
Abstract
A systematic method is presented whereby material from a full course of psychoanalytic treatment is analyzed to assess changes and identify patterns of change. Through an analysis of session notes, changes were assessed using the CHange After Psychotherapy scales (CHAP; Sandell 1987a), which evaluate changes in five rating variables (symptoms, adaptive capacity, insight, basic conflicts, and extratherapeutic factors). Change incidents were identified in nearly every session. Early in the analysis, relatively more change incidents related to insight were found than were found for the other types of change. By contrast, in the third year and part of the fourth year, relatively more change incidents related to basic conflicts and adaptive capacity were found. While changes related to symptoms occurred throughout the course of treatment, such changes were never more frequent than other types of change. A content analysis of the change incidents allowed a determination of when in the treatment the patient’s main conflicts (identified clinically) were overcome. A crossing of quantitative data with clinical and qualitative data allowed a better understanding of the patterns of change.
Keywords
Change models of psychoanalyses or psychoanalytically oriented psychotherapies are typically more or less speculative commonsense notions that appear to have seldom been empirically tested, strictly and systematically. For instance, Blum (1979) argued that after an initial phase there is a phase involving the development of transference neurosis, interpretation, “remobilization,” and the working through of unconscious conflicts. A phase of resolving or dissolving the transference neurosis then follows and after that the termination phase with its own characteristics. According to Gunderson and Gabbard (1999), a sequence of changes in various areas can be expected during the process of psychotherapy: (1) subjective states and dysphoric feelings (after a few weeks); (2) behavior (after some months); (3) interpersonal style (6–18 months); and (4) intrapsychic organization (after two years).
Few studies have empirically and systematically followed and described a course of psychoanalysis through its entire duration. Although Dewald (1972) ambitiously recorded his notes after his sessions with a patient, no systematic summary of the analysis followed. In contrast, Dahl, Kächele, and Thomä (1988) developed and studied the FRAMES model in an exhaustive process study of the six-year psychoanalytic treatment of Mrs. C, a case that has been used in other process research studies. An unusual and inspiring set of psychoanalytic case studies has been produced based on the generous account of the case of Amalia X by the Ulm Textbank group, thoroughly described by Kächele, Schachter, and Thomä (2009).
These examples are exceptions, however. Typically the empirical study of change models has focused on short-term psychotherapies, leaving open questions about changes occurring in treatments of several years’ duration. Few, if any, of the studies included in the recent review by Ablon, Smith-Hansen, and Levy (2012) concerned psychoanalysis in its proper sense; rather, they focused on psychoanalytically oriented psychotherapy. Thus, Jones and collaborators (Ablon and Jones 1999; Jones, Parke, and Pulos 1992; Jones and Pulos 1993) systematically analyzed psychoanalytic therapy courses, more or less in their entirety, in terms of Q-sorts. Similarly, Mergenthaler (1996; McCarthy et al. 2011; Walter et al. 2010) published analyses of emotion-abstraction patterns in terms of the so-called cycles model; however, the analyses focused on rather short-term psychotherapy courses and used small samples of sessions. Members of the Mount Zion Psychotherapy Research Group (Silberschatz and Curtis 1993; Silberschatz et al. 2005; Silberschatz 1991; Weiss et al. 1986) have developed methods to analyze short-term psychotherapy processes in terms of control-mastery theory. Likewise, Howard’s phase model (Howard et al. 1993, 1996) was based on a meta-analysis of rather brief psychotherapies (Fowler et al. 2004). In sum, then, the evidence base for systematic accounts of long-term psychoanalytic change is meager, to say the least.
Change After Psychotherapy (CHAP; Sandell 1987a) was introduced as a partly qualitative and partly quantitative method to assess changes through so-called direct measurement. In contrast to the conventional view of change as a kind of quantitative increment, measured as the difference between the post- and pre-treatment states for a predetermined variable, direct measurement using CHAP is based on a view of change as a qualitative transformation into a new state, with change occurring in any number of aspects. Thus, after an extensive post-treatment interview, the interviewer (independent of or in consensus with colleagues) judges and rates the amount or extent of a patient’s changes on the basis of the transcribed interview. A recent study by Wilczek and Sandell (not yet published) impressively reports high interrater reliability and validity in relation to therapeutic parameters (therapy vs. no therapy; therapy duration) that exceeds those of either raw or residual scores on the Global Assessment of Functioning scale (GAF; DSM IV-R) or the Karolinska Psychodynamic Profile (KAPP; Weinryb and Rössel 1991).
