
Abstract
Background
Direct oral anticoagulant dabigatran was first introduced as a fixed-dose drug without routine coagulation monitoring, but current recommendations suggest that diluted thrombin time can be used to estimate plasma drug level. The aim of this study was to assess a diluted thrombin time assay based on the same thrombin reagent already used for traditional thrombin time measurements that reliably measure low to intermediate plasma dabigatran levels.
Methods
We included 44 patients with atrial fibrillation who started treatment with dabigatran 150 mg (23 patients) or 110 mg (21 patients) twice a day. Blood samples were collected at baseline (no dabigatran) and 2–4 weeks after the beginning of dabigatran therapy at trough and at peak. Plasma dabigatran levels were measured with diluted thrombin time and compared to liquid chromatography with tandem mass spectrometry as the reference method. The performance of the diluted thrombin time was compared to Hemoclot® Thrombin Inhibitor and Ecarin Chromogenic Assay.
Results
In ex vivo plasma samples, diluted thrombin time highly correlated with the liquid chromatography with tandem mass spectrometry (Pearson’s R = 0.9799). In the low to intermediate range (dabigatran concentration ≤ 100 µg/L) diluted thrombin time correlated significantly more closely to the liquid chromatography with tandem mass spectrometry (R = 0.964) than Hemoclot® Thrombin Inhibitor (R = 0.935, p = 0.05) or Ecarin Chromogenic Assay (R = 0.915, p < 0.01). It was also the only functional assay without any significant bias in the low to intermediate range. Both trough and peak diluted thrombin time values were similar to liquid chromatography with tandem mass spectrometry.
Conclusion
We conclude that the diluted thrombin time assay presented in this study reliably detects dabigatran and that it is superior to the Hemoclot® Thrombin Inhibitor assay in the low to intermediate range.
Introduction
Dabigatran is a direct thrombin inhibitor developed for the prevention and treatment of patients with atrial fibrillation and venous thromboembolic disease. Oral administration of the prodrug dabigatran etexilate produces a predictable pharmacodynamic effect; therefore, fixed-dosing without routine coagulation monitoring or dose adjustment is recommended. However, plasma concentrations of the drug vary widely across patient population, depending on absorption, renal function and other patient characteristics. 1 Therefore, in certain clinical situations such as bleeding or thromboembolic event, renal failure, potential overdose and major surgery, measurements of the dabigatran effect may be desirable and even important. 2 The reference method for dabigatran concentration measurement is liquid chromatography with tandem mass spectrometry (LC-MS/MS). 3 However, this method is only available in specialized centres and usually only during weekdays. Therefore, coagulation assays that estimate plasma dabigatran concentrations from its anticoagulant effect are currently used.3,4 Routine coagulation assays such as activated partial thromboplastin time (aPTT) and prothrombin time (PT) were shown to be inadequate for measuring anticoagulant effect of dabigatran, while thrombin time and ecarin clotting time showed linear and steep dose–response relationship in an in vitro study. 5 However, thrombin time was shown to be too sensitive, prolonging the measurement time exceedingly, while ecarin clotting time is not widely used. 5 In recent years, a commercial assay for measuring plasma dabigatran has become available (Hemoclot® Thrombin Inhibitor, HTI). It is based on thrombin time, in which a plasma sample is diluted with saline solution and normal pool plasma (NPP) before initiation of coagulation with thrombin. Such diluted thrombin time (dTT) yields shorter coagulation times 6 and is applicable to different coagulation analysers. Current recommendations from the Scientific and Standardization Committee of the International Society for Thrombosis and Haemostasis indicate that a dabigatran-calibrated dTT can be used to estimate drug levels 2 . However, HTI has been found unreliable in the lower range of drug levels and unsuitable to measure dabigatran levels below 50 µg/L.3,7 Furthermore, since many laboratories already use a thrombin reagent for measuring the traditional thrombin time, it would be preferable to use the same reagent for both the traditional thrombin time and the dTT. The aim of this study was to introduce a dTT assay based on the same thrombin reagent already used for traditional thrombin time measurements, which reliably measures low to intermediate plasma dabigatran levels. This study was conducted as a methodological substudy of the previous submitted paper on the same subjects 8 .
