvement above the prevalence rate in the accuracy of not identifying NS patients as making a suicide attempt (quality of negative predictive power). An IRSI score of four or greater led to a 24.5-fold likelihood of accurately diagnosing an individual patient as at risk of a medically serious suicide attempt. Knowledge of a suicide attempt prior to the index hospitalization (odds ratio = 9.7) and baseline suicidal ideation (odds ratio = 7.9) also increased accuracy of prediction above base rates, yet the IRSI was three times more predictive than knowing if a patient experiences suicidal ideation, and 2.5 times more predictive than knowledge of a prior suicide attempt. A diagnosis of borderline personality disorder was substantially more predictive (odds ratio = 3.4), yet major depressive spectrum disorders minimally predicted later MSSA status (odds ratio = 1.2). The overall finding from these diagnostic efficiency statistics is that the IRSI is a strong predictor of which patients are at high risk for MSSA, significantly better than knowing the prevalence rate and knowledge of past suicide attempts.
Diagnostic efficiency statistics for medically serious suicide attempters vs. all nonsuicidal control sample
These findings support the diagnostic strength of the IRSI; however, would the pattern of results be replicated when comparing the two inpatient groups? To address this question we recalculated the diagnostic efficiency statistics. Results contrasting inpatients in the MSSA group with the nonsuicidal inpatient sample (Table 5) indicated that an IRSI total score of four or greater led to similar rates of true positive prediction (sensitivity = 80%), and improvement in prediction above the prevalence rate in the accuracy of identifying MSSA (quality of positive predictive power = 60%), with a slight diminishment of true negative prediction (specificity = 80%), and improvement above the prevalence rate in the accuracy of not identifying NS patients as making a suicide attempt (quality of negative predictive power = 60%). Inpatients with an IRSI score of four or greater led to a 16-fold likelihood of accurately diagnosing an individual patient as at risk of a medically serious suicide attempt (odds ratio = 16). Knowledge of a suicide attempt before the index hospitalization (odds ratio = 10.6) and baseline suicidal ideation (odds ratio = 6.7) also increased accuracy of prediction above base rates. A diagnosis of borderline personality disorder was predictive (odds ratio = 5.7), yet major depressive disorders remained a relatively poor predictor of later suicide attempts (odds ratio = 2.9).
Diagnostic efficiency statistics for medically serious suicide attempters (n = 25) vs. inpatient control sample (n = 25)

Discussion
Despite decades of research, accurate prediction of suicide and suicide attempts has remained elusive. The American Psychiatric Association’s Guidelines on Suicidal Behavior (2004) concluded that predicting suicide and suicide attempts appears impossible in large part due to its rarity, even in high-risk groups. This judgment may be premature, given the significant limitations of most prediction studies. Beyond the statistical challenges of predicting behaviors that are infrequent and transient in nature, most studies rely on distal, nonpsychological variables such as demographic variables and psychiatric diagnoses (Goldsmith et al. 2002). The result is an ever expanding list of risk factors for suicide; yet the lack of psychological sophistication and excessively high false-positive rates limit their predictive value for clinicians working with individual patients (Fowler 2012). For example, it is widely reported that males are three to five times more likely to die by suicide than females, but what respon-sible therapist loses sleep worrying that all male patients are at risk of killing themselves? A particularly pessimistic view of the state of suicide prediction was made by a renowned suicidologist: “All our past efforts to relate or to correlate suicide with simplistic non-psychological variables, such as sex, age, race, socioeconomic level, case history items (no matter how dire), psychiatric categories (including depression), etc., were (and are) doomed to miss the mark precisely because they ignore the one variable that centrally relates to suicide, namely, intolerable psychological pain . . .” (Schniedman 1993, p. 147).