Originally designed as an outcome instrument, CHAP has never been explored as a measure for identifying and analyzing change incidents in a continuous psychoanalysis course, that is, session by session. We will illustrate here the use of CHAP as a systematic method of analyzing material from a full course of psychoanalysis to assess how change develops over time, accumulating little o’s into a big O (Greenberg and Pinsof 1986).
Method
Participant
Maria was forty-three years old when she sought psychoanalysis. She was divorced, had no children, lived by herself, and was slightly overweight. A college graduate, she held an executive position in a company based in Lisbon.
She sought psychoanalysis because, as she claimed, she “wasn’t living her life.” She reported depressive feelings and a tendency to inhibit affect such as anger. Frequently she had symptomatic complaints such as headaches or a sore throat. In the intake interview, Maria referred to themes such as her sense of guilt, fear of trusting people, and need to feel in control.
When Maria was less than four years old, her mother died. The young girl then moved to her paternal grandparents’ home with her father and a younger brother. Regarding her mother’s death, she said that people always thought that she had faced it better than her brother had. Deep inside, however, she felt it was the opposite, but she could hardly express her feelings. Additionally, she mentioned that she used to ignore her siblings. No one outside her family gave her the attention she craved, and she envied schoolmates and friends for their ease in social relations.
When she was six Maria was manifesting secondary enuresis, and her father took her to a psychologist. Looking back, Maria noted that she had always avoided anything related to pleasure. Three years later her father remarried, and they moved to another house. Maria had an intense reaction, feeling that her father was betraying her. When she was ten a second sibling was born (a girl), and a month later Maria was sent away to boarding school, to return home only at holidays. Nevertheless, she said she was excited about this change because she could attend the same school as her mother.
Regarding her stepmother, she said the relationship was grounded in a mutual feeling of resentment and rivalry concerning Maria’s father but also in the hope for a tie-in between daughter and mother.
Maria felt she was her father’s privileged daughter, but she felt guilty for not being able to fulfill his wishes. For some time, Maria wanted to be a boy, once she learned that her father had wanted one when her mother was pregnant with her. From then on, she rejected everything related to the female role.
When Maria was twelve she had a traumatic experience in which a man took her to a private place and tried to pull up her skirt. She became anxious and eventually told her father. A year later she began having claustrophobic symptoms that manifested when she was visiting some caves and that continued into adulthood. For example, Maria would be anxious and unable to move when she was expected to disembark from an airplane with other passengers.
In adolescence Maria felt that her father was very demanding; nothing she did was ever enough for him. She also felt that she lived in a family environment of repressed sexuality. She discovered the intellectualization of sexuality issues as a way to hide her internal confusion, which was heightened by her religious belief that sex is associated with loss of control.
When Maria was twenty, she went abroad to take a postgraduate course and met a boy with whom she lived for a time. She said that this period was the first time she had felt free of her father’s control. After three years or so, she moved to another European country and found another boyfriend. The couple’s relationship did not last, however, and she returned to Lisbon, where she soon married. Their sexual life was not satisfactory to her, she reported, adding that she was in love with the man only until they were married. The marriage lasted for two and a half years and ended when her husband fell in love with a colleague. At the time, Maria was undergoing fertility treatment, but she did not become pregnant. Her father died shortly afterward, and she again left the country to work abroad. When she began to feel depressed, she undertook a psychoanalytically oriented psychotherapy three times a week for a year and a half, during which time her claustrophobic symptoms disappeared. She then returned to Portugal and shortly thereafter began her psychoanalysis.
From the beginning of the analysis, Maria revealed her main conflicts. In the first stage of analysis, Maria elaborated on the difficulty of defying her father, his repression of sexuality, and her feelings of resentment toward him for preferring her stepmother. In a number of sessions she talked about her difficulties with feminine identification. As a child she had not played with dolls, and had envied her brother because their grandfather would take him for walks. She experienced feelings of anger toward her father and her bosses, along with slight irritation with the analyst. In the transference Maria particularly feared being criticized by the analyst. Sessions about her father alternated with sessions about feelings of loss and grief regarding her mother, including regret for not having had more contact with her. The overall feeling was one of sadness and abandonment, and in the transference Maria was concerned that the analyst did not understand her or was not sufficiently empathic.
Maria’s loss of her mother created a sense of failure and insecurity that led her to please others lest she be abandoned. Maria talked about her efforts to anticipate what others would think and say so she could accommodate them. This insecurity was reinforced by her father’s remarriage and demanding attitude.