Patients and methods
Patients and blood sampling
We included 44 patients with atrial fibrillation who started treatment with dabigatran 150 mg (23 patients) or 110 mg (21 patients) twice a day at the Anticoagulation clinic (University Medical Centre, Ljubljana, Slovenia). A lower dose of dabigatran was prescribed to patients with moderately impaired renal function (estimated glomerular filtration rate 30–50 mL/min), elderly patients (>75 years), those with a history of major bleeding, those on amiodarone, verapamil or antiplatelet drugs and to frail patients. All patients signed a consent form agreeing to participate in the study. The study was approved by the Medical Ethical Committee of the Slovenian Ministry of Health.
Blood was collected from each patient at baseline (no dabigatran) and then again 2–4 weeks after dabigatran therapy initiation at trough (12 ± 1 h after the previous dabigatran ingestion) and at peak (120 ± 5 min after the last dabigatran ingestion) into 4.5 mL vacuum tubes containing 0.11 mol/L sodium citrate (9:1 v/v) (Becton Dickinson, Vacutainer System Europe, Heidelberg, Germany). Plasma was prepared with 30 min centrifugation at 2000 g and 4℃, aliquoted into small plastic vials, snap frozen in liquid nitrogen and stored at −70℃ until analysis.
Methods
The in-house dTT was performed on the CS2100i coagulation analyzer (Sysmex Europe GmbH, Norderstedt, Germany) with the following protocol: 10 µL of patient plasma was diluted with 10 µL of saline solution (sodium chloride Braun 9 mg/mL, B Braun, Melsungen, Germany) and 100 µL NPP prepared in-house from 31 healthy volunteers. After 90 s of incubation, the reaction was started with the addition of 100 µL of the Test-Thrombin reagent (Siemens, Healthcare Diagnostics Products GmbH, Marburg, Germany) and the reaction followed for 350 s. If dTT was above 350 s, plasma was diluted with NPP (one volume of test plasma was mixed with one volume of NPP) and remeasured. The assay was calibrated with the Dabigatran Plasma Calibrator (Hyphen BioMed, Neuvillesur-Oise, France) and NPP (0 µg/L dabigatran). The intra- and inter-assay precision was evaluated using the Dabigatran Control Plasma C1 (target value 105–145 µg/L) and C2 (target value 296–356 µg/L) (Hyphen BioMed, Neuvillesur-Oise, France) measured in duplicates in 20 consecutive days.
dTT results of ex vivo plasma samples from patients receiving dabigatran were compared to free plasma dabigatran concentration determined with liquid chromatography – tandem mass spectrometry (LC-MS/MS), as described previously, 3 which we considered as the reference method. Performance of the in-house dTT was compared to the HTI (Hyphen BioMed, Neuvillesur-Oise, France) and Ecarin Chromogenic Assay (ECA-T, Diagnostica Stago, Asnieres, France). HTI, which is based on the same principle as the in-house dTT, was performed on the CS2100i analyzer (Sysmex Europe GmbH, Norderstedt, Germany) according to the manufacturer’s instructions: after dissolving, the reagents were left at room temperature for 30 min and regularly mixed before they were inserted into the instrument. To 45 µL of plasma 135 µL of saline solution was added. To 25 µL of this mixture additional 25 µL of saline solution was added, followed by 100 µL of buffered NPP and 100 µL of thrombin reagent. ECA-T is a quantitative chromogenic assay for the measurement of direct thrombin inhibitors in plasma. In this assay ecarin, snake venom that activates prothrombin through a specific proteolytic cleavage, was added to the diluted plasma. The formation of p-nitroaniline was detected spectrophotometrically at 405 nm. The assay was performed on the STA-Compact Max (both Diagnostica Stago, Asnieres, France). Both HTI and ECA-T were calibrated, as well as the dTT, with the Dabigatran Plasma Calibrator (Hyphen BioMed, Neuville-sur-Oise, France) and NPP (0 µg/L dabigatran).