When researchers do focus on psychological experience, they typically rely on self-reports from suicidal individuals who may be motivated to dissimulate, or are unable to accurately assess their emotional states and future risk (Hendin, Maltsberger, and Szanto 2007; Nock and Banaji 2007). One study has shed light on the alarming fact that 78 percent of individuals who later committed suicide denied suicidal ideation or intent during their last human contact (Busch, Fawcett, and Jacobs 2003). Some research teams circumvent problems associated with self-report bias by developing computer-based measures that tap into implicit psychological processes (Cha et al. 2010; Nock and Banaji 2007) or use interview strategies focusing on the individual’s current affective states while intentionally avoiding reference to suicide (Hendin, Maltsberger, and Szanto 2007). A third approach uses the Rorschach inkblot method to extract dimensions of cognition and affective functioning related to suicide risk (Affra 1982; Exner 1993; Exner and Wylie 1977; Fowler et al. 2001; Fowler, Hilsenroth, and Piers 2001; Silberg and Armstrong 1992). These indirect measures show considerable predictive validity in small but well-designed studies. The current study adds to this body of evidence and provides considerable support for a psychodynamic formulation of suicide risk.
When compared to empirically validated risk factors such as a prior suicide attempt, BPD diagnosis, or suicidal ideation, the IRSI performs exceptionally well, demonstrating incremental validity over other risk factors, including the strongest predictor—past suicide attempts (Beautrais 2004; Oquendo et al. 2004; Leon et al. 1990). To the best of our knowledge, the IRSI and Cha’s methodology (Cha et al. 2010) are the only two measures demonstrating prediction above and beyond a history of a past suicide attempt. Unfortunately, comparisons cannot be made between these implicit predictors and genetic factors, or immediate stressors such as traumatic loss, due to methodological and sample differences.
Given the surprising accuracy of the IRSI in identifying patients who later made medically serious suicide attempts, the question arises why it is such an efficacious diagnostic tool. Several factors likely influenced this outcome. This study selected high-risk inpatient samples (with high rates of Axis I and Axis II pathology) and elevated-risk outpatient samples, allowing us to detect more instances of suicide attempt in a brief span of time, thus mitigating the effects of maturation or treatment effects on the overall prediction. Use of the Rorschach IRSI circumvents the inherent limitations of self-report measures, as well as capturing multiple dimensions of suicide risk in a single index. Perhaps most important, the IRSI assesses crucial psychological states of underlying vulnerability to affect deluge, fragmentation of the self-representation, and the breakdown of reality testing associated with deteriorating ego functions and grandiosity. As such, the index taps into not only overwhelming affect (which Maltsberger and Shneidman consider the single most crucial psychological risk factor) but also the breakdown products of the inability to mount adequate defenses against overwhelming pain.
The study results must be considered in light of several limitations. Despite the fact that Rorschach data were collected prior to any suicide attempt (a strength of the design), the study was case-control, allowing the researcher to control the base rate of suicide attempts, which can maximize the quotients from diagnostic efficiency statistics (Meehl and Rosen 1955). A full prospective study, now in the planning phase, may yield more modest findings. While diagnoses were assigned using a rigorous methodology (LEAD; Pilkonis et al. 1991), the lack of standardized diagnostic interviews and reliability checks may have attenuated the predictive validity of diagnoses in the analyses. Also, outpatient controls were followed for only six months, whereas the inpatient groups were followed for up to a year, creating an unequal sampling for those in the outpatient group. While the results of this study may not generalize to high-functioning patients (with whom concern about suicide is extremely low), the greatest need for reliable prediction is with high-risk patients. The IRSI has not been tested with completed suicides, and thus our remarks and conclusions must be considered in the light of risk for medically serious suicide attempts not resulting in actual suicide.