In love relationships, Maria tended to push men away as soon as she felt attracted to them, thereby avoiding incestuous fantasies or abandonment. Though she eventually married a man who took care of her, she was not really attracted to him. Moreover, Maria’s early loss of her mother brought difficulties at the level of early feminine and maternal identification, as shown by her lack of interest in dolls. The extended period before her father remarried, the way he treated her as if she were his partner, and the family’s idealization of her mother all hindered her sexual identification and heightened her wish for a male identity, which gave rise to envy and competition with men. She competed with colleagues, especially male colleagues. In addition, Maria could not envision herself as a mother; indeed, later in the analysis it became clear that when she was married she did everything she could to avoid getting pregnant, including avoiding sexual relations when she knew she was fertile.
A conventional psychoanalytic contract was established, with three sessions a week at a fixed time, place, and fee. The treatment lasted for three years and eight months, for a total of 383 sessions. The analyst, a candidate in training, had ten years of experience and a Freudian orientation. His clinical style was characterized by few interventions per session, with interpretations directed mainly to central conflicts. The patient usually saw the interpretations as meaningful and soon began trying to elaborate on them during the session and in following sessions.
The transference has changed from a slight hostility in the early months of analysis (she later said that at the beginning she preferred her previous therapist) to a positive and slightly erotic transference that continued with ups and downs until the end of the third year of analysis, when she was confronted with a more real analyst. She was angry at the analyst’s failures (he arrived quite late for one session and another session ended early, in both cases for reasons beyond his control).
Instrument
We used a Portuguese translation of the CHAP scales, developed by Sandell (1997). The translation was done by Sá (2008) by comparing it with a previous translation (Cunha 2006). The CHAP scales aim to assess whether the patient feels that he or she is being qualitatively “transformed” as a person and how much and in what ways he or she now feels different, consciously and unconsciously.
Based on content analyses of post-therapy interviews, the CHAP scales define four aspects of change: symptoms, adaptive capacity, self-insight, and basic conflicts. The experience of having changed in terms of symptoms may be expressed in a number of ways, such as when the patient says she has no (or fewer) symptoms, does not mention symptoms at all, or reports experiencing the same symptoms as before but being able to use them adaptively or no longer suffering from them. Adaptive capacity is seen when the patient recounts situations that she could not have managed before but now approaches in adaptive ways without experiencing conflict or symptoms. Self-insight is indicated when the patient describes how she now understands previously incomprehensible habits, attitudes, relationships, and actions. Basic conflicts derive from traumata and relational complications and act as filters through which new situations are perceived, interpreted, and acted upon.
In the CHAP instruction manual, the definition of each rating variable is accompanied by an extensive but nonexhaustive list of twelve to twenty examples of signs of change to help the evaluator understand the meaning of each variable: for example, symptoms (S), “Symptoms have decreased in number, frequency, duration, severity, strength”; adaptive capacity (AC), “Patient relates concrete situations where he/she has acted more adequately than before, e.g., more assertively, flexibly, nonaggressively”; insight (I), “Patient says he/she realizes and understands the background and meaning of his/her problems”; basic conflicts (BC), “Patient is not as rigid, stereotypical, extreme as he used to be”; and extratherapeutic factors (EF), “Patient has changed while in some relation posing as therapy (‘pseudo-therapy’).” A single incident or sign of change may indicate change in only one variable (pure) or in more than one variable (mixed). The CHAP rating procedure has adequate reliability and validity (Sandell 1987b). In the present study interrater agreement was obtained by the following formula: total number of incidents where there was agreement divided by the total of agreement plus the total of disagreements. The median agreement between the two raters for all the 383 sessions was .92, with a range between .86 (symptoms) and .96 (insight) across the five scale variables.
Procedure
The data were notes from all sessions of a full psychoanalysis of 383 sessions. Notes were taken by the analyst after each session; initially they were taken not for research purposes but for supervision. The notes have a descriptive character, containing statements (as near verbatim as possible) by patient and analyst, and at times include the analyst’s subjective comments regarding the process. To ensure confidentiality, the analyst deleted any details that might have allowed identification of the patient before the researchers’ ratings.
In this study, we use CHAP in a way different from its original use. Rather than use it to analyze interviews after the end of the treatment, we use it to identify changes session by session. The CHAP manual notes that in addition to follow-up interviews, regular therapy sessions, recorded either on tape or in process notes or similar documents, can be used for rating the experience of change. We chose to rate incidents in two phases. In the first we looked for incidents of change across sessions, while in the second we classified the incidents according to the five variables. Each session was read to identify sentences indicating change. In this study these sentences are identified as incidents (several examples of change incidents are given in the results section). Identifying an incident of change was not difficult. Often the patient used linguistic markers like “now” or “then” that facilitated the identification. Sometimes the verb tense in the sentence allowed us to realize that there had been something different from the previous state. It was more difficult, however, to identify the type of change—for example, to say whether it was a change in adaptive capacity or in the basic conflict—but use of the CHAP manual and training has resolved most of the difficulty.