dTT method validation and statistical analysis
Linearity of the calibration curve was tested with linear regression and reported as R2. R2 was also calculated between the tested methods (dTT, HTI and ECA-T) and the LC-MS/MS. Limit of Blank (LoB) was reported as the highest result of a blank sample (NPP), lower limit of detection (LoD) was calculated as an average of + 3 standard deviations and Limit of Quantification (LoQ) as an average of + 10 standard deviations of NPP. 9 Within-run and between-run imprecision and accuracy of the dTT were determined by performing duplicate low and high control measurements in 20 consecutive days and reported as coefficient of variation (CV). Accuracy was calculated as the difference between the target and the average measured value divided by the target value (×100%). For statistical analysis all negative dabigatran values obtained from ex vivo plasma samples with the dTT, HTI or ECA-T were denoted as 0 µg/L. For statistical purposes all the LC-MS/MS results < 2 µg/L were denoted as 2 µg/L. The significance of the difference between two correlation coefficients was assessed with the Fisher r-to-z transformation. Systemic bias in the lower range was assessed by calculating Pearson’s correlation coefficient between the LC-MS/MS and the difference between the tested method (either dTT, HTI or ECA-T) and LC-MS/MS. Baseline, trough and peak dabigatran levels in ex vivo samples were presented as medians (1st to 3rd quartiles). The differences between baseline, trough and peak values obtained with different methods were tested with non-parametric repeated