While the study results are promising for identifying high-risk patients, what clinical implications has it for patients with these underlying vulnerabilities? First, clinicians conducting long-term psychodynamic treatments with high-risk patients will find the treatment recommendations of Bateman and Fonagy (2004) and Hendin et al. (2006) particularly relevant to their practice with suicidal patients. In the broader context of conducting a treatment tailored to the patient’s presenting complaint, the therapist may consider focusing particular attention on interventions that successfully enhance the patient’s capacity for (1) improving affect modulation and containment of impulsive behaviors during affect storms, especially in the context of stressful life events and alliance ruptures, (2) helping the patient recognize that affects are fleeting and can be survived, (3) increasing adaptive defenses to shore up ego boundaries to stave off fragmentation of the self, and (4) focusing on interventions aimed at restoring good reality testing and strengthening the stability and coherence of self-representations. All of these interventions are aimed primarily at supporting and enhancing ego functions for patients during periods of crisis.
For clinicians treating suicidal patients suffering from borderline personality disorder, there is clear and compelling evidence from well-designed randomized controlled trials that several forms of psychotherapy help borderline patients decrease the frequency of self-destructive behavior, suicide attempts, and emergency hospitalizations (Bateman and Fonagy 2008; Clarkin et al. 2007; Doering et al. 2010; Levy et al. 2006; Linehan et al. 2006). Evidence shows that long-term psychoanalytically informed mentalization-based treatment is particularly efficacious in creating and sustaining improvement; BPD patients in an eighteen-month mentalization-based treatment program demonstrated sustained decreases in suicide attempts five years after discharge (Bateman and Fonagy 2008). This is particularly promising given that most positive effects of psychotherapy treatment tend to diminish over time. Transference-focused psychotherapy (TFP) has also proven effective in decreasing suicide attempts and self-destructive behavior in the treatment of patients with borderline personality disorder. A randomized control trial (Clarkin et al. 2007) comparing TFP, dialectical behavior therapy (DBT), and a psychodynamic supportive psychotherapy (SPT) found significant reductions in suicidality in patients in the TFP and DBT treatments, but not for those in the supportive dynamic treatment. A recent randomized controlled trial comparing TFP to treatments conducted by experienced community therapists found that of those remaining in treatment for one year, those in the TFP group had significantly fewer suicide attempts.
Concluding Remarks
While many psychoanalytic practitioners trust evidence from the consulting room over research evidence, the recent outcome studies cited above, as well as developments in cognitive neuroscience, are strengthening the science behind some psychodynamic concepts (Westen 2006), a fact that may well influence the future practice of psychodynamic psychotherapy and psychoanalysis. While modest in scope, the current study contributes to the growing body of evidence suggesting that psychodynamic concepts can be fruitfully studied to better understand and assess those at risk for medically serious suicide attempts. We approached this line of research in hopes of filling gaps in our clinical understanding, as each of us struggled to understand, empathize with, and effectively treat suicidal patients in our practice. To that end, the IRSI, especially when integrated with Maltsberger’s model, provides a valuable heuristic for understanding the underlying vulnerabilities of patients who lack an effective way of verbally communicating their internal experiences.
This study was unusual in that it examined a broad array of risk factors from multiple domains, a noted shortcoming of many suicide risk factor studies (Goldsmith et al. 2002). The study also adds to a small but growing body of evidence linking implicit cognition with future suicidal behavior (Cha et al. 2010; Fowler et al. 2001; Nock and Banaji 2007). Due to heavy demands on resources, clinicians unfamiliar with the Rorschach may find the assessment cost-prohibitive and impractical in some settings. To address this, one of us (JCF) is developing a computer-based assessment of the IRSI.
Footnotes
J. Christopher Fowler, Associate Professor and Associate Director of Research, Menninger Department of Psychiatry and Behavioral Sciences, Baylor College of Medicine. Mark J. Hilsenroth, Professor of Psychology, Derner Institute of Advanced Psychological Studies, Adlephi University. Michael Groat, Assistant Professor, Menninger Department of Psychiatry and Behavioral Sciences, Baylor College of Medicine; Director, Professionals in Crisis Program, the Menninger Clinic. Spencer Biel, Staff Psychologist, the Austen Riggs Center. Christina Biedermann, Staff Psychologist, the Austen Riggs Center. Steven Ackerman, Staff Psychologist, the Austen Riggs Center.