The study began with a training phase to improve the correct identification of change incidents with guidance of the CHAP manual (Sandell 1997). For this purpose one-sixth of all the sessions were randomly selected and independently evaluated by the two raters (master’s students in psychology). The training consisted first in identifying the incidents and then in a classification in five variables. Every ten rated sessions, the raters and the senior researcher discussed disagreements using the CHAP manual. The training was considered satisfactory when the agreement was greater than .80. The analysis began with reading the initial sessions in order to identify the patient’s symptoms, conflicts, and characteristics at the beginning of treatment.
After the training phase, all 383 sessions were read in chronological order to identify incidents of change. Subsequently, the sessions were reread but in a random sequence. The next step involved the classification of incidents according to the five CHAP variables.
Results
Number of Incidents per Variable
In all, 606 incidents of change were identified in the 383 sessions, with 109 sessions involving no change incident. There were fewer sessions without changes in the third year of analysis. In the first two years, on average, about one change incident occurred per session. From the second year (from June 2006) until the end of the analysis, with the exception of September and October 2006 and April and July 2007, the number of change incidents increased to about two incidents per session on average.
The distribution among the five rating variables revealed 198 incidents related to basic conflicts, 157 related to adaptive capacity, 154 related to insight, and 97 (a significantly lower number) related to symptoms. Only four incidents related to extratherapeutic factors were identified.
Most of the incidents were rated on only one variable (pure) rather than more than one rating variable (mixed incidents). On the symptoms scale, only 67% of incidents were considered pure, whereas a significantly higher percentage of incidents on the other scales were considered pure: insight, 95%; basic conflicts, 87%; and adaptive capacity, 86%. Sixteen incidents revealed simultaneous changes in both symptoms and basic conflicts, and fifteen incidents revealed simultaneous changes in symptoms and adaptive capacity. The four incidents related to extratherapeutic factors were all mixed, two with adaptive capacity, one with insight, and one with basic conflicts.
Change Incidents over Time
Figure 1 shows the number of incidents for each of the five rating variables over the four years of psychoanalysis. Relative frequencies (number of incidents per number of sessions) are grouped in periods of three months. The results presented in Figure 1 are based on ratings by one of the two raters, the translator of the CHAP manual.
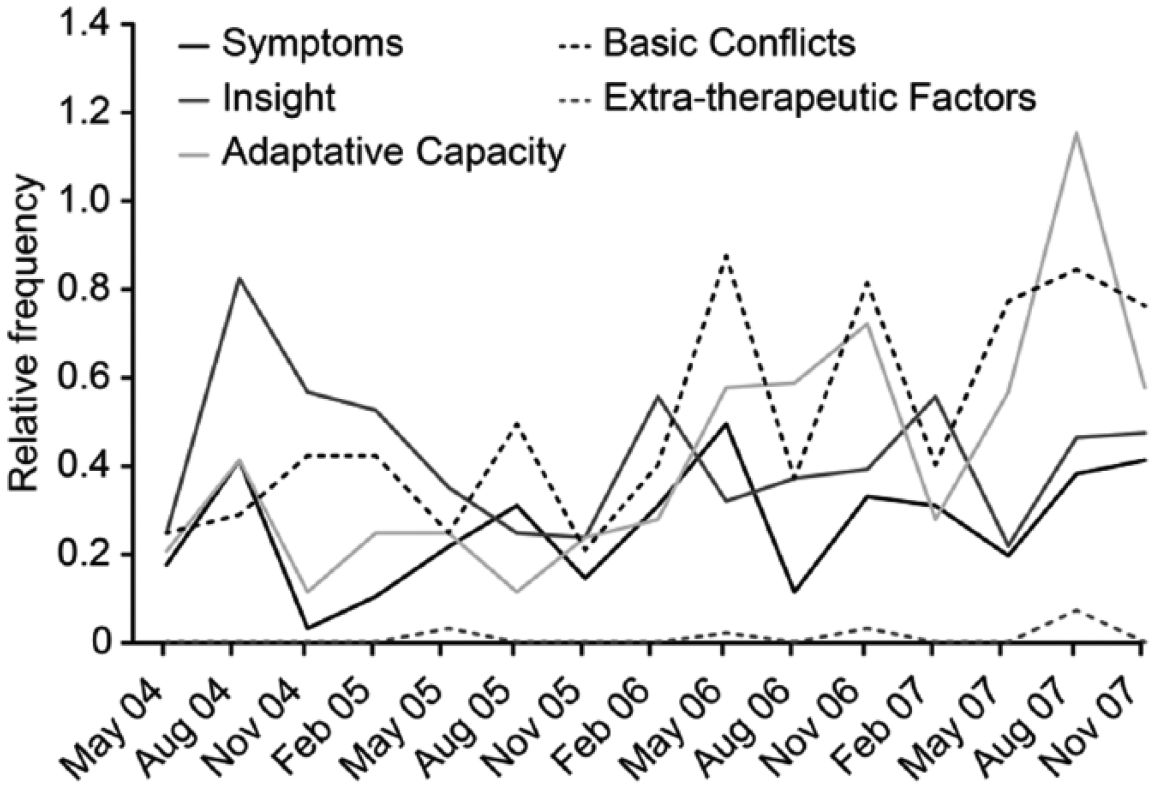
Relative frequency of change incidents for the five dimensions grouped in periods of three months
In the first trimester (May, June, and July 2004), the number of incidents was relatively similar for all the variables (8 incidents for basic conflicts, 7 for adaptive capacity, 6 for symptoms, 8 for insight). In the second trimester, however, incidents related to insight were much more evident (21 incidents); this was the largest number of change incidents related to insight during the first year (a total of 52 incidents related to insight). Interestingly, in the second year few change incidents occurred. However, in the third year the number of incidents increased across all variables, especially related to basic conflicts, adaptive capacity, and insight. Although incidents related to symptoms were generally infrequent, the number of incidents related to symptoms also reached a peak during the third year, at 41. The last year of psychoanalysis (actually only eight months) was similar to the third year, with more changes in adaptive capacity and basic conflicts. Extratherapeutic changes appeared occasionally, but as exceptions, during the entire course of psychoanalysis.