measures ANOVA (Friedman test) and for post-hoc analysis Dunn’s Multiple Comparison Test was utilized. Thrombin time CV obtained from several batches of NPP was 4.9%. Two different test-thrombin lots were tested on a different set of samples and produced comparable results (average CV of 10%).
Results
dTT calibration curve was linear, with R2 of 0.9996 (Figure 1). There was no deviation from linearity up to 920 µg/L. For this assay, LoB of 2.7 µg/L, LoD of 2.8 µg/L and LoQ of 8.2 µg/L were obtained. Assay imprecision and accuracy are shown in Table 1.
Average ± SD of three dTT calibration curves obtained four months apart (28.0 ± 0.3 s at 0 µg/L, 45.6 ± 2.2 s at 35 µg/L, 175.1 ± 4.1 s at 240 µg/L and 298.4 ± 15.7 s at 470 µg/L). The within- and between-run imprecision and accuracy of dTT.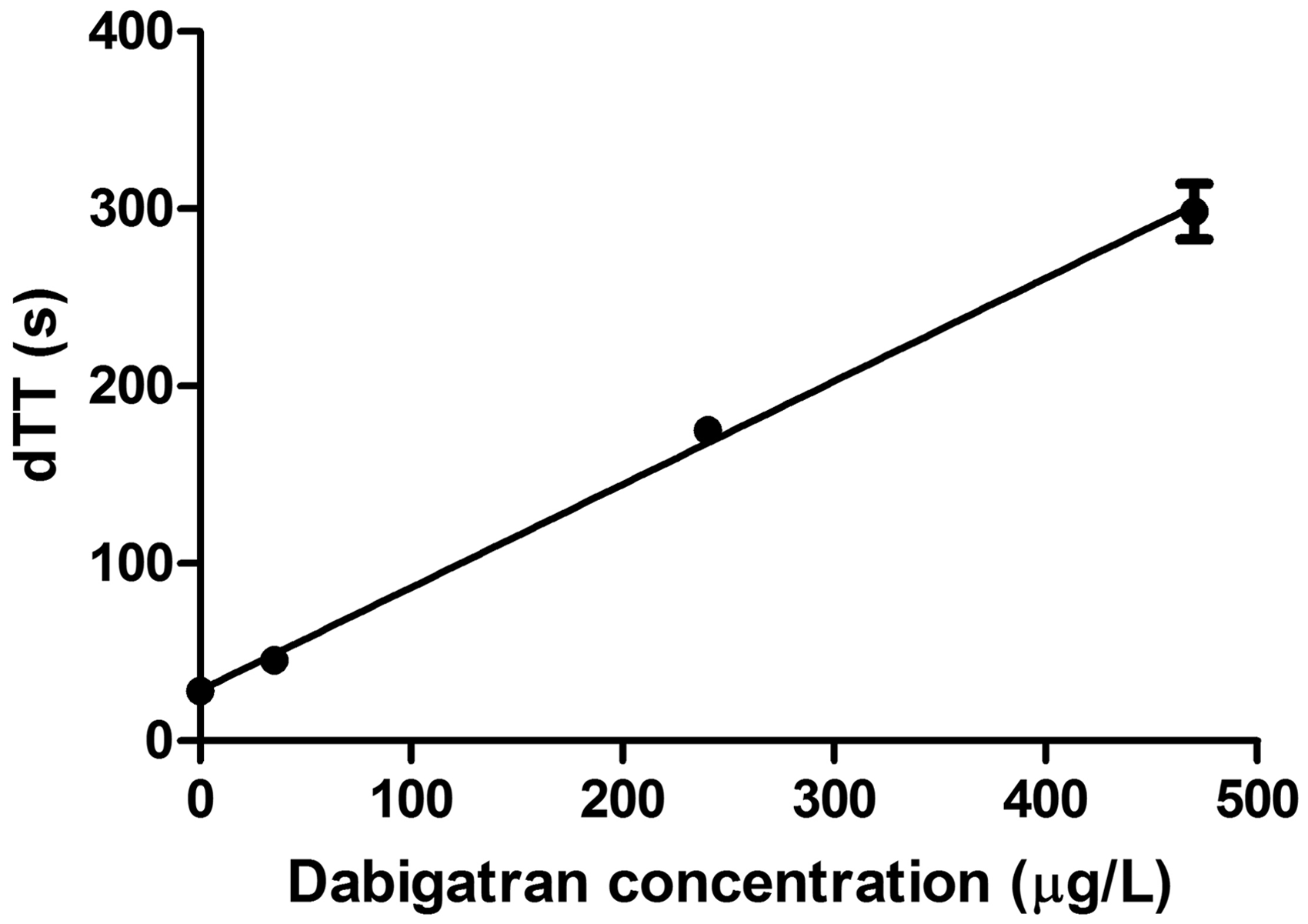

When ex vivo plasma samples were measured, dTT correlated highly with the LC-MS/MS (Pearson’s R = 0.9799). Both HTI and ECA-T also highly correlated with the LC-MS/MS (R = 0.9473 and 0.9801, respectively), but the correlation coefficient of HTI was significantly lower compared to the correlation coefficients of dTT and ECA-T (p < 0.001, Figure 2). In the low to intermediate range (dabigatran concentration ≤ 100 µg/L, n = 86) dTT correlated significantly more closely to the LC-MS/MS (R = 0.964) than HTI (R = 0.935, p = 0.05) or ECA-T (R = 0.915, p < 0.01). The Bland–Altman plot of the low to intermediate range data showed no systemic bias for dTT, while for HTI and ECA-T a systemic bias was evident (R = −0.36 and−0.31, respectively, both p < 0.05) (Figure 2).