Examples of Incidents of Change at Different Stages of Psychoanalysis
To illustrate types of change incidents at different stages, we present some change incidents related to Maria’s loss and grief concerning her mother and her own subsequent reluctance to become a mother. The death of Maria’s mother was addressed from the beginning of the psychoanalysis: “I was the one who reacted more intensely [compared with her siblings], but I could not show it” (session 1). “The death of my mother gives me sadness but also anger. . . . I should have felt angry at the time, but I was not able to. I think that from then on I needed to be well behaved. . . . I had never realized the meaning of anger” (insight; session 4).
Early in the second year of the analysis, Maria confessed that she had done her best not to become pregnant. She thought she would not be a good mother and was afraid that something would happen to her children: “I did not see myself in the role of mother. I did not want children; it terrified me. I believed myself incapable of raising them. I always thought I would not be a decent mother, a mother like I thought I should be” (session 128). “But to think that I would be responsible for someone . . . if anything happened to my child . . . if something happened to them would be unbearable. . . . I remember thinking that I could die. What would they feel if their mother died?” (session 129). However, at the end of the second year, these feelings began to change: “One of my colleagues announced that she is pregnant. In the afternoon, I realized that I was weird. When I was coming here, I realized that I was envious” (insight; session 166).
In the third year of the psychoanalysis, we observed greater changes. Maria no longer needed to hide her sadness and idealize her childhood. She accepted the loss of her mother and felt empowered to live her own life. During this year, the loss of her mother and her grief were addressed repeatedly but to a lesser extent than in the second year. She changed from feeling that she would not be able to be a mother to actually wanting to become pregnant and feeling that she was indeed able to be a mother: “When my mother died, her story came to an end, but not mine. . . . In a way, it seems like I did not know this—as if in some way I thought I had died a bit, or I had to live with this burden of being alive” (insight; session 237). “I started to cry, thinking about my mother. Suddenly, I realized that more than the lack of my mother, I miss not being able to share good things with her; I cannot laugh with her” (starts crying) (insight; session 261). “After weeping, I found myself writing a letter to my mother. It made me feel better. It was what I used to say here, that I could not be happy, and then it was as if the knot or stone inside me shattered, and I felt as if I was allowed to live, to laugh” (basic conflicts; session 261). “Another thing was that I thought about adopting. I woke up one day and had a flash [of insight]. I was afraid that I was deceiving myself. Maybe it was to redeem myself from the guilt of having avoided having children” (insight; session 261). “Although I thought I was incapable of being a mother. . . , now I would be able to do the job” (basic conflicts; session 341). “When I meet people I have not seen for a while and notice that they have children, I find myself with gnawing envy, and this is more intense when they are older people with small children” (insight; session 363).
Overcoming Core Conflicts
In the content analysis of change incidents, we explored when the patient’s main conflicts were overcome. Maria’s insight into and elaboration on her conflicts occurred repeatedly throughout the analysis; nonetheless, we were able to identify phases in which changes were more salient and definitive.
Regarding the loss/mourning conflict, Maria changed from needing to hide her sadness and idealize her childhood to accepting the loss of her mother and feeling empowered to live her own life. This topic was addressed repeatedly but was overcome only after the second year and a half of analysis (see the incidents of session 261 above: “then it was as if the knot or stone inside me shattered”).
For the first time, Maria felt the desire to be a mother, feeling that she had the capacity to be a mother, wanting to become pregnant, and envying couples with children. At the end of the third year, she already felt able to be a good mother. The topic appeared in both her dreams and her speech (“I dreamed I was pregnant . . . ” (insight; session 338); “When I thought I was incapable of being a mother, there were several things . . . ; now I would be able to handle them” (basic conflict; session 341; see also the incident of session 363 above).
Regarding her insecurity, Maria no longer constantly worried about what others thought of her. She began to trust herself and others and to dare to share feelings and experiences with them. At the end of the third year, Maria noted: “Now, I show more ability to say what I like without worrying about what others will think, or if they will criticize me” (basic conflict; session 307). Then, after three and a half years, Maria said, “I speak of myself with a naturalness I did not have. Now I have no desire to hide. I make comments about myself, unimportant comments, that I did not before. But I notice that I do it with a lightness that I did not” (basic conflict; session 363).
Maria’s interactions with other people began to be guided by spontaneity, and her relationships deepened; she began to be receptive and welcoming toward others, and stopped fending people off. At the beginning of the third year, she said: “A coworker . . . was there all weepy, and I asked her why. She burst into tears . . . , and she told me that I had changed so much now. I asked how, and she said I was so aloof before” (basic conflict; session 233). At the end of the third year, Maria said: “today I noticed a curious thing. My office has become a place to open one’s heart for my colleagues” (basic conflict; session 327).
Maria began to be able to be intimate with men, and she no longer attempted to keep them at a distance when she was attracted to them or when she wanted them to care for her, something she confessed would occur with her husband. Her guilt associated with sexuality also waned, and her relationships with men began to be more flexible. She no longer wanted to be like men, and she felt comfortable with her desire to seduce them. At the end of the third year of analysis, Maria started dating men: “Since September, I have been regularly dating a friend with whom I go to concerts and toward whom I have mixed feelings” (adaptive capacity; session 315). She also resumed sexual activity (adaptive capacity; session 342). Referring to two men whom she had been regularly dating, she stated: “Now, I have to manage the time to date one and then the other” (session 325). Moreover, after three and a half years of therapy, she noted: “With men I also feel more relaxed . . . without the fear of being the wrong person” (basic conflict; session 372).
Maria’s competition with colleagues and her boss diminished, and she became more collaborative and creative. Her colleagues began to enjoy working with her and asking for her help in both professional and personal matters. At the end of the third year, she stated: “At work, my boss and I seem to be on a honeymoon. There are lots of projects. I put the old scores aside” (adaptive capacity; session 302). “Of course I’ve changed a lot . . . ; one of the things he [the boss] said was that now I’m the old Maria he once knew and that he likes to work with me” (basic conflict; session 325).
Discussion
We have endeavored here to present a new way of using the CHAP scales. Specifically, our study used the scales to systematically analyze change incidents in every session of a psychoanalysis, and we found incidents of change in three out of four sessions. Among all 383 sessions of the analysis, only 109 lacked a change incident. The analysis seems to show that the change in patients visible at the end of a psychoanalysis results from small changes that accumulate from session to session throughout the course of treatment. Although this conclusion comports with clinical intuition, empirical evidence to support it has heretofore been lacking. We think that the patient’s characteristics facilitated the numerous change incidents and their identification. Maria was a very articulate and verbally explicit patient who used linguistic markers that clearly identified the occurrence of changes. She also had an unusual willingness to engage in the psychoanalytic process.
The list of incidents presented in the CHAP manual provided a suitable guide for identifying change incidents in the sessions; after a period of training in use of the scales, identifying and categorizing these changes was not difficult, as indicated by the high concordance between the two raters. Although CHAP’s five rating variables and list of “change signs” were identified in the original study by using post-psychotherapy interviews, our study showed that they are equally useful for identifying change incidents during psychoanalytic sessions. The CHAP insight scale may be a more robust way of evaluating insight in sessions than the instruments currently used (GAF, KAPP). This will allow further process studies on the relationship between interpretation and insight.