Comparison of dTT, HTI and ECA-T assays with the LC-MS/MS (reference method) for the whole measuring range (first column), low to intermediate range (≤100 µg/L; middle column) and the Bland–Altman plot of the low to intermediate range (last column). Dabigatran levels between 50 and 250 µg/L are denoted by empty circles and levels below 50 and above 250 µg/L are denoted with full circles.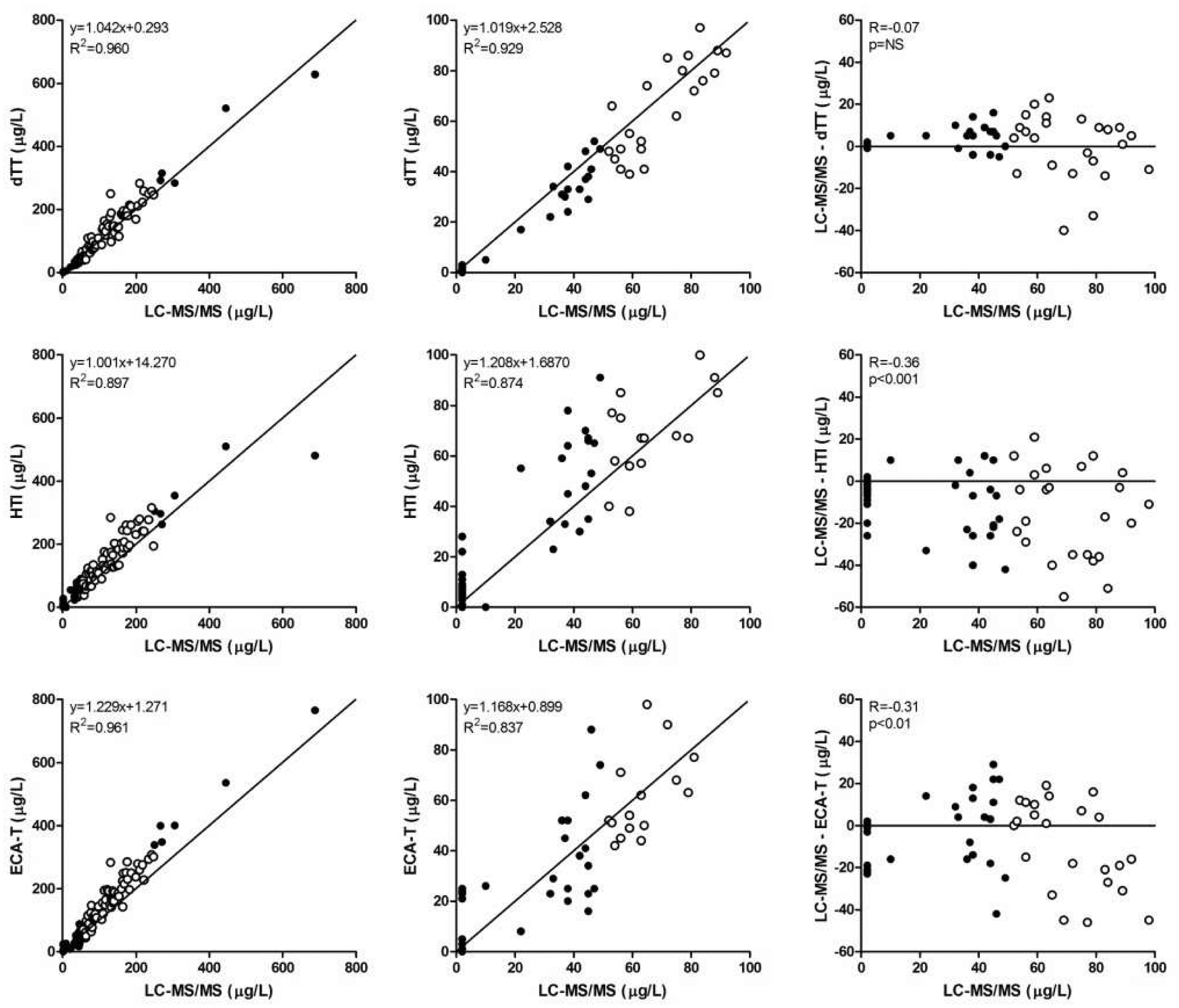
Dabigatran concentrations at baseline (no dabigatran), trough and peak measured with LC-MS/MS (reference method), dTT, HTI and ECA-T.