Among 606 identified incidents of change, most were related to basic conflicts, while the fewest were related to symptoms. We believe that this result stems from effects of the patient’s previous psychotherapy. Before she began her analysis, Maria was in psychoanalytic psychotherapy for a year and a half. In that psychotherapy she worked on her claustrophobic symptoms, and they eventually disappeared. Maria’s initial request upon starting her analysis was not that her symptoms be eliminated but that her difficulties in living authentically be addressed, thus revealing an intrapsychic conflict.
In quantitative terms, the therapy appears to have involved four phases. The first year was characterized by a high frequency of change incidents related to insight, whereas in the second year few change incidents related to any CHAP rating variable occurred. Then, in the third year, the frequency of change incidents related to basic conflicts and adaptive capacity increased considerably, surpassing changes related to insight. The fourth year was similar to the third, but with a spurt of changes related to adaptive capacity, possibly as consequences of the changes in basic conflicts.
Detailed analysis of the data over time allowed us to identify patterns of therapeutic change throughout the full psychoanalysis. What is the meaning of the patterns that we identified? Blum (1979) argued that psychoanalysis develops in a sequence of stages. However, nothing informs us of when these stages occur, what their characteristics are, or whether they follow a specific order in every patient. Globally, compared with the other types of change, relatively more incidents related to insight appear to occur at the beginning of an analysis. This finding is in line with the findings of Johansson et al. (2010) regarding psychodynamic therapy. In their report, insight increased dramatically early in treatment among the transference interpretation group; however, it changed little over the following years, whereas interpersonal functioning continued to improve. In our study, incidents related to basic conflicts and adaptive capacity exceeded those related to insight only in the third year of analysis. It is logical that a patient’s acquisition of self-insight into conflicts and behavior patterns would not lead immediately to changes in adaptive capacity and to resolution of basic conflicts, but rather would take some time before strong, definitive changes would be observed. A review of empirical studies on insight (Castonguay and Hill 2007) provides very little information about patterns of change. However, at least one study (Grande et al. 2003) has shown that patients who had gained definitive insight into their problems during psychotherapy were more competent in addressing life’s daily struggles after their treatment had ended.
The clinical and qualitative evaluation of the content of the changes indicates that the first year corresponded to a phase characterized by Maria’s high curiosity about herself. She elaborated on her castrating father, the loss of her mother, and her relationship with her ex-husband, and competition and conflicts with colleagues were revived. The second year was then a period of a certain stagnation corresponding to a phase that began with the confession of erotic fantasies to the analyst (July 2005) and two meetings abroad with an old boyfriend (September 2005 and March 2006), perhaps to avoid facing the erotic transference. The second meeting helped her elaborate on her relationship with her boyfriend, with men in general, and with her father. The third year was a period of progress and consolidation. Maria’s central conflicts, such as her difficulties with feminine identification, insecurity, and rivalry with men, were substantially worked on and overcome by the end of the third year, with loss and grief having been substantially overcome earlier, in the middle of the second year. Her erotic transference fantasies were also elaborated on and resolved by the end of the third year. In the fourth year changes were consolidated, and topics that had once aroused anxiety disappeared from the sessions.
Crossing the quantitative data with the clinical and qualitative data, we find that Maria’s first year corresponded to a phase of great curiosity and insight and that the second year, in which few change incidents occurred, corresponded to a phase of stagnation. The mildly erotic transference, which showed some signs after the first six months, could be a partial explanation for less change in the second year. This transference was not resolved immediately but had its ups and downs and was completely overcome only at the end of the third year of analysis. The profusion of changes in the third year (the most for all years) in basic conflicts culminated with the resolution of Maria’s main conflicts and with her increased adaptive capacity. In short, we speculate that levels of insight higher than levels for the other variables correspond to phases when the patient’s engagement in resolving her difficulties increased but when her main conflicts were not definitively overcome and adaptive capacity achieved; that a lowering in all rating variables corresponds to periods of stagnation or possibly a period of slowly working through these insights; and that levels in basic conflicts and adaptive capacity higher than levels for other variables correspond to phases in which conflicts were being worked on and resolved and adaptivity increased. The extent to which these characteristics are generalizable to other patients is a matter to be confirmed in future studies.
The phase model suggests that some stages must conclude before others can proceed (Howard et al. 1996). Our results may confirm this model. We assume that the remoralization and remediation phases could have begun and been partly resolved during Maria’s earlier psychotherapy, during which her claustrophobic symptoms disappeared. However, the final phase of this model, the rehabilitation phase, seems to have been completed only in her psychoanalysis, which led Maria to overall improved adaptive functioning.
We conclude that the change patterns for the different categories appear to confirm a structural change during Maria’s psychoanalysis. However, to better understand the qualitative meaning of these changes, we must cross them with the content of the change incidents. Incidents such as “I think that, right now, I would not change my life with anyone. For the first time, I have the feeling that it is me who is living my life” (session 279), “I spent so long wanting to change jobs, being picky, that it is interesting that I now want to keep it. [It’s curious that your boss is the same.] But I am different!”(session 338), and “I feel good; I feel whole” (session 363) all had high scores on the basic conflicts scale; thus, they appear to confirm the resolution of Maria’s initial request for true, adaptive, structural changes. Also, they appear to confirm Sandell’s suggestion (2005) that structural change may primarily be defined by its permanence, as evidenced by repeated observations across time.
Some considerations should be made about the quantitative approach we used. We worked with the frequencies of change incidents and not with the magnitude (the amount of change) of each incident, but frequency of occurrence does not always equal its importance. On the other hand, the quantitative approach allows for the observation of patterns or sequences of change, but only the content analysis of the incidents, of the sessions, and of the therapy as a whole allowed us to know when the basic conflicts of the patient were overcome. In other words, the study reveals the advantage of the combination of quantitative and qualitative/clinical approaches.
The high number of change incidents related to insight during the first year relative to those related to the other variables was somewhat unexpected. We attribute this finding to the function of insight in expediting the analytic process. Blum (1979) underlined the circular interaction between insight and productive analytic work, and our results do not appear to contradict that idea. Our results are also compatible with the study by the Mount Zion Psychotherapy Research Group (Weiss et al. 1986), which showed that in the first hundred sessions of a psychoanalytic psychotherapy a gradual increase in sensibility that appears to reflect the acquisition of insight occurs. Bearing in mind that psychoanalysis is a continuing process even when it ends (Waldron 1997), we could argue that Maria transferred some of her considerable ability to comprehend and recognize some aspects of her life from her psychoanalytic psychotherapy to her psychoanalysis. However, by the end of her psychoanalysis, the number of change incidents related to insight decreased. We assume that this reduction is attributable to the absence of unresolved conflicts and evidence that the psychoanalysis was coming to a successful end. We suggest that the trajectory of change for the insight variable may lead to the same conclusion drawn by O’Connor et al. (1994): insight, even in successful therapy, may not show or contribute to sudden change. Thus, improved individual functioning may best be understood when the evolution of insight through the entire course of therapy is considered, separate from its quality, conviction, and content.
An important limitation of this study concerns the type of data used. Our study is based on written notes rather than audio records. Although the notes do have a descriptive character, containing sentences that are as near verbatim as possible, they are not an entirely acceptable substitute for transcripts, and the study should be repeated with recorded audio sessions. Additionally, although systematic case studies may allow for a better understanding of the process compared with other types of studies, the present case results cannot be generalized. For instance, this patient expressed her changes and insights spontaneously, with sophisticated thinking and language. We would like to use the same procedure with other patients to determine whether changes in patients in which the psychoanalytic work is more silent or “underground” can be evaluated in this manner.
Psychoanalysis is understood as a meticulous step-by-step process, and this is the first report, to our knowledge, that describes this cumulative process throughout a full psychoanalytic treatment. It would be interesting to repeat this study using the same method on multiple cases and to compare them to determine whether common patterns between them arise. Our study is a descriptive study (Llewelyn and Hardy 2001) but the accumulation of descriptive studies like this could help in building models of change. To do that, future studies should also use meaningful outcome measures to relate change patterns to effectiveness of treatment and should address the factors that cause or relate to the observed changes, such as patient personality characteristics or object relations, transference-countertransference processes, and the interpretive work.
Footnotes
António Pazo Pires, Associate Professor, Department of Clinical and Health Psychology, ISPA–Instituto Universitário, Lisbon. João Gonçalves, psychologist in private practice, London. Vânia Sá, psychologist in private practice, Lisbon. Andrea Silva, Psychologist, Instituto de Segurança Social dos Açores, Ponta Delgada, Portugal. Rolf Sandell, Professor and Senior Researcher, Department of Psychology, Lund University, Sweden; member, Swedish Psychoanalytic Association.