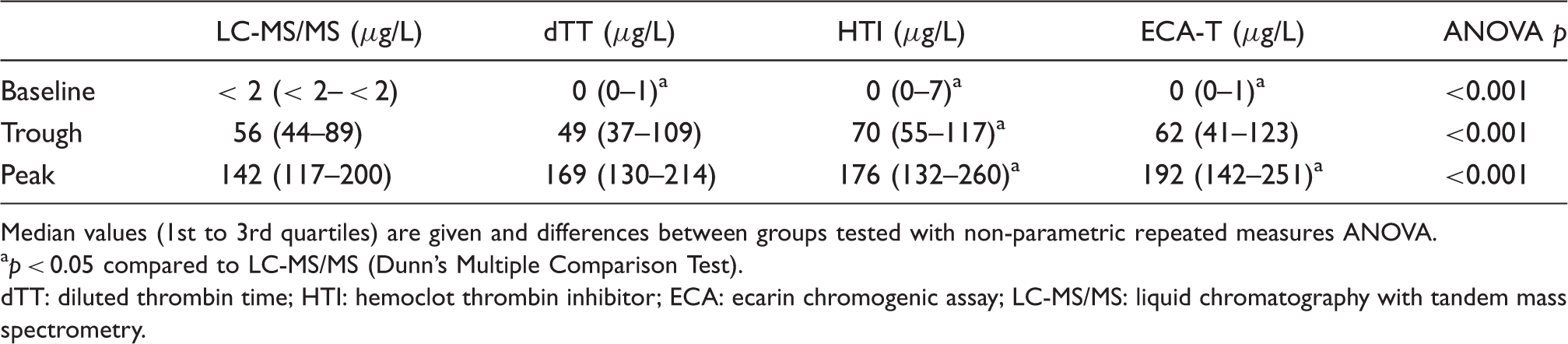
Median values (1st to 3rd quartiles) are given and differences between groups tested with non-parametric repeated measures ANOVA.
p < 0.05 compared to LC-MS/MS (Dunn’s Multiple Comparison Test).
dTT: diluted thrombin time; HTI: hemoclot thrombin inhibitor; ECA: ecarin chromogenic assay; LC-MS/MS: liquid chromatography with tandem mass spectrometry.
Discussion
In this study, a dTT assay that utilizes the same thrombin reagent used in traditional thrombin time measurements is presented. The analysed dTT assay was accurate and reproducible, particularly for detecting plasma dabigatran concentrations below 100 µg/L.
The dTT assay presented in this study showed a wide range of linearity, similar to the traditional thrombin time. 1 The within- and between-run imprecision (all CVs < 10%) and the accuracy (<3%) of the dTT were satisfactory and comparable to previously reported imprecisions of HTI 10 and ECA-T. 11 In ex vivo plasma samples dTT correlated highly with the LC-MS/MS. Identical correlation has been reported for dTT that utilized a different reagent and analyser than in our study. 12 Correlation coefficients of HTI and ECA-T were also high and comparable to previously reported coefficients.3,7 However, for dabigatran concentrations below 100 µg/L, dTT in our study correlated significantly better to LC-MS/MS than HTI and ECA-T. In addition, dTT was the only assay without a systemic bias in the low to intermediate range as shown on the Bland–Altman graph (Figure 2). Good performance of dTT was corroborated with its significantly lower LoD (2.8 µg/L) and LoQ (8.2 µg/L). For HTI, the LoD given by the manufacturer was 30 µg/L, while in two studies the LoD of 22 µg/L 7 and 43.5 µg/L 4 was reported. The assay has been described as unreliable in the lower range despite the introduction of an additional zero calibrator. 7 For ECA-T, one study reported the LoD of 15.3 µg/L, 4 while the correlation coefficient between ECA-T and LC-MS/MS for dabigatran levels below 50 µg/L was similar to ours. 3 The study by Schmitz et al. 4 reported LoD for the in-house modified Stago thrombin time method of 17.4 µg/L. Superior accuracy of dTT in the low to intermediate dabigatran range reported here could be attributed to the lower plasma dilution factor (1:12 in dTT compared to 1:24 in HTI) that resulted in lower final dilution of the assay mixture (1:22 in dTT and 1:40 in HTI), which resulted in significantly longer, but still acceptable clotting times of the dTT assay (Figure 1). The role of the dilution factor is corroborated with the recent report on improved accuracy of the modified HTI assay in which a lower plasma dilution factor (1:10 instead of 1:40) and specific calibrators at lower concentrations are used for samples with dabigatran concentration of ≤ 200 µg/L. 13 Although the dilution factor is even higher in the ECA-T assay (1:59), this assay cannot be directly compared to dTT or HTI, since it is a chromogenic and not a clotting assay. For the in-house modified Stago thrombin time the same dilution factor was used as in HTI assay.11,14
At baseline, trough and peak plasma samples, we have shown that HTI significantly overestimated trough and peak levels, ECA-T significantly overestimated peak, but not trough levels, while no significant deviation was noted for dTT at either trough or peak. It has previously been proven that HTI reflects free dabigatran levels, while ECA-T reflects total dabigatran, the latter being on average 20% higher due to pharmacologically active dabigatran acylglucuronides. 15 Since the concentration of free dabigatran was highly predictable from the total dabigatran and was easier to measure (no need for alkaline hydrolysis), it was concluded that free dabigatran concentrations provide the relevant information needed for the monitoring of dabigatran treatment. 15 In both the previous 15 and the present study, the regression slopes between free dabigatran and HTI were close to 1 and for ECA-T close to 1.2. We therefore expected similar trough and peak HTI values reflecting free dabigatran levels measured with the LC-MS/MS and 20% higher ECA-T values reflecting total dabigatran. However, it was not so in the low to intermediate range. The regression slope of HTI in this range rose from 1.0 to 1.2, and average trough HTI was overestimated compared to LC-MS/MS. For ECA-T, an overestimation of around 20% was expected and confirmed for peak levels, but in the low to intermediate range the overestimation was lower than expected (10%, Table 2). The discrepancies found require further elucidation, but they may lie in the imprecision of the HTI and ECA-T. For dTT, however, both the regression slope of 1 (whole and low to intermediate range) and comparable trough and peak values confirmed that dTT reliably detects free dabigatran levels. At baseline all functional assays significantly differed from LC-MS/MS measurements, but these differences can be attributed to mathematical conversions of very low or negative values needed for statistical analysis.
This study has some limitations. Firstly, only one combination of reagent and analyser at a single site has been tested. The same protocol may not be applicable to other analysers. Secondly, we used NPP prepared in-house. This may not be possible for many laboratories. However, commercially available NPP can be used in the dTT assay, yielding slightly longer coagulation times (data not shown).
This study also has strengths. We performed our study on real-world patients, not on healthy individuals or in vitro-spiked plasma samples. The number of patients/samples is also relatively high compared to other published studies.
In conclusion, the results of our study showed high accuracy and good reproducibility with wide range of linearity of the dTT assay. It was shown to be superior to HTI for measuring trough dabigatran levels.
Footnotes
Declaration of conflicting interests
JPA has received speaker’s honoraria from Siemens and Stago. Other authors declare no conflict of interest related to this work.
Funding
The study was supported by the Slovenian Research Agency (Grant No. P3-0308).
Ethical approval
Slovene National Medical Ethics Committee approved this study (REC number 123/04/13).
Guarantor
MBM.
Contributorship
MBM, NV and AM researched literature and conceived the study. MBM, PŠ and AM developed protocol and gained ethical approval. PŠ, NV and AM recruited patients and analysed patient data. MBM, REM, PM and JPA analysed samples and the data. MBM wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.